arthroscopic treatment for primary hip osteochondromatosis
TRANSCRIPT

2nd International Hip Meeting2nd International Hip MeetingHomburg Homburg 20062006
Arthroscopic treatment for primary hip osteochondromatosis.
Review andReview and Results Results about 147 casesabout 147 cases
T. Boyer, H. DorfmannParis
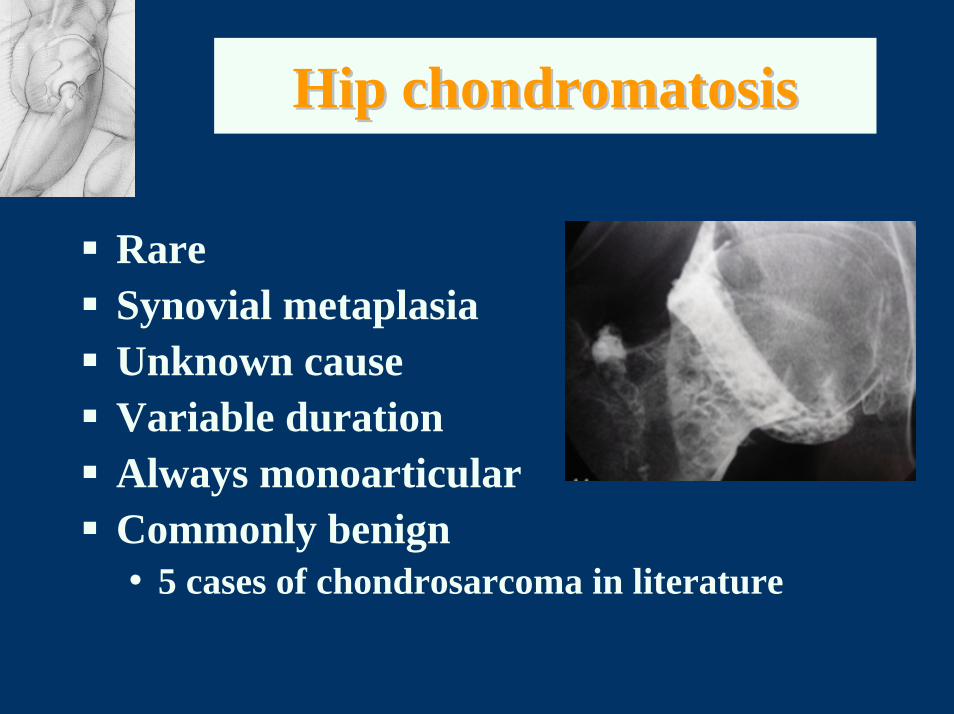
Hip Hip chondromatosischondromatosis
RareSynovial metaplasiaUnknown cause Variable durationAlways monoarticularCommonly benign• 5 cases of chondrosarcoma in literature

Synovial Synovial metaplasiametaplasia
ChondromasChondromasFreeFree PedunculatedPedunculated EmbeddedEmbedded

LiteratureLiteratureClinical Clinical datadata
Age: 20-40 Y.OMen > WomenSlow and unforseeable evolutionAsymptomatic at the beginingLate stiffness• Loose bodies ++• osteoarthritis

ImagingImaging
Plain X rays normal if chondroms (non ossified) 20%Opaque images if osteochondromsArthro CT scan or arthro MRI+++MRI ±
QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.

TreatmentTreatment
Classicaly• Open synovectomy• Loose bodies removal (arthrotomy)
Arthroscopy

Materials and methodsMaterials and methods
Materials
Cohort of 111 primary(osteo)-chondromatosis
147 Arthroscopies

MethodsMethods
Retrospective studyWritten inquiry• Satifactory scale• VAS • Articular mobility
Follow-up Average 78.6 months (12-196)

ProcedureProcedure
Peripheral compartmentCombined Central

ProcedureProcedure
Choice of the technique
Peripheral Combined Central

Peripheral Peripheral techniquetechnique
QuickTime™ et un décompresseu sont requis pour visualiser
cette image.

Procedure Procedure ((PeripheralPeripheral))
Succion by cannulaGraspersFragmentation
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

Procedure Procedure ((PeripheralPeripheral))
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur Codec YUV420
sont requis pour visionner cette image.

Procedure Procedure ((PeripheralPeripheral
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

Ilio femoral approachIlio femoral approach
QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.
QuickTime™ et un décompresse sont requis pour visualiser
cette image.

Iliofemoral Iliofemoral techniquetechnique

ProcedureProcedure
QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.
Classical central approach. 2 or 3 portalsDepends localization
QuickTime™ et undécompresseur Codec YUV420
sont requis pour visionner cette image.

MethodsMethodsAnalyse of Analyse of the resultsthe results
Excellent : >75% subjective improvementNo pain . Normal mobility
Good : > 50% subjective improvementLow pain. Normal mobility
Failure : < 50%, pain or loss of mobility
QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.
The cohortThe cohort1985 - 2002

CohortCohort
120 patients. 9 lost111 patientsSex ratio: 54 Men / 57 WomenRight Hip: 63 - Left: 48
Clinical Clinical patternspatterns
Age average: 40.9 YOAverage duration of symptoms before AS: 31 monthsProgressive : 70%Sudden: 23.3%Fortuitous discovery (Xrays) : 6.7%
PainPain
Type:Méchanic : 93%Inflammatory or mix : 7%
Rythm:Intermittent : 84%Continuous : 16%

Clinical presentationClinical presentation
Loss of motion : 51%Limping : 10%Normal: 39%

Imaging Imaging contributioncontribution((X rays,X rays,AgraphyAgraphy, , ACTscannACTscann, MRI), MRI)
Diagnosis + : 71/111 (56 osteochondromatosis)Suspected diagnosis: 32No diagnosis: 8

Type of Type of chondromaschondromas
Chondromas (Non-ossified) : 45%
Chondromas + OstéoCh : 26%
Osteochondromas : 23%
Intrasynovial (osteo)chondromas : 6%

Types of Types of ChondromasChondromas
Rice-like: 33%
Agglomerate mass : 30%
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

Wafer Wafer into the fossa into the fossa
« Wafers » : 5%
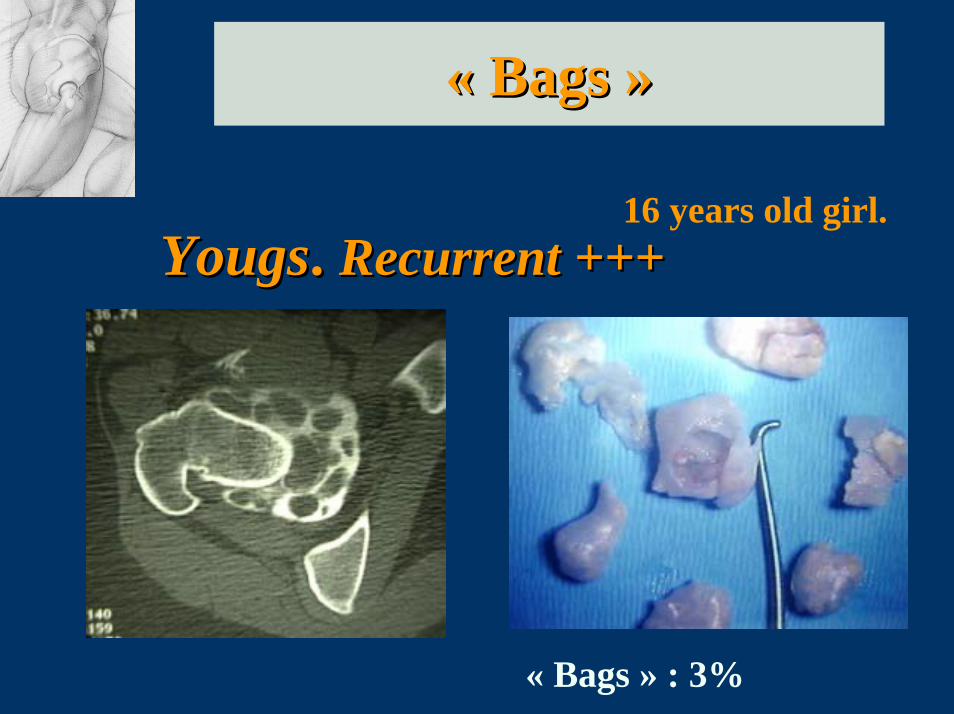
«« BagsBags »»
16 years old girl.YougsYougs. . Recurrent Recurrent ++++++
« Bags » : 3%

Particular Particular cases cases
QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.
QuickTime™ et undécompresseur Codec YUV420
sont requis pour visionner cette image.
V
Sometimes the jointis completely full ofchondromas

Particular Particular casescases
Re-arthroscopyModifications of chondromas
QuickTime™ et un décompresseurPhoto - JPEG sont requis pour visualiser
cette image.
1st arthroscopy 6 months later

Osteochondromas Osteochondromas ( 49%)( 49%)
Size• 2 to 25 mm
Location • Peripheral ++• Iliofemoral • Both• Psoas bursae QuickTime™ et un
décompresseur TIFF (LZW)sont requis pour visionner cette image.
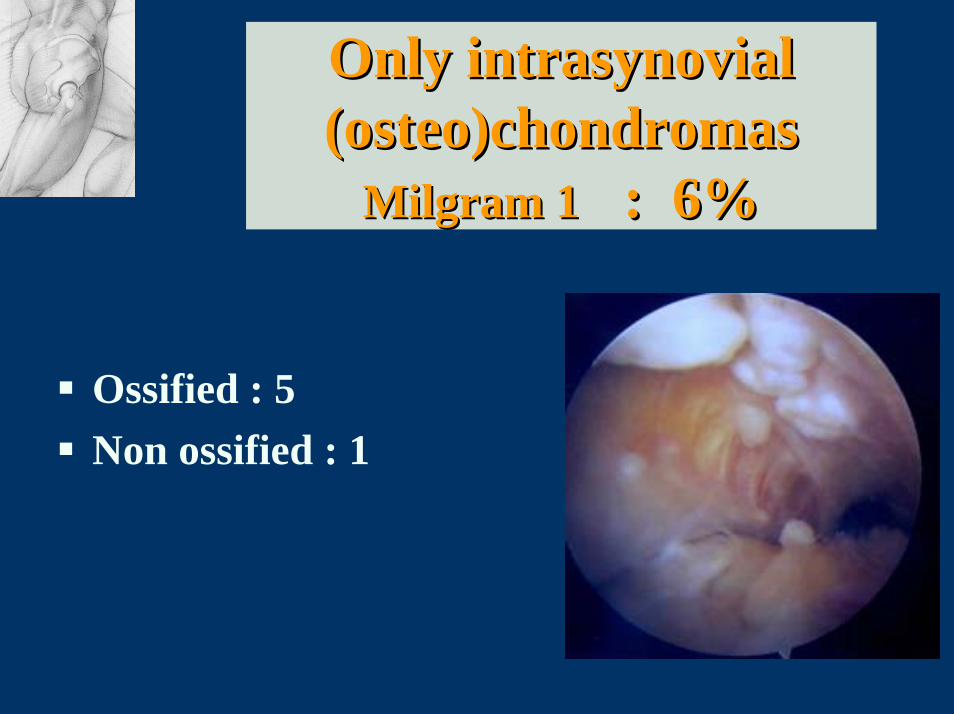
Only intrasynovial Only intrasynovial ((osteoosteo))chondromaschondromas
Milgram Milgram 11 : : 6%6%
Ossified : 5Non ossified : 1
Global Global resultsresultsMean FollowMean Follow--up up 78.6 78.6 mo mo ( 12 ( 12 -- 196 )196 )
Excellent result • Subjective> 75%• Normal motion • No pain
Improved• Subjective> 50% • Motion quite normal • No or low pain
Failure • Subjective< 50%• Loss of motion
Secondary surgery

ResultsResults
3 groups• 69 patients: only one arthroscopy• 24 patients : re-arthroscopies• 42 patients : secondary open surgery
• NB: total > 111 patients
Single Single arthroscopy arthroscopy 69/111 69/111 (62.2%)(62.2%)
Excellent results : 36%Improvement : 20.8%Failure : 5.4%

ReRe--arthroscopies arthroscopies 24/111 24/111 (21.6%)(21.6%)
No secondary open surgery : 17% (19 patients)• Excellent final result : 8%• Improvement : 8%• Failure : 1%
Open surgery (4.6%)• Arthroplasty : 2• Synovectomy and loose bodies : 3
ResultsResults: patients : patients with with a a secondary secondary open open surgery surgery
(37.8%)(37.8%)
• Total hip replacement : (17.1%)• Surgical synovectomy : 10.8%• Micellaneous : 9.9%

DiscussionDiscussion
Literature:• no arthroscopic series• Isolated cases: Elmali, Okada, Witwity,
Dienst, Gouin.Arthroscopy / Arthrotomy• Schoeniger : open synovectomy. 8 cases
Secondary arthroplasty: 25%

Summary Summary (1)(1)
Think chondromatosis in front of a painful hip with normal X raysGood sensibility of the imagingImaging indicates the procedureFrequency of the false positives
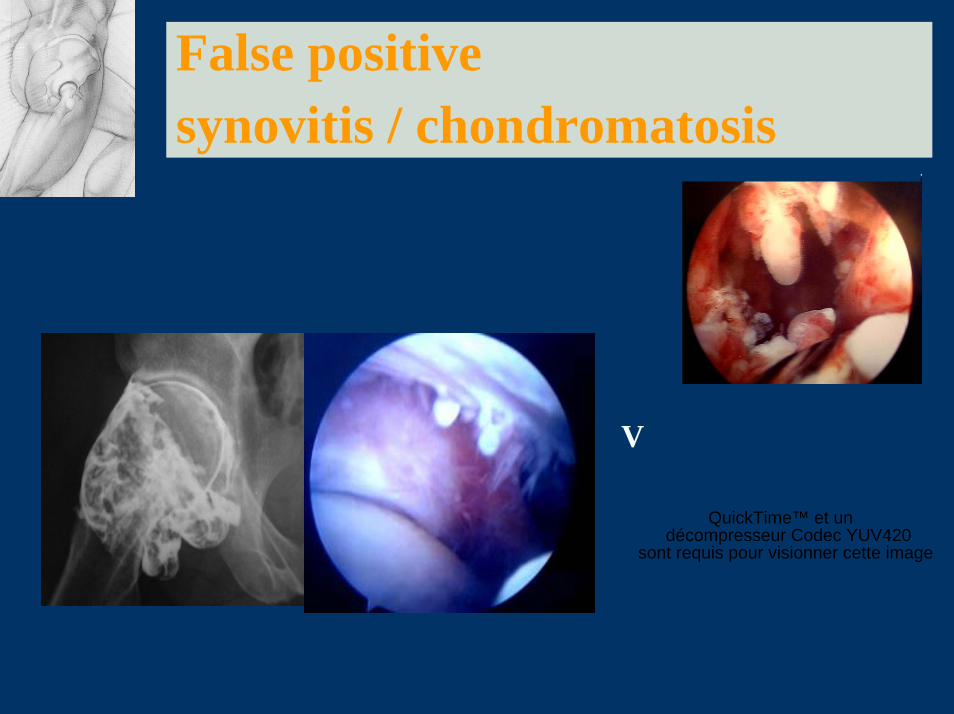
False positive synovitis / chondromatosis
QuickTime™ et undécompresseur Codec YUV420
sont requis pour visionner cette image.
V

Summary Summary (2)(2)
Quite all the loose bodies can be removed
The intrasynovial chondromas can’t be removed
Synovectomy is difficult anduncomplete

Summary Summary (3)(3)
In our cohort the arthroscopic treatment underwent 56.8% of excellent results or improvement with a single arthroscopy and72.8% with re-arthroscopy
17% of patients had a secondary arthroplasty

2ND International Hip Meeting2ND International Hip MeetingHomburg November Homburg November 20062006
Synovial pathologyPectineo-foveal impingement
Thierry BOYERParis

Synovial Synovial pathologypathology
•Rhumatoïd Arthritis•Pigmented villonodular synovitis•Osteoarthritis •Cysts

Synovial Synovial pathologypathology
Peripheral compartmentAnterolateral portals ++
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

OsteoarthritisOsteoarthritis
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

OsteoarthritisOsteoarthritis
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

Villonodular synovitisVillonodular synovitisDiffuseDiffuse formform
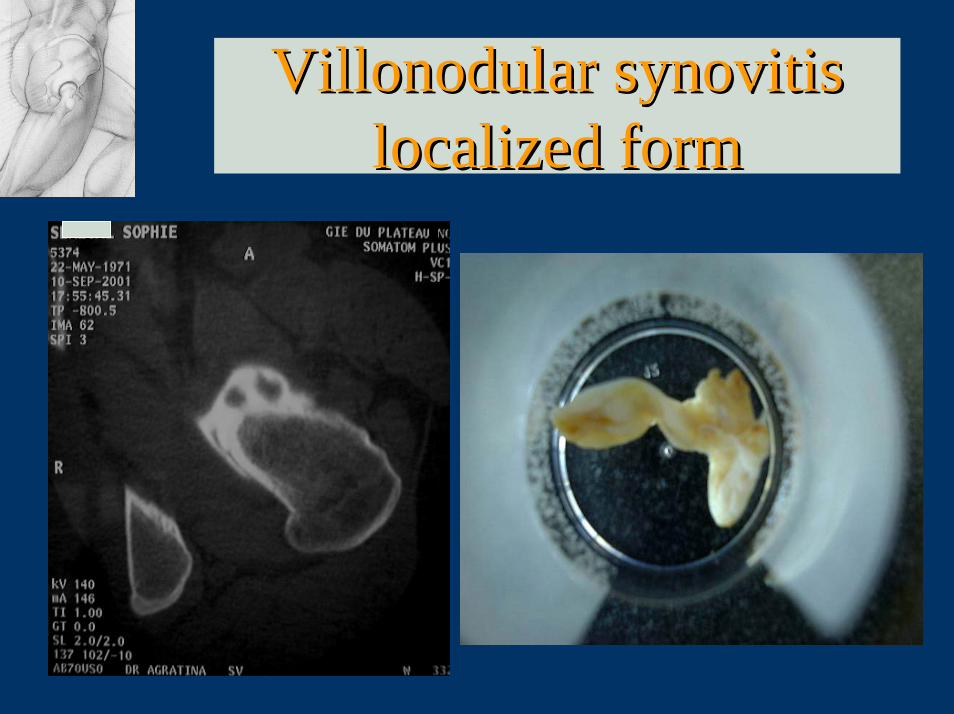
Villonodular synovitisVillonodular synovitislocalized formlocalized form

Villonodular synovitisVillonodular synovitis
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

Rhumatoid arthritisRhumatoid arthritis
Synovitis is usely controledby medical treatment andinjections.
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

PeriPeri--labral cystslabral cysts
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.

PectineoPectineo--foveal impingement foveal impingement (?)(?)
Pectineofoveal fold
Hypothesis: painful pathology of the pectineofoveal fold linked to a medial mechanical impingement of the hip

Pectineofoveal « impingement » (?)
1-Study on cadavers (contrast CT and MRI)
2-Results of arthroscopic resection of « pathological » pectineofoveal fold
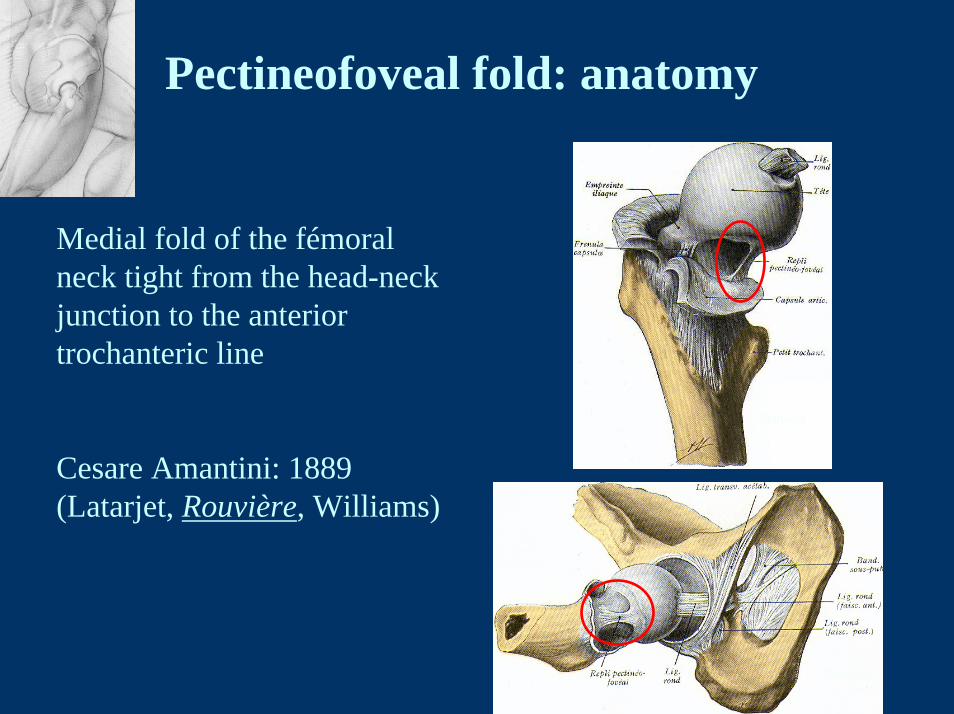
Pectineofoveal fold: anatomy
Medial fold of the fémoral neck tight from the head-neck junction to the anterior trochanteric line
Cesare Amantini: 1889(Latarjet, Rouvière, Williams)
Rouvière
Rouvière

Pectinéofovéal fold: anatomyDissection of 10 unembaumed corpses: constant fold
Description on anatomical section ( O May CHU Lille)

Correlation corpes/ injected MRI and tomography
(Slides reconstructed according to axis of the femoral neck)
Pectinéofovéal fold: anatomy

Pectineofoveal fold
Arthroscopic resection: 12 cases
All patients underwent arthroscopy for unexplained pain
Groin pain in flexion-rotation
Preoperative imaging(Xrays, contrast CT sometimes contrast MRI)was either normal, or suspected a labral tear.
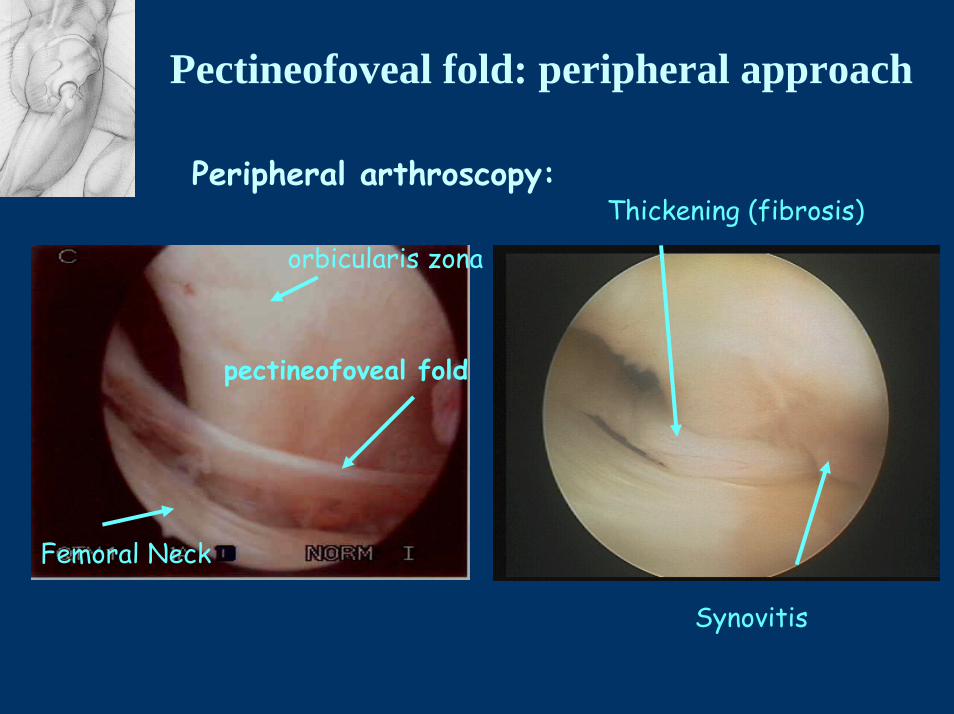
Pectineofoveal fold: peripheral approach
Peripheral arthroscopy: Thickening (fibrosis)
Femoral Neck
orbicularis zona
pectineofoveal fold
Synovitis

Pectineofoveal fold
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
Flexion

Pectineofoveal fold
Material and method
-Retrospective study (medical files, surgical reports)
-All patients were contacted to fill a questionnaire (sports/level, occupation, symptoms before and after surgery
-10 of 12 patients were consulted

Pectineofoveal fold: results
-7 women, 5 men, mean age 26.8 YO
Analysis : 2 groups

Pectineofoveal fold: results
GROUP 1 : homogeneous population (7)
Appeared during a sport practice, obliging to reduce or stop itNormal imaging
Mechanical hip pain in flexion-rotation movements
Arthroscopy :
• on average 20 months after the beginning of pain• ISOLATED « pathological » fold

Pectineofoveal fold: resultsGROUP 2 (5) No homogeneous population
No sportPain associated with-Snapping tendon-Labral tear-Dysplasia of the hip
Arthroscopy :• on average 4.8 years after the beginning of pain• “pathologic” pectineofoveal fold : not isolated
Pectineofoveal fold
Results
GROUP 1: Excellent and good results after arthroscopyAll patients returned to sport with the same level (1 professional)
GROUP 2: Poor resultsOnly one patient was transitorily improved
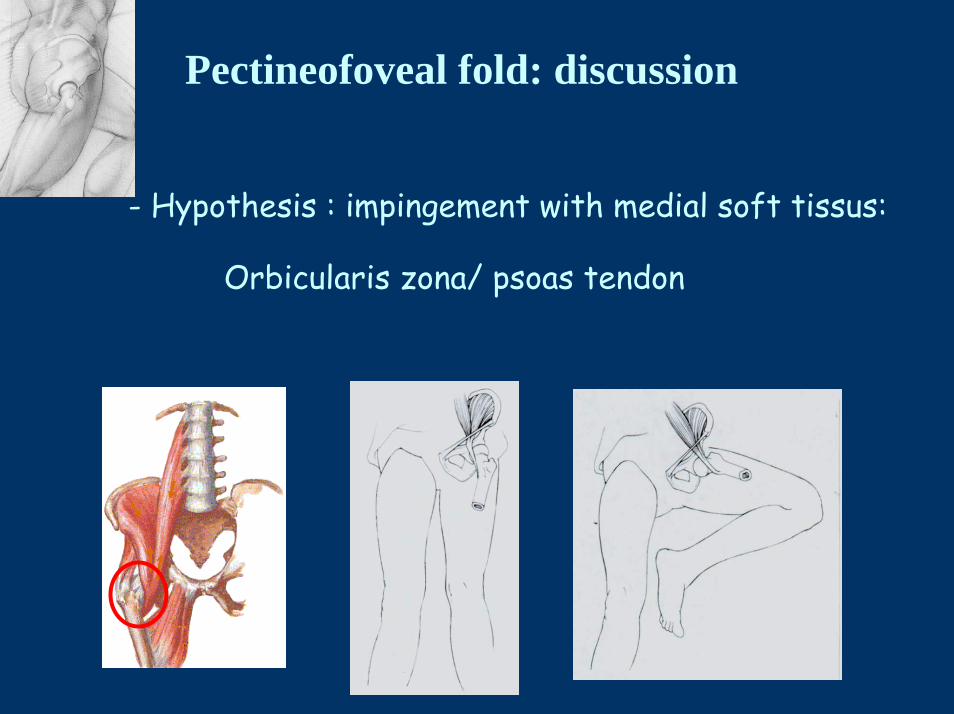
Pectineofoveal fold: discussion
- Hypothesis : impingement with medial soft tissus:
Orbicularis zona/ psoas tendon

Pectineofoveal fold: discussionAnatomic link between pectineofoveal
fold and psoas tendon via orbicularis zona
The fold could be rubbed down against the femoral neck due to intense practice of sports ?
Synovitis
QuickTime™ et undécompresseur codec YUV420
sont requis pour visionner cette image.
Bursoscopy

Pectineofoveal fold: discussion
- Probably rare
- Young sportmen
- Isolated hip pain
- Negative imaging

Pectineofoveal fold: discussion
During arthroscopy for mechanical unexplained pain,the association:
Thick pectineofoveal fold
Synovitis
Normal exploration of the joint (cartilage, labrum)
should lead to arthroscopic resection of the pectineofoveal fold
To be confirmed

QuickTime™ et undécompresseur TIFF (LZW)
sont requis pour visionner cette image.