arterial stiffness in obstructive sleep apnea
TRANSCRIPT

Journal of Sleep Medicine & Disorders
Cite this article: Balanis T, Sanner B (2016) Arterial Stiffness in Obstructive Sleep Apnea. J Sleep Med Disord 3(7): 1070.
Central
*Corresponding authorThomas Balanis, Department of Medicine, Agaplesion Bethesda Krankenhausg, GmbH, Hainstrasse 35, 42109 Wuppertal, Germany, Tel: 49-202-290- 2002; Fax: 49-202-290-2005; Email:
Submitted: 18 October 2016
Accepted: 05 November 2016
Published: 11 November 2016
ISSN: 2379-0822
Copyright© 2016 Balanis et al.
OPEN ACCESS
Keywords•Obstructive sleep apnea•Hypopnea•Arterial stiffness
Review Article
Arterial Stiffness in Obstructive Sleep ApneaThomas Balanis* and Bernd SannerDepartment of Medicine, Agaplesion Bethesda Krankenhaus Wuppertal, Germany
Abstract
Obstructive sleep apnea is a very common disease and is associated with an increased risk of cardiovascular disease, cardiac arrhythmia, and stroke. Arterial stiffness is an emerging risk factor and may be involved in the cardiovascular complications of obstructive sleep apnea. The purpose of this review was to demonstrate the correlation between arterial stiffness and obstructive sleep apnea. Arterial stiffness was increased in obstructive sleep apnea patients compared to controls or increased in severe compared to mild sleep apnea. Although there are relatively few interventional studies that have incorporated a control group, there are two randomized trials showing short-term improvements in arterial stiffness with CPAP treatment. Obstructive sleep apnea seems to play an essential role in arterial stiffness, which may be one of the mechanisms accounting for sleep apnea-associated cardiovascular risk.
INTRODUCTIONObstructive sleep apnea (OSA)-also referred to as obstructive
sleep apnea-hypopnea-is a sleep disorder that involves cessation or significant decrease in airflow in the presence of breathing effort. It is the most common type of sleep-disordered breathing and characterized by recurrent episodes of upper airway collapse during sleep. These episodes are associated with recurrent oxyhemoglobin desaturations and arousals from sleep. OSA patients frequently have several risk factors for cardiovascular disease development, such as obesity, hypertension, and diabetes. Although OSA patients commonly demonstrate one or more established cardiovascular risk factors, there is now a considerable body of evidence indicating that OSA itself is an independent cardiovascular risk factor [1,2]. OSA has been linked to the development of atherosclerosis. In a study of 36 subjects [3] with OSA and 16 matched controls, all without comorbidities, subjects with moderate-to-severe OSA were found to have increased carotid intima-media thickness, increased pulse wave velocity, and increased carotid diameter, all of which are consistent with atherosclerosis. Abnormalities in these parameters were predicted by either the apnea-/hypopnea index or the degree of nocturnal desaturation.
DEFINITIONArterial stiffness is an early marker of atherosclerosis, as it
sets in at an earlier stage than a change in intima-media thickness (IMT) in patients with vascular disease. It increases chronically with age, with the development of chronic conditions (eg. hypertension), and with the presence of vascular risk factors (e. g. smoking) [4,5]. Arterial stiffness determines how quickly the pulse wave generated by the contracting heart travels to the periphery and is reflected from there. The larger arteries of the
cardiovascular system are critical in the conduction of blood flow to the periphery. The elastic properties of these vessels, which are dependent on the stiffness of the arterial walls, allow for the smoothing of oscillations in blood pressure, reduction of the pulse pressure, and perfusion of the myocardium [6,7]. Central pressure and arterial stiffness offer an accurate estimation of the load imposed on the coronary arteries, cerebral arteries, and aorta, and, in turn, of overall vascular damage and prognosis [8-11]. The way in which arterial stiffness leads to heart failure is depicted in Figure (1).
Arterial stiffness can be measured noninvasively by applanation tonometry, echotracking, and Doppler ultrasound. These techniques have very good reproducibility and been widely applied [12]. The most simple and reproducible noninvasive technique to date is the measurement of arterial waveforms (obtained by applanation tonometry), and more specifically pulse wave velocity (PWV), as recommended by the European Network for Non-invasive Investigation of Large Arteries [13] and the European Society of Hypertension and the European Society of Cardiology [14] (Figure 2). PWV is inversely related to arterial distensibility [13] and expresses the speed of the pressure wave traveling through the arteries. The pulse travels at a higher velocity in a stiff artery, and vice versa. Carotid-femoral PWV (cfPWV) is considered the ‘gold-standard’ measurement of the stiffness of the aorta [14,12].
It has been used extensively and has the largest amount of epidemiological evidence to support its predictive value for cardiovascular events in the general and in the diseased populations. Measurements of arterial stiffness are believed to reflect global arterial endothelial function [15,16]. A strong correlation between arterial stiffness and the development of atherosclerosis at various sites in the arterial tree has been noted [17-19].
Balanis et al. (2016)Email:
J Sleep Med Disord 3(7): 1070 (2016) 2/5
Central
These observations have prompted researchers investigating OSA- cardiovascular interactions to study the role of OSA in increasing arterial stiffness.
PATHOPHYSIOLOGYA number of mechanisms could explain the role of OSA in
increasing arterial stiffness. Inflammation, oxidative stress, and sympathetic activity affect endothelial function and are all altered in patients with OSA [20,2]. Intermittent hypoxia is associated with increased production of reactive oxygen species, and therefore, increases oxidative stress [21,22]. Increased inflammation may play a role in the pathogenesis of OSA, increasing arterial stiffness and contributing to the early atherosclerosis found in OSA patients. Several reports consistently showed that OSA is
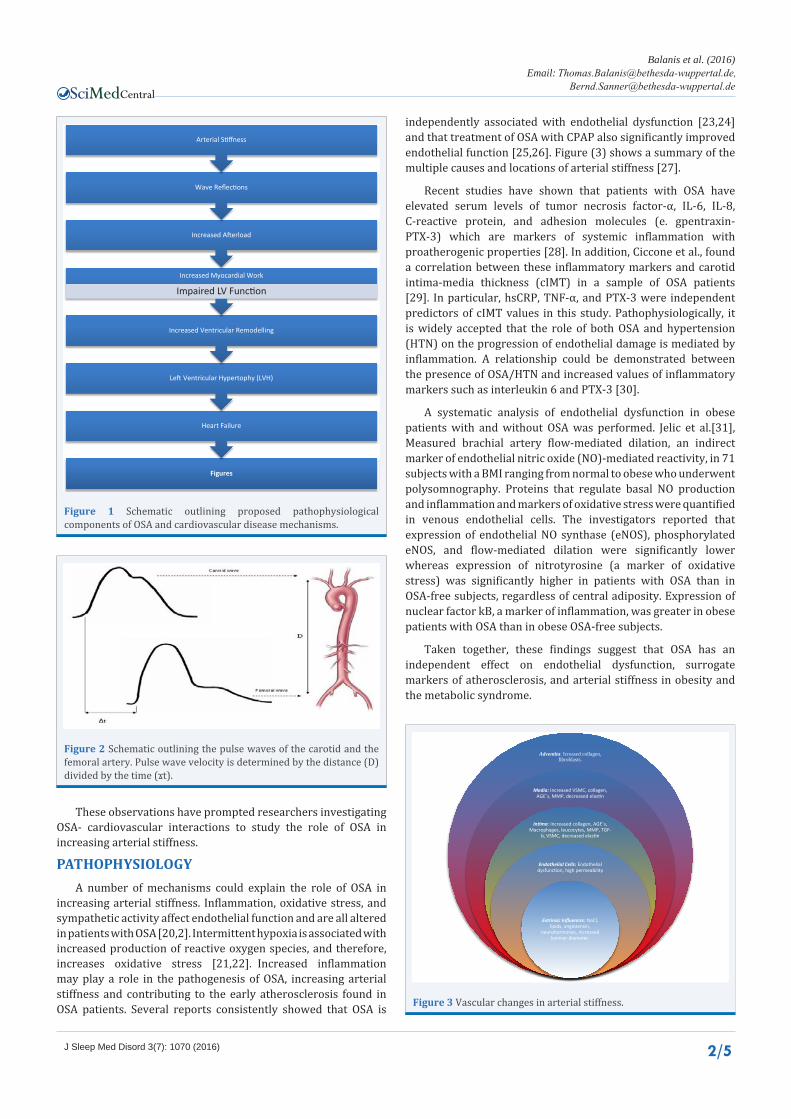
independently associated with endothelial dysfunction [23,24] and that treatment of OSA with CPAP also significantly improved endothelial function [25,26]. Figure (3) shows a summary of the multiple causes and locations of arterial stiffness [27].
Recent studies have shown that patients with OSA have elevated serum levels of tumor necrosis factor-α, IL-6, IL-8, C-reactive protein, and adhesion molecules (e. gpentraxin-PTX-3) which are markers of systemic inflammation with proatherogenic properties [28]. In addition, Ciccone et al., found a correlation between these inflammatory markers and carotid intima-media thickness (cIMT) in a sample of OSA patients [29]. In particular, hsCRP, TNF-α, and PTX-3 were independent predictors of cIMT values in this study. Pathophysiologically, it is widely accepted that the role of both OSA and hypertension (HTN) on the progression of endothelial damage is mediated by inflammation. A relationship could be demonstrated between the presence of OSA/HTN and increased values of inflammatory markers such as interleukin 6 and PTX-3 [30].
A systematic analysis of endothelial dysfunction in obese patients with and without OSA was performed. Jelic et al.[31], Measured brachial artery flow-mediated dilation, an indirect marker of endothelial nitric oxide (NO)-mediated reactivity, in 71 subjects with a BMI ranging from normal to obese who underwent polysomnography. Proteins that regulate basal NO production and inflammation and markers of oxidative stress were quantified in venous endothelial cells. The investigators reported that expression of endothelial NO synthase (eNOS), phosphorylated eNOS, and flow-mediated dilation were significantly lower whereas expression of nitrotyrosine (a marker of oxidative stress) was significantly higher in patients with OSA than in OSA-free subjects, regardless of central adiposity. Expression of nuclear factor kB, a marker of inflammation, was greater in obese patients with OSA than in obese OSA-free subjects.
Taken together, these findings suggest that OSA has an independent effect on endothelial dysfunction, surrogate markers of atherosclerosis, and arterial stiffness in obesity and the metabolic syndrome.
Figures
Heart Failure
Left Ventricular Hypertophy (LVH)
Increased Ventricular Remodelling
Increased Myocardial Work
Impaired LV Function
Increased Afterload
Wave Reflections
Arterial Stiffness
Figure 1 Schematic outlining proposed pathophysiological components of OSA and cardiovascular disease mechanisms.
Figure 2 Schematic outlining the pulse waves of the carotid and the femoral artery. Pulse wave velocity is determined by the distance (D) divided by the time (ϫt).
Adventita: Icreased collagen, fibroblasts.
Media: Increased VSMC, collagen, AGE´s, MMP, decreased elastin
Intima: Increased collagen, AGE´s, Macrophages, leucocytes, MMP, TGF-
b, VSMC, decreased elastin
Endothelial Cells: Endothelialdysfunction, high permeability
Extrinsic Influences: NaCl,lipids, angiotensin,
neurohormones, increased luminar diameter.
Figure 3 Vascular changes in arterial stiffness.

Balanis et al. (2016)Email:
J Sleep Med Disord 3(7): 1070 (2016) 3/5
Central
Dates of arterial stiffness in obstructive sleep apnea
Namtvedt et al., reported a positive association between severity of OSA and impaired endothelial function, independent of obesity and other cardiovascular risk factors [32]. Regarding surrogate markers of atherosclerosis and arterial stiffness, a previous investigation found that patients with both metabolic syndrome and OSA had higher values of pulse wave velocity. The apnea-/hypopnea index was independently associated with impairments in pulse wave velocity (PWV) [33]. Several studies evaluated central arterial stiffness by measuring cfPWV. Tsioufis et al.[34], found a higher cfPWV in OSA patients compared to controls. Drager et al.[35], noted that although cfPWV was higher in OSA patients than in controls, it was even more elevated in OSA patients with hypertension. Another study by the same group compared the cfPWV of non-OSA controls with that of a mild-to-moderate OSA group and with a severe OSA group [36]. Although they did not find the mild-to-moderate group to significantly differ from either the controls or the severe OSA group, they did note a significant difference between patients with severe OSA and non-OSA participants. A further study by Drager et al.[37], examined the effect of the presence of OSA on arterial stiffness in patients with metabolic syndrome. They found cfPWV to be significantly higher in the presence as compared to the absence of OSA in these patients. Moreover, there was a significant positive correlation between cfPWV and AHI [37].
Protogerou et al.[38], determined carotid intima-media thickness (IMT), carotid diameter and plaques, carotid-femoral pulse wave velocity (cfPWV), central augmentation index (AI), and central blood pressures in mild, moderate and severe OSA patients. It was found that the severity of OSAS, expressed as respiratory disturbance index (RDI), was a predictor of two of the most commonly used and well-established markers of
cardiovascular risk: carotid IMT and carotid-femoral PWV. This relation was independent of age and cardiovascular risk factors. As far as the other parameters are concerned, e.g. carotid plaques, carotid diameter, AI, central blood pressures, they were not significantly associated with the severity of OSAS as expressed by RDI or other nocturnal hypoxaemiaindices. Several studies used ultra sonographic methods to evaluate arterial stiffness in OSA patients. Tanriverdi et al.[39], found that the stiffness index of OSA patients was higher as compared to control patients, and that aortic distensibility was lower than in control patients. They also noted a correlation between aortic stiffness and RDI as well as a negative correlation between RDI and distensibility. Kasikcioglu et al.[40], found decreased aortic distensibility and increased stiffness index in OSA patients compared to controls. Table (1) lists the various studies investigating the association between OSA and arterial stiffness.
Effects of continuous positive airway pressure treatment on arterial stiffness
The effects of CPAP therapy on the early signs of atherosclerosis are multi factorial and associated with improvements in inflammation and sympathetic activity. Kohler et al.[41], randomized 102 male OSA patients to 4 weeks of therapeutic or sub therapeutic effects of continuous positive airway pressure (CPAP). They noted a decrease in augmentation index (Aix) in the therapeutic group compared to a slight, non-significant increase in the sub therapeutic group. They also tested the sensitivity of the baroreflex, and found significant improvements following only therapeutic CPAP. The authors hypothesized that CPAP may improve arterial stiffness by acting upon baroreflex sensitivity. Drager et al.[42], performed a similar study with 4 months of CPAP, examining cfPWV, which is the ‘gold standard’ for arterial stiffness measurements. The CPAP group had a decrease in cfPWV,
Table 1: Studies investigating the association between OSA and arterial stiffness.
Author Study population Comparedgroups Arterial stiffness – analyzed parameter Result
Drager et al. [36]OSA:
sleep cliniccontrol: hospital staff
severe OSA vs. mild/moderate OSA vs. control c-f PWV severe OSA> mild/moderate OSA
> control
Drager et al. [35]OSA:
sleep clinic htn&control: staff/relatives
OSA with htn vs. OSA without htn c-f PWV
OSA withhtn>OSA without htn
Drager et al. [37] heart institute MS with OSA vs. MS without OSA c-f PWV MS with OSA >
MS without OSA
Kasikcioglu et al. [40] sleep clinic OSA vs. control aortic stiffness index,aortic distensibility
OSA > controlOSA < control
Kohler et al. [41]
OSA:sleep clinic
control:GP database
OSA vs. control AIX OSA > control
Protogerou et al. [38] sleep clinicvery severe OSA(RDI>50/h) vs. severe OSA (RDI 31-50/h) vs.
mild OSA (RDI 10-30/h)c-f PWV No group differences
Tanriverdi et al. [39] sleep clinic OSA vs. control aortic stiffness index,aortic distensibility
OSA > controlOSA < control
Tsioufis et al. [34] htn clinic with OSA symptoms
htn with OSA vs.htn without OSA c-f PWV htn with OSA >
htn without OSAAbbreviations: OSA: Obstructive Sleep Apnea; htn: Hypertension; GP: General Practitioner; MS: Metabolic Syndrome; AIX: Augmentation Index; c-fPWV: Carotid-Femoral Pulse Wave Velocity; RDI: Respiratory Disturbance Index

Balanis et al. (2016)Email:
J Sleep Med Disord 3(7): 1070 (2016) 4/5
Central
Table 2: Continuous positive airway pressure treatment and arterial stiffness.
Author Study group Post treatment follow-up
Arterial Stiffness Outcome Result
Drager et al. [42] OSA randomized to CPAP or control 4 months c-f PWV CPAP: decreased by 1.1 +/- 0.6 m/s. control: no change.
Kato et al. [23] moderate vs. severe OSA 1 month c-a VI decreased at 1 mo
Kohler et al. [41]moderate to severeOSA randomized to therapeutic vs. sub-therapeutic CPAP
1 month AIX decreased on therapeutic CPAP. No change on sub-therapeutic CPAP.
Ciccone et al. [44]OSA randomised to CPAP therapy started less and more than 3 months before vs. no CPAP therapy
3 months FMD of the brachial artery
significant reversibility of FMD in patients treated with CPAP therapy for more than 3 months
Abbreviations: c-f PWV: Carotid-Femoral Pulse Wave Velocity; c-a VI: Carotid Artery Vasodilation Index; AIX: Augmentation Index; FMD: Flow Mediated Dilation
C-reactive protein, and catecholamines, whereas changes in the non-CPAP control group were not significant [43]. Interestingly, there were parallel decreases in blood pressure with therapeutic CPAP, which may have accounted for the improvement in arterial stiffness. Furthermore, effective treatment of OSA with CPAP significantly increased flow-mediated dilation and expression of eNOS and phosphorylated eNOS, whereas expression of nitrotyrosine and nuclear factor kB significantly decreased [31].The study of Ciccone et al. showed the effect of CPAP on endothelial function. A non-invasive method to assess endothelial function is flow-mediated vasodilation. Data obtained from this study demonstrate the significant reversibility of flow-mediated vasodilation in patients treated with CPAP for more than 3 months [44]. Finally, in a preliminary single-arm study, Oyama et al.[45], reported that CPAP therapy improved endothelial dysfunction and decreased markers of oxidative stress in patients with the metabolic syndrome and OSA. The results of the studies that examined the influence of CPAP on arterial stiffness are given in Table (2).
CONCLUSIONArterial stiffness is an established independent risk
factor for cardiovascular disease. Many of the risk factors and pathophysiological mechanisms linking arterial stiffness to cardiovascular disease (including obesity and hypertension) are present in OSA patients. Most of the cross-sectional studies examining arterial stiffness in OSA have attempted to control for these known confounders. To the best of our knowledge, arterial stiffness is increased in OSA patients compared with non-OSA control patients. The extent of the increase in arterial stiffness appears to be greater in more severely affected OSA patients and in those with other cardiovascular risk factors, such as hypertension. Therefore, arterial stiffness may have a role in the increased risk of cardiovascular complications in OSA. Although there are relatively few interventional studies that have incorporated a control group, there are two randomized trials showing short-term improvements in arterial stiffness with CPAP treatment. Assessment of arterial stiffness in OSA patients by means of currently available, convenient, and noninvasive methods may be an effective method to also monitor disease progression and treatment efficacy.
REFERENCES1. Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley
P, Laurent S. Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients: a longitudinal study. Hypertension. 2002; 39: 10-15.
2. Ciccone MM, Scicchitano P, Zito A, Cortese F, Boninfante B, Falcone VA, et al. Correlation between inflammatory markers of atherosclerosis and carotid intima-media thickness in obstructive sleep apnea. Molecules. 2014; 19: 1651-1662.
3. Ciccone MM, Favale S, Scicchitano P, Mangini F, Mitacchione G, Gadaleta F, et al. Reversibility of the endothelial dysfunction after CPAP therapy in OSAS patients. Int J Cardiol. 2012; 158: 383-386.
4. Cofta S, Wysocka E, Piorunek T, Rzymkowska M, Batura-Gabryel H, Torlinski L. Oxidative stress markers in the blood of persons with different stages of obstructive sleep apnea syndrome. J Physiol Pharmacol 2008; 59(Suppl 6): 183-190.
5. Damiani MF, Annapaola Zito, Pierluigi Carratù, Vito Antonio Falcone, Elioda Bega, Pietro Scicchitano, et al. Obstructive sleep apnea, hypertension, and their additive effects on atherosclerosis. Biochem Res Int. 2015; 2015: 98419.
6. Drager LF, Bortolotto LA, Figueiredo AC, Krieger EM, Lorenzi GF. Effects of continuous positive airway pressure on early signs of atherosclerosis in obstructive sleep apnea. Am J RespirCrit Care Med. 2007; 176: 706-712.
7. Drager LF, Bortolotto LA, Figueiredo AC, Krieger EM, Lorenzi GF. Effects of continuous positive airway pressure on early signs of atherosclerosis in obstructive sleep apnea. Am J Respir Crit Care Med. 2007; 176: 706-712.
8. Drager LF, Bortolotto LA, Figueiredo AC, Silva BC, Krieger EM, Lorenzi-Filho G. Obstructive sleep apnea, hypertension, and their interaction on arterial stiffness and heart remodeling. Chest. 2007; 131: 1379-1386.
9. Drager LF, Bortolotto LA, Lorenzi MC, Figueiredo AC, Krieger EM, Lorenzi-Filho G. Early signs of atherosclerosis in obstructive sleep apnea. Am J Respir Crit Care Med. 2005; 172: 613-618.
10. Drager LF, Bortolotto LA, Maki-Nunes C, Trombetta IC, Alves MJ, Fraga RF, Negrao CE, Krieger EM, Lorenzi-Filho G. The incremental role of obstructive sleep apnoea on markers of atherosclerosis in patients with metabolic syndrome. Atherosclerosis, 2010; 208: 490-495.
11. Drager LF, egues-Silva L, Diniz PM, Bortolotto LA, Pedrosa RP, Couto RB, Marcondes B, Giorgi DM, Lorenzi-Filho G, Krieger EM. Obstructive sleep apnea, masked hypertension, and arterial stiffness in men. Am J Hypertens. 2010; 23: 249-254.
12. Giuseppe Mancia, Robert Fagard, Krzysztof Narkiewicz, Josep Redon, Alberto Zanchetti, Michael Böhm, et al. Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–1536.
13. Hayward CS, Kraidly M, Webb CM, Collins P. Assessment of endothelial

Balanis et al. (2016)Email:
J Sleep Med Disord 3(7): 1070 (2016) 5/5
Central
Balanis T, Sanner B (2016) Arterial Stiffness in Obstructive Sleep Apnea. J Sleep Med Disord 3(7): 1070.
Cite this article
function using peripheral waveform analysis: a clinical application. J Am Coll Cardiol 2002; 40: 521-528.
14. Imadojemu VA, Gleeson K, Quraishi SA, Kunselman AR, Sinoway LI, Leuenberger UA, et al. Impaired vasodilator responses in obstructive sleep apnea are improved with continuous positive airway pressure therapy. Am J Respir Crit Care Med. 2002; 165: 950-953.
15. Ip MS, Tse HF, Lam B, Tsang KW, Lam WK. Endothelial function in obstructive sleep apnea and response to treatment. Am J Respir Crit Care Med. 2004; 169: 348-353.
16. Jelic S, Lederer DJ, Adams T, Margherita Padeletti, Paolo C Colombo, Phillip H Factor, et al. Vascular inflammation in obesity and sleep apnea. Circulation. 2010; 121: 1014-1021.
17. Kasikcioglu HA, Karasulu L, Durgun E, Oflaz H, Kasikcioglu E, Cuhadaroglu C. Aortic elastic properties and left ventricular diastolic dysfunction in patients with obstructive sleep apnea. Heart Vessels. 2005; 20: 239-244.
18. Kato M, Roberts-Thomson P, Phillips BG, Haynes WG, Winnicki M, Accurso V, et al. Impairment of endothelium-dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation. 2000; 102: 2607-2610.
19. Kohler M, Pepperell JC, Casadei B, Craig S, Crosthwaite N, Stradling JR, Davies RJ. CPAP and measures of cardiovascular risk in males with OSAS. EurRespir J. 2008; 32: 1488-1496.
20. Kraiczi H, Caidahl K, Samuelsson A, Peker Y, Hedner J. Impairment of vascular endothelial function and left ventricular filling: association with the severity of apnea-induced hypoxemia during sleep. Chest. 2001; 119: 1085-1091.
21. Kroeker EJ, Wood EH. Comparison of simultaneously recorded central and peripheral arterial pressure pulses during rest, exercise and tilted position in man. Circ Res. 1955; 3: 623-632.
22. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001; 37: 1236-1241.
23. Laurent S, Cockcroft J, Van BL, Boutouyrie P, Giannattasio C, Hayoz D, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006; 27: 2588-2605.
24. Lavie L, Lavie P. Molecular mechanisms of cardiovascular disease in OSAHS: the oxidative stress link. Eur Respir J. 2009; 33: 1467-1484.
25. Lemogoum D, Van BL, Leeman M, Degaute JP, van de BP. Ethnic differences in arterial stiffness and wave reflections after cigarette smoking. J Hypertens. 2006;� 24: 683-689.
26. Lévy P, Pépin JL, Arnaud C, Baguet JP, Dematteis M, Mach F. Obstructive sleep apnea and atherosclerosis. Prog Cardiovasc Dis. 2009; 51: 400-410.
27. Maarek B, Simon AC, Levenson J, Pithois-Merli I, Bouthier J. Heterogeneity of the atherosclerotic process in systemic hypertension poorly controlled by drug treatment. Am J Cardiol. 1987; 59: 414-417.
28. McNicholas WT. Obstructive sleep apnea and inflammation. Prog Cardiovasc Dis. 2009; 51: 392-399.
29. Migrino RQ, Aggarwal D, Konorev E, Brahmbhatt T, Bright M, Kalyanaraman B. Early detection of doxorubicin cardiomyopathy using two-dimensional strain echocardiogra- phy. Ultrasound Med Biol. 2008; 34: 208-214.
30. Morgan T, Lauri J, Bertram D, Anderson A. Effect of different antihypertensive drug classes on central aortic pressure. Am J Hypertens. 2004; 17: 118-123.
31. Namtvedt SK, Hisdal J, Randby A, Agewall S, Stranden E, Somers VK, et al. Impaired endothelial function in persons with obstructive sleep apnoea: impact of obesity. Heart. 2013; 99: 30-34.
32. O’Rourke MF. Arterial pressure waveforms in hypertension. Minerva Med. 2003; 94: 229-250.
33. Oyama J, Yamamoto H, Maeda T, Ito A, Node K, Makino N. Continuous positive airway pressure therapy improves vascular dysfunction and decreases oxidative stress in patients with the metabolic syndrome and obstructive sleep apnea syndrome. Clin Cardiol. 2012; 35: 231-236.
34. Pack AI, Gislason T. Obstructive sleep apnea and cardiovascular disease: a perspective and future directions. ProgCardiovasc Dis. 2009; 51: 434-451.
35. Protogerou AD, Laaban JP, Czernichow S, Kostopoulos C, Lekakis J, Safar ME, et al. Structural and functional arterial properties in patients with obstructive sleep apnoea syndrome and cardiovascular comorbidities. J Hum Hypertens. 2008; 22: 415-422.
36. Remington JW, Wood EH. Formation of peripheral pulse contour in man. J Appl Physiol. 1956; 9: 433-442.
37. Rowell LB, Brengelmann GL, Blackmon JR, Bruce RA, Murray JA. Disparities between aortic and peripheral pulse pressures induced by upright exercise and vasomotor changes in man. Circulation. 1968; 37: 954-964.
38. Safar ME, Lacolley P. Disturbance of macro- and microcirculation: relations with pulse pressure and cardiac organ damage. Am J Physiol Heart Circ Physiol. 2007; 293: 1-7.
39. Tanriverdi H, Evrengul H, Kaftan A, Kara CO, Kuru O, Tanriverdi S, et al. Effect of obstructive sleep apnea on aortic elastic parameters: relationship to left ventricular mass and function. Circ J. 2006; 70: 737-743.
40. Tsioufis C, Thomopoulos K, Dimitriadis K, Amfilochiou A, Tousoulis D, Alchanatis M, et al. The incremental effect of obstructive sleep apnoea syndrome on arterial stiffness in newly diagnosed essential hypertensive subjects. J Hypertens. 2007; 25: 141-146.
41. Van Bortel LM, Struijker-Boudier HA, Safar ME. Pulse pressure, arterial stiffness, and drug treatment of hypertension. Hypertension. 2001; 38: 914-921.
42. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am CollCardiol. 2010; 55: 1318-1327.
43. Wada T, Kodaira K, Fujishiro K, Maie K, Tsukiyama E, Fukumoto T, et al. Correlation of ultrasound-measured common carotid artery stiffness with pathologi- cal findings. Arteriosclerosis Thromb. 1994; 14: 479-482.
44. Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation 2006; 113: 664-670.
45. Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology, and therapy of arterial stiffness, Arterioscler Thromb Vasc Biol. 2005; 25: 932-943.