arterial arcades of pancreas and their variations - welcome …ijhbr.com/pdf/january 2015...
TRANSCRIPT

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
23
www.ijhbr.com ISSN: 2319-7072
Original article:
Arterial arcades of Pancreas and their variations
Chavan NN*, Wabale RN**
[*Assistant Professor, ** Professor and Head]
Department of Anatomy, Rural Medical College, PIMS, Loni , Tal. Rahata, Dist. Ahmednagar, Maharashtra, Pin - 413736.
Corresponding author: Dr Chavan NM
Abstract:
Introduction: Pancreas is a highly vascular organ supplied by number of arteries and arterial arcades which provide
blood supply to the organ. Arteries contributing to the arterial arcades are celiac and superior mesenteric arteries
forming anterior and posterior arcades. These vascular arcades lie upon the surface of the pancreas but also supply
the duodenal wall and are the chief obstacles to complete pancreatectomy without duodenectomy. Knowledge of
variations of upper abdominal arteries is important while dealing with gastric and duodenal ulcers, biliary tract
surgeries and mobilization of the head of the pancreas, as bleeding is one of the complications of these surgeries.
During pancreaticoduodenectomies or lymph node resection procedures, these arcades are liable to injuries.
Material and methods: Study was conducted on 50 specimens of pancreas removed enbloc from cadavers to study
variations in the arcade.
Observation and result: Anterior arterial arcade was present in 98% specimens and absent in 2%. It was formed by
anterior superior pancreaticoduodenal artery(ASPDA) and anterior inferior pancreaticoduodenal artery(AIPDA) in
92%, Anterior superior pancreaticoduodenal artery (ASPDA), Anterior inferior pancreaticoduodenal artery (AIPDA)
and Right dorsal pancreatic artery (Rt.DPA) in 2%, Anterior superior pancreaticoduodenal artery (ASPDA) only in
2%, Anterior superior pancreaticoduodenal artery (ASPDA) and Posterior inferior pancreaticoduodenal artery
(PIPDA) in 2%, Arcade was absent and Anterior superior pancreaticoduodenal artery (ASPDA) gave branches in
2%. Similarly posterior arcade also showed variations with presence in only 98% specimens.
Conclusion: Wide range of statistical records of arterial supply of pancreas, show that it is an organ that lies in three
peripancreatic interlocking arterial circles with varying degree of variations making it difficult to differentiate and
classify normal, variant and anomalous. It shows that developmental probabilities and possibilities associated with
two pancreatic buds approaching each other, enlarging and invading into a meshwork of blood vessels are many.
Key words: Arcades, variations, surgical importance
Introduction
Pancreas is second largest of digestive glands of the
human body having glandular tissue of two different
types for accomplishing two different functions. The
major part is an exocrine gland secreting enzymes for
digestion of ingested food and the other is an
endocrine part for glucose homeostasis and
gastrointestinal motility.
Pancreas is an organ that develops at the boundary
between foregut and midgut. The area of foregut is

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
24
www.ijhbr.com ISSN: 2319-7072
supplied by the celiac trunk and the midgut by
superior mesenteric artery. This explains the
description of classical anatomy of the area that the
blood supply of second part of duodenum and the
head of pancreas originates from several arteries that
spring from the celiac axis and the superior
mesenteric artery.1 The pancreaticoduodenal arcades
which are located anterior and posterior to the
pancreatic head, are major source of blood supply of
pancreatic head and the second part of the duodenum.
Extensive interference with the pancreaticoduodenal
arcades in the course of a 95% pancreatectomy may
compromise the blood supply of the duodenum
because of the shared blood supply of the duodenum
and pancreatic head.2 In addition, because the
duodenojejunal flexure and the first part of the
jejunum may derive their blood supply from branches
of the inferior pancreaticoduodenal artery or the
pancreaticoduodenal arcades, ligation of these vessels
in the course of a resection may render the proximal
jejunum ischemic.3 Typically, the posterosuperior
pancreaticoduodenal artery arises from the
gastroduodenal artery and passes to the right, anterior
to the common bile duct, forming a major source of
blood supply to common bile duct. This relation is of
surgical importance in case of operation involving
mobilization of the lower end of the common bile
duct.3
There are variations in this arcades like; it may be
doubled or tripled. The posterior arcade may also
anastomose with an aberrant right hepatic artery from
the superior mesenteric artery and also there are
variations in the origins of arteries forming arcade.
So the study was conducted to study the pattern of
arterial arcades supplying pancreas and the variations
in arterial arcades of pancreas and to compare the
findings with available literature to establish a data
for this region.
Material and methods
The study was carried out on 50 specimens removed
enbloc from the cadavers, available in the department
of Anatomy of Rural Medical College, Loni,
Maharashtra. The approval of the Institutional Ethical
and Research Committee was sought before
beginning the study.
Inclusion criteria: Formalin embalmed adult
cadavers with normal anatomy of pancreas
irrespective of sex were used in this study. These
were the cadavers meant for utilization by first year
medical students for routine dissection.
Exclusion criteria: The cadaveric specimens with
obvious abdominal pathology or operative procedures
were excluded from the study.
The enbloc removal, along with pancreas included
the duodenum, the spleen, the related part of the
abdominal aorta and portal vein. The dissection
necessary to study the arterial supply of different
parts of the pancreas was carried out. A hand lens
was used wherever necessary. Each and every
specimen thus dissected was documented with the
help of line drawing and photograph.
After removal and cleaning the dissected specimen
all parameters such as origin of arteries forming
arcade, distance of arcade from duodenum, number
of arcades and number of branches were noted. The
data collected was analyzed and expressed as
percentage. Wherever required the data was subjected
to statistical analysis. Other incidental observations in
the course of study were recorded and discussed in
the light of existing literature.
Abbreviations - (AA- Abdominal Aorta ,CT- Celiac
trunk ,CHA- Common Hepatic Artery, HA- Hepatic
Artery Proper, GDA- Gastroduodenal Artery ,

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
25
www.ijhbr.com ISSN: 2319-7072
ASPDA- Anterior Superior Pancreaticoduodenal
Artery PSPDA-Posterior Superior
Pancreaticoduodenal Artery, RGEA- Right
Gastroepiploic Artery ,IPDA- Inferior
Pancreaticoduodenal Artery , AIPDA- Anterior
Inferior Pancreaticoduodenal Artery, PIPDA-
Posterior Inferior Pancreaticoduodenal Artery,
APAr- Anterior Pancreaticoduodenal
Arcade/Anterior arcade, PPAr- Posterior
Pancreaticoduodenal Arcade /Posterior arcade)
Observation
1. Anterior Pancreaticoduodenal Arcade (APAr):
Two major arterial arcades were identified i.e.
anterior and posterior. Anterior arcade is formed by
anterior superior pancreaticoduodenal and anterior
inferior pancreaticoduodenal arteries and posterior
arcade is formed by posterior superior
pancreaticoduodenal and posterior inferior
pancreaticoduodenal arteries, mostly.
Anterior arcade was present in 98% (49/50)
specimens and absent in 2%.
Arteries of origin are shown in table 1 (figure 1 and
Photograph 1,2,3,4).
Table 1: Showing origin of Anterior Pancreaticoduodenal Arcade
Origin No. %
Anterior superior pancreaticoduodenal artery (ASPDA) and Anterior inferior
pancreaticoduodenal artery (AIPDA)
46/50 92%
Anterior superior pancreaticoduodenal artery (ASPDA), Anterior inferior
pancreaticoduodenal artery (AIPDA) and Right dorsal pancreatic artery (Rt.DPA)
1/50 2%
Anterior superior pancreaticoduodenal artery (ASPDA) only 1/50 2%
Anterior superior pancreaticoduodenal artery (ASPDA) and Posterior inferior
pancreaticoduodenal artery (PIPDA)
1/50 2%
Arcade absent and Anterior superior pancreaticoduodenal artery (ASPDA) gives
branches
1/50 2%
Total 50/50 100%

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
24
www.ijhbr.com ISSN: 2319-7072
Figure 1: Showing arteries of origin for Anterior Pancreaticoduodenal Arcade
ASPDA, AIPDA and Rt.DPA 1/50 (2%) ASPDA only1/50 (2%)
(Photograph 1) (Photograph 2)
ASPDA & PIPDA 1/50 (2%) Arcade absent &ASPDA gives branches 1/50 (2%).
(Photograph 3) (Photograph 4)
Distance of arcade from duodenum: The distance of arcade from duodenum ranged from 0(at
pancreaticoduodenal junction) to 3 cm with mean 0.54 and standard deviation of 0.68.
In 20 specimens the arcade was hidden by pancreatic tissue (40%).
Number of Arcade: In all specimens only single arcades were found.
Number of branches by arcade: Average number =8; Range =6 - 10
2. Posterior pancreaticoduodenal arcade (PPAr):
This arcade was present in 98% and absent in 2% specimens. Arteries of origin are shown in table 2 (Figure 2 and
Photograph 5,6,7,8,9,10)
ASPDA
AIPDA
RT. DPA
ASPDA
PIPDA
26

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
25
www.ijhbr.com ISSN: 2319-7072
Table 2: Showing origin of Posterior Pancreaticoduodenal Arcade
Origin No. %
Posterior superior pancreaticoduodenal artery (PSPDA) and Posterior inferior
pancreaticoduodenal artery (PIPDA)
43/50 86%
Posterior superior pancreaticoduodenal artery (PSPDA), Posterior inferior pancreaticoduodenal
artery (PIPDA) and extra branch from superior mesenteric artery (SMA)
2/50 4%
Posterior superior pancreaticoduodenal artery (PSPDA),Posterior inferior pancreaticoduodenal
artery (PIPDA) and extra branch from abdominal aorta (AA)
1/50 2%
Posterior superior pancreaticoduodenal artery (PSPDA) only 1/50 2%
Anterior inferior pancreaticoduodenal artery (AIPDA) and Posterior superior pancreaticoduodenal
artery (PSPDA)
1/50 2%
Arcade absent and Right hepatic artery (RHA) gives branches 1/50 2%
Posterior superior pancreaticoduodenal artery (PSPDA), Posterior inferior pancreaticoduodenal
artery (PIPDA) and Anterior inferior pancreaticoduodenal artery (AIPDA)
1/50 2%
Total 50/50 100%
27

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
26
www.ijhbr.com ISSN: 2319-7072
Figure 2: Showing arteries of origin for Posterior Pancreaticoduodenal Arcade
PSPDA, PIPDA and Extra branch PSPDA, PIPDA and extra branch from
from SMA 2/50 (4%). AA 1/50 (2%).
(Photograph 5) (Photograph 6)
PSPDA only forms arcade 1/50 (2%). PSPDA and AIPDA 1/50 (2%).
(Photograph 7) (Photograph 8)
PPAr is absent and RHA gives PSPDA, PIPDA and AIPDA 1/50 (2%).
branches 1/50 (2%)
(Photograph 9) (Photograph 10)
PSPDA
PIPDA
EXTRA BRANCH
FROM SMA EXTRA BRANCH
FROM AA
PSPDA
PIPDA
AIPDA
PSPDA
RHA
AIPDA
PIPDA PSPDA
28

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
23
www.ijhbr.com ISSN: 2319-7072
Distance from duodenum-The distance of arcade
from duodenum ranged from 0 (at pancreat-
icoduodenal junction) to 2.9 cm, with a mean 1.36
and standard deviation of 0.52. There was a
statistically significant difference (p value< 0.05)
between the mean distance of anterior arcade and
mean distance of posterior arcade from
pancreaticoduodenal junction.
Number of arcades - arcade was single in all cases.
Number of branches by arcade: Average number
=7; Range = 6 - 10.
Discussion
Anterior Pancreaticoduodenal Arcade (APAr): An
arcade of an artery supplying branches to anterior
surface of both duodenum and head of pancreas is
present in 98% cases in this study; same was present
in all cases studied by Kimura W et al.16 In 92%
cases this arcade is formed by anterior superior
pancreaticoduodenal artery and anterior inferior
pancreaticoduodenal artery; whereas same is noted in
all cases studied by Kimura W et al.16In 40% cases
the lower 2/3rd arcade was found to be partly
embedded within pancreatic tissue; this occurrence
finds no mention anywhere in the available literature.
On an average we found eight branches arising from
anterior arcade supplying only the duodenum.
Smaller delicate branches arising from the arcade
sunk directly into substance of pancreas (Photograph
No.11).
Photograph 11: Anterior arcade embedded within
pancreatic tissue.
Posterior Pancreaticoduodenal Arcade (PPAr):
Another arcade artery supplying posterior surface of
duodenum and pancreas is present in 98% of cases in
this study, in all the cases studied by Michel NA et
al9, and 88% of cases studied by Kimura W et
al.16Variable origin of the two source arteries for
arcade was noted in this study; arcade formation by
posterior superior pancreaticoduodenal artery and
posterior inferior pancreaticoduodenal artery was
seen in 86% cases. Similar combination is seen in
78% by Van Damme et al8, and in 88% cases studied
by Kimura W et al.16
Location of this arcade was farther away from
duodenum as compared to anterior arcade. On an
average we found seven branches arising from
posterior arcade supplying duodenum (2nd part) along
with common bile duct. Smaller delicate branches
arising from the arcade sunk into posterior surface of
head of pancreas
There are anastomoses at all levels of pancreas. This
extensive arterial network of the pancreas is an
important source of collateral blood supply in cases
of occlusion of celiac axis, superior mesenteric or
splenic arteries. The existence of individual
differences, development of arterial–arterial
anastomosis asks for obligatory preoperative
supraselective angiography which enables insight
into distribution of blood vessels.17
It is into this meshwork of vessels the pancreatic buds
sprout from two opposite sides i.e. dorsal and ventral
of the second part of duodenum (Picture No.1).
29
International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
24
www.ijhbr.com ISSN: 2319-7072
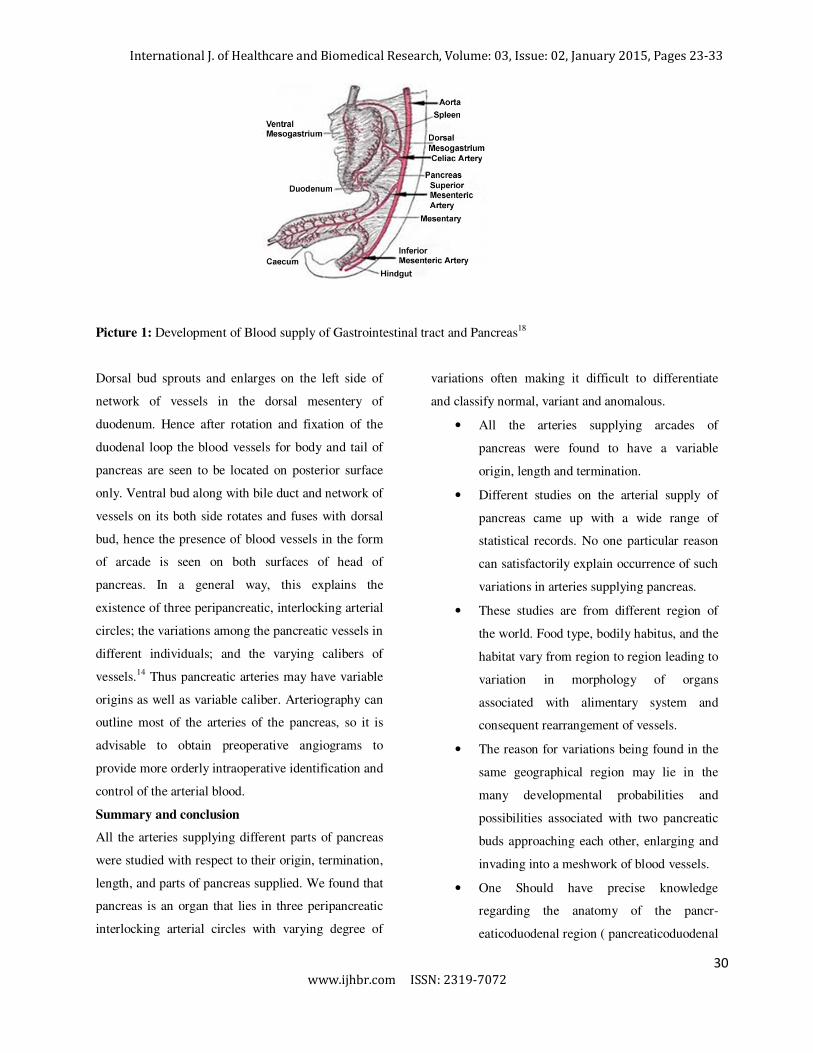
Picture 1: Development of Blood supply of Gastrointestinal tract and Pancreas18
Dorsal bud sprouts and enlarges on the left side of
network of vessels in the dorsal mesentery of
duodenum. Hence after rotation and fixation of the
duodenal loop the blood vessels for body and tail of
pancreas are seen to be located on posterior surface
only. Ventral bud along with bile duct and network of
vessels on its both side rotates and fuses with dorsal
bud, hence the presence of blood vessels in the form
of arcade is seen on both surfaces of head of
pancreas. In a general way, this explains the
existence of three peripancreatic, interlocking arterial
circles; the variations among the pancreatic vessels in
different individuals; and the varying calibers of
vessels.14 Thus pancreatic arteries may have variable
origins as well as variable caliber. Arteriography can
outline most of the arteries of the pancreas, so it is
advisable to obtain preoperative angiograms to
provide more orderly intraoperative identification and
control of the arterial blood.
Summary and conclusion
All the arteries supplying different parts of pancreas
were studied with respect to their origin, termination,
length, and parts of pancreas supplied. We found that
pancreas is an organ that lies in three peripancreatic
interlocking arterial circles with varying degree of
variations often making it difficult to differentiate
and classify normal, variant and anomalous.
• All the arteries supplying arcades of
pancreas were found to have a variable
origin, length and termination.
• Different studies on the arterial supply of
pancreas came up with a wide range of
statistical records. No one particular reason
can satisfactorily explain occurrence of such
variations in arteries supplying pancreas.
• These studies are from different region of
the world. Food type, bodily habitus, and the
habitat vary from region to region leading to
variation in morphology of organs
associated with alimentary system and
consequent rearrangement of vessels.
• The reason for variations being found in the
same geographical region may lie in the
many developmental probabilities and
possibilities associated with two pancreatic
buds approaching each other, enlarging and
invading into a meshwork of blood vessels.
• One Should have precise knowledge
regarding the anatomy of the pancr-
eaticoduodenal region ( pancreaticoduodenal
30

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
24
www.ijhbr.com ISSN: 2319-7072
arteries) which provide blood to the
duodenum.
• There is a need to preserve the
pancreaticoduodenal arteries to avoid
duodenal necrosis
• Preservation of the pancreaticoduodenal
arteries would provide a better supply of
blood to the duodenal wall.
• Distance of posterior arcade from
duodenojejunal junction was found to be
significantly more than the distance of
anterior arcade which is most probably due
to presence of common bile duct between
posterior arcade and duodenum.
• In 40% specimens the arcade was hidden by
pancreatic tissue.
One thing that became apparent in this study was
need to include a larger sample size in view of the
quantum and spectrum of variations that we came
across in a relatively small sample size. Study in a
larger sample size was not possible due to constraints
with respect to time and availability of specimens for
study.
A thorough search of literature did not yield any
publication related to study of arteries of pancreas
from our region. This was probabaly the first attempt
in our region to study and document arteries of
pancreas in detail. The knowledge of the vascular
anatomy of pancreatic region is an important
prerequisite for planned surgical intervention. The
awareness of the existing vascular anomalies
enhances the insight of any region and thus the
chances of successful outcome.
Bibliography
1. Busnardo AC, DiDio LJ, Tidrick RT, Thomford NR. History of Pancreas. AM J Surg. 1983; 146(5): 539-
50.
2. Mackie CR, Lu CT, Noble HG et al. Prospective evaluation of angiography in the diagnosis and
management of patients suspected of having pancreatic cancer. Ann Surg.1979; 189: 11.
3. Pancreas, In: Tadataka Y, David HA, Loren L, Kaplowitz N, Owyang C. Textbook of Gastroenterology,
Vol.2, 4th Edition, Lippincott Williams & Wilkins, 2003: 2016-19.
4. Squillaci E, Fanucci E, Sciuto F, Masala S, Sadani G, Carlani M, Simanetti G. Vascular involvement in
pancreatic neoplasm- a comparison between spiral CT & DSA. Dig Dis Sci. 2003 Mar; 48(3): 449-458.
5. Abdomen, In: Sauerland EK. Grant’s dissector, 7th edition, Baltimore(USA), The Williams and Wilkins
Company, 1973: 40-43.
6. The duodenum, pancreas and spleen, In: Zuckerman L.A new system of Anatomy - A Dissector’s guide
and atlas, 2nd Edition, London, Oxford university press, 1981: 61-67.
7. The Anatomical Basis of Clinical Practice Preface ix, In: Susan Standring, Gray’s Anatomy, 40th Edition,
London(UK), Elsevier, 2008: 1183-1186.
8. Van Damme, Jean-PJ. Behavioral anatomy of the abdominal arteries. Surg Clin North Am. 1993; 73(4):
699-725.
9. Michels NA. The hepatic, cystic and retroduodenal arteries and their relations to the biliary ducts. Ann
Surg. April 1951; 183(4): 503-524.
31

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
24
www.ijhbr.com ISSN: 2319-7072
10. The embryologic and anatomic basis of Modern Surgery: Pancreas, In: Skandalakis JE. Skandalakis
Surgical Anatomy. International student’s edition, Vol.II, Greece, Paschalidis medical publications, 2004:
1151-1228.
11. The Alimentary system-Pancreas, In: Datta AK, Essentials of Human Embryology, 6th Edition, Kolkata,
Current books International, 2005: 143-144.
12. Alimentary & respiratory system XI - Pancreas, In: Hamilton, Boyd and Mossman, Human Embryology,
London and Basingstoke, The MacMillan Press Ltd, 1978: 349-351, 362.
13. Bertelli E, Di Gregorio F, Bertelli L, Mosca S. The arterial blood supply of pancreas: a review I. The
superior pancreaticoduodenal and anterior superior pancreatic-coduodenal arteries. An anatomical and
radiological study. Surg Radiol Anat. 1995; 17: 97-106.
14. Oslen LL, Woodburne RT. The vascular relations of the pancreas. Surg Gynec Obstet.1951; 42: 713-719.
15. Thomford NR, Chandnani PC et al. Anatomic characteristics of the pancreatic arteries. The American
Journal of Surgery. June 1986; 151: 690-693.
16. Kimura W, Nagai H. Study of surgical anatomy for duodenum-preserving resection of the head of the
pancreas. Ann Surg. 1995; 221(4): 359-363.
17. Kulenovic A et al. Investigation of vascularization of human pancreas using method of selective
arteriography with insight into significance to a surgical approach for this organ. Bosnian Journal of Basic
Medical Sciences. 2010; 10(1):15-18.
18. Shiota K, UNSW. [Image on Internet Gray’s 1918 Anatomy]. 2009 Aug. Available
from:http://php.med.unsw.edu.au/embryology/index.php?title=File:GIT blood supply.jyg
19. Braasch JW, Gray BN. Technique of radical pancreaticoduodenectomy with consideration for hepatic
arterial relationships. Surg Clin North Am.1976; 56: 631.
20. Skandalakis JE, Gray SW, Rowe JS, Skandalakis LJ. Surgical anatomy of pancreas. Contemp Surg. 1979;
15: 17-40.
21. Avram M et al. Pancreaticoduodenal resection. Surg. Clin. of North America..
22. Bertelli E, Bertelli L, Di Gregorio F, Civeli L, Mosca S. The arterial blood supply of pancreas: a review. II.
The posterior superior pancreaticoduodenal artery. An anatomical and radiological study. Surg Radiol
Anat. 1996; 18: 1-9.
23. Bertelli E, Di Gregorio F, Bertelli L, Civeli L, Mosca S. The arterial blood supply of pancreas: a review.
III. The inferior pancreaticoduodenal artery. An anatomical and radiological study. Surg Radiol Anat. 1996;
18: 67-74.
24. Bertelli E, Bertelli L, Di Gregorio F, Orazioli D, Bastianini A. The arterial blood supply of pancreas: a
review. IV. The anterior inferior pancreaticoduodenal artery, the posterior inferior pancreaticoduodenal
artery and minor sources of blood supply for the head of pancreas. An anatomical review and a radiological
study. Surg Radiol Anat. 1997; 19: 203-212.
32

International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33
25
www.ijhbr.com ISSN: 2319-7072
25. Bertelli E, Di Gregorio F, Mosca S, Bastianini A. The arterial blood supply of pancreas: a review. V. The
dorsal pancreatic artery. An anatomic review and a radiological study. Surg Radiol Anat. 1998; 20: 445-
452.
26. Michels NA. Variational anatomy of the hepatic, cystic and retroduodenal arteries. Arch. Surg.1953; 66:
20-34.
33