army medic magazine
DESCRIPTION
ARMY MEDIC MAGAZINETRANSCRIPT
THE EXPERIENCES OF NHS HEALTH PROFESSIONALSIN AFGHANISTAN DURING 2007-2008
2008 ISSUE 2
This magazine contains graphic clinical images
FREE
Op HERRICK
MEDICAL
ARMY MEDICARMY MEDICARMY MEDIC
An Overview of Op HERRICK
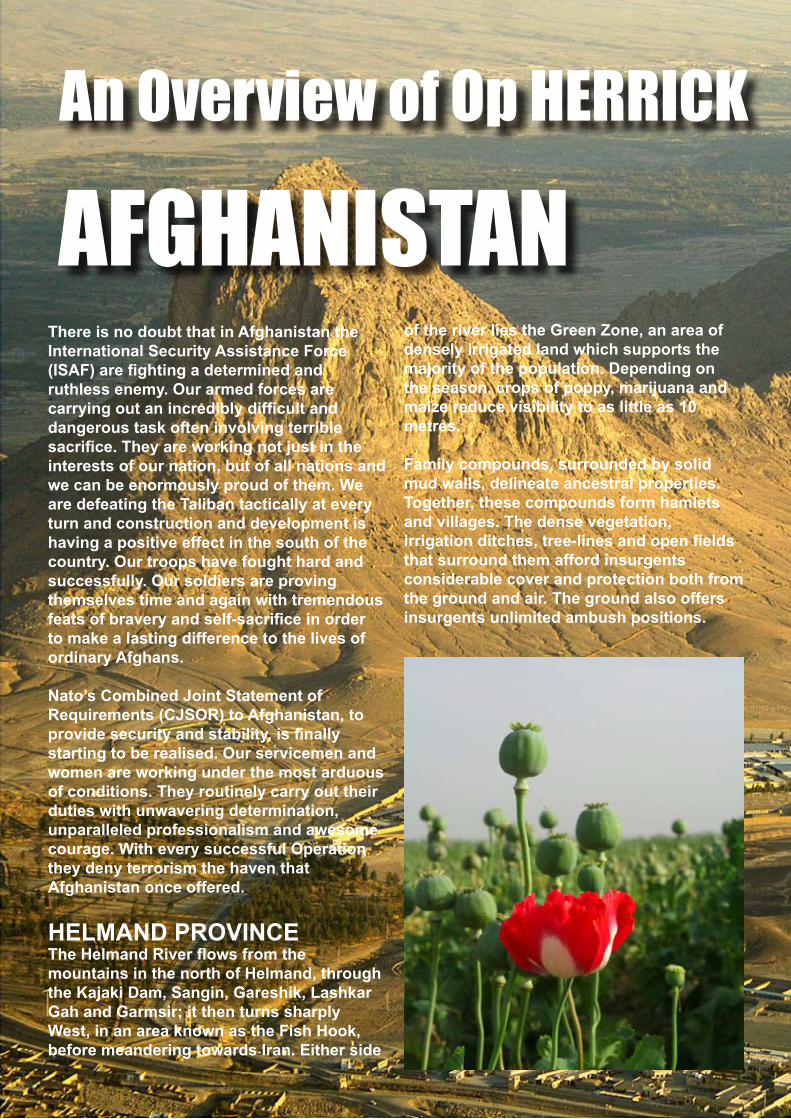
AFGHANISTANThere is no doubt that in Afghanistan the International Security Assistance Force (ISAF) are fi ghting a determined andruthless enemy. Our armed forces are carrying out an incredibly diffi cult and dangerous task often involving terrible sacrifi ce. They are working not just in the interests of our nation, but of all nations and we can be enormously proud of them. We are defeating the Taliban tactically at every turn and construction and development is having a positive effect in the south of the country. Our troops have fought hard and successfully. Our soldiers are provingthemselves time and again with tremendous feats of bravery and self-sacrifi ce in order to make a lasting difference to the lives of ordinary Afghans. Nato’s Combined Joint Statement of Requirements (CJSOR) to Afghanistan, toprovide security and stability, is fi nally starting to be realised. Our servicemen and women are working under the most arduous of conditions. They routinely carry out their duties with unwavering determination, unparalleled professionalism and awesome courage. With every successful Operation they deny terrorism the haven that Afghanistan once offered.
HELMAND PROVINCEThe Helmand River fl ows from the mountains in the north of Helmand, through the Kajaki Dam, Sangin, Gareshik, Lashkar Gah and Garmsir; it then turns sharplyWest, in an area known as the Fish Hook, before meandering towards Iran. Either side
of the river lies the Green Zone, an area of densely irrigated land which supports themajority of the population. Depending on the season, crops of poppy, marijuana and maize reduce visibility to as little as 10 metres.
Family compounds, surrounded by solid mud walls, delineate ancestral properties. Together, these compounds form hamletsand villages. The dense vegetation, irrigation ditches, tree-lines and open fi elds that surround them afford insurgents considerable cover and protection both from the ground and air. The ground also offers insurgents unlimited ambush positions.
Outside of this green zone the terrain is open desert and desert mountains.
According to UNICEF 2007.Public Health in Afghanistan is verylimited. The life expectancy for males is 47 years of age. The mortality in children under fi ve is more than 25% of live births and the lifetime risk of maternal death is 1:6. There are no Intensive Care facilities that offer ventilation and there is no renal dialysis. Literacy is less than 43% in males and 13% in females.
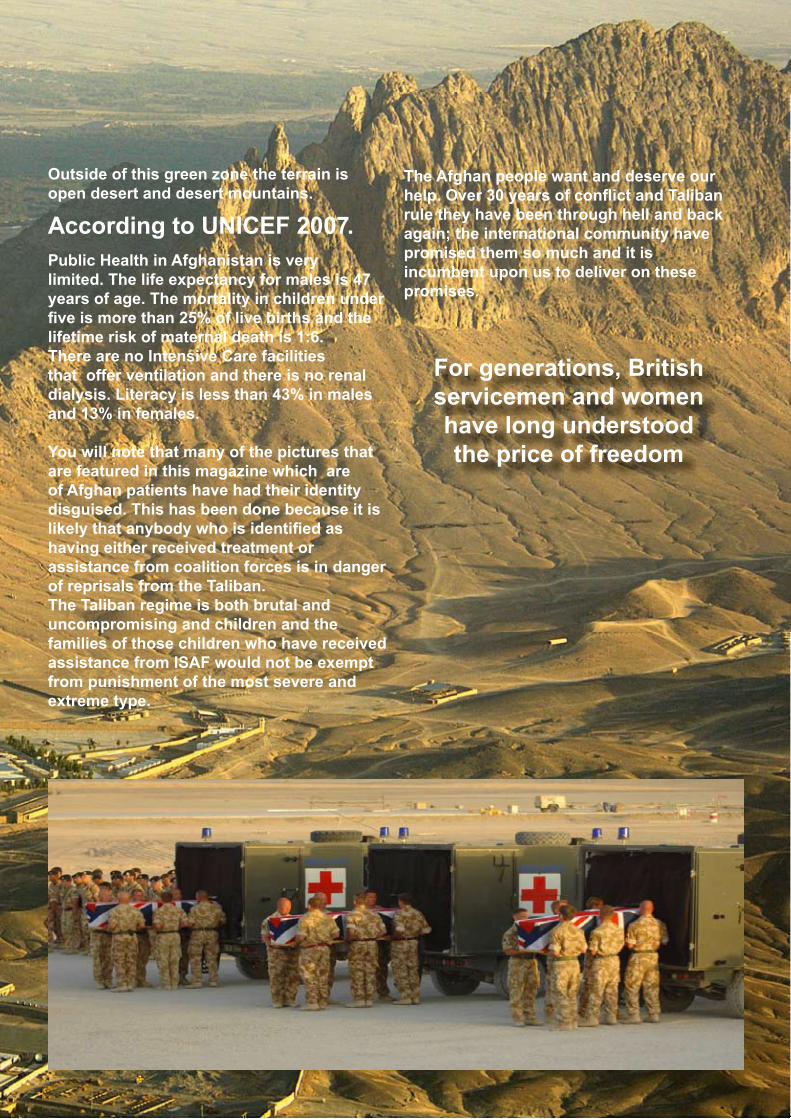
You will note that many of the pictures that are featured in this magazine which are of Afghan patients have had their identity disguised. This has been done because it is likely that anybody who is identifi ed ashaving either received treatment or assistance from coalition forces is in danger of reprisals from the Taliban.The Taliban regime is both brutal and uncompromising and children and the families of those children who have receivedassistance from ISAF would not be exempt from punishment of the most severe and extreme type.
The Afghan people want and deserve our help. Over 30 years of confl ict and Taliban rule they have been through hell and back again; the international community havepromised them so much and it is incumbent upon us to deliver on these promises.
For generations, British servicemen and women have long understood the price of freedom
In this issue
1
6
9
13
22
241 Under Canvas Under the KnifeA surgeon’s story
6 Medical Emergency Response TeamPre-hospital Care, the Military Way
9 A+E @ the Sharp EndManaging one of the Busiest A+E
Departments on the Planet13 A Nurse’s War Diary
ITU in Afghanistan16 Theatre of War
Integrated Medical Planning19 NHS Proud Partners
The Story on the Wards22 Secretary of State for Health
Minister calls on the NHS to Give Support for Reserve Service24 Fighting Spirit
The Road to Recovery26 One ARMY
TA gains a New Identity27 Clinical Training on a Grand Scale
World-class training facilities for Army Medics29 First for Health
A look inside of the Army Primary Healthcare Service30 Hospital fi t for Heroes
Selly Oak Hospital exceeding expectations
April 2008
The British people do not crave or celebrate war and withinour society war is most abhorrent to a professional soldier.This is because it is he or she who must endure its consequences and the inevitable suffering that follows, butwhenever the British people elect to deploy its ArmedForces our soldiers and service people have always donetheir duty and they have always done it willingly. Oursoldiers don’t crave hero status, rather our soldiers have always carried on through adversity with dignity and profes-sionalism. Making a fuss simply isn’t our way of doing busi-ness. What they do expect and deserve is that we should provide them with the fi nest medical care that we can offer, and we are consistently delivering on that promise.
Increasingly we are dependent upon the support of the Territorial Army who normally work as civilian NHS health professionals and time and again they are proving their worth.In comparison to many front-line fi ghting locations, the Enhanced Role 2 Field Hospital is arelatively benign place. However, you should be in no doubt that the work that these healthprofessionals do is absolutely crucial. The Territorial Army has to recruit the best NHSsurgeons, anaesthetists, specialist nurses and other health professionals that it can, andwe must train and equip them to work in some of the world’s toughest clinicalenvironments. In many cases they have dealt with more serious trauma on a three-month tour of duty than they might see in 15 years of working in the NHS. It is no small thing that we ask of them. We rely on professionals like you, professionals who have fulfi lling civiliancareers and family lives and we ask them to volunteer their time to undergo intensivemilitary training that will equip them with the skills that they will need to work in a war zone.With the exception of our soldiers and those civilians who are caught up in this tragedy ofwar, few people will ever truly value the personal sacrifi ces that they endure in order thatthey might serve and save lives.
The following is a collection of experiences taken from people who normally work asprofessionals in the NHS, ordinary anonymous civilians who have normal busy family andprofessional lives, people who serve in the Territorial Army, people who work inextraordinary environments in places like Iraq and Afghanistan. It is our hope that their accounts will inspire some of you to follow in their footsteps and if not that, then you might feel compelled to better support them.
P J BURGESS BA RGN MBACaptainEditor
IN THE ARMY THERE’S NO SUCH THING AS A ROUTINE OPERATION.Want to develop your clinical skills in some of the World’s most challenging environments?
You’ll retain your NHS job and your NHS employer will be supportive of you becoming a Reservist. The NHS will give you up to and extra two weeks annual leave to help you train as a Reservist.
MEDICAL
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Find out more
ARMY MEDIC Magazine 1
Maj Andy Bruce RAMC (V)Age 38Married with 4 young childrenConsultant Orthopaedic SurgeonYorkshire
UNDER UNDER CANVASCANVASUNDER theUNDER the KNIFE KNIFE
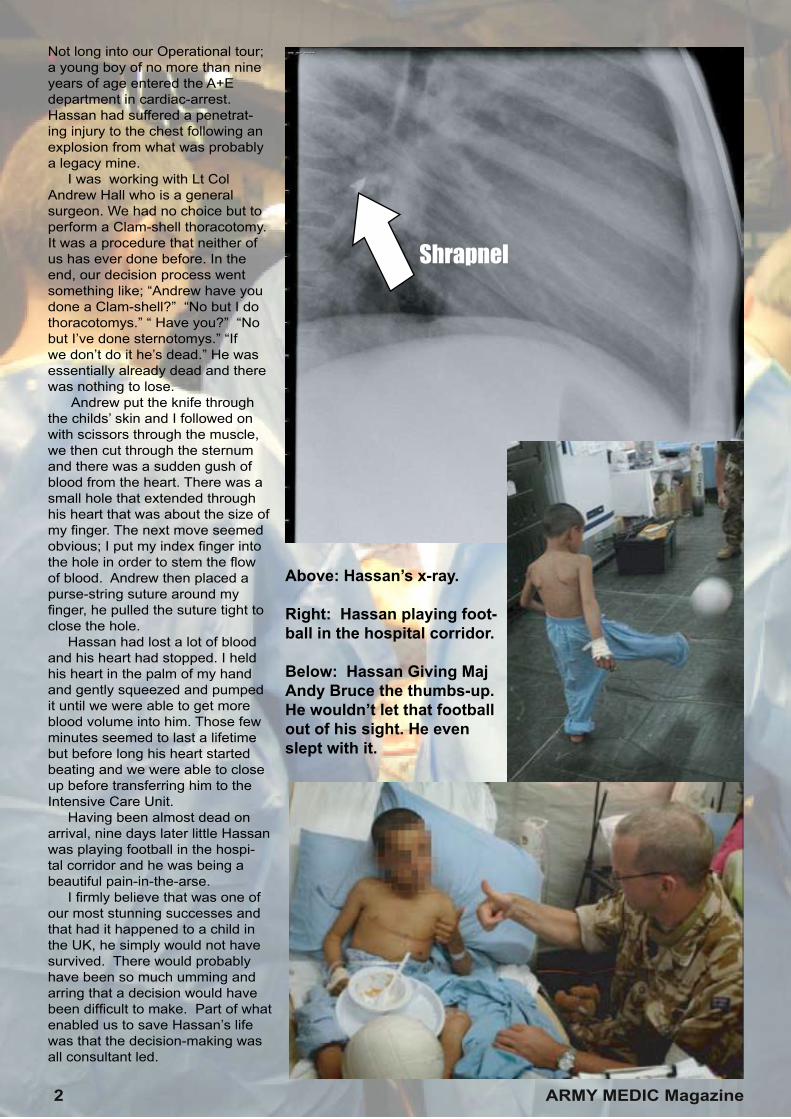
Not long into our Operational tour; a young boy of no more than nine years of age entered the A+E department in cardiac-arrest. Hassan had suffered a penetrat-ing injury to the chest following an explosion from what was probably a legacy mine. I was working with Lt Col Andrew Hall who is a general surgeon. We had no choice but to perform a Clam-shell thoracotomy. It was a procedure that neither of us has ever done before. In the end, our decision process went something like; “Andrew have you done a Clam-shell?” “No but I do thoracotomys.” “ Have you?” “No but I’ve done sternotomys.” “If we don’t do it he’s dead.” He was essentially already dead and there was nothing to lose. Andrew put the knife through the childs’ skin and I followed on with scissors through the muscle, we then cut through the sternum and there was a sudden gush of blood from the heart. There was a small hole that extended through his heart that was about the size of my fi nger. The next move seemed obvious; I put my index fi nger into the hole in order to stem the fl ow of blood. Andrew then placed a purse-string suture around my fi nger, he pulled the suture tight to close the hole. Hassan had lost a lot of blood and his heart had stopped. I held his heart in the palm of my hand and gently squeezed and pumped it until we were able to get more blood volume into him. Those few minutes seemed to last a lifetime but before long his heart started beating and we were able to close up before transferring him to the Intensive Care Unit. Having been almost dead on arrival, nine days later little Hassan was playing football in the hospi-tal corridor and he was being a beautiful pain-in-the-arse. I fi rmly believe that was one of our most stunning successes and that had it happened to a child in the UK, he simply would not have survived. There would probably have been so much umming and arring that a decision would have been diffi cult to make. Part of what enabled us to save Hassan’s life was that the decision-making was all consultant led.
Shrapnel
Above: Hassan’s x-ray.
Right: Hassan playing foot-ball in the hospital corridor.
Below: Hassan Giving Maj Andy Bruce the thumbs-up. He wouldn’t let that football out of his sight. He even slept with it.
2 ARMY MEDIC Magazine
ARMY MEDIC Magazine 3
After the event we looked it up in the literature and there was no published account of any paediat-ric resuscitative thoracotomy that had ever survived before. That was one of many stunning suc-cesses that gave the whole team a incredible boost to their morale. We might have been working in a tented hospital and in itself that was a unique experience, but we were working with world class kit and equipment, the type of which one could only dream of having in the NHS. The Dragon digital x-ray kit was amazing. It enabled us to obtain quality images within seconds and if the x-ray wasn’t quite right, then we were able to simply re-take it there and then. That meant that the time-line between taking a diagnostic x-ray to making a decision about treatment, theatre or to ward a patient was rapid. This instant imaging meant that we could turn around a patient in the resus bay very quickly. All of our radiographers had a marvellous can-do-attitude. Can-do is standard vocabulary in a Field Hospital. They would say “Ok, I haven’t done that before but let’s give it a go, I don’t know if I can get that picture on a McVicar table but I’ll try.” I think that be-cause we were all out there with one primary objective and with-out the everyday distractions of normal life. I am confi dent that not having to worry about cooking or shopping was a key factor in fuel-ling the many proactive attitudes that existed. When we fi rst arrived at the Contingency Operating Base (COB) Camp Bastion, the Military Intelligence people informed us that things would be relatively quiet for at least the next ten days. This was primarily due to the fact that the poppy harvest was just coming to an end. Taliban leaders would be waiting for the exchange of opium (the basis for the drug heroin) for cash and weapons. With new weapons, more am-munition and the means to pay their fi ghters they would be able to renew their offensive on ISAF (The International Security Assistance Force). As predicted, it wasn’t long before the Taliban returned for
round two and with numerous battles and military Operations going on we were placed on mass-casualty stand-by. We didn’t have to wait long. A com-pound that was near to a school was bombed and some 70 civilian casualties resulted. The casualties were dispersed between us, the Canadian Hospital and the Dutch Hospital. Out of that experi-ence, probably the most useful lesson learnt, was the realisation that the way that we had organised ourselves meant that we could have somebody on the Operating table in under twenty minutes of them arriving in the A+E. A second case that will remain burnt into my memory was not so successful. A British soldier had been brought in following a gunshot wound to his chest. He went into cardiac-arrest as the Medical-Emergency-Response-Team (MERT) helicopter landed at the hos-pital. While in the A+E; we performed a thoracotomy and extended into a laparotomy. We got his heart beating in resus, we had cross-clamped his abdominal aorta and I travelled to the Operating theatre straddling the trolley while applying pressure to his liver to stop him bleeding-out venously. We got him into the Operating theatre; Andrew was dealing with his chest and his spleen, his kidney, his diaphragm and his splenic-fl ecture; I was assisting.
Unfortunately; about two and a half hours into the operation he re-arrested on the table. We got him back and he then arrested for a third time. It was felt that his bio-chemical abnor-malities were so huge that there was nothing more that we could do. After having had so many unexpected successes, the sense of devastation that we all felt was palpable. The lad had received some thirty units of blood FFP, platelets and all sorts, but our efforts were in vain. We were still very busy, but for days, the sense of loss was felt by everybody. He was the only patient that died on our Operating table in the whole three months that we were there. The UK coroner and pathologist who performed his post-mortem said, that he had un-survivable injuries, that they were surprised that we were ever able to resuscitate at all, and that even a level 1 trauma centre in the UK could not have saved his life. That was little consolation. In Afghanistan as is the case any-where else in the world, we still have to deal with everyday accidents; the difference is that where major trauma is involved, most Afghan patients would ordinarily not have access to First-World hospital facilities. Half way through our three month tour of
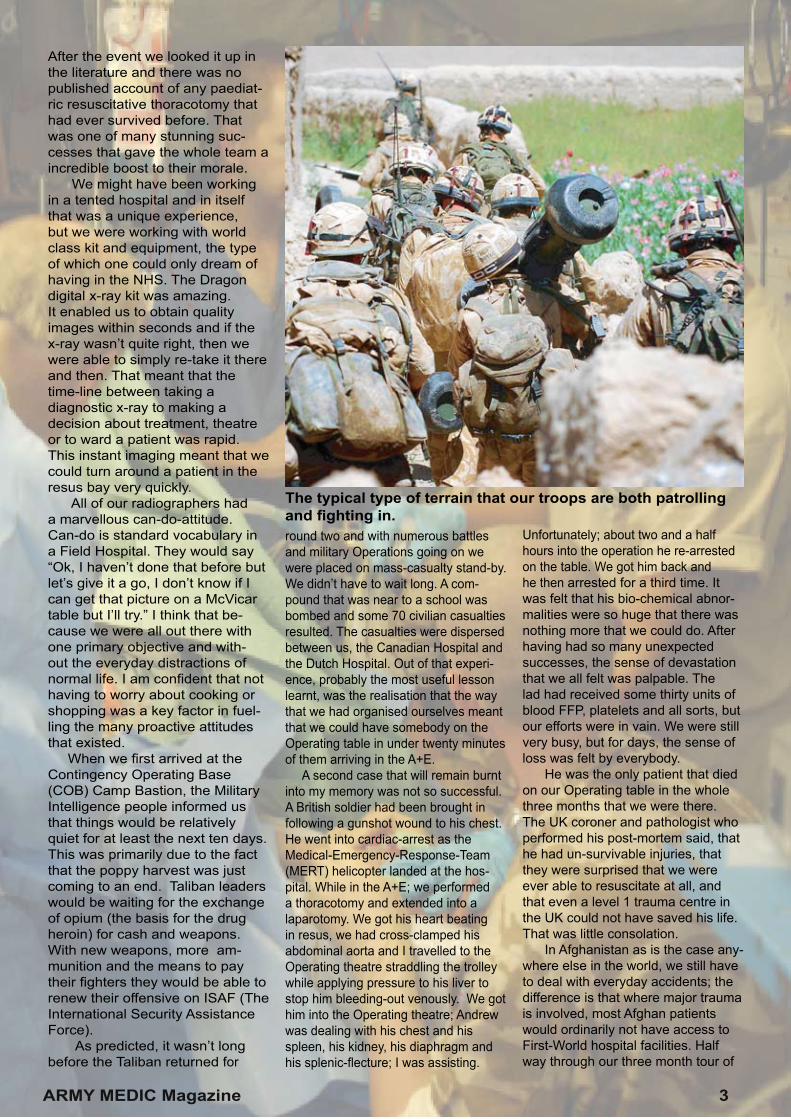
The typical type of terrain that our troops are both patrolling and fi ghting in.
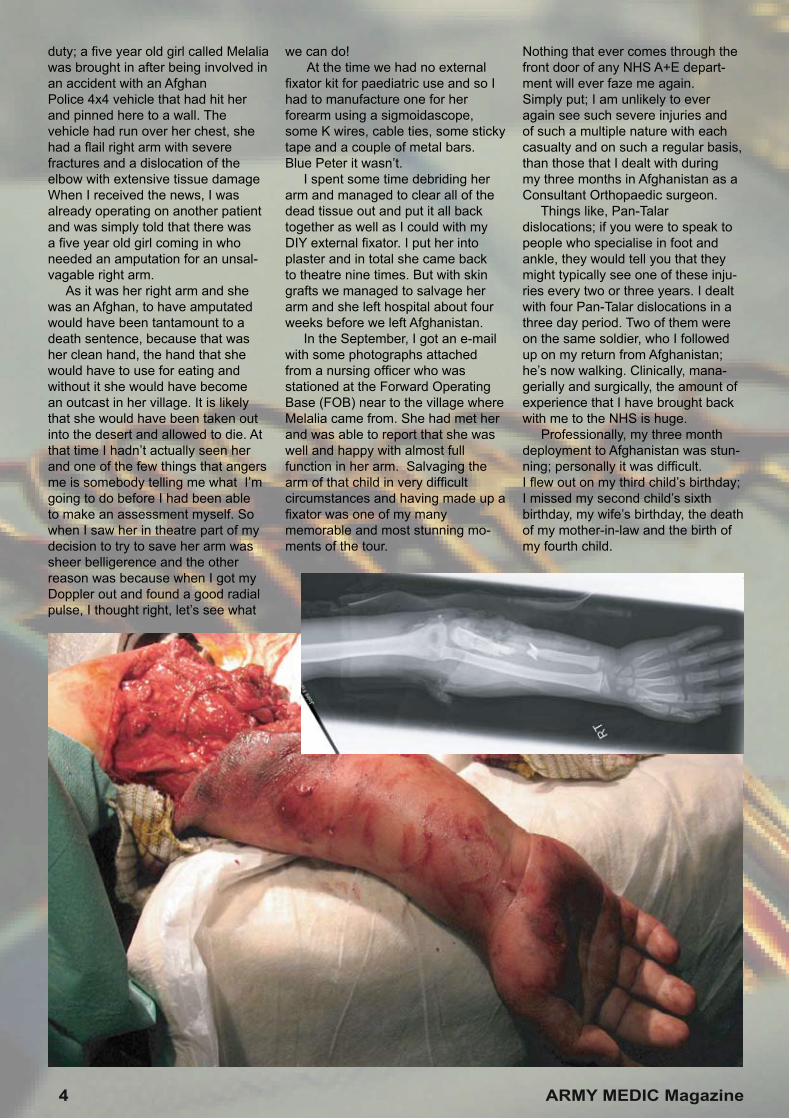
duty; a fi ve year old girl called Melalia was brought in after being involved in an accident with an Afghan Police 4x4 vehicle that had hit her and pinned here to a wall. The vehicle had run over her chest, she had a fl ail right arm with severe fractures and a dislocation of the elbow with extensive tissue damage When I received the news, I was already operating on another patient and was simply told that there was a fi ve year old girl coming in who needed an amputation for an unsal-vagable right arm. As it was her right arm and she was an Afghan, to have amputated would have been tantamount to a death sentence, because that was her clean hand, the hand that she would have to use for eating and without it she would have become an outcast in her village. It is likely that she would have been taken out into the desert and allowed to die. At that time I hadn’t actually seen her and one of the few things that angers me is somebody telling me what I’m going to do before I had been able to make an assessment myself. So when I saw her in theatre part of my decision to try to save her arm was sheer belligerence and the other reason was because when I got my Doppler out and found a good radial pulse, I thought right, let’s see what
we can do! At the time we had no external fi xator kit for paediatric use and so I had to manufacture one for her forearm using a sigmoidascope, some K wires, cable ties, some sticky tape and a couple of metal bars. Blue Peter it wasn’t. I spent some time debriding her arm and managed to clear all of the dead tissue out and put it all back together as well as I could with my DIY external fi xator. I put her into plaster and in total she came back to theatre nine times. But with skin grafts we managed to salvage her arm and she left hospital about four weeks before we left Afghanistan. In the September, I got an e-mail with some photographs attached from a nursing offi cer who was stationed at the Forward Operating Base (FOB) near to the village where Melalia came from. She had met her and was able to report that she was well and happy with almost full function in her arm. Salvaging the arm of that child in very diffi cult circumstances and having made up a fi xator was one of my many memorable and most stunning mo-ments of the tour.
Nothing that ever comes through the front door of any NHS A+E depart-ment will ever faze me again. Simply put; I am unlikely to ever again see such severe injuries and of such a multiple nature with each casualty and on such a regular basis, than those that I dealt with during my three months in Afghanistan as a Consultant Orthopaedic surgeon. Things like, Pan-Talar dislocations; if you were to speak to people who specialise in foot and ankle, they would tell you that they might typically see one of these inju-ries every two or three years. I dealt with four Pan-Talar dislocations in a three day period. Two of them were on the same soldier, who I followed up on my return from Afghanistan; he’s now walking. Clinically, mana-gerially and surgically, the amount of experience that I have brought back with me to the NHS is huge. Professionally, my three month deployment to Afghanistan was stun-ning; personally it was diffi cult.I fl ew out on my third child’s birthday; I missed my second child’s sixth birthday, my wife’s birthday, the death of my mother-in-law and the birth of my fourth child.
4 ARMY MEDIC Magazine
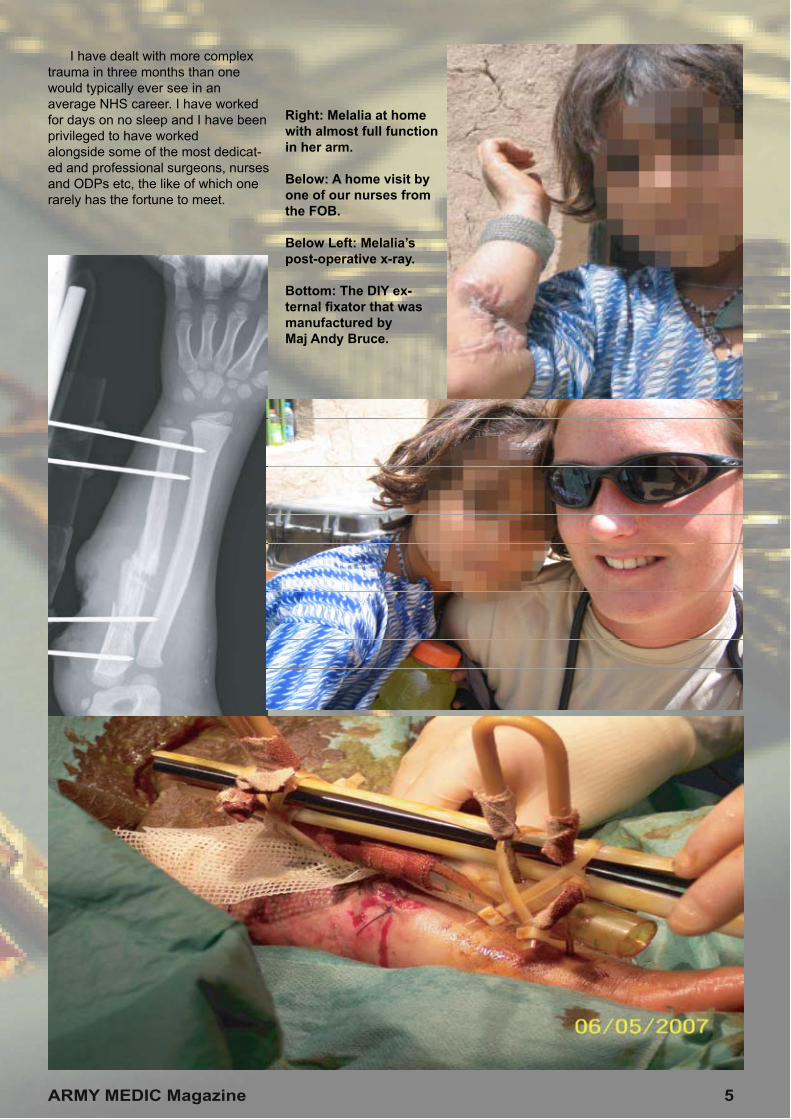
I have dealt with more complex trauma in three months than one would typically ever see in an average NHS career. I have worked for days on no sleep and I have been privileged to have worked alongside some of the most dedicat-ed and professional surgeons, nurses and ODPs etc, the like of which one rarely has the fortune to meet.
Right: Melalia at home with almost full function in her arm.
Below: A home visit by one of our nurses from the FOB.
Below Left: Melalia’s post-operative x-ray.
Bottom: The DIY ex-ternal fi xator that was manufactured by Maj Andy Bruce.
ARMY MEDIC Magazine 5
TAKE YOUR SKILLS FURTHER“Every NHS Trust should be proactive in supporting their clinicians to become reservists”
MEDICAL
Rt Hon Alan Johnson MPSecretary of State for Health
April 2008
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Find out more
Lt Col Ian Nesbitt RAMC (V)Age 41 Married with 4 young childrenConsultant AnaesthetistNewcastle Upon-Tyne
MEDICALMEDICALEMERGENCYRESPONSETEAMTEAM
MERTMERTMERTMERTMERTMERTA teaA teaA teaA teaA teaA team of dedicatedm of dedicatedm of dedicatedm of dedicatedm of dedicatedm of dedicatedpre-hospital traumapre-hospital traumapre-hospital traumapre-hospital traumapre-hospital traumapre-hospital traumapre-hospital traumapre-hospital traumapre-hospital trauma specialists who fl y specialists who fl y specialists who fl y specialists who fl y specialists who fl y specialists who fl y specialists who fl y specialists who fl y specialists who fl y direct into battle direct into battle direct into battle direct into battle direct into battle direct into battle direct into battle direct into battle direct into battle areas to retrieve areas to retrieve areas to retrieve areas to retrieve areas to retrieve areas to retrieve areas to retrieve areas to retrieve areas to retrievewounded soldierswounded soldierswounded soldierswounded soldierswounded soldierswounded soldierswounded soldierswounded soldierswounded soldiers
ARMY MEDIC Magazine 6
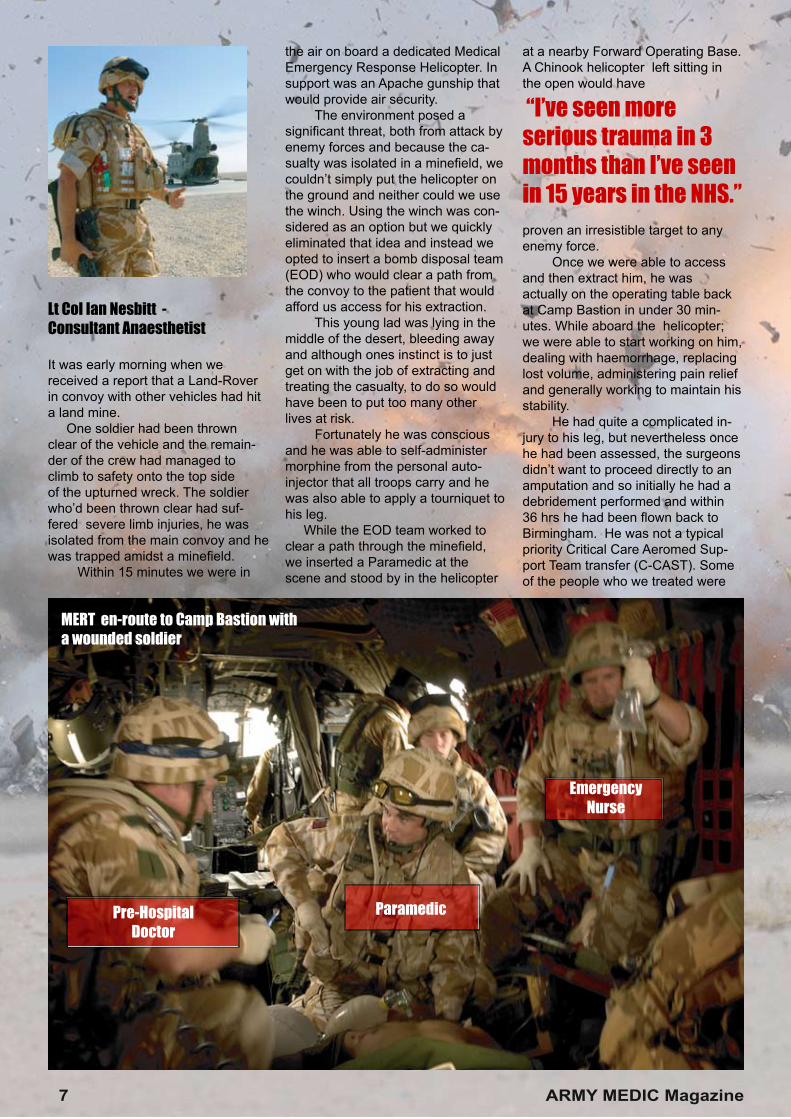
Pre-HospitalDoctor
Paramedic
EmergencyNurse
Lt Col Ian Nesbitt - Consultant Anaesthetist
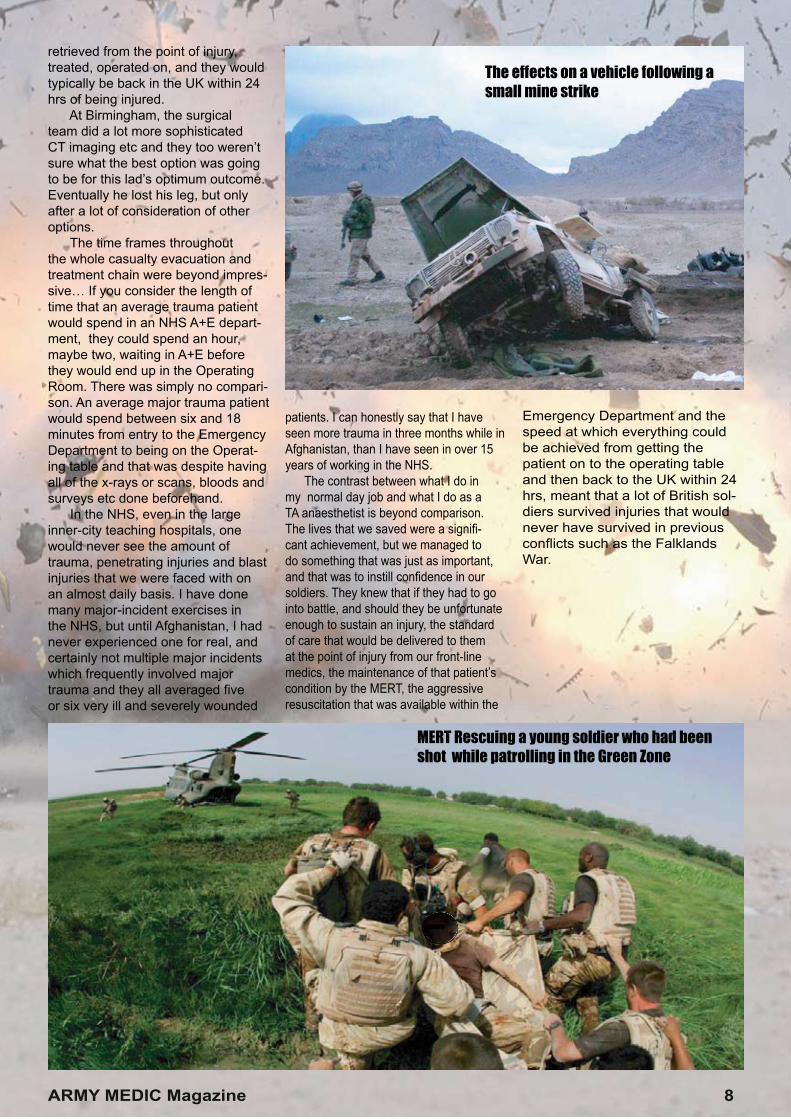
It was early morning when we received a report that a Land-Rover in convoy with other vehicles had hit a land mine. One soldier had been thrown clear of the vehicle and the remain-der of the crew had managed to climb to safety onto the top side of the upturned wreck. The soldier who’d been thrown clear had suf-fered severe limb injuries, he was isolated from the main convoy and he was trapped amidst a minefi eld. Within 15 minutes we were in
the air on board a dedicated Medical Emergency Response Helicopter. In support was an Apache gunship that would provide air security. The environment posed a signifi cant threat, both from attack by enemy forces and because the ca-sualty was isolated in a minefi eld, we couldn’t simply put the helicopter on the ground and neither could we use the winch. Using the winch was con-sidered as an option but we quickly eliminated that idea and instead we opted to insert a bomb disposal team (EOD) who would clear a path from the convoy to the patient that would afford us access for his extraction. This young lad was lying in the middle of the desert, bleeding away and although ones instinct is to just get on with the job of extracting and treating the casualty, to do so would have been to put too many other lives at risk. Fortunately he was conscious and he was able to self-administer morphine from the personal auto-injector that all troops carry and he was also able to apply a tourniquet to his leg. While the EOD team worked to clear a path through the minefi eld, we inserted a Paramedic at the scene and stood by in the helicopter
at a nearby Forward Operating Base. A Chinook helicopter left sitting in the open would have
“I’ve seen more serious trauma in 3 months than I’ve seen in 15 years in the NHS.”
proven an irresistible target to any enemy force. Once we were able to access and then extract him, he was actually on the operating table back at Camp Bastion in under 30 min-utes. While aboard the helicopter; we were able to start working on him, dealing with haemorrhage, replacing lost volume, administering pain relief and generally working to maintain his stability. He had quite a complicated in-jury to his leg, but nevertheless once he had been assessed, the surgeons didn’t want to proceed directly to an amputation and so initially he had a debridement performed and within 36 hrs he had been fl own back to Birmingham. He was not a typical priority Critical Care Aeromed Sup-port Team transfer (C-CAST). Some of the people who we treated were
MERT en-route to Camp Bastion with a wounded soldier
7 ARMY MEDIC Magazine
retrieved from the point of injury, treated, operated on, and they would typically be back in the UK within 24 hrs of being injured. At Birmingham, the surgical team did a lot more sophisticated CT imaging etc and they too weren’t sure what the best option was going to be for this lad’s optimum outcome. Eventually he lost his leg, but only after a lot of consideration of other options. The time frames throughout the whole casualty evacuation and treatment chain were beyond impres-sive… If you consider the length of time that an average trauma patient would spend in an NHS A+E depart-ment, they could spend an hour, maybe two, waiting in A+E before they would end up in the Operating Room. There was simply no compari-son. An average major trauma patient would spend between six and 18 minutes from entry to the Emergency Department to being on the Operat-ing table and that was despite having all of the x-rays or scans, bloods and surveys etc done beforehand. In the NHS, even in the large inner-city teaching hospitals, one would never see the amount of trauma, penetrating injuries and blast injuries that we were faced with on an almost daily basis. I have done many major-incident exercises in the NHS, but until Afghanistan, I had never experienced one for real, and certainly not multiple major incidents which frequently involved major trauma and they all averaged fi ve or six very ill and severely wounded
patients. I can honestly say that I have seen more trauma in three months while in Afghanistan, than I have seen in over 15 years of working in the NHS. The contrast between what I do in my normal day job and what I do as a TA anaesthetist is beyond comparison. The lives that we saved were a signifi -cant achievement, but we managed to do something that was just as important, and that was to instill confi dence in our soldiers. They knew that if they had to go into battle, and should they be unfortunate enough to sustain an injury, the standard of care that would be delivered to them at the point of injury from our front-line medics, the maintenance of that patient’s condition by the MERT, the aggressive resuscitation that was available within the
Emergency Department and the speed at which everything could be achieved from getting the patient on to the operating table and then back to the UK within 24 hrs, meant that a lot of British sol-diers survived injuries that would never have survived in previous confl icts such as the Falklands War.
MERT Rescuing a young soldier who had been shot while patrolling in the Green Zone
The effects on a vehicle following a small mine strike
ARMY MEDIC Magazine 8
MEDICAL
IN THE ARMY THERE’S NO SUCH THING AS A ROUTINE OPERATION.
The Army Medical Services are looking for Territorial Army recruits. You’ll retain your NHS job, bringing your skills to the Army and in return; while deployed both you and your NHS hospital will be financially compensated, but the greatest reward will be the clinical and professional development that you will gain.
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Find out more
MANAGING ONE OF THEBUSIEST A+EDEPARTMENTS ON THE PLANET
Maj Steve Gallacher QARANC (V)Age 48 A+E Charge NurseNorth Wales
ARMY MEDIC Magazine 9

More than 70% of the unit had previ-ous Operational experience in Iraq during 2003-04 and so we thought that we would have a fairly good idea of what to expect. Iraq had provided us with a good grounding, but Afghanistan was going to be a very different experience and we quickly realised that we would have to seriously raise our clinical game if we were going to be ready for the challenges that lay ahead. In preparation for Op HERRICK we began specialist training in Janu-ary 2007. We started by examining how we were going to function as a unit and of course as individual departments. Looking at skill-mix and the abili-ties and experience of the individuals who we would be taking with us was a critical aspect of that process, not just from the perspective of clinical governance; we took a hard-nosed practical look at each individual and we clearly identified their strengths and weaknesses. We started our build-up training with an eight-day hospital exercise that was held at the Army Medical Services Training Centre near York, a state-of- the-art facility that can be adjusted to run almost any scenario that you might imagine. This initial exercise and the training that fol-lowed was essential, because it was
the first time that we, as a depart-ment, had worked together for quite some time, and you have to bear in mind that during our deployment to Iraq, many of us had deployed at dif-ferent times and with different units, and so this exercise was just the first of many training opportunities that we would have to work together as trauma teams before we headed off to Afghanistan. For a full five months we were able to measure our capabilities, test our systems and develop new skills. A lot of us took the chance to at-tend specialist courses in Battlefield Advanced Trauma Life Support and Military Major Incident Management. Some of our surgeons and A+E spe-cialists went across to Denmark to practise specialised trauma surgical techniques and of course because we expected children through the A+E, many of us attended Advanced Paediatric Life Support courses too. During the build-up training phase, one of the things that we identified was that the A+E could become overwhelmed with anything over four T1 or T2 patients and we quickly realised that we would need to expand the size of the department and introduce other teams from ward areas who could augment the A+E specialist teams. Part of the train-ing process involved getting these
augmentees use to the horizontal approach of the trauma team and secondly we clearly identified what they could do within the limits of their scope of clinical practice. So we had rehearsed and trained for multiple scenarios, over and over again, and on the first day, all of that training and preparation paid off in spades. 1600 hrs DAY 1 Camp Bas-tion Afghanistan. A mass-casualty alert was called. At the time, we were shadowing and working along-side the outgoing 212 (Yorkshire) Field Hospital (V). We immediately thought “DRILL.” Wrong! It was the real thing. But we had teams from two Field Hospitals, our own who had just arrived and 212 who were hand-ing over before their return to the UK. That afternoon eight casualties from the Afghan National Army were brought in. Three of them died. Their vehicle had been hit by an Impro-vised Explosive Device (IED). Dealing with that first mass-ca-sualty situation on day-1 proved that all the effort that had gone into our pre-deployment training was worth it. There was one aspect of that training that proved invaluable and that was Casualty Simulation training. The Army uses actors who are amputees, because practising the treatment of major traumatic amputation, even though you know that it’s all done
10 ARMY MEDIC Magazine
using special effects, stage make-up and actors, is an excellent way to desensitise you in preparation for the first time that you see a real life traumatic amputation. On the first day that training paid for itself ten times over. Even if you work in one of the major London trauma hospitals it is unlikely that professionals would have the opportunity to deal with the types of trauma that we were treat-ing. Major trauma, with penetrating injuries to the head, chest, torso and the traumatic amputation of limbs. During our operational tour this ex-perience was not a rarity, this was an everyday event… One of our most successful days as a trauma team occurred when we had to respond to a suicide bombing in a place called Gereshk. 29 people were killed at the scene and there were approximately 60 injured. We were placed on stand-by to receive two T1 casualties, we got eight, and then, no sooner had we cleared our decks, than we got a second wave of casualties. The tempo that day was incred-ible - I doubt if anything could pre-pare you for something like that. All three ISAF hospitals were working flat-out. The Canadians and espe-cially the Dutch were hit hard. Most people pick up a newspaper and they read 50 people killed in a suicide bombing, and 100 injured. These days it seems to be such a common news event that it only warrants page four or five and a couple of inches of column space in a newspaper, and so unless you’ve actually been on the receiving end of dealing with some of these casualties you have no concept of what that scene is go-ing to be like and more importantly how you’re going to manage it. In such a situation, you are depending on everybody to function at the limits of their scope of clinical ability. But when it all pulls together and you’ve successfully managed the situation and when the department is back to normal and good-to-go again, it is a really good feeling to know that even when you’ve all been pushed to the limit, the job got done and was done well… The army has a motto “Train Hard, Fight Easy.” In our case the robust training that we went through made saving so many lives so much easier. Ultimately, the staff that you have
in the hospital is all that you have to work with. There are no agency staff and so it’s imperative that you look after and support your people, keep them motivated, keep them healthy, make sure that they’re eating, make sure that they’re sleeping and give the ones who are fatigued some down-time. The welfare aspect of managing my department was far more intense than any level of re-sponsibility that I’ve ever experienced in an NHS hospital back at home. The bottom line was that the A+E department did not stand alone, it was so very well supported by every other department in the hospital and the flip side of that coin was that we too supported the wards and other departments. What we never forgot was that when we had an influx of casualties, they might spend an hour or two in the A+E, but that wave of chaos swept through the hospital at different rates and created different problems and different workloads for other departments and so once
An actor from the group “Ampu-tees in action” playing the part of a mine-strike victim during pre-deployment training
ARMY MEDIC Magazine 11
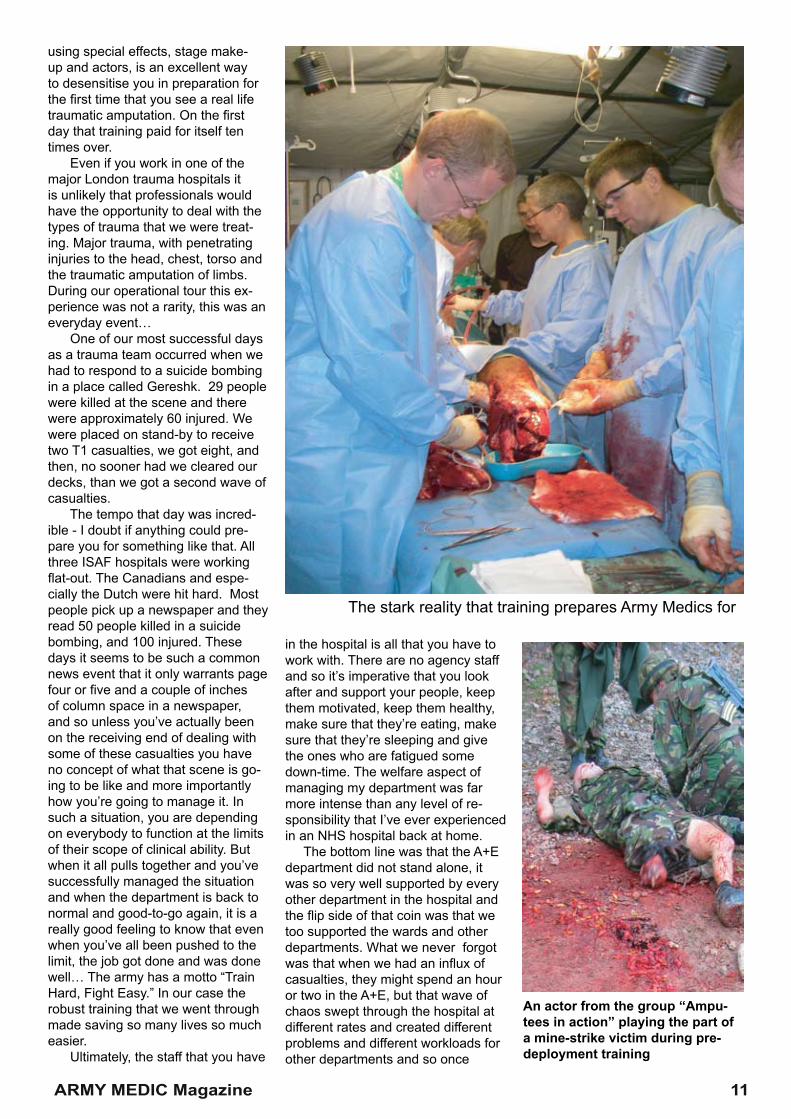
The stark reality that training prepares Army Medics for
the pressure was off the A+E, it was essential that we helped to prop up other clinical areas. All of the routine daily health problems were dealt with by a separate but co-located primary health-care centre and that meant that the A+E was never swamped by inappropriate attendees, the type of which you might get in an A+E back at home. Instead of dealing with patients who were trying to get out of you what they were unable to get from their GP, we were able to focus on trauma management. Also, we were there dealing with the effects of violence, there wasn’t any violence in the depart-ment and there were no drunks or drug addicts to deal with. We weren’t frightened, we didn’t need security and so all of the daily pressures that you might experi-ence in a normal A+E department were all gone. There were no ambulances lined up outside of the department waiting for beds. In to-tal our whole hospital only had 23 beds, but those beds were man-aged extremely well and discharge planning started as soon as the patient arrived in the A+E. I derive a great deal of sat-isfaction from my NHS job, but managing an A+E in a military environment has exceeded my expectations, the rapid pace of personal change that I experi-enced was astonishing and I grew not only as a clinician but as a manager too.
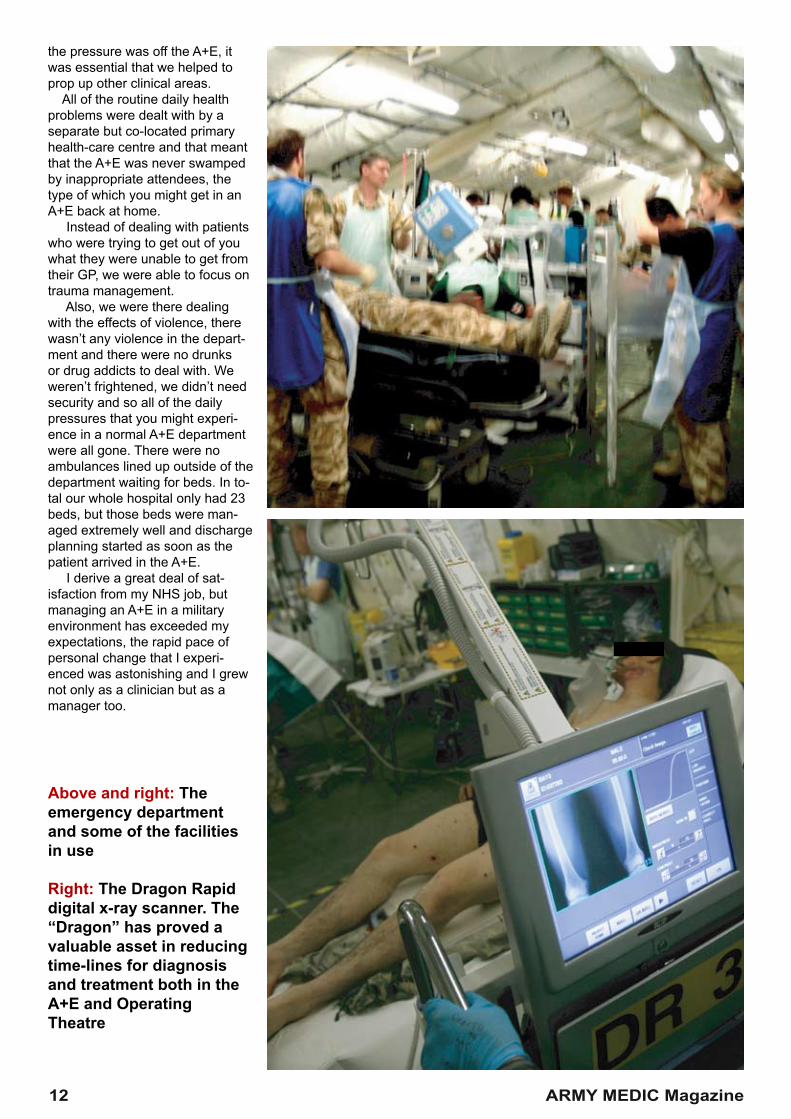
Above and right: The emergency department and some of the facilities in use
Right: The Dragon Rapid digital x-ray scanner. The “Dragon” has proved a valuable asset in reducing time-lines for diagnosis and treatment both in the A+E and Operating Theatre
12 ARMY MEDIC Magazine
A NURSE’S WAR DIARY
Captain Jude Hadfi eldAge 32. MarriedITU NurseNorth East
It was Christmas Eve and everybody was in a really festive mood. But that all changed when we got news that one of our lads was en-route after being blasted in a mine strike. He had suffered multiple traumatic amputations. He was saved but his injuries were horrifi c. It was as if somebody had just cancelled Christ-mas and that was something that was felt throughout the camp, not just in the hospital. It was a really low point, but it was also a sombre high point because I think that everybody felt honoured to just be there and to be able to give of our specialist skills to save this lads life. My deployment to Afghanistan at the end of 2007 was my fi rst Opera-tional Tour of duty. But I, along with my other TA colleagues, was given almost twelve months’ notice and so everybody including my employer had plenty of time to get used to the idea and to make preparations. Until I got there I don’t think that I knew what it was really going to be like. I remember fl ying into Kandahar - that was just surreal… We were fl ying
on what felt like an easy-jet fl ight; of course we were all in uniform, but because of the threat of attack by ground-to-air missiles, half an hour before we landed, the cabin lights were turned off and everybody had to put on their helmets and body-armour. It was only then that I took a deep breath, my heart started pound-ing and I thought, my goodness this is it... After we landed we had a tactical transfer fl ight, this time in a Hercules transport plane and an hour later we fi nally arrived at Camp Bastion. I will always remember the Royal Marines who fl ew into Afghanistan with us. I will never forget seeing so many young lads preparing to go out onto Operations, well-trained and well-prepared Marines who were looking forward to doing the job that they had been trained for, but I had a sick
feeling in my stomach that came with the realisation that this is not a game, and I will never forget how I hoped that the faces that I remembered from our fl ight would not be the faces that I would see coming back into the hospital as casualties. For the fi rst couple of days I felt quite lost and a little intimidated by my surroundings. There was so much activity on the camp and there were so many people walking around, all carrying weapons and all getting ready to go out on Opera-tions. It wasn’t just the hospital that was having a change-over of staff, most of the Combat Regiments were changing over too. That fi rst night, I couldn’t sleep for the sound of Chinook and Apache helicopters taking off and landing, they seemed so close and I remem-ber thinking: Yep! I am defi nitely in Afghanistan… It’s not that I went there with any real expectations, but despite hav-ing seen the place in presentations, until I actually arrived, I could never have had a true appreciation of what it was going to be like. I shared my accommodation with seven other people. One of them was a Danish nurse who would be working with me in ITU. I only knew three of the girls and even then I didn’t know them
“It was as if somebody had just cancelled
Christmas”
ARMY MEDIC Magazine 13
ITU IN AFGHANISTAN

reading them because I would start getting emotional too. But at least they would know that their mates had been beside them when they were at their lowest point. The bonds that ex-ist between soldiers, warriors really, are unlike any other that I’ve ever experienced. These men are tough profes-sionals, but the compassion that they have isn’t just reserved for their comrades it is demonstrated every day on the fi eld of battle. Caring for the visitors was harder in some ways, because these big strong lads would come into the ITU to see their mate who just a few hours earlier they’d been having a laugh and a joke with; seeing their mate lying in bed, attached to a ven-tilator and all of the monitoring and machinery that makes up an ITU; the colour would simply drain from their faces. You cant help yourself, your heart goes out to them, you know that in a few hours these visitors will be back out on the front lines at their Forward Operating Bases (FOBs), facing the same dangers and the same enemy that only hours or days before had come so close to taking their mate’s life. Many a time I would want to give them a hug, but you
Flight 2: A tactical fl ight on-board a military transport plane to our fi nal destination
Flight 1: The RAF’s answer to easy-jet - a non-tactical fl ight until shortly before our approach to Kandahar when the lights went off and we had to put on helmets and body armour because of the risks from ground-to-air missile attack
14 ARMY MEDIC Magazine
to know people because you live around them, the layout is such that you always seem to see people from other departments and despite a busy tempo there always seems to be time for a quick chat in the corri-dor. I don’t think that I’ve ever expe-rienced the same type of friendship or the same sociable atmosphere in a normal NHS environment. This may have something to do with there being no place for pettiness or selfi sh behaviour in a war environ-ment. I don’t know, but it’s a great place to work. It may sound like a cliché but to look after our soldiers was a privi-lege. Many of them were young but they were also very professional and so very brave. Often their friends or their Com-manding Offi cers would come in to visit patients in the ITU. We encour-aged visitors to write little messages so that the patients might be able to read them if they recovered and woke up. Those patients that were ventilated and awaiting C-CAST (Critical-Care Aeromed Support Team) particularly stuck in my mind. Some of the messages that were written were heart wrenching… and after a while I just had to stop
that well, at least not well enough to share intimate stuff with. Of course that situation didn’t last for too long. With regard to work, I wasn’t worried about my ability to do my job but I was concerned about being able to look after the Afghan patients and being able to do it well. That was more about understanding them and their culture, their beliefs and cus-toms more than anything else. I knew that they were a proud, almost ancient, civilisation whose customs and culture had remained largely isolated from western Euro-pean infl uences for decades, even longer… I also knew that they lived in fear of the Taliban returning and that if they were found to have had any contact with ISAF (International Security Assistance Force) that they might be killed. However, there is very limited healthcare available in the Afghan communities and what is available is, to say the least, poor. They under-stand this, and if they found there way into our hospital, for whatever reason, they were always grateful for our help. The Field Hospital is unlike any-where I’ve ever worked. It’s such a sociable place. Apart from getting

can’t, I could tell that it was taking all of their resolve to keep it together and that a hug might just tip them over the edge. Ultimately they have their own unique ways of coping with the stresses that are generated following the loss or near loss of a mate. But I have such admiration for the way that they maintain their standards and values despite situa-tions like this. When a casualty arrived, rarely would there be a straightforward story, sometimes the story would be very sketchy but more often we would never know what had hap-pened. I remember three children being brought in and unfortunately one didn’t survive. Basically they had been brought in because they’d been playing catch with an old Butterfly mine from the 1980s. It exploded and the children had received severe penetrating shrapnel injuries. When we had to look after chil-dren, some of them were very ill in-deed, often they would be at death’s door, but before long they were taken off the ventilator and within days they were running about the hospital. So in that sense caring for children was really rewarding. Afghanistan is a very different world from that which we know, these people have grown up knowing nothing else but mines, and they’ve suffered this across three genera-
tions. So a child being injured by a mine was a commonplace occurrence long before we arrived. At least now a lucky few survive because they have ac-cess to a First- World medical facility. There were so many patients who weren’t expected to survive and yet they did. Some who we thought would never see again regained their sight and some who suffered neurological trauma and who we thought would be permanently disabled we not. Every Thursday there was a trau-ma conference between the hospital at Camp Bastion, Iraq and the Royal College of Defence Medicine at Bir-mingham and they were able to feed back on the progress of patients back in the UK and US. It became such an important aspect of our working week to be able to follow up on those pa-tients who had been flown home and whose recovery hung in the balance. Coming home was strange, I was excited to be going home and to see my husband and family again, but it was a low point because I was really going to miss all of the people that I’d been working with, the
friends I’d made and the work that we were doing, the experience as a whole had been so fulfilling and so I definitely had mixed emotions. But seeing my family again was great, even though a part of me is still in Afghanistan. It’s easy to forget that while we were there in the midst of war, nothing much ever changes at home and people’s lives at home continue to revolve around the shop-ping, Coronation Street and X Factor. There is something quite small and some might say petty that sticks in my memory and that was receiving, or not receiving, mail. I remember phoning home and saying, just send me a letter so that I’ve got something to open. A few days without mail was devastating in a way that I can’t ex-plain. People back at home just didn’t seem to realise how important receiv-ing post was out here. OK, we had e-mail access and satellite phones,
Living conditions are basic to say the least,but they are more than compensated for by the high levels of morale and team spirit
ARMY MEDIC Magazine 15
The Intensive Care Unit
but when you are on an Operational tour it still doesn’t beat having some-thing to open. I’ve never experienced anything like that before. I’m at home now with my central heating on full-blast and I can have a lovely warm bath whenever I need one, but I’ll always have an apprecia-tion of what our soldiers and service people are enduring on Operations. I’ll remember the final weeks of our tour when because of a fuel shortage and amidst a very cold Afghan winter, we were often so very cold and damp that I could feel a constant chill in my bones. I’ll remember thinking that I might never feel warm again, but how we were still in such relative comfort and luxury compared to the soldiers that were out at the FOBs. When there are reports on TV of heavy fighting, I’ll be thinking about everybody standing-by at the hospital waiting to receive casualties, and every time there’s a 30-second news story about another soldier being killed, I’ll think about all of the ramp ceremonies that I attended, when we watched a soldier’s coffin draped in the flag being taken onto a Hercules to be flown back home. That will stay with me always. But more than any other, the memory that will endure for the rest of my life, is the memory of those patients that we saved, the unex-pected survivors. It’s been a big chapter in my life and so different to anything that I’d ever done before. I’ve been travelling, I’ve seen a big chunk of the world and I’ve had my adventures, but this was something completely different and something that I’m really glad that I’ve done.
RADIOGRAPHERSWANT TO SEETHINGS YOUHAVEN’T SEENBEFORE?We want to be transparent with you. Become a Radiographer in the TA and you’ll travel.
You’ll put your skills to the test in some of the most demanding conditions in the world.
But you’ll also receive the personal and professional training that will help you move on in your NHS job too.
You’ll get paid. And hopefully have fun. Everything clear?
ARMY MEDIC Magazine
List of abbreviations:Military abbreviations that you might not recog-nise. Here are a few.
QARANC Queen Alexandra’s Royal Army Nursing Corps.
RAMC. Royal Army Medical Corps.the (V) at the end of these abbreviations denotes Volunteer, indicating that the person is a reservist.
Cpl CorporalSgt SergeantCapt CaptainMaj MajorLt Col Lieutenant Colonel
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Clinical excellence: Maj MarkSaunders, QARANC, managedcomplex operations from BastionField Hospital’s two-bed theatre
Theatreo f w a r
Top-class treatment a certaintyat Helmand’s hi-tech hospital
Article Reproduced with permission: Soldier Magazine Mar 2008
ARMY MEDIC Magazine 16

Report: Stephen TylerPictures: Graeme Main
N the heat of a contact in Afghanistan’s volatile Helmand province, a soldier falls victim toenemy fire. As the battle rages, a medic arriveson the scene, puts well-rehearsedemergency battlefield first aid drills intoaction and calls for a casevac to fly thestricken soldier to a dedicated helipadyards away from the front door ofBastion’s field hospital. What follows is a military medicalresponse envied and admired the world over and one which has been responsible for saving the lives of scores of soldiers and civilians injured in the field. Immediately after being brought to thehospital, patients are whisked into a four- bed emergency room where a team of upto nine specialists assesses their injuries,applies initial treatment and coolly andquickly prepares the patient for surgery,often in less than 20 minutes. Officer in command of the emergencyroom, Maj Mick Carr, QARANC, a Territorial Army volunteer who works as a resuscitationofficer in civvy street, isunderstandably proud ofhis team’s efficiency. “When we get a warn-ing we sometimes use a little bit of guesswork and experience to set the team up and make sure we have enough staff,” said Maj Carr, emphasising that every member of the unitis given a specific role to concentrate on. “In a way we don’t worry about wastehere. If we hear someone is coming in,we get the drugs out and don’t worry if they aren’t used for whatever reasonbecause we would sooner have the drugsready to go. “In Europe you have the golden hourbetween being injured and getting onthe treatment table and although that’swhat we aim for, it isn’t always possible.To combat that we throw resources atthe treatment to try and catch up. “We work in quite a tight area and I manage the team so that everyone isconcentrating on doing their job andtheir job only.” Before progressing to surgery, a patient requiring an X-ray can have thescan done without being moved fromthe treatment bay thanks to two high- tech Dragon direct digital scanners.The technology in the £10,000
machines is so new that they are rarelyfound even in NHS hospitals, but Bastion’s radiographers have immediateaccess to two. Fully portable and touchscreen-operated, the scanners provideemergency room staff with on-screenX-rays in a matter of seconds – a poten-tially life-saving improvement on the several minutes traditional scans take to produce. Radiographer Cpl Catherine Lee, anRAMC volunteer who carries out thesame role in her day job at a hospital in Exeter, demonstrated the machine’s abil-ity to zoom in and out, change focus and even look at saved X-rays with just a few touches of the display screen. “It means that the doctors can look at the scans there and then alongside the patient,” she said. “We are the only people who employ it in this sort of role and it makes a massive amount of difference. I hope that I can use everything I’m learning here when I go back home.” Anyone requiring surgery for their injuries can take comfort in the fact that
Bastion’s two fully-functional operating theatres are staffed by expert general, vascular and orthopaedic surgeons and con-tain the same equipment found in UK hospitals. Support for neurological surgery is based a short flight away in Kandahar and the entire streamlined pro-cess makes OC theatres Maj Mark Saunders, QARANC, very proud. “I think coming here has been a tick in the box
for all of us,” he told Soldier. “The guys throughout the process deserve to get the praise they are due.” Maj Saunders’ second in command, Maj Jack Hornby, QARANC, added that despite the desert setting of the two theatres, Bastion’s surgical staff are always confident of performing operations just as expertly as they would in the UK. “The kit and equipment is pretty much the same,” he said. “When we have finished in theatre and everyone is clean and dry, we hope the outcome is also the same.” The next link in Bastion’s well-oiled medical chain is moving patients into one of the four intensive care ward beds or one of the 23 bays in the two regular wards. The human touch provided by the expert nursing staff on the wards makes recuperation an easier pill to swallow for any of the multinational troops or Afghan civilians who find themselves treated there. Maj Shaun Jones, QARANC,
explained: “We have had a lot of busy times, but when it quietens down it is nice because we can spend a bit more time with the local children. “It is quite hard for them because they don’t speak the language, but we try to make it easier by spending as long as possible with them while they are recovering. This is superior to the NHS because on rounds we have the surgeons and the rest of the staff all standing around the bed and making important decisions there and then.” Cpl Tracy Bazzard, a registered nurse serving with QARANC, added: “Work-ing in theatre gives me the chance to treat patients I would never get to treat in the UK. Here you get to overcome the communication barrier and make sure that they receive the best care we can give them.” Despite the number of injuries recorded on the current Operation Her-rick being higher than on any previous deployments, it is worth noting the slightly less dramatic truth behind the headlines. For every serious battlefield injury treated at Bastion field hospital there are dozens more minor complaints,
‘The amount ofpenetrating traumawe see is farabove what civilianteams deal with, sopeople are goingto want to listento what we havelearned out here’
I
17 ARMY MEDIC Magazine
ranging from pulls and strains picked up at the gym to cuts and grazes that are an occupational hazard for some of the Army’s tradesmen. Maj Carr concluded: “The majority of work we do is on minor injuries and illnesses, things like ankles and wrists. “There are also trade-specific injuries– cooks get burnt, locally employedcivilians might cut their hands and me-chanics get oil in their eyes. It isn’talways major trauma. Having said that,the amount of penetrating trauma we see is far above what civilian teams deal with so people are going to want to listen to what we have learned out here.” Whether patients end up being released to carry on with their duties or are returned home to continue their recovery, they can rest assured that their care is managed by seasoned profession-als. In a conflict where casualties fromboth military and civilian backgroundsare an unfortunate inevitability, it iscomforting to know that no expensehas been spared in making their returnto good health a priority. ■
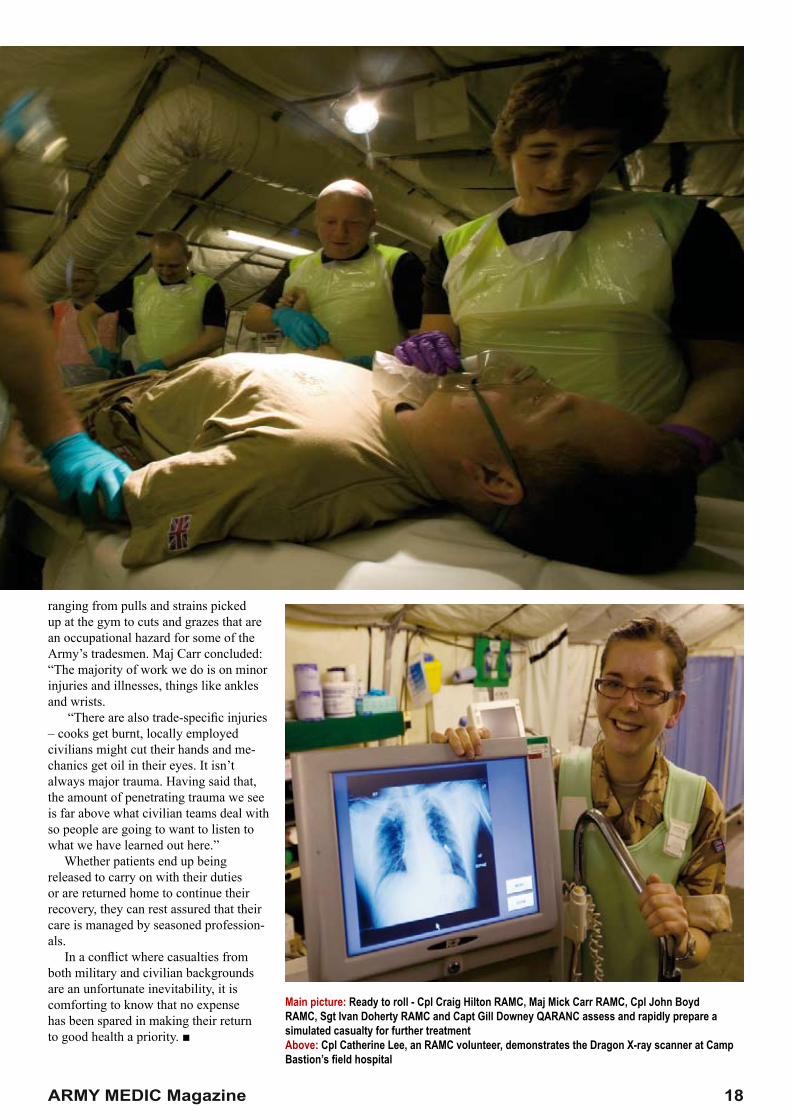
Main picture: Ready to roll - Cpl Craig Hilton RAMC, Maj Mick Carr RAMC, Cpl John BoydRAMC, Sgt Ivan Doherty RAMC and Capt Gill Downey QARANC assess and rapidly prepare asimulated casualty for further treatmentAbove: Cpl Catherine Lee, an RAMC volunteer, demonstrates the Dragon X-ray scanner at Camp Bastion’s field hospital
ARMY MEDIC Magazine 18
YOU HELP US SAVE LIVES WE HELP YOU CHANGE YOURS.
If you learn to use your clinical skills in some of the worlds most demanding and challenging clinical environments, you’ll be able to use them anywhere.
You’ll retain your NHS job and your NHS employer will be supportive of you becoming a Reservist. The NHS will give you up to and extra two weeks annual leave to help you train as a Reservist.
MEDICAL
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Find out more
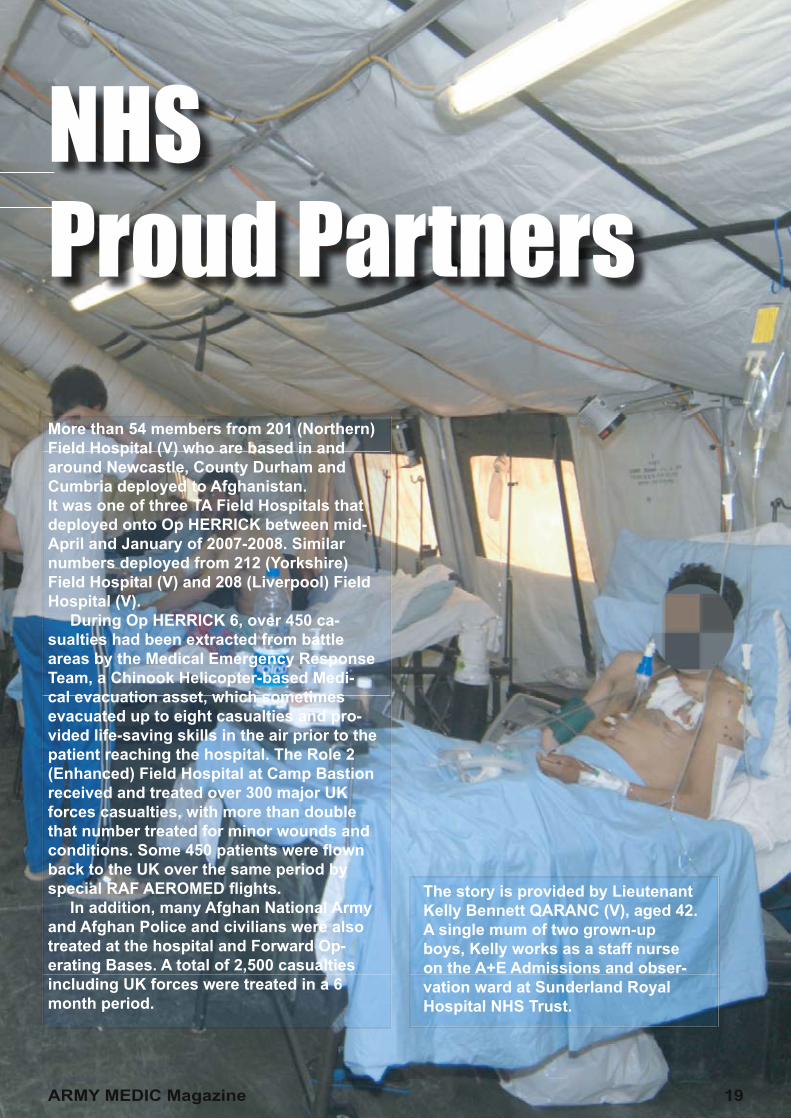
NHSProud PartnersMore than 54 members from 201 (Northern) Field Hospital (V) who are based in and around Newcastle, County Durham and Cumbria deployed to Afghanistan. It was one of three TA Field Hospitals that deployed onto Op HERRICK between mid-April and January of 2007-2008. Similar numbers deployed from 212 (Yorkshire) Field Hospital (V) and 208 (Liverpool) Field Hospital (V). During Op HERRICK 6, over 450 ca-sualties had been extracted from battle areas by the Medical Emergency Response Team, a Chinook Helicopter-based Medi-cal evacuation asset, which sometimes evacuated up to eight casualties and pro-vided life-saving skills in the air prior to the patient reaching the hospital. The Role 2 (Enhanced) Field Hospital at Camp Bastion received and treated over 300 major UK forces casualties, with more than double that number treated for minor wounds and conditions. Some 450 patients were fl own back to the UK over the same period by special RAF AEROMED fl ights. In addition, many Afghan National Army and Afghan Police and civilians were also treated at the hospital and Forward Op-erating Bases. A total of 2,500 casualties including UK forces were treated in a 6 month period.
The story is provided by Lieutenant Kelly Bennett QARANC (V), aged 42. A single mum of two grown-up boys, Kelly works as a staff nurse on the A+E Admissions and obser-vation ward at Sunderland Royal Hospital NHS Trust.
ARMY MEDIC Magazine 19

Six clinicians were mobilised from my hospital: including myself there were two Ward Sisters, a Matron, a Sur-geon and an Operating Department Practitioner. The Trust appealed for two of our team to be withdrawn from mobilisation. One, the Matron, was withdrawn on appeal but the second, the ODP, was upheld and he was sent despite the Trust’s appeal. Even though the MoD provided excellent levels of funding to help the NHS replace us while we were away, I along with my other TA colleagues were acutely aware that our absence from work for a four-month period could have an impact on our depart-ments. But we were all of us grateful for the excellent support that both the Trust and our work colleagues showed us. Our being mobilised was well planned for and with a year’s notice there were few surprises for anybody. To draw a comparison - it is no different from an individual re-questing a leave of absence, except this way the post isn’t just gapped, it is funded and well supported by an external body In fact the Army gives a longer period of notice for mobilisation than anyone would normally be able to give if they were to be injured, become ill or even if they became pregnant. So I suppose that in an or-ganisation as large as an NHS Trust, they must have to deal with so many un-planned episodes of sickness and absence that a funded absence must
have been a welcome change. Personally speaking, the TA and this operational tour has been excel-lent value. Prior to my mobilisation to Afghanistan, I attended a two-week offi cer training course held at both the Army Medical Services Training Centre near York and at the world famous offi cer training college, The Royal Military Academy Sandhurst. The Army provided me with the per-sonal and professional development that I would need to prepare me for working in a management role and, in contrast to my NHS career, I hadn’t yet had that opportunity to develop myself in such an intensive waybecause in the NHS I was still work-ing as a junior staff nurse. The ward that I was working on in Afghanistan was very similar to that where I work in the NHS, the main difference being that I was mostly caring for Afghan National Army, civil-ian adults and children and on oc-casions Taliban fi ghters. There were obvious cultural differences that I had to come to terms with and working through interpreters was an inter-esting experience, but patients are patients and the demands of nursing in a busy department are the same the world over. In any confl ict those who are in the most need of our help are often the innocent and the vulnerable, the old, the sick and of course children, those who are either too weak or too young to escape the fi ghting.
The injuries were different, usually penetrating injuries from explosions or gunshots, but otherwise the work was very similar to that which I do at home. Some of the cultural differences were very diffi cult to come to terms with. I remember two children who had been brought to the hospital by their families and both children were equally ill following major trauma. The difference between the two chil-dren was that one was a boy of about ten years of age and the other was a girl of about eight. Whenever a male child was admitted, a male family member would always remain at the patient’s bedside for the duration of his stay in hospital, but typically whenever we had a female child admitted the family would abandon the little girl and might not return for weeks. Working in a Field Hospital for the fi rst time was strange - ultimately you apply exactly the same standards to those which you would fi nd in the NHS. We were regularly audited on everything from infection control and clinical governance to anything that might happen in any NHS hospital, the major difference is that your working in a tent. Also, we didn’t have cleaners or ancillary staff and so if the fl oors needed mopping, or if the bins needed emptying it was the Registered nurse or the HCA who would do it. The equipment that we used was basic, it has to be, because it has to be robust and there were times when we might have to impro-vise and if anything that has made me really appreciate how much I actually have back in the NHS. I would certainly think twice about complaining about how hard done to we are in the future. One example: we were waiting on a delivery of Monkey Poles from the UK and nurs-ing orthopaedic patients who want to sit themselves up without such a simple device can be a nightmare. So, one of the lads got the combat engineers who were based in an-other part of the camp to weld some poles together and come up with a design. They were basic, but they did the trick… If I’ve learnt anything from being an Army nurse, it’s the ability to adapt and fi nd a way to get things done and to use everything and everybody to contribute to fi nding a solution to a problem. Moaning about stuff serves only to fuel the problem
Kelly working alongside one of her nurses
20 ARMY MEDIC Magazine

and create inertia, while proactive problem solving and a can-do at-titude can not only resolve problems but it can provide the team with a dif-ferent and more rewarding sense of fulfi lment. The opposite outcome and the opposite approach of blaming the world for your ills and never solving anything is not something that I could tolerate again. The atmosphere in the hospi-tal was very relaxed and so I really enjoyed nursing there. I can only imagine that was the way that nurs-ing use to be. At home there is a constant pressure on us for beds and to make beds available, but even though we were only a 23-bed facility and, should a mass-casualty situation arise, all of those beds could be required at any time, there wasn’t the same pressures. The bed manager did his job and we were relied upon to provide the most effi cient and ef-fective use of the resources that we had available to us. I think too, that although we had admin to do, it was signifi cantly less than that which I do at home. Everything was hand writ-ten and I didn’t have to spend a third of my day sitting at a computer and neither did anybody else. The care that we delivered was completely patient-focused and it seemed that nothing was allowed to undermine that focus. Consequently, the whole experience was enjoyable. I had time to sit with patients and time to spend with my colleagues, we were less well resourced in comparison with the critical care areas but the morale and sense of purpose that we
all shared ensured that the burden of the job and the responsibility to get things done was shared too.The team spirit in the hospital was second to none and I think that was one of the main reasons why things got done and why people were so eager to co-operate and help each other out. Inter-departmental relation-ships were excellent and we all felt comfortable spending time in each others departments. Nobody would ever comment that you shouldn’t be in a particular ward or department, even people off-duty would pop in for a cup of tea. And even though we were a part of a massive organisa-tion; i.e. the Army, everybody felt really appreciated and we felt that we counted and that what we were doing counted for so much. It’s so easy to get lost in large organisations, but in the Army I was never treated as a number or as just one more cog in the machine. We all knew each other and all looked out for each other and that made such a difference to the way that we worked as a whole. I thought that I’d have returned exhausted - in fact I have returned in-vigorated and with a renewed sense of purpose and direction. After my experience as a team leader in Afghanistan and the intense package of personal and professional development that I underwent during my offi cer training, I am now ready for the challenge of the next step in my NHS career and I anticipate ap-plying for a junior sister’s post in the very near future.
Ken Bremner CEO City Hospitals Sunderland NHS Trust
“We are very proud of all our staff who have recently returned from serving with military units overseas,” said chief executive Ken Bremner. ‘‘To know that their professionalism has helped medical teams in such circumstances is a hum-bling experience and during their absence friends and colleagues from City Hospitals Sunderland have kept in touch with them, passing on good wishes and news as well as Christ-mas cakes and gifts and of course organising welcome home celebrations. For some of those concerned, this was not their fi rst posting to front-line units and we know the dedication that is needed to leave loved ones behind and place themselves in positions of danger far away from friends and family.”
ARMY MEDIC Magazine 21
Kelly and a few mates at the EFFI
Secretary of State for HealthCalls on NHS Trusts to Support Reserve ServiceSpeaking at a dinner to host NHS executives from across the North West of England, the Secretary of State for Health the Rt Hon Alan Johnson MP asked NHS executives to be proactive in their support of clinicians to become reservists in the Territorial Army Medical Services.
In his address the Secretary of State said; April 2008 marks the centenary of the Territorial Army. With ongo-ing military commitments across the globe, the role of reservists has never been more important. Increas-ingly, the TA is not just peripheral to what the regular army does – it is an essential part of all its operations. There is perhaps no more appro-priate time or place to talk about how the NHS and the armed forces can work together to improve healthcare for both serving troops and veterans. And in particular, what else we can do to encourage more NHS staff to become reservists. The House of Commons Defence Select Committee said in their report published in February this year, that the clinical care for UK servicemen and women who have been seriously injured is second to none. Defence Medical Services, working with the NHS, provide a truly world-class service, and this is something that we should commemorate this evening. But that doesn’t mean that there aren’t problems to resolve. Currently, there are nearly 12,000 men and women serving in Iraq and Afghani-stan alone. The majority of those who sign up to the armed forces are in better health when they leave the service than when they joined. But there are also more men and women returning from active service with serious injuries or lifelong health problems.
I am certain that my view refl ects the view of the public at large. The men and women who serve in the Brit-ish armed forces, who put their lives at risk on a daily basis, deserve the fi nest healthcare that it is possible to provide – regardless of whether they’re on active duty, if they’ve re-tired or if they are no longer in active service.
In November last year, I announced that we would extend the right to priority treatment on the NHS to include all veterans with service-related conditions, regardless of whether they were pensioners or not. I am proud that it was my own PCT in Hull that was the fi rst PCT to recognise the need to give veterans priority treatment - and I was pleased to extend what had been achieved locally into a national programme. So it is important to give veterans faster access to care, but in addition, I want to make clear today that the NHS has a duty to provide continuity of care to veterans. Ex-service men
and women have the right to receive exactly the same, high standards of care when they are civilians as they did when they were in the armed forces. For example, those who have lost an arm or a leg serving their coun-try and need their prosthetic limbs replaced, should be able to access the same state-of-the-art models they were supplied by Defence Medical services. And whilst waiting times have reduced dramatically every-where over the past ten years, armed forces personnel and their families should not fall to the bottom of any waiting lists for treatment when they move to a different location. Recent guidance makes clear that patients who are on waiting lists, but for what-ever reason, have moved to a differ-ent area, should not be penalised. Our armed forces deserve the best possible treatment and this is what they should get.
Recruiting More NHS Reservists:
The relationship between the NHS and the armed forces is not just about the care it offers to veterans. Right now, most of the medical staff working in our Field Hospital in Afghanistan are NHS Reservists. The benefi ts of being in the TA for NHS staff and their employers in terms of training and development are clear. It’s been estimated that
“I want to see moreNHS employers actively supporting their staff to become reservists”
22 ARMY MEDIC Magazine

Left to Right: Colonel RG Jackson, Commanding Offi cer of 207 (Manchester) Field Hospital (V), Rt Hon Alan Johnson MP, Secretary of State for Health, and Brigadier E Carmichael MBE, Commander 2nd Medical Brigade.
during a three month operational tour in Iraq or Afghanistan, a reservist will deal with more trauma than during fi fteen years working for the NHS. Just as important as building clini-cal skills are issues such as leader-ship, communication, adaptability and teamwork – often misleadingly thought of as “soft skills,” But of huge importance to today’s employers. In the words of Lieutenant Kelly Bennett, who served in a fi eld hos-pital in Afghanistan: “If I’ve learnt anything from being an Army nurse, it’s the ability to adapt and fi nd a way to get things done and to use every-thing and everybody to contribute to fi nding a solution to a problem.” I want to see more NHS employ-ers actively supporting their staff to become reservists. Being a member of the TA shouldn’t be simply tolerated by employers as an eccentricity as if it’s some kind of hobby or social club. It demands serious commitment and training and increasingly, it attracts the fi nest talent in the NHS and else-where. I know that most trusts are sup-portive of employees who want to serve in the TA, but some worry about managing staff absences and other diffi culties this may cause. But even if every NHS reservist was called up for an operational tour, the absence rate would comprise of less than one per cent of the average daily sickness absence rate of the NHS. All employers get six months to a year’s notice before an employee is called up for active duty and the TA works with employers and the reservist in question to ensure that any absence causes minimum dis-
ruption. The TA pays the salary of the individual in question during their tour of duty and tops up pension contribu-tions.
Future initiatives:
I know that there are particular short-ages of health specialists, such as intensive care nurses and neuro surgeons in the Defence Medical Services, available for deployment to both Iraq and Afghanistan. For some senior clinicians, signing up to the Territorial Army is simply not the right option for them. So, I am delighted to tell you that we are working with the Defence Medical Services and the NHS Trusts such as University College London Hospitals, to pro-mote Sponsored Reserves across these “pinch-point” disciplines. This means that there will be opportunities for clinicians and nurses with much-needed specialist skills to undertake short assignments in confl ict zones, in support of our armed forces and allies on operations. I am confi dent that the Sponsored Medical Reserve will bring great benefi ts to all individu-als and organisations involved. I believe that all Trusts can benefi t from encouraging their employees to be reservists or sponsored reservists.
The skills that NHS reservists learn on their operational tours are abso-lutely invaluable. I think the Major Andy Bruce put it better than I ever could when he said that after working in Afghanistan: “I will never again be intimidated by anything else that will come through the doors of an NHS hospital.” Over the last hundred years, the Territorial Army has given thousands of men and women the experience of a lifetime. For many, being a reservist has proved a unique opportunity to develop new skills and responsibili-ties, testing themselves beyond the normal boundaries of their day job. I would like to pay tribute to all NHS reservists who give up so much of their time and energy to support our servicemen and women. Their dedication and commitment is being felt by troops and civilians all over the world. And the NHS continues to benefi t from their experience.
“The Territorial Army Medical Services are increasingly attracting the fi nest talent in the NHS”
ARMY MEDIC Magazine 23
Contact us:0800 389 5459
www.sabre.mod.uk

Fightingspirit3 Para’s war-woundedwinning battle for fi tness
Report: Stephen TylerPicture: Graeme Main
HEN soldiers from the 3rd Battalion, The Parachute Regiment arrived in Helmand last year they could never have envisaged the ferocity of fi ghting they were to encounter.Constant contacts with Taliban fi ghtersacross the province took a deadly toll on the proud regiment, which lost three men during the intense tour. As if the fi re-fi ghts were not enough, the Paras also faced the indirect but very real threat posed by landmines and several more soldiers were forced out of theatre after being caught up in explosions. The injuries were horrifi c. Young men at the peak of their physical prowess were left facing up to life with missing limbs or restricted mobility. But the much-lauded airborne spirit is alive and well among the injured soldiers who are now fi ghting fi t in new roles thanks to their own incredible determination and the help of their regiment. Commanding offi cer Lt Col Stuart Tootal has been at the heart of the drive
to ensure the Op Herrick veterans are given every chance to rejoin their mates, but he admits the successful rehabilitation is entirely reliant on the soldiers’ own determination and resolve.“We have been continually struck by the fortitude, the determination and the para-trooper spirit that these guys have shown,” Lt Col Tootal told Soldier. “The fact that they want to go back into the battalion is admirable and we have never failed to be impressed or humbled by their attitude. It’s very important that the nation looks after its war wounded and that has been well recognised by the chain of command as something that needs to attract resources. “We are asking our soldiers to go intoharm’s way and they deserve to be properly looked after if they pay a personal cost for that dedication and service.” Former sniper Cpl Stuart Hale is a casein point. The 25-year-old stepped on alandmine in Kajaki on September 6 last year as he tried to get within range of a Taliban vehicle checkpoint. The incident led to the death of Cpl Mark Wright and caused severe injuries to three
other men, including Cpl Hale who lost his right leg in the blast and was extracted from theatre to Selly Oak hospital in Birmingham. Despite the physical and mental strainof his ordeal, Cpl Hale admits that he never gave leaving the Army more than a passing thought and he hopes to play a part in future 3 Para deployments as a sniper trainer. “I’m working in the intelligence cell now and it’s the best way I can contribute to the war effort,” he said. “I’m really keen to deploy again because I know that if I didn’t go I would just be sat in front of Sky Newsand Al Jazeera all day. “Being a paratrooper gives you a lot ofrespect for your regiment and we think very highly of ourselves. That’s what gives ussuch pride in everything we do and that hasbeen a big factor in pulling me through.”The steely determination to remain anintegral part of 3 Para’s strength is alsoevident in Sgt Stuart Pearson. The 32-year-old lost his left leg after stepping on alandmine as he cleared a helicopter landingsite for the casevac of Cpl Hale. As with his colleague, Sgt Pearson
W
24 ARMY MEDIC Magazine

Returning to duty: Soldiersfrom 3 Para who sufferedserious injuries on Op Herrickhave been rehabilitatedand given new roles in theregiment. Cpl Stuart Hale, left,and Sgt Stuart Pearson, right,who both lost legs in landmineexplosions, say the regiment’shelp has allowed them tocontinue their Army careers inspite of their injuries.You can be miserableand blame the worldor you can crack on
Article Reproduced with permission: Soldier Magazine Dec 2007
remained focused on continuing his Armycareer and, thanks to the support of Lt ColTootal, he is now working in the PRI shop atHyderabad Barracks in Colchester. “I have not got a bad word to say about the way I was treated,” said Sgt Pearson, who completed a tandem parachute jump with the Red Devils in July. “I never gave giving the Army up a thought for more than five minutes. I have eight years left of my 22 and I intend seeing them out.” Another of 3 Para’s injured troops isSgt Paddy Caldwell, who was directing firefrom a rooftop in Sangin when he was shotthrough the neck in August 2006. He awokeweeks later in Selly Oak to find he wasunable to move from the neck down.Although he is currently consigned toa wheelchair, Sgt Caldwell is graduallyregaining his movement and was wellenough to start a new job in the battalionwelfare office at the end of October. Praising his regiment, Sgt Caldwell said that he hopes the exemplary treatment he received will be used as a template to help ease the transition back into working life for
any soldiers injured on future operational tours. “The regiment has been outstanding forany needs that I have got. I have been a bit of a pathfinder,” he said. “As Afghan-istan goes on, there might be people that are worse off than me and I hope that I will have been in the forefront of get-ting things changed. “If I had a chance I would deploy again. Because of the level of my injury I was recommended to be medically discharged, but the CO worked to keep me on, so as long as I want to serve I will be able to continue to do so. ‘‘You can be miserable and blame the world or you can crack on. I’m determined to get back on my feet,” said Sgt Caldwell. Regardless of the level of injury suffered, each of 3 Para’s
war-wounded troops have used equal measures of personal strength and regimental support to get back into the career they love. “The thing that is significant is that these guys have surpassed a lot of people’s expectations,” concluded Lt Col Tootal.
“What the medical staff and clinicians didn’t realise when they gave them their prognosis is that these are paratroopers and they are excelling because of the
mental attitude and approach that they take.”
“You can be miserableand blame the worldor you can crack on”
ARMY MEDIC Magazine 25
MEDICAL
HOW TO WORK IN A LAB AND STILL SEE THE WORLD.
armyjobs.mod.uk
0845 700 1700
Text ARMY to 61110
Find out more
Even the most basic research will reveal that being a Biomedical Scientist in the TA is different.
You’ll retain your NHS job, but you’ll expe-rience Clinical Chemistry, Haematology / Transfusion as well as Microbiology.
You’ll receive the training that enables you to work in field hospitals, outdoors, at home and abroad.
You’ll also get paid and hopefully meet new friends and have some fun. An open-and-shut case, surely?
The Army is committed to Equal Opportunities.

ONE ARMYThe Territorial Army bids farewell to its old yellow and green logo as it becomes integrated with the Regular Army logo, refl ecting the interchangeable nature of the full-time and part-time careers that reservists now experience.
The integration of the Territorial Army into the Regular Army logo refl ects the “One Army” concept that now exists. Increasingly, the TA plays a vital role in support of Operations in theatres such as Iraq and Afghani-stan and reservists are mobilised as either key individuals or as fully formed units. In today’s Army it would be impossible to spot who is the regular soldier or offi cer and who is the reservist. Historically, some reservists might have joined the TA with a primary focus on making new friends and expanding their social lives, others might have been more adven-turous and wanted to ski, sail or sky dive etc. The changing profi le of the Territorial Army and in particular the Medical Services is testament to the seriousness of the role that they now perform. Today nobody joins the TA Medical Services unless they posses the correct clinical skills for the job that they will be asked to do. Increasingly we are attracting some of the most talented NHS clinicians and this is because they realise that mobilisation into an Operational Theatre will present opportunities for their clinical devel-opment that the NHS would be hard pushed to deliver. Our TA clinicians are given the opportunity to work in some of the world’s most challenging and well-resourced clinical environ-ments… Anybody making an application to join the TA must be able to dem-onstrate their commitment to both military training and mobilisation. Although fl exibility is built into the very core of the TA ethos, the Territo-rial Army is a secondary career and we expect individuals to be clini-cally, physically and mentally robust
enough to meet the challenges of that career. Clinicians are expected to attain a level of military training either as an offi cer or a soldier that will prepare them to work in a hostile environ-ment. This is the same common military syllabus that all soldiers undergo. All offi cers will attend the Royal Military Academy Sandhurst and they must attain the same level of leadership ability expected of any offi cer in the British Army. The Territorial Army is proving its worth, day in, day out, on the battle-fronts of Iraq and Afghanistan. Its health professionals are saving the lives of more unexpected survivors than could ever have been anticipat-ed and they have earned their right of passage into this “One Army.”
ARMY MEDIC Magazine 26
“As an organisation we invest less time
trying to motivate our people and spend
more time ensuring that they do
not become demotivated”
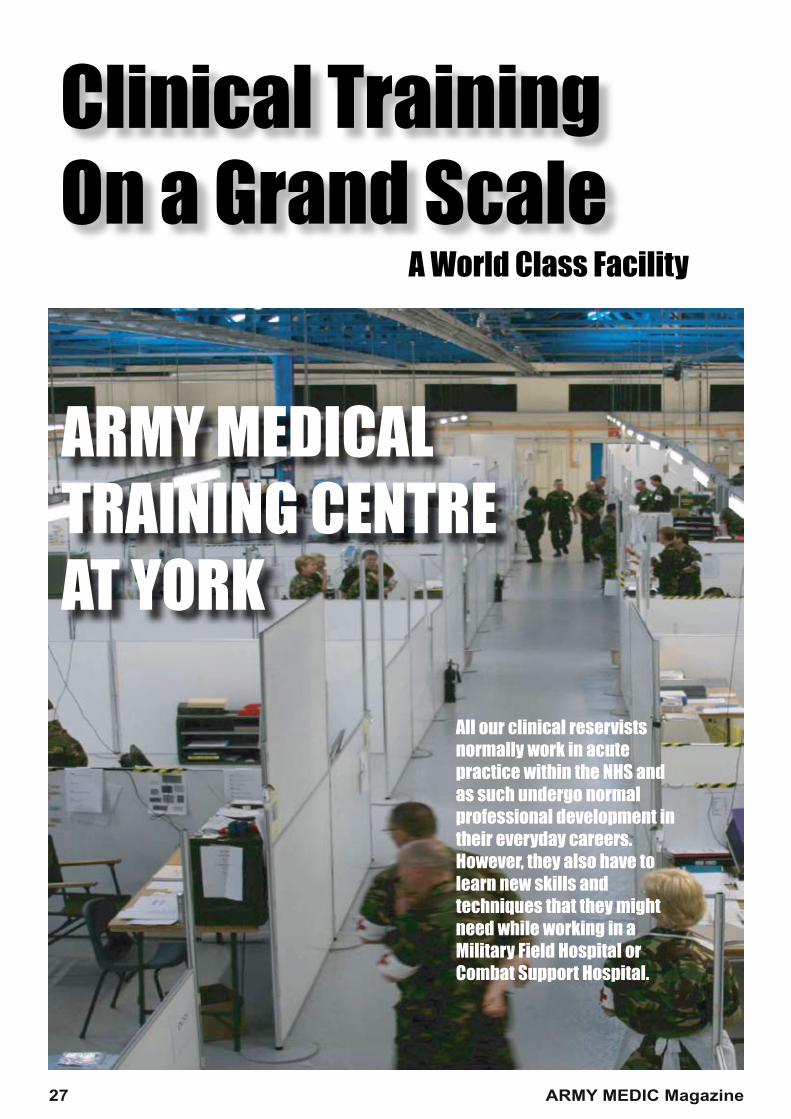
Clinical TrainingOn a Grand Scale
ARMY MEDICAL TRAINING CENTRE AT YORK
27 ARMY MEDIC Magazine
All our clinical reservists normally work in acute practice within the NHS and as such undergo normal professional development in their everyday careers. However, they also have to learn new skills and techniques that they might need while working in a Military Field Hospital or Combat Support Hospital.
A World Class Facility

The Army Medical Services Train-ing Centre (AMSTC) near York is the only facility of its kind, either military or civilian. The site, which covers over two hectares, contains every department including operating theatres, A+E, ITU, X-ray, Labs and Wards etc, and it can be re-config-ured in hours to facilitate any medical training exercise, including Chemical, Biological, Radiological and Nuclear (CBRN) simulations. All personnel who are preparing to mobilise into an Operational envi-ronment such as Iraq or Afghanistan attend the centre and take part in a two-week intensive training pack-age that includes elements such as Battlefield Advanced Trauma Life Support and Major Incident Manage-ment. On average, every TA Medical Unit attends the facility at least twice in a three-year training cycle when they participate in large clinical train-ing exercises that serve to test skills that have been taught during that training period. Realism has to be an essential element of any simulated training package and so the casualties that we put through the facility are as close to the real thing as possible. To that end, we use trained actors and amputees who are actors, who have been dressed and made up by professional casualty simulation (make-up) artists who normally work in the film industry. Each department has an ob-server/assessor that evaluates both the reality of the training and the response of clinicians to the various simulations that they are presented with. The models used in each simulation are extracted from real life situations or, indeed, the facility can be used to test situations that have not previously happened but that we anticipate might happen. Patient through-put can be increased or reduced depending upon the exer-cise aims and the exercise can be paused at any stage to allow trainers to intervene or to facilitate discus-sion. Individually we might have some of the best health professionals in the country, but this facility is all about getting people to work together as a team. In the words of the American baseball star Babe Ruth: “ The way a team plays as a whole determines its success. You may have the greatest bunch of individual stars in the world,
but if they don’t play together, the club won’t be worth a dime.”
When we get the atmosphere and tempo of an exercise right, the ten-sion and pressure can be as near to the real thing as anybody could expect. Under these conditions the benefits are as much about what we learn from our mistakes and about building or strengthening professional relationships than it is about provid-ing reassurance that our systems and training are working well. With 11 Reservist Field Hospitals, three Regular Army Field Hospitals and various pre-hospital care units to serve, the facility is busy all year. The training centre also contains classrooms where small workshops can take place and there is a large state-of the-art lecture theatre that can accommodate up to 200 stu-dents. Significant investment has been made in kit and equipment, the latest of which are several Laerdal SIM-MAN, which are fully computer integrated casualty simulation dolls. The latest addition to the training centre is a purpose built helicopter simulator. One of the key factors in successful trauma outcomes involves what happens in the pre-hospital environment. Almost exclusively, patients are extracted from the battlefield or point of wounding by Chinook helicopter.
On board is the Medical Emergency Response Team (MERT). Few civil-ian pre-hospital environments can prepare a clinician for working in these conditions. The noise of the engines and the level of vibration in-side of the cabin makes verbal com-munication difficult, at best. Often these teams are working in low light conditions and more often than not the helicopter is flying tactically and that doesn’t necessarily lend itself to a smooth flight. This new simulator is able to generate many of the condi-tions that the MERT will experience when they deploy for real. While significant investment has been made in both equipment and facilities, the Training Centre staff never forget that the best tool is the one that we all have between our ears and the biggest investment of all is made in developing the abilities of clinicians to, first and foremost, adapt, improvise and achieve with the use of their brains.
A simulated burns casualty played by a professional actor
ARMY MEDIC Magazine 28
YOUR SOLDIERS ARE PROUD TO BE SERVING BRITAIN - ARE YOU PROUD OF THEM?Leave your messages for the serving men and women of the British Army and let them know that you are thinking about them.
tothebest.army.mod.uk
UBLICITY surrounding the conscientious work of the med-ical teams and hospitals which care for soldiers wounded on Operations is fi nally being given oxygen, writes Karen
Thomas. Combat medics use the “golden hour” to save a bomb blast victim and fi eld hospitals perform emergency surgery. Selly Oak Hospital stabilises the patient and Headley Court gets them back on their feet. The 3rd Battalion, The Parachute Regiment, is leading the way in ensuring the permanently wounded continue in a fulfi lling and active Army career (see December issue), and the scars of public stigmatism are gradually fading. Yet one group of healthcare professionals, who play an enormous role in keeping the Army fi ghting fi t, have been largely overlooked. The primary healthcare (PHC) team, including GPs and physiotherapists, might lack the drama of combat medics braving enemy fi re but represent a vital link in the chain of care. Pte Craig Gordon, 1 R Anglian, deployed to Helmand in Afghanistan on Op Herrick 6. He was wounded in the stomach and shoulder while fi ghting on the front line but, with the help of his mates, he limped onto the Chinook that casevaced him to Camp Bastion. “The pain relief and healthcare over there was brilliant,” Pte Gordon told Soldier during his rehabilitation at the Pirbright PHC centre after being discharged from Selly Oak Hospital. “Here, I’ve had physiotherapy, had my staples removed and an infection has healed. The physiotherapist ensures I have free movement in my side and shoulder by rubbing tight and tense scar tissue. I’m told everything they’re going to do and if I’ve not understood, they are more than happy to help me understand.” The Army Primary Healthcare Service (APHCS) has to ensure soldiers are fi ghting fi t for operations – “fi tter faster” – by preventing injury and illness. But it is also crucial in the fi nal recovery stages of trauma and injuries incurred in theatre. The service has an active role in catching soldiers discharged from hospital and completing their rehabilitation back to full health. After extensive restructuring, the service is now more patient-focused with concentrated efforts in staff development to provide technically and professionally excellent facilities. Brig Timothy Finnegan, RAMC, confi rmed that soldiers would be treated from a holistic perspective, in the same way that the NHS approaches patient care. “We put ourselves in the patient’s shoes from when we make a diagnosis to completing therapy – the whole business of treating you as a person,” he told Soldier, add-ing that the voice of grass-roots soldiers and what is happeningto them in the unit was of paramount importance. “The physical fi tness of young men affects theircareer but the PHC team is now much more tuned tothe balance between work and health.” ■
P
First for healthUnsung medical heroes quietly get soldiers back on their fighting feet
APHCS delivers:• General practice services• Public health • Occupational health• Prescribing and dispensing• Rehabilitation• Community mental health
Article Reproduced with permission: Soldier Magazine Jan 2008
ARMY MEDIC Magazine 29

Report: Mervyn Wynne JonesPictures: Stuart Bingham
ECOVERING in the S4 trauma and orthopaedic ward at Selly OakHospital, Birmingham, LSgt AdaBall of the 1st Battalion, Grenadier
Guards is a focused and resilient man. Eight weeks earlier, he had lost a leg in combat with the Taliban in Afghanistan. Praising the clinical and welfare support he had received – and delaying a lunchtime excursion with two of the hospital’s military liaison officers so he could speak to me – the 22-year-old NCO was upbeat . . . and mobile again. “Just stay positive and let them get on with their job because, believe me, it really does work. I cannot fault it. They’ve got your best interests at heart and you know you’re in good hands. The military nurses have a real sense of what you’ve been through, obvious-ly, and the NHS nurses are excellent too.” The admiration is mutual. Just going to a pub so soon after a grievous injury reflects the remarkable fitness and mental attitude of troops returning injured from Iraq and Afghanistan. Heartening, too, are the many tales heard in Selly Oak of public support for those hurt on Ops. WO2 Dave Schofield, 2 Yorks, a military liaison officer at the Royal Centre for Defence Medicine (RCDM) on the Selly Oak Hospital site, recalled taking a group of injured sol-diers from the ward to a nearby pub and of a fellow customer stepping in to settle the bill. “Things like that, by no means a one-off, make you realise there are lots of people who really do care about the welfare of these guys,” he said. An elderly patient on the same ward,an old soldier, told his family he wanteddonations at his funeral to be given to the
hospital’s military welfare fund. In duecourse they were gratefully received. The RCDM, created in 2001, provides medical support to Service personnel de-ployed on Ops. It does so by training military medical personnel, by researching the best possible methods of treating the wounded in the field and back at home and by providing a clinical division and staff for a ward managed by the military at Selly Oak Hospital. Gen Sir Richard Dannatt, the Chief ofthe General Staff, told the BBC: “There is no-where better in the country, nowhere more ex-pert at polytrauma medicine, than the hospital at Selly Oak.” Ward S4 has 39 military nurses who, with matron-led NHS counterparts,deliver round-the-clock care to noncombat and operational military casualties. Kept in close proximity whenever possible, injured soldiers have access to a complete range
of surgical specialisms at five Birmingham hospitals. Maj Christine Birkby, senior militarynurse, said: “We try as best we can, de-pending on clinical need, to cohort patients together on the ward. Overall, it is working well and everyone is integrating.” She admit-ted it could be distressing to see badly injured soldiers arriving at the hospital, but there was a real buzz when they visited during their rehabilitation phase and told staff “it’s all down to you”. “The downside can be reading the often ill-informed stuff that the press recycle about this place. There’s no doubt that it affects us all morale-wise. Nowhere’s perfect, but the quality of care here is second-to-none.” NHS matron Marie Hale agreed. “It’ssoul-destroying,” she said. “I don’t buy newspapers any more. We’ve learned a lot to-gether, both civilian and military. There’s no doubt there were difficulties and challenges at first and perhaps a clash of cultures, but it’s about looking forward now. What would I say to a soldier wondering whether he might be here one day? I would reassure him that we fully understand his journey, that the entire clinical team understands the extraordinary circumstances of his point of injury, that we deliver the highest quality care, and that he is at the very centre of everything we do.” Maj Andy Main RLC, who is in chargeof the military liaison officers, said: “Thelows are when you see our lads come in, but the highs are when you see them recover. It’s unbelievable, and it can get quite emotional. In more than two decades in the Army, this is far and away the best job I’ve had.” LSgt Ball, whose regiment keeps inregular touch while he recovers from his injury, said: “It’s a big shock to the system. One minute you’re war-fighting, and the next you’re a casualty. I’m a positive man though and, despite the bad days and a few night-mares, I look ahead. I’ve seen a mate with a similar injury and I see how well he’s getting on with life; it gives me confidence for the future.”
R Hospitalheroes
F I T F O R
B a d l y w o u n d e d g u a r d s m a n s a y s c a s u a l t i e s c a n h a v e f a i t h i n S e l l y O a k ’ s s u p e r b s t a f f
30 ARMY MEDIC Magazine

RCDM Commandant-designate Col Chris Parker said: “Day after day you see hospital trust staff going out of their way to ensure the best possible care for our Service patients but also helping us to create a military environment around these patients in which both they and their families can feel as comfortable as possible. It is a very positive partnership and one that I am confi dent will develop and endure over the decades to come. ‘‘There have been some problems; not to acknowl-edge that would be a disservice to some patients and families who have felt their experience here to have been less than satisfactory. However, we have learned from those experiences and many of our patients are now our best advocates. I feel that a corner has been turned but we cannot and will not take our eye off the ball. ‘‘We are also on the cusp of seeing Birmingham realise its ambition – of which we will be part – of opening a brand-new, state-of-the-art hospital, one of the biggest and most modern in Europe.”
Patients now ourbest advocates
Right: Road to recovery - LSgt Adam Ball, who lost a leg in combat with the Taliban, now recovering at Selly OakLeft: Top team - RCDM Commandant designate Col Chris Parker, NHS Matron Marie Hale and senior military nurse Maj Christine Birkby
ARMY MEDIC Magazine 31
Article Reproduced with permission: Soldier Magazine Jan 2008
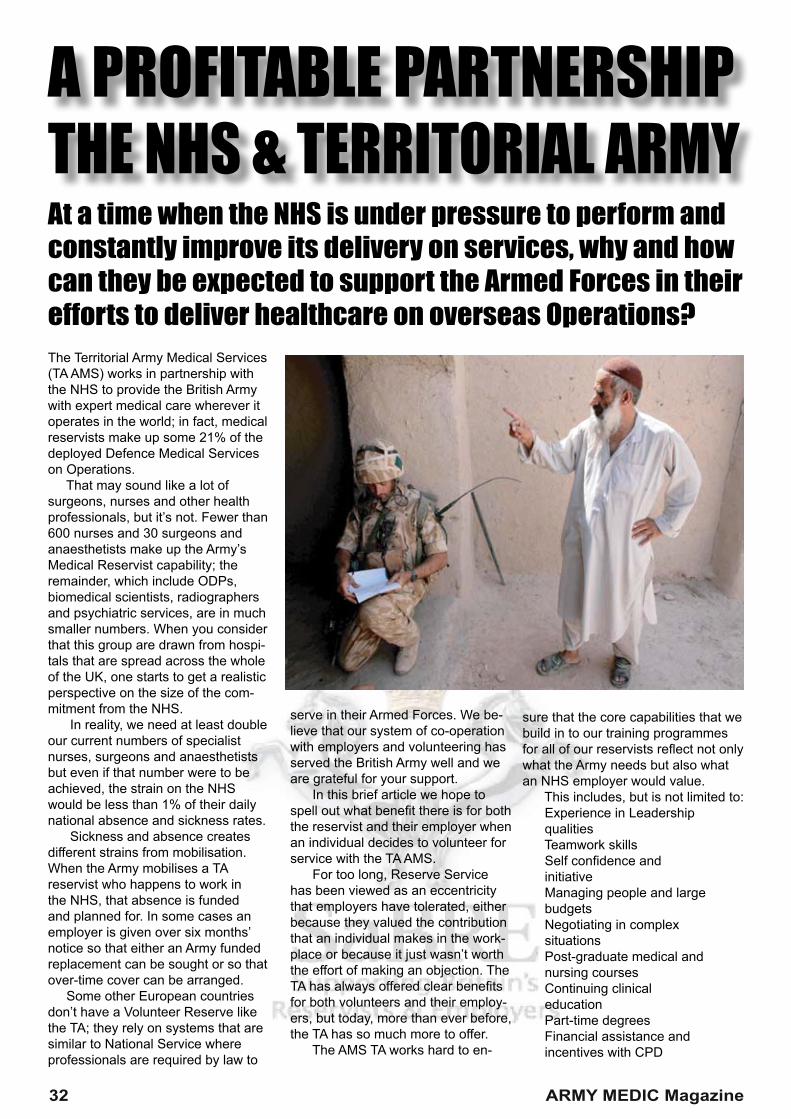
The Territorial Army Medical Services (TA AMS) works in partnership with the NHS to provide the British Army with expert medical care wherever it operates in the world; in fact, medical reservists make up some 21% of the deployed Defence Medical Services on Operations. That may sound like a lot of surgeons, nurses and other health professionals, but it’s not. Fewer than 600 nurses and 30 surgeons and anaesthetists make up the Army’s Medical Reservist capability; the remainder, which include ODPs, biomedical scientists, radiographers and psychiatric services, are in much smaller numbers. When you consider that this group are drawn from hospi-tals that are spread across the whole of the UK, one starts to get a realistic perspective on the size of the com-mitment from the NHS. In reality, we need at least double our current numbers of specialist nurses, surgeons and anaesthetists but even if that number were to be achieved, the strain on the NHS would be less than 1% of their daily national absence and sickness rates. Sickness and absence creates different strains from mobilisation. When the Army mobilises a TA reservist who happens to work in the NHS, that absence is funded and planned for. In some cases an employer is given over six months’ notice so that either an Army funded replacement can be sought or so that over-time cover can be arranged. Some other European countries don’t have a Volunteer Reserve like the TA; they rely on systems that are similar to National Service where professionals are required by law to
serve in their Armed Forces. We be-lieve that our system of co-operation with employers and volunteering has served the British Army well and we are grateful for your support. In this brief article we hope to spell out what benefi t there is for both the reservist and their employer when an individual decides to volunteer for service with the TA AMS. For too long, Reserve Service has been viewed as an eccentricity that employers have tolerated, either because they valued the contribution that an individual makes in the work-place or because it just wasn’t worth the effort of making an objection. The TA has always offered clear benefi ts for both volunteers and their employ-ers, but today, more than ever before, the TA has so much more to offer. The AMS TA works hard to en-
sure that the core capabilities that we build in to our training programmes for all of our reservists refl ect not only what the Army needs but also what an NHS employer would value. This includes, but is not limited to: Experience in Leadership qualities Teamwork skills Self confi dence and initiative Managing people and large budgets Negotiating in complex situations Post-graduate medical and nursing courses Continuing clinical education Part-time degrees Financial assistance and incentives with CPD
A PROFITABLE PARTNERSHIPTHE NHS & TERRITORIAL ARMYAt a time when the NHS is under pressure to perform and constantly improve its delivery on services, why and how can they be expected to support the Armed Forces in their efforts to deliver healthcare on overseas Operations?
32 ARMY MEDIC Magazine

As well as invaluable experience of other cultures According to a 2002 report by business academics at Liverpool John Moores, Leeds Metropolitan and Bradford universities, the aver-age reservist receives training in transferable skills which would nor-mally cost an employer over £9,000 per annum. In addition, many of the TA Field Hospital units provide free partner-ship training for the NHS in the form of leadership and personal develop-ment weekends and open access to most clinical seminars and CPD updates for NHS professionals who are not in the TA. Reservists are usually physi-cally fi tter than most of their civilian equivalents and we certainly foster a “can-do attitude” in all of our mem-bers. It is also true that reservists are often given a much higher level of responsibility early on in their military careers than in their civilian employ-ment.
The commitment is completely fl exible. NHS employers provide reservists with up to two weeks’ ad-ditional paid leave and the reservist makes up the remainder of their time, approximately 13 days during se-lected weekends and on occasional Tuesday evenings
What happens when a Reservist is called up for active service?
We call this mobilisation. In the current environment it is likely that in a three-year period professionally qualifi ed health service personnel will be mobilised. This will normally be for three months in location which will mean approximately four-and-a-half months away from the workplace. In special circumstances this can be re-duced to six weeks, 10 weeks away from the workplace in total. The additional time outside of the deployed location is taken up by pre-deployment training and leave following deployment. In the case of healthcare professionals, we try to give a minimum of three months’
notice to employers prior to the mobilisation of a reservist, longer if possible. This enables the hospital to arrange for locum, agency or over-time cover which, including advertis-ing and training costs, the MoD will fully reimburse. While the reservist is mobilised the NHS does not continue to pay them, the reservist will receive enhanced Regular Army pay at their equivalent rank and professional group rates. On very rare occasions a reserv-ist can be mobilised with 28 days’ notice.
The roles and professions might vary but all Reservists are“SOLDIERS & OFFICERS FIRST”
ARMY MEDIC Magazine 33
Contact us:0800 389 5459
www.sabre.mod.uk
RECRUITING NOW...
All applicants must be medically fi t. Generally this means that you should not suffer from any chronic illness such as asthma, epilepsy, diabetes or heart disease, thyroid problems, obesity and mental health problems. If you have been prescribed anti-depressants within the last fi ve years this will also disqualify an applicant. A comprehensive medical will be done by a GP before proceeding with your application. It should be noted that corrected vision with spectacles or lenses doesn’t normally hinder entry. If you are in any doubt you can contact your nearest TA Field Hospital for a confi dential discussion. All applicants should have a good basic level of fi tness: you will be expected to complete a “risk assessment run” of 1.5 miles in under 14 minutes. Remedial fi tness advice and support is available to applicants who fall short of the standard.
Orthopaedic SurgeonsConsultants & training gradesGeneral SurgeonsConsultants & training grades Neuro SurgeonsConsultants & training gradesAnaesthetistsConsultants & training grades Emergency Medicine DoctorsConsultants & training gradesGeneral MedicineConsultants & training grades RadiographersMid to Senior level grades Biomedical ScientistsRegistered and working in the NHS. Haematology, biochemistry and pathology.
Operating Department Practitioners (ODPs)Theatre NursesIntensive Care + HDU NursesA+E Nurses
Orthopaedic, Burns, Opthalmic & General Surgical NursesGeneral Nurses
Healthcare AssistantsMinimum NVQ Level 2 in Health and Social Care who are working in an acute NHS environmentParamedicsCurrent front line ambulance personnel NHS ONLY
Dentists Post VT periodRegistered Dental Nurses
Next Steps...Contact you local Territorial Army Field Hospital
201 (Northern) Field Hospital (V) 0191 239 5351 Newcastle, Newton-Aycliffe, Norton, Carlisle202 (Central) Field Hospital (V) 0121 483 4325Birmingham, Trent, Shrewsbury, Oxford203 (Welsh) Field Hospital (V) 02920 562291 Cardiff, Swansea, Aberystwyth204 (Northern Ireland) Field Hospital (V) 028922 60358Belfast, Ballymena, Newtownards, Armagh205 (Scottish) Field Hospital (V) 0845 603 8761Edinburgh, Glasgow, Dundee, Aberdeen207 (Manchester) Field Hospital (V) 0161 232 4985Manchester, Stockport, Ashton-Under-Lyne, Bury, Blackburn208 (Liverpool) Field Hospital (V) 0151 488 6655 Liverpool, Wirral, Blackpool, Lancaster212 (Yorkshire) Field Hospital (V) 01904 66 8228Sheffi eld, Leeds, Bradford, Nottingham, Lincoln243 (Wessex) Field Hospital (V)Keynsham, Exeter, Plymouth, Portsmouth256 (London) Field Hospital (V) 020 7091 2661Walworth, Kensington, Kingston, Mile End
306 Hospital Support Medical Regiment (V) 335 Medical Evacuation Regiment (V) 0800 731 1201UK Wide
During their fi rst year, new recruits will spend their full commitment in recruit training.The average commitment is 27 days per year. This time is divided up into weekend training which equates to 2.5 days’ pay and usually lasts from Friday evening until Sunday afternoon. You can also attend on a mid-week evening (usually a Tuesday) and these equate to 1/4 of a day’s pay + travel expenses. Tuesday evening training usually occurs between 1930 hrs and 2130 hrs. All reservists must complete a two-week annual camp. Reservists receive up to two weeks’ special leave from NHS Trust. This leave is in addition to normal annual leave entitlement and it is usually paid. The UK Wide Unit 306 Hospital Support Medical regiment (V) and 335 Medical Evacuation Regiment (V) have a 19 day commitment. This comprises a two week annual camp and two week-ends.
The current Operational tempo forecasts that medical reservists should expect to be deployed for at least 4 months in any 3 to 5 year period. (The 4 months includes approx 4 weeks of pre-deploy-ment training and post-tour leave. This relates to approx 3 months in the Operational location).