aremanagement - academyccm.orgacademyccm.org/pdfs/15cm_jun_jul_2013.pdf · interventions needed to...
TRANSCRIPT
CareManagementOfficial JOurnal Of The academy Of cerTified case managers Vol. 19, No. 3 JuNe/July 2013
Departments:
2 From the Editor-in-Chief Care Coordination and Hospital Readmissions
3 Legal Update What’s New? “Patient Engagement”
4 News from CCMC Case Management Facts:
The Role of the Certified Case Manager
6 News from CDMS Advocate for Disabled Hopes Affordable Care Act
Will Change Common Wisdom
29 How to Contact Us
29 ACCM Membership Benefits
30 Membership Application
join/renew ACCM online at academyCCM.org
or use the application on page 30
7 Coordinating Care for Patients Needing Renal Replacement Therapies CEU By Caroline Steward, MSN, RN, APN-C, CCRN, CNN
Learn what you can do to ensure patients who are receiving renal replacement therapies receive the other important interventions needed to prevent cardiovascular and other complications.
12 University of California, San Francisco Medical Center: Reducing Readmissions Through Heart Failure Care Management: Part I CEU
By Douglas McCarthy
This article provides good food for thought as your hospital makes strides to reduce readmissions for disorders like heart failure. Hear how nurses provided the key coordination elements needed for successful readmission reductions at the University of California, San Francisco.
18 CE Exam CEU
special sections:
5 NewsNewsNews Certified Case Manager News
Trends, issues, and updates in health care.
20 PharmaFacts for Case Managers Approvals, warnings and the latest information on clinical trials—timely drug information case managers can use.
24 LitScan for Case ManagersThe latest in medical literature and report abstracts for case managers.
I N S I D E t h I S I S S U E
What you need to know about your CareManagement subscription!
If you haven't signed up your digital copy of CareManagement, click here or go to the website link and choose the tab "Provide/Update Your Email Address" to add your e-mail address now. You'll receive notification by e-mail when the next issue is available.
Continue taking CE tests online or by mail using your ACCM membership ID.

2 CareManagement June/July 2013
Editor-in-ChiefGary S. Wolfe, rn, ccm
Editorial BoardBarbara Aubry, rn, cpc,
chcqm, faihcqToni G. Cesta, rn, phd, faan
Patrick Conlon, rn-bc, msn, cfnp, cde, ccm, bc-adm, pnp, faanp, fnap
Beverly Cunningham, rn, ms, fnapBarbara (Bobbi) Kolonay, rn,
bsn, ms, ccmFrank D. Lewis, phd, cbist
Sharon Silow-Carroll, msw, mbaDeborah Smith, rnc, mn
Annette Watson, rn-bc, ccm, mbaAdele Webb, rn, phd, aacrn, cpnap,
faan
Executive Editor Jennifer Maybin, ma, els
Certified Case Manager News EditorJennifer Maybin, ma, els
Art Director Laura D. Campbell
Production Director Sue Moul
Circulation Manager Robin Lane Ventura
Member Services CoordinatorKathy Lynch
Senior VP Finance & Administration Jacqueline Abel
Publisher, President Howard Mason, rph, ms
Vol. 19, No. 3, June/July 2013. CareManagement (ISSN #1531-037X) is published electronically six times a year, February, April, June, August, October, and December, and its contents are copyrighted by Mason Medical Communi ca tions Inc., 1 0 Covlee Dr., Westport, CT 06880; Tel: 203-454-1333; Fax: 203-227-9495.
Subscription rates: $120 per year for ACCM members; $150 for institutions.
Opinions expressed in articles are those of the authors and do not necessarily reflect the opinions of the editors or the publisher or the Academy of Certified Case Managers. One or two copies of articles for personal or internal use may be made at no charge. For copying beyond that number, contact Copyright Clearance Center, Inc. 222 Rosewood Dr., Danvers, MA 01923, Tel: 978-750-8400.
CareManagement is indexed in the CINAHL® Database and Cumulative Index to Nursing & Allied Health Literature™ Print Index and in RNdex.™
CareManagementOfficial JOurnal Of The academy Of cerTified case managers
fRoM thE EDItoR-IN-ChIEf
Gary S. Wolfe
Section 3025 of the Affordable Care Act established the Hospital Readmissions Reduction Program,
which requires the Centers for Medicare & Medicaid Services (CMS) to reduce payments to hospitals with excess readmissions, effective for discharges beginning on October 1, 2012. The regulations that implement this provision are in subpart I of 42 CFR part 412 (§412.150 through §412.154).
Readmission MeasuresIn the FY 2012 final rule, CMS finalized the following policies with regard to the readmission measures under the Hospital Readmissions Reduction Program:• Defined readmission as an admission to
a subsection(d) hospital within 30 days of a discharge from the same or another subsection(d) hospital
• Adopted readmission measures for the applicable conditions of acute myocardial infarction (AMI), heart failure (HF), and pneumonia (PN)
• Established a methodology to calculate the excess readmission ratio for each applicable condition, which is used, in part, to calculate the readmission payment adjustment. A hospital’s excess readmission ratio for AMI, HF, and PN is a measure of a hospital’s readmission performance compared to the national average for the hospital’s set of patients with that applicable condition
• Established a policy of using the risk adjustment methodology endorsed by the National Quality Forum (NQF) for the readmissions measures for AMI, HF, and PN to calculate the excess readmission ratios, which includes adjustment for factors that are clinically relevant including patient demographic characteristics, comorbidities, and patient frailty
• Established an applicable period of 3 years of discharge data and the use of a minimum of 25 cases to calculate a hospital’s excess readmission ratio for each applicable condition — For FY 2013, the excess readmission
ratios are based on discharges occurring during the 3-year period of July 1, 2008 to June 30, 2011
— For FY 2014, the proposed excess readmission ratios will be based on discharges occurring during the 3-year period of July 1, 2009 to June 30, 2012. However, the excess readmission ratios used for the purposes of modeling the proposed FY 2014 proxy readmission payment adjustment factors are based on the FY 2013 applicable period of July 1, 2008 to June 30, 2011
Despite valid financial concerns, hospital executives are expressing a growing desire to avoid readmissions for the sake of good patient care—because it’s the right thing to do.
As Medicare turns up the heat on hospitals by imposing financial penalties for readmissions it considers preventable, provider organizations are caught in a catch-22.
By avoiding readmissions and the corresponding Medicare payment consequences, hospitals also drive down their patient volume, and, therefore, their revenue, which is still mainly based on a fee-for-service reimbursement model. Although health care is undoubtedly moving toward a value-based payment structure, it hasn’t gotten there yet.
Despite this valid financial concern around preventing readmissions, hospital executives often express a growing desire within their organizations to avoid read-missions for the sake of good patient care.
Care Coordination and Hospital Readmissions
continues on page 28

June/July 2013 CareManagement 3
What’s New? “Patient Engagement”
Elizabeth E. hogue, Esq.
t here’s a new buzzword for health care providers: “patient engagement.” The application of
this concept to relationships between patients and providers, including dis-charge planners, is becoming more prevalent. In the commentary to final regulations governing the establish-ment of accountable care organiza-tions (ACOs), for example, the Centers for Medicare & Medicaid Services (CMS) responded to comments about the inability to control patients’ behaviors so that monies are saved, including for the benefit of participants in ACOs. CMS responded to these comments by emphasiz-ing that it is the responsibility of provid-ers to “engage patients” so that patients follow their recommendations.
In 2011, the Center for Advancing Health (CFAH) published an “Engagement Behavior Framework.” Below are some of CFAH’s recommen-dations for patients that require involve-ment by providers:• “Ask questions when explanations or
next steps are not clear and express any concerns about recommendations or care experiences
• Ensure that relevant medical informa-tion is conveyed between providers and institutions
• Negotiate a treatment plan with provider(s)
• Learn about any newly prescribed medications and devices, including possible side effects or interactions with existing medications and devices
• Monitor symptoms and conditions (eg, for diabetes—monitor glucose regularly, check feet; for depression—
prescribe medical medication and/or counseling and monitor symptoms; for hypertension—measure blood pressure regularly, maintain blood pressure diary), including danger signs that require urgent attention
• Set and act on priorities for changing behavior to optimize health and pre-vent disease
• Identify and secure services that sup-port changing behavior to maximize health and functioning and maintain those changes over time
• Manage symptoms by following treat-ment plans, including diet, exercise and substance use agreed upon by them and their provider
• If diagnosed with a chronic disease, understand the condition(s), the risks and benefits of treatment options and
personal behavior change(s) by seek-ing opportunities to improve health/disease knowledge”
This concept of “patient engage-ment” is not only increasingly important to payors, but also is significant from the perspective of risk management. When patients are nonadherent or not engaged, it is difficult to separate non-
adherence from poor quality of care. Providers must take steps to get patients engaged and to document that they have done so. It is not enough for providers to simply throw up their hands and bemoan the fact that patients will not do what they recommend. It is the job of professionals to uti-
lize their expertise to engage patients in a way that will likely support adher-ence and compliance.
Providers have a history of concerns about noncompliance or nonadherence by patients. The tendency has been for providers to complain that patients are noncompliant. It is clear that a different “wind” is starting to blow now. Providers must prepare to take on more responsibility for patient engagement, including involvement in all of the activities described above and more. CM
this concept of “patient engagement” is not only increasingly important to
payors, but also is significant from the perspective of risk management.
©2013 Elizabeth E. Hogue, Esq. All rights reserved. Reprinted with permission.
lEgAl UPDAtE
See the CFAH Engagment Behavior Framework and Resources for Consumers at: www.cfah.org/engagement/research/engagement-behavior-framework.

Case Management facts: The Role of the Certified Case Manager By Patrice V. Sminkey, RN, CEO, Commission for Case Manager Certification (CCMC)
the commission for case manager certification
NEwS fRoM
t he future for board-certified case managers is looking particularly bright. With the implementation of the Patient
Protection and Affordable Care Act (commonly known as “health care reform” or ACA), new models of care continue to emerge that emphasize the critical function of care coordina-tion to improve quality and efficiency. Professional case managers, particu-larly those who are board-certified, are uniquely qualified with the proven capabilities and expertise to fulfill the care coordination role.
Increasingly, employers recognize the value of board certification and its validation of case management knowl-edge, skills, and abilities. These factors combine to make a persuasive case for the board-certified case manager to advance the aims of the National Quality Strategy—for better care, better health, and lower costs.
The Commission for Case Manager Certification (CCMC), the first and larg-est nationally accredited organization that certifies case managers, continues to survey the community of professional case managers regarding the practice of case management. Here’s what we’re from board-certified case managers about the most important roles of a case manager:• Assure patients receive the care they
need, when and where they need it• Empower patients to make informed
decisions• Coordinate among multiple providers.• Help clients navigate the patient care
system
• Help clients improve the quality of life
• Help clients understand disease impact
Clearly, case managers play an important role in delivering patient-centered care. Through patient engage-ment and patient empowerment, case managers support the individual’s decision-making process. For the case manager, this means providing the client and support system with informa-tion and education about all available treatment options and the possible impact on the person’s health or medi-cal status—not only in light of a par-ticular treatment episode, but also with the perspective of the entire patient lifecycle.
Studies show that case manage-ment represents a valuable, effective care delivery tool, reducing barriers to appropriate, high quality care—especially for the most vulnerable populations—and empowering patients to become more involved in their own care. Those who are not actively involved are three times as likely to have unmet medical needs. As more emphasis is placed on outcomes (includ-ing clinical, financial, and patient satis-faction), the importance of professional case management is elevated.
Across the care continuum, pro-fessional case managers are uniquely well-suited to act as advocates as they coordinate care, design and monitor care plans, improve communication, evaluate patient progress, and track outcomes. The ability to pursue these aims in a complex health care delivery
system is the unique contribution of the board-certified case manager, who sees beyond a single episode of care, and considers how case management services delivered in one setting (e.g., acute care) can achieve desired out-comes—clinical and financial—beyond that episode.
These are some of the “facts” about case management. (To learn and share more, see the CCMC’s “CMCoordinates.”)
As board-certified case managers “tell the story” of their expertise, with supervisors, in community settings, and education sessions with other profes-sionals—as well as with those who might be interested in pursuing case management as a career—the word is spreading about the benefits of profes-sional case management. CM
Patrice V. Sminkey is the CEO of the Commission for Case Manager Certification (CCMC), the first and largest nationally accred-ited organization that certifies case managers. More than 35,000 case managers have been awarded the Certified Case Manager® (CCM) credential.
About the Commission: The Commission for Case Manager Certification is the first and largest nationally accredited organization that certifies case managers. Board certification demonstrates a level of expertise in the field; it is often considered by employers as a benchmark requirement for case managers seeking leadership roles and career advancement. The Commission is currently taking applications for the upcom-ing certification exam; more information can be found at ccmcertification.org.
4 CareManagement June/July 2013

June/July 2013 CareManagement 5
Certified Case Manager News • Certified Case Manager News
The CosT of CaNCer Care
Outcomes of Consumer-Directed Health Plans
Spinal Injections for Pain Increase Fracture RiskSpinal injections of steroids for relief of back pain increase bone fragility in the vertebrae of older patients. Each succes-sive translaminar lumbar epidural steroid injection increased the risk of vertebral fracture by a factor of 1.21 (95% CI 1.08-1.30, P=0.003) in a study recently published in the Journal of Bone and Joint Surgery. n
According to a recent study reported in Health Affairs, consumer-directed health plans (CDHPs), which are designed to make employees more cost- and health-conscious by exposing them more directly to the costs of their care, reduced physician office visits per enrollee per year and the number of prescriptions filled, but increased the number of emergency department visits.
Also, the likelihood of receiving recom-mended cancer screenings was lower under the CDHP after 1 year and lower than baseline at the study’s conclusion. If CDHPs succeed in getting people to make more cost-sensitive decisions, plan sponsors will have to design plans to incentivize primary care and prevention and educate members about what the plan covers. n
New targeted cancer therapies, includ-ing immunotherapies, are flooding the marketplace, giving oncologists new tools for their treatment armamen-tarium, but at quite a cost. Treatment costs for some recently approved therapies top $100,000 per year, and immunotherapies are expected to be even higher at $110,000 per year in the US. Patients are shouldering a greater portion of the cost, usually with 20% co-pays. Thus, cancer care will have to change, according to the experts. Just think of Memorial Sloan-Kettering’s decision to block use of Sanofi’s Zaltrap,
which launched at a cost of about $10K per month—a move that forced Sanofi to halve the cost of the drug. Insurers are more often prereviewing drug therapies and are less inclined to approve off-label use. Eighty percent of US insurers told PricewaterhouseCoopers that they won’t add new therapies to their formularies without evidence of cost savings and clinical benefits. If doctors don’t have cost-of-cancer-care discussions with patients, it may be up to case managers to have these frank discussions about the relative cost-benefit of cancer treatments. n
Radiation Therapy Alone May Be Enough for Some Breast Cancer PatientsResults of the AMAROS study presented at the recent ASCO meeting indicate that breast cancer patients with a posi-tive but nonpalpable sentinel lymph node may be better off with radiation than with further axillary surgery. Recurrence rates were similar and low with either axillary lymph node dis-section or axillary radiotherapy over 5 years. Overall survival was also similar, but those having surgery had twice the rate of lymphedema. n
Limit Magnesium for Preterm Labor to Protect Fetal BonesThe FDA recently advised clinicians not to give pregnant women magnesium sul-fate to prevent preterm labor for more than 5 to 7 days because it may harm developing fetal bones. A warning is being added to the drug’s labeling, and the teratogenicity category is being changed to Pregnancy category D from A. n
aPa’s DsM-V Now aVailableThe American Psychiatric Association has published the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders. A synopsis of changes from DSM-IV were recently published in a MedPage Today article. n
bariatric surgery beneficial for improving Glycemic ControlPatients with diabetes who were mildly obese and underwent bariatric surgery had greater weight loss and better gly-cemic control than those who received nonsurgical treatment, according to a systematic review published in JAMA. However, the evidence for long-term efficacy and safety remains limited. n continues on page 28

6 CareManagement June/July 2013
NEwS fRoM
certification of Disability management specialists commission
Advocate for Disabled Hopes Affordable Care Act Will Change Common Wisdom
I t’s a confusing world out there—full of myths and misunderstand-ing—particularly when it comes to government-funded health
programs.John Coburn, director of train-
ing at Chicago-based Health and Disability Advocates, hopes that imple-mentation of the Affordable Care Act (ACA)—also called “Obamacare”—will remedy much of that confusion for people with disabilities, especially as it relates to reentering the workforce.
Coburn, whose job includes pushing for policies that help dis-abled people find work, laments the pervasive misunderstanding among impoverished people that getting a job automatically means losing public health benefits. He hopes that the ACA, which allows everyone who wants publicly funded care to fit into one category of eligibility or another, will effectively wipe the slate clean and create a new common under-standing of the system.
“There seems to still always be a message out there that you’re going to lose everything and you’re not going to have health care anymore,” Coburn says. “When health care access and insurance is a given, it’ll be interesting to see how many more people return to work.”
Even now, before the ACA takes full effect, more than enough safety nets exist to allow a disabled person
suffering from, say, multiple sclerosis, to qualify for Social Security disability insurance (SSDI) and keep it for up to 93 months after getting a job. However, eligibility rules are so complex, and many people simply don’t understand what they qualify for.
“I can tell you, in Illinois, there’s no reason why an individual should hold themselves back from trying to find work or going back to work out of fear of losing their health care,” Coburn
says. “We’ve spent a lot of time discuss-ing that with people and trying to get them to understand that they will still be able to move into another category of eligibility if they go back to work.”
Better Access Equals Better RecordsStarting in 2014, the ACA allows any-one with an income less than 138% of the federal poverty level (FPL) to gain access to a new category of Medicaid called, among other things, Adult Medicaid. Access to the program no longer will require proof of disability, which, in theory, will eliminate wait-ing periods for people to qualify for coverage.
Coburn’s hope is that this will
lead to people with disabilities getting more regular care, which means better medical records and easier disability determinations.
“Disability determinations are made on medical evidence,” Coburn says. “If you don’t have health insurance, then you’re not seeing the doctor regularly, or [you don’t] have the doctor’s notes to prove the disability case. So there are folks in our office … who feel like this new avenue of health insurance
is going to make their jobs easier because if people receive regular care because they have health insurance, the doctor’s notes are going to be more thorough and consistent because they have had that access to care.”
All in all, Coburn hopes that people applying for federal benefits such as Medicare, Medicaid, SSDI, or Supplemental Security Income will come to understand that the new system allows for everyone to have the care they need paid for.
“I hope they’ll understand that there is something for everybody,” he says. “Right now we live in a world where you have to fit in a certain cat-egory in order to get health care. The question right now is, “Do you fit into a category?” And sometimes the answer is no, and you have nothing. With ACA, it’s going to change from, “Do you fit into a category?” to “Which category do you fit in?,” which I think changes the entire dynamic.” CM
starting in 2014, the aca allows anyone with an income less than 138% of the federal poverty level (fpl) to gain
access to a new category of medicaid called, among other things, adult medicaid. access to the program
no longer will require proof of disability….

o ne of the primary goals of case management is coordination of care. Navigating patients through
the various care providers is one of the keys toward improving outcomes and minimizing costs.1 This article will review evidence-based guidelines used in the management of patients requiring renal replacement therapies (RRT) that have been shown to reduce the mortality and morbidity linked to longer and more frequent hospitalizations.
As of 2010, there were 594,374 patients receiving chronic RRT in the United States. Renal disease has many causes, and treatment of the underlying disease process will need to continue, thereby complicating the management and increasing mortality. In 2011, there were 116,395 new patients started on chronic dialysis. Of these, 63% have dia-betes (38.5%) or hypertension (25.2%) listed as their cause for renal failure.2
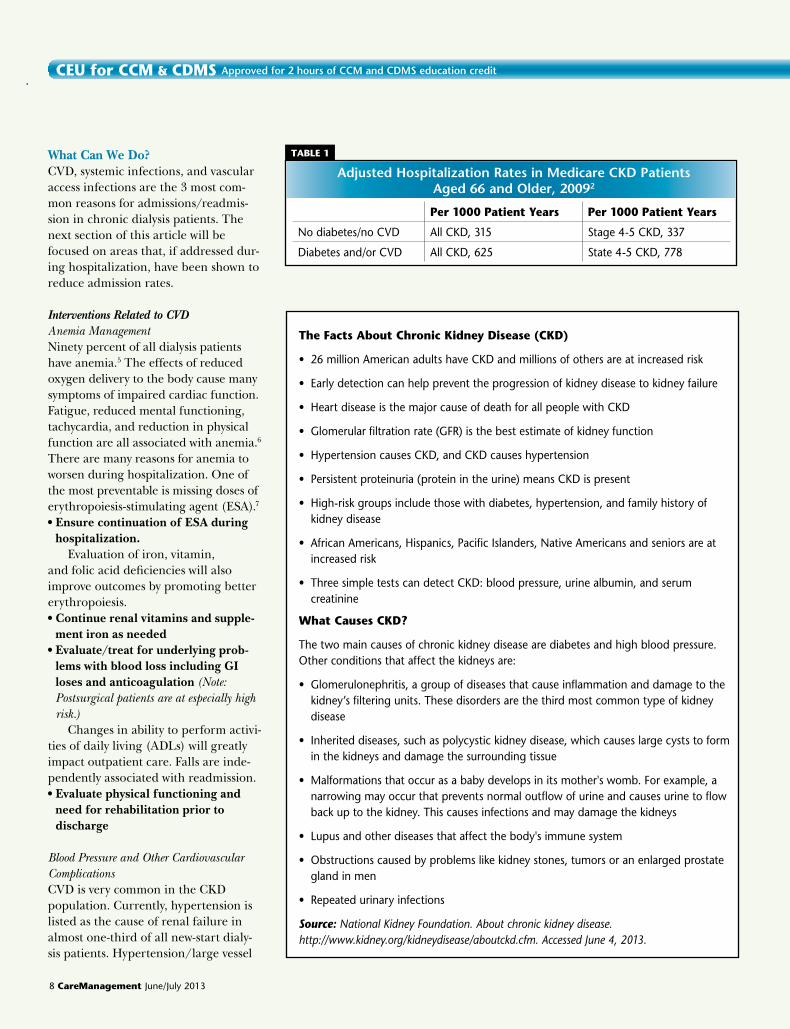
HospitalizationAdjusted hospitalization rates for Medicare patients aged 66 and older show that per 1000 patient years, those with chronic kidney disease (CKD; stage 1 through 5; Box 1) with diabetes and/or cardiovascular disease (CVD) have roughly twice the risk of hospital-ization rate as those without diabetes
and/or CVD (Table 1).2 On average, all patients receiving
RRT will spend 11.8 days/year hospital-ized. Hemodialysis patients spend the most at 11.9, followed by peritoneal patients at 11.8 and transplant recipi-ents at 5.7 days/year.2
Over the years, reasons for hospital admissions have remained unchanged among those receiving RRT. Rates for all cause and CVD-related admissions are highest, general infections second highest, and vascular access–related
infections third. Those at highest risk for hospitalization appear to be older, female, African American, or have diabetes as the cause of renal failure. Vascular access–related admissions are highest in the youngest patients.2
RehospitalizationThe rehospitalization rate for dialy-sis patients is 33% (highest among patients aged 20 to 44 years), equal-ing 1.5% of total hospital admissions. Rehospitalization rates at 14 days are at 24%, but rise to 38% by 30 days,2 indicating that most readmissions occur later.4
The number of rehospitalizations per year is higher in the first 3 months after the initiation of dialysis. Factors associated with this increased risk for rehospitalization within the first 3 months include non-HMO insurance, ischemic heart disease, late referral to a nephrologist, and use of a temporary dialysis catheter for the first dialysis.
Patients on dialysis have a multitude of clinical problems that require con-tinual monitoring that is often either given low priority or overlooked during hospitalization. These include anemia, mineral bone disorders, malnutrition, inflammation/infection, and fluid vol-ume status. All of these impact not only quality of life, but also overall mortality and morbidity and require aggressive efforts to restabilize in the outpatient dialysis setting.5 All of these, if not care-fully addressed, can result in hospital admission and readmission.
June/July 2013 CareManagement 7
CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit Exclusively for ACCM Members
Coordinating Care for Patients Needing Renal Replacement TherapiesBy Caroline Steward, MSN, RN, APN-C, CCRN, CNN
Caroline Steward, MSN, RN, APN-C, CCRN, CNN, is an advanced nurse practitioner from Ewing, NJ, who works in a private practice with renal patients. t
Box 1
Stage 1: Signs of mild kidney disease but with normal or better GFR (greater than 90% kidney function)
Stage 2: Signs of mild kidney disease with reduced GFR (indicating 60% to 89% kidney function)
Stage 3: Signs of moderate chronic renal insufficiency (where the GFR indi-cates 40% to 59% kidney function)
Stage 4: Signs of severe chronic renal insufficiency (where the GFR indicates 15% to 29% kidney function)
Stage 5: Signs of end stage renal failure (where the GFR indicates less than 15% kidney function)
GFR = glomerular filtration rate, the rate at which the kidneys filter waste; relates to a patient’s “kidney function.”
stages of chronic Kidney Disease (cKD)3
8 CareManagement June/July 2013
CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit
What Can We Do?CVD, systemic infections, and vascular access infections are the 3 most com-mon reasons for admissions/readmis-sion in chronic dialysis patients. The next section of this article will be focused on areas that, if addressed dur-ing hospitalization, have been shown to reduce admission rates.
Interventions Related to CVD Anemia ManagementNinety percent of all dialysis patients have anemia.5 The effects of reduced oxygen delivery to the body cause many symptoms of impaired cardiac function. Fatigue, reduced mental functioning, tachycardia, and reduction in physical function are all associated with anemia.6 There are many reasons for anemia to worsen during hospitalization. One of the most preventable is missing doses of erythropoiesis-stimulating agent (ESA).7
• Ensure continuation of ESA during hospitalization.
Evaluation of iron, vitamin, and folic acid deficiencies will also improve outcomes by promoting better erythropoiesis. • Continue renal vitamins and supple-
ment iron as needed• Evaluate/treat for underlying prob-
lems with blood loss including GI loses and anticoagulation (Note: Postsurgical patients are at especially high risk.)
Changes in ability to perform activi-ties of daily living (ADLs) will greatly impact outpatient care. Falls are inde-pendently associated with readmission. • Evaluate physical functioning and
need for rehabilitation prior to discharge
Blood Pressure and Other Cardiovascular ComplicationsCVD is very common in the CKD population. Currently, hypertension is listed as the cause of renal failure in almost one-third of all new-start dialy-sis patients. Hypertension/large vessel
adjusted hospitalization rates in medicare cKD patients aged 66 and older, 20092
tABlE 1
Per 1000 Patient Years Per 1000 Patient Years
No diabetes/no CVD All CKD, 315 Stage 4-5 CKD, 337
Diabetes and/or CVD All CKD, 625 State 4-5 CKD, 778
the facts About Chronic Kidney Disease (CKD)
• 26 million American adults have CKD and millions of others are at increased risk
• Early detection can help prevent the progression of kidney disease to kidney failure
• Heart disease is the major cause of death for all people with CKD
• Glomerular filtration rate (GFR) is the best estimate of kidney function
• Hypertension causes CKD, and CKD causes hypertension
• Persistent proteinuria (protein in the urine) means CKD is present
• High-risk groups include those with diabetes, hypertension, and family history of kidney disease
• African Americans, Hispanics, Pacific Islanders, Native Americans and seniors are at increased risk
• Three simple tests can detect CKD: blood pressure, urine albumin, and serum creatinine
what Causes CKD?
The two main causes of chronic kidney disease are diabetes and high blood pressure. Other conditions that affect the kidneys are:
• Glomerulonephritis, a group of diseases that cause inflammation and damage to the kidney’s filtering units. These disorders are the third most common type of kidney disease
• Inherited diseases, such as polycystic kidney disease, which causes large cysts to form in the kidneys and damage the surrounding tissue
• Malformations that occur as a baby develops in its mother's womb. For example, a narrowing may occur that prevents normal outflow of urine and causes urine to flow back up to the kidney. This causes infections and may damage the kidneys
• Lupus and other diseases that affect the body's immune system
• Obstructions caused by problems like kidney stones, tumors or an enlarged prostate gland in men
• Repeated urinary infections
Source: National Kidney Foundation. About chronic kidney disease. http://www.kidney.org/kidneydisease/aboutckd.cfm. Accessed June 4, 2013.

June/July 2013 CareManagement 9
Exclusively for ACCM Members
disease is listed as the cause for 28.1% of all patients requiring RRT, mak-ing it second only to diabetes, which is responsible for 44.6%.2 Medications used to treat hypertension, diabetes and other cardiovascular disease are often changed while admitted. • Carefully explain dosing guidelines
to the patient and family and the outpatient dialysis facility
An important component of hyper-tension management in dialysis patients is the need to achieve euvolemic status. Evaluation of changes in body weight is a way to evaluate overall fluid status. Hypotension and hypertension are directly related to fluid volume. Weight changes that occur during hospitaliza-tion but are not communicated to the treatment team are associated with an increased risk for readmission.8 “Dry weight” adjustments need to be com-municated to the outpatient dialysis setting. Because fluid volume status and cardiovascular stability greatly affect the delivery of dialysis, treatment parameters used during a dialysis ses-sion may need to be adjusted. These adjustments improve a patient’s long-term ability to tolerate dialysis and decrease readmissions. • Communicate any change in “dry
weight” to the dialysis center at discharge
• Communicate any changes in car-diac function (eg, ejection fraction, cardiac/surgical procedures) to the dialysis unit at discharge
Mineral Bone DensityMineral bone disease (MBD) is linked to altered metabolism of phosphorus/calcium due to loss of the kidneys’ abil-ity to convert vitamin D into a useable form. This results in long-term bone demineralization and calcification of both the soft tissue and vasculature.6 Vascular calcification is associated with increased cardiovascular mortal-ity.9 Treatment for hyperphosphatemia has been shown to be independently
associated with increased mortality.10 Continuation and ongoing evaluation of phosphorus, calcium and parathy-roid hormone with the adjustment of phosphate binders and vitamin D analogs has been reported to reduce repeat hospitalizations by 6%.5 Careful attention to continuation of phosphate binders, vitamin D analogs, and para-thyroid-suppressing medications is nec-essary while the patient is hospitalized.• Ensure that patients continue MBD
treatment whenever hospitalized
DiabetesIn the United States, 44.6% of all patients receiving dialysis are diabetic.2
It is estimated that 33% to 69% of all medication-related hospitalizations are due at least in part to medication non-adherence, costing hundreds of billions of dollars per year. Social and eco-nomic factors like insurance benefits, insurance restrictions, copays, and lack of social or community support system affect the ability of patients to maintain adherence.11
• Communicate about any and all med-ication changes to all who are car-ing for the patient when discharged (including family members)
• Send updated medication lists to dialysis facilities
• Ensure that patient and family edu-cation about medication use is com-pleted and understanding is apparent
• Ensure that written prescriptions for all medications are given to patients and families
• Evaluate the patient’s ability to obtain and afford medications after discharge
Interventions Related to Infections Bloodstream InfectionsA leading cause of death among dialysis patients is bloodstream infections. In 2007, the Centers for Disease Control and Prevention (CDC) estimated that 37,000 bloodstream infections occurred in hemodialysis patients with central
access lines. One out of 4 of these patients may have died as the result of these infections. Since 1993, hospitaliza-tion rates for bloodstream infections has risen to 47%, and vascular access infec-tions have increased by 87%.12 Because of the high risk of infections, dialysis units will be required to report both bloodstream and central venous access infections to the National Healthcare Safety Network (NHSN) by 2014 to get full payment for services from Medicare.
In CKD patients, high levels of uremic toxins decrease the efficiency of the immune response to infection. Alterations include decreased granulo-cyte counts, impaired humoral and cell-mediated immunity, defective phago-cyte function, dysfunctional acute inflammatory response, and delayed hypersensitivity reactions. In addition 18% to 75% of dialysis patients have protein-energy malnutrition caused by the inflammation created by the hyper-catabolic states induced by chronic disease and the dialysis treatment itself. It is not surprising that malnutrition and inflammation are predictors of hos-pitalization. Fortunately increasing the level of albumin through nutritional support has been shown lower the risk of hospitalization and death in dialysis patients.5 Proactive nutritional interven-tions need to be started early during hospitalization.• Begin nutritional consultation early,
and start supplements • If indicated, obtain a swallowing
evaluation Identifying and treating infection
and inflammation will always remain a mainstay of treatment. Following up with the surgeon or infectious disease professional is often necessary after discharge. Many patients will be dis-charged while still receiving antibiotics. Completion of antibiotic therapy is piv-otal in both ensuring successful treat-ment and minimizing antibiotic resis-tance. Many antibiotics are not readily available in the dialysis setting, so t

10 CareManagement June/July 2013
early notification may be necessary so the medications can be obtained. • Communicate with the outpatient
unit about the continued need for antibiotics
• Schedule a follow-up visit with the infectious disease specialist or surgeon
• Notify the dialysis unit notified about follow-up appointments
• Notify the dialysis unit of wounds or other open areas that need evaluation
• Discuss the potential need for isolation requirements with the outpatient facility
Vascular AccessAdmission for infections or other com-plications due to vascular access makes up the third most common reason for hospitalization of patients with CKD on RRT. As stated earlier in this article, repeat hospitalization is more common in new hemodialysis patients who are started on dialysis using a temporary catheter. According to the CDC,12 37,000 patients are started on dialysis with catheters. Many of these patients are hospitalized, and, often, temporary catheters (uncuffed) are used for the initial treatments. Temporary catheters need to be converted to permanent catheters (cuffed) before discharge, increasing the opportunity for catheter-related infection (CRI).13 In general, use of subclavian and other central lines should be minimized because of the high risk of developing chronic cen-tral vein stenosis, complicating more distal access creation.14
Once dialysis has begun and a cath-eter has been placed, it is imperative to initiate planning for an arteriovenous fistula (AVF) or arteriovenous graft (AVG). Preserving veins by minimizing
the use of peripherally inserted cathe-ters (PICC) lines and arterial punctures in the forearm and upper arm will greatly increase the chances for AVF creation15 and ultimately lower rates of infections and hospitalizations. Early consultation with a vascular surgeon will facilitate vein preservation and early access placement.
Data show that AVF have the low-est infection rate, last the longest, and require the least amount of interven-tions to keep them working.16 In July of 2003 the End Stage Renal Disease Network created the National Vascular Access Improvement Initiative (NVII) with the goal of increasing the use of AVFs.17 The program was been extremely successful and reached the goals of 50% incidence and 40% prevalence of AVFs by 2005. CMS rec-ognized the project and deemed it a breakthrough initiative; it was renamed the Fistula First Breakthrough Initiative (FFBI). The program continues today, and the current prevalence rate has improved to 66%.18 The program has now changed it’s focus to “fistula first/catheter last” with the goal of starting new dialysis patients with AVFs instead of catheters. • Initiate a Save the Vein program at
your institution• Ensure that procedures for facilitat-
ing evaluation for permanent access by a vascular surgeon are completed before discharge from the hospital
• Educate the patient and family regarding catheter/AV access care before discharge
• Communicate with the dialysis center about the consulting surgeon, when catheter/AV access placement is scheduled, and what follow-up care is needed
Case ManagementThe Case Management Society of America’s (CMSA) current definition of case management states that it is “a collaborative process of assessment, plan-ning, facilitation and advocacy for options and services to meet an individual’s health needs through communication and avail-able resources to promote quality cost-effective outcomes1….”
Certainly case management in the case of CKD patients fits well into this definition. In the preface of the Standards of Practice for Case Management 2010 revision, is a list of important factors that case managers need to address1:• Minimizing fragmentation in the
health care system• Using evidence based guidelines in
practice• Navigating transitions of care• Incorporating adherence guidelines
and other standardized tools• Expanding the interdisciplinary team
in planning care for individuals• Improving patient safety Hopefully this article has provided some information to help you as you strive to meet these Standards. CEU
References1. Case Management Society of America. Standards of Practice for Case Management. Little Rock, AK: Case Management Society of America; 2010. www.cmsa.org/portals/0/pgf/membersonly/standardsofpractice.pdf. Accessed June 3, 2013.
2. US Renal Data System. USRDS 2012 Annual Data Report: Atlas of End Stage Renal disease in the United States. Bethesda, MD: National Institute of Diabetes & Digestive & Kidney Diseases; 2012. www.usrds.org/ard.aspx. Accessed May 30, 2013.
3. National Kidney Center. Chronic kidney disease. Stages. http://www.nationalkidneycen-
CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit
as stated earlier in this article, repeat hospitalization is more common in new hemodialysis patients who are started on dialysis using a temporary catheter.

April/ May 2013 CareManagement 11
Exclusively for ACCM Members
ter.org/chronic-kidney-disease/stages/?gclid=CMrB8NmIxrcCFQFnOgodvQkAng. Accessed June 2, 2013.
4. Arora P, Kausz A, Obrador G, et al. Hospital utilization among chronic dialysis patients. J Am Soc Nephrol. 2000;11:740-746.
5. Castner D. Management of patients on hemodialysis before, during and after hospital-ization: challenges and suggestions for improve-ments. Nephrol Nurs J. 2011;38(4):319-330.
6. Count C. ANNA Core Curriculum for Nephrology Nursing. 5th ed. Pitman, NJ: American Nephrology Nurses Association; 2008.
7. Brophy D, Gitlin M, Mayne T. Characterizing hospitalizations of end stage renal disease patients on dialyisis and inpatient utilization of erythropoiesis-stimulating agent therapy. Ann Pharmother. 2010;44(1):43-49.
8. Chan K, Lazarus M, Wingard R, Hakim Y. Association between repeat hospitalization and early intervention in dialysis patients following hospital discharge. Kidney Int. 2009;76:331-341.
9. Spiegel D, Brady K. Calcium balance in nor-mal individuals and in patients with chronic kidney disease on low- and high-calcium diets. Kidney Int. 2012. Epub ahead of print.
10. Isakova T, Gutierrez O, Chang Y, et al. Phosphorus binders and survival on hemodi-alysis. J Am Soc Nephrol. 2009;20:388-396.
11. Wolfgram N. Medication adherence. What’s a prescriber’s responsibility? Adv NPs PAs. 2012;3(9):27-28.
12. Centers for Disease Control and Prevention. Clinician education. Dialysis safety. www.cdc.gov/dialysis/clinician/index.html. Last updated May 9, 2013. Accessed June 3, 2013.
13. Bakke C. Clinical and cost effective guide-lines to prevent intravascular catheter-related infection in patients on hemodialysis. Nephrol Nurs J. 2010;37(6):601-615.
14. Steward C. Preventing the Decline of Kidney Function in Hospitalized Patients. Mosby Nursing Consult. Clinical Update. http://www.nursingconsult.com/das/stat/view/174015352-2/cup. Published 2011. Accessed June 3, 2013.
15. Ray T. Save the vein: what nurses need to know. Nephrol Nurs J. 2011;38(1):85-86.
16. National Kidney Foundation. KDOQI Guidelines for Vascular Access. http://www.kidney.org/professionals/KDOQI/guide-line_upHD_PD_VA/index.htm. Accessed June 3, 2013.
17. Peters V, Clemons G, Augustine B. Fistula first: vascular access update. Nephrol Nurs J. 2005;32(6):686-687.
18. Fistula First. http://fistulafirst.org/AboutAVFistulaFirst/History.aspx. Accessed June 3, 2013.
Ensure continuation of erythropoiesis-stimulating agents (ESA) during hospitalization.
Continue renal vitamins and supplement iron as needed.
Evaluate/treat for underlying problems with blood loss including GI loses and anticoagulation. (Note: Postsurgical patients are at especially high risk.)
Evaluate physical functioning and need for rehabilitation prior to discharge.
Carefully explain dosing guidelines to the patient and family and the outpatient dialysis facility.
Communicate any change in “dry weight” to the dialysis center at discharge.
Communicate any changes in cardiac function (eg, ejection fraction, cardiac/surgical procedures) to the dialysis unit at discharge.
Ensure that patients continue mineral bone density (MBD) treatment whenever hospitalized.
Communicate about any and all medication changes to all who are caring for the patient when discharged (including family members).
Send updated medication lists to dialysis facilities.
Ensure that patient and family education about medication use is completed and understanding is apparent.
Ensure that written prescriptions for all medications are given to patients and families.
Begin nutritional consultation early, and start supplements.
If indicated, obtain a swallowing evaluation.
Evaluate the patient’s ability to obtain and afford medications after discharge.
Communicate with the outpatient unit about the continued need for antibiotics.
Schedule a follow-up visit with the infectious disease specialist or surgeon.
Notify the dialysis unit notified about follow-up appointments.
Notify the dialysis unit of wounds or other open areas that need evaluation.
Discuss the potential need for isolation requirements with the outpatient facility.
Initiate a Save the Vein program at your institution.
Ensure that procedures for facilitating evaluation for permanent access by a vascular surgeon are completed before discharge from the hospital.
Educate the patient and family regarding catheter/AV access care before discharge.
checklist of interventions for patients With cKD Who receive rrt

CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit
12 CareManagement June/July 2013
University of California, San francisco Medical Center:
Reducing Readmissions Through Heart Failure Care Management: Part I
By Douglas McCarthy
Organization: The University of California, San Francisco (UCSF) Medical Center is a leading academic medical center with several inpatient and outpatient facilities and primary care clinics in San Francisco, including a 559-bed main hospital at its Parnassus campus, the site of the intervention.
Objective: Reduce by 30% the rate of hospital readmissions for any cause within 30 and 90 days of a hospital discharge among the target population.
Target Population: Medicare patients age 65 and older (average age 80) hospitalized with a primary or secondary diagnosis of HF (representing approximately 700 admissions during the year the program began); more than half of these patients identified with a racial/ethnic minority group and almost one-third spoke a language other than English.
Team: Two HF program nurse coordinators, supported by a multidisciplinary team comprising a cardiovascular service line director, hospitalists, cardiologists, clinical nurse specialists, case managers, social workers, pharmacists, dieticians, chaplains, educators, primary care physicians, skilled nursing facility staff, home care nurses, and outpatient nurse practitioners.
Approach: Create an ideal transition from hospital to home through the following interventions:
1. Form a multidisciplinary team to support learning and improvement.
2. Engage in extensive patient education using “teach-back” techniques.
3. Schedule a follow-up physician appointment to occur within 7 days of discharge.
4. Make a follow-up telephone call to the patient within 7 days of discharge.
5. Refer the patient to needed services and home care.
6. Collect and analyze readmission data to measure progress.
7. Communicate and collaborate with clinicians/ providers across the continuum of care.
The HF management program also coordinates with skilled nursing facilities to support consistent education and successful transitions for patients needing institutional postacute care.
Timeline and Funding: UCSF initiated the program in late 2008 in collaboration with the Institute for Healthcare Improvement and with funding from the Gordon and Betty Moore Foundation. The program has since become self-sustaining and is being expanded to include all adult patients with HF.
Results in Brief: Within the target population, there was a 46% relative reduction in the 30-day all-cause HF readmission rate, from 24% in 2009 to 13% in 2011. Likewise, there was a 35% relative reduction in the 90-day all-cause HF readmission rate, from 40% in 2009 to 26% in 2011.
the program at a glanceBox 1
In 2008, the University of California, San Francisco (UCSF) Medical Center embarked on a grant-funded program to reduce hospital readmissions for elderly patients with heart failure (HF) (Box 1). With support from medical center leaders and a multidisciplinary team, program coordinators provide enhanced patient education and follow-up care connections to promote the patient’s successful transition to home or to skilled nursing care. Over 2 years, rates of all-cause HF readmissions in the target population declined by 46% within 30 days of hospital discharge and by 35% within 90 days. With internal funding, the program is being sustained and expanded to younger patients. The medical center applies learning from the program to support the goal of reducing all readmissions as part of a performance incentive program for public hospitals. Program staff highlight collaboration and communication as key factors to the program’s success.
Part I of this article is presented in this issue, and Part II will be in the August/September issue.

Exclusively for ACCM Members
June/July 2013 CareManagement 13
The ChallengeHF—the inability of the heart to pump enough blood to meet the body’s needs—is a serious and costly condition affecting up to 1 of 10 older people. Nationally, almost one-quarter of Medicare patients hospitalized with HF are readmitted to the hospital within 30 days and one-half are readmitted within 6 months—a reflection of the difficulty patients and family caregiv-ers face in successfully managing this chronic condition. Comprehensive discharge planning and disease man-agement programs that offer sustained follow-up care have reduced read-missions among HF patients in con-trolled trials but remain underused in practice, owing in part to misaligned financial incentives. The potential of less intensive approaches focused on improving patient education in the hospital and transitioning patients to postdischarge care has not been fully explored.
The Impetus for ChangeIn 2008, the UCSF Medical Center (Table 1) received a 2-year grant
from the Gordon and Betty Moore Foundation to optimize discharge plan-ning and reduce hospital readmissions among frail elders with HF. The grant enabled UCSF to participate in the Institute for Healthcare Improvement’s (IHI) Transforming Care at the Bedside collaborative, which provided improvement tools, institutional men-toring, and a framework for creating an ideal transition from the hospital to home (Box 2).1 This framework was subsequently adopted by IHI’s State Action on Avoidable Rehospitalizations (STAAR), a Commonwealth Fund– sponsored initiative for which UCSF has served as a mentor.
Implementing and adapting this improvement framework to UCSF’s circumstances required institutional and day-to-day leadership together with multidisciplinary teamwork. During the first year of the grant, the program’s leaders focused on establishing a firm foundation for success on three units within the hospital where most HF patients are treated. In the second year, they invited outpatient and post-acute care providers to collaborate on improving transitional care and adopt a common approach to patient educa-tion. Since then, the leaders have been working to sustain the program with internal funding and to expand its reach to include younger adults.
Leadership and Teamwork. Karen Rago, RN, MPH, director of the medical center’s cardiovascular service line, has provided executive leader-ship to establish the program and help overcome organizational barriers to its implementation, with the support of Maureen Buick, RN, the medical center’s director of nursing education and performance improvement. They recruited two former staff nurses on the heart and vascular unit, Eileen Brinker, RN, MSN, and Maureen Carroll, RN, CHFN, to work together on a part-time basis (equivalent to
1.6 full-time staff) as program coor-dinators. The program coordinators’ responsibilities include educating patients and family caregivers, ensur-ing appropriate consultations, coor-dinating discharge support, making postdischarge phone calls to patients, collecting and analyzing data, and col-laborating with outpatient providers on transitions to postdischarge care.
After receiving training in IHI’s approach to improvement, Brinker and Carroll introduced themselves to more than 50 clinicians and staff to understand current care processes, identify opportunities for improvement, and build interest in the program. They analyzed the medical records of patients readmitted in the past to assess historical patterns of care and
Douglas McCarthy, MBA, is senior research adviser to The Commonwealth Fund and the Institute for Healthcare Improvement in Cambridge, Mass. He conducts qualitative research on efforts to promote health system transformation, supports The Commonwealth Fund’s scorecard project, and is a contribut-ing editor to the bimonthly newsletter Quality Matters. His 25-year career has spanned research, policy, operations, and consulting roles for government, corporate, academic, and phil-anthropic organizations. He has authored and coauthored 50 case studies of high-performing organizations and initiatives. Mr. McCarthy received his bachelor’s degree with honors from Yale College and a master’s degree in health care management from the University of Connecticut. During 1996–1997, he was a public policy fellow at the Hubert H. Humphrey School of Public Affairs at the University of Minnesota.
the institute for healthcare improvement’s framework for creating an ideal transition from hospital to home2
Box 2
1. Enhanced admission assessment for postdischarge needs
2. Enhanced teaching and learning
3. Patient and family-centered handoff communication
4. Postacute care follow-up
t
profile of Ucsf medical center’s parnassus campus (annual figures)
tABlE 1
559 Licensed beds
29,000 Admissions
40,000 Emergency visits
770,000 Outpatient encounters
700 Medicare admissions for heart failure (primary or secondary diagnosis) at the start of the intervention
7,000 Employees

CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit
14 CareManagement June/July 2013
potential causes of readmissions—a practice they continue—and developed a tracking system to measure the pro-gram’s progress toward its goals.
These activities led to a kickoff meeting with a multidisciplinary team, an event that generated common understanding and support for launching the program. The team continues to meet every other month to review progress toward goals, offer advice on plans, and share experience and learning about issues of common concern. The team’s
membership has since expanded to include representatives of the entire care continuum: the HF program coordinators, hospitalists, cardiologists, clinical nurse specialists, case mangers, a dietician, the medical center’s palliative care service and home care agency, educators and a statistician from the nursing school, nurse practitioners in the medical center’s HF outpatient clinic, the local district manager of a nursing home chain, and a geriatrician from a local skilled nursing facility.
The Steps of ChangeEnhanced Assessment and Referral.Floor nurses assess HF patients after admission to the unit to identify refer-ral needs, such as for rehabilitation therapy, home care, and consultations by dieticians, case managers, social workers, and spiritual or palliative care services. Brinker and Carroll review the assessments to ensure that all appro-priate referrals and consultations are made for patients. The program set a goal for these assessments to be com-pleted within 24 hours of a patient’s admission for at least 90% of patients, though that goal has proven challeng-ing. The coordinators track selected risk factors—whether the patient has a primary care physician, is taking 10 or more medications, has support at home, has poor health literacy, or has been hospitalized in the past 6 months—in order to tailor interven-tions to patients’ individual needs. Further work to improve patient assess-ments is being undertaken as part of a broader program to reduce readmis-sions at the medical center.
Enhanced Teaching and Learning.After a hospital visit, patients and fam-ily caregivers often do not fully recall self-care information or recognize a deterioration in their condition in time to get help before emergency care becomes necessary. Understanding this, Brinker and Carroll began revis-ing patient education materials and developing tools to promote health literacy. They drew on advice from patients recruited for an advisory group established to suggest ways to make the materials easier to comprehend. The materials were translated into four lan-guages common to the patient popula-tion and organized into a binder, for easy reference.
In addition to offering group “Heart Healthy” classes on a hospital unit, Brinker and Carroll arranged their schedules so they would be
patient education Using teach-back
Box 3
teach-back is a patient education technique that:
• Asks people to explain in their own words what they need to know or do
• Offers a way to check for understanding and, if needed, to restate or clarify the information
• Promotes health literacy and places responsibility for success on the teacher
Principles for effective application:
• Identify and teach to the primary learner (patient or responsible family caregiver)
• Use plain language; avoid jargon
• Maintain a shame-free environment (teach-back is not a test)
• Keep teaching sessions short and frequent, if possible
• Limit information to what is needed
• Use open-ended questions; avoid yes/no questions, such as “Do you understand?”
• Listen before teaching; try to ascertain the learner’s baseline knowledge and situation, for example, by asking, “Tell me what you know about your heart?”
Sample teach-back questions:
• “I want to be sure that I did a good job of teaching you today about how to stay safe and well after you go home. Could you please tell me in your own words the reasons you should call the doctor?”
• “Would you explain to me how you will weigh yourself (at home) so that I can make sure that I have explained it correctly?”
teaching goal in UCSf’s heart failure program:
The patient or family caregiver will take appropriate action when there is a change in the patient’s health.

Exclusively for ACCM Members
June/July 2013 CareManagement 15
available throughout the week to teach patients and family caregivers indi-vidually about HF and managing the condition at home. When possible, they attempt to build and rein-force learn-ing during several short teaching ses-sions throughout the hospital stay, since teaching everything at once can be overwhelming to patients and caregiv-ers. HF patient education has four core topics derived from evidence-based guidelines for self-care3:1. Routinely taking a diuretic medica-
tion (“water pill”). 2. Limiting salt intake by avoiding cer-
tain foods. 3. Monitoring and reporting weight
gain to the doctor. 4. Calling the doctor when there is a
change in health.The care coordinators instituted a
“teach-back” technique (already used by pharmacists on patient rounds at the medical center) to promote patient comprehension and retention of HF teaching (Box 3). They also trained floor nurses on the core content of HF education as well as the teach-back technique, so that every patient encoun-ter could serve as an opportunity to reinforce core messages. By system-atically tracking patient responses to teach-back questions, the program team observed a temporal association between an increasing level of patient comprehension on the four HF teach-ing topics and a decreasing rate of readmissions over time. This finding validated their belief in the efficacy of teach-back.
Over time, the program team sought the support of nursing lead-ers to make teach-back a part of the culture of teaching on the three pilot
units. The team identified a nurse to “champion” teach-back on each unit and encouraged nursing staff to use the method routinely in all patient interactions, such as when explaining medications or giving instructions on use of the call button. In the second year, the care coordinators extended the program’s reach by inviting the participation of local skilled nursing facilities and home care agencies in fol-lowing a consistent approach to patient education after discharge. The coor-dinators provide periodic in-service training to skilled nursing facility staff and host a meeting of home care agen-cies twice a year to review the interven-tion and promote consistent patient communication.
As Brinker and Carroll listened to patients’ stories, they found that patients with advanced HF, as well as their family members, often did not fully comprehend the seriousness of the condition, which can have a prog-nosis similar to late-stage cancers. In response, they accompanied the medi-cal center’s palliative care service staff on patient rounds—and later attended formal training—to learn techniques for engaging patients in conversations about setting goals for care.*
This attention led to a modest increase in palliative care consultations among HF patients. Moreover, by rais-ing awareness of the issue, their efforts prompted the medical center to set a new clinical standard for offering pal-liative care consultations to all high-risk HF patients—those readmitted three or more times in a year. The medical center’s spiritual care services recently assigned a chaplain trained in psychol-ogy to work with the team.
Arranging for Postacute Follow-Up Care. The coordinators emphasize the importance of follow-up care during teaching and work with the medical center’s clerks to schedule follow-up physician visits before patients are discharged. The goal is to secure an appointment within the critical 7-day period following the discharge date. When they found this goal difficult to achieve for all patients, Brinker and Carroll opened a dialogue with primary care physicians who refer patients to the medical center’s cardiologists. This strengthened follow-up relationships and, as a result, the 7-day goal was achieved for 76% of program patients in 2011, up from 68% in 2010.
During the program’s second year, in August 2010, UCSF expanded follow-up options for a limited number of high-risk patients who require close monitoring or medication management. These patients are able to make appointments in the medical center’s outpatient HF clinic with a cardiologist, primary care physician, or nurse practitioner. Visits with the nurse practitioner last one hour and include a thorough review of medications, a knowledge assessment, further patient and family education using the teach-back method, and referrals to specialists. The nurse practitioners are available for follow-up calls and may continue to see the patient biweekly or as needed, for medication titration and education, during the critical interim period before the patient has stabilized and is ready to transition to routine primary care.
Also in 2010, USCF created a Geriatric Transitions, Consultation, and Comprehensive Care (GeriTraCCC)
patients with advanced hf, as well as their family members, often did not fully comprehend the seriousness of the condition, which can have a prognosis similar to late-stage cancers.

CEU for CCM & CDMS approved for 2 hours of ccm and cDms education credit
16 CareManagement June/July 2013
program that offers certain high-risk HF patients the opportunity to receive “house calls” by a UCSF physician trained in geriatric medicine. The physician collaborates with home health nurses and the patient’s primary care physician and cardiologists to promote a smooth transition home, discuss goals of care, provide palliative
care, and address issues that may impede optimal recovery at home. The service, funded by the medical center, is offered each month to an average of 5 frail elderly patients who have end-stage heart disease and concerns such as multiple admissions, missed appointments, medication nonadherence, impaired cognition, or
inadequate caregiver support. Initial GeriTraCCC visits are made in the hospital prior to discharge or within 48 hours of returning home from the hospital or a nursing facility. Visits continue as long as needed until risk factors are reduced or the patient is stabilized or expires; on average, patients receive 3 to 4 visits.
For HF patients who are discharged to home (about 80% of patients), Brinker or Carroll call the patient or family caregiver within 7 days of discharge, and again at 2 weeks, whenever possible, to check on the patient’s progress and reinforce the 4 core teaching topics using the teach-back method. Through persistent call-back efforts, they reach approximately 95% of these patients. This follow-up contact offers the opportunity to build on the relationship and knowledge of the patient’s situation established during the hospital stay. Patients can call the coordinators during the day or leave a message for nonurgent questions. The coordinators may ask the medical center’s pharmacist or dietician to call the patient to answer questions about medication or diet. The coordinators educate and coach patients to call their physician if they are not feeling well, or to call 911 if they are having an acute episode.
The coordinators also seek to obtain home care for patients within 48 hours of hospital discharge, when possible. Given the physical and cognitive challenges faced by this patient population, the medical center recently began offering home care referrals to all HF patients on the assumption that most will qualify for services and that it is best to assess their situation in the home environment. (About half of the HF patients select UCSF’s home health care provider, which pays for the home assessment in rare cases when the patient’s insurance does not cover the visit.)
secure e-mail to Virtual care team
Box 4
Dear Team,
We wanted to let you know that we are following patient X in the Heart Failure Program.
The Heart Failure Program is for patients 50 and older who are admitted to the hospital with a primary or secondary diagnosis of heart failure. Our program includes thorough patient education on heart failure, follow-up phone calls after discharge, and assistance with other discharge planning needs.
We encourage all physicians to order RN Home Care visits for CHF patients (see patient’s case manager and write CHF protocol on PDP). Please schedule a follow-up appointment with patient’s PCP, NP, or Cardiolo-gist within 7 days of discharge for those patients with primary or active heart failure. The standard of care for the Heart Failure Program is to request a consult from the Palliative Care team for a goals-of-care discussion (the PC team has agreed to this) if the patient has been admitted three times within 12 months.
If we can help with any of these planning needs or answer any questions, please feel free to call us at X.
Our goal is to reduce readmissions and improve patient care.
CMS Core Measure Reminders for Physicians:
• Document results of LVS function assessment
• Prescribe ACEI or ARB for LVSD at discharge (or document reason not prescribed for ACEI and ARB)
• Document follow-up appointment on patient’s discharge paperwork
• Discharge medications listed on discharge summary MUST match patient discharge prescription and medication list
Thank you,
Maureen Carroll, RN, CHFN Heart Failure Program Coordinator UCSF Medical Center

Exclusively for ACCM Members
June/July 2013 CareManagement 17
Patient-Centered Handoff Communication. During the second year of the grant, Brinker and Carroll built close working relationships with nurse practitioners in the medical center’s outpatient HF clinic, as well as with home care nurses and the home-visiting geriatric physician, to institute a formal patient “hand-off” procedure. As part of the discharge plan, the handoff identifies follow-up concerns for each patient, including patient education topics in need of reinforcement based on responses to teach-back questions. To enhance communication with postacute providers, two skilled nursing facilities recently added a clinical liaison staff person and, likewise, UCSF asks each home care agency to identify a primary clinical contact person.
Two related interventions were aimed at improving communication and coordination during patient transitions in care. The first involved strengthening the process of “medica-tion reconciliation” by increasing phar-macist consultations before hospital discharge and developing a patient-friendly tool so that patients would leave the hospital with an accurate and easy-to-understand list of medica-tions to be continued after discharge. Second, the medical center’s medicine team set a goal to improve the timeli-ness of discharge summaries so that they would be ready for postacute care providers when the patient is dis-charged from the hospital (or shortly thereafter).
In another key innovation, Brinker and Carroll began using the medical center’s secure e-mail system to
enhance communication among care providers, who often see patients on different days and times. By sending out an e-mail alert when a HF patient was admitted to the program (Box 4), they created the opportunity for electronic communication among a virtual multidisciplinary care team, including the patient’s attending and resident physicians, case manager, pharmacist, and dietician in the hospital, as well as post-acute care providers such as the skilled nursing facility or home care nurse. (About two-thirds of HF patients are seen by physicians affiliated with UCSF; the coordinators may call the patient’s primary care physician if she or he is not part of the UCSF system and does not have access to secure e-mail.)
Although the care coordinators found that managing this e-mail stream was time-consuming, they observed its clear benefits in facilitating shared understanding of patient needs so that providers could better anticipate and deliver appropriate care throughout and following a patient’s hospital stay. Brinker and Carroll note that e-mail’s immediacy prompts attention to concerns and facilitates electronic conversations; hence, it serves as an adjunct rather than a replacement to documentation in the electronic health record. Anecdotal evidence suggests that such communication has helped to avert some readmissions. CEU
Part II: The Results will be presented in the August/September issue of CareManagement.
This case study was conducted under a grant to the Institute for Healthcare Improvement from The Commonwealth Fund. Pat Rutherford, R.N., M.S., vice president at the Institute for Healthcare Improvement, arranged the site visit, participated in the interviews, and offered advice on the project. The author is grateful to staff at UCSF Medical Center who graciously shared their time, experience, and insights for the case study, in particular Karen Rago, RN, MPH, who recently retired from her position as director of the medical center’s cardiovascular service line, and Eileen Brinker, RN, MSN, and Maureen Carroll, RN, CHFN, the heart failure program coordinators.
Editorial support was provided by Paul Frame.
Reprinted with permission of The Common-wealth Fund at www.commonwealthfund.org.
References1. Institute for Healthcare Improvement. Transforming Care at the Bedside. Cambridge, MA: Institute for Healthcare Improvement; 2008.
2. Nielsen GA, Bartely A, Coleman E, et al. Transforming Care at the Bedside How-to Guide: Creating an Ideal Transition Home for Patients with Heart Failure. Cambridge, MA: Institute for Healthcare Improvement; 2008.
3. Riegel B, Moser DK, Anker SD, et al. State of the science: promoting self-care in persons with heart failure. A Scientific Statement from the American Heart Association. Circulation. 2009;120(12):1141-1163.
although the care coordinators found that managing this e-mail stream was time-consuming, they observed its clear benefits in facilitating shared understanding of
patient needs so that providers could better anticipate and deliver appropriate care throughout and following a patient’s hospital stay.

18 CareManagement June/July 2013
Exam 2Exam 1
18 CareManagement June/July 2013
1. Nationally, almost ____ of Medicare patients hospitalized with HF are readmitted to the hospital within __ days and ____ are readmit-ted within 6 months.a. one-quarter, 60, one-half c. one-half, 30, one-quarterb. one-quarter, 30, one-half d. one-half, 60, one-quarter
2. Comprehensive discharge planning and disease management programs that offer sustained follow-up care have been unable to reduce readmissions among HF patients in controlled trials.a. True b. False
3. UCSF participated in the IHI's Ensuring Access to Care for HF col-laborative.a. True b. False
4. One of the ways in which UCSF overcame institutional barriers in adapting its improvement framework for HF care was to recruit two former staff nurses on the heart and vascular unit to work together on a part-time basis.a. True b. False
5. UCSF’s steps of change included:a. Enhanced assessment and referralb. Enhanced teaching and learningc. Arrangement for postacute follow-up cared. Patient-centered handoff communicatione. All of the above
6. The steps of change outlined in question 5 are part of the frame-work of the:a. CDC b. CMS c. IHI d. USCF
7. Teach-back is a patient education technique that:a. Asks people to explain in their own words what they need to know
or do b. Offers a way to check for understanding and, if needed, to restate
or clarify the informationc. Promotes health literacy and places responsibility for success on the
teacher d. All of the above
8. Principles for effective teach-back include maintaining a shame-free environment. a. True b. False
9. CMS core measures for physicians who care for patients with HF include:a. Document results of LVS function assessment b. Document follow-up appointment on patient’s discharge paperworkc. Give brand name medications onlyd. a and ce. a and b
10. The goal of the UCSF program was to reduce by ___ the rate of hospital readmissions for any cause within 30 and 90 days of a hos-pital discharge among the target population.a. 10% b. 20% c. 30% d. 40%
1. As of 2010, there were ________ patients receiving chronic RRT in the United States. a. 594,374 b. 650,367 c. 325,990 d. 243,130
2. Renal disease has many causes, and treatment of the underly-ing disease process will need to continue, thereby complicat-ing the management and increasing mortality.a. True b. False
3. On average, all patients receiving RRT spend almost ___ days/year hospitalized. a. 6 b. 15 c. 12 d. 3
4. The rehospitalization rate for dialysis patients is ____ (highest among patients aged 20 to 44 years), equaling 1.5% of total hospital admissions.a. 50% b. 33% c. 40% d. 25%
5. Factors associated with this increased risk for rehospitaliza-tion within the first 3 months include: a. Non-HMO insuranceb. Ischemic heart diseasec. Late referral to a nephrologistd. Use of a temporary dialysis catheter for the first dialysise. All of the above
6. The three most common reasons for admissions/readmission in chronic dialysis patients include:a. CVD c. Vascular access infectionsb. Systemic infections d. All of the above
7. There are many reasons for anemia to worsen during hospitalization. One of the most preventable is:a. Missing doses of erythropoiesis-stimulating agent (ESA)b. Poor dietc. Poor nursing cared. Nonadherence to vitamin supplementation
8. Currently, _______ is listed as the cause of renal failure in almost one-third of all new-start dialysis patients.a. Anemia c. Coronary artery diseaseb. Hypertension d. Diabetes
9. Data show that AVF have the lowest infection rate and last the longest.a. True b. False
10. In CKD patients, high levels of uremic toxins decrease the efficiency of the immune response to infection. Increasing the level of ______ through nutritional support has been shown to lower the risk of hospitalization and death in dialysis patients.a. Phosphorus c. Sodiumb. Antibiotics d. Albumin
University of California, San Francisco Medical Center: Reducing Readmissions Through Heart Failure Care Management: Part I
Coordinating Care for Patients Needing Renal Replacement Therapies
CEU for CCM & CDMS
NEw! CEU exams may be taken online! Click the links below to take the test online and then immediately print your certificate after successfully completing the test. Or print, complete and mail the exam on the next page. Members only benefit! Exams expire July 31, 2014.
take this exam > take this exam >

June/July 2013 CareManagement 19June/July 2013 CareManagement 19
Exam 1: Coordinating Care for Patients Needing Renal Replacement Therapieslearning objectives:
1. Explain the most frequent reasons for morbidity among patients receiving RRT in the United States.
2. Outline 5 steps that can be taken to promote better health during hospitalization and/or at discharge for patients receiving RRT.
Please indicate your answer to the exam questions on page 18 by filling in the letter:
1. _____ 2. _____ 3. _____ 4. _____ 5. _____ 6. _____ 7. _____ 8. _____ 9. _____ 10. _____
Exam 2: University of California, San Francisco Medical Center: Reducing Readmissions Through Heart Failure Care Management: Part I
learning objectives: 1. Describe the need for programs to reduce readmission rates among patients with HF.
2. Delineate steps of change that made the UCSF program for improving care of HF patients viable.
Please indicate your answer to the exam questions on page 18 by filling in the letter:
1. _____ 2. _____ 3. _____ 4. _____ 5. _____ 6. _____ 7. _____ 8. _____ 9. _____ 10. _____
Continuing Education Program Evaluation Please indicate your rating by circling the appropriate number using a scale of 1 (low) to 5 (high). Exam 1: Exam 2:
1. The objectives were met. 1 2 3 4 5 1 2 3 4 5
2. The article was clear and well organized. 1 2 3 4 5 1 2 3 4 5
3. The topic was both relevant and interesting to me. 1 2 3 4 5 1 2 3 4 5
4. The amount and depth of the material was adequate. 1 2 3 4 5 1 2 3 4 5
5. The quality and amount of the graphics were effective. 1 2 3 4 5 1 2 3 4 5
6. I would recommend this article. 1 2 3 4 5 1 2 3 4 5
7. This has been an effective way to present continuing education. 1 2 3 4 5 1 2 3 4 5
8. Additional comments: _____________________________________________________________________________________________________________
Please print:
Certificant’s Name: ___________________________________________________ CCM ID# _____________________________________________
Email Address: ___________________________________________________ CDMS ID# ___________________________________________
Mailing Address: ___________________________________________________ *ACCM Membership# _________________________________
___________________________________________________ *ACCM Expiration Date: ______________________________
___________________________________________________ *Free CEU exams cannot be processed without above information.
CEU applied for: CCM CDMS
Each educational manuscript has been approved for 2 hours of CCM and CDMS education credit by The Commission for Case Manager Certification and the Certification of Disability Management Specialists Commission. Provider #00059431. Exams are for ACCM members only.* ACCM members must indicate their membership number and membership expiration date in the space provided on the answer sheet. Exams cannot be processed without this information.** To receive credit for either exam, you must score 80% or above. Exams expire July 31, 2014.
Please note: Exams may be taken online at www.academyCCM.org. Click the link in the journal, take the exam, and immediately print your certificate after successfully completing the test. Mailed exams should be sent to: Academy of Certified Case Managers, 1574 Coburg Road #225, Eugene, Oregon 97401. Please allow 4 to 6 weeks for processing of mailed exams.
This CEU exam is protected by US Copyright law. ACCM members are permitted to make one copy for the purpose of exam submission. Multiple copies are not permitted.
*If you are not an ACCM member and wish to become one, please use the application found on page 30 and submit it with this exam and dues.
**I f you have lost or misplaced your membership information, please print the exam and mail it to the address above with a check in the amount of $5.00 made payable to ACCM; your exam will be processed and your membership number and expiration date will be emailed to you.
Exclusively for ACCM Members CareManagement Vol. 19, No. 3 JUNE/JULy 2013

20 CareManagement June/July 2013
PharmaFacts for Case Managers
New Approvals
Nesina (alogliptin); Kazano (alogliptin and metfor-min); Oseni (alogliptin and piolitazone)
Indication and Combination TherapyNesina is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus in mul-tiple clinical settings. It should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis, as it would not be effective in these settings.
Dosage and Administration The recommended dose of Nesina is 25 mg once daily. Nesina may be taken with or without food. Nesina is available in the fol-lowing dosages:• 25-mg tablets are light red, oval, biconvex, film-coated, with “TAK ALG-25” printed on one side. • 12.5-mg tablets are yellow and similarly shaped and marked. • 6.25-mg tablets are light pink and similarly shaped and marked.
Patients With Renal Impairment No dose adjustment of Nesina is necessary for patients with mild renal impairment (creatinine clearance [CrCl] ≥ 60 mL/min). The dose of Nesina is 12.5 mg once daily for patients with moder-ate renal impairment (CrCl ≥ 30 to < 60 mL/min). The dose of Nesina is 6.25 mg once daily for patients with severe renal impair-ment (CrCl ≥ 15 to < 30 mL/min) or with end-stage renal disease (ESRD) (CrCl < 15 mL/min or requiring hemodialysis). Nesina may be administered without regard to the timing of dialysis. Nesina has not been studied in patients undergoing peritoneal dialysis. Because there is a need for dose adjustment based upon renal function, assessment of renal function is recommended prior to initiation of Nesina therapy and periodically thereafter.
Contraindications History of a serious hypersensitivity reaction to alogliptin-contain-ing products, such as anaphylaxis, angioedema, or severe cutane-ous adverse reactions.
Warnings and Precautions Pancreatitis There have been postmarketing reports of acute pancreatitis in patients taking Nesina. After initiation of Nesina, patients should be observed carefully for signs and symptoms of pancreatitis. If pancreatitis is suspected, Nesina should promptly be discontinued and appropriate management should be initiated. It is unknown whether patients with a history of pancreatitis are at increased risk for the development of pancreatitis while using Nesina.
Hypersensitivity Reactions There have been postmarketing reports of serious hypersensitivity reactions in patients treated with Nesina. These reactions include anaphylaxis, angioedema, and severe cutaneous adverse reactions including Stevens-Johnson syndrome. If a serious hypersensitiv-ity reaction is suspected, discontinue Nesina, assess for other potential causes for the event, and institute alternative treatment for diabetes. Use caution in a patient with a history of angioedema with another DPP-4 inhibitor because it is unknown whether such patients will be predisposed to angioedema with Nesina.
Hepatic Effects There have been postmarketing reports of fatal and nonfatal hepatic failure in patients taking Nesina, although some of the reports contain insufficient information necessary to establish the probable cause. In randomized controlled studies, serum alanine aminotransferase (ALT) elevations greater than 3 times the upper limit of normal (ULN) were observed: 1.3% in alogliptin-treated patients and 1.5% in all comparator-treated patients.
Patients with type 2 diabetes may have fatty liver disease, which may cause liver test abnormalities, and they may also have other forms of liver disease, many of which can be treated or managed. Therefore, obtaining a liver test panel and assessing the patient before initiating Nesina therapy is recommended. In patients with abnormal liver tests, Nesina should be initiated with caution.
Measure liver tests promptly in patients who report symptoms that may indicate liver injury, including fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice. In this clini-cal context, if the patient is found to have clinically significant liver
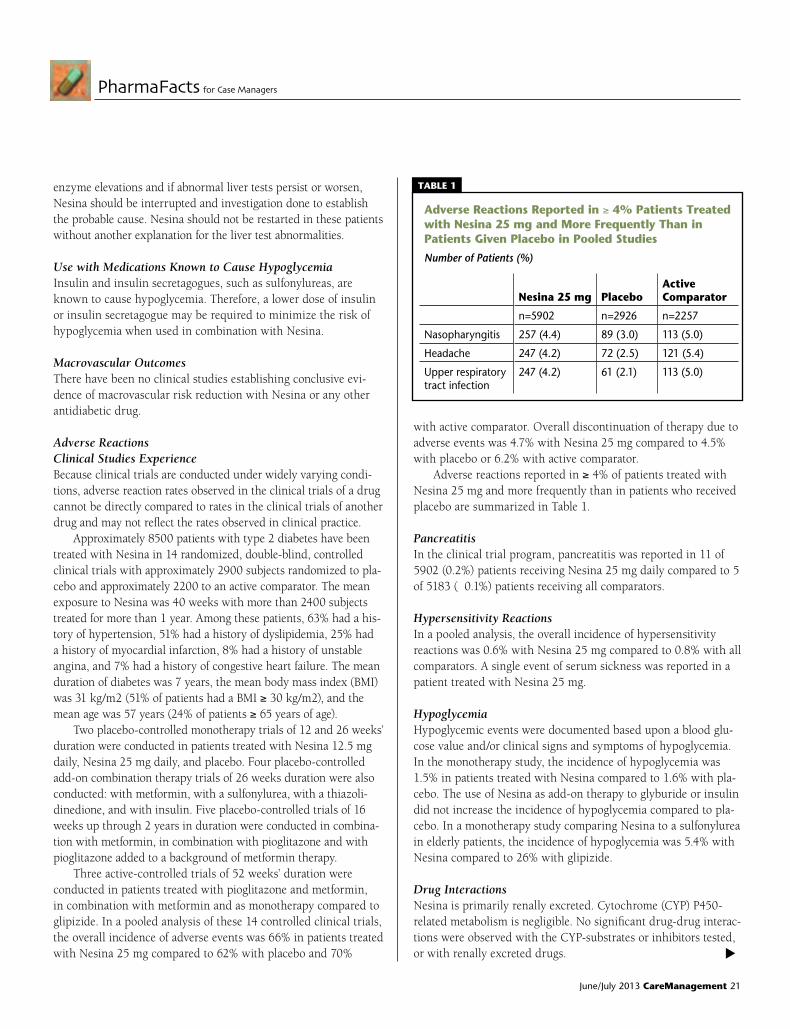
June/July 2013 CareManagement 21
PharmaFacts for Case Managers
enzyme elevations and if abnormal liver tests persist or worsen, Nesina should be interrupted and investigation done to establish the probable cause. Nesina should not be restarted in these patients without another explanation for the liver test abnormalities.
Use with Medications Known to Cause Hypoglycemia Insulin and insulin secretagogues, such as sulfonylureas, are known to cause hypoglycemia. Therefore, a lower dose of insulin or insulin secretagogue may be required to minimize the risk of hypoglycemia when used in combination with Nesina.
Macrovascular Outcomes There have been no clinical studies establishing conclusive evi-dence of macrovascular risk reduction with Nesina or any other antidiabetic drug.
Adverse Reactions Clinical Studies Experience Because clinical trials are conducted under widely varying condi-tions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Approximately 8500 patients with type 2 diabetes have been treated with Nesina in 14 randomized, double-blind, controlled clinical trials with approximately 2900 subjects randomized to pla-cebo and approximately 2200 to an active comparator. The mean exposure to Nesina was 40 weeks with more than 2400 subjects treated for more than 1 year. Among these patients, 63% had a his-tory of hypertension, 51% had a history of dyslipidemia, 25% had a history of myocardial infarction, 8% had a history of unstable angina, and 7% had a history of congestive heart failure. The mean duration of diabetes was 7 years, the mean body mass index (BMI) was 31 kg/m2 (51% of patients had a BMI ≥ 30 kg/m2), and the mean age was 57 years (24% of patients ≥ 65 years of age).
Two placebo-controlled monotherapy trials of 12 and 26 weeks’ duration were conducted in patients treated with Nesina 12.5 mg daily, Nesina 25 mg daily, and placebo. Four placebo-controlled add-on combination therapy trials of 26 weeks duration were also conducted: with metformin, with a sulfonylurea, with a thiazoli-dinedione, and with insulin. Five placebo-controlled trials of 16 weeks up through 2 years in duration were conducted in combina-tion with metformin, in combination with pioglitazone and with pioglitazone added to a background of metformin therapy.
Three active-controlled trials of 52 weeks’ duration were conducted in patients treated with pioglitazone and metformin, in combination with metformin and as monotherapy compared to glipizide. In a pooled analysis of these 14 controlled clinical trials, the overall incidence of adverse events was 66% in patients treated with Nesina 25 mg compared to 62% with placebo and 70%
with active comparator. Overall discontinuation of therapy due to adverse events was 4.7% with Nesina 25 mg compared to 4.5% with placebo or 6.2% with active comparator.
Adverse reactions reported in ≥ 4% of patients treated with Nesina 25 mg and more frequently than in patients who received placebo are summarized in Table 1.
Pancreatitis In the clinical trial program, pancreatitis was reported in 11 of 5902 (0.2%) patients receiving Nesina 25 mg daily compared to 5 of 5183 (˂ 0.1%) patients receiving all comparators.
Hypersensitivity Reactions In a pooled analysis, the overall incidence of hypersensitivity reactions was 0.6% with Nesina 25 mg compared to 0.8% with all comparators. A single event of serum sickness was reported in a patient treated with Nesina 25 mg.
Hypoglycemia Hypoglycemic events were documented based upon a blood glu-cose value and/or clinical signs and symptoms of hypoglycemia. In the monotherapy study, the incidence of hypoglycemia was 1.5% in patients treated with Nesina compared to 1.6% with pla-cebo. The use of Nesina as add-on therapy to glyburide or insulin did not increase the incidence of hypoglycemia compared to pla-cebo. In a monotherapy study comparing Nesina to a sulfonylurea in elderly patients, the incidence of hypoglycemia was 5.4% with Nesina compared to 26% with glipizide.
Drug Interactions Nesina is primarily renally excreted. Cytochrome (CYP) P450-related metabolism is negligible. No significant drug-drug interac-tions were observed with the CYP-substrates or inhibitors tested, or with renally excreted drugs. t
Adverse Reactions Reported in ≥ 4% Patients treated with Nesina 25 mg and More frequently than in Patients given Placebo in Pooled Studies
Number of Patients (%)
Nesina 25 mg
Placebo
Active Comparator
n=5902 n=2926 n=2257
Nasopharyngitis 257 (4.4) 89 (3.0) 113 (5.0)
Headache 247 (4.2) 72 (2.5) 121 (5.4)
Upper respiratory tract infection
247 (4.2) 61 (2.1) 113 (5.0)
tABlE 1

22 CareManagement June/July 2013
PharmaFacts for Case Managers
Clinical StudiesNesina has been studied as monotherapy and in combination with metformin, a sulfonylurea, a thiazolidinedione (either alone or in combination with metformin or a sulfonylurea), and insulin (either alone or in combination with metformin). A total of 8673 patients with type 2 diabetes were randomized in 10 double-blind, placebo- or active-controlled clinical safety and efficacy studies conducted to evaluate the effects of Nesina on glycemic control. The racial distribution of patients exposed to study medi-cation was 68% Caucasian, 15% Asian, 7% Black, and 9% other racial groups. The ethnic distribution was 30% Hispanic. Patients had an overall mean age of 55 years (range 21 to 80 years).
In patients with type 2 diabetes, treatment with Nesina pro-duced clinically meaningful and statistically significant improve-ments in A1C compared to placebo. As is typical for trials of agents to treat type 2 diabetes, the mean reduction in A1C with Nesina appears to be related to the degree of A1C elevation at baseline. Nesina had similar changes from baseline in serum lipids compared to placebo.
Patients with Inadequate Glycemic Control on Diet and Exercise A total of 1768 patients with type 2 diabetes participated in three double-blind studies to evaluate the efficacy and safety of Nesina in patients with inadequate glycemic control on diet and exercise. All three studies had a 4-week, single-blind, placebo run-in period followed by a 26-week randomized treatment period. Patients who failed to meet pre-specified hyperglycemic goals during the 26-week treatment periods received glycemic rescue therapy.
In a 26-week, double-blind, placebo-controlled study, a total of 329 patients (mean baseline A1C = 8%) were randomized to receive Nesina 12.5 mg, Nesina 25 mg, or placebo once daily. Treatment with Nesina 25 mg resulted in statistically significant improvements from baseline in A1C and fasting plasma glucose (FPG) compared to placebo at Week 26 (Table 3). A total of 8% of patients receiving Nesina 25 mg and 30% of those receiving placebo required glycemic rescue therapy. Improvements in A1C were not affected by gender, age, or baseline BMI.
In a 26-week, double-blind, active-controlled study, a total of 655 patients (mean baseline A1C = 8.8%) were randomized to receive Nesina 25 mg alone, pioglitazone 30 mg alone, Nesina 12.5 mg with pioglitazone 30 mg, or Nesina 25 mg with piogli-tazone 30 mg once daily. Coadministration of Nesina 25 mg with pioglitazone 30 mg resulted in statistically significant improve-ments from baseline in A1C and FPG compared to Nesina 25 mg alone and to pioglitazone 30 mg alone. A total of 3% of patients receiving Nesina 25 mg coadministered with pioglitazone 30 mg, 11% of those receiving Nesina 25 mg alone, and 6% of those receiving pioglitazone 30 mg alone required glycemic rescue.
Improvements in A1C were not affected by gender, age, or baseline BMI. The mean increase in body weight was similar between pioglitazone alone and Nesina when coadministered
with pioglitazone.In a 26-week, double-blind, placebo-controlled study, a total
of 784 patients inadequately controlled on diet and exercise alone (mean baseline A1C = 8.4%) were randomized to 1 of 7 treat-ment groups: placebo; metformin HCl 500 mg or metformin HCl 1000 mg twice daily, Nesina 12.5 mg twice daily, or Nesina 25 mg daily; Nesina 12.5 mg in combination with metformin HCl 500 mg or metformin HCl 1000 mg twice daily. Both coadmin-istration treatment arms (Nesina 12.5 mg + metformin HCl 500 mg and Nesina 12.5 mg + metformin HCl 1000 mg) resulted in statistically significant improvements in A1C and FPG when com-pared with their respective individual alogliptin and metformin component regimens (Table 5). Coadministration treatment arms demonstrated improvements in 2-hour postprandial glucose (PPG) compared to Nesina alone or metformin alon . A total of 12.3% of patients receiving Nesina 12.5 mg + metformin HCl 500 mg, 2.6% of patients receiving Nesina 12.5 mg + metformin HCl 1000 mg, 17.3% of patients receiving Nesina 12.5 mg, 22.9% of patients receiving metformin HCl 500 mg, 10.8% of patients receiving metformin HCl 1000 mg and 38.7% of patients receiving placebo required glycemic rescue.
Improvements in A1C were not affected by gender, age, race, or baseline BMI. The mean decrease in body weight was similar between metformin alone and Nesina when coadministered with metformin.
Combination Therapy Add-On Therapy to Metformin
A total of 2081 patients with type 2 diabetes participated in two 26-week double-blind, placebo-controlled studies to evaluate the efficacy and safety of Nesina as add-on therapy to metformin. In both studies, patients were inadequately controlled on met-formin at a dose of at least 1500 mg per day or at the maximum tolerated dose. All patients entered a 4-week, single-blind, placebo run-in period prior to randomization. Patients who failed to meet pre-specified hyperglycemic goals during the 26-week treatment periods received glycemic rescue therapy.
In the first 26-week, placebo-controlled study, a total of 527 patients already on metformin (mean baseline A1C = 8%) were randomized to receive Nesina 12.5 mg, Nesina 25 mg, or placebo. Patients were maintained on a stable dose of metformin (median dose = 1700 mg) during the treatment period. Nesina 25 mg in combination with metformin resulted in statistically significant improvements from baseline in A1C and FPG at Week 26, when compared to placebo. A total of 8% of patients receiving Nesina 25 mg and 24% of patients receiving placebo required glycemic rescue. Improvements in A1C were not affected by gender, age, baseline BMI, or baseline metformin dose. The mean decrease in body weight was similar between Nesina and placebo when given in combination with metformin.

June/July 2013 CareManagement 23
PharmaFacts for Case Managers
Add-On Therapy to a Thiazolidinedione In a 26-week, placebo-controlled study, a total of 493 patients
inadequately controlled on a thiazolidinedione alone or in combi-nation with metformin or a sulfonylurea (10 mg) (mean baseline A1C = 8%) were randomized to receive Nesina 12.5 mg, Nesina 25 mg, or placebo. Patients were maintained on a stable dose of pioglitazone (median dose = 30 mg) during the treatment period; those who were also previously treated on metformin (median dose = 2000 mg) or sulfonylurea (median dose = 10 mg) prior to randomization were maintained on the combination therapy dur-ing the treatment period. All patients entered into a 4-week sin-gle-blind, placebo run-in period prior to randomization. Patients who failed to meet pre-specified hyperglycemic goals during the 26-week treatment period received glycemic rescue therapy.
The addition of Nesina 25 mg once daily to pioglitazone therapy resulted in statistically significant improvements from baseline in A1C and FPG at Week 26, compared to placebo . A total of 9% of patients who were receiving Nesina 25 mg and 12% of patients receiving placebo required glycemic rescue. Improvements in A1C were not affected by gender, age, baseline BMI, or baseline pioglitazone dose. Clinically meaningful reductions in A1C were observed with Nesina compared to placebo regardless of whether subjects were receiving concomitant metformin or sulfonylurea (-0.2% placebo versus -0.9% Nesina) therapy or pioglitazone alone (0% placebo versus -0.52% Nesina). The mean increase in body weight was similar between Nesina and placebo when given in combination with pioglitazone.
Add-on Combination Therapy with Pioglitazone and Metformin In a 52-week, active-comparator study, a total of 803 patients inadequately controlled (mean baseline A1C = 8.2%) on a cur-rent regimen of pioglitazone 30 mg and metformin at least 1500 mg per day or at the maximum tolerated dose were randomized to either receive the addition of Nesina 25 mg or the titration of pioglitazone 30 mg to 45 mg following a 4-week single-blind, placebo run-in period. Patients were maintained on a stable dose of metformin (median dose = 1700 mg). Patients who failed to meet pre-specified hyperglycemic goals during the 52-week treat-ment period received glycemic rescue therapy. In combination with pioglitazone and metformin, Nesina 25 mg was shown to be statistically superior in lowering A1C and FPG compared with the titration of pioglitazone from 30 mg to 45 mg at Week 26 and at Week 52. Improvements in A1C were not affected by gender, age, race, or baseline BMI. The mean increase in body weight was similar in both treatment arms.
Add-On Therapy to a Sulfonylurea In a 26-week, placebo-controlled study, a total of 500 patients inadequately controlled on a sulfonylurea (mean baseline A1C = 8.1%) were randomized to receive Nesina 12.5 mg, Nesina 25 mg,
or placebo. Patients were maintained on a stable dose of glyburide (median dose = 10 mg) during the treatment period. All patients entered into a 4-week single-blind, placebo run-in period prior to randomization. Patients who failed to meet pre-specified hyper-glycemic goals during the 26-week treatment period received glycemic rescue therapy. The addition of Nesina 25 mg to gly-buride therapy resulted in statistically significant improvements from baseline in A1C at Week 26 when compared to placebo. Improvements in FPG observed with Nesina 25 mg were not statistically significant compared with placebo. A total of 16% of patients receiving Nesina 25 mg and 28% of those receiving placebo required glycemic rescue. Improvements in A1C were not affected by gender, age, baseline BMI, or baseline glyburide dose.
Add-On Therapy to Insulin In a 26-week, placebo-controlled study, a total of 390 patients inadequately controlled on insulin alone (42%) or in combination with metformin (58%) (mean baseline A1C = 9.3%) were random-ized to receive Nesina 12.5 mg, Nesina 25 mg, or placebo. Patients were maintained on their insulin regimen (median dose = 55 IU) upon randomization and those previously treated with insulin in combination with metformin (median dose = 1700 mg) prior to randomization continued on the combination regimen during the treatment period. Patients entered the trial on short-, intermedi-ate- or long-acting (basal) insulin or premixed insulin. Patients who failed to meet pre-specified hyperglycemic goals during the 26-week treatment period received glycemic rescue therapy.
The addition of Nesina 25 mg once daily to insulin therapy resulted in statistically significant improvements from baseline in A1C and FPG at Week 26, when compared to placebo (Table 11). A total of 20% of patients receiving Nesina 25 mg and 40% of those receiving placebo required glycemic rescue. Improvements in A1C were not affected by gender, age, baseline BMI, or base-line insulin dose. Clinically meaningful reductions in A1C were observed with Nesina compared to placebo regardless of whether subjects were receiving concomitant metformin and insulin (-0.2% placebo versus -0.8% Nesina) therapy or insulin alone (0.1% placebo versus -0.7% Nesina).
Patient Counseling Information • Inform patients of the potential risks and benefits of Nesina. • Patients should be informed that acute pancreatitis has been
reported during use of Nesina. Patients should be informed that persistent, severe abdominal pain, sometimes radiating to the back, which may or may not be accompanied by vomiting, is the hallmark symptom of acute pancreatitis. Patients should be instructed to promptly discontinue Nesina and contact their physician if persistent severe abdominal pain occurs.
• Patients should be informed that allergic reactions have been reported during use of Nesina. If symptoms of allergic reactions
continues on page 28

24 CareManagement June/July 2013
LitScan for Case Managers reviews medical literature and reports abstracts that are of particular interest to
case managers in an easy-to-read format. Each abstract includes information to locate the full-text article
if there is an interest. This member benefit is designed to assist case managers in keeping current with clinical
breakthroughs in a time-effective manner.
LitScan
Clin Infect Dis. 2013 Jun 4. [ePub ahead of print}
Incidence and timing of cancer in HIV-infected individuals following initiation of combination antiretroviral therapy.
Yanik EL, Napravnik S, Cole SR, et al.
BaCkgRouNd: Cancer is an important cause of morbidity and mortality in individuals infected with human immunodeficiency virus (HIV), but patterns of cancer incidence after combination antiretroviral therapy (aRT) initiation remain poorly character-ized. METHodS: We evaluated the incidence and timing of cancer diagnoses among patients initiating aRT between 1996 and 2011 in a collaboration of 8 uS clinical HIV cohorts. Poisson regression was used to estimate incidence rates. Cox regression was used to identify demographic and clinical characteristics associated with cancer incidence after aRT initiation. RESuLTS: at initiation of first combination aRT among 11,485 patients, median year was 2004 (interquartile range [IQR], 2000-2007) and median Cd4 count was 202±14 cells/mm3 (IQR, 61-338). Incidence rates for kaposi sarcoma (kS) and lymphomas were highest in the first 6 months after aRT initiation (P < .001) and plateaued thereafter, while incidence rates for all other cancers combined increased from 416 to 615 cases per 100,000 person-years from 1 to 10 years after aRT initiation (average 7% increase per year; 95% confidence interval, 2%-13%). Lower Cd4 count at aRT initiation was associated with greater risk of kS, lym-phoma, and human papillomavirus-related cancer. Calendar year of aRT initiation was not associated with cancer incidence. CoNCLuSIoNS: kS and lymphoma rates were highest immedi-ately following aRT initiation, particularly among patients with low Cd4 cell counts, whereas other cancers increased with time on aRT, likely reflecting increased cancer risk with aging. our results underscore recommendations for earlier HIV diagnosis followed by prompt aRT initiation along with ongoing aggressive cancer screening and prevention efforts throughout the course of HIV care.
Department of Epidemiology.
Hepatology. 2013 May 31. Epub ahead of print.
Neutralization resistance of hepatitis C virus can be overcome by recombinant human monoclonal antibodies.
Pedersen J, Carlsen TH, Prentoe J, et al.
BaCkgRouNd: Immunotherapy and vaccine development for hepatitis C virus (HCV) will depend on broadly reactive neutralizing antibodies. However, studies in infectious JFH1-based culture systems expressing patient derived Core-NS2 proteins have suggested neutralization resistance for specific HCV strains, in particular of genotype 2. To further examine this phenomenon, we developed a panel of HCV genotype 2 recombinants for testing of sensitivity to neutralization by chronic-phase patient sera and lead human monoclonal antibodies. The novel Core-NS2 recombinants, with patient derived genotype 2a (strain T9), 2b (strains dH8 and dH10), and 2c (strain S83) consensus sequences, were viable in Huh7.5 hepatoma cells without requirement for adaptive mutations, reaching HCV infectivity titers of 3.9-4.5 log10 focus-forming units per mL. In in vitro neutralization assays, we demonstrated that the novel genotype 2 viruses as well as prototype strains J6(2a) and J8(2b), all with authentic envelope proteins, were resistant to neutralization by genotype 2a, 2b, 2c, 2j, 2i, and 2q patient sera. These patient sera, however, had high titers of HCV-specific neutralizing antibodies, since they efficiently reduced the infectivity of J6(2a) and J8(2b) with deleted hypervariable region 1. The genotype 2a, 2b, and 2c viruses, found resistant to polyclonal patient sera neutralization, were efficiently neutralized by two lead human monoclonal antibodies, aR4a and HC84.26. CoNCLuSIoN: using novel 2a, 2b, and 2c cell culture systems, expressing authentic envelope proteins, we demonstrated resistance of HCV to patient-derived polyclonal high-titer neutralizing antibodies. However, the same genotype 2 culture viruses were all sensitive to human monoclonal HCV antibodies recognizing conformational epitopes, indicating that neutralization resistance of HCV can be overcome by applying recombinant antibodies. These findings have important implications for HCV immunotherapy and vaccine development.

June/July 2013 CareManagement 25
Copenhagen Hepatitis C Program (CO-HEP), Department of Infectious Diseases and Clinical Research Centre, Copenhagen University Hospital, Hvidovre, and Department of International Health, Immunology and Microbiology, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
AIDS. 2013 Jun 3. Epub ahead of print.
Liver stiffness measurement versus liver biopsy to predict survival and decompensations of cirrhosis among HIV/HCV-coinfected patients.
Macías J, Camacho a, Von Wichmann Ma, et al.
oBJECTIVE: To compare the prognostic performance of liver biopsy (LB)with that of liver stiffness measurement (LSM) to predict survival and liver decompensations among HIV/HCV-coinfected patients. dESIgN: Retrospective cohort study. METHodS: Cohort of 297 HIV/HCV-coinfected patients, who underwent aLB and LSM separated by 12 months or less, fol-lowed in ten Spanish tertiary care centers from december 2005 to december 2011 (median follow-up, 5 years; interquartile range, 4.2-5.4 years). LB were staged following the Scheuer’s score. LSM was obtained by hepatic transient elastometry. a survival analysis was carried out and the integrated discrimination improvement was computed to compare the ability of the survival models to predict outcomes. The incidence of death from any cause and of development of the first decompensation of cirrhosis were cal-culated. RESuLTS: overall mortality rate was 1.63 (95%CI: 1.06-2.49) per 100 person-years. The adjusted hazard ratio [aHR (95%CI)] of baseline fibrosis (per stage of fibrosis) was 1.52 (1.08-2.15, P = 0.017) and of LSM (per 5 kPa increase) 1.28 (1.12-1.46, P < 0.001). LMS including models yielded a performance 3.9% better than the LB-based models (P = 0.072). For the prediction of liver decompensations, the aHR (95%CI) of baseline fibrosis by LB (per stage of fibrosis) was 1.67 (1.15-2.43, P = 0.007) and of LSM (per 5 kPa increase) 1.37 (1.21-1.54, P < 0.001). LMS-based models yielded a performance 8.4% better than the LB-based models (P = 0.045). CoNCLuSIoN: LSM-based prediction achieves a similar yield than LB-based models to predict overall mortality in HIV/HCV-coinfected patients. Models including LSM couldpredict better liver decompensations than LB.
Hospital Universitario de Valme, Instituto de Biomedicina de Sevilla (IBiS), Seville, Spain; Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC), Hospital Universitario Reina Sofía, Cordoba, Spain; Hospital Donostia, San Sebastian, Spain; Hospital General Universitario de Valencia, Valencia, Spain; Fundació Lluita Contra la SIDA, University Hospital GermansTrias I Pujol, Universitat
Autònoma de Barcelona, Barcelona, Spain; Hospital Universitario Virgen Macarena, Seville, Spain; Complejo Hospitalario de Huelva, Huelva, Spain; Hospital de La Línea de la Concepción, Cadiz, Spain; Hospital Universitario Virgen de la Victoria, Malaga, Spain.
Transplant Proc. 2013 May;45(4):1540-1543.
Insulin resistance and insulin secretion in renal transplant recipients with hepatitis C.
uchida J, Iwai T, Machida Y, et al.
BaCkgRouNd: Several reports have suggested an associa-tion between hepatitis C virus (HCV) infection and new-onset diabetes after transplantation (NodaT). NodaT is a common complication after renal transplantation, and it has been associ-ated with increased long-term morbidity and mortality. HCV-positive recipients may have abnormal glucose metabolism, even though NodaT has never been previously diagnosed. The aim of this study was to analyze the pathogenic factors responsible for glucose metabolism in a series of HCV-positive renal transplant recipients. METHodS: The study population comprised 16 renal transplant patients who received their grafts from deceased or liv-ing donors with anti-HCV antibodies. HCV-negative transplant recipients were individually matched with these HCV-positive recipients by year of transplantation, sex, age, serum creatinine levels, and type of calcineurin inhibitors. None of the patients had been diagnosed with diabetes. Insulin secretion and insu-lin resistance were determined by a 75-g oral glucose tolerance test (ogTT) and compared between the 2 groups. Categories of glucose tolerance were defined according to World Health organization criteria. RESuLTS: glucose intolerance (impaired fasting glucose, impaired glucose tolerance, diabetes mellitus) as assessed by ogTT was detected in 7 of the HCV-positive recipients (43.8%) and 3 of the HCV-negative recipients. The homeostasis model assessment of insulin resistance was greater in the HCV-positive recipients than in the HCV-negative recipients. The homeostasis model assessment of β-cell function was higher in the HCV-positive recipients than in the HCV-negative recipients. CoNCLuSIoNS: The frequency of glucose intolerance tended to be higher in HCV-positive recipients. Furthermore, insulin resis-tance was greater and insulin secretion higher in HCV-positive recipients, which indicated that the increase in insulin secretion compensated for insulin resistance observed in these patients. However, HCV-positive renal transplant recipients may ultimately develop NodaT as this compensation diminishes with time.
Department of Urology, Osaka City University Graduate School of Medicine, Osaka, Japan.
t

26 CareManagement June/July 2013
LitScanf o r C a s e M a n a g e r s
Am J Cardiol. 2013 May 28. Epub ahead of print.
Effectiveness of moxonidine to reduce atrial fibrillation burden in hypertensive patients.
deftereos S, giannopoulos g, kossyvakis C, et al.
BaCkgRouNd: There is substantial evidence that the auto-nomic system plays an important part in the pathogenesis of atrial fibrillation (aF). It appears that, although some patients have a preponderantly sympathetic or vagal overactivation leading to aF, a combined sympathovagal drive is most commonly responsible for aF triggering. The purpose of this hypothesis-generating study was to test whether moxonidine, a centrally acting sympathoin-hibitory agent, on top of optimal antihypertensive treatment, can lead to a decrease in aF burden in hypertensive patients with par-oxysmal aF. This was a prospective, double-blind, 1-group, cross-over study. Hypertensive patients with paroxysmal aF sequentially received treatment with placebo and moxonidine for two 6-week periods, respectively. The change in aF burden (measured as min-utes of aF per day in three 48-hour Holter recordings) between the 2 treatment periods was the primary outcome measure. Fifty-six patients (median age 63.5 years, 35 men) were included. during moxonidine treatment, aF burden was reduced from 28.0 min/day (interquartile range [IQR] 15.0 to 57.8) to 16.5 min/day (IQR 4.0 to 36.3; P < 0.01). European Heart Rhythm association symptom severity class decreased from a median of 2.0 (IQR 1.0 to 2.0) to 1.0 (IQR 1.0 to 2.0; P = 0.01). Systolic blood pressure levels were similar in the 2 treatment periods, whereas diastolic blood pressure was lower (P < 0.01) during moxonidine treatment. The most frequent complaint was dry mouth (28.6%). No seri-ous adverse events were recorded. In conclusion, treatment with moxonidine, a centrally acting sympathoinhibitory agent, results in reduction of aF burden and alleviation of aF-related symptoms in hypertensive patients with paroxysmal aF.
Department of Cardiology, Athens General Hospital “G. Gennimatas,” Athens, Greece.
Am J Hypertens. 2013 Jun 1. Epub ahead of print.
Impact of miscuffing during home blood pressure measurement on the prevalence of masked hypertension.
Mourad JJ, Lopez-Sublet M, aoun-Bahous S, et al.
BaCkgRouNd: Masked hypertension has been associated
with obesity. However, because most studies do not mention the specific cuff size used for home measurements, masked hyperten-sion prevalence may have been overestimated in obese patients because of undersized cuffs. In this prospective, observational study, the effect of miscuffing on hypertension status was evalu-ated in patients with large arms. METHodS: Fifty-three patients with an upper-arm circumference > 33 cm, undergoing treatment for mild-to-moderate hypertension, took 2 sets of home blood pressure (BP) measurements (standard vs large cuff) using the validated Microlife BP a100 Plus automated device. RESuLTS: Mean BP was 143/85 mm Hg at the office using a large cuff, 141/84 mm Hg at home using a standard cuff, and 134/80 mm Hg at home using a large cuff. Standard vs large cuff home BP mean differences were 6.9 mm Hg (95% confidence interval (CI) = 4.7-9.2; P < 0.0001) for systolic BP and 4 mm Hg (95% CI = 2.4-5.5; P < 0.0001) for diastolic BP. Hypertension status differed significantly between standard vs. large cuffs: sustained hypertension (56.6% vs 41.5%, respectively; P = 0.002), con-trolled hypertension (20.8% vs 28.3%, respectively; P = 0.04), white coat hypertension (7.5% vs 22.6%, respectively; P = 0.002), masked hypertension (15.1% vs 7.5%, respectively; P = 0.04). CoNCLuSIoNS: In patients with large arms, use of an appropriately sized large cuff for home BP measurements led to a 2-fold reduction in masked hypertension. Regarding clinical and epidemiological implications, future studies investigating masked hypertension should specify cuff size for home BP measurements. The low market availability and increased cost of large cuffs should also be addressed.
Excellence Center for Hypertension, CHU Avicenne, AP-HP, Bobigny, France.
Circ Heart Fail. 2013 May 23. Epub ahead of print.
Risk-stratification and transplant benefit in children listed for heart transplant in the United States.
Singh TP, almond CS, Piercey g, gauvreau k.
BaCkgRouNd: The sickest children among those listed for heart transplant (HT) are also at higher risk of post-transplant mortality. We hypothesized that transplant benefit, defined as percent reduction in risk of 1-y mortality on receiving HT, increases with higher risk of wait-list mortality. METHodS aNd RESuLTS: We analyzed all children < 18 y old listed for first HT in the uS between 07/2004 and 12/2010. We developed a model for 90-day wait-list mortality (or removal due to dete-

June/July 2013 CareManagement 2727 CareManagement June/July 2013
rioration) and stratified listed children into deciles based on their risk of wait-list mortality. Listed children were followed for 1 y to assess cumulative 1-y wait-list mortality among the 10 risk-groups. We developed a model for 1 y post-transplant mortality to estimate the risk of post-transplant mortality for children in each risk-group. of 2979 listed children, 15% reached the wait-list end-point within 90 days and 18% within 1 y of 2034 HT recipi-ents, 6.8% died within 90 days and 10.8% within 1 y. The risk of 90-day wait-list mortality increased progressively from 2.4% to 51.6%% from the first to the tenth risk-decile. Transplant benefit increased progressively across the wait-list risk-groups (P < 0.001 for trend). However, transplant benefit for children in the top 5% of risk (7.4%) was lower than that for children in the 91st to 95th percentile of risk (10.3%). CoNCLuSIoNS: Sicker children on the wait-list benefit more from HT unless the post-transplant mortality is predicted to be very high. Whether consideration of transplant benefit in allocation policy can improve overall survival among listed children requires further analysis.
Children’s Hospital Boston, Harvard Medical School, Boston, MA.
J Clin Oncol. 2013 Jun 3. Epub ahead of print.
Underuse of hospice care by Medicaid-insured patients with stage IV lung cancer in New York and California.
Mack JW, Chen k, Boscoe FP, et al.
PuRPoSE: Medicare patients with advanced cancer have low rates of hospice use. We sought to evaluate hospice use among patients in Medicaid, which insures younger and indi-gent patients, relative to those in Medicare. PaTIENTS aNd METHodS: using linked patient-level data from California (Ca) and New York (NY) state cancer registries, state Medicaid programs, NY Medicare, and Ca Surveillance, Epidemiology, and End Results-Medicare data, we identified 4,797 Ca Medicaid patients and 4,001 NY Medicaid patients ages 21 to 64 years, as well as 27,416 Ca Medicare patients and 16,496 NY Medicare patients ages ≥ 65 years who were diagnosed with stage IV lung cancer between 2002 and 2006. We evaluated hospice use, timing of enrollment, and location of death (inpatient hospice; long-term care facility or skilled nursing facility; acute care facility; home with hospice; or home without hospice). We used multiple logis-tic regressions to evaluate clinical and sociodemographic factors associated with hospice use. RESuLTS: although 53% (Ca) and 44% (NY) of Medicare patients ages ≥ 65 years used hospice, fewer than one-third of Medicaid-insured patients ages 21 to 64 years enrolled in hospice after a diagnosis of stage IV lung cancer
(Ca, 32%; NY, 24%). a minority of Medicaid patient deaths (Ca, 19%; NY, 14%) occurred at home with hospice. Most Medicaid patient deaths were either in acute-care facilities (Ca, 28%; NY, 36%) or at home without hospice (Ca, 39%; NY, 41%). Patient race/ethnicity was not associated with hospice use among Medicaid patients. CoNCLuSIoN: given low rates of hospice use among Medicaid enrollees and considerable evidence of suffering at the end of life, opportunities to improve palliative care delivery should be prioritized.
Dana-Farber Cancer Institute; Children’s Hospital, Boston, MA; New York State Department of Health, State Cancer Registry and Office of Quality and Patient Safety, Albany, NY.
Arch Bronconeumol. 2013 Jan;49(1):10-14.
Home intervention and predictor variables for rehospitalization in chronic obstructive pulmonary disease exacerbations.
Jurado gámez B, Feu Collado N, Jurado garcía JC, et al.
BaCkgRouNd: Chronic obstructive pulmonary disease (CoPd) exacerbation increases mortality and resources used associated with hospitalization. We studied whether early home monitoring reduces the rate of readmission and if there are any predictor variables. PaTIENTS aNd METHodS: We per-formed a prospective, controlled, parallel-group study in patients who were hospitalized for CoPd. Patients whose residence was within less than 15km from the hospital were assigned to an inter-ventional group (home visits by nurses about 48-72hours after discharge), the remainder were assigned to a conventional care group. The rate of rehospitalization within the first month was compared between the two groups, as well as those variables that showed a predictive capability. RESuLTS: Seventy-one patients were included: 35 in the conventional care group and 36 in the interventional group. In the latter, the treatment was modified in 13 patients (36%). The hospital readmission rate was 17%, which was similar in both groups (P = .50). For every 5-year increase in age, the risk for readmission was 2.54 (95%CI, 1.06-5.07) and for each increase of 10mmHg in PaCo2, the risk of readmission was 8.34 (95%CI, 2.43-18.55). CoNCLuSIoNS: Early home monitoring did not decrease the readmission rate during the first month. older age and high PaCo
2 are factors that identify the
group with a high risk for rehospitalization.
Servicio de Neumología, Hospital Universitario Reina Sofía, Córdoba, España.

28 CareManagement June/July 2013
This attitude is also reflected in the HealthLeaders Media Industry Survey 2013, in which 92% of respondents identified reduced reimbursements as the number one threat to their organizations, while citing patient satisfaction/experience and clinical quality as their top two priorities for the next 3 years, at 54% and 48%, respectively. Health care leaders are clearly worried about finances, but are still focusing their attention on improving quality.
In response, hospitals across the country have been hustling to thwart readmissions. Some are giving out free prescriptions to patients who cannot afford them. Others are making checkup appointments and dispatching nurses to patients’ homes.
Last month, Jonathan Blum, a top Medicare official, told a US Senate committee that the national readmission rate dropped to 17.8% in the last 3 months of 2012 “after fluctuating between 18.5% and 19.5% for the past 5 years.” This decrease is an early sign that our payment and delivery reforms are having an impact.
The government is looking at the number of heart attack, heart failure, and pneumonia patients who return to the hospital within 30 days of discharge. Hospitals with more readmissions than Medicare expected given their mix of patients are penalized by losing up to 1% of their regular payments. The maximum penalty ramps up to 2% starting this October and grows to 3% the following year.
Hospital readmissions are only going to decrease with effective care coordination. Without effective care management, patients will fall through the cracks and are readmitted to the hospital. Case managers must develop sophisticated tracking systems to follow the patients who have been hospitalized. With appropriate care management interventions, hospital readmissions can continue to decrease. By managing hospitalized patients, case managers can demonstrate their worth and improve the health care delivery system.
Editor-in-Chief [email protected]
accm: improving case management practice through education
Care Coordination and Hospital Readmissions continued from page 3
Certified Case Manager News • Certified Case Manager News • Certified Case Manager News
Medicare readmissions Drop; reasons UnclearA new study finds that US hospitals recorded about 70,000 fewer cases than expected of Medicare patients being readmitted for inpatient care last year. Good news for sure, but the reasons are unclear. The results were published in the online academic journal Medicare & Medicaid Research Review. n
(including skin rash, hives, and swell-ing of the face, lips, tongue, and throat that may cause difficulty in breathing or swallowing) occur, patients should be instructed to discontinue Nesina and seek medical advice promptly. Patients should be informed that postmarketing reports of liver injury, sometimes fatal, have been reported during use of Nesina. If signs or symptoms of liver injury occur, patients should be instructed to discontinue Nesina and seek medical advice promptly.
• Inform patients that hypoglycemia can occur, particularly when an insulin secretagogue or insulin is used in com-bination with Nesina. Explain the risks, symptoms, and appropriate management of hypoglycemia.Instruct patients to take Nesina only as prescribed. If a dose is missed, advise patients not to double their next dose.
• Instruct patients to read the Medication Guide before starting Nesina therapy and to reread each time the prescription is refilled. Instruct patients to inform their healthcare provider if an unusual symp-tom develops or if a symptom persists or worsens.
PharmaFacts for Case Managers
continued from page 23
Pediatric Bacterial Sinusitis Guidelines IssuedThe American Academy of Pediatrics revamped the guidelines for diagnosing and managing pediatric bacterial sinusitis. Imaging to differentiate bacterial from viral sinusitis is no longer recommended as a diagnostic tool, and use of antibiotics should be reserved for only the worst cases. Previously updated in 2001, these new guidelines designate certain criteria to diagnosis acute upper
respiratory tract infection including persistent illness, worsening cough, and severe onset of symptoms. The guideline authors noted that corticosteroids may more rapid resolve symptoms while decongestants and nasal sprays are similarly effective at 14 days. Mucolytic agents were no more helpful than placebo in lessening symptoms. n
continued from page 5

hoW to contact Us
Editor-in-Chief: Gary S. Wolfe, RN, CCM 831-443-6847; email: [email protected]
Executive Editor: Jennifer Maybin, MA, ELS 203-454-1333, ext. 3; email: [email protected]
Publisher/President: Howard Mason, RPH, MS 203-454-1333, ext. 1; e-mail: [email protected]
Art Director: Laura D. Campbell 203-256-1515 e-mail: [email protected]
Subscriptions: 203-454-1333 Website: www.academyCCM.org
CareManagementOfficial JOurnal Of The academy Of cerTified case managers
phone: 203-454-1333; fax: 203-227-9495 Website: www.academyccm.org
Executive Vice President: Gary S. Wolfe, RN, CCM 831-443-6847; email: [email protected]
Member Services: 203-454-1333, ext. 3 e-mail: [email protected]
Vol. 19, No. 3 June/July 2013. CareManagement (ISSN #1531-037X) is published electronically six times a year, February, April, June, August, October and December and its contents copyrighted by Mason Medical Communi ca tions, Inc., 10 Covlee Dr., Westport, CT 06880; Tel: 203-454-1333; Fax: 203-227-9495.
June/July 2013 CareManagement 29
join/renew ACCM online at www.academyCCM.org
refer A ColleAgue to ACCM
Help your colleagues maintain their certification by referring them to ACCM for their continuing education needs. They can join ACCM at www.academyCCM.org or by mailing or faxing the Membership Application on the next page to ACCM.
Why join ACCM? Here are the answers to the most commonly asked questions about ACCM Membership:
Q: Does membership in ACCM afford me enough CEUs to maintain my CCM or CDMS certification?
A: If you submit all of the CEU home study programs offered in CareManagement, you will accumulate 90 CEUs every 5 years.
Q: Are CEUs available online?A: Yes, ACCM members may mail exams or take them online. When
taking the exam online, you must print your certificate after successfully completing the test. This is a members only benefit. If mailing the exam is preferred, print the exam from the PDF of the issue, complete it, and mail to the address on the exam form.
Q: Where can I get my membership certificate?A: Print your membership certificate instantly from the website or click
here. Your membership is good for 1 year based on the time you join or renew.
Q: How long does it take to process CEU exams?A: Online exams are processed instantly. Mailed exams are normally
processed within 4 to 6 weeks.
Q: Do CEU programs expire?A: Continuing education programs expire in 12 months.
Q: Is your Website secure for dues payment?A: ACCM uses the services of PayPal, the nation’s premier payment processing organization. No financial information is ever transmitted to ACCM.
application on next page
ACCMAcademy of Certified Case Managers

First Name Middle Name Last Name
Home Address
City State Zip
Telephone Fax e-mail (required)
Certification ID #_____________________ (ACCM mailings will be sent to home address)
Practice Setting:Which best describes your practice setting?
q Independent/Case Management Company q HMO/PPO/MCO/InsuranceCompany/TPA
q Rehabilitation Facility q Hospital
q Medical Group/IPA q Home Care/Infusion
q Hospice q Academic Institution
q Consultant q Other: _____________________________
Join ACCM todAy!q 1 year: $120 (year begins at time of joining)
q Check or money order enclosed made payable to: Academy of Certified Case Managers. Mail check along with a copy of application to: Academy of Certified Case Managers, PO Box 210, Green’s Farms, CT 06838-0210.
q MasterCard q Visa q American Express If using a credit card you may fax application to: 203-227-9495
Card # ________________________________________ Exp. Date: ______________ Security Code: _______________
Person’s Name on Credit Card: ____________________________Signature: ________________________________
Credit Card Billing Address: ______________________________________________________
City: ________________________________ State: _________ Zip: ________________________________________
s
Do not use this application after December 31, 2013.
Date
ACCMAcademy of Certified Case Managers
Membership Application
s
!
join/renew ACCM online at www.academyCCM.org
q I wish to become a member.
For office use only:__________________Membership #__________________ Membership expiration__________________

I N S I D E t h I S I S S U E
We have gone digital! PDFs of the issue are available on the ACCM website
at www.academyccm.org. To avoid interruption in receipt of the journal,
click here to add your e-mail address now. You’ll receive notification by e-mail
when the next issue is available.
Continue taking CE tests online or by mail using your ACCM membership ID.
What you need to know about your subscription!
6 CareManagement June/July 2012
Federal Contractors May Soon Face Changes to Hiring GoalsDOL’s proposed rule aims to improve job opportunities for people with disabilities
NEWS FROM
CERTIFICATION OF DISABILITY MANAGEMENT SPECIALISTS COMMISSION
T he month of July reminds most people of upcoming Independence Day celebrations, school vacations,
summer getaways, and fun! If you are involved with CARF, it is also a reminder that the new 2012 Standards Manuals are used on all surveys from July 1, 2012, through June 30, 2013. Case managers who work with workers compensation cases, attorneys, courts, and so forth will be interested in our Independent Evaluation Services (IES) standards—a new set of standards in Medical Rehabilitation.
If you work with individuals who, because of court order or a long-standing case, may be required to have an independent evaluation com-pleted, these new standards should be reviewed. Until now, there were no Standards that reviewed this type of work. It is an area in which there is wide diversity among individuals providing evaluations and their quali-fications, as well as in what is included in the evaluations and how they are recorded.
CARF was approached by a vari-ety of providers and institutions to create a group to review these issues. CARF held sessions and focus groups to explore this topic. An International Advisory Standards Committee was held in the summer of 2011, and field review was completed in the fall of 2011. The new Independent Evaluation Services Standards were printed in the 2012 CARF Medical Rehabilitation Standards Manual.
Independent Evaluation Services coordinate and facilitate objective, unbiased evaluations based on the following:
Effective and efficient use of resources
implications
stakeholders
In view of the multiple stakeholders involved, the Independent Evaluation Services support transparency and exchange of information.
Independent evaluations may be completed by a variety of professionals who are not involved in the care of the person served for the purpose of clari-fying clinical and case issues. The deliv-ery of Independent Evaluation Services may occur in a variety of settings including, but not limited to, a health care environment, a private practice, a community-based setting, or a private or group residence.
As case managers, you may interact with independent evaluators on behalf of your clients. A key in this description is that IES supports transparency and exchange of information. There are multiple standards that also address how the evaluation services learn about
uniqueness of the person being evalu-ated including transportation needs, cultural diversity, need for translation, adaptive equipment, etc. The more an evaluation services can meet the needs of the individual being evaluated, the better the chance for results that will be meaningful and useful for those requesting the evaluation to better inform decisions about need, benefits, and compensation.
These Standards will be in place beginning July 1, 2012. CARF has received a mandate from an insur-ance company that beginning July 1, 2012, will only use CARF-accredited Independent Evaluation Services pro-viders. Their strategy is to decrease fraud and abuse, better meet the needs of their clients, and also have a stan-dard in place that requires interaction with them as stakeholders.
For more information, please con-tact Chris MacDonell at [email protected].
The 2013 CARF Medical Rehabilitation Standards Manual will also feature a new Brain Injury and Interdisciplinary Pain Rehabilitation program Standard. The field reviews were well received for both sets of stan-dards. CARF staff are now reviewing the comments and making appropriate changes suggested by field reviewers. These two sets of Standards will be available in January 2013 and will go into effect July 1, 2013. Watch this col-umn for more information as we move through the review of these Standards.
Have a great summer! CM
June/July 2012 CareManagement 7
CARF’s 2012 Standards ManualBy Chris MacDonell, Managing Director, Medical Rehabilitation and International Aging Services/Medical Rehabilitation
Independent Evaluation Services support transparency and
exchange of information.
F ederal contractors and subcontractors will likely face significant changes to hiring goals if a proposed new rule by the US Department of Labor (DOL) to improve job opportunities for Americans with disabilities is
enacted, which is widely anticipated to happen later this year. The proposed rule would require federal contractors and subcontractors to set a 7% hiring goal for employing people with disabilities, among other requirements.
The proposal, which was published in the December 9, 2011, Federal Register, is intended to strengthen the affirma-tive action requirements established in Section 503 of the Rehabilitation Act of 1973 obligating federal contractors and subcontractors to ensure equal employment opportunities for qualified workers with disabilities. Proposed changes include specific actions contractors must take in recruiting, training, record keeping, and disseminating policy—the same actions currently required to promote workplace equality for women and minorities.
Christine Moranda, LSW CDMS CCM, chair-elect of the Certification of Disability Management Specialist (CDMS) Commission, says that CDMS members are well positioned to assist federal contractors and subcontractors with regulation changes, if enacted. “I think that CDMS members can play a role on a number of levels, whether they work for one of these [contractor] compa-
nies or as outside consultants,” she says. Moranda, who is manager of disability services at
OhioHealth in Columbus, OH, stresses that CDMS certifica-tion lends expertise to training contractors, gathering needed information, and serving as liaison between contractors and people with disabilities. She points to two areas of the pro-posed rule where a CDMS can play a significant role: reason-able accommodation and disability sensitivity.
Reasonable accommodation. A new section in the Section 503 rule requires a contractor to develop and implement
written procedures for processing requests for reasonable accommodation. To improve accountability, the proposed rule would ensure annual self-reviews of employers’ recruitment and outreach efforts and enhance data collection and record-keeping requirements.
Leslie Wilson, MS, president and CEO of Wilson Resources, Inc., Palmetto, FL, (www.wilres.com) rules outline minimum elements to be included in the reasonable accom-modation procedures. These include a responsible person’s contact infor-mation, requests for accommodation, written confirmation of request, time-line for processing, process description,
supporting medical documentation, and denial of reasonable accommodation and confidentiality.
Disability sensitivity and self-identification. The proposed revisions require that a contractor invite all applicants to vol-untarily self-identify as people with disabilities whenever the applicant applies for or is considered for employment. The invitation may be included with the application materials, but must be separable or detachable from the job application. Wilson says that DOL’s Office of Federal Contract Compliance Programs (OFCCP) believes that these “significant, substantive changes” to the contractors’ responsibilities will:
monitor the contractor’s hiring and selection process with respect to people with disabilities
with disabilities who apply for jobs with contractors-
ness of the contractor’s recruitment efforts over time and to refine and improve a contractor’s recruitment strate-gies where necessary
According to the OFCCP, although Section 503 regulations have been in place for decades, the current unemployment
continues on page 28
CARF…THE REHABILITATION ACCREDITATION COMMISSION
NEWS FROM
IMPROVING PR ACTICE THROUGH EDUCATIONIMPROVING PR ACTICE THROUGH EDUCATION
OFFICIAL JOURNAL OF THE ACADEMY OF CERTIFIED CASE MANAGERS& THE COMMISSION FOR CASE MANAGER CERTIFICATION

Official JOurnal Of The academy Of cerTified case managers
PO Box 210, Greens Farms, CT 06838-0210 Tel: 203-454-1333 • Fax: 203-454-1344
© Mason Medical Communicatons, Inc. 2013
CareManagement