arbor rehabilitation and healthcare services, inc. · herniated nucleus pulposus (herniated disk)...
TRANSCRIPT

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 1
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
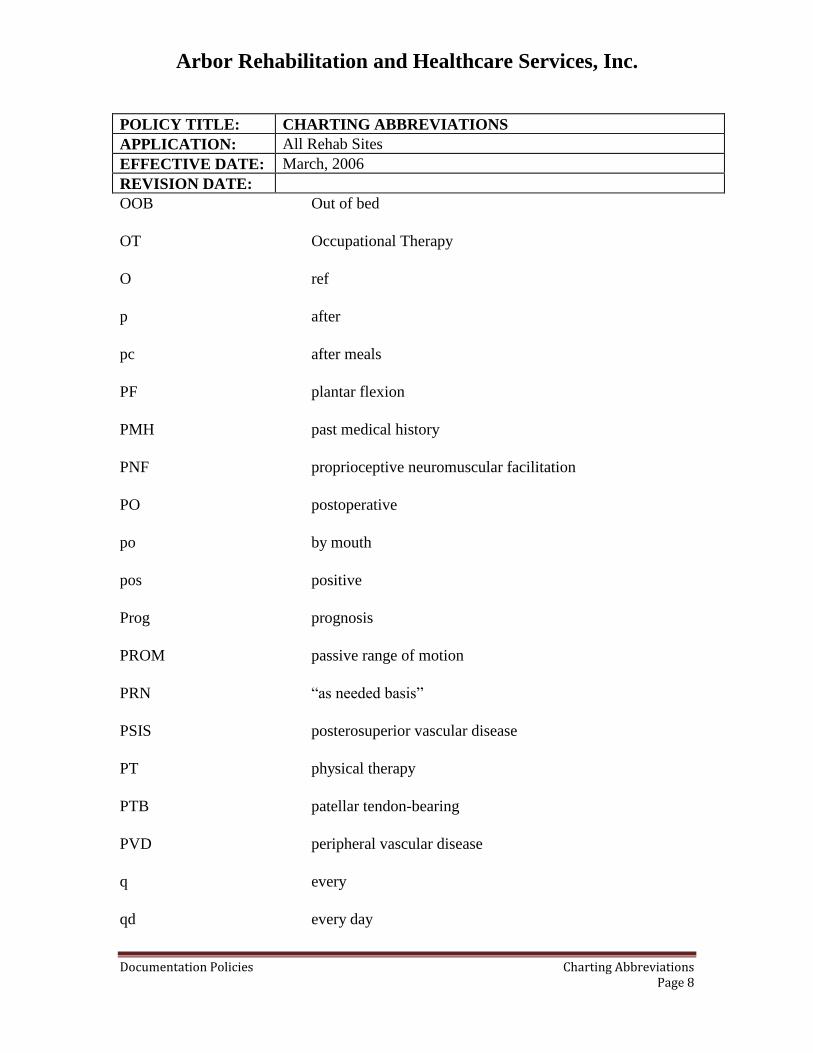
The following list of commonly used abbreviations may be used in the documentation of
patient care. Abbreviations save time, but their excessive use should be discouraged
because of the wide variations in meaning. When ambiguity is likely, terms should be
spelled out to make the documentation more accessible to others.
A
AAROM
ABD
ac
AC>BC
AD
ADD
ADJ
ADM
ADL
AE
AFO
AK
AKA
AM
amb
AMP
Assessment (SOAP note)
Active assisstive range of motion
Abduction
Before meals
Air conduction greater than bone conduction
Right ear (auris dextra)
Adduction
Adjustable
Admission
Activities of daily living
Above elbow
Ankle-foot orthosis
Above knee
Above knee amputation
Morning
Ambulation, ambulate
Amputee

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 2
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
A&O
AROM
AS
AU
Aud
Aud Haluc
audio
B
B>A
bal
B&B
BC>AC
BE
b.i.d
bil
b.i.w.
BK
BKA
BLE
Alert and oriented
Range of motion
Left ear
Both ears (aures unitas)
Auditory
Auditory hallucinations
Audiogram
Both
Bone greater than air
Balance
Bowel and bladder
Bone conduction greater than air conduction
Below elbow
Twice daily
Bilateral
Twice a week
Below knee
Below-knee amputation
Bilateral lower extremities

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 3
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
BP Blood pressure
B.R.
BUE
c
C
Ca
CAD
CAE
cath
CBS
CC
CHD
CHF
CHI
C/o
COPD
COTA
CPM
C.P.T.
Bathroom
Bilateral upper extremities
With
Complaint
Carcinoma
Coronary artery disease
Complete audiometric evaluation
Catheter
Chronic brain syndrome
Chief complaint
Coronary heart disease
Congestive heart failure
Closed head injury
Complains of
Chronic obstructive pulmonary disease
Certified occupational therapy assistant
Continuous passive motion
Chest physical therapy

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 4
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
CVA
d/c
Decr
deg
DF
DI
dias.
DJD
DOB
DOI
DTR
Dx
ed
EENT
elev
end
ENT
Eval
EWHO
Cerebral Vascular Accident
Discharged
Decreased
Degenerative
Dorisflexion
Diabetes insipidus
Diastolic
Degenerative joint disease
Date of birth
Date of injury
Deep tendon reflexes
Diagnosis
Education
Eye, ear, nose, and throat
Elevation
Endurance
Ear, nose, and throat
Evaluation
Elbow wrist hand orthosis

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 5
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
EXT
EXT. ROT.
F
FAM
FL
fl. dr.
fl. oz.
flds
flex
fluoro
F.
FO
Ft.
Func
FWB
Fx
HPB
HEENT
HNP
Extension
External Rotation
female
family
Fluid
Fluid dram
Fluid ounce
Fluids
Flexion
Fluoroscopy
Fairly nourished
Foot orthosis
Foot
Fuction
Full weight-bearing
Fracture
High blood pressure
Head, eyes, ears, nose, and throat
Herniated nucleus pulposus (herniated disk)

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 6
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
HOB Head of Bed
HP Hot Pack
H/O History of
H&P
HR
HVGS
Hx
IDDM
Inc
inf
INJ
Int
I&O
IR
Jt.
LBP
lig
LLE
LOH
LOS
LS
History and Physical
Heart rate
High-voltage galvanic stimulation
History
Insulin-dependent diabetes mellitus
Increased
Inferior
Injury
Internal
Intake and output
Internal rotation
Joint
Low back pain
Ligament
Left lower extremity
Loss of hearing
Length of stay
Lumbosarcal

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 7
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
Lt.
LTM
LUE
M
MAFO
Max
MI
Min
mo
mod
NA
NDT
neg
nl
NPO
N/S
Nsg
NWB
OA
OBS
Left
Long Term Memory
Left upper extremity
Male
Molded ankle-foot orthosis
Maximal
Myocardial infraction
Minimal
Months
Moderate
Not applicable
Neural developmental treatment
Negative
Normal
Nothing by mouth
Normal saline
Nursing
Non-weight bearing
Osteoarthritis
Organic brain syndrome
Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 8
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
OOB
OT
O
p
pc
PF
PMH
PNF
PO
po
pos
Prog
PROM
PRN
PSIS
PT
PTB
PVD
q
qd
Out of bed
Occupational Therapy
ref
after
after meals
plantar flexion
past medical history
proprioceptive neuromuscular facilitation
postoperative
by mouth
positive
prognosis
passive range of motion
“as needed basis”
posterosuperior vascular disease
physical therapy
patellar tendon-bearing
peripheral vascular disease
every
every day
Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 9
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
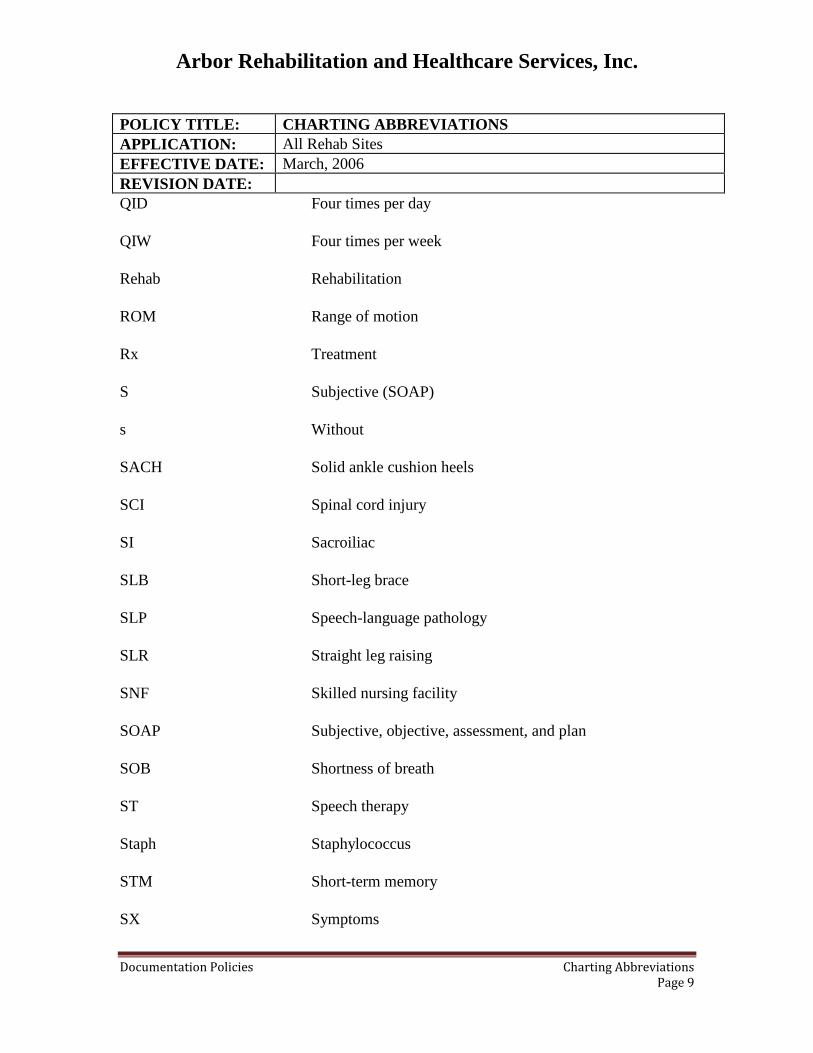
QID
QIW
Rehab
ROM
Rx
S
s
SACH
SCI
SI
SLB
SLP
SLR
SNF
SOAP
SOB
ST
Staph
STM
SX
Four times per day
Four times per week
Rehabilitation
Range of motion
Treatment
Subjective (SOAP)
Without
Solid ankle cushion heels
Spinal cord injury
Sacroiliac
Short-leg brace
Speech-language pathology
Straight leg raising
Skilled nursing facility
Subjective, objective, assessment, and plan
Shortness of breath
Speech therapy
Staphylococcus
Short-term memory
Symptoms
Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 10
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
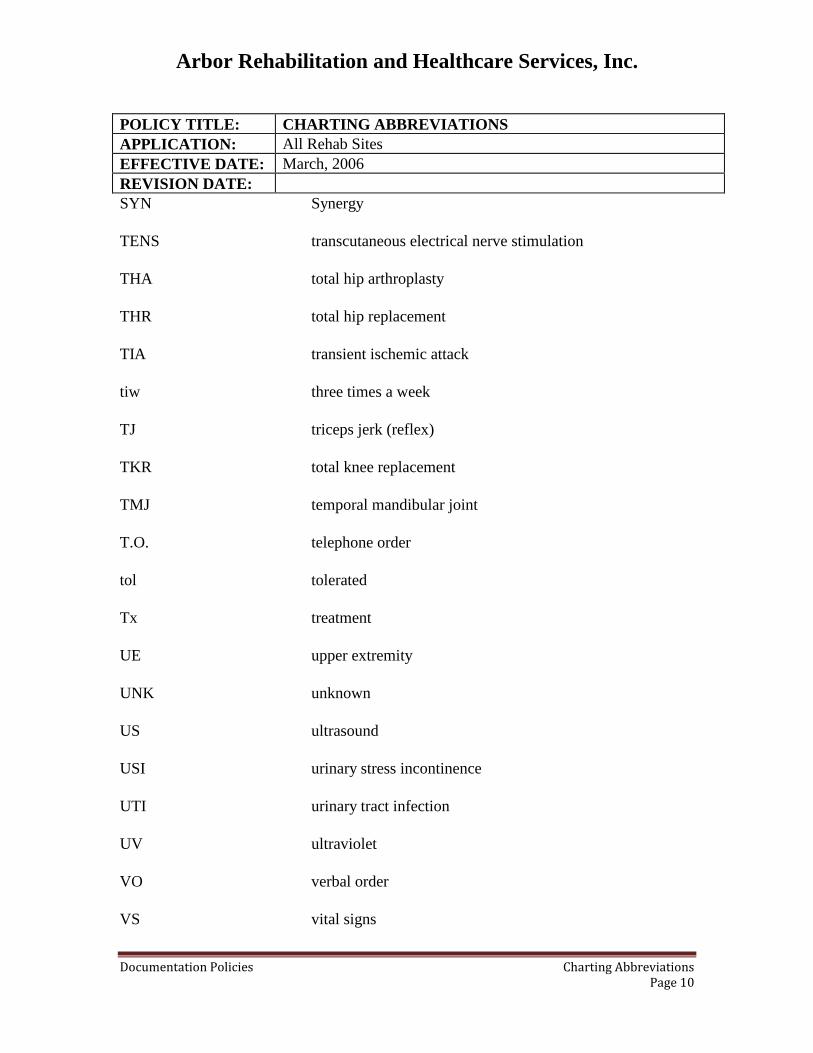
SYN
TENS
THA
THR
TIA
tiw
TJ
TKR
TMJ
T.O.
tol
Tx
UE
UNK
US
USI
UTI
UV
VO
VS
Synergy
transcutaneous electrical nerve stimulation
total hip arthroplasty
total hip replacement
transient ischemic attack
three times a week
triceps jerk (reflex)
total knee replacement
temporal mandibular joint
telephone order
tolerated
treatment
upper extremity
unknown
ultrasound
urinary stress incontinence
urinary tract infection
ultraviolet
verbal order
vital signs

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Charting Abbreviations Page 11
POLICY TITLE: CHARTING ABBREVIATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE:
WB
WC
WFL
wk
WN
WNL
w/o
WP
wt
YO
Yr
Weight-bearing
Wheelchair
Within functional limits
Week
Well-nourished
Within normal limits
Without
Whirlpool
Weight
Years old
year

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Clarification Orders Page 1
POLICY TITLE: CLARIFICATION ORDERS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December, 2014
POLICY
Clarification orders will be obtained on all residents prior to initiating treatment.
PURPOSE
To provide a formal review of the specific treatment plan prior to initiating treatment
services and ensure physician authorization of planned treatments.
PROCESS
1. Clarification orders are obtained either by writing the order out on a telephone
order slip or using facility based electronic medical record system, per facility
directives.
2. Telephone orders completion- be sure to include the following:
A. Type of service: PT, OT, SLP
B. Frequency- Be specific in frequency per week.
Example: 3 times per week not 3-5 times per week
C. Duration- Be specific in the duration of the plan of treatment.
Example: 4 weeks not 4-6 weeks
D. Procedures/Modalities
E. Date, name and discipline of therapist writing the order
3. A new clarification treatment order is required to be written when there is change
in the Plan of Treatment. For example: change in frequency; adding or deleting a
modality/procedure. The new clarification order will include the complete plan of
treatment.
4. Therapy discharge orders may be required as well per facility directives.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Documentation Page 1
POLICY TITLE: DOCUMENTATION
APPLICATION: All Rehab Sites
EFFECTIVE DATE: October, 2010
REVISION DATE: December, 2014
POLICY
Documentation will be completed in a timely manner.
PURPOSE
To ensure adherence to professional standards, promote team communication, and comply with
payor mandates.
PROCESS
All documentation and related billing will be completed at the time of service delivery.
Evaluation and re-certification forms are to be completed with ensuing physician orders on the
day they are billed.
Daily notes are due each day before leaving the building; tenth visit progress reports are due upon
each tenth therapy date.
Discharge documentation is due at the time of patient discharge from therapy.
All documentation is to be completed according to the standards per the Rehab Optima
documentation system and per Arbor Rehabilitation’s documentation training webinars.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Evaluations Page 1
POLICY TITLE: EVALUATIONS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December, 2014
POLICY
Upon receipt of physician’s order, evaluations will be completed.
PURPOSE
The evaluation provides information for the establishment of the plan of treatment,
interdisciplinary communication, MDS completion, care planning, reimbursement,
accreditation and regularly requirements.
PROCESS
1. All disciplines will complete the appropriate sections of the discipline specific
evaluation form.
2. Objective Data: Complete the areas that are assessed and document the specific
and objective clinical data gathered at the time of the initial evaluation. Identify
objective measurement tools used to gather data. Areas not tested should be
marked N/A if area will not be addressed on the POC. If the area is to be
addressed on the POC it should be noted as “Unable” or “Totally Dependent”.
3. Patient/ caregiver goals should reflect the actual goals specified or stated by the
resident, family or caregiver. Example: “I want to walk again”, “I want to be able
to play golf”, and “I want to eat real food”.
4. All fields indicated in Red on the Rehab Optima must be completed. Descriptors
may be found by hovering the cursor over each section.
5. Electronic signatures are required upon completion of the evaluation.
6. All procedures or modalities rendered must be indicated on the Plan of Treatment.
7. All POCs must have at least one long and one short term goal. Goals are not to be
repeated.
8. Physician signature is required on OT, PT, ST Plans of Care.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Interdisciplinary Screen Page 1
POLICY TITLE: INTERDISCIPLINARY HISTORICAL SCREEN
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December 8, 2010
POLICY
It is the policy of Arbor Rehabilitation and Healthcare Services Inc. to screen all residents for
possible therapy intervention. These screenings may be completed upon admission/readmission,
upon facility referral, upon resident change in functional status or according to a quarterly/annual
schedule.
PURPOSE
The purpose of the therapy screen is to ensure that all residents have the opportunity to receive
therapy services if a functional decline has occurred and skilled services are indicated. Screening
policy compliance will support compliance with OBRA regulations for promotion of optimal
levels of function.
PROCESS
1. All screens will consist of a brief review of the medical record, interview of the
resident/staff/family and observation of the resident in the environment. NO hands-on
intervention is performed. No direct recommendations are made based on the screen with
the exception of whether or not a therapy evaluation is indicated. Completion of the
screening form occurs after the above tasks. (see instructions for form completion)
2. The screening is/may be performed by one discipline which includes the chart review,
resident observation and or interview/staff interview and completion of the form. It is
expected that this process will be done in 48 business hours for new admissions
/readmissions, facility referred residents, residents for whom a change in status has been
noted.
3. Annual/quarterly screens need to be completed two weeks prior to the Assessment
Reference Date per the RNAC.
a. The MDS schedule should be provided to the FRC mid month for the scheduled
quarterly and annual assessments due the following month.
b. Residents on schedule will be reviewed during the routine Medicare meeting
regarding the results of the screen, plan to evaluate and interdisciplinary team
input regarding the resident’s need for therapy. If a resident has shown a decline,
nursing documentation should support this change. Completed screens may be
brought to the meeting for review.
c. Residents receiving part B services will be discussed at the routine Medicare
meeting. During this meeting the FRC needs to ensure that the RNAC has a rehab
score for each resident on therapy that quarter. If the resident does not have a
rehab score, the facility and rehab should agree upon an appropriate ARD.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Interdisciplinary Screen Page 2
4. FRC attendance at daily nursing meetings may also trigger the need for a therapy screen.
As the FRC is made aware of falls, new physician orders, and changes in status such as
confusion, difficulty in transfers/ambulation/ADL’s, hygiene, positioning and oral intake,
a screen should occur. In this way a resident’s status may be informally monitored daily.
5. A therapists’ observation of any resident may also trigger the need for a screen if a change
in status is noted.
6. The therapy department will maintain the screening form in a specially marked binder
that is available to appropriate facility staff during business hours. A copy of all discharge
summaries should be included in this screening binder in order to better highlight
potential changes in patient status.
7. All screens will be completed according to state regulations for each therapy discipline.
All disciplines and licensees are able to perform therapy screens. Screening forms should
be co-signed if an assistant has completed the screen.
8. Please see the Instructions for the Completion of the Interdisciplinary Historical
Screen/Data Collection Form for further information regarding screening process
completion.
Attachments:
Interdisciplinary Historical Screen Form
Interdisciplinary Historical Screen Form Instructions

Interdisciplinary Historical Screen/Data Collection Facility:
Name:____________________________ Rm.________ Significant PMH:__________________________________________
Status Areas Date: Date: Date: Date:
Reason For
Screen
Relevant order
change
Prior Level Mobility Change yes/no Change yes/no Change yes/no Change yes/no
Wheelchair mobility
Ambulation
Falls
Balance
ADL’s Change yes/no Change yes/no Change yes/no Change yes/no
Grooming
Dressing
Toileting/Continence
Self feeding/ equip
Effective adapt equip
Positioning/Skin Change yes/no Change yes/no Change yes/no Change yes/no
Wound
Bed, W/C position
Effective equipment
Pain/Contractures Change yes/no Change yes/no Change yes/no Change yes/no
UE ROM
LE ROM
Contractures/Splint
Pain complaints
Swallowing Change yes/no Change yes/no Change yes/no Change yes/no
Intake method/amt.
Diet
Coughing/drooling
Weight change
Communication Change yes/no Change yes/no Change yes/no Change yes/no
Alert/Oriented
Safety/ Behaviors
Signature:
Co Signature:
Please circle as
appropriate
Refer to
PT/OT/ST/None Refer to
PT/OT/ST/None Refer to
PT/OT/ST/None Refer to
PT/OT/ST/None
Date/Comments:_____________________________________________________________________
Date/Comments:_____________________________________________________________________
Date/Comments:_____________________________________________________________________
Date/Comments:_____________________________________________________________________

Instructions for the Completion of the
Interdisciplinary Historical Screen/Data Collection Form
1. Therapist initiating this form completes the top section for the
patient’s name, room number and therapy relevant medical history.
2. Under the date, the reason for the screen should be noted for
clarification, (IE: a fall or quarterly screen).
3. Any relevant physician order changes should be noted in this
section to further support the screen and possible referral (IE: diet
texture changes).
4. As a therapist initiates the screening, he or she should look back at
any previous therapy discharge summaries for long term care
residents and enter that information in the column titled “Prior
level” and the date. If a resident is new to the facility, or only on
for a brief episode of rehab. or was not previously on therapy, this
section may be filled out with the notation “Per pt. report” or “Per
facility report” It is essential that this section reflects the
resident’s highest level of functioning in the recent past. For
example: A resident that was independent in the community 1
month ago, went to the hospital and admitted to rehab at a max
assist level, returned to the hospital and now readmitted at a max
assist level would be best described as “Independent in the
community one month ago” This prior status must reflect the
person’s highest recent functional level to support the need for
skilled therapy if indicated per the results of the screen. One
therapist may complete this historical data for all discipline areas.
5. For each subsequent column, the date the screening occurs must
be completed along with a yes/no notation if there is an
observed/reported change in any of the functional/safety areas
listed.
6. The screening form must be signed/co-signed each time a column
is completed.
7. The therapist completing the form must circle the appropriate
discipline for a referral or circle “None” if no evaluations are
indicated. Please note that a screening should be brief. If
questions/concerns require an extended amount of time (IE: more
than 10-15 minutes) a referral for an evaluation should be made to
the appropriate discipline. Remember there is no hands-on contact
during a screen.
8. Lines at the bottom of the page may be used for additional
comments or to clarify the reason for a referral.
9. .This form is to be placed in a binder in the department. A copy or
the original may need to be placed in the chart per facility policy.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Medical Record Corrections Page 1
POLICY TITLE: CORRECTING THE MEDICAL RECORD
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December, 2014
POLICY
All therapists will comply with accepted practice for medical record entries and deletions.
This includes all paper and electronic entries.
PURPOSE
To maintain the integrity of medical records.
PROCESS
1. The medical record is a legal document. Accuracy of all entries is a requirement
of regulatory, accreditation and reimbursement authorities. If the medical record
needs to be altered, the correction must be done appropriately; otherwise the
accuracy of the entire record will be called into question. This would be
disastrous in any court or legal proceeding, affecting both the professional
administering care and the patient/resident him/herself.
2. Correcting One’s Own Error In The Medical Record: If a mistake is made while
making an entry, a single line should be drawn through the error followed by the
date and signature or initials of the individual making the correction. Never
scribble over, erase, or use white-out on an entry. When more space is needed,
make the new entry as close as possible to the original error as an addendum. The
addendum is dated and signed and must refer to the location of the record being
corrected.
3. For those therapists who can write orders in the medical record and need to make
a correction, draw a single line through the error followed by the date, time and
signature or initials of the individual making the correction, then have the nurse
countersign the order immediately.
4. If the error is not found while making the entry, the correction is made as a late
entry addendum. The original document is not altered at this time. The
addendum must refer back in time to the erroneous entry and is dated, timed, and
signed at the exact time it is written. Never backdate an entry!

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Medical Record Corrections Page 2
5. Correcting Another Person’s Error In The Medical Record: If it is discovered an
error has been made by another person, inform that person immediately so the
correction can be made.
6. Prohibited Medical Record Entries and Deletions Include:
a. Use of white-out
b. Use of erasers
c. Use of pencils
d. Back dating or entering a date or time that is other than the actual date and
time the entry is made.
e. Making a medical record entry for someone and signing the same for the
other person
f. Rewriting a portion of or an entire medical record

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Medical Record Organization Page 1
POLICY TITLE: ORGANIZATION OF THE REHABILITATION SECTION
OF THE MEDICAL RECORD
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December, 2014
POLICY
The rehabilitation section of a patient’s medical record must be maintained in an orderly
manner that is consistent with sound medical record keeping practice. If facility specific
medical record procedures indicate a format for maintaining the rehabilitation section,
those procedures must be followed. However, if procedures are not specified, the
following organization is to be followed for those facilities with paper based hard charts.
PURPOSE
To maintain proper organization of the rehabilitation section of the medical record.
PROCESS
1. As approved by the facility Administration, the rehabilitation section must be
subdivided with separate discipline specific sections. If tabs are not available, an
alternate divider such as colored sheets should be used to divide documents by
discipline.
2. Within each section, the order must be chronologically built by certification
period with the most current documentation on top. Original certifications/
recertifications and printed out electronic documents are to be maintained in the
patient’s hard chart per facility policy.
3. The respective certification periods are maintained as follows from bottom to top:
(certification period 1) Plan of Treatment, Progress Notes, Daily treatment
encounter notes, (certification period 2) Updated Plan of Progress, Progress Notes,
Daily treatment encounter notes, and so on.
4. Physician orders for rehabilitation services must be clearly delineated in the
medical record.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Medical Record Page 1
POLICY TITLE: THE MEDICAL RECORD
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: December, 2014
POLICY
It is the policy of Arbor Rehabilitation that each therapist will maintain clinical records
on all patients/residents that reflect the current professional standards and practices and
complies with the facility’s policies and procedures.
PURPOSE
To provide a medical record, which is an accurate record of service delivery, maintain
confidentiality and to meet established state or federal guidelines for record keeping.
PROCESS
1. Medical Records Storage
a. All records (including documents that have not been filed in the
medical record) kept in the rehab department will be maintained under
lock and key overnight or when not in use, providing access to
qualified personnel only.
b. The medical record (paper or electronic versions) should be monitored
at all times to protect the confidential nature of the information
included in the record. This includes keeping the medical record
closed, out of plain view from the unqualified personnel.
c. The original medical record will not be removed from the facility for
any reason.
2. Medical Record Documentation and Use
a. The medical record is the property of the facility. The staff will follow
written guidelines/policies of the facility regarding medical record use
and release of information.
b. All documentation will be filed in the medical record immediately after
completion or per facility guidelines such as upon discharge from therapy.
c. Corrections are to be made per the correction policy.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Medical Record Page 2
f. Soft files containing signed certifications/ recetifications will be
maintained in the department or designated location for a period of no
less than 2 years.
g. The medical record will contain at the minimum, an evaluation with
the original signed certification, all original signed re-certifications,
progress reports, service log and discharge summary. Other
documents may be included per facility request.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Multidisciplinary Therapy Screen Page 1
POLICY TITLE: MULTIDISCIPLINARY THERAPY SCREEN
APPLICATION: All Rehab Sites
EFFECTIVE DATE: May 1, 2006
REVISION DATE:
POLICY
In the absence of evaluation orders for all disciplines, patients may be screened by therapy
staff upon admission and readmission. Long term care and assisted living residents may
be screened quarterly with physician orders; upon facility request and/or physician request
based on a documented change in status. If necessary and appropriate, state regulations
will take precedence.
PURPOSE
To provide the patient and/or resident with the opportunity to receive therapy services if
functional declines are present; skilled services are required; and to ensure compliance
with OBRA regulations for maintenance of optimal levels of function.
PROCESS
1. All screens will consist of a brief review of the medical record; interview of
patient/resident, staff, family; observation of patient/resident in environment. No
“hands on” formal testing is completed. No direct recommendations are made
based on information obtained from a screen with the exception that further
evaluation is indicated.
2. When to perform a Multidisciplinary Therapy Screen:
Admission/Readmission: All patients are screened within 48 hours of
admission/readmission to the facility.
Referrals from Physician/Nursing: These patients are screened by the specific
discipline to which the referral was made.
Quarterly with Physician Order: These patients are screened by one therapy
discipline to determine the need for OT, PT, and/or ST.
3. All screens are to be completed in accordance with specific State rules and
regulations.
4. The Multidisciplinary Therapy Screen will be completed according to the
Instructions for Completing the Multidisciplinary Therapy Screen.
Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Physician Order/Telephone Orders Page 1
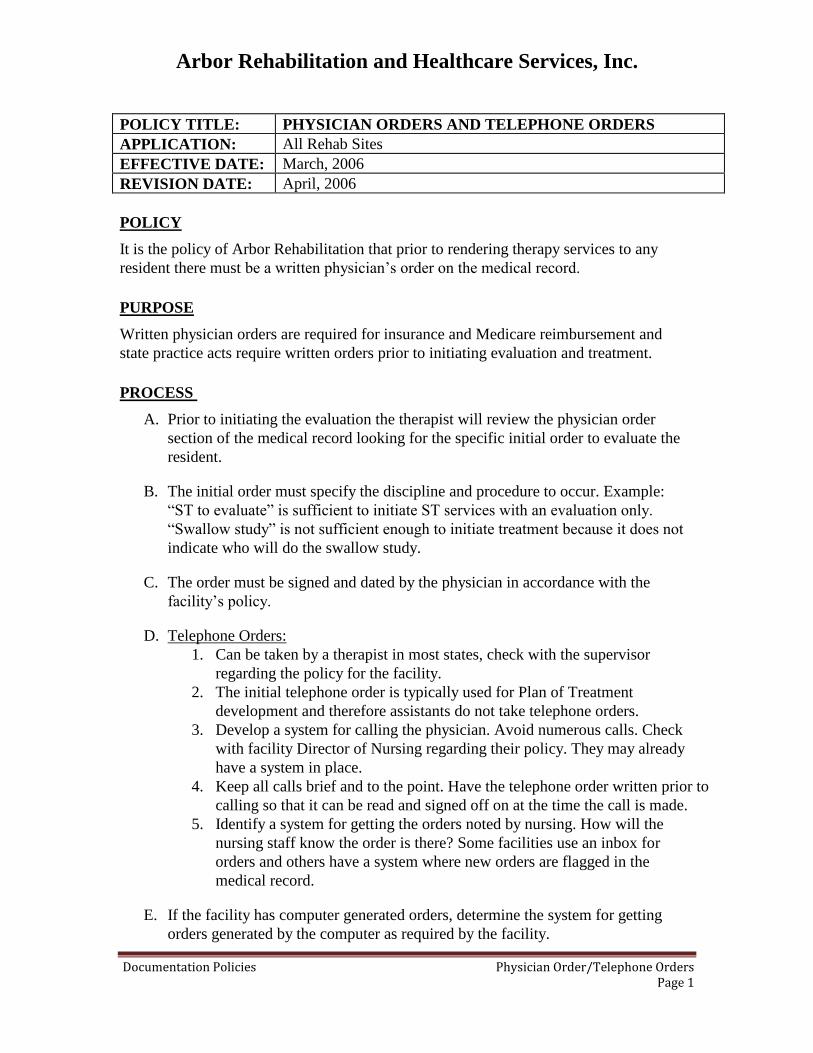
POLICY TITLE: PHYSICIAN ORDERS AND TELEPHONE ORDERS
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: April, 2006
POLICY
It is the policy of Arbor Rehabilitation that prior to rendering therapy services to any
resident there must be a written physician’s order on the medical record.
PURPOSE
Written physician orders are required for insurance and Medicare reimbursement and
state practice acts require written orders prior to initiating evaluation and treatment.
PROCESS
A. Prior to initiating the evaluation the therapist will review the physician order
section of the medical record looking for the specific initial order to evaluate the
resident.
B. The initial order must specify the discipline and procedure to occur. Example:
“ST to evaluate” is sufficient to initiate ST services with an evaluation only.
“Swallow study” is not sufficient enough to initiate treatment because it does not
indicate who will do the swallow study.
C. The order must be signed and dated by the physician in accordance with the
facility’s policy.
D. Telephone Orders:
1. Can be taken by a therapist in most states, check with the supervisor
regarding the policy for the facility.
2. The initial telephone order is typically used for Plan of Treatment
development and therefore assistants do not take telephone orders.
3. Develop a system for calling the physician. Avoid numerous calls. Check
with facility Director of Nursing regarding their policy. They may already
have a system in place.
4. Keep all calls brief and to the point. Have the telephone order written prior to
calling so that it can be read and signed off on at the time the call is made.
5. Identify a system for getting the orders noted by nursing. How will the
nursing staff know the order is there? Some facilities use an inbox for
orders and others have a system where new orders are flagged in the
medical record.
E. If the facility has computer generated orders, determine the system for getting
orders generated by the computer as required by the facility.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Plans of Treatment - Changes Page 1
POLICY TITLE: CHANGES IN PLAN OF TREATMENT AND
RE-CERTIFICATION
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: April, 2006
POLICY
1. If a therapist wants to change the Plan of Treatment, the telephone order
procedures must be followed.
2. For Medicare Part A and Part B residents, the physician must re-certify any
changes to the Plan of Treatment. AND,
3. The Plan of Treatment must be re-certified every 30 days or less.
PURPOSE
1. Written physician orders are required for insurance and Medicare reimbursement.
Therefore any changes to the Plan of Treatment would need to be documented by
the physician in order to comply with Medicare regulations.
2. Medicare requires re-certification of the Plan of Treatment. Therefore, the
recertification of the plan of treatment would need to be documented and signed
by the physician in order to comply with Medicare regulations.
PROCESS
1. Follow the procedure established at the facility for changes to the Plan of
Treatment. The following process is recommended:
a. The therapist will try to contact the physician for a verbal telephone order
to initiate the new treatment.
b. If the physician is unable to be reached, the Plan of Treatment or telephone
order will be faxed or mailed to the appropriate physician.
2. For Medicare only. Follow the procedure established at the facility for re-
certification. The following process is recommended:
a. Complete the Plan of Treatment form; check off 30-day re-certification.
b. Make a copy of the completed Plan of Treatment form.
c. Fax or mail the plan care form to the physician.
d. Take the copy of the completed form and write faxed or mailed and the
date in the physician’s signature space.
e. File the copy of the form in the physician’s order section of the medical
record until the signed copy is returned. When the signed copy is received,
replace the copy with the signed one in the medical record.
f. Keep a log of faxes sent or mailed to track responses.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Wound Care Documentation Page 1
POLICY TITLE: DOCUMENTATION OF WOUND CARE
APPLICATION: All Rehab Sites
EFFECTIVE DATE: March, 2006
REVISION DATE: June, 2006
POLICY
All Physical therapists will complete required documentation for wound care prior to the end of
the working day of the provision of service at each facility. Documentation will meet all
Medicare and Medicaid requirements.
PURPOSE
Arbor provides practice guidelines for the accurate and appropriate documentation of wound care
service provided by Physical Therapy.
PROCESS
1. Evaluation:
a. The evaluation is completed within 24 hours of receipt of order.
b. Utilize the Arbor Rehab. Physical Therapy Wound Evaluation form.
c. Complete the form in its entirety.
d. Us the clinical reasoning process to determine the reasons for Physical Therapy
involvement, keeping in mind the Medicare reimbursable guidelines.
2. Wound Care Orders:
a. The Physical Therapy orders will include:
i. Date
ii. Physical Therapy
iii. Frequency, intensity (BID, QD) and duration of treatment
iv. Location of the wound
v. Treatment modalities/procedures and dressing specifications
vi. Physician signature
b. In the event that nursing and physical therapy are both providing wound care, a separate
order for each discipline indicated each responsibility should exist.

Arbor Rehabilitation and Healthcare Services, Inc.
Documentation Policies Wound Care Documentation Page 2
3. Goals:
The long term and short term goals should be established using the following criteria:
a. Patient specific
b. Measurable, percentages, stages, centimeters, etc.
c. Realistic and achievable
d. Functional
4. Daily Note:
a. A daily entry is completed using the Arbor Rehab. Services wound treatment and
progress note form.
b. One form is used per wound being treated.
c. If nursing is also treating, both disciplines may document on the same form.
d. A narrative note is made on a progress note page if there is a significant issue, problem
or change that requires supporting documentation.
e. Documentation will include the skilled intervention that was required for the patient to
achieve their goals; a summary of the functional benefits as a result of skilled
intervention; specific measurements of pain, stages, level, percentages, etc., and the
recommendations for continued treatment or discontinuation of treatment.