appropriate laboratory investigation
TRANSCRIPT
16/11/55
1
Laboratory interpretation
Lalita Norasetthada, MD Hematology Division,
Department of internal medicine, CMU
Laboratory interpretation
•Hematology lab
▫ CBC
▫ Coagulogram
•Blood chemistry
▫ Liver function
▫ Kidney function
▫ FPG and lipid profile
•Serologic test

16/11/55
2
Normal Laboratory Values
2 SD
Abnormal Normal
normal values = mean ± 2SD of normal population
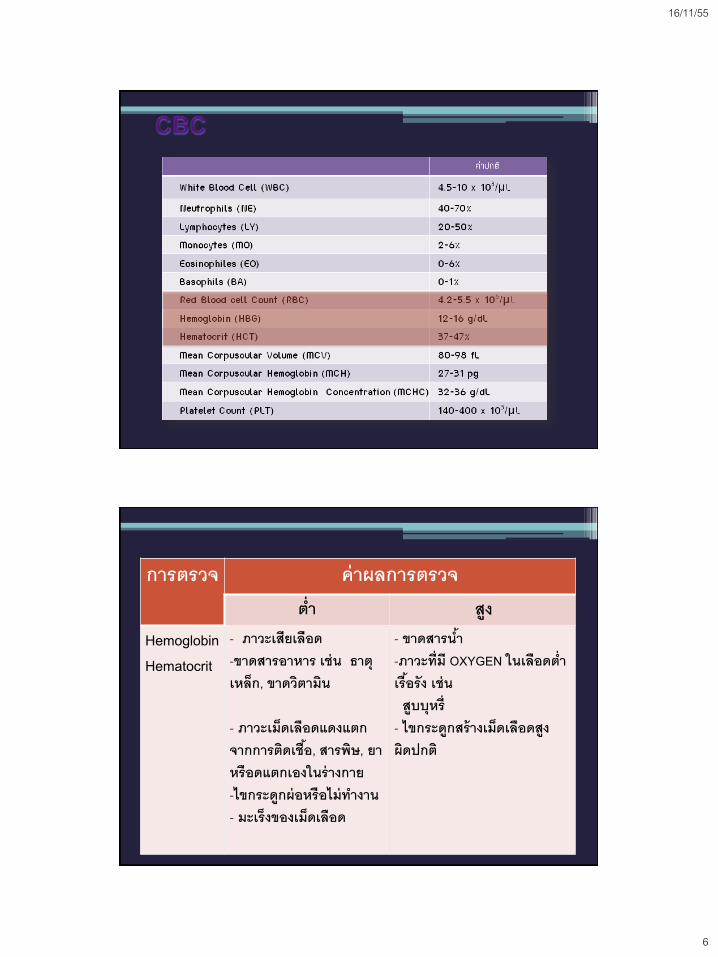
CBC : Complete Blood Count

16/11/55
3
• ปริมาณลดลง ▫ การตดิเชือ้ไวรัส ▫ ยาบางชนิด ▫ โรคของไขกระดูกท าให้สร้างเม็ดเลือดขาวลดลง
• ปริมาณเพิ่มขึน้ ▫ การตอบสนองของร่างกายปกตทิี่เกิดในภาวะตดิเชือ้หรือการอักเสบ (< 30,000/uL)
▫ มะเร็งเม็ดเลือดขาว
• Normal range • 4,500-10,000 cell/mm3
• 4.5-10 x 103/uL
White blood cell count

16/11/55
4

16/11/55
5
WBC morphology
16/11/55
6
การตรวจ ค่าผลการตรวจ
ต ่า สูง
Hemoglobin Hematocrit
- ภาวะเสียเลือด -ขาดสารอาหาร เช่น ธาตุเหล็ก, ขาดวิตามิน
- ภาวะเม็ดเลือดแดงแตก จากการติดเชือ้, สารพิษ, ยา หรือดแตกเองในร่างกาย -ไขกระดูกผ่อหรือไม่ท างาน - มะเร็งของเม็ดเลือด
- ขาดสารน า้ -ภาวะที่มี OXYGEN ในเลือดต ่าเรือ้รัง เช่น สูบบุหร่ี - ไขกระดูกสร้างเม็ดเลือดสงูผิดปกติ

16/11/55
7
RBC morphology
Concerning values
•For general dental procedure
▫ Hb > 7 gm/dl
•Procedure under GA
▫ Hb > 9.5-10 gm/dl

16/11/55
8
การนับจ านวนเกร็ดเลือด (platelet count)
•Platelet count
▫ 100,000-450,000/mm3
▫ 100-450 x 103/uL

16/11/55
9
การตรวจ ค่าผลการตรวจ
ต ่า สูง
เกร็ดเลือด
- ม้ามโต - เกร็ดเลือดถูกท าลายมากขึน้ จากยา, ภูมิต้านทาน - เกร็ดเลือดสร้างได้น้อยจากความผิดปกติของไขกระดูก • ไขกระดูกฝ่อ หรือ
ท างานผิดปกติ • ไขกระดูกถูกแทรกซึม
จากการติดเชือ้หรือมะเร็ง
• โรคมะเร็งเม็ดเลือด
-การอักเสบหรือการติดเชือ้เรือ้รัง -มะเร็งของอวัยวะอื่น -โรคไขกระดูกสร้างเม็ดเลือดเพิ่มมากผิดปกติ -มะเร็งเม็ดเลือดขาวเรือ้รัง
Platelet morphology

16/11/55
10
Increased risk of bleeding when
• Platelet count
▫ <50,000/mm3 or < 50 x 103/uL
▫ > 1,000,000/mm3 or > 1,000 x 103/uL
• In mild thrombocytopenia, all dental
procedure can be done safely (50,000-
100,000/mm3)
Coagulation test

16/11/55
11
Primary hemostasis
Secondary Hemostasis
In vivo
In vitro

16/11/55
12
Coagulation test
• PT : prothrombin time
▫ Range 8-11 seccods
• aPTT : activated partial thromblastin
time ▫ Range 28-32 seconds
Isolated PT Prolongation
Inherited
• FVII deficiency
Acquired
• Vitamin K deficiency
• Liver disease
• Warfarin
administration
• Inhibitor of FVII

16/11/55
13
Isolated PTT prolongation
Inherited
• Deficiency of F VIII, IX, XI
• Deficiency of FXII, prekallikrein, HMW kininogen
• VWD
Acquired
• Lupus anticoagulant
• Inhibitor to FVIII, IX, XI, XII
• Heparin administration
Combined PT and PTT prolongation
Inherited
• Deficiency of FV, X,
fibrinogen, prothrombin
Acquired
• Liver disease
• DIC
• Supratherapeutic dose of
warfarin and heparin
• Inhibitor of FV, X,
fibrinogen, prothrombin
• Primary amyloidosis
associated FX deficiency

16/11/55
14
Bleeding risk
• Increased risk of bleeding after
invasive procedure when
▫ Either PT or aPTT increases > 1.5
folds above mid normal range
▫ Ex.
PT 24 secs (8-12), INR 2.5
PTT 40 secs (28-32)
Bleeding disorder in the setting
of normal screening test
• Platelet dysfunction
▫ Drug : aspirin, NSAID, clopidrogrel
▫ Chronic disease : liver/kidney failure
▫ Hereditary disorder
• Impaired fibrin crosslink and
fibrinolytic disorder

16/11/55
15
Blood Chemistry BUN
Cr
Albumin / Globulin
GOT / GPT
Alk. Phosphatase
Cholesterol
Bilirubin
Cholesterol
Triglyceride
HDL
LDL
Plasma glucose
Kidney function
Liver function test
Lipid Profile
Kidney function test

16/11/55
16
Laboratory test to evaluate kidney
function
• Glomerular filtration rate (GFR)
• Plasma creatinine
• Plasma urea
• Urine volume
• Urine electrolytes, protein, urea, osmolality
Glomerular filtration rate
• Value always adapted to the BSA!! Ideal BSA
in adults is 1.73m2
•Schwartz equation : GFR= v x 0.808
• Pcr
(umol/L)
•How to assess easy if plasma creatinine is OK

16/11/55
17
Creatinine and Urea Plasma
Concentration- hyperbolic correlation
GFR 50%
pCr,
pUrea
140 mL/min
(100%) 0 mL/min
(0%)
Lower limit 90 ml/Min./1.73
m2 Normal
range->
Plasma urea (BUN)
• BUN (blood urea nitrogen) 10-20 mg/dl
• Urea: product of protein catabolism
• Synthesized by liver, excreted by kidney,
partially reabsorbed in tubuli
• Plasma concentration increases with
decreased GFR

16/11/55
18
BUN in patients
with kidney diseases
• Useful test but must be interpreted with
great care ▫ urea plasma level is more than creatinine
dependent on protein intake
• Most useful when considered along
with creatinine ▫ High in high protein intake, UGI bleeding
▫ Low in severe liver dysfunction
Creatine Creatinine (Waste product)
H2O
• Creatine : main storage compound of high
energy phosphate needed for muscle
metabolism
• Creatinine: anhydride of creatine
• Creatinine is freely filtered by the glomerulii
and is not reabsorbed
Plasma creatinine and renal function

16/11/55
19
• Plasma creatinine
Male 0.6-1.2 mg/dL,
Female 0.5-1.0 mg/dL
• Pre-renal disorder ▫ BUN:Cr ratio >20
• Renal and postrenal
disorders
▫ BUN: Cr 10-20 both
elevated
Analytic method
Filter
Processor
Input
Arterial
Output
Venous
Output
Urine
Liver function test

16/11/55
20
Liver Function Test
Liver chemistry test Clinical implication of abnormality
ALT Hepatocellular damage
AST Hepatocellular damage
Bilirubin Cholestasis, impair conjugation, or biliary obstruction
ALP Cholestasis, infiltrative disease, or biliary obstruction
PT Synthetic function
Albumin Synthetic function
GGT Cholestasis or biliary obstruction
Bile acids Cholestasis or biliary obstruction
5`-nucleotidase Cholestasis or biliary obstruction
LDH Hepatocellular damage, not specific
Normal values

16/11/55
21
Advantages
• Sensitive, noninvasive method of screening liver dysfunction
• Pattern of laboratory test abnormalities to recognize type of liver disorder
• Assess severity of liver dysfunction
• Follow cause of liver disease
Disadvantages
• Not specific for liver
dysfunction
• Seldom lead to specific
diagnosis
Liver Function Test
Liver function test

16/11/55
22
Classified in 3 groups
•Synthetic function : albumin,
prothrombin time (PT)
•Hepatocyte injury : AST, ALT
•Cholestasis : bilirubin, ALP, GGT
PT, albumin, bilirubin : most common tests used as prognostic factors
Liver Function Test
Liver function test

16/11/55
23
Albumin
•Depending on nutrition, volume status, vascular integrity, catabolism, hormone, loss in stool and urine •Not specific for liver disease •T1/2 19-21 D
Globulin
• Produced by stimulated B-lymphocyte
• Elevation in
• chronic liver disease
• chronic inflammation and malignant
disease

16/11/55
24
Hypoalbuminemia
globulin chol/TG Hb
1.decrease synthesis
-protein malnutrition
-chronic liver disease
-chronic inflammation
2.increase loss
-Protein loosing enteropathy
-NS
3.increase Vd (ascites, overhydration)
Metabolic Syndrome

16/11/55
25
Abnormal Lipid
Metabolism
LDL
ApoB
HDL
Trigly.
Cardiometabolic Risk Global Diabetes / CVD Risk
Overweight / Obesity
Inflammation
Hypercoagulation
Hypertension
Smoking
Physical Inactivity
Unhealthy Eating
Age, Race,
Gender,
Family History
Glucose BP Lipids
Age Genetics
Insulin Resistance
Insulin Resistance
Syndrome
Cardiometabolic Risk - Graphic
Interpreting Blood
Glucose Levels
• Fasting glucose : No caloric intake > 8 hours ▫ Healthy BG FPG < 100 mg/dL
▫ Pre-diabetes FPG 100–125 mg/dL
(Impaired fasting glucose)
▫ Diabetes FPG ≥126 mg/dL
• Random plasma glucose ▫ PG > 200 mg/dl

16/11/55
26
Total Cholesterol Goals34
• Desirable — Less than 200 mg/dL
• Borderline high risk — 200–239 mg/dL
• High risk — 240 mg/dL and over
American Diabetes Association. Understanding Cardiometabolic Risk: Broadening Risk Assessment and Management,
Dyslipidemia Richard M Bergenstal, MD International Diabetes Center
Lipid profile
•No caloric intake > 12 H
•Lipid profle
▫ Total choleterol
▫ LDL
▫ HDL
▫ TG

16/11/55
27
Cholesterol Management
Category of risk LDL-C Goal
0-1 risk factor* < 160 mg/dL or lower
Multiple (2+) risk factors* < 130 mg/dL or lower
People with coronary heart
disease or risk equivalent
(e.g., diabetes)
< 100 mg/dL or lower
Known CAD and DM < 70 mg/dL or lower may be ideal
LDL-C-lowering
Serologic tests
16/11/55
28
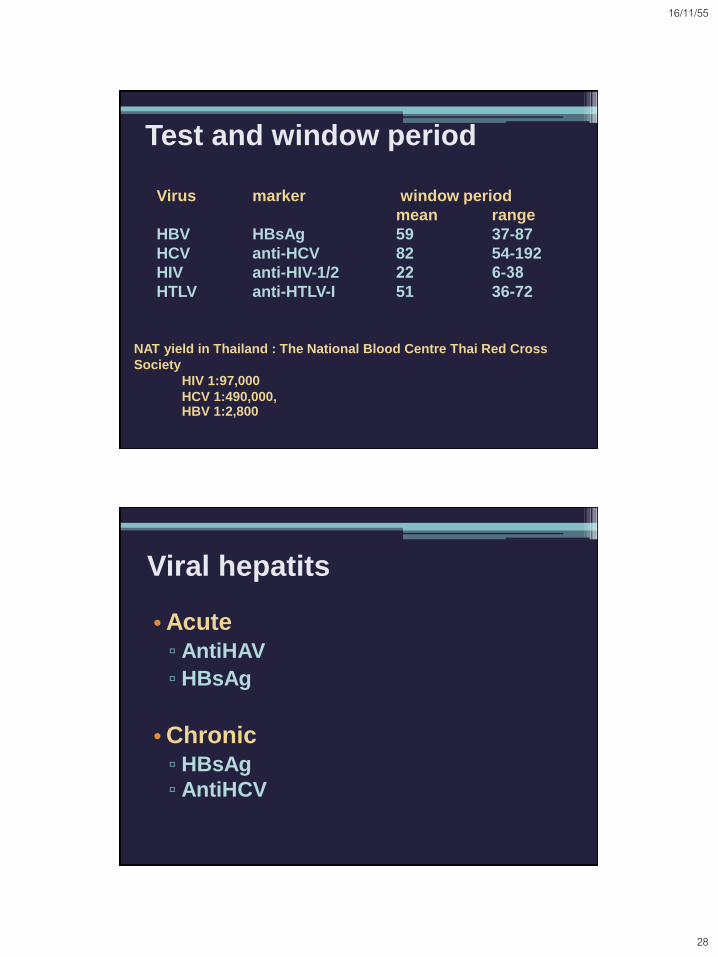
Test and window period
Virus marker window period
mean range
HBV HBsAg 59 37-87
HCV anti-HCV 82 54-192
HIV anti-HIV-1/2 22 6-38
HTLV anti-HTLV-I 51 36-72
NAT yield in Thailand : The National Blood Centre Thai Red Cross
Society
HIV 1:97,000
HCV 1:490,000, HBV 1:2,800
Viral hepatits
•Acute
▫ AntiHAV
▫ HBsAg
•Chronic
▫ HBsAg
▫ AntiHCV

16/11/55
29
Main Ways to Get Hepatitis A
Fecal-oral route
Viral hepatitis A

16/11/55
30
Having sex without condoms with
someone who has hepatitis B
Main Ways to Get Hepatitis B
Sharing needles and syringes
Being born to a mother who has
hepatitis B
Receiving blood component from
HBV infected donor
Natural history of HBV - related infection
Acute
hepatitis Contamination
Resolution Chronic infection
95%
Chronic hepatitis
5%
Inactive carriage
HCC Cirrhosis
3-5% yearly
Asymptomatic 30%
Fulminant hepatitis 1%
66% 33%
10-20%

16/11/55
31
Viral hepatitis B
If you have never had hepatitis B,
you can get 3 shots . . .
. . . and get long lasting
protection.
3 2 1
Hepatitis B can be prevented!

16/11/55
32
Main Ways to Get Hepatitis C
Sharing needles and syringes
Receiving blood component from
HCV infected donor
Hepatitis C Virus (HCV)
•HCV Infection
- Acute infection
- Mild symptoms
- 50-70% of affected patients develop
chronic hepatitis
- 20% of affected patients develop
cirrhosis or hepatocellular carcinoma

16/11/55
33
Viral hepatitis C
HIV infection
•AIDs situation in Thailand, March
2011
•Prevalence 0.6% ▫ Total HIV infected cases 372,874 persons
▫ Already died 98,153 persons

16/11/55
34
Having sex without condoms with HIV
infected persons
Main Ways to HIV
Sharing needles and syringes
Being born to a mother who has
HIV
Receiving blood component from
HBV infected donor
Strauss JM & Strauss EG,2002
HIV
16/11/55
35
Who to Test for HIV
• High risk groups include ▫ MSM
▫ Injection drug users or history injection drugs
▫ Heterosexual partners of those listed above
▫ Those interested in HIV testing
▫ People presenting with an opportunistic infection or recurrent/severe infections that can not otherwise be explained
HIV Testing
• EIA- standard serologic screening test ▫ Needs to be repeatedly positive
▫ Should not give the patient this test result until
confirmed
• Western Blot-confirmatory test. ▫ 2 bands of the following: p24, gp41 or gp120/160
Antibodies to p24 and p55 appear earliest but decrease or
become undetectable.
Antibodies to gp31, gp41, gp120, and gp160 appear later but are
present throughout all stages of the disease
▫ EIA and Western Blot >99.9% sensitive and
specific

16/11/55
36
Window period in HIV infection
HIV Testing
• 4-20% of test results are indeterminate with WB assays with positive bands for HIV-1 proteins
• Causes of indeterminate tests include ▫ Patients in the process of
seroconversion ▫ HIV-2 infection ▫ Cross-reacting nonspecific antibodies ▫ Testing should be repeated at 6-8 weeks,
3, and 6 months

16/11/55
37
HIV Testing
•Rapid testing ▫ Two tests FDA approved, SUDS and
Oraquick
▫ Oraquick much easier and very accurate
▫ Sensitivity and Specificity is 99.5%
▫ Positives still need confirmation ▫ Similar to performing a pregnancy
test
The End