approach to renal disorders
DESCRIPTION
Approach to Renal Disorders. AIMGP Seminar Revised by Nick Hariton November 2006. Objectives. To identify appropriate strategies for investigation of the patient with kidney disease To discuss interventions that may alter the course of disease - PowerPoint PPT PresentationTRANSCRIPT
Approach to Approach to Renal DisordersRenal Disorders
AIMGP SeminarAIMGP SeminarRevised by Nick Hariton November Revised by Nick Hariton November
20062006
ObjectivesObjectives
To identify appropriate strategies for To identify appropriate strategies for investigation of the patient with investigation of the patient with kidney diseasekidney disease
To discuss interventions that may To discuss interventions that may alter the course of diseasealter the course of disease
To discuss indications for referral to To discuss indications for referral to a nephrologist a nephrologist
GuidelinesGuidelines
Elevated Serum creatinine: Elevated Serum creatinine: recommendations for management and recommendations for management and referral. CMAJ 1999: 161:413-17referral. CMAJ 1999: 161:413-17
National Kidney Foundation: Kidney National Kidney Foundation: Kidney Disease Outcomes Quality Initiative Disease Outcomes Quality Initiative (NKF-KDOQI), 2002(NKF-KDOQI), 2002
Practice guidelines for Chronic Kidney Practice guidelines for Chronic Kidney Disease. 2003. Annals of Internal Disease. 2003. Annals of Internal medicine. Vol. 139 Number 2.medicine. Vol. 139 Number 2.

Stages of Renal FailureStages of Renal Failure
Stages of Renal Stages of Renal FailureFailure
GFR (cc/min)GFR (cc/min)
Stage 1 >90
Stage 2 (Mild)Stage 2 (Mild) 60-9060-90
Stage 3 (Moderate)Stage 3 (Moderate) 30-5930-59
Stage 4 (Severe)Stage 4 (Severe) 15-2915-29
Stage 5 (End-stage)Stage 5 (End-stage) <15<15

Creatinine is an estimate Creatinine is an estimate of GFRof GFR
Cockcroft-Gault:Cockcroft-Gault:(140-age) x wt x 100(140-age) x wt x 100 = GFR (cc/min) = GFR (cc/min)72 x serum Cr72 x serum CrGFR (females) = GFR (males) x 0.85GFR (females) = GFR (males) x 0.85
MDRDMDRD
24 hour urine for creatinine24 hour urine for creatinine

CASES: What is CASES: What is Considered an Considered an
ELEVATED Creatinine?ELEVATED Creatinine?
55 yo 70 kg male with Cr of 220:55 yo 70 kg male with Cr of 220:
75 yo 45kg female with Cr of 75 yo 45kg female with Cr of 220: 220:
75 yo 45kg female with Cr of 85:75 yo 45kg female with Cr of 85:
75 yo 45kg female with Cr of 45:75 yo 45kg female with Cr of 45:
GFR =37moderate
GFR =40moderate
GFR = 16severe
GFR =76mild

Workup of a decreased Workup of a decreased GFRGFR ApproachApproach
1. Identify chronicity (Acute vs chronic) 1. Identify chronicity (Acute vs chronic)
2. Identify the cause, especially reversible 2. Identify the cause, especially reversible causescauses
3. Identify Indications for Referral to a 3. Identify Indications for Referral to a NephrologistNephrologist
4. Initiate a cause specific management 4. Initiate a cause specific management plan in a multidisciplinary team.plan in a multidisciplinary team.
Acute vs Chronic Renal Acute vs Chronic Renal FailureFailure
ACUTEACUTE- FeverFever- HypovolemiaHypovolemia- SepsisSepsis- New hypertensionNew hypertension- Recent nephrotoxinsRecent nephrotoxins- No hypocalcemiaNo hypocalcemia- No No
hyperphosphatemiahyperphosphatemia- No anemiaNo anemia
CHRONICCHRONIC- previous confirmed previous confirmed
nephropathynephropathy- Already diminished Already diminished
CrClCrCl- Atrophic kidneys Atrophic kidneys
(<10cm on U/S)(<10cm on U/S)- Normochromic Normochromic
normocytic anemianormocytic anemia- HypocalcemiaHypocalcemia- HyperphosphatemiaHyperphosphatemia

Abdominal ImagingAbdominal Imaging
Normal size kidneys in chronic Normal size kidneys in chronic kidney diseasekidney disease
DiabetesDiabetes Polycystic kidney diseasePolycystic kidney disease Myeloma KidneyMyeloma Kidney AmyloidosisAmyloidosis HIV NephropathyHIV Nephropathy

Underlying CauseUnderlying Cause
CHRONIC KIDNEY DISEASE
PRE-RENAL RENAL POST-RENAL
GLOMERULAR INTERSTITIAL VASCULAR
Pre-Renal DiseasePre-Renal Disease Medications:Medications:
NSAIDNSAID DiureticDiuretic
Renal Artery StenosisRenal Artery Stenosis Decrease effective circulating volumeDecrease effective circulating volume
Congestive heart failureCongestive heart failure CirrhosisCirrhosis Hypovolemia (losses or decreased intake)Hypovolemia (losses or decreased intake)
Normal urine sediment, decreased urine Normal urine sediment, decreased urine [na+], increased BUN:Cr[na+], increased BUN:Cr

Post-Renal DiseasePost-Renal Disease
Intraluminal obstruction:Intraluminal obstruction: NephrolithiasisNephrolithiasis
Luminal obstructionLuminal obstruction Transitional cell carcinomaTransitional cell carcinoma Severe BPHSevere BPH
Extraluminal obstructionExtraluminal obstruction Retroperitoneal fibrosisRetroperitoneal fibrosis Lymphadenopathy (lymphoma)Lymphadenopathy (lymphoma) MassMass

Glomerular DiseaseGlomerular Disease
Active Sediment (RBC casts, Active Sediment (RBC casts, hematuria)hematuria) IgA NephropathyIgA Nephropathy Post-infectious GNPost-infectious GN Autoimmune disease and vasculitisAutoimmune disease and vasculitis Chronic hepatitis and HIVChronic hepatitis and HIV
Nephrotic Syndrome (bland sediment, Nephrotic Syndrome (bland sediment, >3g/day proteinuria)>3g/day proteinuria) Primary and secondary causesPrimary and secondary causes DIABETESDIABETES

Interstitial DiseaseInterstitial Disease
Polycystic Kidney DiseasePolycystic Kidney Disease Chronic infectious pyelonephritisChronic infectious pyelonephritis Allergic interstitial nephritisAllergic interstitial nephritis Autoimmune interstitial nephritisAutoimmune interstitial nephritis Reflux nephropathyReflux nephropathy Myeloma KidneyMyeloma Kidney

Vascular DiseaseVascular Disease
Large-sized ArteriesLarge-sized Arteries Renal artery stenosisRenal artery stenosis
Medium-sized ArteriesMedium-sized Arteries HYPERTENSIVE NEPHROSCLEROSISHYPERTENSIVE NEPHROSCLEROSIS VasculitisVasculitis
ArteriolesArterioles Microangiopathies (scleroderma, Microangiopathies (scleroderma,
HUS/TTP, cyclosporine)HUS/TTP, cyclosporine) Venous thrombosis Venous thrombosis

History and Physical History and Physical ExamExam
signs or symptoms of signs or symptoms of underlying disorder: i.e. volume status, flank underlying disorder: i.e. volume status, flank
pain, obstruction, diabetes, hypertension, pain, obstruction, diabetes, hypertension, vasculitisvasculitis
altered kidney function: urine output, urine altered kidney function: urine output, urine discoloration, edemadiscoloration, edema
renal failure: anorexia, vomiting, altered renal failure: anorexia, vomiting, altered mental status, HTNmental status, HTN
medications: NSAID, ACEI, analgesics, medications: NSAID, ACEI, analgesics, aminoglycosides, contrast, Chinese aminoglycosides, contrast, Chinese herbsherbs

Laboratory Laboratory InvestigationsInvestigations
Required:Required: Estimation of GFREstimation of GFR UrinalysisUrinalysis Albumin:Creatinine RatioAlbumin:Creatinine Ratio Renal ImagingRenal Imaging CBC, Electrolytes, Calcium, Phosphate, Bicarb, AlbuminCBC, Electrolytes, Calcium, Phosphate, Bicarb, Albumin
Potentially useful:Potentially useful: 24-hour Urine protein24-hour Urine protein Fasting GlucoseFasting Glucose Serum / Urine Protein ElectrophoresisSerum / Urine Protein Electrophoresis HIV and Hepatitis serologyHIV and Hepatitis serology Autoimmune serologiesAutoimmune serologies MR AngiographyMR Angiography
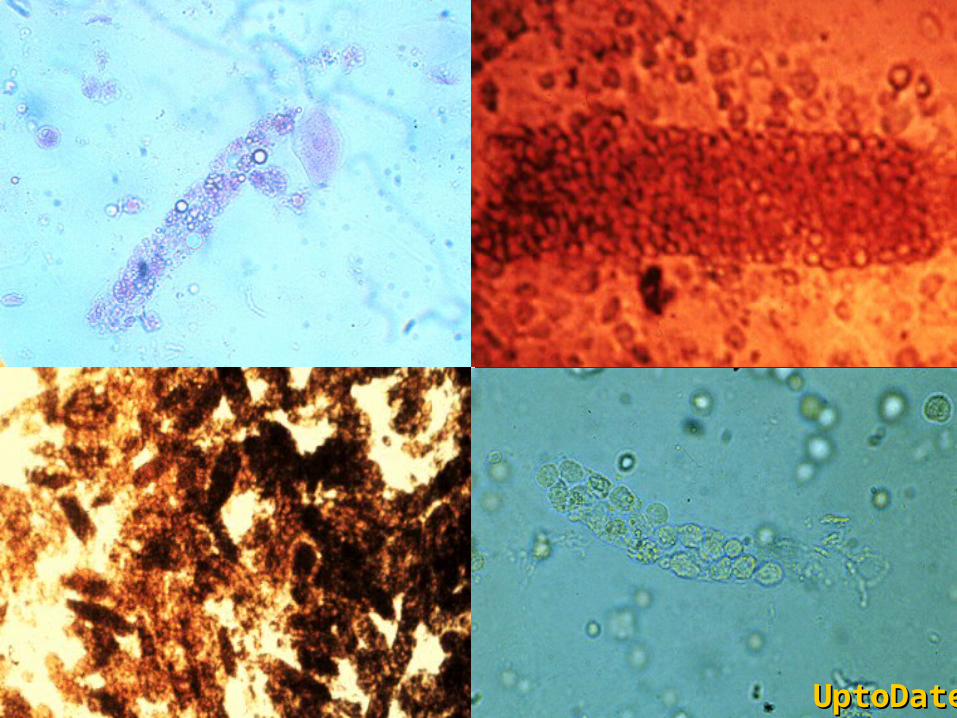
UptoDateUptoDate
Renal BiopsyRenal Biopsy
Should be considered:Should be considered: Ff noninvasive tests have failed to Ff noninvasive tests have failed to
establish a diagnosis in a patient with:establish a diagnosis in a patient with: Nephrotic syndrome (except in DM or Nephrotic syndrome (except in DM or
established amyloid)established amyloid) Non-nephrotic proteinuria if associated with Non-nephrotic proteinuria if associated with
renal dysfunctionrenal dysfunction Lupus nephritis (for dx and staging)Lupus nephritis (for dx and staging) Acute nephritic syndromeAcute nephritic syndrome Unexplained acute/ subacute renal failureUnexplained acute/ subacute renal failure
To direct and evaluate effectiveness of To direct and evaluate effectiveness of therapy therapy

Management of Renal Management of Renal DiseaseDisease
Treatment of Reversible CausesTreatment of Reversible Causes
Preventing or Slowing ProgressionPreventing or Slowing Progression
Treating and Preventing the Treating and Preventing the ComplicationsComplications
Identifying Individuals Requiring Identifying Individuals Requiring Renal Replacement TherapyRenal Replacement Therapy

Slowing ProgressionSlowing Progression
HypertensionHypertension
ACE inhibitors preferred because:ACE inhibitors preferred because: More potent antiproteinuric effect, More potent antiproteinuric effect,
especially in non-diabeticsespecially in non-diabetics Large body of evidence from RCTs (in Large body of evidence from RCTs (in
diabetics and non-diabetics)diabetics and non-diabetics) RRR 30% for progression to ESRDRRR 30% for progression to ESRD
Benefit persists in severe kidney Benefit persists in severe kidney diseasedisease

Management of Management of ComplicationsComplications
Coronary artery diseaseCoronary artery disease AnemiaAnemia Calcium and phosphate homeostasisCalcium and phosphate homeostasis Renal osteodystrophyRenal osteodystrophy Platelet dysfunctionPlatelet dysfunction Fluid overloadFluid overload Acidosis and hyperkalemiaAcidosis and hyperkalemia Decreased drug clearanceDecreased drug clearance

Referral to NephrologistReferral to Nephrologist
Late referral (< 12 months pre dialysis) is commonLate referral (< 12 months pre dialysis) is common Survey of Ontario Family MDs:Survey of Ontario Family MDs:
84% would not refer with creat 120-150 (>50% loss of 84% would not refer with creat 120-150 (>50% loss of GFR)GFR)
28% would not refer with creat 150-30028% would not refer with creat 150-300 almost all would refer with creat>300almost all would refer with creat>300
Consequences of referral shortly before dialysis:Consequences of referral shortly before dialysis: more complicationsmore complications longer hospitalization to initiate dialysislonger hospitalization to initiate dialysis more difficulty with initiation of dialysismore difficulty with initiation of dialysis worse survival!worse survival!
Better outcomes with early multidisciplinary careBetter outcomes with early multidisciplinary care
CMAJ 1999: 161:413-17

Canadian GuidelinesCanadian Guidelines Renal replacement therapy is NOT rationed Renal replacement therapy is NOT rationed
(i.e. everyone should be considered)(i.e. everyone should be considered) Reversible causes should be sought at Reversible causes should be sought at
diagnosisdiagnosis At least 1 year is required to prepare for At least 1 year is required to prepare for
dialysisdialysis Refer, at the latest, at Cr clearance of 30 Refer, at the latest, at Cr clearance of 30
ml/min, or Cr of 300ml/min, or Cr of 300 But…there are probably not enough But…there are probably not enough
nephrologists/ clinics to meet this demandnephrologists/ clinics to meet this demand Adequate communication with the Nephrologist Adequate communication with the Nephrologist
will allow proper stratification of patientswill allow proper stratification of patients
CMAJ 1999: 161:413-17
For AIMGP ClinicFor AIMGP Clinic
It is reasonable to follow stable renal failure It is reasonable to follow stable renal failure patients, and work up and manage appropriatelypatients, and work up and manage appropriately
Refer to nephrology when:Refer to nephrology when: Cr >300 or Cr clearance <30 ml/minCr >300 or Cr clearance <30 ml/min Renal biopsy indicatedRenal biopsy indicated Indicators of aggressive disease are present:Indicators of aggressive disease are present:
Rapid decline in creatinineRapid decline in creatinine homeostatic derangement i.e. acidosis, volume overload, high homeostatic derangement i.e. acidosis, volume overload, high
KK high protein excretionhigh protein excretion Difficult to control BPDifficult to control BP low HDLlow HDL black raceblack race
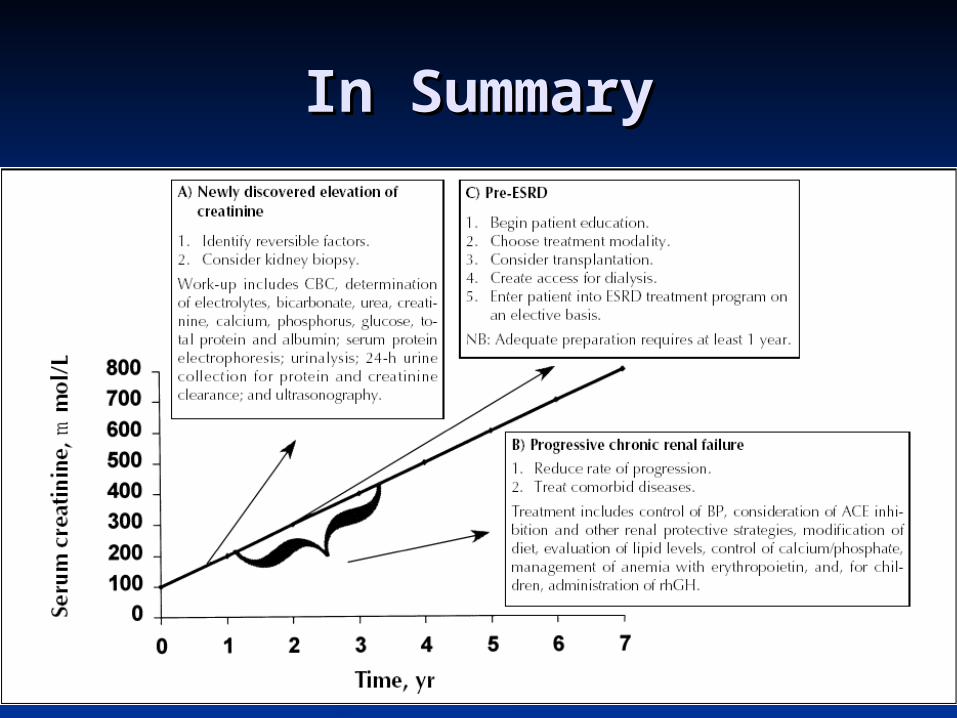
In SummaryIn Summary

Appoach To ProteinuriaAppoach To Proteinuria
Normal Protein Elimination:Normal Protein Elimination: < 150mg / day protein< 150mg / day protein < 30mg / day albumin< 30mg / day albumin
Classification of ProteinuriaClassification of Proteinuria TransientTransient OrthostaticOrthostatic PersistantPersistant

Glomerular barrier
tubule
• Normally, the larger proteins are excluded at the glomerular barrier
• Smaller proteins can pass, but are mostly reabsorbed

Mechanisms of Mechanisms of ProteinuriaProteinuria
Glomerular DysfunctionGlomerular Dysfunction Leakage of large proteins through Leakage of large proteins through
glomerular membrane and podocytesglomerular membrane and podocytes Transient (epinephrine and AII mediated)Transient (epinephrine and AII mediated)
FeverFever ExerciseExercise Congestive Heart FailureCongestive Heart Failure
PersistantPersistant Glomerular DiseaseGlomerular Disease
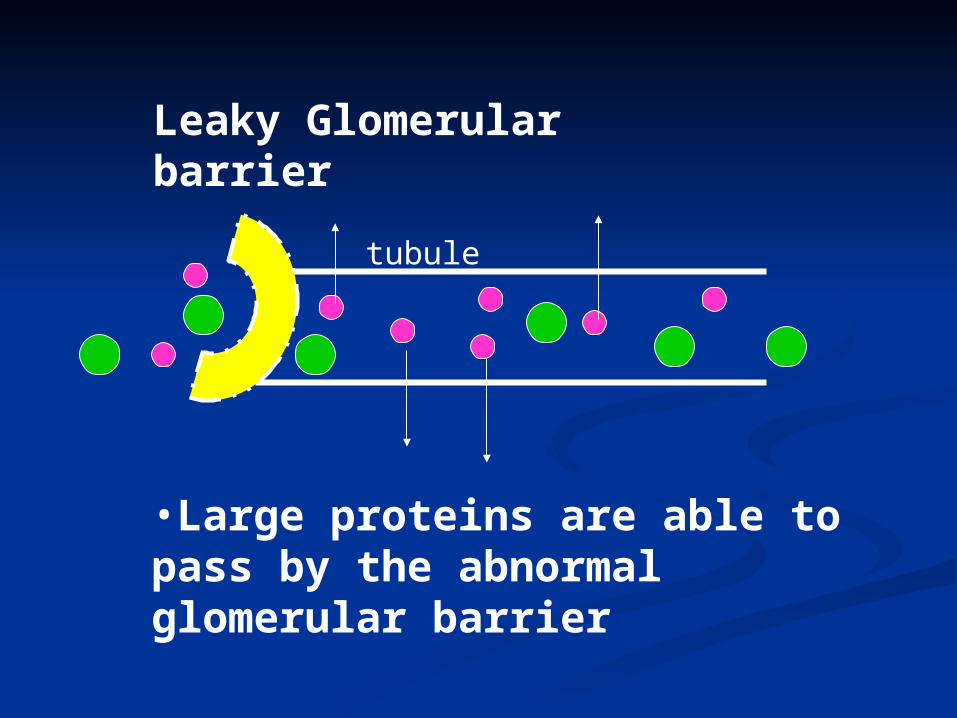
tubule
•Large proteins are able to pass by the abnormal glomerular barrier
Leaky Glomerular barrier
Mechanisms of Mechanisms of ProteinuriaProteinuria
Tubular DysfunctionTubular Dysfunction Inability of renal tubules to reabsorb Inability of renal tubules to reabsorb
small filtered proteinssmall filtered proteins Specific transporter dysfunctionSpecific transporter dysfunction
Eg Fanconi’s syndromeEg Fanconi’s syndrome Generalized tubular dysfunctionGeneralized tubular dysfunction
Progressive chronic renal failureProgressive chronic renal failure Interstitial DiseaseInterstitial Disease
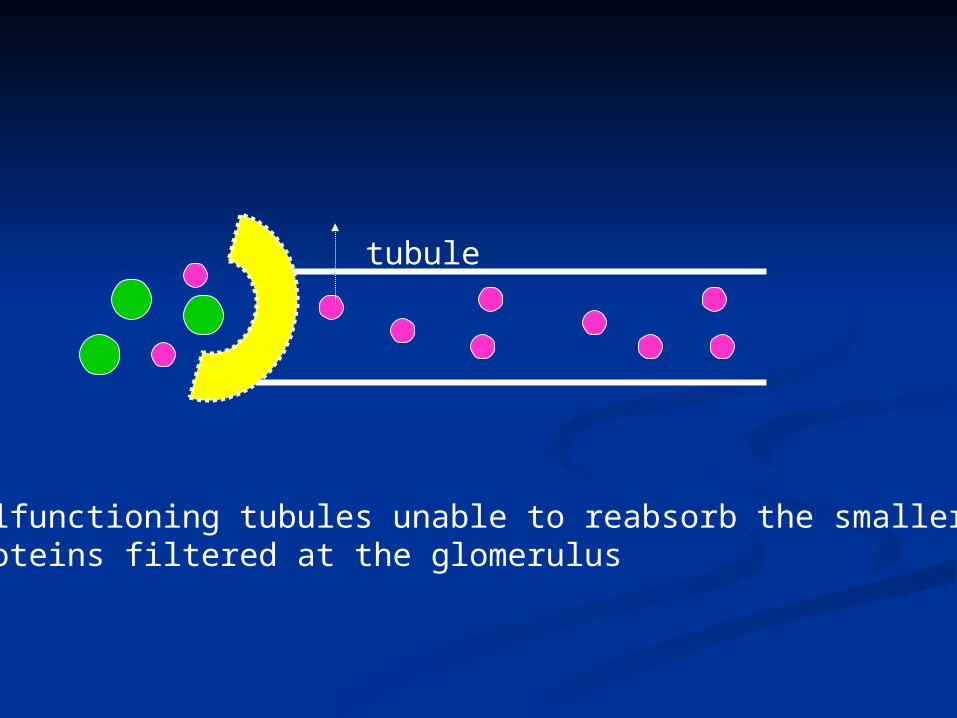
tubule
Malfunctioning tubules unable to reabsorb the smaller proteins filtered at the glomerulus

Mechanisms of Mechanisms of ProteinuriaProteinuria
Increased filtered protein loadIncreased filtered protein load Overwhelms ability of kidney to Overwhelms ability of kidney to
reabsorb proteinreabsorb protein
Increased GFR (mild proteinuria)Increased GFR (mild proteinuria) Pregnancy, feverPregnancy, fever
Increased filtered proteinIncreased filtered protein Myeloma, MGUSMyeloma, MGUS
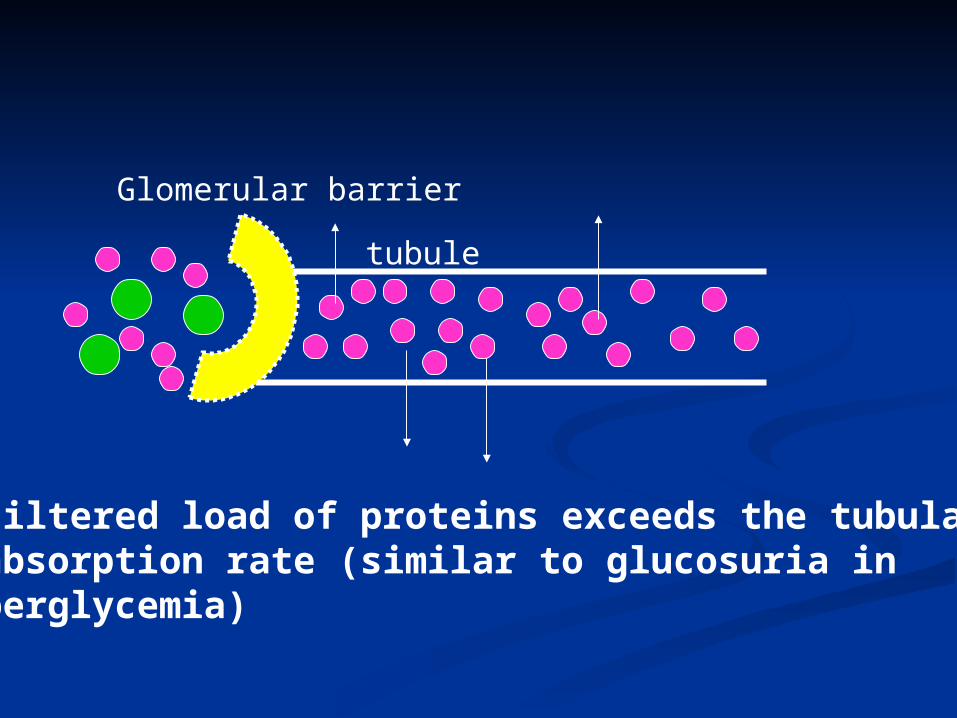
Glomerular barrier
tubule
• Filtered load of proteins exceeds the tubular reabsorption rate (similar to glucosuria in hyperglycemia)

Diagnostic ApproachDiagnostic Approach Step 1Step 1
Clinical Assessment (History and Physical) and Clinical Assessment (History and Physical) and examination of urinary sedimentexamination of urinary sediment
History: urinary symptoms, infections, rash, risk History: urinary symptoms, infections, rash, risk factors for HIV and hepatitis factors for HIV and hepatitis
Pmhx: Cancer, CHF, HTN, CTD, DMPmhx: Cancer, CHF, HTN, CTD, DM FHx: Alports, Fabry’sFHx: Alports, Fabry’s Drugs: NSAIDS, Gold, HeroinDrugs: NSAIDS, Gold, Heroin Physical exam: vitals, JVP, peripheral edema, Physical exam: vitals, JVP, peripheral edema,
ascites, rash, joint swellingsascites, rash, joint swellings

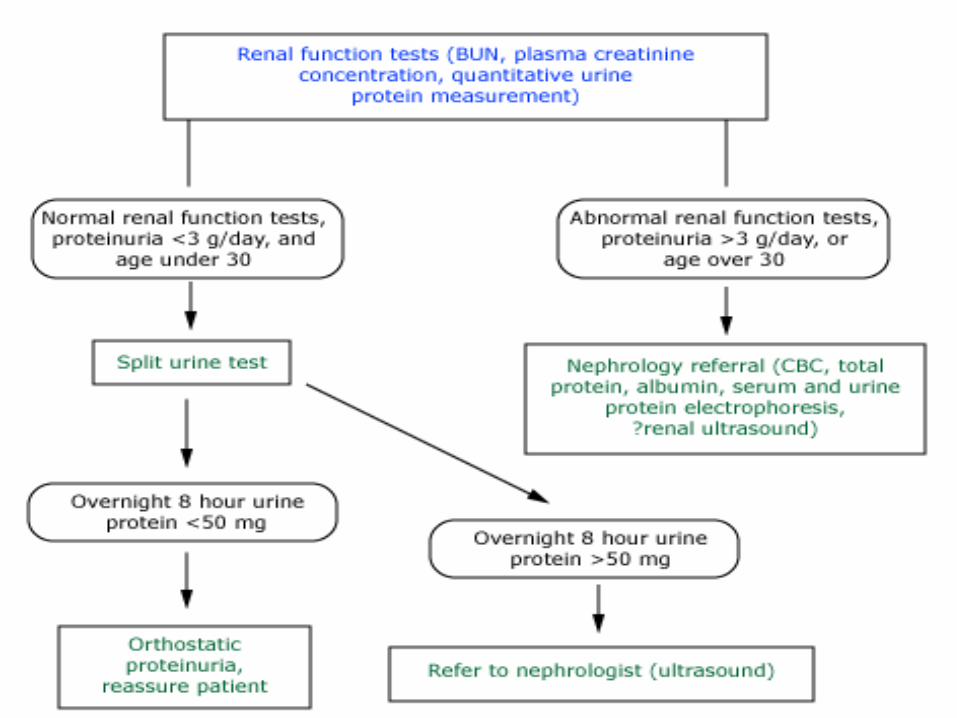
Diagnostic ApproachDiagnostic Approach
Rule out transient proteinuria with repeat Rule out transient proteinuria with repeat urinalysis:urinalysis: Fever, exercise, UTIFever, exercise, UTI
In young patients (age < 30) perform a In young patients (age < 30) perform a split urine collection (upright and supine) split urine collection (upright and supine) to exclude orthostatic proteinuriato exclude orthostatic proteinuria
If the above investigations are negative - If the above investigations are negative - STOPSTOP
Diagnostic ApproachDiagnostic Approach
Persistant proteinuria not due to a known Persistant proteinuria not due to a known underlying cause (eg CHF or diabetes) underlying cause (eg CHF or diabetes) requires further investigation for glomerular requires further investigation for glomerular and interstitial disease:and interstitial disease: 24h urine for protein or urine albumin:creatinine 24h urine for protein or urine albumin:creatinine
ratioratio Serum creatinine and estimation of GFRSerum creatinine and estimation of GFR CBC, electrolyes, Fasting blood sugarCBC, electrolyes, Fasting blood sugar Serum and urine protein electrophoresisSerum and urine protein electrophoresis Serology: Hep B, Hep C, HIV, ASOT, VDRLSerology: Hep B, Hep C, HIV, ASOT, VDRL ANA, Rheum factor, C3/C4, ANCAANA, Rheum factor, C3/C4, ANCA Renal Imaging (eg ultrasound)Renal Imaging (eg ultrasound) Malignancy screenMalignancy screen
Renal BiopsyRenal Biopsy
Indications for renal biopsy:Indications for renal biopsy: Diagnosis unclear andDiagnosis unclear and
Persistant proteinuria with > 3g / dayPersistant proteinuria with > 3g / day Increasing proteinuriaIncreasing proteinuria Declining GFRDeclining GFR
Prognosis and managementPrognosis and management Eg staging SLE nephritisEg staging SLE nephritis

SummarySummary Asymptomatic proteinuria is a common Asymptomatic proteinuria is a common
problemproblem
Initial investigations are targeted to rule Initial investigations are targeted to rule out transient, self-limited conditions and out transient, self-limited conditions and benign orthostatic proteinuriabenign orthostatic proteinuria
Persistent proteinuria, particularly Persistent proteinuria, particularly nephrotic range or associated with nephrotic range or associated with declining GFR, requires further declining GFR, requires further investigationinvestigation

ConclusionsConclusions
When evaluating a patient with a When evaluating a patient with a renal disorder:renal disorder: Identify and treat reversible causes of Identify and treat reversible causes of
renal failurerenal failure Initiate management to slow the decline Initiate management to slow the decline
in renal functionin renal function Manage coexisting conditionsManage coexisting conditions Have clear indications for when to refer Have clear indications for when to refer
to nephrology subspecialiststo nephrology subspecialists Organize an approach to asymptomatic Organize an approach to asymptomatic
proteinuriaproteinuria