approach to liver disease occurring during pregnancy naghshineh e.md
TRANSCRIPT

Approach to liver disease occurring during pregnancy
Naghshineh E .MD
Liver disease in pregnancy2
liver diseases that are specific to pregnancy, or multisystem diseases unique to pregnancy
pregnancy-related physiologic changes that may worsen the severity of, or predispose to hepatobiliary diseases
diseases that are unassociated with pregnancy but can occur during pregnancy
Pregnancy can also occur in women with underlying chronic liver disease

Liver disease in pregnancy3
THE LIVER DURING NORMAL PREGNANCY
• Physical examination — Spider angiomas and palmar erythema

Liver disease in pregnancy4
• Ultrasound examination :Fasting gallbladder volume and residual volume after contraction may be increased
• Pathology• Serum proteins and lipids : albumin , Serum
total cholesterol and triglyceride
Liver disease in pregnancy5
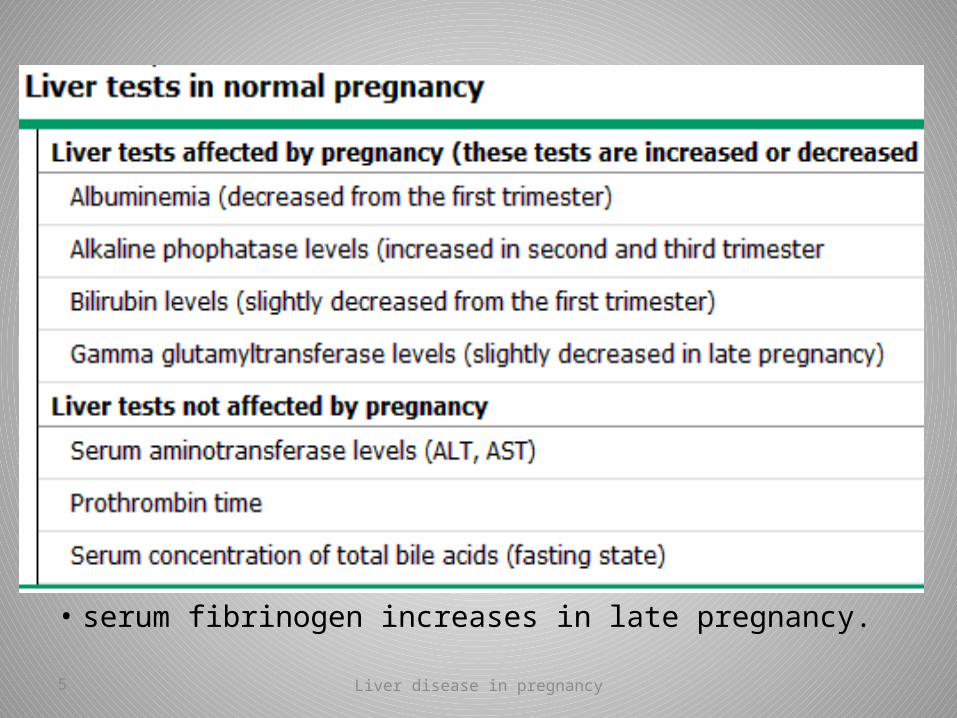
• serum fibrinogen increases in late pregnancy.

Liver disease in pregnancy6
• Hyperemesis gravidarum• Intrahepatic cholestasis of pregnancy• Acute fatty liver of pregnancy• HELLP• preeclampsia

Liver disease in pregnancy7
PATTERNS OF HEPATOBILIARY DISEASE IN PREGNANCY
• jaundice• Pruritus• abdominal pain• nausea, vomiting• liver biochemical test abnormalities
Liver disease in pregnancy8
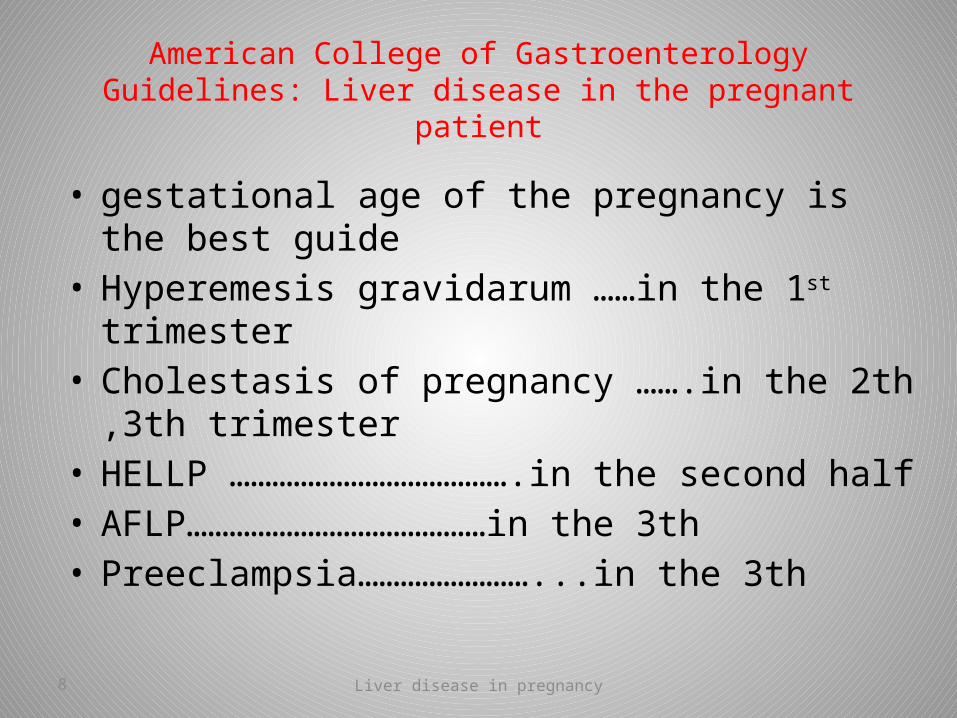
American College of Gastroenterology Guidelines: Liver disease in the pregnant patient
• gestational age of the pregnancy is the best guide• Hyperemesis gravidarum ……in the 1st trimester• Cholestasis of pregnancy …….in the 2th ,3th trimester• HELLP ………………………………….in the second half • AFLP……………………………………in the 3th• Preeclampsia……………………...in the 3th

Liver disease in pregnancy9
Evaluation of liver disease in pregnancy
Liver disease in pregnancy10
Case 1
• A 26-year-old woman gravida 3 para 2 currently in her 10th week with a singleton gestation is hospitalized with intractable nausea, vomiting, and dehydration
• During her two prior pregnancies, she also had severe nausea and vomiting, which resolved early in the second trimester.

Liver disease in pregnancy11
• Her physical examination is notable for dry mucus membranes, and a gravid uterus
• She has no abdominal pain, and does not have a palpable liver or spleen
Liver disease in pregnancy12
What is your first diagnosis?

Liver disease in pregnancy13
• ALT (175 IU/L), AST (122 IU/L), serum total bilirubin (2.1 mg/dL)
• Amylase and lipase are normal• The albumin is slightly decreased from normal
values• Liver biochemical tests prior to pregnancy are
not available• A right upper quadrant ultrasound is normal. • Urinalysis shows elevated ketones.

Liver disease in pregnancy14
• Serology for hepatitis A, B, and C is negative, • antinuclear antibodies are absent, and serum
protein electrophoresis is normal • TSH is normal• Obstetrical ultrasound examination
demonstrates a normal singleton gestation.

Liver disease in pregnancy15
• patient's clinical course and occurrence of symptoms early during pregnancy are consistent with hyperemesis gravidarum

Liver disease in pregnancy16
• Common criteria for diagnosis of hyperemesis are persistent vomiting accompanied by weight loss exceeding 5 percent of prepregnancy body weight and ketonuria unrelated to other causes

Liver disease in pregnancy17
• Abnormal liver enzyme values occur in approximately 50 percent
• The most striking abnormality is an increase in serum aminotransferases
• in the low hundreds or two to three times the upper limit of normal, and rarely as high as 1000 U/L
• Hyperbilirubinemia can occur, but rarely exceeds 4 mg/dL

Liver disease in pregnancy18
• Serum amylase and lipase may increase as much as 5-fold (as opposed to a 5- to 10-fold increase in acute pancreatitis) and are of salivary rather than pancreatic origin

Liver disease in pregnancy19
• Preeclampsia, HELLP syndrome and acute fatty liver of pregnancy are also causes of pregnancy-related nausea and vomiting, but :
onset is in the latter half of pregnancy (usually the third trimester)
hypertension is usually present thrombocytopenia is common
Liver disease in pregnancy20
Case 2
• A 23-year-old woman gravida 2 para 1 currently at 35 weeks with a singleton gestation is referred from a dermatologist for intractable itching
• The itching is primarily on the palms of her hands and soles of her feet
• It is present day and night, and keeps her from sleeping.

Liver disease in pregnancy21
• The patient also had itching during her first pregnancy in which the fetus died in utero in the third trimester

Liver disease in pregnancy22
What is your first diagnosis?

Liver disease in pregnancy23
Intrahepatic cholestasis of pregnancy
• Intrahepatic cholestasis of pregnancy (ICP) occurs in the second and third trimester
• is characterized by pruritus and an elevation in serum bile acid concentrations
• For unknown reasons the disease is seen more commonly in the
colder months

Liver disease in pregnancy24
PATHOGENESIS
• The cause of ICP is unknown but genetic, hormonal, and environmental factors are likely involved

Liver disease in pregnancy25
Estrogens and progesterone
• It is recommended that progesterone treatment be avoided in pregnant women with a previous history of ICP and immediately withdrawn when cholestasis occurs during pregnancy

Liver disease in pregnancy26
CLINICAL MANIFESTATIONS
• Pruritus may precede laboratory abnormalities • Abdominal pain is uncommon• Encephalopathy or other stigmata of liver failure are
unusual • Physical examination is nonspecific• may show excoriations due to scratching• Jaundice occurs in less than 10 percent
Liver disease in pregnancy27
Laboratory findings
• Serum total bile acid concentrations increase in ICP, and may be the first or only laboratory abnormality
• Serum cholic acid increases more than chenodeoxycholic acid
• most women with an elevated bile acid ratio also have elevated total bile acid levels; as a result, obtaining a ratio does not enhance diagnostic performance
• The ratio of glycine/taurine conjugates is decreased

Liver disease in pregnancy28
• elevations in alkaline phosphatase, 5' nucleotidase, and total and direct bilirubin concentrations
• Total bilirubin levels rarely exceed 6 mg/dL• gamma glutamyl transpeptidase (GGT) are normal or
modestly elevated• aminotransferases may reach values greater than
1000 U/L• The prothrombin time is usually normal• prolonged prothrombin times reflect vitamin K
deficiency due to cholestasis or to the use of bile acid sequestrants rather than liver dysfunction.

Liver disease in pregnancy29
ULTRASONOGRAPHY
• the biliary ducts are not dilated and hepatic parenchyma appears normal

Liver disease in pregnancy30
DIAGNOSIS
• Most women are diagnosed during the second or third trimester
• The diagnosis of ICP is based upon the presence of pruritus associated with elevated total serum bile acids levels and/or aminotransferases

Liver disease in pregnancy31
PATHOLOGY
• is rarely necessary for the diagnosis• histopathology is characterized by cholestasis
without inflammation • Bile plugs in hepatocytes and canaliculi
predominate in zone 3• The portal tracts are unaffected.

Liver disease in pregnancy32
TREATMENT
• UDCA is considered as the first line treatment for ICP(500 BID or 300 TDS)
• Hydroxyzine (25 to 50 mg/day)• Cholestyramine (8 to 16 g/day)

Liver disease in pregnancy33
Complications of cholestasis
• hypoprothrombinemia induced by vitamin K deficiency; should be treated before delivery to prevent hemorrhage.

Liver disease in pregnancy34
• Cholestasis recurs during subsequent pregnancies in 60 to 70 percent
• increased risk for gallstones• some women who develop ICP have underlying liver
disease :
women in whom ICP is suspected and/or who have elevated serum aminotransferase during pregnancy should be tested for chronic hepatitis (especially hepatitis C)
liver function tests should be checked several months after the delivery

Liver disease in pregnancy35
Hormonal contraception
• contraceptives with a low dose of estrogen can be initiated after normalization of liver function tests
• check liver function tests after three or six months of such contraception.

Liver disease in pregnancy36
FETAL FOLLOW-UP AND OUTCOME
• In contrast to the favorable prognosis for mothers, ICP carries significant risk for the fetus
• fetal prematurity• meconium stained amniotic fluid• intrauterine demise• neonatal respiratory distress syndrome

Liver disease in pregnancy37
Timing of delivery
• 37 wk
• 35-37 wk :• Severe itching• Jaundice• Prior fetal death

Liver disease in pregnancy38
Case 3• A 32 year-old woman gravida 1 para 0 with a
singleton gestation at 34 weeks of gestation is admitted to the hospital with a three-day history of nausea and vomiting, malaise, and jaundice
• Her blood pressure is mildly elevated• Urinalysis shows trace protein• aminotransferases range between 200 to 500 • glucose is in the low-normal range• White blood cell count and prothrombin time are
elevated
Liver disease in pregnancy39
•What is your diagnosis ?

Liver disease in pregnancy40
Acute fatty liver of pregnancy
• characterized by microvesicular fatty infiltration of hepatocytes, is a disorder which is unique to human pregnancy
• early diagnosis and prompt delivery have dramatically improved the prognosis, and maternal mortality should now be the exception rather than the rule

Liver disease in pregnancy41
EPIDEMIOLOGY
• is rare with an approximate incidence of 1 in 7000 to 1 in 20,000 deliveries
• It is more common with multiple gestations and possibly in women who are underweight.

Liver disease in pregnancy42
CLINICAL MANIFESTATIONS
• Acute fatty liver occurs typically in the third trimester• The disease is always present before delivery,
although it is not always diagnosed prior to delivery
• Symptom?

Liver disease in pregnancy43
• The most frequent initial symptoms are nausea or vomiting 75 percent
• abdominal pain :50 percent• Anorexia• Jaundice• one-half of patients have signs of preeclampsia at
presentation or at some time during the course of illness

Liver disease in pregnancy44
• infection • major intraabdominal bleeding• Transient polyuria and polydipsia due to
central diabetes insipidus • pancreatitis, which can be severe. Pancreatitis
generally becomes apparent only after development of hepatic and renal dysfunction
Liver disease in pregnancy45
Laboratory tests • aminotransferase ranging from modest values up to
1000 • Serum bilirubin levels are also usually elevated• The platelet count may be decreased with or without
other signs of disseminated intravascular coagulation (DIC)
• Severely affected patients also have elevations in serum ammonia, prolongation of prothrombin time, and hypoglycemia caused by hepatic insufficiency
• Acute renal failure and hyperuricemia are often present

Liver disease in pregnancy46
DIAGNOSIS
• made clinically based upon the setting, presentation, and compatible laboratory and imaging results
• Laboratory tests that are helpful include serum aminotransferases, serum bilirubin, coagulation studies, electrolytes, serum glucose, uric acid level and creatinine, and a white blood cell count.

Liver disease in pregnancy47
TREATMENT AND COURSE
• the primary treatment is prompt delivery, usually emergently, after maternal stabilization

Liver disease in pregnancy48
• Maternal stabilization requires glucose infusion and reversal of coagulopathy
• Attention should be paid to the women's overall fluid status because the low plasmatic oncotic pressure can lead to pulmonary edema
• Hypoglycemia is common and all patients should have glucose monitored until normal liver function returns

Liver disease in pregnancy49
• The liver tests and coagulopathy usually start to normalize shortly after delivery
Liver disease in pregnancy50
RECURRENCE
• Acute fatty liver can recur in subsequent pregnancies
Liver disease in pregnancy51
Case 4
• A 23-year-old woman gravida 1 para 0 currently with twin gestations at 32 weeks is hospitalized with hypertension, for which methyldopa had been prescribed earlier in her pregnancy
• Despite treatment, she continues to be mildly hypertensive and is developing a progressive rise in serum aminotransferases, which are over 85
• Hepatitis serology and markers for autoimmune hepatitis are negative. Her platelet count, peripheral blood smear, urinalysis, and right upper quadrant ultrasound are normal
Liver disease in pregnancy52
• The differential diagnosis in this case includes:
• preeclampsia• toxicity due to methyldopa • early acute fatty liver of pregnancy
Liver disease in pregnancy53
HELLP syndrome
• characterized by hemolysis with a microangiopathic blood smear, elevated liver enzymes, and a low platelet count
• 15 to 20 percent of affected patients do not have antecedent hypertension or proteinuria

Liver disease in pregnancy54
INCIDENCE AND ONSET OF DISEASE
• HELLP develops in approximately 1 to 2 per 1000 pregnancies overall and in 10 to 20 percent of women with severe preeclampsia/eclampsia
• The majority of cases are diagnosed between 28 and 36 weeks of gestation
Liver disease in pregnancy55
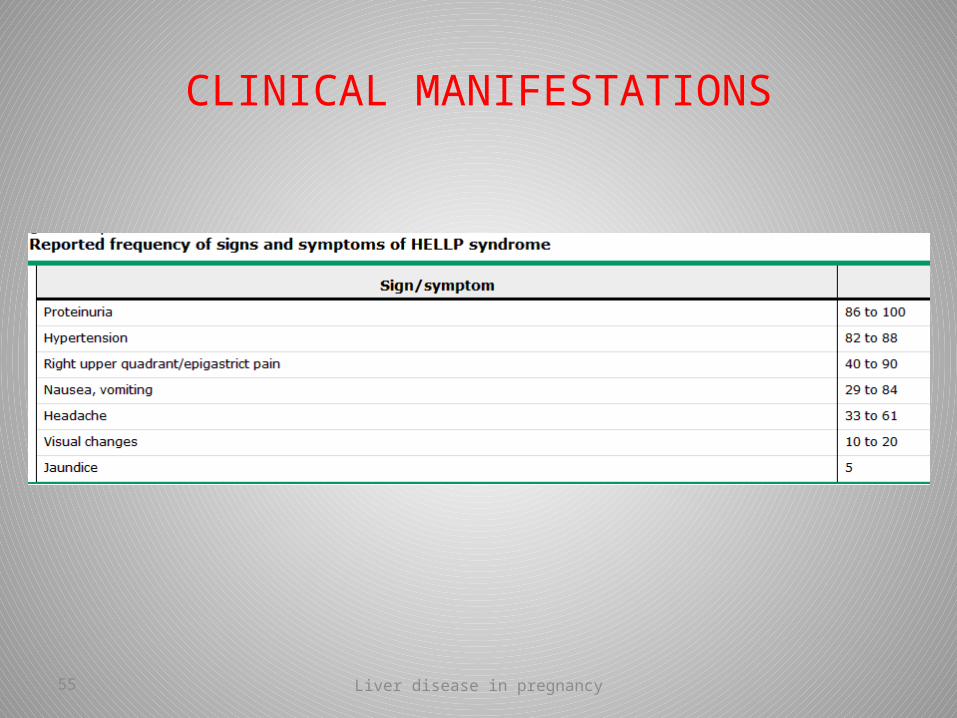
CLINICAL MANIFESTATIONS

Liver disease in pregnancy56
• Symptoms typically develop in the third trimester, (second trimester or postpartum disease )
• The most common clinical presentation is abdominal pain and tenderness in the midepigastrium, right upper quadrant, or below the sternum
• nausea, vomiting, and malaise• Hypertension (blood pressure ≥140/90) and
proteinuria
Liver disease in pregnancy57
• Serious maternal morbidity may be present at initial presentation or develop shortly thereafter
disseminated intravascular coagulation (DIC)abruptio placentaeacute renal failurepulmonary edemasubcapsular liver hematomaretinal detachment
Liver disease in pregnancy58
• Microangiopathic hemolytic anemia• signs suggestive of hemolysis include an elevated
indirect bilirubin and a low serum haptoglobin concentration (≤25 mg/dL).
• Platelet count ≤100,000 cells/microL• Total bilirubin ≥1.2 mg/dL• Serum AST ≥70 IU/L.
Liver disease in pregnancy59
MANAGEMENT
• The cornerstone of therapy is delivery
Pregnancies ≥34 weeks of gestationNonreassuring tests of fetal status (eg, biophysical
profile, fetal heart rate testing)Presence of severe maternal disease: multiorgan
dysfunction, DIC, liver infarction or hemorrhage, renal failure, or abruptio placenta.

Liver disease in pregnancy60
Platelet transfusion
• significant maternal bleeding (spontaneous or from surgical incisions)
• less than 20,000 cells/microL• preoperative platelet count greater than
40,000 to 50,000 cells/microL

Liver disease in pregnancy61
NVD OR CS?
• cesarean delivery is probably preferable in pregnancies less than 30 to 32 weeks of gestation if the cervix is unfavorable for induction
Liver disease in pregnancy62
Role of dexamethasone
• PLT< 100000 ???

Liver disease in pregnancy63
chronic liver disease
• Pregnancy is unusual in women with severe chronic liver disease. Most such women are not of child-bearing age, or, because of the associated anovulatory state, they are infertile
Liver disease in pregnancy64
CIRRHOSIS AND PORTAL HYPERTENSION
• Some women with cirrhosis can sustain pregnancy without any worsening of hepatic function
• others may develop jaundice with progressive liver failure, ascites, and hepatic coma

Liver disease in pregnancy65
• The increase in total blood volume associated with pregnancy may worsen pre-existing portal hypertension
• upper endoscopy to look for varices before pregnancy

Liver disease in pregnancy66
Hepatitis B virus
• Pregnancy is generally well tolerated by women who are chronic carriers of hepatitis B virus
• The overall risk of HBV transmission from the mother to infant is about 40 percent.
• Transmission at birth is more likely if the mother is hepatitis B e antigen (HBeAg) positive or has high circulating levels of HBV DNA
• Prenatal screening of all pregnant women for HBsAg is now performed routinely in many countries

Liver disease in pregnancy67
Hepatitis C virus
• Women chronically infected with hepatitis C virus (HCV) can have an uneventful pregnancy without worsening of liver disease or other adverse effects on the mother or fetus
• Transmission of the virus from mother to infant occurs in about 5 to 10 percent of infants born to anti-HCV positive women
• no evidence that breastfeeding is a risk for infection

Liver disease in pregnancy68
THANK YOU