approach to large airway obstruction in childrenold.criticalcare.org.za/images/presentations/pierre...
TRANSCRIPT

Approach to large airway
obstruction in children
Pierre Goussard, Robert Gie
Tygerberg Children`s Hospital. University
of Stellenbosch
• Children with large airway obstruction can
be asymptomatic and only becomes
symptomatic during intercurrent infections
• Presentation can either be acutely or
chronic depending on the eitiology
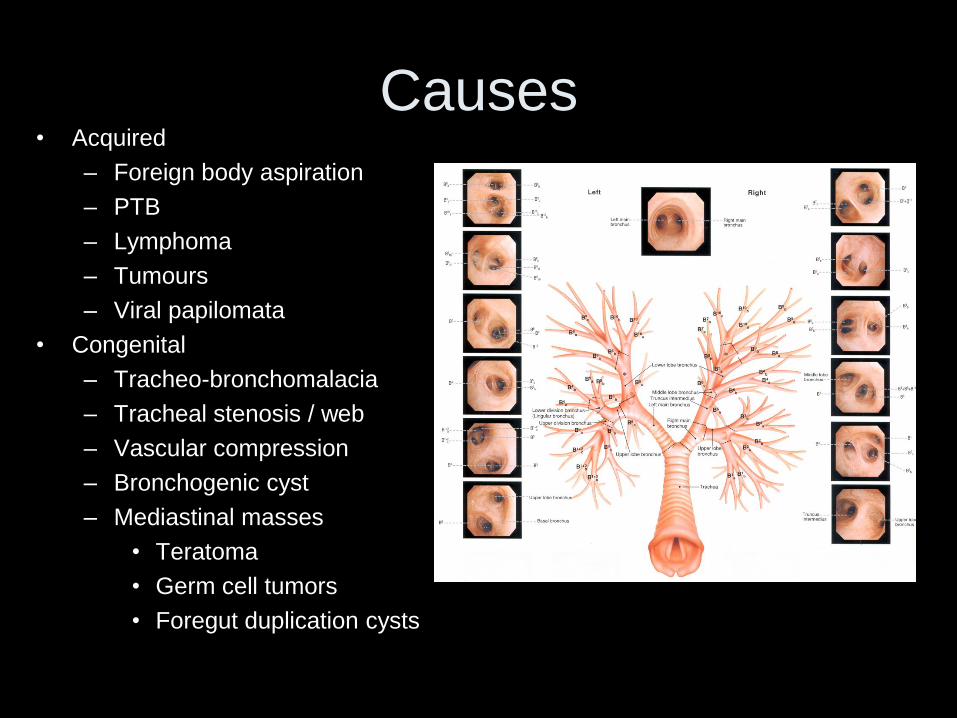
Causes• Acquired
– Foreign body aspiration
– PTB
– Lymphoma
– Tumours
– Viral papilomata
• Congenital
– Tracheo-bronchomalacia
– Tracheal stenosis / web
– Vascular compression
– Bronchogenic cyst
– Mediastinal masses
• Teratoma
• Germ cell tumors
• Foregut duplication cysts


History
• When did symptoms start
– Present since birth
– Noisy breathing
– Worse with infection
– Acute onset
• Other symptoms associated with airway
obstruction
– Swallow and feeding problems
– Apnea episodes

Signs and symptoms
• Children with airway narrowing present with signs of airway obstruction which do not respond to bronchodilators
• Symptoms varies according to the degree of airway obstruction.
• Children frequently present with a persistent unremitting cough. As the disease progress the cough will become more prominent and can become brassy or bifonal, often with associated large airway wheezing or stridor.

• Classically, large intrathoracic airway obstruction presents with monophonic wheezing
• Wheeze is harsh and low pitched and audible without an stethoscope.
• Hyperinflation and subcostal retraction are not as prominent as in small airway obstruction.
• Audible on one side of the chest or on both sides depending on the area and the degree of obstruction.
• This clinical presentation is often confused with asthma, but these children will not respond to inhalation steroids and the airway obstruction might be worsened by the use of β2 agonist
Finder JD. J Pediatr 1997;130: 59- 66

Chest x-ray
• Previous x-rays
• Airways visible on x-rays
• Mediastinal mass or lymphnodes around
airways
• Movement of trachea : to left always
abnormal
• Ball valve effects
• Dilated esophagus
Tools for diagnosis
• Chest X-ray
• Tracheo-bronchogram
• Barium studies
• Lung funtions
• Bronchoscopy
• Chest CT-scan
• FDG- scan
• MR
• Echo

Airway compression
Chest X-ray

Ball-valve effect :airway obstruction
• Outside lumen : TB glands
Lymphoma
Bronchogenic cyst
Vascular compression
• Luminal obstruction : Foreign body
Tumor
• Lumen wall : Bronchomalacia

Tracheo- bronchogram

Esophageal compression from posterior

Bronchoscopy
Anterior tracheal compression
by inominate artery Foreign body in bronchus intermedius

FDG CT-scan
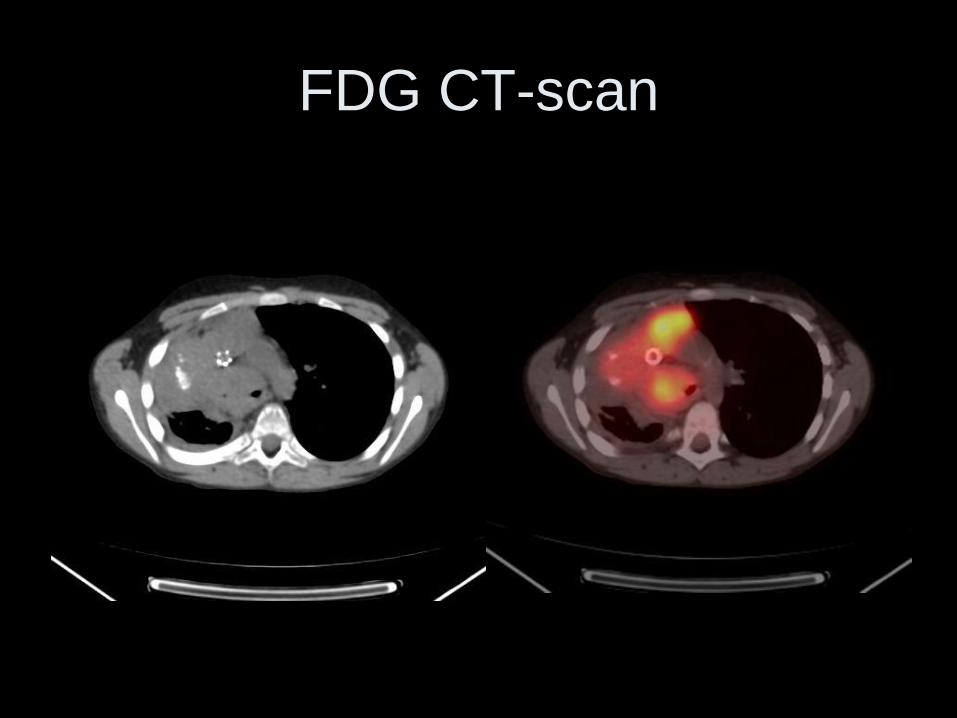
FDG CT-scan

MR: Fig a: Large cystic hygroma causing airway compression.
Fig b: Follow up MR after injection of bleomycin
a b
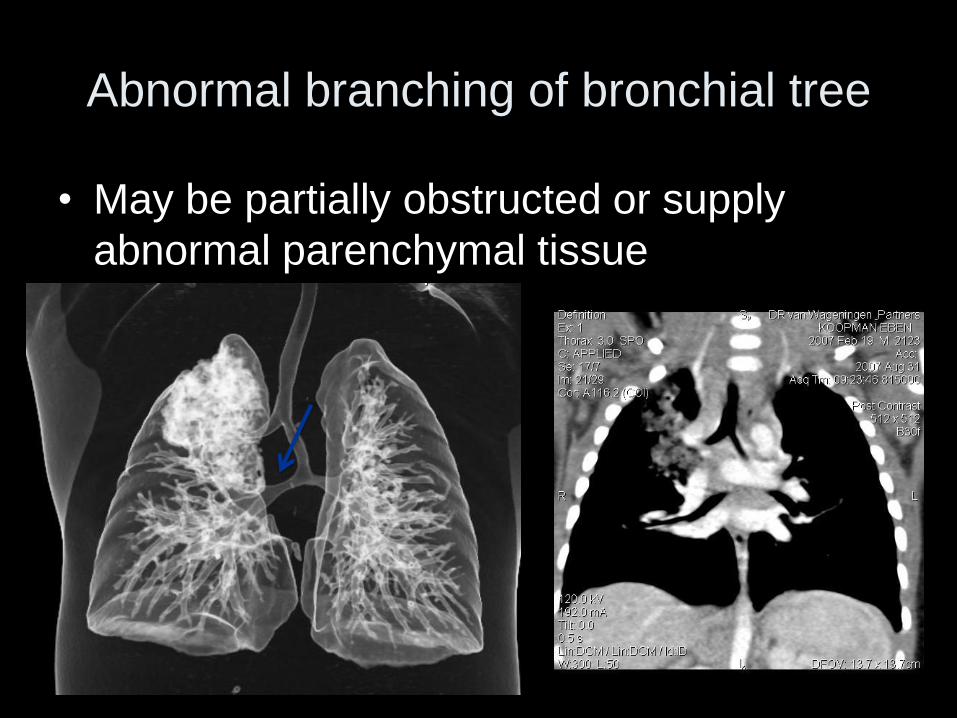
Abnormal branching of bronchial tree
• May be partially obstructed or supply
abnormal parenchymal tissue
Acquired causes of airway
obstruction in children

Acquired causes
Lymphoma causing and anterior mediastinal mass with severe airway
compression of the trachea
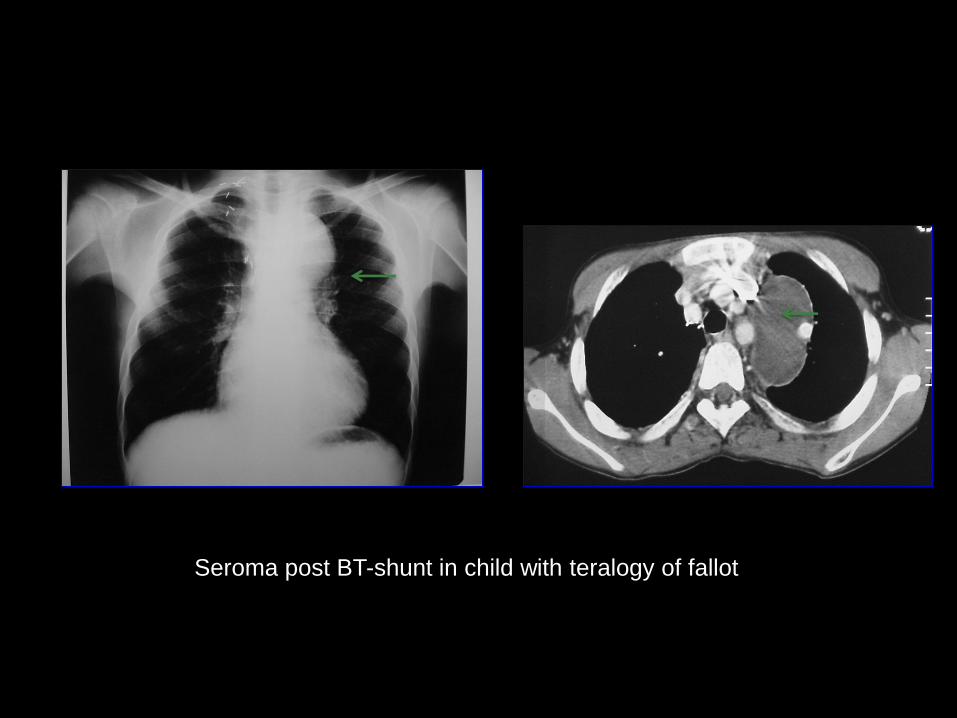
Seroma post BT-shunt in child with teralogy of fallot
PTB
• Lymph gland disease involving the airways is common
following primary infection in children younger than 5
years of age where the small airway size makes young
children vulnerable
• The exact incidence of children with airway obstruction
due to primary tuberculosis in the chemotherapeutic era is
not known.
• The incidence of complicated lymph node disease in 2
recent reports varied from 8-38% in children less than 15
years of age.
Marais BJ. Int J Tubercle Lung Dis. 2006 10:1-7.

• During adequate anti-tuberculosis treatment the
size of the lymph nodes may increase and airway
obstruction worsen. This has also been seen in
children on TB and anti- retroviral drugs
• Luminal involvement of the airway is very rare in
children. In these cases the lumen of the airway is
involved and airway disease is not caused by
external compression or because glands have
herniated into the airways
Fishman JE. AJR 2000;174;43 – 49

Clinical Presentation
• Depends on– The degree of airway narrowing
– Whether infected gland has infiltrated the airway wall,
– Herniated into the lumen and discharged caseous material into the lumen of the airway.
• Progression– As the obstruction increases, a ‘ball valve effect’ which leads to
an unilateral hyperinflation of the lobe or lung can develop.
– If the obstruction is complete collapse of a lobe or segment of a lobe occurs.
– Ulceration of the lymph gland into the airway can lead to inhalation of tuberculous material.

Chest x-ray appearance of PTB
1. Airway compression
2. Unilateral hyperinflation
3. Expansile pneumonia

• The most important groups of glands are located in the paratracheal and subcarinal regions.
• In young infants the only sign of enlarged lymph nodes is the visualization of airway compression on the chest radiograph
• As the trachea in a child normally deviates to the right ,deviation to the left indicated pathology.
• Subcarinal glands can be detected directly or indirectly. – The direct signs on chest radiograph includes a double shadow below
the carina and a shift to the right of the para-oesophageal adhesion line.
– The indirect signs is compression of both main bronchi
• Collapse will be visible on chest x-rays if the external compression of the lumen is complete or if glands have herniated into the airway. – Bronchus intermedius is a common region for the complete airway
obstruction resulting in collapse of the right middle and the right lower lobes.
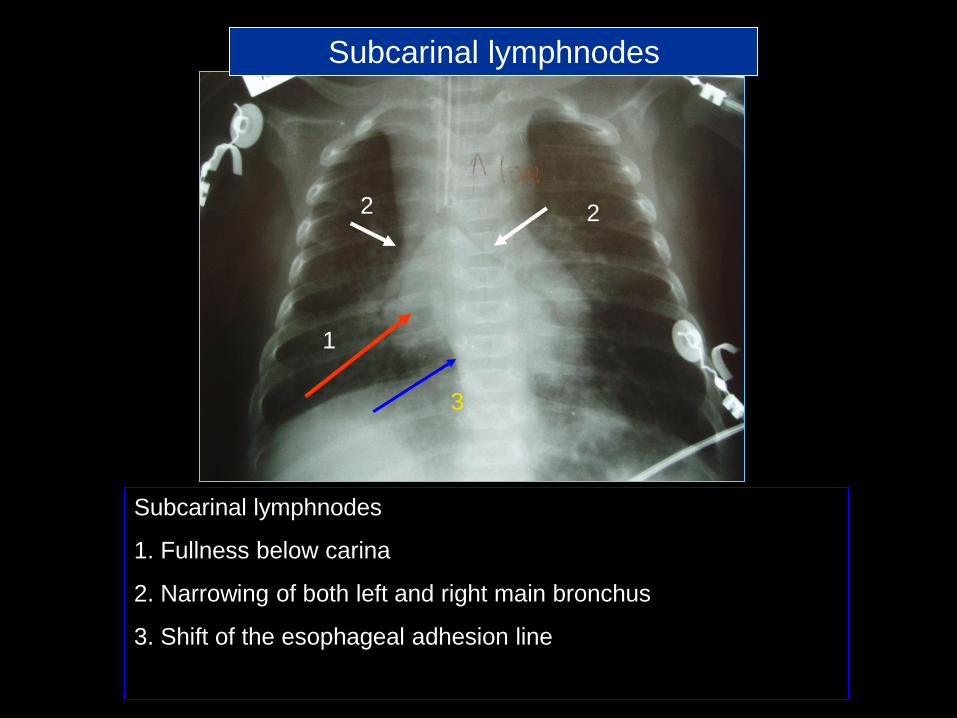
Subcarinal lymphnodes
1. Fullness below carina
2. Narrowing of both left and right main bronchus
3. Shift of the esophageal adhesion line
1
22
3
Subcarinal lymphnodes

Computer tomography scan
appearances.• Indications
– In children with clinically and radiological significant airway compression to determine the location of glandular involvement and the relationship of these glands to the airways.
– Useful to determine the nature of mediastinal glands and to demonstrate the ghost like enhancement of the rims of the lymph glands after contrast administration
– The most common location for lymph gland enlargement in children is the subcarinal (90%), right hilar (74%), left hilar (72%), bilateral hilar (61%), anterior mediastinum (79%), precarinal (64%) and the right paratracheal position (63%) .
Andronikou S. Ped Radiology 2004;34:232-236

Chest CT-scan

Bronchoscopy findings
• The most common reported bronchoscopic
finding are extrinsic compression (37%) of the
bronchi or the tracheal.
• Bronchial involvement , granulation tissue,
obstructing caseating material and mucosal
inflammation was found in 48% of children
without detectable lymph gland enlargement on
the chest x-rays.
de Blic J. Chest 1991; 100: 688–692

Tracheal compression Gland herniating into airway
Bronchus intermedius obstruction

Bronchomalasia
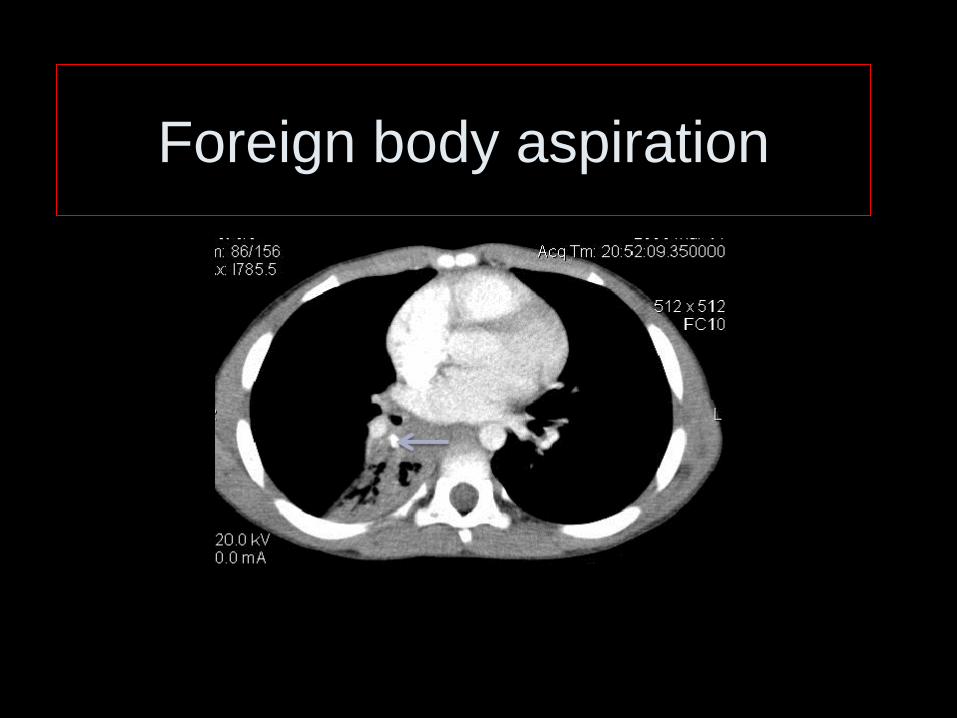
Foreign body aspiration



Virus papilomata

Post intubation tracheal stenosis

Tracheal tumor
Congenital causes of airway
obstruction in children


Bronchoscopy
Pulsatile compression of the posterior(black arrow) and lateral wall
(green arrow) of the trachea can be seen on bronchoscopy.

Ct- scan: Double aortic arch visible, posterior of trachea

Inmominate arterial compression

Four patterns of vascular-induced
esophageal indentations
1. Anterior tracheal, posterior esophageal indentations
– vascular ring
2. Normal tracheal , posterior esophageal indentation
– Aberrant subclavian artery
3. Posterior tracheal , anterior esophageal indentation
– Pulmonary sling
4. Anterior tracheal indentation , normal esophageal
– Inmominate arterial compression

Left Pulmonary Sling

• Vascular compression of the airways were
observed in 13% - 26% of children , who
underwent bronchoscopy for persistent
wheezing , stridor and apnea
• 11 -15 % of persistently wheezing children
in whom bronchoscopy was performed had
bronchomalacia or narrowing of the left
main-stem bronchus
1. Wood RE . Pediatric Clin North Am. 1984; 785 -799
2. Filston HC . Ann Surg. 1987; 205 ; 541 -549

Lower airway abnormalities in
Down`s syndrome• Tracheal stenosis
• Tracheomalacia
• Tracheal bronchus
• Bronchomalacia
• Vascular compression because of CHD
Ignacio Sa´nchez : Pediatr Pulmonol. 2003; 35:288–291

Congenital tracheal stenosis
Congenitale causes

Tracheal bronchus
• Tracheal bronchus was described by Sandifort in 1785 as a
right upper bronchus originating in the trachea
• Congenital anomaly in which the right upper lobe has its origin
in the trachea rather than distal to the carina.
• Tracheal bronchi occur almost exclusively on the right trachea
and are associated with other congenital anomalies, particularly
trisomy 21
• Right tracheal bronchus has a prevalence of 0.1%–2% and left
tracheal bronchus a prevalence of 0.3%–1% in bronchographic
and bronchoscopic studies

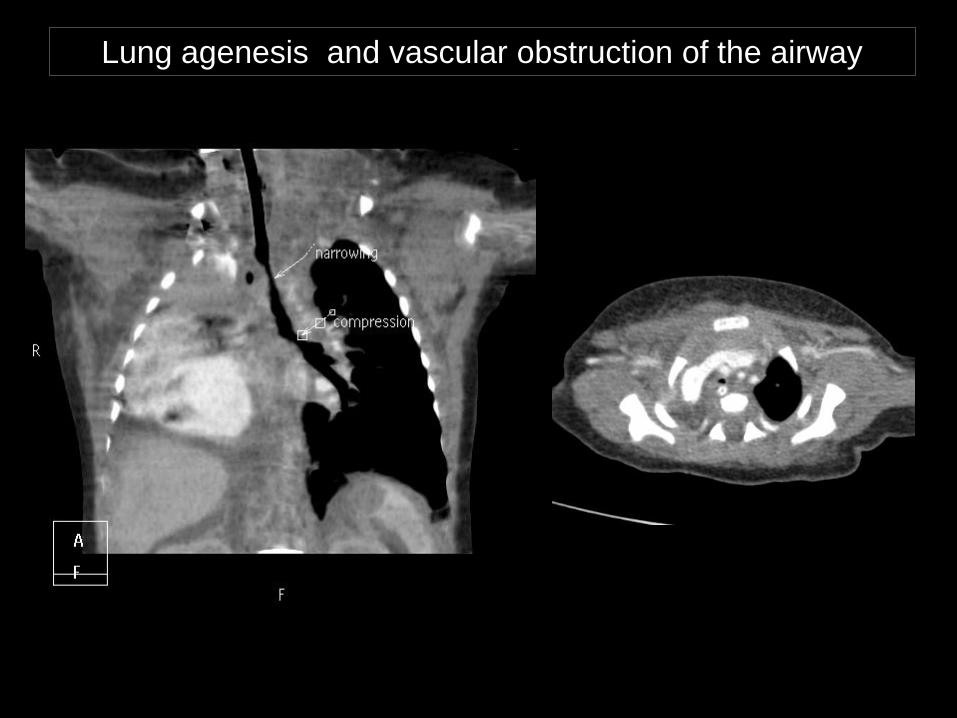
Lung agenesis and vascular obstruction of the airway


Large airway obstruction in HIV positive children
• PTB
• Lymphoma
• Cryptococcus
• Karposi sacroma
• Interluminale tumors

Chest CT-scan: Fig 1 anterior mediastinal lymphnodes and para tracheal
lymphnodes causing tracheal compression from the right side. Fig 2
Subcarinal lymphnodes and anterior mediastinal glands causing
compressio of carina and right main bronchus
Fig
1
Fig
2

Bronchoscopy
Bronchoscopy: Fig a demonstrates tracheal compression and fig b external
compression of both Right upper lobe bronchus and bronchus intermedius
Fig
aFig
b

Approach to large airway obstruction
< 6 Months > 6 Months
Congenital
TB
Acquired
Congenital
Clinical presentation : acute or chronic
Chest x-ray
Ba-study
Lung functions
Bronchoscopy
CT-scan
Diagnostic or therapeutic
Exclude foreign body aspiration
Cardiac Echo and
BA-study in
congenital cases
to excluded
associated
abnormalities
Conclusions
• Noisy breathing , apnea , monophonic
wheeze must alert clinician to the
possibility of large airway obstruction
• Severe obstruction at birth is a challenging
situation acquiring multi –disciplinary input
• Foreign body aspiration remain a common
cause in children
• Other common causes is PTB, lymphoma
and vascular compression of the airway
• Bronchoscopy is necessary to rule out
large airway obstruction