approach to inborn errors of metabolism
DESCRIPTION
Approach to Inborn Errors of Metabolism. Dr Yaser A. Mohammad. Why did you choose this topic ?. 2 Cases. 2 yrs old boy KCO Ethylmalonic Aciduria. Presenting with bronchopneumonia & Metabolic crisis. Drowsy, acidotic breathing, tachycardic , BP & SPo2 maintained with O2. - PowerPoint PPT PresentationTRANSCRIPT
Approach to Inborn Errors of MetabolismDr Yaser A. Mohammad
Why did you choose this topic ?
2 Cases2 yrs old boy KCO Ethylmalonic Aciduria.Presenting with bronchopneumonia &
Metabolic crisis.Drowsy, acidotic breathing, tachycardic , BP
& SPo2 maintained with O2.BGA PH: 7.15 CO2: 2 HCO3: 12 BE: -15 RBS : 8 Lactate: 6.5 Ammonia : 40
5 yrs old boy KCO Arginosuccinic Aciduria.Presenting sleepy & vomiting after taking an
overdose of his antiepileptics(phenobarbitone & Keppra) & missing 2-3 doses of his metabolic medicine.
Drowsy GCS 11-12 , HR 70, BP & SPo2 maintained in R.A.
BGA PH 7.43 PC02: 5 HCO3: 23 BE : -1.5 K : 1.9 RBS : 8 Ammonia 246
Outline Brief description of types of IEM that have an
acute presentation.Approach to metabolic emergencies.Diagnostic cluesQuiz
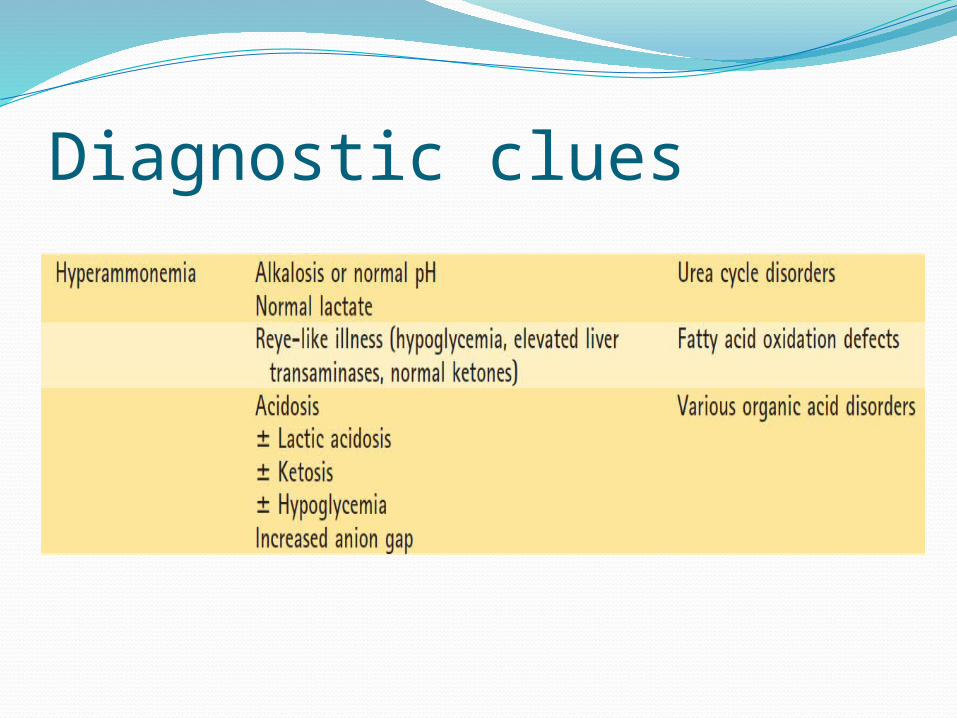
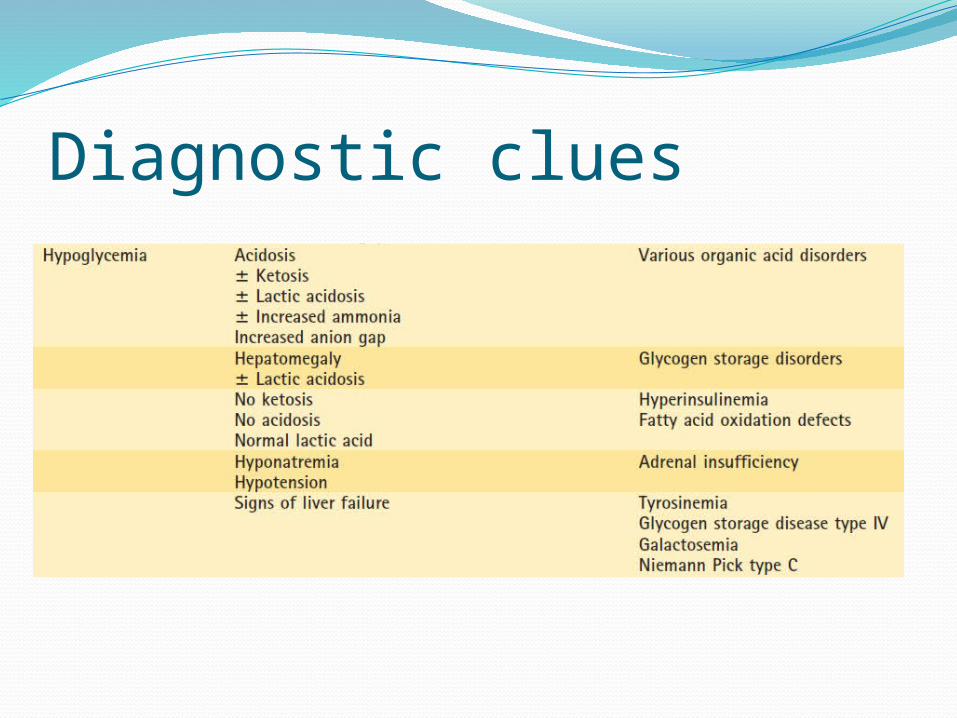
Organic Acid Disorders- Results from enzyme deficiencies in the pathway of Amino acids degradation.- Presentation with acidosis, hypoglycaemia
lactic acidosis & hyperammonaemia. Ketosis may also occur.
- Analysis of the urine for Organic Acids is the mainsty of the Dx.
- E.g. Methylmalonic, Ethylmalonic & propionic Acidaemia.
- Rx low protein diet, avoid catabolic state; high carbs feeds during illness & carnitine.
Urea Cycle DefectDefect in the metabolism of Ammonia in the Urea
Cycle, so high Ammonia.Presentation : poor feeding, lethargy, convulsion,
coma & Resp. alkalosis.Difficult to Dx due to lack of biochemical abnormality
apart of hyperammonaemia.Treated as sepsis initially.Dx with raised Plasma Amino Acids.E.g. Ornithine transcarbomylase, Arginosuccinic
aciduria.Rx low protein diet, Na benzoate, phenylbutyrate &
arginine. Avoid catabolic state.
Fatty acid oxidation defectFA oxidised in skeletal muscle, heart & liver.4 enzymes inolved (Chain Acyl-CoA Dehydrogenase). SCAD, MCAD, LCAD & VLCAD.Presentation: Non-ketotic hypoglycaemia, lethargy,
siezures, myoglubiuria, mucsle weakness & cardiomyopathy.
Dx: Reye like illness ( hypoglycaemia, raised ALT & AST , no ketosis). Hyperammonaemia.
Dx: Acylcarnitine profile by tandem mass spectrometry. Urine O.A & skin fibroblasts enzyme assay.
Rx prevention of fasting stress & carnitine.
Mitochondrial DOHave their own DNA & are derived from the
ovum, so all mtDNA DO are mternally inherited.Presentation: weakness, abnormal tone,
opthalmoplegia, seizures, cadiomyopathy, liver failure. Lactic acidosis with normal glucose.
Dx enzyme analysis of fibroblast, muscle or liver biopsy.
E.g MELAS ( Mitochondrial Encephalopathy, Lactic acidosis & Stroke like episodes).
MERRF ( Myoclonic Epilepsy with ragged red fibres)
Carbohydrate metabolism DOGalactosaemia; GAL-1-PUT. Accumulatiom of
GAL-1 phosphate damages liver , brain & kidney
Presentation: vomiting, hypoglycaemia, irritibility siezures, jaundice, hepatomegaly & cataracts.E.coli sepsis.
Dx enzyme assay in RBC. Urine: non-glucose reducing substance.
Rx Lactose & galactose free diet.
Carbohydrate metabolism DOGlycogen Storage disease- Threre are several enzyme deficiencies that
leads to glycogen accumulation.- Primarly affect liver, muscle or both.- Presentation : hypoglycaemia, hepatomegaly,
lactic acidosis, weakness & cardiomyopathy.- Dx : enzyme assay of blood, liver or muscle
biopsy.- Rx : avoidance of fasting, continuous
overnight feeds & uncooked corn starch.
How IEM present?Non-specific symptomsAttributed to infection or sepsisRoutine blood tests could be normalSuspect when lack of improvement with
standard therapy.Neontal screening.
Metabolic crisisMetabolic crisis occur when there is build up
of toxic metabolites. Triggers factors that increase catabolism:
- Infection - Fasting- trauma- Surgery- Increase consumption of protein.
Clinical presentationAn acute presentation with multisystem
involvement is strongly suggestive of an IEM. It can include:
- Vomiting and anorexia or failure to feed.- Lethargy that can progress to coma.- Seizures, particularly intractable.- Rapid, deep breathing that can progress to apnea.- Hypothermia (related to illness, not specific to a particular metabolic pathway).
In one review of 53 patients who presented to an emergency department and were subsequently diagnosed with an IEM:-
- 85 % had neurologic signs or symptoms.- 58 % had gastrointestinal signs or symptoms.- 51 % had both neurologic and
gastrointestinal signs and/or symptoms.
investigationsGlucoseABGCBC, U &E, LFTUrine: color, odor, dipstick & ketonesAmmoniaLactate
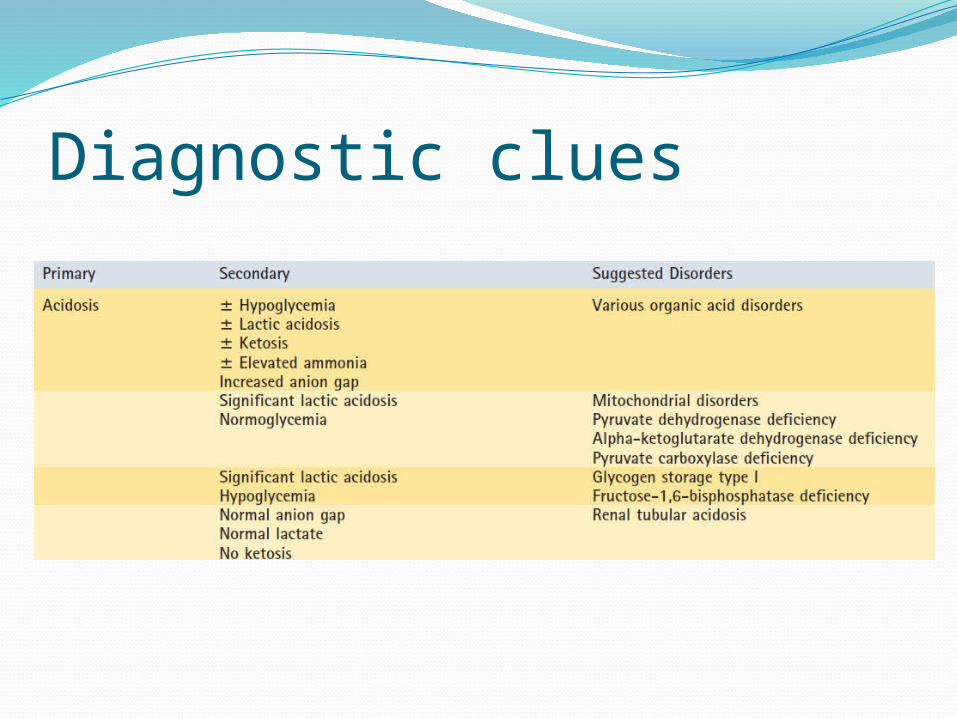
Diagnostic clues
Diagnostic clues
Diagnostic clues
Immediate MxFluid resuscitationTreatment of hypogycaemiaVentilation supportHCO3 for correction of acidosis ( rapid
correction have adverse effect on CNS).Empiric IV antibioticStop oral feeding pending Dx.Avoid catabolism by administration of IV
D10% with electrolyte. 8-10mg/kg/min.
Provision of co-factors:- Pyridoxine: 100mg iv for uncontrolled seizures.- Cobalmine: (Vit B 12 1mg im) metabolic
acidosis & suspected organic acidaemia.- Carnitine: (100 mg/kg per day in three divided
doses either orally or IV) may be useful in patients with organic acidemias, fatty acid oxidation disordersor carnitine defeciency.
- Biotin: 10 mg for neonate with recurrent seizures
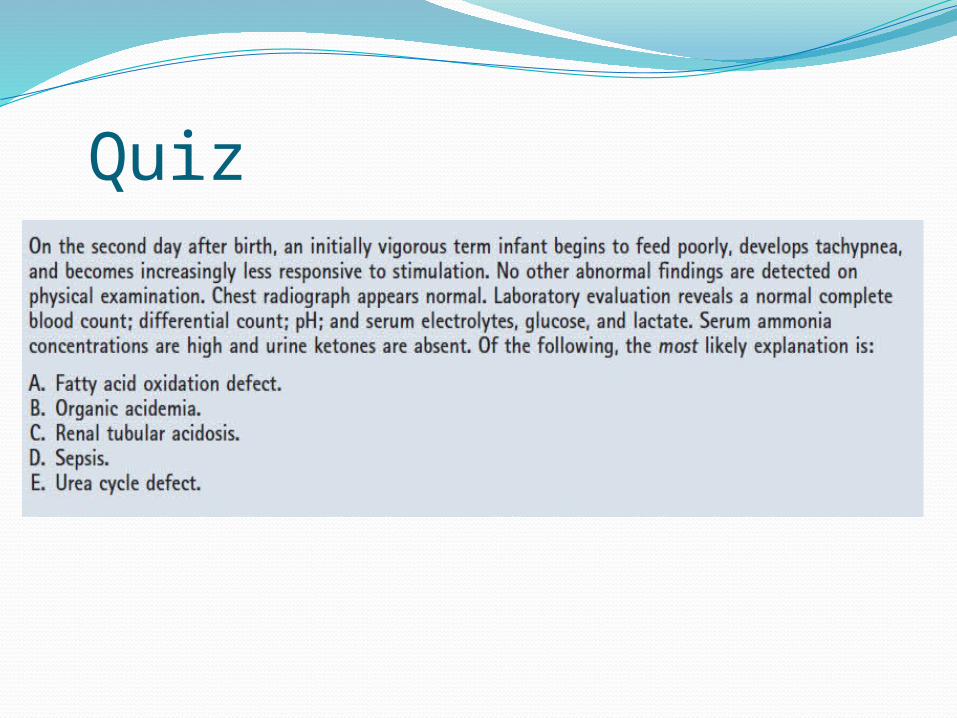
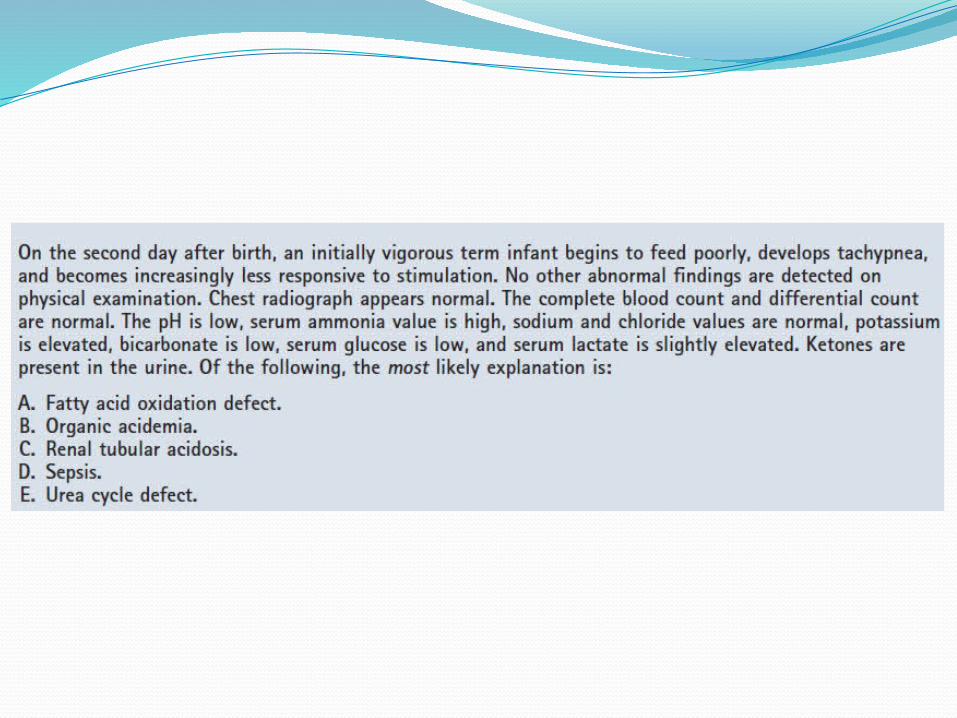
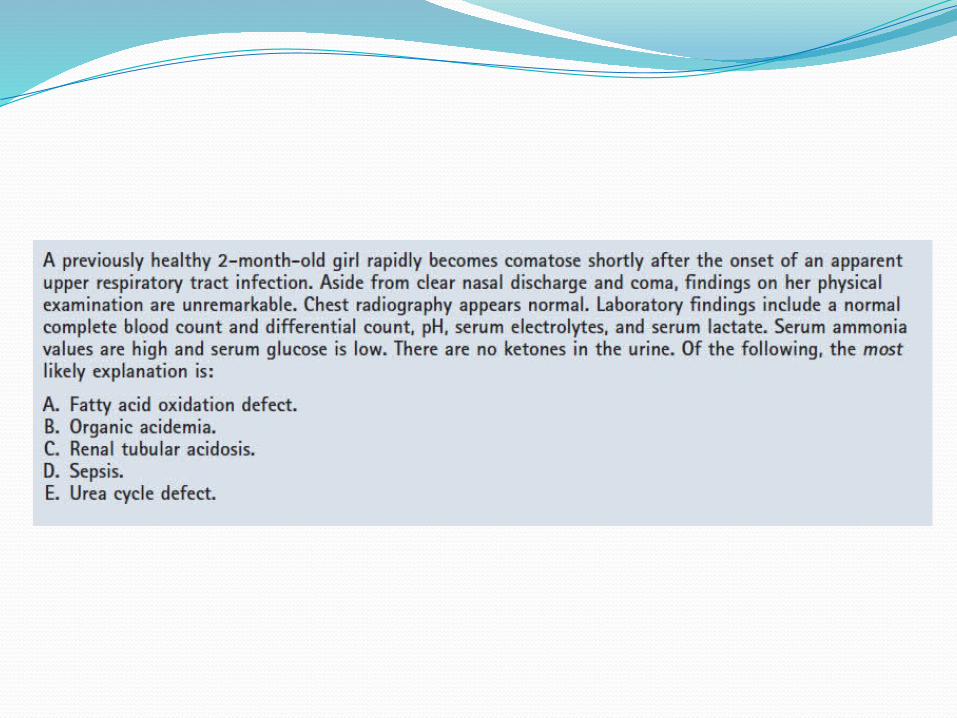
Quiz
Summary Optimal outcome of IEM depends on early
recognition, diagnosis, treatment of metabolic decompensation.
Symptoms are non-specific Initial investigation could give a clue to
diagnosis pending more detailed ones.management of metabolic decompensation
must be initiated promptly to avoid long term sequele.
ReferencesInborn Errors of Metabolism overview &
specific disorders by Paul Levy. Pediatrics in review vol 30. No. 4 April 2009.
Inborn errors of metabolism : metabolic emergencies. Uptodate, pediatrics. Reid Sutton.