approach to bleeding disorders
DESCRIPTION
APPROACH TO BLEEDING DISORDERS. History of Bleeding. Spontaneous vs. trauma/surgery-induced Ecchymoses without known trauma Medications or nutritional supplements. Clinical Presentations. Spontaneous hemarthroses - factors VIII and IX deficiency - PowerPoint PPT PresentationTRANSCRIPT
APPROACH TO BLEEDING DISORDERS
History of Bleeding
• Spontaneous vs. trauma/surgery-induced
• Ecchymoses without known trauma
• Medications or nutritional supplements

Clinical Presentations
• Spontaneous hemarthroses
- factors VIII and IX deficiency
- severe deficiencies of fibrinogen, prothrombin, and FV, VII, and X
• Mucosal bleeding symptoms
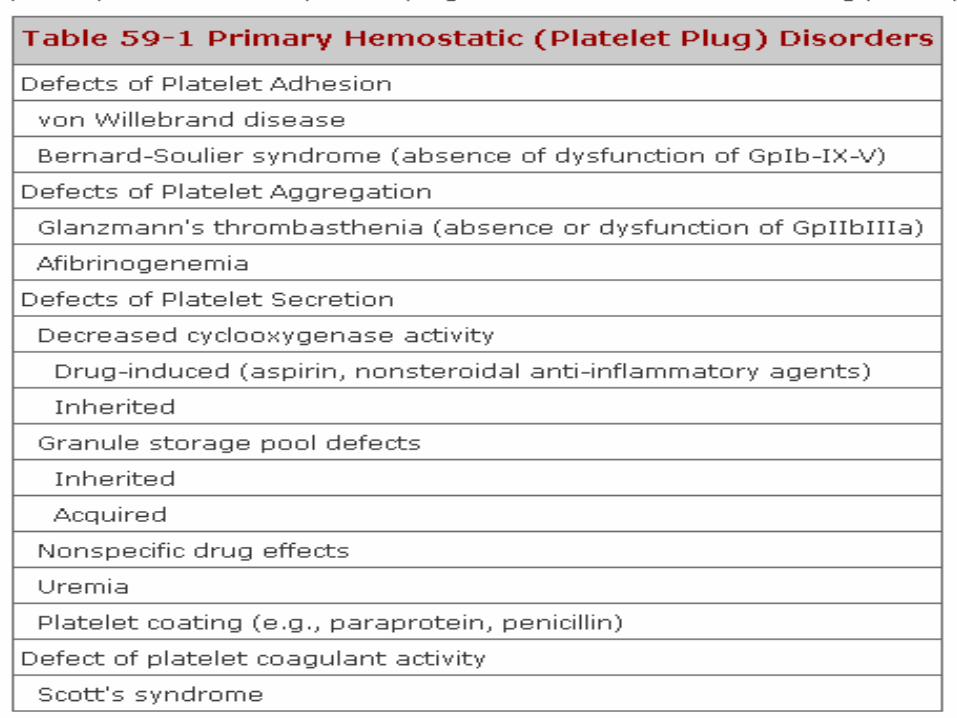
- platelet disorders
- von Willebrand disease (vWD)
Clinical Presentations
• Subcutaneous bleeding
- Cushing's syndrome
- Chronic steroid use
- Senile purpura
• Epistaxis
- hereditary hemorrhagic telangiectasia
- vwd

Clinical Presentations
• Menorrhagia
- vWD ,factor XI deficiency and symptomatic carriers of hemophilia A

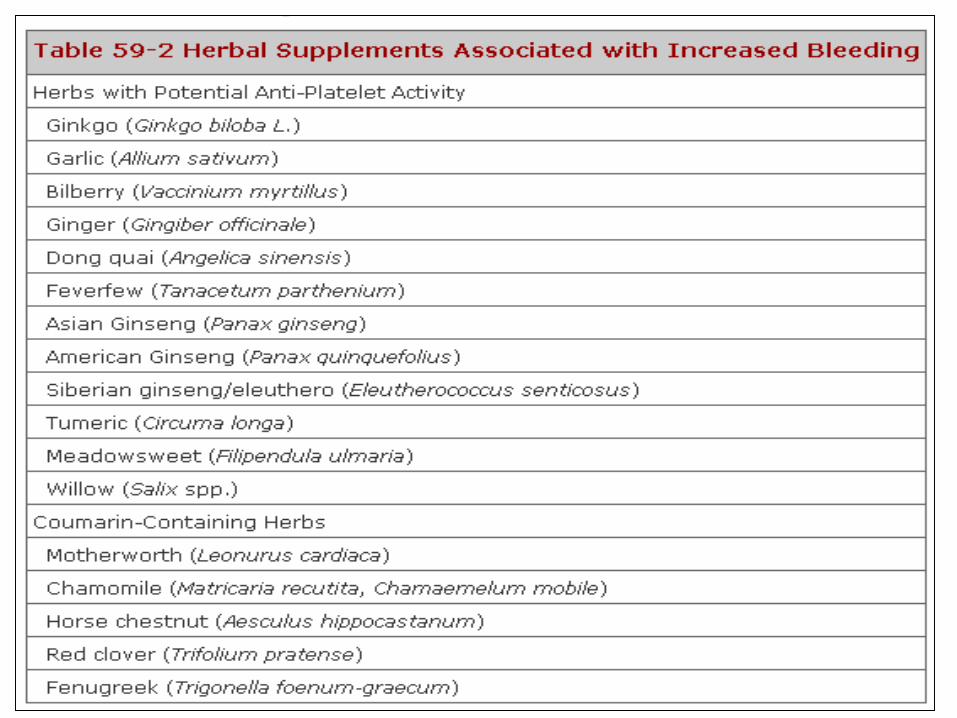
Prohemorrhagic medications and dietary supplements
• NSAID’s
• Aspirin
• Fish oil (omega 3 FA)
• Vitamin E
Systemic Diseases that Cause or Exacerbate Bleeding
• Bruising or mucosal bleeding may be a presentation of:
- liver disease, renal impairment, hypothyroidism, paraproteinemias or amyloidosis, and bone marrow failure

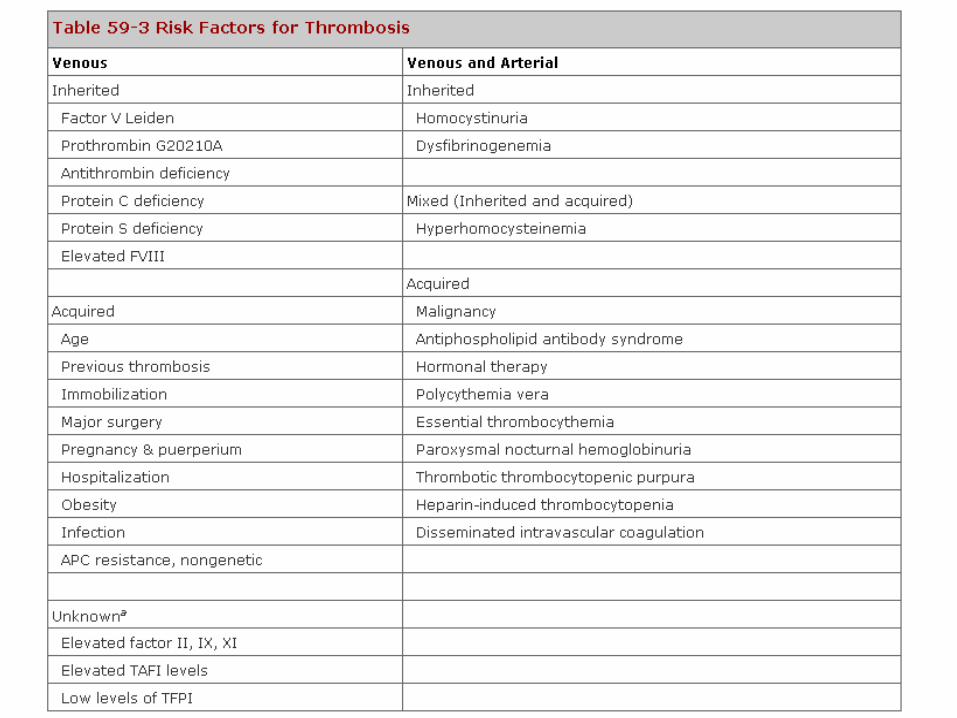
History of Thrombosis
• Risk Factors– Arterial : Atherosclerosis– Venous: Immobility, surgery, medical
conditions, HRT, Obesity, Genetic.
Idiopathic event is the stongest predictor of recurrence of venous thromboembolis Age is an important risk factor for thromboembolism Thrombotic events often has more than one contributing event

SCREENING ASSAYS
• PT
• aPTT
• Platelet count
MIXING STUDIES
Evaluate prolonged Aptt or less commonly PT Factor deficiency vs presence of inhibitor Normal plasma and patient plasma in a 50:50 ratio Incubate ar 37oC for 30, 60, and/or 120 min Factor deficiencies –with corection Lupus anticoagulant - no correction
Specific Factor Assay
• Requested based on clinical situation and the results of coagulation screening tests
• Precise diagnosis and effective management
• patient's plasma is mixed with plasma deficient in the factor being studied
Antiphospholipid Antibodies
• Antibodies to phospholipids (cardiolipin) or phospholipid-binding proteins (β 2-microglobulin detected by ELISA
OTHER COAULATION TESTS
• Thrombin time and Reptilase Time– Fibrinogen conversion to fibrin
• Anti-Factor Xa Plasma Inhibitory Activity-LMWH activity-UFH activity
Platelet Function
• Bleeding time
• PFA-100
• vWF assays
• platelet aggregometry
Hemostatic Disorders and Coagulation Test Abnormalities
• Prolonged (aPTT) No clinical bleeding – factors XII, high-
molecular-weight kininogen, protein kinase Variable, but usually mild, bleeding – factor
XI, mild FVIII and FIX Frequent, severe bleeding – severe
deficiencies of FVIII and FIX Heparin

• Prolonged prothrombin time (PT) Factor VII deficiency Vitamin K deficiency – early Warfarin anticoagulation
Hemostatic Disorders and Coagulation Test Abnormalities
Hemostatic Disorders and Coagulation Test Abnormalities
• Prolonged aPTT and PT Factor II, V or X deficiency Vitamin K deficiency – late Direct thrombin inhibitors
• Prolonged thrombin time Heparin or heparin-like inhibitors Mild or no bleeding – dysfibrinogenemia Frequent, severe bleeding – afibrinogenemia
Hemostatic Disorders and Coagulation Test Abnormalities
• Prolonged PT and/or aPTT not correct with mixing with normal plasma Bleeding – specific factor inhibitor No symptoms, or clotting and/or pregnancy
loss – lupus anticoagulant Disseminated intravascular coagulation Heparin or direct thrombin inhibitor
Hemostatic Disorders and Coagulation Test Abnormalities
• Abnormal clot solubility Factor XIII deficiency Inhibitors or defective cross-linking
Hemostatic Disorders and Coagulation Test Abnormalities
• Rapid clot lysis Deficiency of 2-antiplasmin
or plasminogen activator inhibitor 1Treatment with fibrinolytic therapy