applying genomics in the management of early-stage … education... · 2015-12-22 · ozzy osborne....
TRANSCRIPT

Applying Genomics in the Management of
Early-Stage Breast Cancer
Deborah Davison, DNP, CRNP Genomic Health Medical Affairs

2
WHO Definitions: Genetics & Genomics
•GENETICS: The study of heredity •GENOMICS: The study of genes and their
functions
Genetics examines the function of a single gene (or chromosome) while genomics examines groups of genes and their relationships in order to identify their combined influence on an organism

3
Clinical Utility of Genetics in Oncology
• Can be used to predict risk of disease development – BRCA1 & 2: Increased risk of breast, ovarian, and
other tumors – APC (Adenomatous polyposis coli): Increased
risk of familial adenomatous polyposis/colon CA
• Can be used to locate “targets” for intervention
•Generally involves mutations, variations
Confidential- Not for distribution

4
4 4
Clinical Utility of Genomics in Oncology
•Early and accurate diagnoses •Greater individualization of treatment decisions •Targeted therapy based on individual disease •Greater likelihood of clinical trial success •More rational drug discovery •Faster drug development
– Patient selection – Trial design
Normal gene expression and interaction

5
‘Given the swimming pools of booze I’d guzzled over the years – not to mention all the [drugs] – there’s really no plausible medical reason why I should be alive’ Ozzy Osborne

6
Ozzy’s DNA: •Well the results are in… • Researchers studying his DNA have determined that
he is the descendant of a Neanderthal. • Neanderthals were a human species that lived in
parts of Europe and Asia until about 30,000 years ago, and were said to be stronger and more aggressive than Homo sapiens, from which modern man evolved.
• The study also determined that Ozzy is a distant relative of outlaw Jesse James, Russian tsar Nicholas II and England’s King George I. He also shares some genes with ancient Romans.

7
Evidence-Based Practice
• Enables clinicians to provide highest quality of care
• Five steps: – Ask the clinical question – Collect the most relevant and best evidence – Critically appraise the evidence – Integrate the evidence with the individual
patient situation – Evaluate the practice decision
Melnyk B & Fineout-Overholt E, 2010

8
Revised Criteria for Level of Evidence in Tumor Marker Studies
Level of evidence Study design Validation studies available
I Prospective None required
I Prospective using archived samples
One or more with consistent results
II Prospective using archived samples
None, or inconsistent results
II Prospective / observational
Two or more with consistent results
III Prospective / observational
None, or one with consistent results, or inconsistent results
IV-V Retrospective / observational
Not applicable*
Simon RM, et al. J Natl Cancer Inst. 2009;101:1446-1452.
*Level of evidence IV and V studies will never be satisfactory for determination of medical utility
The Oncotype DX® assay fulfills the criteria for Level I evidence: more than one prospective validation study using archived samples with consistent results.
8

9
For genomic assays, my questions…
•Does the assay provide insight into the biology of the tumor? – What is the risk that my cancer will recur? – What treatment is best for me?
•Does the assay provide information that we didn’t already have?
• Is there clinical significance to the result? • Can I be confident in the result?

10
The Recurrence Score® Result Uses Key Genes Linked to Critical Molecular Pathways
16 BREAST CANCER RELATED GENES
Paik S, et al. N Engl J Med. 2004;351:2817-2826.
ER PR
Bcl2 SCUBE2
GRB7 HER2
Ki-67 STK15
Survivin Cyclin B1
MYBL2
Stromelysin 3 Cathepsin L2
GSTM1
CD68
BAG1
Beta-actin GAPDH RPLPO GUS TFRC
5 REFERENCE GENES
Estrogen Proliferation HER2 Invasion Others
10

11
The Recurrence Score® Result Assesses Individual Tumor Biology for ER+ Breast Cancer
Paik S, et al. N Engl J Med. 2004;351:2817; Paik S, et al. J Clin Oncol. 2006;24:3726; Habel LA, et al. Breast Cancer Res. 2006;8:R25-R39.
Dist
ant r
ecur
renc
e at
10
year
s
Recurrence Score value
CONTINUOUS BIOLOGY 4 0 %
3 5 %
3 0 %
2 5 %
2 0 %
1 5 %
1 0 %
5 %
0 % 0 5 1 0 1 5 2 0 2 5 3 0 3 5 4 0 4 5 5 0
LOW RECURRENCE SCORE DISEASE Indolent
Hormone therapy-sensitive Minimal, if any, chemotherapy benefit
HIGH RECURRENCE SCORE DISEASE Aggressive
Less sensitive to hormone therapy Large chemotherapy benefit
11

12
First Question: Prognosis
What is the risk that my cancer with recur?
Confidential- Not for distribution

13
Oncotype DX® Clinical Validation: NSABP B-14
• Objective: Prospectively validate the Recurrence Score®
result as a predictor of distant recurrence in node-negative, ER+ patients
• Multicenter study with prespecified 21-gene assay, algorithm, endpoints, analysis plan
Randomized
Registered
Placebo—not eligible
Tamoxifen—eligible
Tamoxifen—eligible
Paik S, et al. N Engl J Med. 2004;351:2817-2826.
13

14
Oncotype DX® Clinical Validation: B-14 Results – Distant Recurrence
Distant Recurrence Over Time – All 668 Patients
Proportion Without Distant Recurrence at
10 years = 85%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
0 2 4 6 8 10 12 14 16 Years
Paik et al. N Engl J Med. 2004;351:2817-2826.
Pro
porti
on w
ithou
t Dis
tant
Rec
urre
nce

15
Oncotype DX® Clinical Validation: B-14 Results – Distant Recurrence
Distant Recurrence for the three distinct cohorts identified
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
0 2 4 6 8 10 12 14 16 Years
P <0.001
RS <18 n = 338
RS 18-30 n = 149
RS ≥31 n = 181
Paik et al. N Engl J Med. 2004;351:2817-2826.
Pro
porti
on w
ithou
t Dis
tant
Rec
urre
nce

16
First Question: Prediction
What treatment is appropriate for me?
Confidential- Not for distribution

17
• Objective: Prospectively determine the relationship between Recurrence Score® result and chemotherapy benefit in node-negative, ER+ patients
• Multicenter study with prespecified 21-gene assay, algorithm, endpoints, analysis plan
Tam
Oncotype DX® Clinical Validation: NSABP B-20
Randomized
Tam + MF
Tam + CMF
Paik S, et al. J Clin Oncol. 2006;24:3726-3734.
17

18
B-20 Results
0 2 4 6 8 10 12 Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
All Patients Tam + Chemo Tam P = 0.02
Pro
porti
on w
ithou
t Dis
tant
Rec
urre
nce
Tam vs Tam + Chemo – All 651 Patients
Paik et al. J Clin Oncol. 2006.
4.4% absolute benefit from tam + chemo at 10 years

19
B-20 Results: Tam vs Tam + Chemo
28% absolute benefit from tam + chemo
Paik et al. J Clin Oncol. 2006.
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DRFS
Low Risk Patients (RS < 18) Tam + Chemo Tam
p = 0.61
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DRFS
Int Risk (RS 18 - 30) Tam + Chemo Tam
p = 0.39 Low RS
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DRFS
High Risk Patients (RS ≥ 31) Tam + Chemo Tam
p < 0.001
Int RS
High RS
High Risk Patients (RS≥31) N Events TAM + Chemo 117 13 TAM 47 18
Low Risk Patients (RS<18) N Events TAM + Chemo 218 8 TAM 135 4
Int Risk Patients (RS 18-30) N Events TAM + Chemo 89 9 TAM 45 4
Pro
porti
on w
ithou
t Dis
tant
Rec
urre
nce

20
Second Question
Does the assay provide information that I didn’t already
have?
Confidential- Not for distribution

21
NSABP B-20: Many Small Tumors Have Intermediate to High Recurrence Score® Disease
Paik S, et al. J Clin Oncol. 2006;24:3726-3734.
33%
20% 19% 23% 21%
46%
N = 110 N = 318 N = 196 N = 24
Rec
urre
nce
Scor
e
≤1 cm 1.1-2 cm 2.1-4 cm >4 cm
Clinical tumor size
0
20
40
60
80
100 P=0.001
64% 56% 46%
16% 25% 30%
21

22
NSABP B-20: Many Younger Patients Have Low Recurrence Score® Disease
P=0.018
41% 24% 28% 19%
14% 21% 22% 21%
44% 55% 50% 60%
N = 63 N = 226 N = 166 N = 196
Rec
urre
nce
Scor
e
Paik S, et al. J Clin Oncol. 2006;24:3726-3734.
22

23
NSABP B-20: Significant Proportion of High-Grade Tumors Have
Low Recurrence Score® Disease
12% 22% 42%
16% 22% 22%
73% 56% 36%
N = 77 N = 339 N = 163
P < 0.001 P<0.001
5% 12% 61%
12% 24% 19%
83% 64% 19%
N = 119 N = 340 N = 190
Rec
urre
nce
Scor
e
Rec
urre
nce
Scor
e
Paik S, et al. J Clin Oncol. 2006;24:3726-3734.
23

24
Third Question
Is there clinical significance to the result?
Confidential- Not for distribution

Does the Recurrence Score® Impact Treatment Decisions?
Is the Oncotype DX® Assay Cost-
Saving and Cost-Effective?

26
Meta-Analysis: The Recurrence Score® Result Changes Decisions Across 7 Independent Decision Impact Studies
Before RS CT + HT HT Total After RS CT + HT HT CT + HT HT
Asad et al. 24 36 8 13 81 Henry et al. 6 7 2 14 29 Klang et al. 69 105 20 119 313 Liang et al. 125 85 3 47 260 Lo et al. 20 20 3 40 83 Oratz et al. 19 14 3 32 68 Thanasoulis et al. 8 30 2 38 78
Consistent, large impact of RS on treatment decisions in both directions: • Half of patients initially recommended CT+HT are changed to HT only • Some patients initially recommended HT alone have CT added upon being
informed of “High RS Disease” Asad J, et al. Am J Surg. 2008;196:527-529; Henry LR, et al. J Surg Oncol. 2009;99:319-323; Klang SH, et al. Value Health. 2010;13:381-387; Liang H, et al. SABCS 2007: Abstract 2061; Lo SS, et al. J Clin Oncol. 2010;28:1671-1676; Oratz R, et al. J Oncol Pract. 2007;3:182-186; Thanasoulis T, et al. Am Soc Br Surg Annual Meeting 2008. Hornberger J, et al. SABCS 2010. Poster P2-09-06.
RS, Recurrence Score® result; CT, chemotherapy; HT, hormone therapy N = 912 patients
26

27
Meta-Analysis: Overall Impact of Recurrence Score® on Treatment Decisions
52% 48% 88% 12%
Treatment plan prior to Oncotype DX®
Treatment plan after RS
Treatment plan after RS
CT + HT
HT
Overall, the RS led to a 37% change in treatment decisions • 33% from CT + HT HT • 4% from HT CT + HT
4% change 33% change
Hornberger J, et al. SABCS 2010. Poster P2-09-06.
RS, Recurrence Score result 27

Clinical Utility of Genomics
Confidential- Not for distribution

36-year-old with 1.1-cm tumor Menopausal Status: Premenopausal Tumor Type: Infiltrating Ductal Carcinoma (IDC) Tumor Size: 1.1 cm ER Status (IHC): Positive (80%, 3+) PR Status (IHC): Positive (80%, 3+) HER2/neu Status: Negative (FISH) Histologic Grade: 6/9 with no LVI Lymph Node Status: Negative Submitted by: Victor G. Vogel MD
39-year-old with 2.0-cm tumor Menopausal Status: Premenopausal Tumor Type: Infiltrating Ductal Carcinoma (IDC) Tumor Size: 2.0 cm ER Status (IHC): Positive PR Status (IHC): Negative HER2/neu Status: Negative Histologic Grade: 2 Lymph Node Status: Negative Submitted by: Ruth M. O’Regan MD

30 RESULTS: Recurrence Score = 36
RESULTS: Recurrence Score = 8

31
Fourth Question
Can I be confident in the results?
Confidential- Not for distribution

32
Refer to the Guidelines Oncotype DX
Newly diagnosed patients with node-negative, ER+ breast cancer who will receive tamoxifen ASCO Guidelines
NCCN Guidelines TM
St. Gallen Consensus
Consider use in > 0.5 cm, HR+, HER2– disease pT1, pT2, or pT3; pN0 and pN1mi
(≤ 2 mm axillary node metastasis)
Oncotype DX has been shown to predict chemotherapy benefit among patients with
HR+ disease
Harris L, et al. J Clin Oncol. 2007;33(25):5287-5312. Adapted from NCCN Practice Guidelines in Oncology – v.2.2011. Goldhirsch A, et al. Ann Oncol. 2011;22:1736-1747. ASCO is a trademark of the American Society of Clinical Oncology. NCCN and NCCN Guidelines are trademarks of the National Comprehensive Cancer Network. ASCO and NCCN do not endorse any therapy or product.
32

33
Background: Oncotype DX®
• The 21-gene Oncotype DX Recurrence Score® breast cancer assay is performed using an RT-PCR platform and provides a quantitative assessment of risk of recurrence and likelihood of chemotherapy benefit.
• The Oncotype DX assay has been validated in multiple clinical trials with consistent results as a prognosticator of breast cancer recurrence1-7 and as a predictor of the likelihood of benefit from chemotherapy in patients with ER-positive early stage invasive breast cancer.3,6
• The Oncotype DX assay is incorporated in major international guidelines, including NCCN®, ASCO®, St Gallen, and ESMO guidelines.8-11
Poulet et al. SABCS 2012.
1. Paik S, et al. N Engl J Med. 2004; 351: 2817-26. 2. Habel LA, et al. Breast Cancer Res. 2006; 8: R25. 3. Paik S, et al. J Clin Oncol. 2006; 24: 3726-34. 4. Goldstein LJ, et al. J Clin Oncol. 2008; 26: 4063-71. 5. Dowsett M, et al.J Clin Oncol. 2010; 28: 1829-34. 6. Albain KS, et al. Lancet Oncol. 2010; 11: 55-65. 7. Mamounas EP, et al. ASCO Breast Cancer 2012. 8. NCCN Breast Cancer Guidelines. www.nccn.org, v3.2012. 9. Harris L, et al. J Clin Oncol. 2007; 25: 5287-5312. 10. Goldhirsch A, et al. Ann Oncol. 2009; 20: 1319-29. 11. Aebi S, et al. Ann Oncol. 2010; 21 Suppl 5: v9-14.

34
Background: MammaPrint®
• MammaPrint is a 70-gene assay performed on a microarray platform and characterizes breast cancer patients without systemic treatment as either high or low risk for distant recurrence.
• MammaPrint has been validated in a heterogeneous patient population that included ER-positive, ER-negative, triple negative, and HER2-positive patients.1-2
• MammaPrint is included as a prognosticator in the St Gallen and ESMO guidelines.3-4
• There are no published data from randomized studies supporting that MammaPrint is predictive of chemotherapy benefit.
Poulet et al. SABCS 2012.
1. van de Vijver MJ, et al. N Engl J Med. 2002;347:1999-2009. 2. Buyse M, et al. J Natl Cancer Inst. 2006;98:1183-1192. 3. Goldhirsch A, Ann Oncol. 2009; 20: 1319-29. 4. Aebi S, et al.. Ann Oncol. 2010; 21 Suppl 5: v9-14.

35
Clinical Considerations Between MammaPrint® and the Oncotype DX® Assay
MammaPrint Oncotype DX
Clinical validity
•Validated for prognosis in a heterogeneous pooled population of both treated and untreated patients
•Validated in multiple homogeneous populations to predict risk of recurrence (prognosis) and treatment benefit (prediction) in node-negative and node-positive patients with ER+ breast cancer
Clinical utility
•No available data on impact of test on treatment decisions or patient satisfaction; risk may or may not be reduced in “high risk” patients by treatment; there is no data to indicate whether treatment should be hormonal treatment or chemotherapy treatment or both
•Numerous studies showing impact of test on treatment decisions and patient satisfaction
Economic validity
• Cost-neutral or cost-effective
•Overall cost-savings and cost-effective1,2
1. Hornberger J, et al. Am J Manag Care. 2005;11:313-324. 2. Hornberger J, et al. J Clin Oncol. 2010;28:e382.
These comparisons are not based upon findings from comparative studies.

Risk Classification of Early Stage Breast Cancer as Assessed by
MammaPrint® and Oncotype DX® Genomic Assays
Poulet B,1 Jamshidian F,2 Butler S,2 Cherbavaz DB,2
Svedman C,2 Levy E1, Clough KB1
1L'Institut du Sein-Paris Breast Centre, Paris, Ile de France, France 2Genomic Health, Inc., Redwood City, CA.
Poulet et al. SABCS 2012.

37
Objectives
While the development and validation for Oncotype DX® and MammaPrint® are substantially different, the tests are frequently believed to provide equivalent information.
• Primary: • The study was designed to compare classifications by Oncotype DX and
MammaPrint in the same patient specimens. • The study also evaluated the success of each test in generating results.
• Secondary: • To describe the distribution of the continuous Oncotype DX Recurrence Score® result
within each MammaPrint risk category. • To describe the tumor characteristics of patients who were successfully tested. • To describe the tumor characteristics of the patients in subgroups based on the risk
classification according to both assays.
Poulet et al. SABCS 2012.
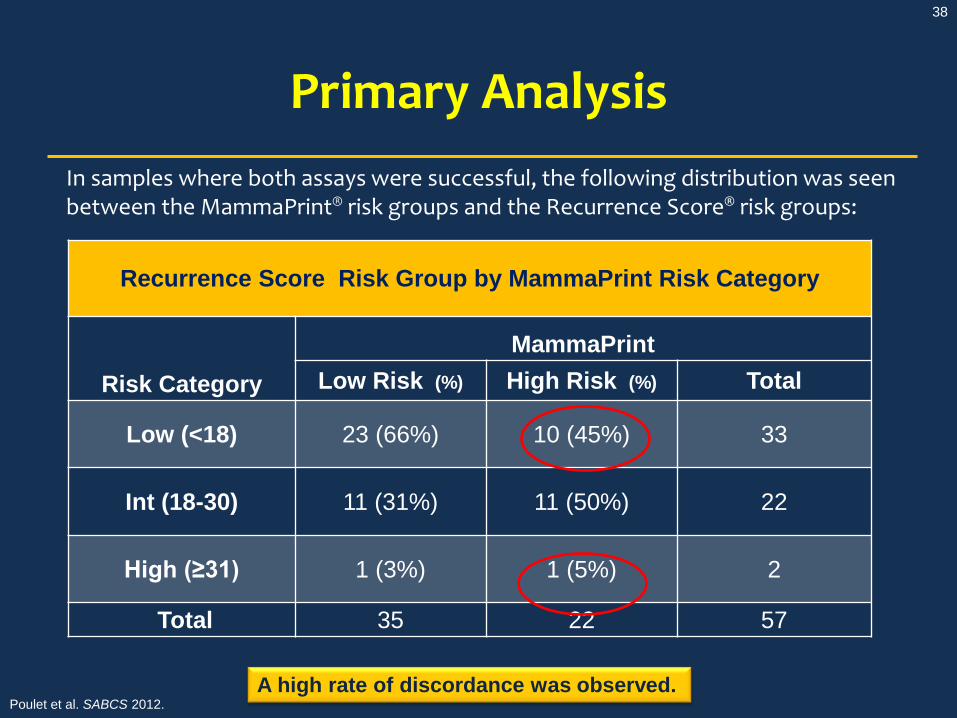
38
Primary Analysis In samples where both assays were successful, the following distribution was seen between the MammaPrint® risk groups and the Recurrence Score® risk groups:
Recurrence Score Risk Group by MammaPrint Risk Category
Risk Category
MammaPrint Low Risk (%) High Risk (%) Total
Low (<18) 23 (66%) 10 (45%) 33
Int (18-30) 11 (31%) 11 (50%) 22
High (≥31) 1 (3%) 1 (5%) 2
Total 35 22 57
A high rate of discordance was observed. Poulet et al. SABCS 2012.

39
Recurrence Score® Distribution Within MammaPrint® Categories
A wide distribution of Recurrence Score results was observed within each MammaPrint risk category.
Poulet et al. SABCS 2012.

40
40
Why is measurement of ER important?

41
ER Expression by RT-PCR
High Intermediate Low
Recurrence Score® Result
• There was a wide range of ER expression (assessed by RT-PCR) within both low and high MammaPrint® result risk groups.
• A number of the MammaPrint high risk patients had low Recurrence Score results (blue circles) and high ER expression and would be expected to have large benefits from hormonal therapy alone. Poulet et al. SABCS 2012.

42
Closing Thoughts
• Importance of understanding and treating the underlying individual tumor biology
• Importance of standardizing emerging “next generation” technologies
• Genomic assays for clinical decision-making must be “Fit for Purpose”
– Clinically validated in prospectively-designed studies of sufficient size and statistical power
– Supported by evidence in target patient population, with demonstrated value beyond existing measures
– Standardized and reproducible – Practical and clinically impactful

43
Thank You!