applying evidence – blood conservation in clinical practice victor a. ferraris, m.d., ph.d....
TRANSCRIPT
Applying Evidence – Blood Conservation in
Clinical Practice
Victor A. Ferraris, M.D., Ph.D.University of Kentucky
Linda & Jack Gill Heart InstituteLexington, KY
Real-world guideline application
Presenter Disclosure Information
Victor A. Ferraris, M.D., Ph.D.Research grant support from
American Heart Association, Aventis, Bayer, BioMarin Pharma, Guilford, Medtronic, NHLBI, and The Medicines Company.
Lecture or consulting fees from AstraZeneca, Aventis, Bayer, Network for Advancement of Transfusion Alternatives (NATA), and The Medicines Company.
Real-world guideline application
Blood Conservation Guidelines
61 recommendations regarding blood conservation.6 Class I recommendations39 Class II recommendations
20 Class IIa19 Class IIb
16 Class III recommendations
Ferraris, et al. Ann Thorac Surg, 2007. (in press)

Real-world guideline application
Blood Conservation Interventions – Class I Recommendations
Identify high risk preoperatively. Blood transfusion algorithm w/ point-
of-care testing. Multimodality approach. Anti-fibrinolytic drugs (esp. for high
risk) Cell saver & cell salvage Preop platelet count and HCT for risk
prediction. Ferraris VA, et al. STS Guidelines on blood conservation. Ann Thorac Surg, 2007. In press.
Real-world guideline application
Class IIa or IIb Blood Conservation Interventions
Class IIa OPCAB DDAVP for high
risk only. Stop clopidogrel
5 days before OR. Continue ASA
unless totally elective.
Class IIb BT/PFA-100 for
screening in high risk. r-FVIIa for recalcitrant
bleeding. Autologous
hemodilution. Retrograde priming.
Ferraris VA, et al. STS Guidelines on blood conservation. Ann Thorac Surg, 2007. In press.
Real-world guideline application
Things That Are Not Indicated for Blood Conservation (Preliminary)
Class III indicationsUnwashed shed mediastinal blood re-
infusion.PEEP for control of bleeding.Dipyridamole for ‘platelet anesthesia’.Plasma or platelet-pheresis.Routine DDAVP.Leukocyte depletion filters during CPB.
Ferraris VA, et al. STS Guidelines on blood conservation. Ann Thorac Surg, 2007. In press.

Real-world guideline application
Purpose
Apply evidence-based blood conservation interventions to real world situations.
Describe the process of guideline development.
Real-world guideline application
Case #1 – Clopidogrel – “the Devil’s Drug”
Patient History80 y/o woman w/ unstable
angina & continued chest pain.Cath shows 3-v CAD w/ 60% left
main.600 mg clopidogrel loading
dose before cath. (Class I recommendation by AHA/ACC).
AODM, HTN, CRF (creat = 2.0), HCT = 34%. BSA = 1.5.
Real-world guideline application
Case # 1 - Questions
1. Is this patient at high risk for bleeding?
2. Can you stop anti-platelet drugs?
3. What are the options to limit bleeding in this patient?
Real-world guideline application
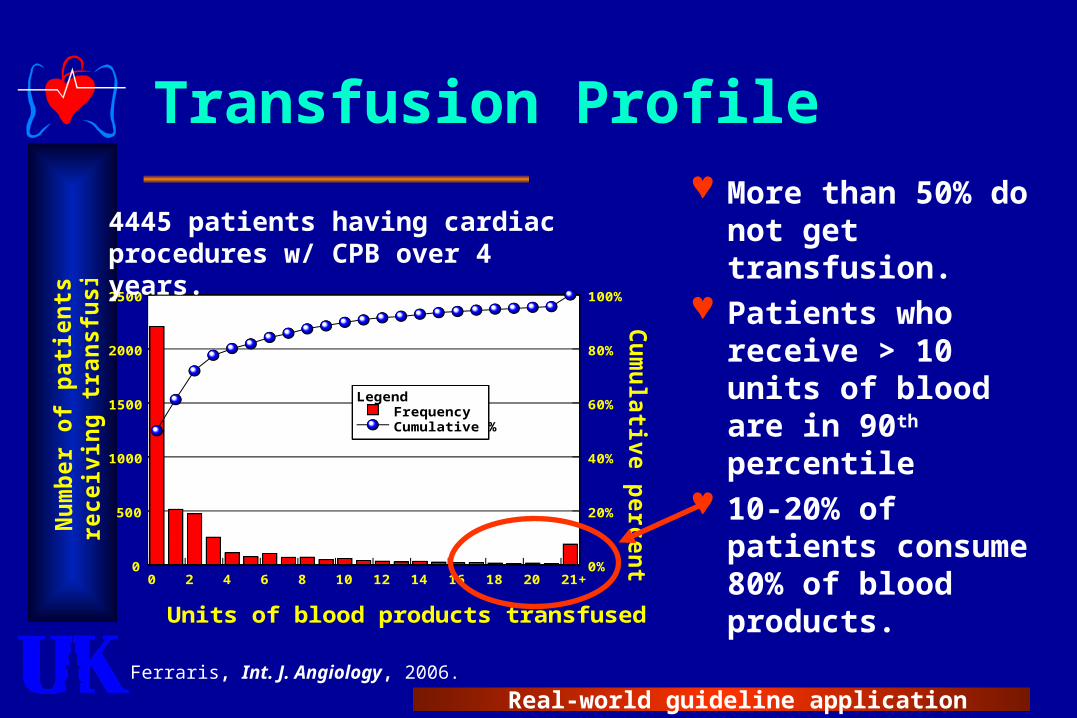
Transfusion Profile More than 50%
do not get transfusion.
Patients who receive > 10 units of blood are in 90th percentile
10-20% of patients consume 80% of blood products.
0 2 4 6 8 10 12 14 16 18 20 21+
Units of blood products transfused
0
500
1000
1500
2000
2500
Nu
mb
er
of
pa
tie
nts
re
ce
ivin
g t
ran
sfu
sio
n
0%
20%
40%
60%
80%
100%
Cu
mu
lativ
e p
erc
en
t
LegendFrequencyCumulative %
4445 patients having cardiac procedures w/ CPB over 4 years.
Ferraris, Int. J. Angiology, 2006.
Real-world guideline application
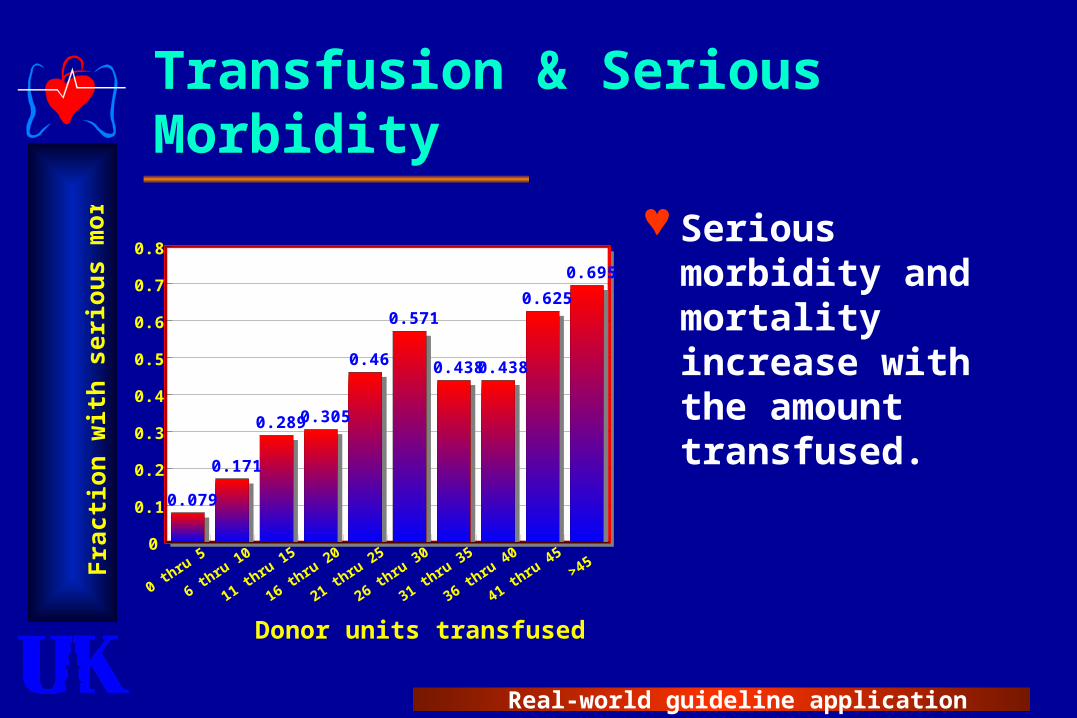
Transfusion & Serious Morbidity
0 thru
5
6 thru
10
11 thru
15
16 thru
20
21 thru
25
26 thru
30
31 thru
35
36 thru
40
41 thru
45>45
Donor units transfused
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Fra
cti
on
wit
h s
eri
ou
s m
orb
idit
y
0.079
0.171
0.289 0.305
0.46
0.571
0.438 0.438
0.625
0.695
Serious morbidity and mortality increase with the amount transfused.
Real-world guideline application
Predictors of Postoperative Bleeding – The Big 6
1) Advanced age2) Small body size or preoperative
anemia (low RBC volume)3) Anti-platelet & anti-thrombotic
drugs.4) Prolonged operation (CPB time) –
high correlation with OR type.5) Emergency operation6) Other co-morbidities (CHF, COPD,
HTN, PVD, renal failure, etc.)Ferraris VA, et al. STS Guidelines. Ann Thorac Surg. 2005;79:1454-61.; Ferraris VA, et al. Ann Surg. 2002;235:820-7.
Real-world guideline application
Two Causes of Postoperative Bleeding & Blood Transfusion
Patient-related Age Red blood cell
volume Co-morbidities
CHF Renal failure COPD
Procedure-related Prolonged
operation Emergency
operation Surgical site
bleeding (‘hole in the artery’)
Real-world guideline application
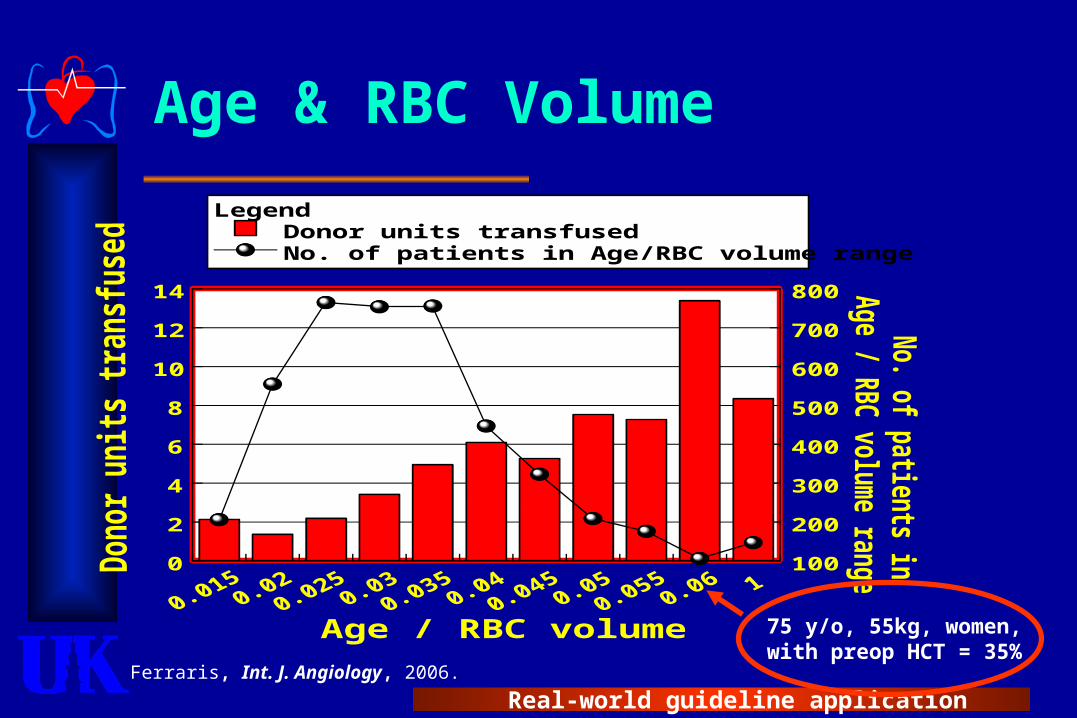
Age & RBC Volume
Age / RBC volume
0
2
4
6
8
10
12
14
100
200
300
400
500
600
700
800
LegendDonor units transfusedNo. of patients in Age/RBC volume range
75 y/o, 55kg, women, with preop HCT = 35%Ferraris, Int. J. Angiology, 2006.
Real-world guideline application
Case #1 – Question #1
Is this patient high risk?Risk factors
AgeAnemia (red blood cell volume)Anti-platelet drugsUrgent operationMultiple co-morbidities (CRF, HTN,
AODM,
AnswerYes!

Real-world guideline application

Real-world guideline application
Real-world guideline application
Managing Risk Factors
Anti-platelet drugs as an exampleCommon problem – almost all
patients have anti-platelet drug on-board at OR.
Evidence is available to guide decisions.
Likely to show tangible benefit.
Real-world guideline application
Does Aspirin Cause Increased Postoperative Bleeding?
21 studies reviewed the effect of aspirin on postoperative bleeding.5 of 6 RCT’s showed increased
bleeding due to aspirin (Level A evidence).
Evidence less convincing in 15 observational studies (Level B or C evidence).
Ferraris VA, et al. STS Guidelines. Ann Thorac Surg. 2005;79:1454-61.

Real-world guideline application
Long-term Efficacy of ASA in Reducing Long-term Efficacy of ASA in Reducing Death or MI in Patients with Unstable Death or MI in Patients with Unstable AnginaAngina
Wallentin LC et al JACC 1991;18:1587–1593
0.00
0.05
0.10
0.15
0.20
0.25
00 33 66 99 1212MonthsMonths
Probabilityof death or MI
PlaceboPlacebo
ASA 75 mgASA 75 mg
Risk ratio after 1 year 0.52Risk ratio after 1 year 0.5295% Cl 0.37–0.72 (95% Cl 0.37–0.72 (pp=0.0001)=0.0001)
Real-world guideline application
Guidelines & Aspirin – the Dilemma
Aspirin causes increased bleeding. Amount of bleeding is small (0.5
units/patient)
Aspirin important for better outcome in acute coronary syndromes Nothing more important than aspirin including
heparin, thrombolytics, 2b/3a, & PCI.
STS recommendation – stop aspirin for a few days in very low risk patients, continue in all others.
Ferraris VA, et al. STS Guidelines. Ann Thorac Surg. 2005;79:1454-61.
Real-world guideline application
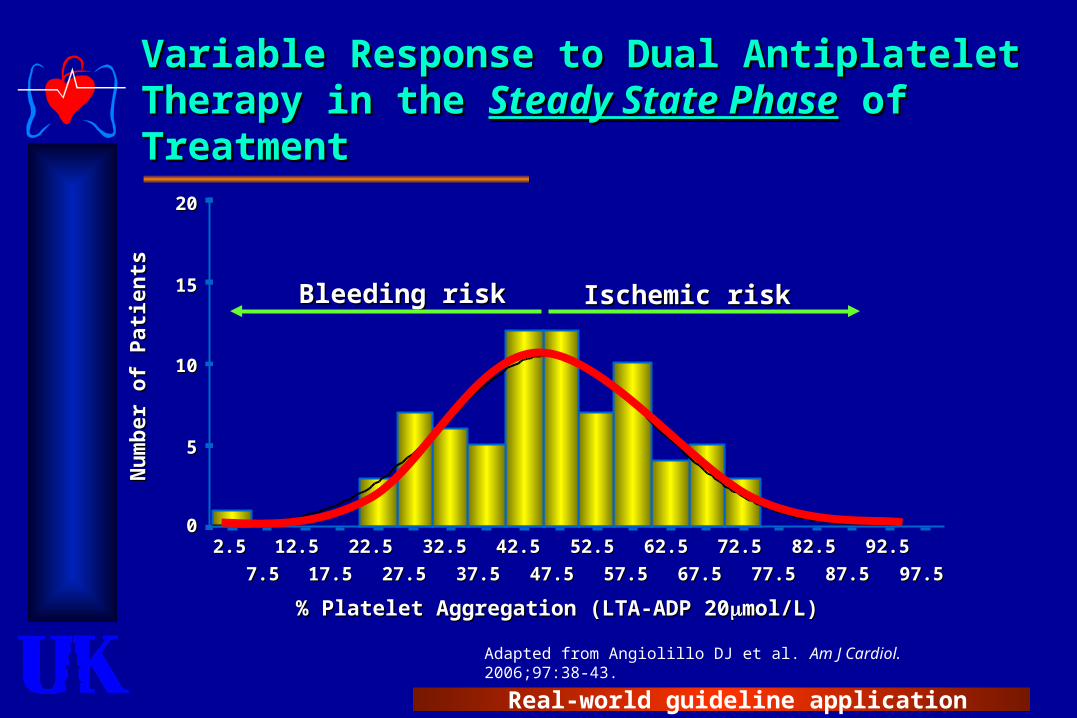
Adapted from Angiolillo DJ et al. Am J Cardiol. 2006;97:38-43.
Variable Response to Dual Antiplatelet Variable Response to Dual Antiplatelet Therapy in the Therapy in the Steady State PhaseSteady State Phase of of TreatmentTreatment
% Platelet Aggregation (LTA-ADP 20% Platelet Aggregation (LTA-ADP 20mol/L)mol/L)
97.597.5
92.592.5
87.587.5
82.582.5
77.577.5
72.572.5
67.567.5
62.562.5
57.557.5
52.552.5
47.547.5
42.542.5
37.537.5
32.532.5
27.527.5
22.522.5
17.517.5
12.512.5
7.57.5
2.52.5
2020
1515
1010
55
00
Nu
mb
er o
f P
atie
nts
Nu
mb
er o
f P
atie
nts
Bleeding riskBleeding risk Ischemic riskIschemic risk

Real-world guideline application
There Is a Problem – Aspirin & Bleeding Time
Some patients have hyper-response to aspirin.
Bleeding time back to normal in 2-3 days even in hyper-responders.
0 1 2 3 4 5 6 7 8
Days following ASA ingestion
0
2
4
6
8
10
12
14
16
Te
mp
late
ble
ed
ing
tim
e (
min
)
Ferraris VA, et al. Ann Surg. 2002;235:820-7.
Real-world guideline application
Another Problem – Aspirin Resistance
Topol, 20035–10% of patients taking usual
doses of aspirin are ‘aspirin resistant’. Normal platelet aggregation to ADP &
Arachidonic acid.
Aspirin resistant patients have 2 to 3 times increased incidence of death, MI, or stroke.
Gum PA, JACC. 2003;41:961-5.
Real-world guideline application
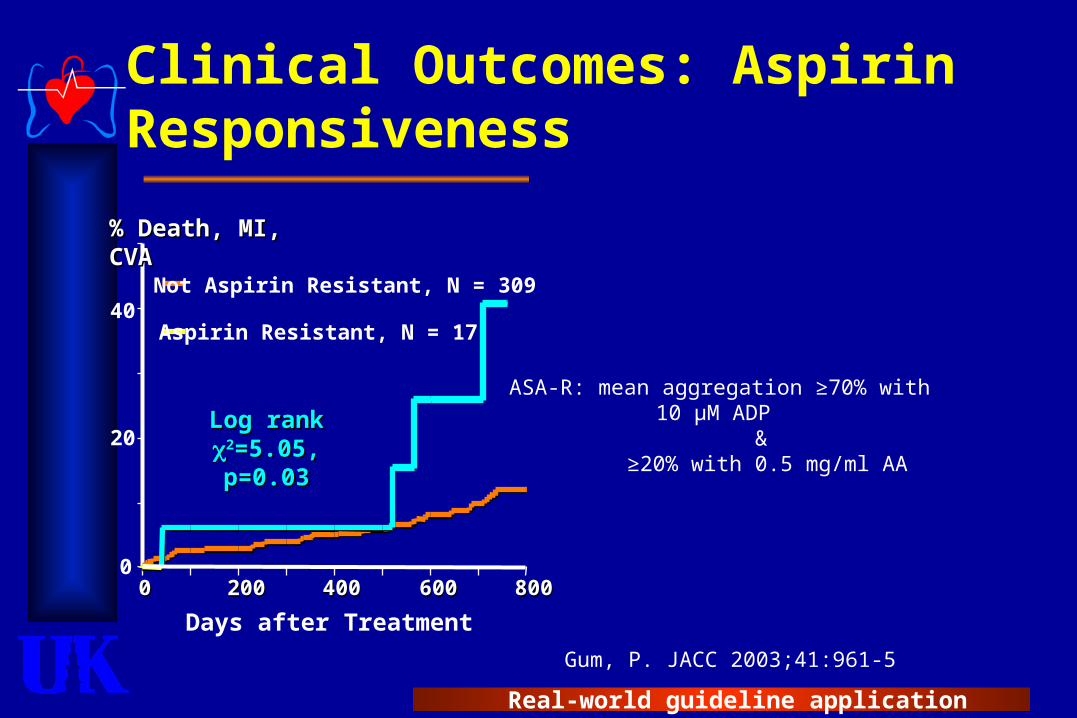
ASA-R: mean aggregation ≥70% with 10 µM ADP
& ≥20% with 0.5 mg/ml AA
Clinical Outcomes: Aspirin Responsiveness
0
20
40
00 200200 400400 600600 800800
Days after Treatment
Not Aspirin Resistant, N = 309
Aspirin Resistant, N = 17
% Death, MI, CVA% Death, MI, CVA
Log rank Log rank 22=5.05, =5.05, p=0.03p=0.03
Gum, P. JACC 2003;41:961-5
Real-world guideline application
What to Expect From Guidelines
Aspirin & postoperative bleeding.Guidelines recommend stopping
aspirin in only very elective patients before operation.Class IIa recommendation.
Variability in response to aspirin is common and should be expected.
Practice variation should be reduced if guidelines are followed.
Ferraris VA et al. Ann Thorac Surg. 1998;45:71-4.;Gum PA, JACC. 2003;41:961-5.
Real-world guideline application
Do Thienopyridines Cause Postoperative Bleeding?
Evidence is more compelling than for aspirin
11 studies with clopidogrel & CABG. All studies show increased bleeding
when clopidogrel given within 5 days of CABG – some with increased mortality.
AHA/ACC & STS guidelines recommend stop clopidogrel for 5 days before operation, if possible.
Ferraris VA, et al. STS Guidelines. Ann Thorac Surg. 2005;79:1454-61.; www.acc.org, Accessed Jan. 2006.

Real-world guideline application
Thienopyridines (Plavix®) & Postoperative Bleeding
Study Pts. Outcome in clopidogrel-treated patients.CURE Investigators. NEJM,
2005; 345:492.910
Increased major bleeding if plavix-treated within 5 days of CABG in UA/NSTEMI patients.
van der Linden, Circulation.2005;112:I276.
37Increased bleeding & re-exploration – aprotinin used in one
group
Akowuah, ATS. 2005;80:149.
24Increased mortality, transfusion, and re-exploration in
placebo - aprotinin & EACA used in one group.
Von Heymann, CCM;2005:33:2241.
36 Increased chest tube drainage & non-heme.
Lindvall, ATS. 2005;80:922. 18 Increased transfusion (heme & non-heme), & re-exploration
Ascione, ATS. 2005;79:1210.
91 Increased mortality, transfusion and re-exploration.
Chu, ATS. 2004;78:1536. 41 Increased transfusion (heme & non-heme)
Chen, JTCVS. 2004;128:425. 45 Increased transfusion (heme & non-heme)
Gansera, Thorac Cardiovasc Surg.2003;51:185.
64Increased transfusion (heme and non-heme), & re-
exploration
Ray, BMC Cardiovasc Disord, 2003;3:3.
57 Increased re-exploration & transfusion
Yende, CCM. 2002;29:2271. 51 Increased transfusion (heme & non-heme) & re-exploration.
Hongo, JACC. 2002:40:231. 59 Increased morbidity, transfusion, & re-exploration.
Real-world guideline application
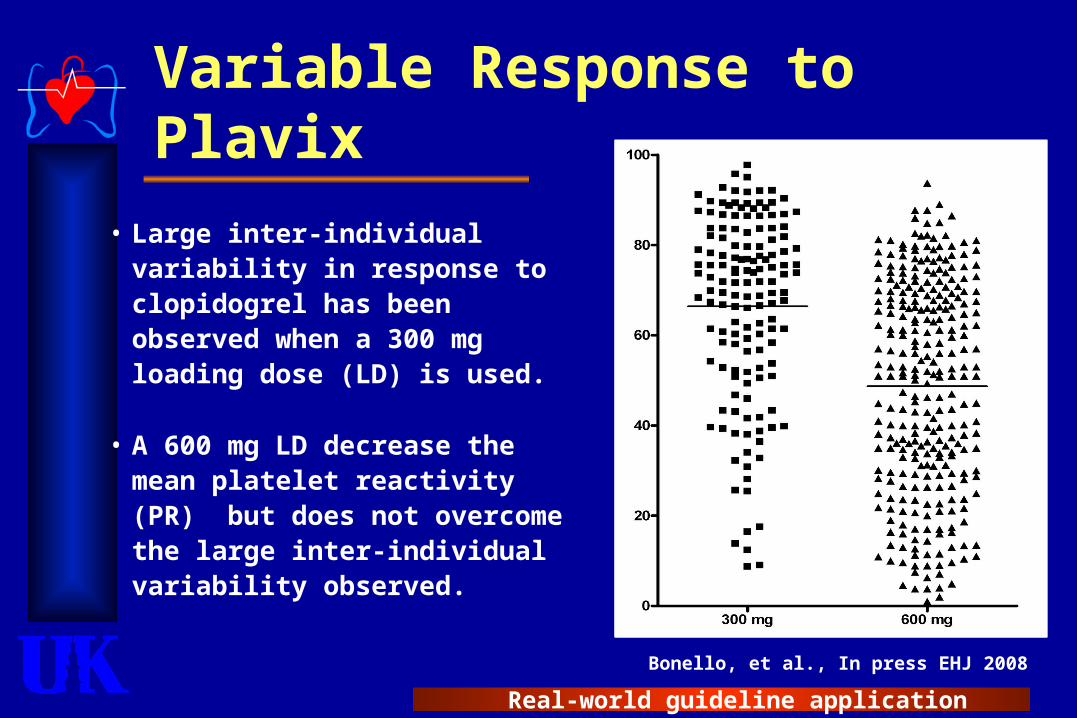
Variable Response to Plavix
• Large inter-individual variability in response to clopidogrel has been observed when a 300 mg loading dose (LD) is used.
• A 600 mg LD decrease the mean platelet reactivity (PR) but does not overcome the large inter-individual variability observed.
Bonello, et al., In press EHJ 2008

Real-world guideline application
VASP Index
++ADP AC
cAMP
PKA
VASPVASP VASP-VASP-PP
GP 2b/3a complexGP 2b/3a complex
Fibrinogen bindingFibrinogen binding
Inactivated PlateletsInactivated Platelets
PGE1PGI2
--
Activated platelets
P2Y12 ADP-receptor
VASP index : standardized and reproducible.
Highly specific for response to clopidogrel.
Horstrup et al. Eur J Biochem 1994;225:21-7Horstrup et al. Eur J Biochem 1994;225:21-7 Geiger et al. Arterioscler Thromb Vasc Biol. Geiger et al. Arterioscler Thromb Vasc Biol. 1999;19:2007-11.1999;19:2007-11.
Real-world guideline application
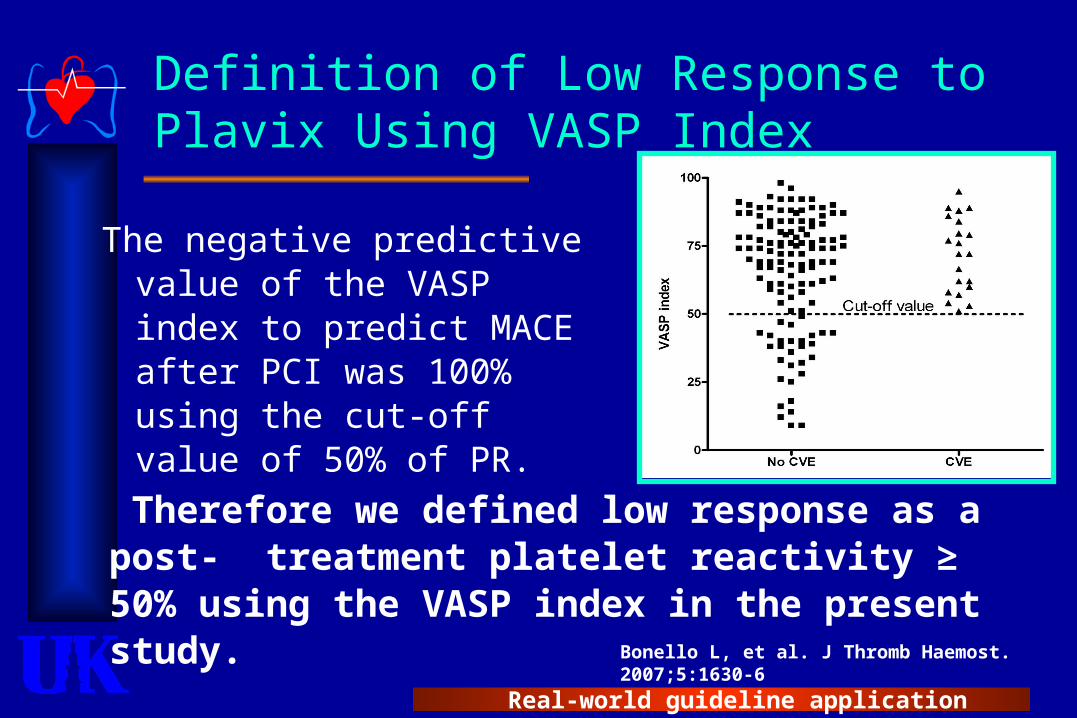
Definition of Low Response to Plavix Using VASP Index
The negative predictive value of the VASP index to predict MACE after PCI was 100% using the cut-off value of 50% of PR.
Bonello L, et al. J Thromb Haemost. 2007;5:1630-6
Therefore we defined low response as a post- treatment platelet reactivity ≥ 50% using the VASP index in the present study.
Real-world guideline application
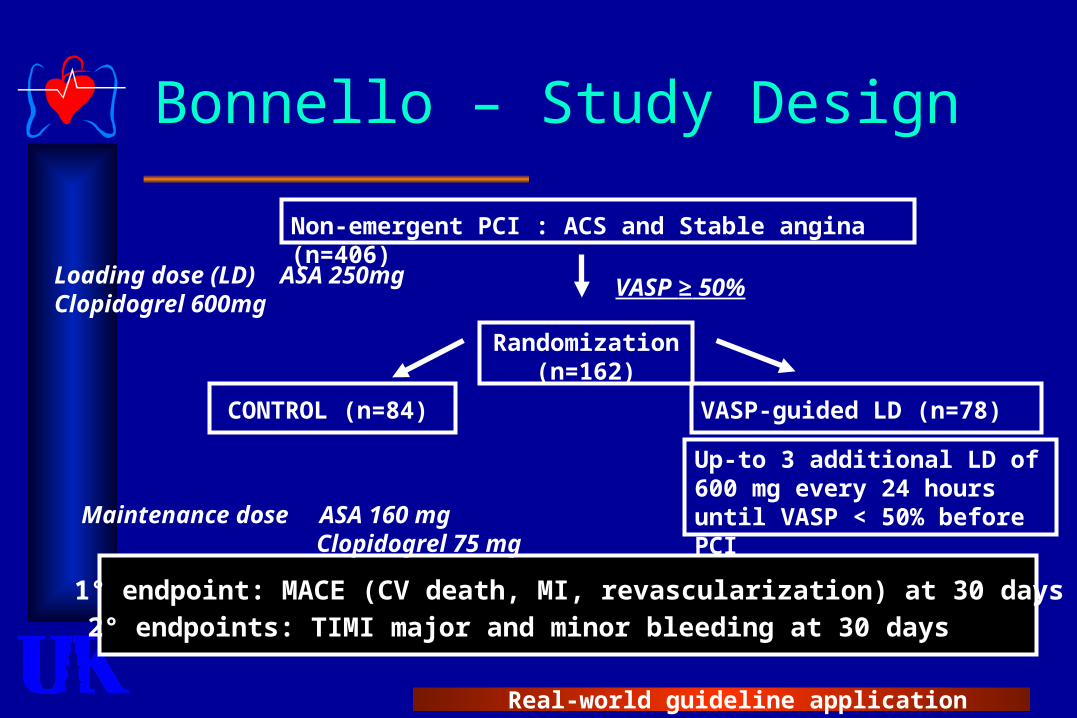
Bonnello – Study Design
Non-emergent PCI : ACS and Stable angina (n=406)
Loading dose (LD) ASA 250mg Clopidogrel 600mg
VASP ≥ 50%
Randomization(n=162)
CONTROL (n=84) VASP-guided LD (n=78)
Up-to 3 additional LD of 600 mg every 24 hours until VASP < 50% before PCIMaintenance dose ASA 160 mg
Clopidogrel 75 mg
1° endpoint: MACE (CV death, MI, revascularization) at 30 days
2° endpoints: TIMI major and minor bleeding at 30 days
Real-world guideline application
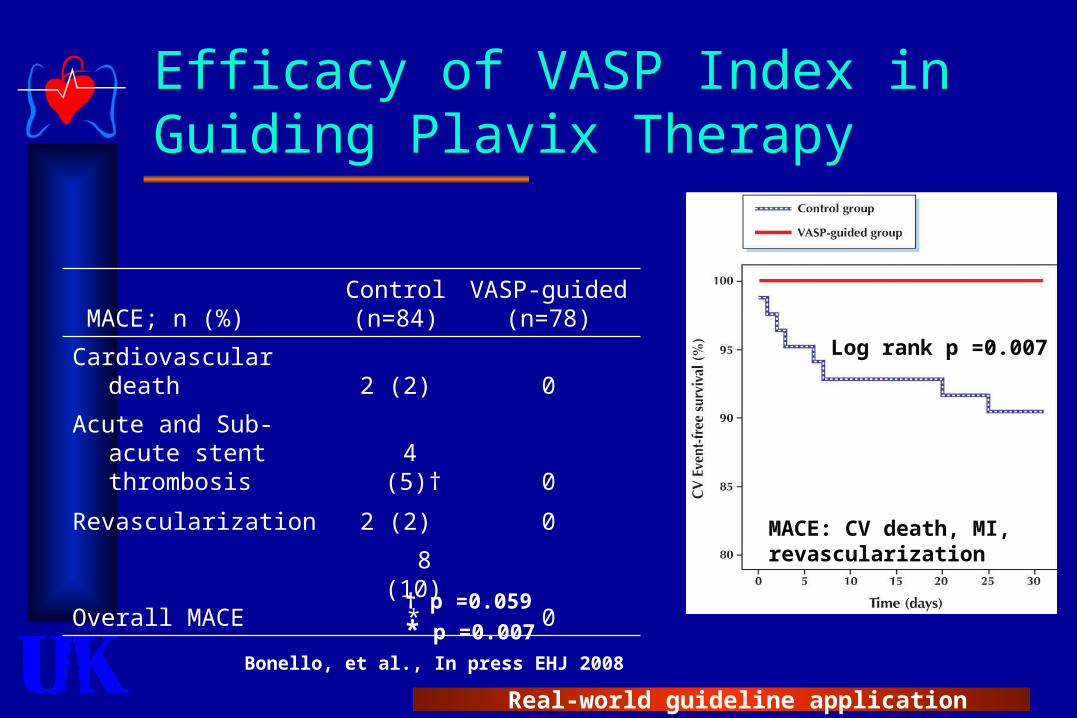
Efficacy of VASP Index in Guiding Plavix Therapy
MACE; n (%)Control(n=84)
VASP-guided(n=78)
Cardiovascular death 2 (2) 0
Acute and Sub-acute stent thrombosis 4 (5)† 0
Revascularization 2 (2) 0
Overall MACE 8 (10)* 0
† p =0.059
* p =0.007
MACE: CV death, MI, revascularization
Log rank p =0.007
Bonello, et al., In press EHJ 2008
Real-world guideline application
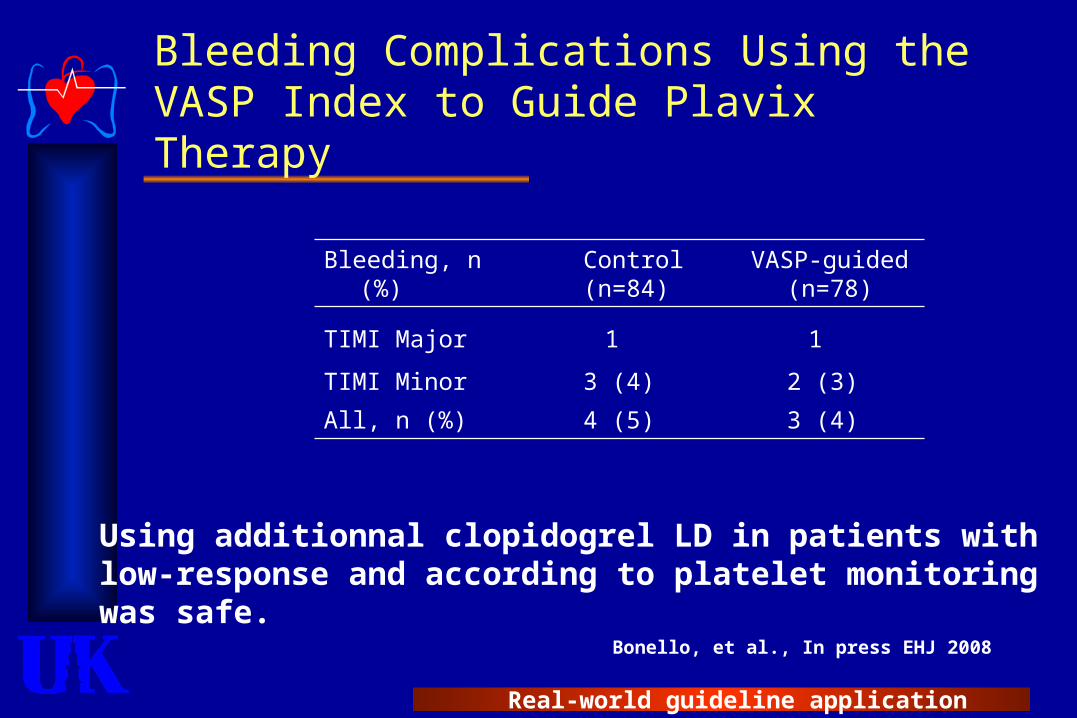
Bleeding Complications Using the VASP Index to Guide Plavix Therapy
Bleeding, n (%) Control (n=84)
VASP-guided (n=78)
TIMI Major 1 1
TIMI Minor 3 (4) 2 (3)
All, n (%) 4 (5) 3 (4)
Using additionnal clopidogrel LD in patients with low-response and according to platelet monitoring was safe.
Bonello, et al., In press EHJ 2008

Real-world guideline application
Real-world guideline application
Real-world guideline application
Case #1 – Question #2
Can you stop clopidogrel?No good information.
Common side-effect of evidence-based review.
Identify knowledge deficits.
AnswerUnknown!Not enough evidence.
Real-world guideline application
Evidence-Based Blood Conservation Strategies
Top 4 Preoperative interventions
Select high risk – “pull out all the stops” Limit anti-thrombotic & anti-platelet drug effect.
Limit blood loss during operation Anti-fibrinolytics Off-pump procedures Perfusion strategies (centrifugal pump w/ membrane)
Salvage & sequester blood (not as helpful in high-risk)
Cell saver, pump salvage, etc. Hemodilution (predonation)
Manage blood resources (process of care variables) Multimodality approach Transfusion algorithm & point-of-care testing.

Real-world guideline application
What Works for Blood Conservation?
Multiple interventions are better than a few ‘favorite’ interventions.
TQM approach – ‘Measurement & Management’.
‘Outcome greater than sum of parts’ Examples
Normovolumic hemodilutionAprotinin
Real-world guideline application
Normovolemic Hemodilution – Class IIb Recommendation
5 prospective studies 3 showed no benefit 2 showed benefit Not possible to do meta-analysis.
Contraindications Urgent operation Anemia Sepsis
May be beneficial when used as part of a multimodality approach.
Real-world guideline application
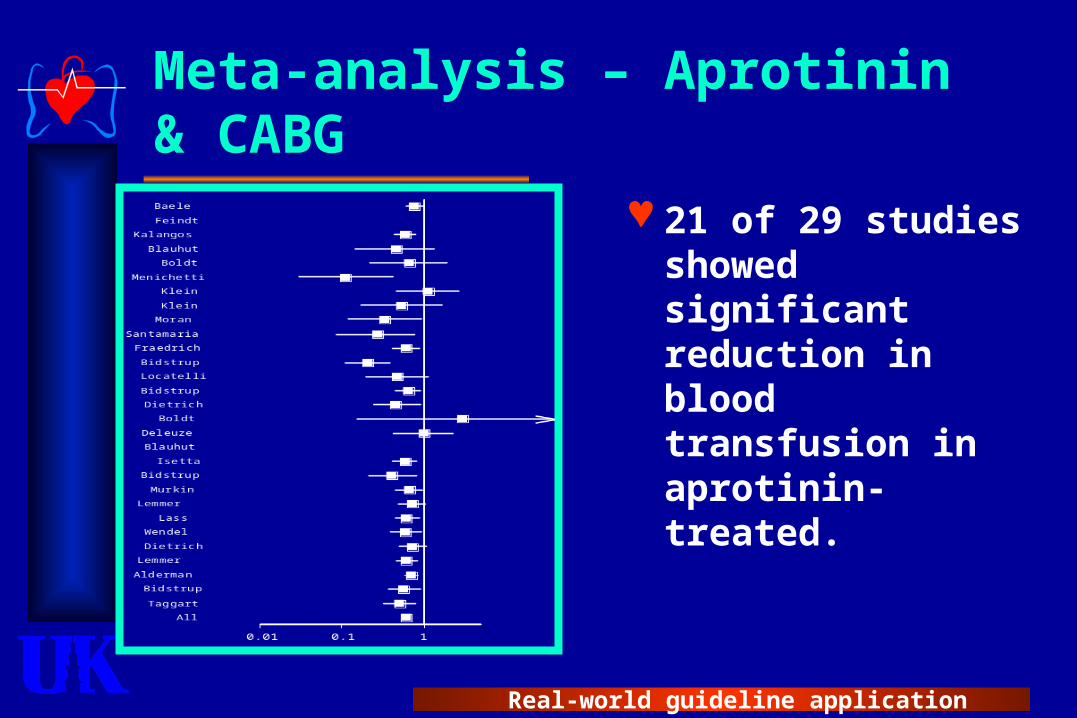
Meta-analysis – Aprotinin & CABG
21 of 29 studies showed significant reduction in blood transfusion in aprotinin-treated.

Real-world guideline application
Aprotinin Safety Issues
Safety concerns3 observational studies suggest
increased renal toxicity, possibly increased mortality, and no benefit in blood usage.
No mortality benefit despite reduced transfusion – problem of competing risks.
Bayer no longer markets aprotininOnly available for compassionate use.
Real-world guideline application
Anti-fibrinolytic Drugs & Guidelines
Class I.Anti-fibrinolytic drugs
indicated to reduce blood transfusion & re-exploration in high risk patient.
Aprotinin is probably best but not readily available.

Real-world guideline application
Case #1 – Question #3
Are there interventions that can help? Multimodality blood management
program is best. 61 recommendations, not just ‘one
magic bullet’. Aprotinin is not the only blood
conservation intervention!
Answer Yes!

Real-world guideline application
Case #2 – Postoperative Bleeding
Patient history 62 year-old man
Unstable angina. Drug-eluting stent 2 years ago (now on ASA
only) Started on eptifibatide (Integrelin®) in CCU Uneventful 3-v CABG 4-6 hours after stopping
eptifibitide. Four hours after operation, he is bleeding 100
to 200 cc per hour. Stat Hg is 7 mg/dL He has had 1000cc of 5% albumin and 1000cc
of crystalloid solution.
Real-world guideline application
Postoperative BleedingShould you be worried?
You’d better start swimmingOr you’ll sink like a stone.
… It’ll soon shake your windows
And rattle your walls.For the times they are a-changin.
Bob Dylan
Real-world guideline application
Case #2 - Questions
1. Will this patient benefit from transfusion?
2. Is there an evidence-based transfusion algorithm that guides therapy in this patient?
3. Should routine clotting & coagulation tests be ordered?
Real-world guideline application
More Is Known About the Risks of Blood Transfusion Than the Benefits!
RBC Shape Change During Storage
RBC Shape Change During Storage
Day 1 Day 21 Day 35Horvav T et al Horvav T et al Transfusion Transfusion 1999 39(3):277-2811999 39(3):277-281

Real-world guideline application
Bleeding After PCI Is a Risk for 1-year Mortality (5,384 patients)
Independent predictors of 1-year mortality.
Ndrepepa, 2008
Variable Hazard Ratio (95% CI)
Bleeding w/in 30 days 2.96 (1.96 -4.48)
MI w/in 30 days 2.29 (1.52 – 3.46)
Urgent revascularization w/in 30d
2.49 (1.16 - 5.35)
Age (years) 2.27 (1.78 – 2.89)
Diabetes 1.47 (1.11 – 1.96)
Multivessel CAD 2.72 (1.58 -4.67)
Elevated troponin 1.77 (1.27 -2.47)
LV ejection fraction 0.71 (0.60 – 0.85)
Creatinine 1.10 (1.06 – 1.14)

Real-world guideline application
Two Evil Things About Postoperative Bleeding
Blood loss Hypovolemia Shock Worse outcome
from organ failure
Re-operation for tamponade or bleeding.
Blood transfusion Diseases
transmission Immune
modulation (TRALI)
Transfusion errors
Real-world guideline application
Competing Risks
Risk of intervention (e.g. PCI, CABG) Bleeding Transfusion Reintervention MI, stroke, etc.
Risks of disease state (e.g. UA/NSTEMI) Death MI Stroke
Equation favors interventions in highest risk patients

Real-world guideline application
Case #2 – Question #1
Will this patient benefit from transfusion? Jehovah’s witness would say no. There are two bad things about blood
management Blood loss Blood transfusion
Answer Highly uncertain ‘Maybe’ (consensus)
Biggest benefit may be to increase cardiac output.

Real-world guideline application
Two Reasons For Variability in Transfusion Practices
Physician & institution practices are hard to manage (control is a bad word!).
Accurate & timely information is not available (‘lab’ takes too long).
Stover, Anesthesiology. 1998;88:327.

Real-world guideline application
Problems with Interventions - Consensus Guidelines for RBC Transfusion
Transfusion indicated Transfusion not indicated Uncertain benefit of transfusion
Hgb ≤ 6.0 on CPB Hgb ≥ 10 after CPB without critical end-organ ischemia.
Hgb between 8 -10g/dl in a stable patient benefit is unclear.
Hgb ≤ 8.0 in high risk (age > 65, and/or co-morbidity).
Acute blood loss (30% of blood volume).
Rapid blood loss without immediate control.
Hgb ≤ 10 g/dl in certain patients with critical end-organ ischemia.
Ferraris VA, et al. STS Guidelines on blood conservation. Ann Thorac Surg, 2006. In press.
Real-world guideline application
Guidelines for Transfusion of Non-red Cell Hemostatic Factors
No evidence base!Transfuse for clinical
bleeding only.
Can be guided by accurate & timely point-of-care tests (e.g. Platelet count, PFA-100, TEG, POC PT/PTT, etc.). Ferraris VA, et al. STS Guidelines on blood
conservation. Ann Thorac Surg, 2006. In press.
Real-world guideline application
Transfusion Algorithms
7 RCT’s tested transfusion algorithms w/ point-of-care testing to reduce transfusion.6 of 7 RCT’s showed reduced
transfusion or re-exploration rates. Didn’t matter what type of POC testing.Various algorithms used.
Ferraris VA, et al. STS Guidelines on blood conservation. Ann Thorac Surg, 2006. In press.
Real-world guideline application
Point-of-Care Testing
Fibrinolysis & fibrinogenTEG, MCA 210, TAS system
Coagulation factorsWhole blood aPTT & PT
PlateletsBleeding time, PFA-100, TEG, RPFA
Despotis, Semin Thorac Cardiovasc Surg, 11:84-104. 1999

Real-world guideline application
Transfusion Algorithms & POC Testing – An Example
Study Pts Algorithm POC tests Outcome
Avidan, 2004
210 •Transfuse PRBC for Hb ≤ 8.0.
•DDAVP for abnormal PFA-100 followed by platelets if no response to DDAVP.
•Aprotinin for abnormal TEG amplitude.
•Explore for failure to respond & continued bleeding.
•TEG•PFA-100•Hepcon
Decreased transfusion of heme & non-heme blood products.
Avidan MS, Br J Anaesth. 2004; 92:178.
Real-world guideline application
Case #2 – Question #2
Is there an evidence-based transfusion algorithm that guides therapy in this patient? Defining an algorithm is more
important than the content of the algorithm.
Answer Yes! (if everybody agrees on
algorithm)

Real-world guideline application
Case #2 – Question #3
Should routine clotting & coagulation tests be ordered?Routine tests don’t help – too
little too late
AnswerNo! (point-of-care tests are best,
combined with algorithm).

Real-world guideline application
Conclusions – Take Home Messages
High risk patients benefit most. Multimodality approach is best –
especially with algorithm-driven transfusion.
Benefits of blood transfusion not as great as expected.
Inconsistent response to interventions is common (e.g. aspirin and plavix).
Guideline preparation identifies deficit in data.

Real-world guideline application
STS Evidence-Based Workforce
Blood conservation writing groupWriter Organization
Victor A. Ferraris, M.D., Ph.D. (Chair)
University of Kentucky
Suellen P. Ferraris, Ph.D. University of Kentucky
Sibu P. Saha, M.D., M.B.A. University of Kentucky
Constance K. Haan, M.D. University of Florida
B. David Royston, M.D. Harefield Hospital, UK
Charles R. Bridges, M.D. (Chair, Evidence-Based Workforce)
University of Pennsylvania
Robert S.D. Higgins, M.D. Rush Presbyterian, St. Luke’s Medical Center
George J. Despotis, M.D. Washington University
Jeremiah R. Brown, Ph.D. Dartmouth Univ.
Real-world guideline application
Society of Cardiovascular Anesthesia Guideline ReviewersBlood conservation reviewing group
Reviewer Organization
Bruce Spiess, M.D. (Chair) Virginia Commonwealth University
Linda Shore-Lesserson, M.D. Mount Sinai School of Medicine
Mark Stafford-Smith, M.D. Duke University
C. David Mazer, M.D. St. Michael’s Hospital, Toronto
Elliott Bennett-Guerrero, M.D. Duke University
Steven E. Hill, M.D. Duke University
Simon Body, M.B., Ch.B., M.P.H. Harvard University
Real-world guideline application
Thanks
Questions?