application of adult health nursing skills ( nur 317...
TRANSCRIPT
0
King Saud University
College of Nursing
Medical Surgical Department
Application of Adult Health Nursing Skills
( NUR 317 )
1
Course Outline
Topic
Date
No. of
Weeks
Faculty Responsible
for the Lecture
Registration week January 27, 2015 1 Ms.AlwahAlKathiri
Miss. GhadaAlbothi
Orientation / Introduction / Overview
Review Health assessment of patients
Clinical Package
February 3, 2015 2
Care for patients with pain
Pain Rating Scale
Patient Controlled Anesthesia
Medications: Morphine, Paracetamol, Tramadol
February 4, 2015
2
Ms.AlwahAlKathiri
Care for patients undergoing surgical intervention
- Pre Operative Instructions
- Preoperative Checklist
- Skin Preparation
- Early Ambulation
- Wound Care
- Home Care
Medications: Co Amoxiclav, Cefazolin, Ceftriaxone
Return Demonstration:
Deep Breathing Exercises/ Leg exercises
Miss.GhadaAlbothi
Care for patients with fluid and electrolytes imbalance
Assessment of Edema, Dehydration
IVF
February 10, 2015
3
Ms.AlwahAlKathiri
2
Care for patients with Respiratory system disorders
Nebulization
Suctioning
Incentive Spirometry
Medications: Aminophylline, Salbutamol
February 11, 2015 3
Miss.GhadaAlbothi
Care for patients with Cardiovascular system disorders
Cardiac Catheterization
Electrocardiogram (ECG)
Medications: Captopril, Digoxin. Heparin
Return Demonstration:
Nebulization
Suctioning
Application of ECG Leads
Ms.AlwahAlKathiri
Quiz 1
(Health Assessment, Care of patients with Pain,)
February 17, 2015
4
Midterm Exam
(Care for patients with Fluid and Electrolyte Imbalance
,undergoing surgical intervention , with Respiratory,
Cardiovascular System Disorders)
February 24, 2015
5
Care of Patients with Neurological Disorders
Electroencephalogram (EEG)
Medications: Dilantin, Mannitol
March 3,2015 6
Miss.GhadaAlbothi
Care of patients with Gastrointestinal system disorders
Endoscopy, Proctoscopy
NGT Feeding
Medications: Ranitidine, Metoclopramide,Dolcolax
March 10,2015 7
Ms.AlwahAlKathiri
3
Care of patients with Urinary system disorders
Intravenous Pyelogram (IVP)
KUB Ultrasound, Lithotripsy
Catheterization
Arteriovenous (AV)Shunt
Medications: Lasix, Aldactone
March 17,
2015 8
Miss.GhadaAlbothi
Spring Break
Quiz 2
(Care of Patients with Neurological, Gastrointestinal
System Disorders)
March 31,
2015 9
Care of patients with Endocrine system disorders
Blood Glucose Monitoring
Insulin Administration
Radioactive Iodine Uptake
Medications: Insulin, Glucophage, Thyroxine
April 7,
2015
10
Ms.AlwahAlKathiri
Care of Patients with Musculoskelatal Disorders
Orthopedic Bed
Traction
Assistive Devices (Crutch, Canes. Braces)
Medications: Baclofen, Diazepam, Ampicillin
Sulbactam
April 14,
2015
11
Miss.GhadaAlbothi
CASE PRESENTATION
April 21,2015 12
By students April 28 ,2015 13
May 5,2015 14
FINAL EXAMINATION
(Care of patients with Urinary, Endocrine ,
Musculoskeletal System Disorders)
May 14,2015 15

4
Pain rating scale
Patient controlled anesthesia
Pain medications
Care for patients with pain

5
Care for patients with pain
Because perception and tolerance of pain vary widely from individual to individual, pain is difficult to
define and describe. There are two types of pain acute and chronic.
Acute pain is short duration pain usually occur as a result of injury, surgery or illness. This type of pain includes acute injuries, post postoperative pain .
Chronic pain is an ongoing condition usually develops more slowly and lasts much longer than acute such as back pain and headaches.
Pain Assessment
• Precipitating/Alleviating Factors:
– What causes the pain? What aggravates it? Has medication or treatment worked in the past?
• Quality of Pain:
– Ask the patient to describe the pain using words like “sharp”, dull, stabbing, burning”
• Radiation
– Does pain exist in one location or radiate to other areas?
• Severity
– Have patient use a descriptive, numeric or visual scale to rate the severity of pain.
• T iming
– Is the pain constant or intermittent, when did it begin, and does it pulsate or have a rhythm
Assessment ToolsPain
6
Pharmacological Interventions
Opioids:
• are medications that relieve pain.
• They reduce the intensity of pain signals reaching the brain and
• Used for moderate or severe pain
• Agonists is a drug that activates certain receptors in the brain to reduce pain
• Agonists-antagonists is a drug that blocks brain receptors .
Nonopioids:
• Used alone or in conjunction with opioids for mild to moderate pain
• Acetaminophen
• NSAIDS
Adjuvants:
• as a pharmacological agent added to a drug to increase or aid its effect
• Used for analgesic reasons and for sedation and reducing anxiety.
• Tri-cyclic antidepressants
• Anticonvulsants
Non-Pharmacological Pain Management
• Heat & Cold applications
• Relaxation techniques, distraction
• Music therapy
• Massage
NOTE: The above management techniques are meant to supplement, not replace
pharmacological interventions.
What is Patient Controlled Analgesia?
• Patient Controlled Analgesia (PCA) uses a
programmable syringe pump to allow patients
to self-administer their own intravenous
analgesia

7
Understanding PCA
The PCA device is a programmable syringe pump, which delivers the opioid infusions according to
individualised settings:
– Bolus dose
– Lockout time
– Dose duration
– Background infusion
Bolus dose
• When the patient presses the remote button, the PCA delivers the programmed bolus
dose
• In cases of severe pain or in patients with large opioid requirements the bolus dose may
be several times higher than the usual protocol
Lockout time
• Lockout time is usually set at 5 minutes
• The PCA will not deliver a dose during lockout time, even if the patient presses the button
• This allows each bolus to reach peak effect before the patient has another bolus
• Lockout time reduces the risk of overdose
Good tries / Bad tries
• A good try is when the PCA delivers a bolus dose of analgesia
• A bad try is when the patient presses the button during the lockout time and no bolus
dose is delivered
• Knowing the proportion of good and bad tries allows medical staff to adjust the PCA
settings to meet the patient’s needs or whether further patient education is required.
Dose duration
• Dose duration is normally set as ‘stat’
– Alaris PCA ‘stat’ is 70 seconds
– The dose duration may be increased to prevent problems such as light-
headedness or nausea associated with a rapid peak of onset of analgesia.

8
Background infusion
• Background infusion (continuous infusion) may be added to improve analgesia
• Generally background infusion is only required for patients following major surgery or
patients with oncology-related pain and high opioid requirements
• Background infusions may increase the risk of the side effects associated with opioids:
– sedation, respiratory depression, itch, nausea.
Advantages of PCA
• Pain is in “control” by patient
• Rapid response to demand for analgesia
• Reduced patient anxiety
• Fewer complications
• Increased staff, patient and family satisfaction
• Decreased staff workload
Patient selection ( Indication ) :
PCA is suitable for treatment of most types of acute and acute-on-chronic pain:
• Surgical
• Medical
• Trauma
• Burns
• Oncology
Contraindications to PCA
• Inability to understand the concept of PCA
• Children not wishing to control their own analgesia.
Nursing role for patient using PCA
• Adjust Correct dose of opioid
• Accurate documentation
• Observation of vital signs
• Documented pain scores
• Monitoring:
9
• sedation scores
• respiratory effort, rate, depth
• oxygen saturation
• heart rate
• The number of good and bad tries are documented
• The total dose of opioid received is also recorded
operative education-Pre
• The anaesthetist will discuss PCA with the patient pre-operatively
• Explain the basic principles of PCA to patient prior to surgery
• Reminding patient post-operatively about using PCA effectively
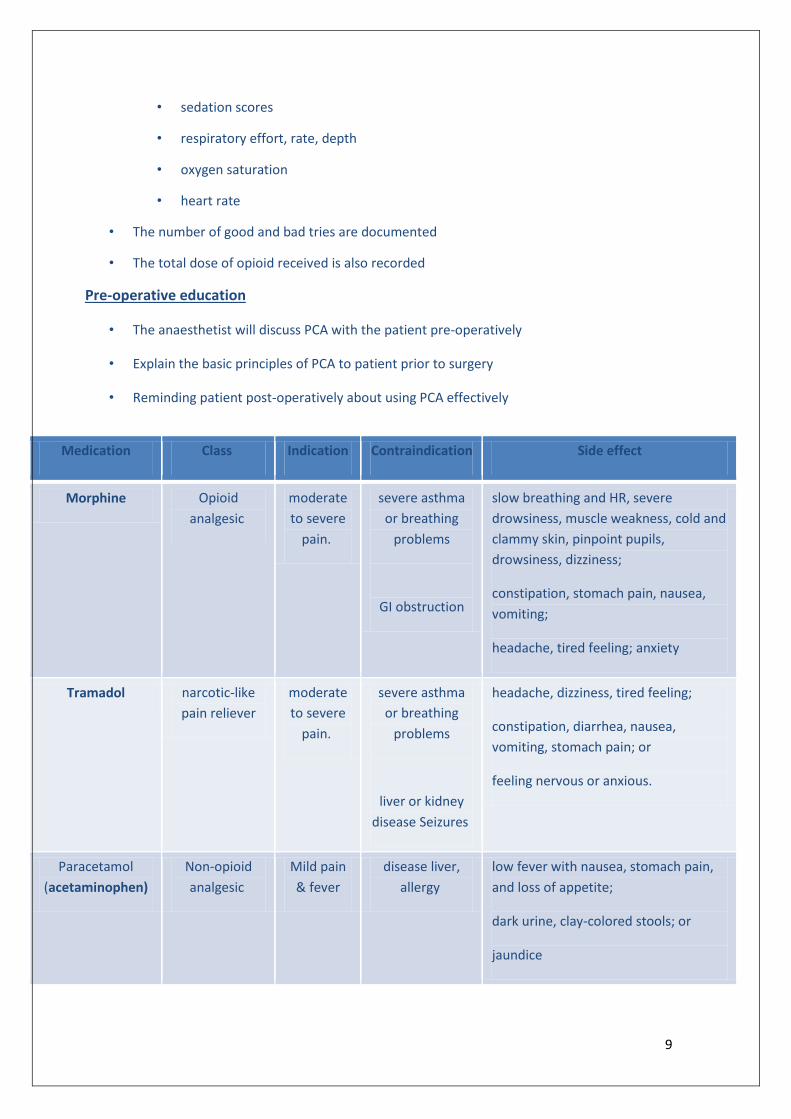
Side effect Contraindication Indication Class Medication
slow breathing and HR, severe
drowsiness, muscle weakness, cold and
clammy skin, pinpoint pupils,
drowsiness, dizziness;
constipation, stomach pain, nausea,
vomiting;
headache, tired feeling; anxiety
severe asthma
or breathing
problems
GI obstruction
moderate
to severe
pain.
Opioid
analgesic
Morphine
headache, dizziness, tired feeling;
constipation, diarrhea, nausea,
vomiting, stomach pain; or
feeling nervous or anxious.
severe asthma
or breathing
problems
liver or kidney
disease Seizures
moderate
to severe
pain.
narcotic-like
pain reliever
Tramadol
low fever with nausea, stomach pain,
and loss of appetite;
dark urine, clay-colored stools; or
jaundice
disease liver,
allergy
Mild pain
& fever
Non-opioid
analgesic
Paracetamol
(acetaminophen)

10
Pre- Operative Instructions
Preoperative Checklist
Skin Preparation
Early Ambulation
Wound Care
Home Care
Medications: Co Amoxiclav, Cefazolin, Ceftriaxone
Care for patients undergoing surgical
intervention
11
Care for patients undergoing surgical intervention
Phases of Perioperative Period
1. Preoperative - begins when the decision for surgical intervention is made and ends with the transference of the patient to the operating room
ROLE OF THE NURSE:
Establishing a baseline assessment of the patient in clinical setting or at home
Carrying out a preoperative interview
Preparing the patient for anesthetic he is to receive and the surgery he is to undergo
2. Intraoperative – begins when the patient is admitted or transferred to the Surgery department and ends when he is admitted to the recovery area
ROLE OF THE NURSE:
Starting the IV and giving IV medications
Carrying out the full scope of physiologic monitoring throughout a surgical procedure
Providing for the patient safety
Acting in the role of the scrub nurse / circulating nurse a- Circulating nurse : Registered nurse who coordinates and documents
patient care in the operating room b- Scrub nurse : Registered nurse , licensed practical nurse , or surgical
technologist who scrubs and dons sterile surgical attire , prepares instruments and supplies , and hands instruments to the surgeon during the procedure
Assisting in positioning the patient on the operating table using basic principles of body mechanics
3. Post operative- begins with the admission of the patient in the recovery room and ends with the follow up evaluation in the clinical setting or at home
ROLE OF THE NURSE:
Assessing the post operative status of the patient in terms of anesthetic effect and the impact of surgery on body image or role function
Evaluating the family’s perception of the surgery
Communicating patient’s information about surgery to personnel in the Recovery or Surgical nursing unit
I - PERIOPERATIVE PERIOD Nursing process overview
1. ASSESSMENT A. General physical Assessment
Nutritional status Respiratory status ( difficulty of breathing, bronchial Asthma, Blood gas
analysis) Cardiovascular Status Hepatic and Renal Function

12
Endocrine Function (life threatening hazard: hypoglycemia, glucosuria) Immunologic function (Allergy, Blood transfusion Reactions,
Immunosuppressive medications Effects of aging ( hydration status, modified lifestyle) Prior drug therapy (history of drug use ( adrenal steroids, diuretics,
phenothiazines, antidepressants, insulin, antibiotics ( “Mycin “ drugs) B. Psychosocial Nursing Assessment
Preoperative Anxiety (fears of pain or death, fear of the unknown, fear of destruction of body image, fear of separation) Financial worries, Poor prognosis
Denial of anxiety
C. Patient problems l Nursing Diagnosis insufficient / inadequate information related to disease condition/
anesthetic agent worry, depression and fear related to diagnosis and outcome of surgery post operative pain and complication risk factors related to previous lifestyle and history ( weight problems,
smoking history, allergy
2. PLANNING AND IMPLEMENTATION
A. Preparation: Approach the patient with an air of decision and interest in his well
being Determine exactly what procedures are to be performed Explain what you are about to do
B. General physical Status
replacement of deficits, obesity, addiction to narcotics, drugs or alcohol stop smoking 4-6 weeks before surgery, maintain adequate ventilation ,
antibiotics avoid sudden changes in position, prolonged immobilization, hypotension,
hypoxia and overloading of the body with fluids or blood report sneezing , coughing, sniffling to the physician
C. Preoperative Anxiety
Have the patient express his anxiety. Listen to the patient Spiritual Therapy Recreation and diversion
D. Nutrition and Fluids
Intravenous Access Light diet for dinner NPO post midnight
E. Intestinal Preparation
Warm cleansing enema
F. Preoperative Skin Preparation Warm, relaxing bath or shower prior to surgery, using betadine soap

13
Skin at and around the operative site NOT be shaved (check hospital policy)
3. OPERATIVE PERMIT/ INFORMED CONSENT Surgeon informs the patient regarding complications, disfigurement,
postoperative expectations in clear and simple terms Permission is repeated for each operation, for each procedure to enter a
body cavity and when general anesthesia is given Patient may sign his own permit for operation if he is of age and
mentally capable No patient should be forced to sign an operative permit
4. PREOPERATIVE PATIENT EDUCATION
a. Deep Breathing and Coughing Patient placed in sitting position Instruct patient to breathe deeply, exhale through his mouth take a short breath and cough from deep in the lungs Splint incision so that pressure is minimized and pain is controlled
b. Turning and Active Body Movement
Turn patient side to side assuming Sim’s Lateral position ROM Exercises (Extension and flexion of the knees and hip joints, Rotation of
foot
c. Immediate Preoperative Preparation Patient is brought to the OR 30-60 minutes before anesthesia is to be started Patient in hospital gown, untied and open in the back For long hair, Hair is plaited in two braids, hairpins removed, cover hair with
disposable paper cap Remove jewelries, dentures, prosthetic devices and labelled clearly with the
patient’s name and stored in a safe place according to hospital policy Have patient void, measure urine and note time and amount and record in
the preoperative checklist Administer preanesthetic medications to reduce patient’s anxiety or reduce
secretions 45 to 75 minutes before anesthesia is begun
II - INTRA OPERATIVE PERIOD a. Anesthesia – produces a state of narcosis, analgesia, relaxation and reflex loss
General (liquid, gas)
Parts of the body (regional, spinal, local, topical)
Position in the Operating Room
Dorsal recumbent
Trendelenburg Position
Lithotomy
Sim’s Lateral
b. Principles of Perioperative Asepsis ( sterile to sterile, unsterile to unsterile)
14
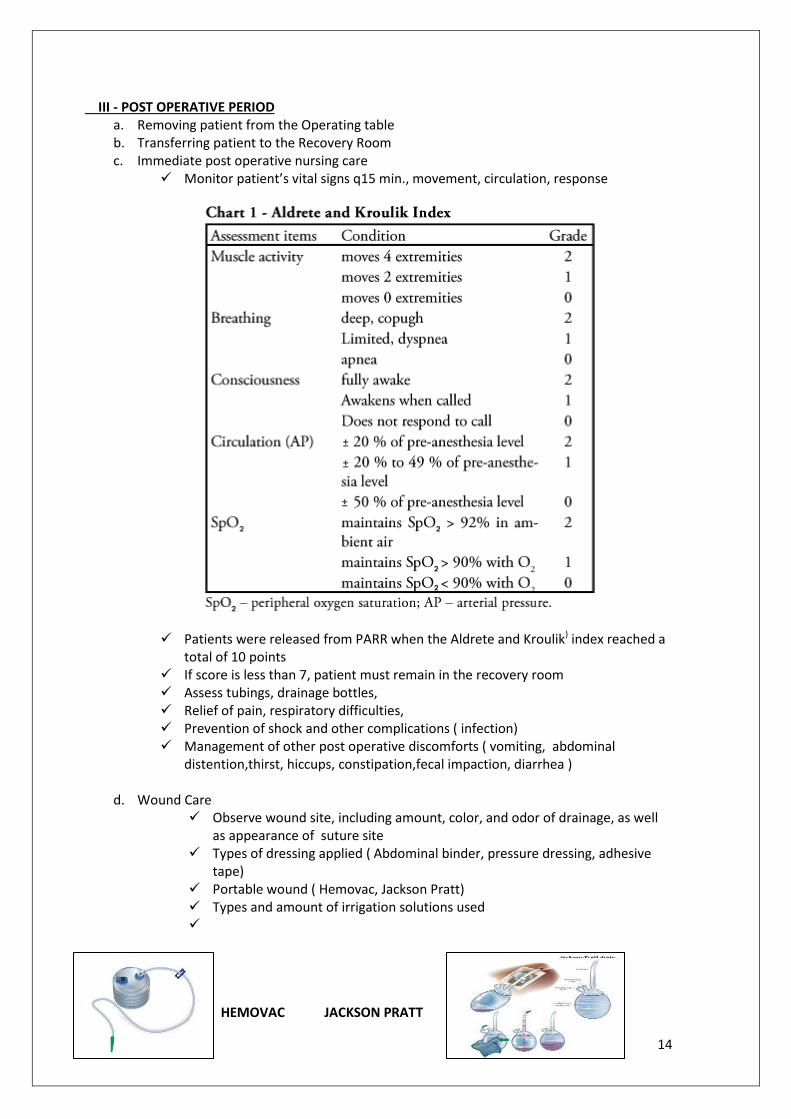
III - POST OPERATIVE PERIOD a. Removing patient from the Operating table b. Transferring patient to the Recovery Room c. Immediate post operative nursing care
Monitor patient’s vital signs q15 min., movement, circulation, response
Patients were released from PARR when the Aldrete and Kroulik) index reached a total of 10 points
If score is less than 7, patient must remain in the recovery room Assess tubings, drainage bottles, Relief of pain, respiratory difficulties, Prevention of shock and other complications ( infection) Management of other post operative discomforts ( vomiting, abdominal
distention,thirst, hiccups, constipation,fecal impaction, diarrhea )
d. Wound Care Observe wound site, including amount, color, and odor of drainage, as well
as appearance of suture site Types of dressing applied ( Abdominal binder, pressure dressing, adhesive
tape) Portable wound ( Hemovac, Jackson Pratt) Types and amount of irrigation solutions used
HEMOVAC JACKSON PRATT

15
e. Home Care Pain management Wound care and dressing changes Monitoring for infection Activity restrictions Recommended sexual activity Ability to perform self care activities Eating
Bowels
Diaphragmatic Breathing Exercises This is the most effective form of breathing exercise. During inspiration, the upper abdominal muscles enlarge displacing the dome of the diaphragm and enabling the air to rush into the lungs. During expiration, the abdominal muscles contract and air moves out.
Steps Rationale
1. Position the head of a bed in 45 degrees (semi-fowlers position).
2. Make a loose fist and allow one of your hands to rest lightly on the upper chest and the other one below your rib cage
This will allow you to feel
the chest movement as
you breathe.
3. Breath out gently and fully as the ribs sink down and inward toward midline
4. Breathe in gently and fully through the nose and mouth letting the abdomen rise as the lungs fill with air. As much as possible do not move the hand positioned on the upper chest.
5. Hold this breathe for a count of five.
6. Tighten your abdominal muscle and let out all the air through your mouth (exhale). Use the pursed lip breathing techniques (as if you are blowing off a candle). Do not move the hand positioned on the upper chest.
7. repeat this exercise around 15 times, twice a day by taking short rest in between a group of five.
Coughing Exercises Coughing exercises help in clearing mucus by dislodging it in the respiratory tract. Sometimes, coughing exercises may feel very uncomfortable but the good thing is that, it cannot harm the incision site.
1. In a sitting position, lean forward and position your interlaced fingers across the incision site in order to give it support when coughing. You can also use a pillow to support the incision.
2. Inhale around 3-4 deep breathe through your nose and exhale by use of pursed lip technique as discussed above.
3. Take a deep breath through your nose. Hold the breath for a few seconds.
4. Expel the air out sharply by saying “hack” around 3-4 times.
5. Take another deep breath and immediately give a strong cough once or twice
6. Repeat this exercise 3-4 times a day or as long as you feel comfortable doing it.

16
Leg Exercises This is done to improve the leg circulation and to promote venous return.
Turning Patient on the Side •Flex uppermost leg and use a pillow to support it while turning on the side. •Instruct patient to Hold on the side rail to give him extra support that he needs during turning. These exercises can help in preventing possible complications and improving the recovery process but should only be performed if recommended by a physician. Some exercises like early ambulation requires assistance from health care personnel and should not be attempted by any unstable patient. Other patients are put under complete bed rest and no exercise should be performed. Consult your physician before starting any form of exercise.
Medications;
Co Amoxiclav,
Cefazolin,
Ceftriaxone
Co-Amoxiclav , Amoxicillin Classification:
Antibiotic
Action:
Amoxicillin is a semisynthetic penicillin (beta-lactam antibiotic) that inhibits peptidoglycan synthesis leading to weakening of the cell wall, which is usually followed by cell lysis and death.
Indications
Sinus Infection • Pneumonia
Acute otitis media • Acute exacerbations of chronic bronchitis (adequately diagnosed) • Community acquired pneumonia • Cystitis, Urinary Tract infection (UTI) • Pyelonephritis • Skin and soft tissue infections in particular cellulitis.
STEPS
1. Position the head of the bed in a 45 degree or lie in a semi-fowler’s position.
2. Slightly flex or bend your knee and raise your foot up, hold it in that same position for a few seconds. Extend it and lower it on the bed.
3. Perform this exercise for five times with one leg then move to the other leg and repeat the same exercise.
4. Assume that you are tracing a circle by use of your feet. Bend the legs down, towards each other, up and then outwards.
5. Perform this exercise for at least five times.
17
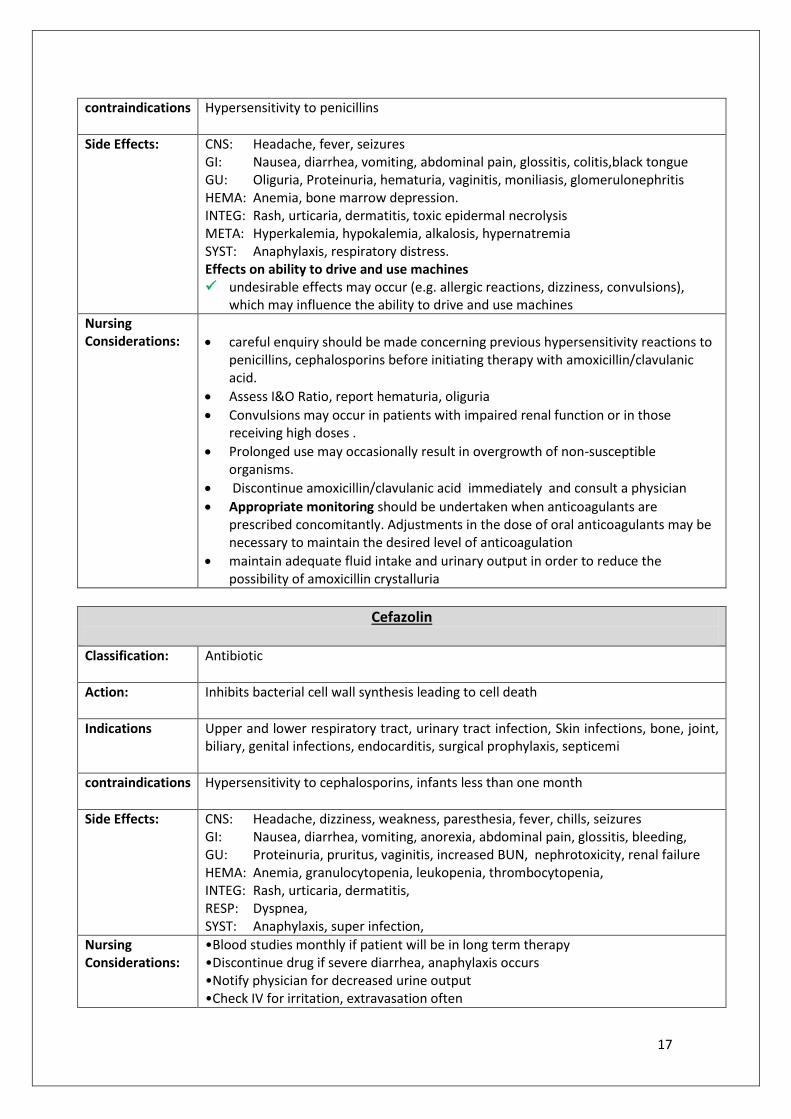
contraindications
Hypersensitivity to penicillins
Side Effects:
CNS: Headache, fever, seizures GI: Nausea, diarrhea, vomiting, abdominal pain, glossitis, colitis,black tongue GU: Oliguria, Proteinuria, hematuria, vaginitis, moniliasis, glomerulonephritis HEMA: Anemia, bone marrow depression. INTEG: Rash, urticaria, dermatitis, toxic epidermal necrolysis META: Hyperkalemia, hypokalemia, alkalosis, hypernatremia SYST: Anaphylaxis, respiratory distress. Effects on ability to drive and use machines undesirable effects may occur (e.g. allergic reactions, dizziness, convulsions),
which may influence the ability to drive and use machines
Nursing Considerations:
careful enquiry should be made concerning previous hypersensitivity reactions to penicillins, cephalosporins before initiating therapy with amoxicillin/clavulanic acid.
Assess I&O Ratio, report hematuria, oliguria
Convulsions may occur in patients with impaired renal function or in those receiving high doses .
Prolonged use may occasionally result in overgrowth of non-susceptible organisms.
Discontinue amoxicillin/clavulanic acid immediately and consult a physician
Appropriate monitoring should be undertaken when anticoagulants are prescribed concomitantly. Adjustments in the dose of oral anticoagulants may be necessary to maintain the desired level of anticoagulation
maintain adequate fluid intake and urinary output in order to reduce the possibility of amoxicillin crystalluria
Cefazolin
Classification:
Antibiotic
Action:
Inhibits bacterial cell wall synthesis leading to cell death
Indications
Upper and lower respiratory tract, urinary tract infection, Skin infections, bone, joint, biliary, genital infections, endocarditis, surgical prophylaxis, septicemi
contraindications
Hypersensitivity to cephalosporins, infants less than one month
Side Effects:
CNS: Headache, dizziness, weakness, paresthesia, fever, chills, seizures GI: Nausea, diarrhea, vomiting, anorexia, abdominal pain, glossitis, bleeding, GU: Proteinuria, pruritus, vaginitis, increased BUN, nephrotoxicity, renal failure HEMA: Anemia, granulocytopenia, leukopenia, thrombocytopenia, INTEG: Rash, urticaria, dermatitis, RESP: Dyspnea, SYST: Anaphylaxis, super infection,
Nursing Considerations:
•Blood studies monthly if patient will be in long term therapy •Discontinue drug if severe diarrhea, anaphylaxis occurs •Notify physician for decreased urine output •Check IV for irritation, extravasation often

18
Ceftriaxone
Classification:
Antibiotic
Action:
Inhibits bacterial cell wall synthesis leading to cell death
Indications
Upper and lower respiratory tract, urinary tract infection, Skin infections, bone, joint, biliary, genital infections, endocarditis, surgical prophylaxis, septicemi
contraindications
Hypersensitivity to cephalosporins, infants less than one month
Side Effects:
CNS: Headache, dizziness, weakness, paresthesia, fever, chills, seizures GI: Nausea, diarrhea, vomiting, anorexia, abdominal pain, glossitis, bleeding, GU: Proteinuria, pruritus, vaginitis, increased BUN, nephrotoxicity, renal failure HEMA: Anemia, granulocytopenia, leukopenia, thrombocytopenia, INTEG: Rash, urticaria, dermatitis, RESP: Dyspnea, SYST: Anaphylaxis, super infection,
Nursing Considerations:
Check blood glucose if diabetic
Report sore throat, bruising, bleeding, joint pain; may indicate blood dyscrasia; diarrhea with mucus; blood may indicate pseudomembranous colitis
Report persistent diarrhea
19