appendix a1 - springer978-0-387-22427-5/1.pdf · place for bone consolidation to occur. following...
TRANSCRIPT

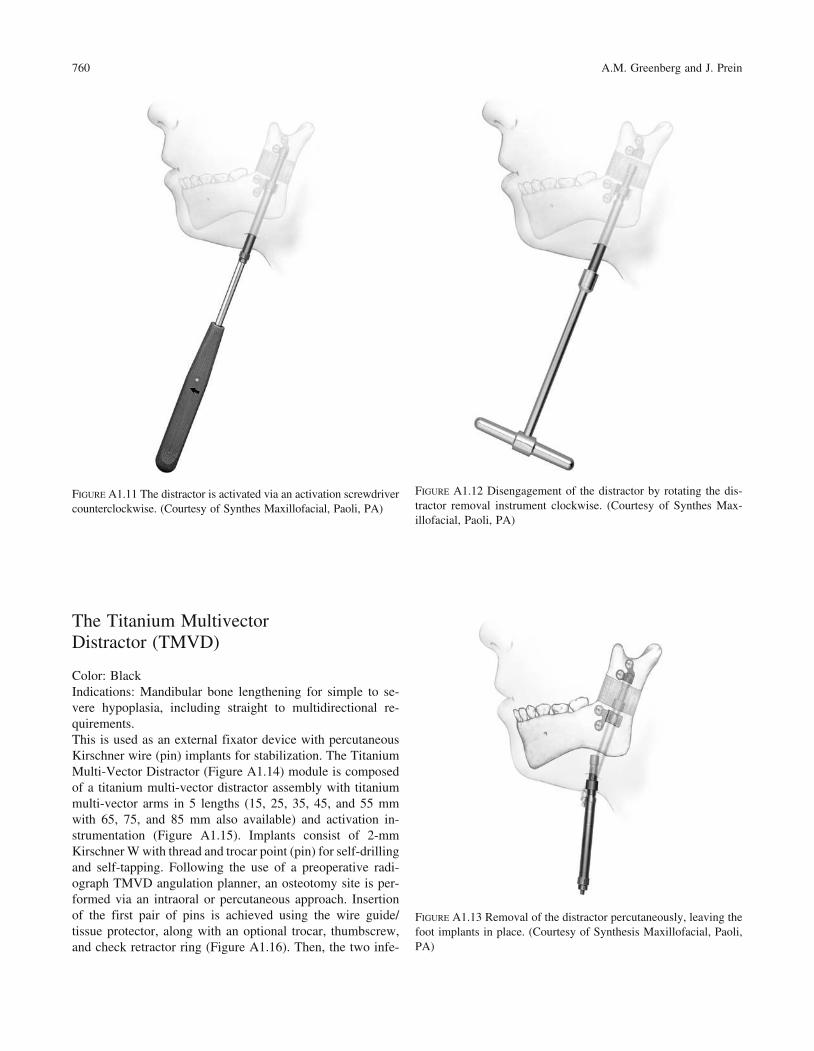
tal attachments (Figure A1.7). In addition, detached right footand left foot proximal implants for initial bone anchorage andsubsequent are mandibular distractor attachment included(Figure A1.8). The distractor is placed on the mandible span-ning the osteotomy site, with an external activator extendingthrough a small submandibular percutaneous incision. Thescrews utilized are 2.0 self-tapping screws in 6-, 8-, 10-mmlengths (12 and 14 are also available) and 2.4-mm emergencyscrews in 6-, 8-, 10-mm lengths (12 and 14 are also available).In evaluating ramus height on radiographs, the Single VectorAngulation Planner should be used to determine distractorlength as well as vector and foot placement. The drilling ofholes and insertion of screws is performed utilizing the plateholding trocar, which stabilizes the implant (Figure A1.9).First, on the superior aspect of the planned osteotomy, the de-tachable proximal foot is placed with slot inferior (FigureA1.10a). Then, the distractor body is inserted into the proxi-mal foot (Figure A1.10b) to complete screw fixation of thedistractor device. Activation and percutaneous exposure areachieved (Figure A1.10c). The implants are activated by anactivation screwdriver with an internal hex (Figure A1.11),which has a directional arrow for counterclockwise activationin which one rotation equals .5 mm. Usually two rotations,which equal 1 mm of distraction, are recommended on a dailybasis, but this is subject to variability at the surgeon’s discre-tion. The total days of distraction multiplied by two equals thenumber of days recommended for the distractor to remain inplace for bone consolidation to occur. Following consolida-tion, a 3-step procedure is followed for distractor body re-moval. First, the activator screwdriver is turned clockwise 10rotations (opposite to the arrow handle marker). Then distalfoot disengagement is achieved by turning the distractor re-moval instrument 4 clockwise rotations (in the direction of thearrow marker) (Figure A1.12). Then the distractor body is re-moved via the percutaneous port (Figure A1.13). The modulecontains the black narrow screwdriver blade (self-retaining),1.5-mm drill bits (Stryker J latch), distractor removal instru-ment, and activation screwdriver.
757
Appendix A1Distraction Osteogenesis of the MandibleAlex M. Greenberg and Joachim Prein
Mandible Single Distractor Module Stainless Steel Set
Color: BlackIndications: Mandibular ramus lengthening
The Mandible Distractor Module Set (Figure A1.1) is com-posed of stainless steel implants, specifically a mandibulardistractor with right foot and mandibular distractor with leftfoot (Figure A1.2). The distractor is placed on the mandiblespanning the osteotomy site with an external activator ex-tending through a small submandibular percutaneous incision(Figure A1.3). The screws utilized are 2.0-mm stainless steelself-tapping screws in 10-, 12-, and 14-mm lengths, and 2.4-mm stainless steel emergency screws in 10-, 12-, and 14-mmlengths. The implants are activated by an activation screw-driver. Figure A1.4 with an internal hex (Figure A1.5). Thisscrewdriver has a directional arrow for counterclockwise ac-tivation, in which one rotation equals .5 mm. Usually, two ro-tations, equal to 1 mm of distraction, are recommended on adaily basis, but this is subject to variability at the surgeon’sdiscretion. The total days of distraction multiplied by twoequals the number of days recommended for the distractor tobe in place for bone consolidation to occur. The placement ofthe distractor requires the use of the trocar system (FigureA1.6). The module also contains the black narrow screwdriverhandle, cruciform screwdriver blade (self-retaining), and 2.0-mm holding forcep (for screws).
The Titanium Single Vector Distractor
Color: BlackIndications: Mandibular ramus lengthening
The Titanium Single Vector Distractor Module is composedof titanium implants, specifically 20-mm and 30-mm lengthmandibular distracts with right foot and left foot types as dis-

758 A.M. Greenberg and J. Prein
FIGURE A1.1 Mandible distractor module set. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.4 Mandible distractor activation screwdriver. (Courtesyof Synthes Maxillofacial, Paoli, PA)
FIGURE A1.2 Mandible distractor with left foot. (Courtesy of Syn-thes Maxillofacial, Paoli, PA)
FIGURE A1.3 Mandible distractor in place. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.5 Mandible distractor activation. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.6 Mandible distractor placement with transcutaneous tro-car system. (Courtesy of Synthes Maxillofacial, Paoli, PA)

Appendix A1. Distraction Osteogenesis of the Mandible 759
FIGURE A1.7 Titanium single vector distractor. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.8 Right and left titanium single vector distractors withdetachable feet. (Courtesy of Synthes Maxillofacial, Paoli, PA)
FIGURE A1.9 Insertion of screws utilizing the plate holding trocar.(Courtesy of Synthes Maxillofacial, Paoli, PA)
a
b
c
FIGURE A1.10 (a) The detachable proximal foot is initially placedwith slot inferior, (b) the distractor is inserted for attachment, and(c) the percutaneous incision is made exposing the activation screw.(Courtesy of Synthes Maxillofacial, Paoli, PA)
The Titanium Multivector Distractor (TMVD)
Color: BlackIndications: Mandibular bone lengthening for simple to se-vere hypoplasia, including straight to multidirectional re-quirements.This is used as an external fixator device with percutaneousKirschner wire (pin) implants for stabilization. The TitaniumMulti-Vector Distractor (Figure A1.14) module is composedof a titanium multi-vector distractor assembly with titaniummulti-vector arms in 5 lengths (15, 25, 35, 45, and 55 mmwith 65, 75, and 85 mm also available) and activation in-strumentation (Figure A1.15). Implants consist of 2-mmKirschner W with thread and trocar point (pin) for self-drillingand self-tapping. Following the use of a preoperative radi-ograph TMVD angulation planner, an osteotomy site is per-formed via an intraoral or percutaneous approach. Insertionof the first pair of pins is achieved using the wire guide/tissue protector, along with an optional trocar, thumbscrew,and check retractor ring (Figure A1.16). Then, the two infe-
760 A.M. Greenberg and J. Prein
FIGURE A1.11 The distractor is activated via an activation screwdrivercounterclockwise. (Courtesy of Synthes Maxillofacial, Paoli, PA)
FIGURE A1.12 Disengagement of the distractor by rotating the dis-tractor removal instrument clockwise. (Courtesy of Synthes Max-illofacial, Paoli, PA)
FIGURE A1.13 Removal of the distractor percutaneously, leaving thefoot implants in place. (Courtesy of Synthesis Maxillofacial, Paoli,PA)

normal mandibular body horizontal size. This case report il-lustrates this procedure in a male with mandibular retrog-nathia secondary to a shortened ramus for which the patientunderwent bilateral mandibular single vector distraction os-teogenesis using the AO/ASIF Single Vector Distractor withimprovement in occlusion from Class II to Class I and moresatisfactory facial appearance (Figures A21–27). (Case reportof Prof. Dr. med Joachim Prein, Kantonsspital Basel, Basel,Switzerland).
Appendix A1. Distraction Osteogenesis of the Mandible 761
rior pins are inserted and the distractor assembly is placed,followed by completion of the osteotomy. Pins are cut to thedesired length and adjustment of the distractor assembly isperformed. Mandibular lengthening is achieved by turning theactivation instrument two rotations counterclockwise; fol-lowing the arrow marker is recommended (Figure A1.17), butis subject to the surgeon’s discretion. After a bony regener-ate of at least 10 mm has been achieved, angular adjustmentis performed using the angular adjustment instrument (Fig-ures A1.18A and B). After consolidation has occurred, the4.0-mm carbon fiber rod (60 and 80 mm, also available in100-200 mm in 20-mm increments) are applied with theTMVD clamp for carbon fiber rods after the distractor as-sembly has been removed (Figures A1.19 and A1.20).
Distraction Osteogenesis of the Mandible Case Report
Single vector distraction osteogenesis of the mandible is in-dicated for deformities of mandibular ramus hypoplasia with
FIGURE A1.14 Titanium multivector distractor. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.16 Insertion of screws via trocar. (Courtesy of SynthesMaxillofacial, Paoli, PA)
FIGURE A1.15 Titanium multivector distractor activation instrumen-tation. (Courtesy of Synthes Maxillofacial, Paoli, PA)
FIGURE A1.17 Activation of titanium multivector distractor withcounterclockwise turns. (Courtesy of Synthes Maxillofacial, Paoli,PA)

762 A.M. Greenberg and J. Prein
FIGURE A1.18 (a) Angular adjustment using the angular adjustmentinstrument. (b) Transverse adjustment using the angular adjustmentinstrument. (Courtesy of Synthes Maxillofacial, Paoli, PA)
FIGURE A1.19 (a) First, the carbon rod is placed. (b) The multivec-tor distractor body is removed. (c) The multivector distractor armsare then removed. (d) The carbon rod remains in place for consoli-dation. (Courtesy of Synthes Maxillofacial, Paoli, PA)
a
a
b
c
d
b

Appendix A1. Distraction Osteogenesis of the Mandible 763
FIGURE A1.20 Carbon rod in place maintaining the segment posi-tions while the bony regenerate undergoes consolidation. (Courtesyof Synthes Maxillofacial, Paoli, PA)
FIGURE A1.22 Patient with mandibular retrognathia lateral profileview.
FIGURE A1.21 Patient with mandibular retrognathia facial view. FIGURE A1.23 Preoperative lateral cephalometric radiograph demon-strating Class II malocclusion with mandibular ramus hypoplasia.

764 A.M. Greenberg and J. Prein
FIGURE A1.24 Postoperative lateral cephalometric radiographdemonstrating mandibular ramus lengthening with single vector dis-traction device with occlusion corrected to Class I.
FIGURE A1.26 Postoperative facial view with improved mandibularlengthening.
FIGURE A1.25 Postoperative lateral profile view with distractors stillin place with percutaneous exposure.
FIGURE A1.27 Postoperative lateral profile view with improvedmandibular lengthening and chin position.

Appendix A2ITI Strauman Dental Implant SystemAlex M. Greenberg
Recent developments in the ITI Strauman dental implant sys-tem (Figure A2.1) (Institut Strauman AG, Waldenburg,Switzerland) have improved the surface layer (SLE) as wellas the basic prosthetic procedures (Figures A2.2 and A2.3).Illustrated here are several examples of these techniques. A
simplified technique using solid abutments (Figures A2.4 andA2.5), transfer systems for impressions (Figures A2.6–A2.8),laboratory steps (Figures A2.9–A2.12) is shown. A specialorthodontic appliance is also available (Figure A2.13).
765
FIGURE A2.1 ITI implant in situ with ideal bone contact and gingi-val contour. (Courtesy of Institut Strauman AG, Waldenburg,Switzerland)
FIGURE A2.2 Corresponding abutment to the synOcta implant. (Cour-tesy of Institut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.3 Finite element model of entire synOcta implant testsetup. (Courtesy of Institut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.4 Overview of solid abutments. (Courtesy of InstitutStrauman AG, Waldenburg, Switzerland)
766 A.M. Greenberg
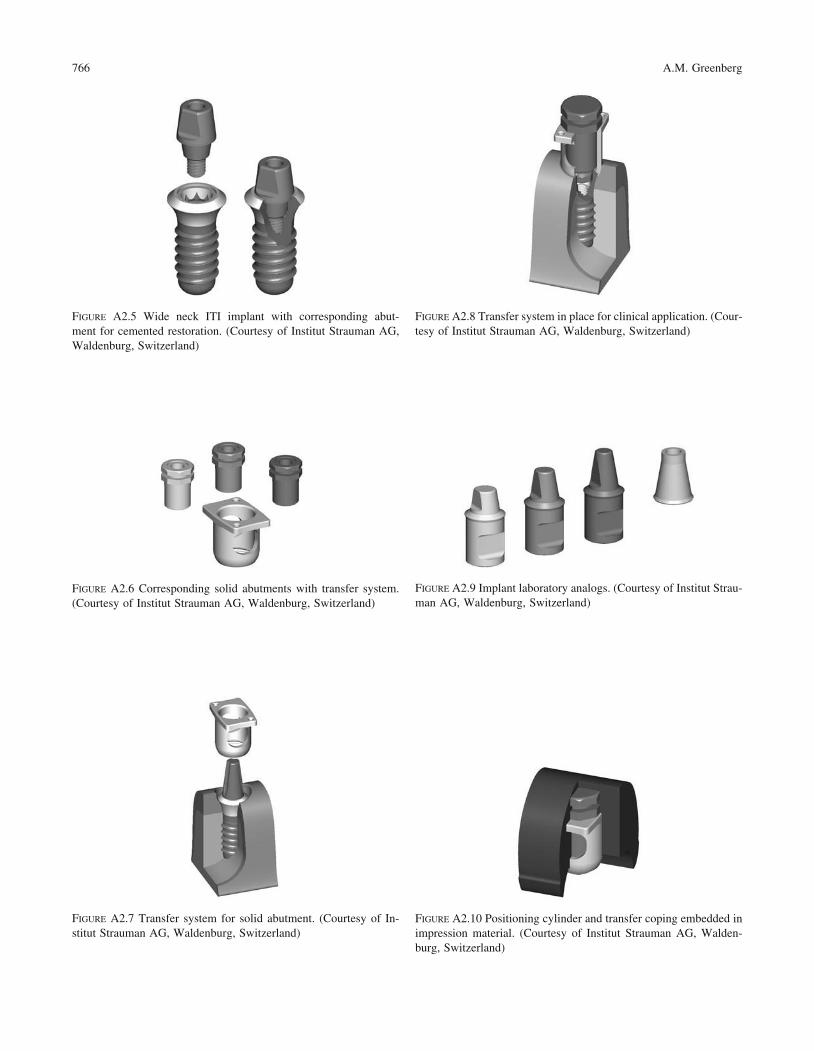
FIGURE A2.5 Wide neck ITI implant with corresponding abut-ment for cemented restoration. (Courtesy of Institut Strauman AG,Waldenburg, Switzerland)
FIGURE A2.6 Corresponding solid abutments with transfer system.(Courtesy of Institut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.7 Transfer system for solid abutment. (Courtesy of In-stitut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.9 Implant laboratory analogs. (Courtesy of Institut Strau-man AG, Waldenburg, Switzerland)
FIGURE A2.8 Transfer system in place for clinical application. (Cour-tesy of Institut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.10 Positioning cylinder and transfer coping embedded inimpression material. (Courtesy of Institut Strauman AG, Walden-burg, Switzerland)

Appendix A2. ITI Strauman Dental Implant System 767
FIGURE A2.13 Indication for use with an orthodontic appliance in combination with ITI implants. (Courtesy of Institut Strauman AG,Waldenburg, Switzerland)
FIGURE A2.11 Full metal implant laboratory analog in situ. (Cour-tesy of Institut Strauman AG, Waldenburg, Switzerland)
FIGURE A2.12 Master cast with implant laboratory analog. (Courtesyof Institut Strauman AG, Waldenburg, Switzerland)

AAbrasion injuries, craniomaxillofacial, 48Abutments
intrusion of, 248–250for ITI dental implants, 143–152selection of, by the restorative dentist,
234–235surgery at, and progressive bone
loading, 189Achondroplasia, saddle nose deformity in,
52Acrocephalosyndactyly. See Apert
syndromeAcrocephaly, defined, 10Acrylic implants
fractures of, 256self-cure versus light cured or
autopolymerized, 238–239wafer
construction of, cleft lip and palate,561
placement in a Le Fort I osteotomy,cleft lip and palate, 566
Actinomycotic osteomyelitis, 80Adaptation
membrane, in localized ridgeaugmentation, 156
in response to osteotomy, 639Adenoid cystic carcinoma, involving the
mandibular angle, 392–393Adenoid faces, 40Advantages
of genioplasty, 652of intraoral vertical ramus osteotomy,
646of mandibular midline split, 648of midface osteotomy, 657of rigid fixation
with mandibular sagittal split ramusosteotomies, 642–643
with maxillary surgery, 654of subapical osteotomy, 651
Aestheticsin craniomaxillofacial bone surgery,
280–286in Crouzon syndrome, assessment of,
713–714of dental implant restoration, 255–256
769
Index
in dental implant restoration, mandibleversus maxilla, 236–237
in Treacher Collins syndrome, 283Alar base, support of, in cleft lip and
palate, 540, 542Alar crease (A), for evaluation of
craniomaxillofacial deformity, 7Allogeneic grafts
healing of, 126–127for the maxillary sinus, 181–182for sinus lift procedures, outcomes, 132
Alloplastic graftsdefect-bridging, 419healing of, 126–127maxillary sinus, 182–184
Alternatives, consideration of risks andbenefits of bimaxillary surgery, 523
Alveolar augmentation, 160Alveolar defect, secondary, 549–550Alveolar nerve, inferior, computerized
tomography imaging of, 198, 201Amblyopia, preventing with surgery, in
Apert syndrome, 750Ameloblastomas, 59–61
bone resection and reconstruction in,166, 324
condylar prosthesis after surgery, 375panoramic images, 223–224reconstruction after surgery for, 406–408
American Association of Cleft PalateRehabilitation (AACPR), 23
Anastomoses, end-to-end, revascularizationof grafts as a result of, 125
Anatomyfacial, analysis of, 623–624in Le Fort II osteotomy, 660of the maxillary sinus, 179of midface hypoplasia, 664soft tissue landmarks, 7–8See also Facial anatomy
Andy Gump Deformity, 414–415Anesthesia
local, for hemostasis, 591during maxillary surgery, 528
Aneurysmsbasilar tip, transfacial access osteotomies
for repair of, 494
basilar tip and midbasilar artery,transfacial access osteotomies forrepair of, 489
midbasilar artery, transfacial accessosteotomies for repair of, 492
Angiofibromas, juvenile nasopharyngeal,resection with transfacial accessosteotomy, 489, 493
Angle classification, in skeletalmalocclusions, 38
Ankylosisbilateral condylar replacement with steel
prosthesis in, 376condylar prostheses in patients with,
377–381fibrous, of the temporomandibular joint,
following rigid fixation, 619Anterior areas, in maxillary implant
positioning, 244, 246–247Anterior examination, before orthognathic
surgery, 506–509Anterior mandibular defects, microvascular
tissue transfer for, 414–418Antibiotics
for posttraumatic osteomyelitistreatment, 433
in transfacial access osteotomies, 496Apertognathia
anteriormaxillary osteotomies for correction
of, 603secondary to posterior maxillary
vertical hyperplasia, 586tongue habits as a cause of, 647
Apert syndrome (acrocephalosyndactyly),35–36, 664, 679–680, 682
bilateral coronal synostosis in, 675craniosynostosis in, 673hypertelorism and telecanthus in, 509surgical correction of craniofacial
deformities in, 749–755temporal abnormality in, 11
Apicocoronal positioning, in single toothrestorations, 250
Application, of classification of cranialbone deformities, 96–97
Arteriogram, of a midbasilar arteryaneurysm, 492

Arthroplastyautogenous, 343costochondral, relative advantages and
disadvantages of, 343interpositional, for treating restricted
mobility of the temporomandibularjoint, 353–354
partial, replacement of the condyle in,372
Arthrosis, before costochondralreconstruction, 463
Ascending ramus, microvascularreconstruction of, 462–477
Assessment. See EvaluationAsymmetry assessment, 8Auricle
deformity of, 16in hemifacial microsomia, 730
reconstruction of, in hemifacialmicrosomia, 733
Autogenous bone graftscontraindications to, 377maxillary sinus, 180–181for maxillofacial reconstruction,
295–309for ridge augmentation, 157
Autoimmune disorders, deformitiesinfluenced by, 5
Autologous bone graftshealing of, 125–126resorption of, 129vascularized, healing of, 126
Avulsion injuries, craniomaxillofacial, 43
BBar-retained overdentures, 241–242Barrier membrane, for localized ridge
augmentation, 155–156Basalioma, forehead, 368Basel approach, to cleft lip and palate,
544–546Bicoronal suture release, in initial
treatment for Crouzon syndrome,717
Bicortical grafts, for mandibularreconstruction, 300
Bilateral complete cleft lip and palate(UCLP), deformities in, 557
Bilateral sagittal split ramus osteotomy(BSSRO), 527, 639–645
Bimaxillary retrusion, aesthetic repair in,284
Binder syndrome (maxillonasal dysplasia),51–52, 520, 660
Biocompatibilityof grafts, and success of incorporation,
127of polymers for bone fixation, 114–115
Biodegradable materials, for bone fixation,113
Biomechanical considerationsfor mandibular fixed reconstructions,
239–240in single tooth replacement, 253
Bioresorbable materials, for bone fixation,113–123
Birth process, nasal injuries during, 54Bite, recording, in planning for
orthognathic surgery, 514–518Block grafts, experimental comparison
with particulate grafts, 128Blood transfusion, autologous, in elective
surgery, 591Bolton standard heads and faces, 514–518Bone
benign tumors of the maxillofacialregion, 59–64
fixation of, bioresorbable materials for,113–123
fragments of, rotation and interpositionof, 631
principles of healing, 101quality and strength of, in fixation, 104quality and volume of, for dental
implant restoration, 233resection of tumors and reconstruction,
condyle and ascending ramus, 470substitutes for, in mandibular
reconstruction, 336trimming of, and maxillary positioning,
597–600See also specific entries, e.g. Frontal bone
Bone-anchored hearing aid (BAHA), 132Bone grafts
for alveolar cleft defect, 542–554calvarial, harvesting techniques,
700–712fixation of, for mandibular continuity
defects, 317–326free autogenous, in maxillofacial
reconstruction, 295–300iliac, factors affecting success of
mandibular continuity defectreconstruction, 339–341
to improve stability of maxillaryosteotomies, clinical studies, 587
for nasal reconstruction, 483–488pedicled, in maxillofacial reconstruction,
300–308secondary, 554–555See also Autogenous bone grafts;
Autologous bone grafts; Cancellousbone grafts; Corticocancellous bonegrafts; Endochondral bone grafts;Iliac entries
Bone morphogenic protein (BMP), 180Boo-Chai classification, of facial clefts, 23Brachycephaly
in Apert syndrome, 675–677in Crouzon syndrome, 675–677, 713
simple, versus Crouzon syndrome,715–717
Braincoverage of, with musculocutaneous
flaps, 364limitation on growth, in
craniosynostosis, 673Breathing, difficulty in, Crouzon
syndrome, 713Bridging osteosynthesis, 321
for mandibular continuity defects, 327Buccolingual atrophy, 204
computerized tomography imaging of,206–207
CCaldwell “C” osteotomy, 610Callostasis, 648–650Calvaria
bone flaps from, for reconstruction inmaxillary midface defects, 356–359
defects in, from traumatic injury, 708,710
graft harvestingmorbidity in, 668techniques, 700–712
Cancellous bone grafts, 125–126, 130harvesting blocks from the iliac crest,
299–300healing of, maxillary sinus grafting, 180
Cancer. See MalignanciesCarpenter syndrome, 29–30
facial features in, 36Case example
abutments and overdentures, 146–153cleft lip and alveolus, unilateral
complete, 548–550cleft lip and palate
bilateral complete, 548, 551, 554,557–559
unilateral, 547unilateral complete, 551–553
cleft palate, in one of identical twins,557, 560
cranial-based defect reconstruction, withcalvarial bone grafts, 711–712
distraction osteogenesis, 649–650early relapse, after mandibular sagittal
split ramus osteotomy, 643–644genial deficiency, 652–653genioplasty, 653infection followed by anterior frontal
bone collapse, 711infraorbital rim defect, 705–706intraoral vertical ramus osteotomy,
646–647the Le Fort I maxillary osteotomy
for apertognathia and mandibularexcess, 655–657
midface, 657–658
770 Index
long-term relapse, mandibular sagittalsplit ramus osteotomy, 644–645
mandibular midline split, study of rigidfixation versus wire osteosynthesis,648
maxillary advancement and downwardmovement, in cleft lip and palate,unilateral, 567, 572–573
maxillary and chin advancement, in cleftlip and palate, unilateral, 567,570–571
maxillary buttress defect, 705, 707–708maxillary hypoplasia, in cleft lip and
palate, bilateral complete, 562, 565
naso-maxillary hypoplasia, in cleft lipand palate, unilateral complete,574–576
orbital floor defects, 704–705orbital reconstruction, 480–482osteotomy, in cleft lip and palate,
bilateral complete, 567–569overdentures, 262–265premaxilla repositioning, cleft lip and
palate, bilateral complete, 562–564radiologic follow-up of bone grafts,
220–231ridge augmentation, 159–162of subapical osteotomy, 651THORP-plate reconstruction of bilateral
maxillary defects, 439–444zygomatic arch defect, 708–709
Casts, mastertransfer copings for fabrication of dental,
238–239verification of fit, 239
Cephalometrics, 285, 514Cervical spine
deformities of, in Apert syndrome,750–751
osteomyelitis of, 85–86Cheeks, assessing deformity of, 14–15Chemical reactions, of metals in solution,
109–110Chemicals, association with craniofacial
malformation, 671Children
craniomaxillofacial implants in, 134–135effects on growth capacity of harvesting
vascularized bone grafts, 361Children’s Medical Center, Dallas, orbital
rim advancement at, 673Chin, as a donor site for bone grafts,
295–296. See also GenioplastyChin-neck contour, assessment of, in
craniomaxillofacial deformity,18–19
Chromosome disorders, nasalmanifestations of, 50. See alsoHereditary conditions
Classificationof bone quality and quantity, Lekholm
and Zarb, 234of cleft lip and palate deformities,
539–540of craniofacial deformities, 22of craniomaxillofacial deformities,
90–97nasal, 49–58traumatic, 43–46
of craniosynostosis, 673–678syndromes, 35–36
of facial clefts, 23of genioplasties, 627of hemifacial microsomia, 683–684,
730–733of nasal encephaloceles, 53
Cleft lip and palate, 22–29cancellous bone grafting for, 356nasal deformity in, 50–51reconstruction of osseous defects in,
539–580segmental osteotomy in, 587
Cleft palate (CP)association with Apert syndrome, 679case example, 557narrowing the mandible for, 648treatment planning for, 526
Clefts, all-in-one surgery to close, 545–546Clinical characteristics
of hemifacial microsomia, 682–683,728–730
of Treacher Collins syndrome, 685Clinical examination
findingsin acute osteomyelitis, 80–81in osteomyelitis of the frontal bone,
85history of craniomaxillofacial deformity,
6–7before orthognathic surgery, 497–512
Clinical implications, of metal implants,111
Clinical studiesof biodegradable materials in fracture
surgery, 116–117of osteotomy segments, with and
without bone grafts, 587of radiation, effects of reconstruction
plates, 422–429See also Research
Clivus chordomas, resection of, withtransfacial access osteotomies,489–496
Cocaine, nasal deformities from abuse of,57
Cohen classification, of craniosynostosissyndromes, 35–36
Collateral circulation, labiobuccal andpalatal vascular, 581, 585
Complicationsof bone graft harvesting, 703of dental implant restoration, 253–257of free-tissue transfer, 393of genioplasty, 631–638of iliac corticocancellous grafts, 339of irradiation, effects on soft tissue, 427of Le Fort I osteotomy, necrosis of the
maxilla, 83of Le Fort III osteotomy
in Crouzon syndrome, 723–724midface reconstruction, 667–668
of mandibular condylar prostheses,379–387
with mandibular condylar prosthesis,377–388
of maxillary osteotomies, 587, 590–591of maxillary sinus grafting, 189–195of orthognathic surgery, 519–520of reconstruction
with cancellous bone and marrow intitanium trays, 299–300
in irradiated fields, 290of mandibular continuity defects,
317–319of rigid internal fixation, 618–619of temporomandibular joint surgery, 346
Compression, toleration by dental implants,233–234
Computed tomography (CT)in craniomaxillofacial bone infections,
78for craniomaxillofacial dental
implantology, 198–209for evaluating craniofacial deformities,
672in infantile osteomyelitis, 83of the maxillary sinus, 176in oral malignancies, 69
three-dimensional reconstruction,oromandibular complex, 291
for quantitative assessment of the cranio-orbito-zygomatic skeleton, 714
reformatting into cross-sectional views,for dental implant restoration, 232
three-dimensional reconstructions from,for planning surgical procedures, 462
for visualization of the bony orbit, 478Computer packages, for planning
orthognathic surgery, 561Condylar heads, remodeling and resorption
of, 618Condyle
abnormality of, in hemifacialmicrosomia, 729
benign tumor of, image aftertemporomaxillary jointalloarthroplasty, 380
microvascular reconstruction of,462–477
Index 771
Condyle (Continued)resorption of, and late relapse after
osteotomy, 639, 643setting the position of, in bimaxillary
surgery, 527Congenital deformity
craniomaxillofacial, 5dysplasia as an indication for
costochondral grafting, 354facial clefting, 22–29nasal, 49–54See also Hereditary conditions
Connective tissue, around dental implants,plasma-sprayed titanium, 142–143
Contraindicationsto autogenous transplants, 377to fibula donation, smoking as, 414
Coronal synostosis, unilateral, 675Corrosion, of metal in internal fixation,
107Cortical bone
for grafts and implants, clinicaloutcomes, 130
healing of grafts of, 126maxillary sinus grafting, 180
skull donor sites for grafting of, 300Corticocancellous bone grafts, 130–131
autologous intramembranous, to maxilla,131–132
free, for the maxilla, 356–371hip inner surface as a donor site for, 300for mandibular continuity defects, 321for the maxillary sinus, 180–181
Cosmetic failure, in genioplasty, 634–638Costochondral arthroplasty, polymer
screws for fixation of, 121Costochondral grafts
advantage of, response to growth, 353for condylar reconstruction,
disadvantages of, 462free, mandibular condyle reconstruction
with, 343–355in hemifacial microsomia, 733–735
Cranial basecalvarial bone grafts for reconstruction
of, 711–712microsurgical reconstruction of large
defects of, 356–371Cranial bones
deformities of, classification, 95as donor sites
in cranio-orbito-zygomatic procedures,715
in midface reconstruction, 662Cranial circumference, for evaluating
craniomaxillofacial deformity, 9–10Cranial deformities
clefts, 25in hemifacial microsomia, 728
Cranial modular fixation system, 456–458
Cranial suturesexamination of, 10premature closure of, classification of
anomalies from, 29Cranial vault, in Crouzon syndrome
osteotomy, 722–723reshaping of, 718–719
Craniocervical junction, exposure of, 494Craniofacial deformities, 22–37
clefts, 25dysostosis, 678–681
in Crouzon syndrome, 713principles of management of, 671–692surgical correction of, in Apert
syndrome, 749–755Craniofacial fixation system
effects on the growing craniofacialskeleton, 693–699
hardware review, 445–461Craniofacial Modular Fixation System,
445–450Craniofacial osteotomy instrumentation
sets, 629Craniofacial reconstruction, vascularized
bone grafts for, 313Craniofacial Repair System (CRS),
459–461Craniofacial synostoses, inherited, 52Craniomaxillofacial bone
healing ofbiomechanics and rigid internal
fixation, 101–106after surgery, 124–137
infections of, 76–89radiographic diagnosis, 78
metal for internal fixation, 107–112radiographic evaluation of, 210–219
Craniomaxillofacial deformityclassification system for, 90–97evaluation of, 5–21nasal, 49–58traumatic, 43–48
Craniomaxillofacial dental implantology,198–209
Craniomaxillofacial surgery, 1reconstructive
versus corrective, 41–42current practice and trends in, 310–316
Cranio-orbital decompression, in Crouzonsyndrome, 715–717
Cranio-orbito-zygomatic procedures,cranial bones as donor sites in, 715
Craniostenosis, surgical correction of thebony forehead in, 8
Craniosynostosis, 673–678classification of, 29–37in Crouzon syndrome, 713
Craniotomy bone flap, 703Cranium, donor site, for nasal
reconstruction, 483, 486–488
Creeping substitutiondefined, 125fixation required for, 327in maxillary sinus grafting, 180in ridge augmentation, 157
Cross sectional images, computer-generated, 200–201
Crouzon syndrome, 29, 32, 35, 664, 673,678–679
basic dysmorphology and staging ofreconstruction, 713–726
bilateral coronal synostosis in, 675Cupar technique, 601
for anterior maxillary osteotomydownfracture, 591
Cuspid area, in maxillary implantpositioning, 243
DDegenhardt classification, of craniofacial
deformity, 23Delaire analysis, in planning orthognathic
surgery, 514Demineralized freeze-dried bone (DFDB),
bone morphogenic protein in,181–182
Dental compensations, in hemifacialmicrosomia, 729
Dental examination, before orthognathicsurgery, 512
Dental implantsgrafts from the fibula for insertion of,
327ITI system, 138–154
Dentascan program, examples of imagesgenerated by, 198, 201–208
Dermoids, nasal, 54Developmental deformity,
craniomaxillofacial, 5. See alsoEmbryology
Dexamethasone, postoperativeadministration of, in transfacialaccess osteotomy, 496
Diagnosisdifferential, of hemifacial microsomia,
727of oral squamous cell carcinoma, 67–68of orbital hypertelorism, 738of osteomyelitis of the cervical spine, 86
Disadvantagesof genioplasty, 652of intraoral vertical ramus osteotomy,
646of mandibular midline split, 648of midface osteotomy, 657of rigid fixation
in mandibular sagittal split ramusosteotomy, 643
in maxillary surgery, 654of subapical osteotomy, 651
772 Index

Diseasematernal, and nasal deformities, 50systemic, and nasal deformities, 57See also Infection
Displacement, osseous, in osteotomy, 639
Distraction osteogenesis, 648–650Donor sites
for alveolar grafts, 544calvarial, reconstruction with alloplastic
materials, 702for mandibular reconstruction, 310–313for midface reconstruction, 662
morbidity at, 668for nasal reconstruction, 483
parietal bone, 742Dosimetry, on an irradiation phantom,
420–421Double barrel graft, fibular, for arched
mandibular defects, 329–333Downfracture, risks of, 567Drugs, association with craniofacial
malformation, 671Dura, coverage of, with musculocutaneous
flaps, 364Dysmorphology
in cleft lip and palate, 540–542defined, 672
Dysostosis, craniofacial, in Crouzonsyndrome, 713. See alsoMandibulofacial dysostosis
EEconomic considerations
in internal fixation, 2in primary reconstruction, in gunshot
wounds, 416in rigid internal fixation, for bimaxillary
surgery, 522Ectodermal cysts, nasal dermoid, 54Edentulous restorations, dental implant,
236–237partial, 245–250
Embryologyof the calvarium, 700–701of the craniofacial region, 671of nasal deformities, 49–50of the palate, lip and alveolus, 539–542
Emergence Profile System, for single toothabutments, 252
Encephaloceles, nasal, 53Endochondral bone grafts
for maxillary sinus grafting, 180–181preformed, clinical use of, 130–131
Endocrine disorders, deformities causedby, 5
Endosseous implantsand bone grafting, 124–132selection of, 184–185
Eosinophilic granuloma, treatment for, 63
Epidemiologyof craniomaxillofacial fractures and
defects, 5of hemifacial microsomia, 727of oral squamous cell carcinoma, 65
Epiphyseal dysplasia, in Apert syndrome,750
Epithelium, around dental implants,plasma-sprayed titanium, 142–143
Ethanol, nasal deformities due to in uteroexposure to, 50
Etiologyof cleft lip and palate, 539of craniofacial deformities, congenital,
671–672of craniomaxillofacial deformities
in Apert syndrome, 749–750nasal, 49–58
of hemifacial microsomia, 727–728of oral malignancies, 65of osteomyelitis, 76–77
of the frontal bone, 84of skeletal malocclusion, 38–42of suppurative osteomyelitis of the
mandible, 80See also Pathogenesis
Etiopathology, of orbital hypertelorism,739–740
Evaluationof Apert syndrome patients, 750–751of craniomaxillofacial deformity
patients, 5–21before reconstructive surgery, 390of tumor extension, in oral malignancies,
68–69Examination cycle, before orthognathic
surgery, 500Exophthalmus, association with
hyperthyroidism, 5Exorbitism
in Apert syndrome, 35, 750in bilateral coronal synostosis, 675in malar deficiency, 15
Expectations, patient’s, in dental implantrestoration, 256–257
Explosions, craniomaxillofacial injuriesfrom, 47
Extender System, ITI, 164Extracranial procedures, in orbital
hypertelorism management, 744Eye, evaluating, 11–12. See also VisionEyebrows, position of, evaluating, 12–13Eyelids
deformities of, in Apert syndrome, 752
evaluating, 13
FFacial anatomy
analysis of, for genioplasty, 623–624
clinical evaluation of, in cleft lip andpalate, 551
growth of, in hemifacial microsomia,729–730
planning height, in bimaxillary surgery,526–527
proportions, for clinical examination,506–507
width, describing in a clinicalexamination, 508–509
Facial angles, for evaluation ofcraniomaxillofacial deformity, 7–8
Facial appearanceclinical evaluation of, in cleft lip and
palate, 556concepts of harmony in, 280–284
Facial bipartition, in orbital hypertelorismmanagement, 742–745
Facial clefting, 22–29embryological origin of, 671rare, 52–53
Facial contour angle (FCA), for evaluation ofcraniomaxillofacial relationships, 8
Facio-auriculo-vertebral (FAV)malformation complex, 727
Faciolingual orientation, in single toothrestorations, 250
Farm injuries, craniomaxillofacial, 47–48Fetal compression, nasal injuries from, 54Fibroma, ossifying, reconstruction after
removal, in a child, 368–369Fibrous dysplasia, treatment for, 63Fibula
and combined flaps, for maxillofacialreconstruction, 306–308
dissection of, 391as a donor site
advantages of, 414for ascending ramus and condyle
grafts, 466for mandibular continuity defects, 321for mandibular reconstruction, 310,
312–313, 471–474, 475–476indications and technical
considerations for use of, 327–334Fibular flap, for mandibular reconstruction,
389–390Finnish Cancer Registry, standardized
incidence ratio for oral cancer, 65–66Fixation methods
in bimaxillary surgery, 532–533biodegradable polymer screws for, in
sagittal osteotomy, 119, 121during bone healing, 101–106, 336–337in the craniofacial system, hardware
review, 445–461in genioplasty, 628–633in nasal reconstruction, 483–484in orbital hypertelorism reconstruction, 744See also Plates; Screws
Index 773

Fixture insertioncomputerized tomography images for
reviewing placement, 205surgical technique, maxillary sinus
grafting, 187Flap contouring, for maxillofacial
reconstruction, 303–304Follow-up
after oral cancer treatment, 72–73after temporomandibular joint surgery,
350–351See also Outcomes
Fontanellesin craniomaxillofacial deformity, Apert
syndrome, 749description of, 671evaluating, in craniomaxillofacial
deformity, 10Forehead
advancement of, in Apert syndrome, 751
landmarks of, 10–11Foreign body reactions, to self-reinforcing
polylactide copolymer, 115Fractures
fixation of, self-reinforced polymers for,120–121
posttraumatic osteomyelitis at the site of,433
spontaneous, of an irradiated edentulousmandible, 229–230
Franceschetti-Zwahlen-Klein syndrome,Tessier classification of, 28
Frankfort horizontal plane (FH), forevaluation of craniomaxillofacialdeformity, 7
Free-tissue transfer, in mandibularreconstruction, 338
Frontal boneanterior, calvarial bone graft
reconstruction, 711deformities of, classification, 95osteomyelitis of, 84–85
Frontal view, for evaluatingcraniomaxillofacial deformity, 9
Frontonasal dysplasia, 52Full-thickness outer cortex calvarial bone
graft, 702Functional considerations
in Crouzon syndrome, 713problems associated with
craniosynostosis, 673
GGallium-67 scans
in craniomaxillofacial bone infection, 79in osteomyelitis of the frontal bone, 85
Garre sclerosing osteomyelitis, 82Genetic counseling
in craniofacial deformity, 672
for orthognathic surgery candidates,497–500
Genetic diagnosis, in craniofacialdeformities, 672
Genetic predisposition, in primarycraniosynostosis, 29
Genial deficiency, aesthetic repair of, 282Genioplasty, 574, 651–653
combination with ramus osteotomy, 648considerations for rigid internal fixation,
623–638mandibular horizontal osteotomy for,
611passive, 624–626sliding, 612
rigid fixation in, 617Giant cell granulomas, 62Gingival tissues, evidence of implant
failure in, 253–254Glenoid reconstruction, in hemifacial
microsomia, 734Gliomas, nasal, 53Globe, position of, and craniomaxillofacial
deformity, 13Gnathion (Gn), for evaluation of
craniomaxillofacial deformity, 7Gold
for dental restoration substructures, 239for octa-abutment screw-retained dental
restorations, 145–147Goldenhar syndrome, 463, 727
macrostomia in, 730vertebral defects in, 728
Gonzalez-Ulloa line, for evaluatingcraniomaxillofacial deformity, 9
Graftscantilevered bone, for orbital
reconstruction, 480corticocancellous block, harvesting for
ridge augmentation, 157factors affecting success of, 127fixation of, in mandibular continuity
defect reconstruction, 319–320materials for maxillary sinus grafting,
179metatarsal, for mandibular
reconstruction, 474for nasal reconstruction, 483–488reconstructive, 124–132resorption as a measure of failure in,
216tertiary, in cleft lip and palate, 556See also Bone grafts
Grisel syndrome, 86Growth
disturbances ofassociation with cleft lip and palate,
541–542association with midface
reconstruction, 668
effects of plate and screw fixation on thecraniofacial skeleton, 693–699
excessive, after reconstruction of themandible, 464
facialeffect of cleft lip and palate surgery,
500in hemifacial microsomia, 729–730
of nonvascularized grafts, 462restricted, after osteotomy and fixation,
696–699Guided bone regeneration (GBR), 155–163
biodegradable membranes used in,118–120
case report, 161chin, after harvesting bone, 296
Guided tissue regeneration (GTR), 127Gunshot wounds, 43–46
HHandgun injuries, 47Haptens, metals as, 110Hardware
for internal fixation, 599–601in intraoral vertical ramus osteotomy,
646in mandibular sagittal split ramus
osteotomy, 640–642in ramus osteotomy, 648in subapical osteotomy, 651
for Le Fort I maxillary osteotomy, 654midface, 657
for stabilizing genioplasty, 652Harkens classification, of cleft lip and
palate, 23Harvesting, of calvarial bone grafts,
701–703Healing
duration of, in ridge augmentation,157–158
in maxillary sinus grafting, 179–181of posttraumatic osteomyelitis, by
secondary intention, 433process of, 125of reconstruction, after radiation therapy,
335soft-tissue, in the presence of a
membrane, 156after surgery, craniomaxillofacial,
124–137Hearing disorders
in cleft infants, 541in Crouzon syndrome, 713external hearing aids for, skin-
penetrating implants, 132–133Helsinki University Central Hospital,
Department of Oral andMaxillofacial Surgery, 377
Hematomas, nasal, deformity fromuntreated, 55
774 Index

Hemifacial microsomia (HFM), 681–685,727–737
presurgery and postsurgery views,686–687
Hemimandibulectomyfor osteogenic sarcoma, 469reconstruction following, 471reconstruction with alloplast, 385
Hemorrhagein craniofacial surgery, 667–668in maxillary sinus grafting, 194
Hemostasis, in maxillary surgery, 528Hereditary conditions
autosomal dominantApert syndrome, 679Crouzon syndrome, 678–679hemifacial microsomia, 727–728
nasal deformity in, 50–52See also Congenital deformity
Heterotopic bone, formation of, intemporomandibular jointarthroplasty, 381
Histology, clinical, of implants in bonegrafts, 128–130
Historyof the Le Fort I osteotomy, 581of mandibular osteotomies, 606–609Mesopotamian, of craniofacial cleft, 27observation of osteomyelitis, 76Roman, of osteomyelitis of the frontal
bone, 84of segmental maxillary osteotomy, 587of a surgical approach to
craniosynostosis, 715History, patient’s, assessment of
craniomaxillofacial deformity, 6Holoprosencephaly, facial anomalies in, 52Human experimentation, on the stability of
maxillofacial implants, 135Hunsuck effect, avoiding, 615–616Hydantoin, nasal deformities due to in
utero exposure to, 50Hydrocephalus
association with Crouzon syndrome, 713
in Kleeblatschumldel deformity, 36Hydroxyapatite (HA), synthetic, 182–184Hyperbaric oxygen treatment (HBO), effect
of, on implant success, 133–134Hypertelorbitism, in cleft lip and palate,
bilateral complete, 567–569Hypertelorism, in clefts, 28–29
IIatrogenic injuries, nasal deformities from,
57Iliac bone grafts
morbidity in harvesting, 668onlay grafts, outcomes, 131radiologic follow-up, 222
with soft tissue flaps, for maxillofacialreconstruction, 301–303
Iliac corticocancellous graftscomplications of, 339immediate versus delayed placement,
study, 131Iliac crest, donor site
for ascending ramus and condyle grafts,465–467
for free bone grafts, 298–300for mandibular continuity defect repair,
321for mandibular reconstruction, 310–311,
389–390, 414for nasal reconstruction, 483
Ilizarov method, for distractionosteogenesis, 648–650
Imagingmethods for evaluation of the
craniomaxillofacial region, 210–212in osteomyelitis of the frontal bone,
85in suppurative osteomyelitis, 81
Immunocompetence, and osteomyelitisincidence, 76–77
Implantsconnecting to natural teeth, 247–248defined, 124–125dental
failure of, 253–254full-body-screw (S), 138, 164hollow-cylinder, 139–140hollow-screw, 138–139
fracture of, 254metal, mechanical properties of,
110–111module selections, 451–456osseointegrated, in cleft lip and palate,
548, 551Incidence
of clefting, by geographic location andracial group, 539
of cleft lip and palate, 22of nasal fractures, 55of oral squamous cell carcinoma, 65
Incisor display, noting in a clinicalexamination, 509–510
Indicationsfor bilateral sagittal split ramus
osteotomy, 639–640for bimaxillary surgery, 522–523for calvarial bone grafts, 704–711for condyle replacement, 372for fibula grafts, 327–334for free bone grafts, 295for genioplasty, 624–627, 651for hemifacial microsomia treatment,
733–734for intraoral vertical ramus osteotomy,
645–647
for Le Fort I maxillary osteotomy, 656for Le Fort II osteotomy, 660for Le Fort III osteotomy, midface
reconstruction, 664for microvascular bone flaps, 301for onlay grafting, 177–178for orthognathic surgery, 557, 561for subapical osteotomy, 650for temporomandibular joint restoration,
343Indium scan, white blood cell, in
craniomaxillofacial bone infection,79
Infantile osteomyelitis, 83Infection
in craniofacial surgery, 667–668of craniomaxillofacial bone, location of,
79frontal bone collapse after, calvarial
bone graft reconstruction, 711in genioplasty, 634maternal, craniofacial deformities
associated with, 671in maxillary sinus grafting, 194opportunistic, nasoseptal manifestations
of, 57postoperative, demonstration on
computerized tomography image,204
Inferior vermilion border (Vi), forevaluation of craniomaxillofacialdeformity, 7
Infraorbital rim defect, calvarial bone graftfor reconstruction of, 705–706
Inner cortex calvarial bone graft, 703Instrumentation sets, craniofacial
osteotomy, 629Instruments, craniofacial modular fixation
system, 450–451Intermaxillary fixation, placement with
powerchain, 566Internal fixation
considerations in radiation therapy,419–432
functionally stable, 1Le Fort II osteotomy, 662–663Le Fort III osteotomy, midface
reconstruction, 666–667technique for, 599–601, 603See also Rigid internal fixation
Interocclusal splintpreparing from models, 523–525transitional, 525–526
Intracranial pressurein Apert syndrome, before or after
forehead advancement, 750and hypertension, association with
craniosynostosis, 673, 713monitoring of, in young children with
Crouzon syndrome, 718
Index 775
Intracranial procedures, for orbitalhypertelorism management,740–744
Intracranial volume, in Apert syndrome, 749Intramembranous grafts and implants,
131–132Intraoperative radiation therapy (IORT),
advantages of, 427–429Intraoral technique, for stabilization in
mandibular sagittal split ramusosteotomy, 642
Intraoral tissue, restoration of, after cancersurgery of the head and neck, 290
Intraoral vertical ramus osteotomy (IVRO),606–607, 614–615
indications for, 645–647In utero exposure, nasal deformities due to,
50Irradiated bone, osteogenetic potential of,
444ITI Strauman Dental Implant System,
765–767
JJaw
deformity in Crouzon syndrome,management of, 724
dysfunction of, psychological aspects in,634
lower, reconstructive surgery of,radiographic assessment, 213–218
upper, imaging sequence andinterpretation, 212
KKeratocysts, recurrence of, 59–61, 350–351Key area, in repair of the orbit, 478–479Kirschner wires, for craniomaxillofacial
bone healing, 102Kleeblatschumldel deformity, 29, 35–37Kufner osteotomies, posterior maxillary, 588
segmental, 602–603
LLacrimal apparatus, damage to, in Le Forte
III osteotomy, 668Lag screw technique
advantages of, in craniofacial surgery, 715in mandibular osteotomy, 615–616
sagittal split ramus, 609, 641in nasal reconstruction, 484–488
Lambdoid synostosis, unilateral, 676–678Lateral arm free flap, for mandibular
reconstruction, 338–339Latissimus-dorsi musculocutaneous flaps,
361, 370–371Le Fort I maxillary osteotomy
advantages of, 523in cleft lip and palate, 562
bilateral complete, 565–566
examples of fracture patterns, 582history of, 581maxillary, 653–656
necrosis as a complication of, 83multiple segment, planning for, 526surgical technique, 591–601types of, 583–584
Le Fort II osteotomyin midface reconstruction, and
considerations for internal fixation,660–668
in nasomaxillary hypoplasia, 574Le Fort III osteotomy
in Crouzon syndrome, history of, 715malar maxillary, 574for midface reconstruction
considerations for internal fixation,660–668
in Crouzon syndrome, 678–679,719–721, 723–724
Limberg oblique osteotomy, 610Lips, clinical assessment of, in
craniomaxillofacial deformity, 17–18Loading, of grafts
maxillary sinus, 175progressive, 189and success of incorporation, 127
Lower facial plane (LFP), for evaluation ofcraniomaxillofacial relationships, 8
Lund classification, of craniofacialdeformity, 23
Lymphomas, of extranodal origin, 70
MMagnetic resonance imaging
in craniomaxillofacial bone infections,78
in oral malignancies, 69Malar bone
absence of, in Franceschetti-Zwalen-Klein syndrome, 28
aesthetic repair of deficiency of, 282–283evaluating, in craniomaxillofacial
deformity, 15Malar prominence, defining, in a clinical
examination, 509Malignancies
carcinoma of the tongue, 400condylar reconstruction in, 381head and neck cancer, reconstruction in,
289–294oral, 65–75
mandible resection in, 317recurrence rates, after marginal
mandibulectomy, 411See also Tumors
Malocclusionin Crouzon syndrome, management of,
724after Le Forte III osteotomy, 668
Mandibleanteroposterior deficiency of, in cleft lip
and palate, 557–559atypical ossifying fibroma in, panoramic
image, 225–226biomechanical considerations in
reconstruction of, 239–240classification of deformities of, 91–92comminuted fracture of, 165continuity defects of
decisions about reconstruction of, 335fixation of bone grafts in
reconstruction, 317–326distraction osteogenesis of, 757–764edentulous, 237–243
with overdenture bar, 263fixation of
with experimental polymers, 116with polyglycolide materials, 117
hardware review, 269–279implants in, study, 131internal fixation of, 1, 533with maxillary fixed bridge, 263–264midline split of, 647–650multiple fractures of, aesthetic repair, 281ossifying fibroma in, computerized
tomography image, 227–228osteomyelitis of, 80–82posttraumatic osteomyelitis of, 433–438reconstruction of, with vascularized bone
grafts, 310–313resection due to carcinoma, and
restoration, 166–167resorption of, in edentulous patients, 236
Mandible Distractor Module Set, 269,278–279
Mandible reconstruction module, 273Mandible trauma module, 271–273Mandibular alveolar osteotomy, total, 606,
650–651Mandibular alveolar ridge, atrophy of,
168–169Mandibular angle
deficiency in, aesthetic repair of, 282reconstruction of defects of, 389–394
Mandibular body reconstruction, 395–410Mandibular condylar reconstruction
with free costochondral grafting,343–355
problems with prostheses, 377–388Mandibular continuity, reconstruction of,
with an angular THORP plate,404–405
Mandibular osteotomy, 104–105, 529anterior midline, 611–613
rigid fixation in, 617with rigid internal fixation, 606–622,
639–659Mandibular prognathism, 5
in cleft patients, 574
776 Index

intraoral vertical ramus osteotomy fortreatment of, 606
Mandibular reconstruction plate, exposureof, and infection, 444
Mandibular resection, in oral cancer, 70–72Mandibular sagittal split ramus osteotomy,
612–614Mandibular segmental subapical osteotomy
anterior, 606, 608–611rigid internal fixation and acrylic splint
in, 617Mandibular-temporomandibular joint
complex, in hemifacial microsomia,729
Mandibulectomy, marginal, 411–413Mandibulofacial dysostosis
familial, ear deformities in, 16Tessier classification of, 28in Treacher Collins syndrome, 685
Mandibulotomy, stable fixation of, 494Maternal idiosyncrasies, as potential causes
of malformation, 671Maxilla
atrophied, augmentation of, 131bilateral defects of, 439–444deformities of, 92–93edentulous, 243–245implants in, study, 131internal fixation of, 532–533microsurgical reconstruction of large
defects of, 356–371osteomyelitis of, 82–83sarcoma of, 366–367
Maxillary alveolar hyperplasia, history oftreatment for, 581
Maxillary and chin advancement, afterrepair of a cleft lip and palate,unilateral complete, 567, 570–571
Maxillary buttress defect, calvarial bonegraft reconstruction in, 705,707–708
Maxillary hyperplasia, posterior,management of, 598–599
Maxillary hypoplasia, in a cleft patient,556–557
outcome of surgery for, 498Maxillary/midface defects, reconstruction
of, 356–359Maxillary osteotomies, 581–605
in cleft lip and palate, 551–577stability of, with rigid internal fixation,
639–659Maxillary segmental osteotomies
anterior, 601posterior, 602–603
Maxillary sinuscomputerized tomography imaging of
pathology of, 206, 208grafting and osseointegration surgery,
174–197
Maxillofacial bonesITI dental implant system for, 164–173tumors of, and bone invasion, 59–64
Maxillofacial surgery, 1advantages of rigid internal fixation in,
581Maxillomandibular fixation (MMF)
for autogenous transplants, 377history of, 606in orthognathic surgery, radiologic
record keeping for, 513for vertical ramus osteotomy, 615
Maximal Interincisal Opening (MIO),reduction in, and fixation method,618
Mechanical considerations, in fixation, 104Medication, maternal exposure to, and
nasal deformities, 50Melanoma, of the oral cavity, 70Membrane reflections, surgical technique,
maxillary sinus grafting, 186–187Meningiomas, sphenoid wing, transfacial
access osteotomies for resection of,489–496
Mental protuberance, defined, 623Mentocervical angle (MCA), in evaluation
of craniomaxillofacial relationships,8
Mentolabial sulcus (MLS), in evaluation ofcraniomaxillofacial deformity, 7
Menton (M), soft tissue, for evaluation ofcraniomaxillofacial deformity, 7
Mesh module, cranioplast, 456–458Mesh plate, for orbital reconstruction, 480Mesiodistal orientation, in single tooth
restorations, 250Metal, for craniomaxillofacial internal
fixation, 107–112Metastatic tumors, of the oral cavity, 70Metopic synostosis, 675–678Microbiology
of osteomyelitis of the frontal bone, 85of suppurative osteomyelitis of the
mandible, 80Microplate fixation, resorbable, in surgery
for metopic suture release, 675Microsomia, hemifacial, 22, 40
reconstruction in, 362–363Microsurgery, for reconstruction of large
defects, 356–371Microtia
craniomaxillofacial microsomiaassociated with, 16
prosthesis for, 133Microvascular bone surgery
composite flaps, for maxillofacialreconstruction, 301
current practice and trends in correctivesurgery, 310–316
for reconstruction of defects of the
mandibular angle, 389for reconstruction of the condyle and
ascending ramus, 462–477Microvascular free flaps, for head and
neck reconstruction, 289–290Microvascular module, 273Microvascular tissue transfer, in
reconstruction of anterior defects ofthe mandible, 414
Midfacedefects of, in hemifacial microsomia,
729Le Fort I osteotomy for deformity of,
656–657history, 581
management of deformity of, inchildhood, 719
microsurgical reconstruction of largedefects of, 356–371
multiple fractures of, aesthetic repair, 281reconstruction of
after cancer surgery, 291–292Le Fort II and III osteotomies,
660–668Miniplate fixation systems, 445
anterior mandibular segmental andgenioplasty osteotomies, 611–613
craniofacial system, 599–600in mandibular osteotomies, 617
sagittal split ramus, 642–643modules, United States and worldwide,
445titanium, in orbital hypertelorism
reconstruction, 744Models
dental, for planning bimaxillary surgery,523
for planning orthognathic surgery, 561three-dimensional, fabrication from
computerized tomography data, 463Modules
cranial bone flap fixation, 1.0–1.5 mm,457–458
craniofacial modular fixation system,1.0–20 mm, 445–448
Monobloc osteotomiesin Apert syndrome, 751–752
avoiding, 752–753in Crouzon syndrome, 722–723
Morbidityversus benefit from bimaxillary surgery,
523disability from radical excision of oral
cancer, 70–73long-term, in mandibular continuity
defect repair, 327in repeat craniotomy for Crouzon
syndrome, 718–719Morian classification, of craniofacial
deformity, 22–23
Index 777
Mucosal coverage, utilization forreconstruction incraniomaxillofacial deformity,classification, 90
Multidisciplinary team conceptfor managing craniofacial deformities,
672, 733for managing hemifacial microsomia,
727Myocutaneous flap, pectoralis major, 289,
412–413for bilateral maxillary defect repair,
442–444
NNasal aperture, donor site for free bone
grafts, 296Nasal dermoids, 54Nasal dorsum hematomas, 55Nasal encephalocele, description of, 53Nasal gliomas, 54Nasal structure
cavity, nonseparation from the oralcavity, 540
classification of deformities, 94description of bone, 483restoring with bone grafts and rigid
internal fixation, 483–488septum, managing in transfacial access
osteotomy, 495Nasoendotracheal tube, placing and
securing in maxillary surgery, 528Nasofacial angle, measuring, 14Nasofrontal angle (NFA), for evaluation of
craniomaxillofacial relationships, 7Nasomaxillary region, reconstruction of,
after cancer surgery, 292Naso-orbital-ethmoid deformities, 94Necrosis, aseptic, following maxillary
osteotomy, 590Nerve damage
in genioplasty, 634in Le Forte III osteotomy, 668in rigid internal fixation using bicortical
screws, 615Nerve tissue availability, in
craniomaxillofacial deformity,classification, 90
Neural crest cells, role in craniofacialdevelopment, 38. See alsoEmbryology
Neuralgia-inducing cavitationalosteonecrosis (NICO), 82
Neurologic manifestations, in hemifacialmicrosomia, 728
Neuropsychiatric disorders, associationwith craniosynostosis, 673
Neurosensory disturbances, as acomplication of rigid internalfixation, 619
Nickel, in tissue, toxicity of, 109–110Nomenclature
of alveolar bone grafting, 543of hemifacial microsomia, 727See also Classification
Noseassessing the structure of, 13–14functions of, 49
Nutritionin cleft infants, 540–541disorders of, affecting development, 5
OOcclusion, assessment of
in cleft lip and palate, 556in craniomaxillofacial deformity, 19–20in dental implant restoration, 241in mandibular overdentures, 243
Occupational injuries, craniomaxillofacial,47–48
Ocular mobility, in craniomaxillofacialdeformity, 13–14. See also Vision
Odontogenic tumors, 59–62Onlay bone grafts
in Apert syndrome, 754maxillary, versus sinus inlay graft, 177
Open bite deformitiesanterior, bilateral posterior segmental
osteotomies for treating, 587correction of, preoperative and
postoperative x-rays, 535–536Operative procedure. See Surgical
approach/proceduresOphthalmopathy, association with
hyperthyroidism, 5Oral cavity
assessment of, in craniomaxillofacialdeformity, 19
nonseparation from the nasal cavity, 540
Orbitclinical evaluation of, 12deformities of, in hemifacial
microsomia, 728–729reconstruction of, 478–482
Orbital blowout, polylactide plates forrepairing, 115–116
Orbital cleftcentral superior, 28superolateral, 28superomedial, 28
Orbital expansion, in hemifacialmicrosomia, timing of, 733
Orbital floor repairof defects, 362–365
calvarial bone graft reconstruction,704–705
polymers for fracture fixation, 117Orbital hypertelorism, 738–748
analysis of malformation in, 738–739
in bilateral coronal synostosis, 675in metopic synostosis, 675
Orbital implants, 133Orbital rim advancement (ORA),
preoperative and postoperativeviews, 675–676
Orbitomaxillary cleft, medial, 26–27Orbitozygomatic reconstruction, 105Orientation
compromised, restoring dental fixtureswith, 255
of single-tooth restoration, 250Oromandibular complex, reconstruction of,
290–291three-dimensional, software for, 291
Oronasal fistulae, closing, 542Orthodontia
for children with cleft lip and palate,541–542, 561
in hemifacial microsomia, 735Orthodontist, role in bimaxillary surgery,
523Orthognathic examination, 497–521Orthognathic modules, craniofacial
modular fixation system, 454–455Orthognathic surgery
after bone graft closure of a palatalfistula, 572–573
in cleft lip and palate, 567defined, 639examination before undertaking,
506–520indications for, in cleft lip and palate,
557, 561models used for planning, 514–518
Orthopedics, preoperativefor cleft infants, 542–543effect on later bone grafting for alveolar
clefts, 555–556Ortho Treatment Planner (software), 514Osseointegration
of dental implants, 155in bone grafts, 327–328
in dentistry, 232evaluation of, with computerized
tomography imaging, 203of implants in cleft lip and palate
reconstruction, 548, 551maintaining, in dental implant
restoration, 253in maxillary sinus grafting, 174–197of metal implants, 124of screws in microvascular grafts, 322of titanium, 110
effects of irradiation on, 419experimental study in dogs, 128plasma-sprayed, 140–142
Osteitisdefined, 76osteoblastic, 83
778 Index

Osteoarthritis, as an indication forcostochondral grafting, 353–354
Osteocutaneous flap, from the fibula,327–328
Osteogenesiseffects of irradiation on, before and after
implantation, 425–426head and neck, 41
Osteogenic sarcoma, hemimandibulectomy,chemotherapy and radiotherapy for,469
Osteoinduction, defined, 180Osteomyelitis
chronic, ankylosis of thetemporomandibular joint caused by,354
historic observation of, 76infantile, 83of the mandible
nonsuppurative, 81–82posttraumatic, 433–438
Osteoplastic segment, maintaining bone as,in skull base surgery, 491
Osteoradionecrosis (ORN), 86–87, 433mandibular, reconstruction in, 475–476
Osteosarcomabone resection and reconstruction in,
324replacement of chin and mandible due
to, 374–375Osteosynthesis, hardware-supported, 1Osteotome
for separation of the pterygoid plates,history of, 581
sinus floor elevation using, 195Osteotomies
mandibular, 104–105maxillary, 581–605surgical technique, maxillary sinus
grafting, 186transfacial access, 491–496
Outcomesof mandibular condyle reconstruction,
347–351of mandibular condyle replacement with
a prosthesis, 374–375unsatisfactory, in orthognathic surgery,
500See also Follow-up
Overdenturesimplant failure rate associated with,
244–245for support in dental restorations,
146–147, 237, 241–243Overdrilling, of holes in genioplasty, 631
PPalate, embryological development of, 539Papilloedema
association with craniosynostosis, 713
association with intracranialhypertension, 673
Parathesia, after maxillary sinus grafting,194
Partial-thickness calvarial bone grafts,outer cortex, “potato chip” graft,701–702
Pathogenesisof craniosynostosis, 673of hemifacial microsomia, 681–682,
728of osteomyelitis, 77
of the frontal bone, 84of the mandible, 80
See also EtiologyPathology, bony, radiology for identifying
before orthognathic surgery, 513Pedicled flaps, for soft tissue involved in
mandibular reconstruction, 338Periodontal problems, in mandibular
midline split, 648Periorbital/cranial base defects,
reconstruction of, 361–367Periorbital region
evaluating, 11reconstruction of defects in, 361–367
Perko-Bell technique, for posteriormaxillary osteotomies, 588, 603
Perthes osteotomy, 610Pfeiffer syndrome, 680–683
facial features of, 36, 664Phagocytosis, in resorption of polylactide,
115Physiological insult, from corrosion of
metals in internal fixation, 107–110Pigs, experimental grafting of mandibular
defects, 127–128Pindborg tumor, panoramic image, graft
with healing, 221Pins, for craniomaxillofacial bone healing,
102Plagiocephaly, 33
anterior, 674defined, 10, 30timing of surgery for, 733
Plain film, for evaluation of thecraniomaxillofacial region, 210
Planningfor bimaxillary surgery, 522–538for maxillary sinus grafting, 174–179for maxillary surgery, 528–547for orthognathic surgery, 561
data base record for training in,501–505
radiologic examination for, 513–518for treatment for oral malignancies,
69–70Planning cycle, completing, for
orthognathic surgery, 519–520Plate and screw fixation, effects on the
growing craniofacial skeleton,693–699
Platesfor craniomaxillofacial bone healing,
104, 451–456polylactide, for mandible fixation, 116See also Reconstruction plates
Pogonion (Pg), soft tissue, for evaluationof craniomaxillofacial deformity, 7
Polychondritis, relapsing, nasoseptalmanifestations of, 57
Polydioxanone (PDS)for fixation of fractures, 113tissue compatibility of, 115
Polyglycolide (PGA)for fixation of fractures, 113tissue compatibility of, 115
Polylactide (PLA)for fixation of fractures, 113lag screws, in temporomandibular joint
repair, 346membranes, for defect repair, 117–118self-reinforcing (SR) technique for
fixation of fractures, 114Polymorphic reticulosis (T-cell
lymphoma), nasoseptalmanifestations of, 57
Polymorphonuclear neutrophil (PMN)function, and sinus lift surgery,178–179
Porcelain, for dental implant restoration,241
Positioningof maxillary sinus implants,
complications of, 194–195to stabilize a mandibular sagittal split
ramus osteotomy, 641in temporomandibular joint prostheses,
381Posterior areas, in maxillary implant
positioning, 243–246Posterior maxillary segmental osteotomies,
602–603Postoperative management
computed tomography imaging to assessosseointegration, 203
mandibular angle grafts, 391–393maxillary sinus grafts, 187–189
Posttraumatic osteomyelitis of themandible (PTOM), 80, 433–438
Pott puffy tumor, 84–85Prediction, measurements for, in
genioplasty, 627Preformed grafts, endochondral, 130–131Premaxilla
in bilateral alveolar cleft, 540union with the maxillary alveolar
process, during development, 539Premaxillary osteotomy, in cleft lip and
palate, 561–562
Index 779

Press-fit implants, for patients with limitedintermaxillary opening, 246
Primary bone repairwith osseointegrated dental implants,
429in posttraumatic osteomyelitis, 434versus secondary bone repair, 323–324
Primates, craniomaxillofacial surgeryresearch using, 693–699
Profile examinationfor evaluating craniomaxillofacial
deformity, 9before orthognathic surgery, 509–512
Prognathismmandibular, correction of, preoperative
and postoperative x-rays, 537in skeletal malocclusion, 39
Prognosis, in oral cancer, 69Progressive condylar resorption (PCR),
with rigid internal fixation,mandibular osteotomy, 617
Projection, nasal, 14Proportional centrofacial T, 746–747Prostheses
condylar, for replacement of themandibular condyle, 372–376
craniomaxillofacial, 132–135in craniomaxillofacial deformity,
classification system, 90facial, skin-penetrating implants for
anchorage of, 133–134mandibular
fixed, 237–241removable, 241–243
maxillaryfixed, 244removable, 244–245
metal, for primary functionalreconstruction, 399
removable, 439–444retention of, screw versus cement for
dental implant restoration, 235–236Prosthodontic concept
dental implant restoration, 232–261ITI dental implant system, 143–146solutions for compromised implant
placement, 254–255Psychological effects
of cleft lip and palate, 542in patients seeking orthognathic surgery,
497–500Psychosocial considerations
adjustment in hemifacial microsomia,735–736
in treatment of oral cancer, 73
QQuantification, of facial harmony, 284–285Quantitative assessment, in Crouzon
syndrome, 714
RRabbits, experimental grafting of tibia
defects, 127–128Race, and incidence of cleft lip and palate,
22Radial forearm flap
advantages and disadvantages of using,389–390
for mandibular reconstruction, 338–339Radial forearm osteomuscular-
fasciocutaneous flap, formaxillofacial reconstruction, 308
Radiated mineralized cancellous allografts(RMCA), experimental evaluationof, 130
Radiationassociation with microcephaly, 671effect on implant failure, 133–134
Radiation therapyeffect on choice of graft procedure, 327,
341, 369and internal fixation devices, 419–432osteoradionecrosis as a result of, 86–87
Radical excision, of oral cancers, 70Radiographic assessment
of craniofacial deformities, 672of craniomaxillofacial region, 210–219for diagnosis of craniomaxillofacial bone
infections, 78in mandibular grafting, 407in maxillary sinus grafting, 175–176of osteomyelitis of the maxilla, 84See also Computed tomography
Radiographynarrow-beam, detailed, 210panoramic, 210–211
Radiologyfor evaluation of the mandibular
condylar prosthesis, 378for evaluation of the temporomandibular
joint, 343–345for examination before orthognathic
surgery, 512–518for follow-up of bone grafts, case
reports, 220–231for observation of condylar prosthesis,
375Radionuclide imaging
in craniomaxillofacial bone infections,78–79
in osteomyelitisof the frontal bone, 85suppurative, 81
Ramus osteotomycombination with midline split, 648vertical, 614–615
Recipient sitepreparation of, in calvarial bone grafting,
703–704in surgery for cleft lip and palate, 543
Reconstructioncomplications of, in irradiated fields,
290head and neck, for the oncologic patient,
289–294mandibular
after surgery for oral cancer, 71–72timing of, 335
orbital, technique for, 479–480Reconstruction plate
for bridging bony defects, 317, 320,336–337
development of, 1for double barrel graft fixation, 331–332for extensive anterior mandibular defect
repair, 414after oral surgery for cancer, 73permanence of, 395–397three-dimensional, for mandibular angle
defect reconstruction, 389Record keeping, radiologic examination as
part of, in orthognathic surgery, 513Rectus abdominis free flap, for mandibular
reconstruction, 338Rectus abdominis musculocutaneous flaps,
361–364Relapse
in genioplasty, 652in intraoral vertical ramus osteotomy,
after bone screw fixation, 646in the Le Fort I maxillary osteotomy,
654–656midface, 657
in mandibular sagittal split ramusosteotomy, 643–645
in subapical osteotomy, 651Remodeling, in osteotomy, 639Research
animalon the effects of plate and screw
fixation, 693–699experimental grafting of iliac crests,
128current, on prefabrication of
vascularized bones flaps, 313experimental studies of grafts and
implants, 127–128human experimentation, on the stability
of maxillofacial implants, 135studies of radiation, effects on grafting
with use of reconstruction plates,420–422
See also Clinical studiesReserpine, nasal deformities due to in
utero exposure to, 50Resin, for dental implant restoration, 241Resorbable Fixation System, 458–459Resorbable materials
for microplate fixation, in surgery formetopic suture release, 675
780 Index

plates and screws, in craniosynostosisreconstruction, 673
Resorptionof bone after extraction of all teeth, 236condylar
in late relapse after osteotomy, 639,643–645
positioning to prevent, 614with rigid internal fixation, 617
of grafts, 462effect of screw fixation on, 484reconstruction of the ascending ramus
and condyle, 464maxillary, significance of patterns in, 243
Respiratory problems, accompanying Apertsyndrome, 752
Restoration, single-tooth, 250–253. Seealso Reconstruction
Retinoic acid syndrome (RAS), earmalformations in, 728
Retrognathia, in skeletal malocclusion, 39Retromolar region, donor site for free bone
grafts, 296Revascularization, of cortical bone grafts,
126Rhabdomyosarcoma, soft-tissue grafts in
children, 365Rhesus monkeys (Macaca mulatta),
research using, 695–699Rheumatic ankylosis (RA), complications
in treating, 379–381Rheumatoid arthritis
bilateral alloarthroplasty for, 383bilateral temporomandibular joint
arthroplasty for, 384Rhinion (Rh), for evaluation of
craniomaxillofacial deformity, 7Rib as donor site
for free bone grafts, 298for nasal reconstruction, 483for pedicled bone grafts, 300
Rickett analysis of the head and face, useof, in planning orthognathicsurgery, 515–518
Ridge augmentation, localized, usingguided bone regeneration, 155–163
Ridge fracture, in maxillary sinus grafting,194
Rifle injuries, craniomaxillofacial, 47Rigid fixation
in craniomaxillofacial calvarial bonegraft harvesting, 700–712
in osteotomies for Apert syndromereconstructions, 753–754
Rigid internal fixation (RIF)for bimaxillary surgery, 522–538in the growing facial skeleton,
disadvantages of, 693in horizontal osteotomy of the
symphysis, 612
in mandibular osteotomy, 606–622in maxillary osteotomy, 581–605in maxillary surgery, 527–528for nasal reconstruction, 483–488in posttraumatic osteomyelitis treatment,
434–435, 436–437stability of maxillary and mandibular
osteotomies with, 639–659Rods, polylactide, for mandible fixation,
116Rotation, nasal, 14
SSaethre-Chotzen syndrome, facial features
of, 36Sagittal interrelationships, in skeletal
malocclusion, 38–39Sagittal osteotomy, fixation with
biodegradable self-reinforcingpolymer screws, 119, 121
Sagittal split ramus osteotomy (SSRO),606
bilateral, 639–645condylar torquing in, 618mandibular, 612–614morbidity in, 523
Sagittal suture synostosis, 675–676Sarcomas
ameloblastic fibrosarcomas orodontosarcomas, 61, 70
mandibular fibrosarcomas,reconstruction after removal of, 386
Scanning, of bone in oral malignancies,68–69
Scaphocephalydefined, 10, 675deformity in, 31lateral and superior views, 679
Scapuladonor site for ascending ramus and
condyle grafts, 465–466with flaps
for mandibular continuity defectrepair, 321
for maxillofacial reconstruction,304–306
myocutaneous flaps from, advantage inanterior defects of the mandible, 414
vascularized bone grafts from, formaxillofacial reconstruction, 313,359–361, 472
Scapular flap, for mandibularreconstruction, 389–390
Scar tissue, fibrous, in bone healing, 125Schneiderian membrane, tearing of, in the
sinus lift procedure, 189, 193–194Schuchardt procedure, posterior maxillary
osteotomy, 586–587Schwannoma, suprasellar, transfacial
access to, 493
Sclerosing osteomyelitis, chronic, 81–82Screw and drill bit chart, craniofacial
modular fixation system, 449Screws
for craniomaxillofacial bone healing,102–103
in dental implants, loose or fractured,254
effect of fixation with, on boneresorption, 484
failure of, comparison of conventionaland THORP plates, 402–403
polylactide copolymer, for mandiblefixation, 116
technique of fixation with, 532–534Secluded space, creation and maintenance
of, in guided bone regeneration,156–157
Secondary bone grafting, delay of, afterirradiation, 429
Segmental osteotomies, periodontal defectsresulting from, 523
Segment control, during surgery, with atransbuccal trocar, 534–535
Self-reinforcing technique, polymers forfracture fixation, 114
Septal hematoma, septal abscess from, 54Serratus anterior muscle (SAM), for
oromandibular defect repair, 338Sex
and cleft lip and palate incidence, 22and Garre sclerosing osteomyelitis
incidence, 82and hemifacial microsomia incidence,
727Sheep, experimental grafting of iliac crests,
127–128Shotgun injuries, craniomaxillofacial, 47Shotgun wound, repair of, 416Silver-palladium, for dental substructure
fabrication, 239Simmons-Peyton classification
of craniofacial deformities, 36of facial clefting, 30
Single-tooth osteotomy, 606Sinus, cranialization for management of,
495Sinus lift graft procedure, 174
smoking, 178–179Skeletal malocclusion, etiology of, 38–42Skull, donor site for free bone grafts,
296–297Skull base
reconstruction of, after cancer surgery,292
transfacial access osteotomies to,489–496
Smokingassociation with mandibular
osteomyelitis, 435
Index 781
Smoking (Continued)as a contraindication to fibula donation,
414as a contraindication to sinus lift in,
178–179Soft tissue
alterations ofin cleft and noncleft patients, 561in orbital hypertelorism, 744
closure in genioplasty, 631effects on, of irradiation, 427–429for evaluation of craniomaxillofacial
deformity, 7flaps for coverage of craniomaxillofacial
osseous continuity defects, 335–342healing of
delayed, as a complication ofmaxillary sinus surgery, 194
in the presence of a membrane, 156isolated grafts of, 359–361local flaps for reconstruction of, in
maxillary midface defects, 356–359
macrostomia in hemifacial microsomia,730
malformation ofassociation with cleft, 28in hemifacial microsomia, 683
prevention of growth into grafts, andsuccess of incorporation, 127
for reconstruction in craniomaxillofacialdeformity, 90
restoration after surgery, 310, 337–338for oral cancer, 72
surgical access viaLe Fort II osteotomy, 660Le Fort III osteotomy, 664–665
Spark erosion prosthesis, maxillary, 245Speech
effect onof cleft lip and palate, 556of dental implant restoration, 237
patterns of, evaluating in cleft lip andpalate, 551
problems with, in cleft infants, 541Sphenoid bone, locating targets for skull
base surgery relative to, 489–490Spiessl technique, for mandibular sagittal
split ramus osteotomy, 616Squamous cell cancer
bilateral total maxillectomy for, 439–444involving the jaw joint, 291mandibulectomy for, 411–413oral, 65–70patterns of spread, and margins of safety
in resection, 336repair of deformity after surgery for, 415
Stabilityof grafts, 127
long-term, of maxillary and mandibularosteotomies with rigid internalfixation, 639–659
of maxillary osteotomies, 587segmental, 603
of midfacial advancement osteotomies incleft patients, 574, 577
of rigid fixation versus wireosteosynthesis, in the Le Fort Imaxillary osteotomy, 655–656
Stabilizationof the Le Fort II osteotomy, midface
reconstruction, 662–663of the Le Fort III osteotomy, midface
reconstruction, 666–667in metopic suture release, 675in orbital rim advancement, 675–676
Stainless steel implants, 111Standardized incidence ratio, for oral
cancer, Finnish Cancer Registry,65–66
Staples, for craniomaxillofacial bonehealing, 102
Stent, surgical, for dental implantrestoration, 232–233
Step defects, in Le Fort III osteotomy,723–724
Step osteotomy, 606Von Eiselberg, 609
Stomion (St), for evaluation ofcraniomaxillofacial deformity, 7
Stress, physiologic, and bone density,233–234
Stud-retained overdentures, 242Subantral grafting and implant insertion,
185Subapical osteotomy, 650–651Subcondylar osteotomy, 610
horizontal, 609vertical ramus, 606
Subcranial orbital rotation, 746Substructure fabrication, dental implant
restoration, 239Superior vermilion border (Vs), for
evaluation of craniomaxillofacialdeformity, 7
Supracrestal connective tissue, arounddental implants, plasma-sprayedtitanium, 142–143
Supraorbital contour, reshaping, in Apertsyndrome surgery, 751
Surgical approach/proceduresin angioplasty, 627–628in cleft lip and palate, 543–546condylar prosthesis for replacement of
the mandibular condyle, 372–374in craniosynostosis, staging of
reconstruction, 673in Crouzon syndrome, 715–724
dental implant system, 164and fixation method, for
craniomaxillofacial bone healing,104–105
for genioplasties, 628for mandibular restoration, 390–391for orbital hypertelorism management,
740–748for osteotomies, in cleft lip and palate,
561–574planning of, for oral cancer, 70–73for temporomandibular joint repair,
345–346See also Planning
Surgical techniquefor Le Fort II osteotomy, midface
reconstruction, 660–662for Le Fort III osteotomy, midface
reconstruction, 665–666for maxillary osteotomies, 591–601
segmental, anterior, 601–602for maxillary segmentation, 596for maxillary sinus grafts, 185–187See also Techniques
Suturescraniofacial, closure and fusion of,
40–41polylactide, for mandible fixation,
116Swansea approach, to bone grafting in cleft
lip and palate, 546–548Symphysis
as a donor site for corticocancellousblocks, 181
horizontal osteotomy of, 612rigid fixation in, 617
Syndactylyin Apert syndrome, 36, 679, 682,
749in Pfeiffer syndrome, 680–681
Synostosis, bilateral coronal, 675Synovitis, acne, pustulosis, hyperostosis,
osteitis (SAPHO) syndrome, 82Systemic disorders, observation of, before
orthognathic surgery, 500
TTandem screw fixation, in mandibular
osteotomies, 615–616Tearing injuries, craniomaxillofacial, 48Technetium scan
of bone repair with fibula double-barrelvascularized graft, 332–333
in craniomaxillofacial bone infection,78–79
Techniquesin genioplasty, 651–652in intraoral vertical ramus osteotomy,
645–646
782 Index

in the Le Fort I maxillary osteotomy,654
midface, 656–657in mandibular midline split, 648in mandibular sagittal split ramus
osteotomy, 640in nasal reconstruction, 484–488in subapical osteotomy, 650–651See also Surgical technique
Teethcharacteristics of, in bilateral cleft
patients, 557cleft-adjacent, variations of, 540eruption of, effect of cleft alveolar
osseous defect, 542Telecanthus, in a Tessier No. 12 cleft,
28Temporalis osteomuscular flap, for
maxillofacial reconstruction, 301Temporal region, evaluating in
craniomaxillofacial deformity, 11Temporomandibular joint (TMJ)
ankylosis of, condylar prostheses insurgery for, 377
defective, replacement of, in hemifacialmicrosomia, 734
degenerative changes in, andimmobilization of the mandible,606
dysfunction of, identifying prior toorthognathic surgery, 506
restoration of, 291, 343Tessier classification
of craniofacial clefts, 23–29of craniofacial deformities, 52–53of craniosynostosis syndromes, 35–37
Thalidomide, hemifacial microsomia-likedefects from animal studies with,728
Three-Dimensionally BendableReconstruction Plate system, forfixation of bone grafts, 321, 323
Throat point (C), for evaluation ofcraniomaxillofacial deformity, 7
Tibia, donor site for autogenous bonegrafts, 300
Tip-defining point (Tp), for evaluation ofcraniomaxillofacial deformity, 7
Tissue reactionsto ITI material in implants, 140versus polarization resistance of metals
and metal alloys, 107–108to polymers for bone fixation,
114–115See also Soft tissue
Titanium Hollow Screw ReconstructionPlate (THORP)
advantages of, 323–324in condylar reconstruction, 381
for anterior mandibular archreconstruction, after surgery, 290
for bilateral maxillary defectreconstruction, 439–444
combination with adaptable condyles,372
for dental implant restoration, 275–278for reconstruction of mandibular
continuity defects, 321–323, 337,397
Titanium implants, 1, 110–111experimental evaluation of
osseointegration of, 128–129miniplate, in orbital hypertelorism
reconstruction, 744plasma-sprayed, dental, 140reactivity of metal in, 110reconstruction plates, 336–337substructure fabrication, 239
Tobacco use, and mouth cancer, 65. Seealso Smoking
Tomography, multidirectional, of thecraniomaxillofacial region, 211–212
Torquing, with rigid fixation, 639Townes view, of screw fixation of a plate
reconstruction, 401Tragion (Tg), for evaluation of
craniomaxillofacial deformity, 7Transcutaneous suction-irrigation systems,
for managing posttraumaticosteomyelitis, 433
Transfacial access osteotomies, 489–496Transglabellar approach, for transfacial
access osteotomy, 495Transmandibular approach
to the central and anterolateral skullbase, 491–494
Transmaxillary approachto the central and anterolateral skull
base, 491–494to the skull base, 494–495
Transorbitozygomatic approach, to theskull base, 496
Transplant, defined, 124–125Transverse interrelationships, in skeletal
malocclusion, 39–42Trauma
avulsion injuries, 43mandible module for repair in, 269–271nasal injury from, 56
Treacher Collins syndromeaesthetic repair in, 283classification of cranial bone
deformities, 97incomplete form of, Tessier No. 6 cleft,
27–28principles of management of, 685–686,
688–689
Treatmentfor hemifacial microsomia, 684,
733–736for orbital hypertelorism, 740
Treatment planning. See PlanningTrends, in craniomaxillofacial reconstruction,
310–316. See also ResearchTrigonocephaly deformity
in metopic synostosis, 675–677secondary, 34
Tumorsbenign
differentiating, 62maxillofacial, 59–64
lymphatic and hemopoietic, in patientswith steel hip implant, 619
nasal, 55, 57nonodontogenic, within the facial bones,
62–64odontogenic, 59–62resection of, craniomaxillofacial
deformity secondary to, 6suprasellar, 489See also Malignancies
Turricephaly, defined, 10Twins, monozygotic, discordance for
hemifacial microsomia in, 727–728
UUnilateral complete cleft lip and palate
(UCLP), deformities in, 556–557Unilock module, 273–275Universal fracture plates, maintenance of
the blood supply of microvasculargrafts with, 322–324
Upper facial plane (UFP), for evaluation ofcraniomaxillofacial relationships, 8
Vvan der Meulen classification, of clefts, 29Vascularized bone grafts (VGBs), 310–313
for mandibular reconstruction, 389–390for temporomandibular joint
reconstruction, 462Vascularized free-bone grafts, to bridge
mandibular defects, 399Vascular supply
of the anterior maxillary segment, 590in bone grafts, 125–126of the chin bone, preserving in
genioplasty, 623in craniomaxillofacial deformity, 90ensuring in maxillary osteotomies,
595–596of grafts, 127
and outcomes, 132Velopharyngeal incompetence, timing of
evaluation for correctivepharyngoplasty, 551
Index 783

Veneering materials, for dental implantrestoration, 240–241
Virchow classificationof craniofacial deformities, 35of facial clefting, 30
Visionimpairment of, in craniosynostosis, 673improving with surgery, in Apert
syndrome, 750measuring the acuity of, 12
Vitamin D deficiencies, effect ondevelopment, 5
WWaardenburg syndrome, 12Warfarin, nasal deformities due to in utero
exposure to, 50
Wassmund technique, 601inverted “L” osteotomy, 610in labial and palatal anterior segmental
osteotomy, 589, 653–654Water’s view
for assessing maxillary sinus, 175for assessing osteosynthesis plate
location, 212Wegener granulomatosis, nasoseptal
manifestations of, 57Wire fixation, for craniomaxillofacial bone
healing, 101–102Wound dehiscence, in genioplasty,
634Wunderer technique, 601
for anterior maxillary segmentalosteotomy, 590
XXenogeneic grafts, maxillary sinus, 184X-ray, of bone repair with fibula double-
barrel vascularized graft, 332
ZZygoma
biodegradable materials for fixation offractures of, 117
classification of deformities of, 93–94Zygomatic arch
defect of, calvarial bone graft forreconstruction of, 708–709
evaluating, in craniomaxillofacialdeformity, 15
Zygomatic maxillary complex (ZMC),fracture of, aesthetic repair, 281
784 Index