apls update booklet 2013 - mededcoventry.com update... · • paediatric basic life support ......
TRANSCRIPT
APLS Update 2013
Contents
• Paediatric Advanced Life Support
• BSPED Recommended DKA Guidelines 2009
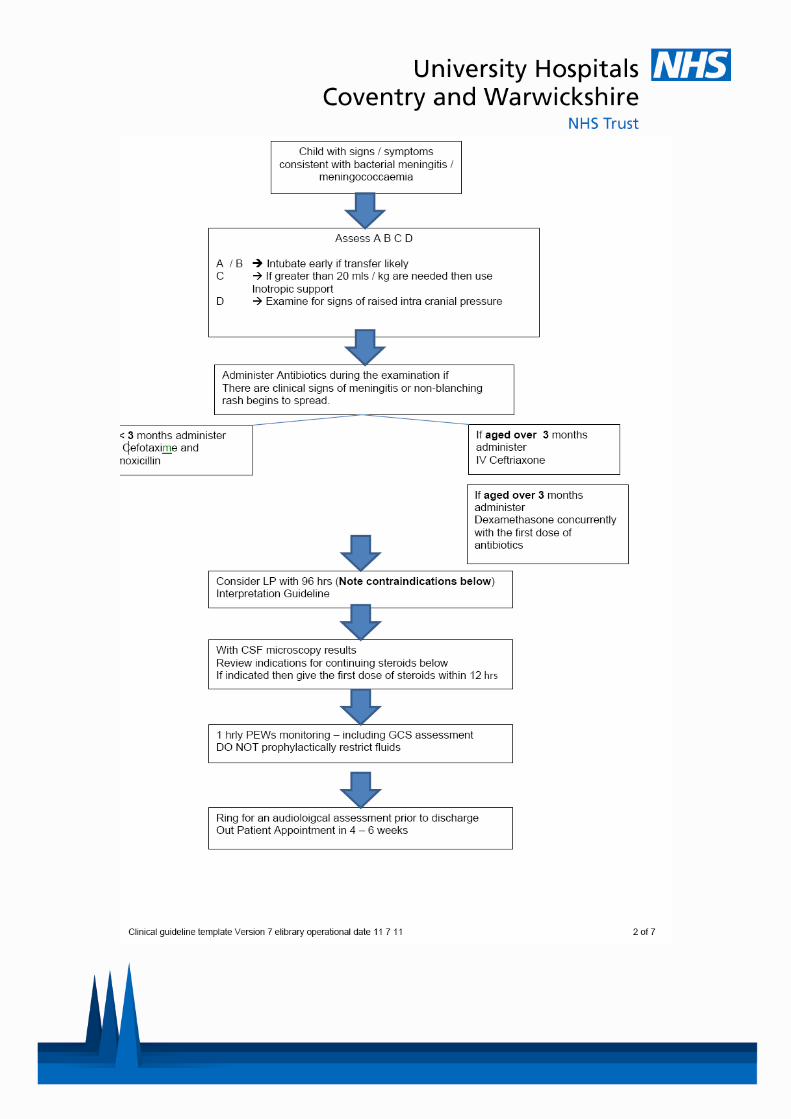
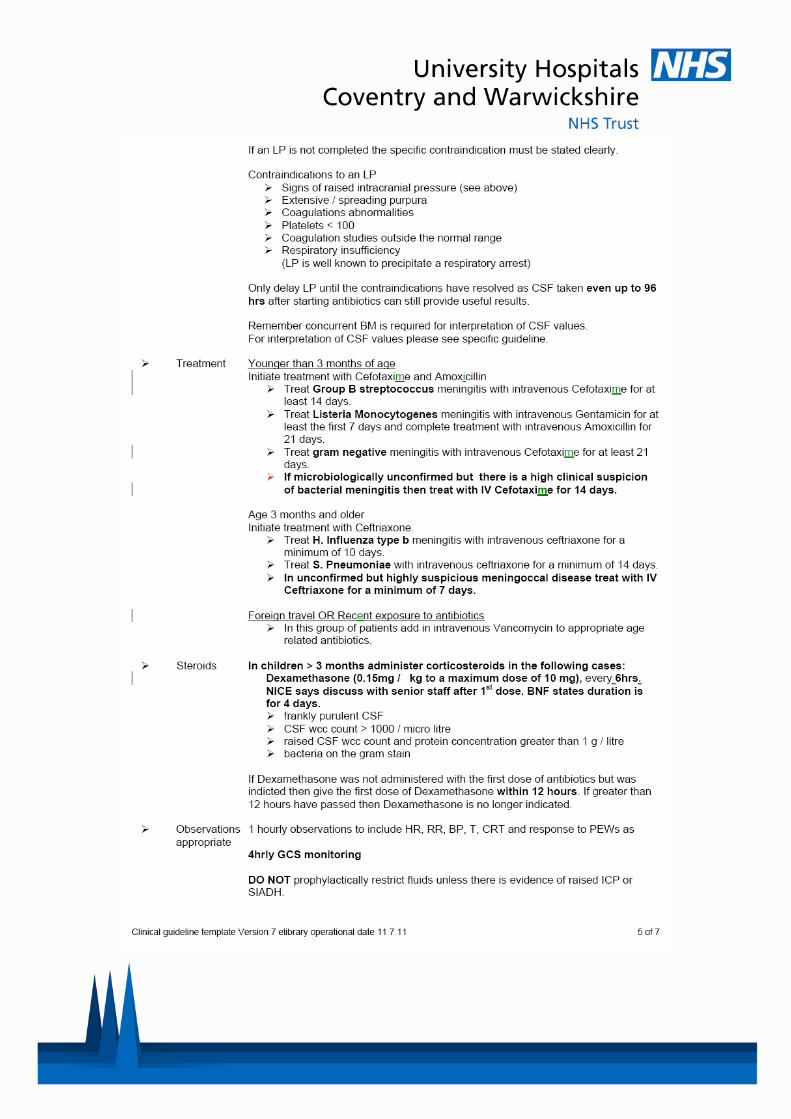
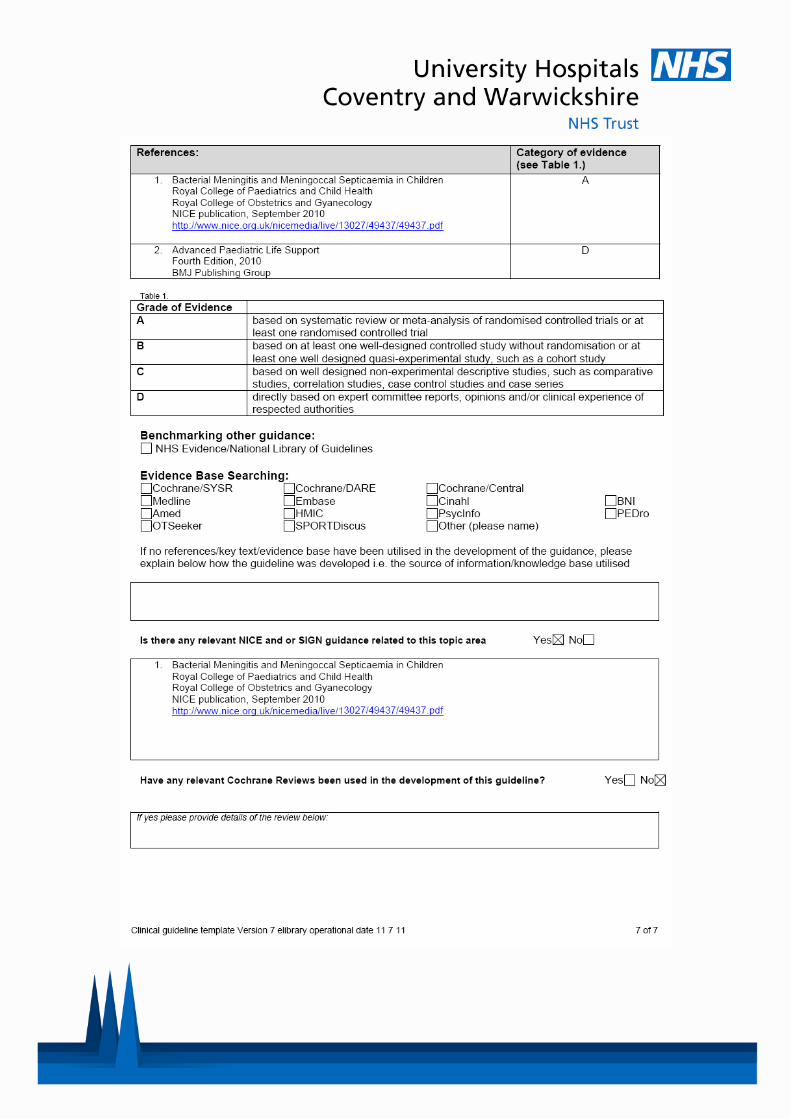
• UHCW Trust Guidelines Meningitis
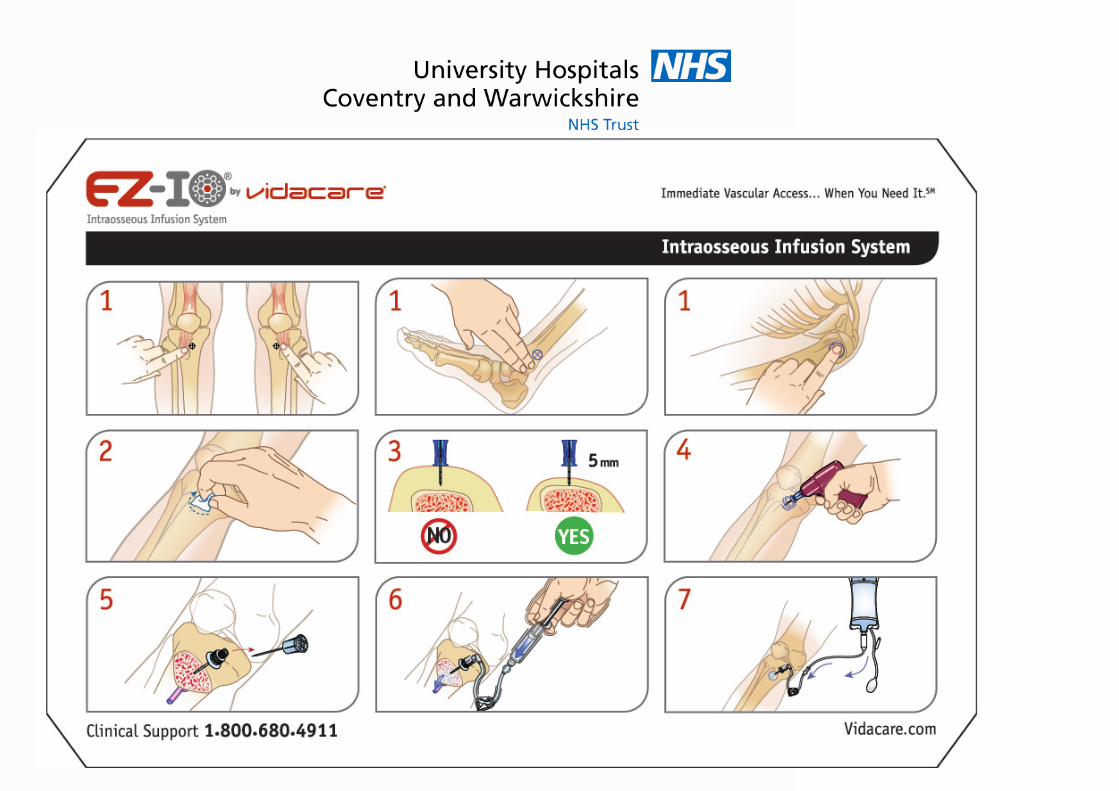
• EZ-IO Directions for Use
• Weight Estimation
• Glucose Dose
Quick Reference Contents
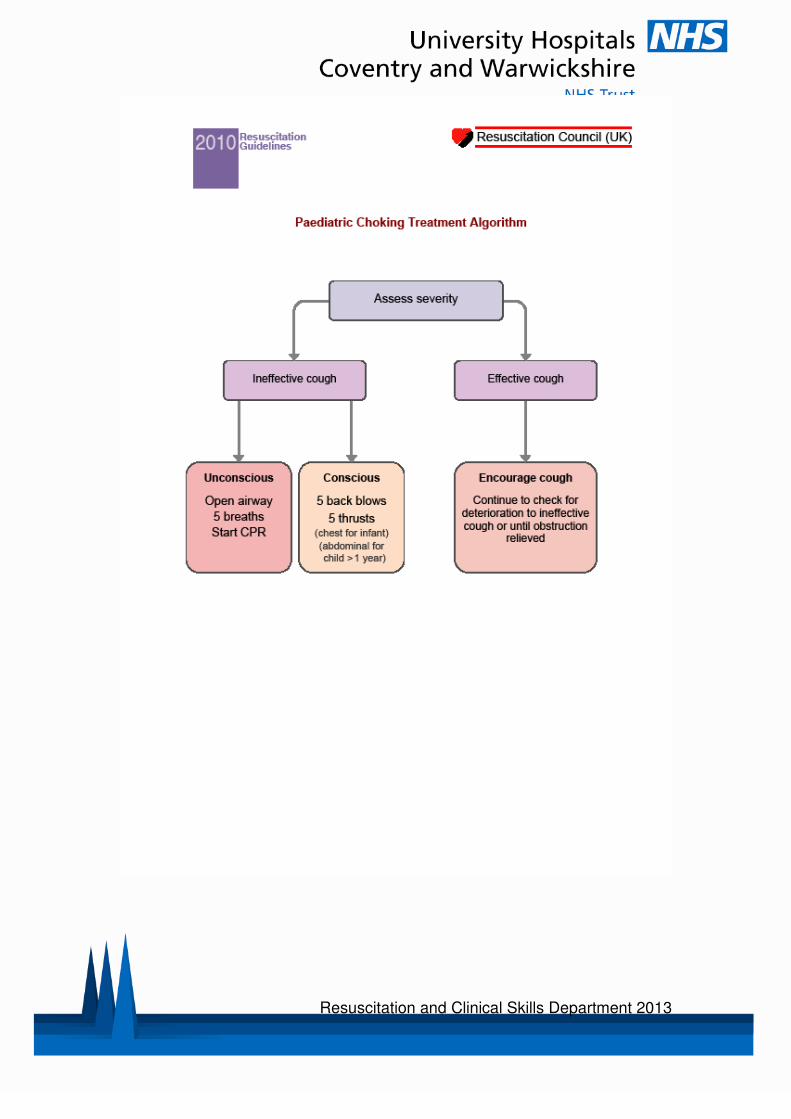
• Paediatric Choking Treatment
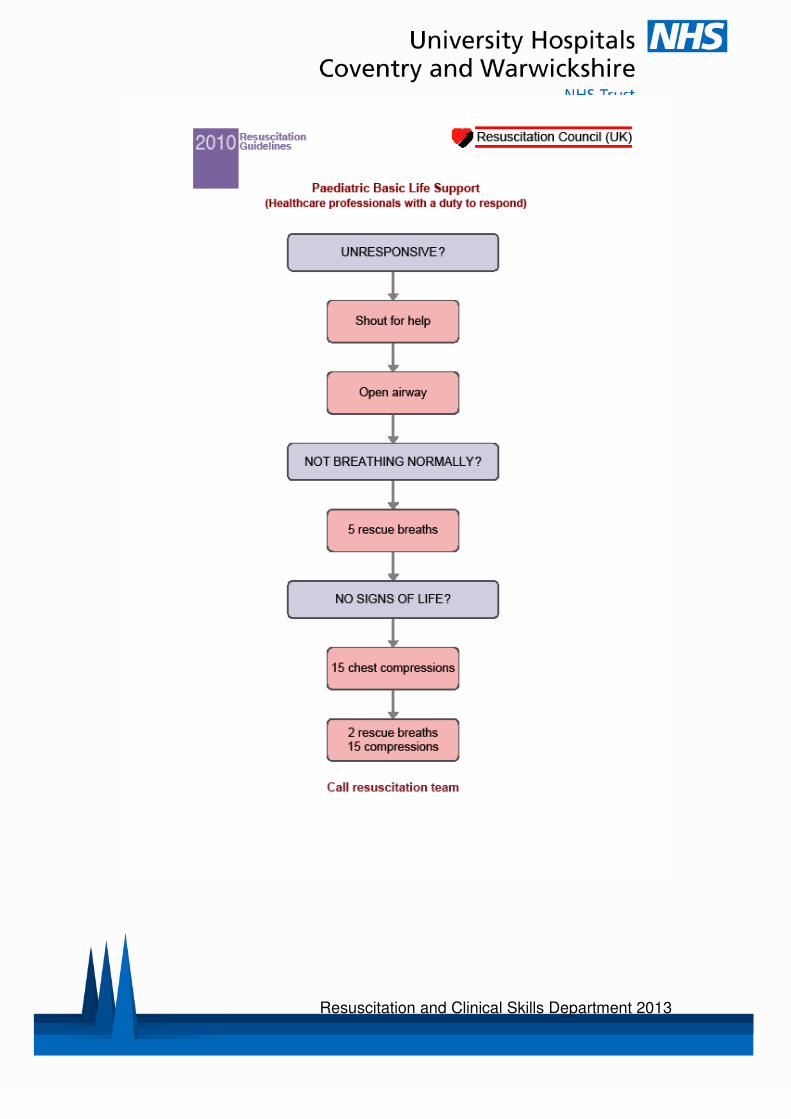
• Paediatric Basic Life Support
• Paediatric Advanced Life Support
• Anaphylaxis
• Status Epilepticus
• Management of VT
• BTS Asthma Guidelines • Paediatric Emergency Drugs calculations ( RC UK)
























Resuscitation and Clinical Skills Department 2013
APLS 5e: FAQ: Weight Estimation
The old weight formula ([age+4] x 2) has worked well for estimating weights in 1 to 10 year olds for about 20 years. However, evidence shows that the weights of children in richer countries have generally increased over this time and this formula therefore underestimates weights, especially for older children (Appendix 1). The evidence suggests that the new formula ([agex3] + 7) is better for older children, but can overestimate for smaller children. There has been much debate about the use of formulae, including whether it is better to under- or over-estimate true weight, and what should be used in resource-poor populations, given APLS is used in over 20 countries. This was debated at the Annual Instructors' Day December 2008 (Appendix 2). It is clear that the use of any formula at a single age may have a wide error and that weights in different populations also differ widely. Thus ALSG decided that we would no longer advocate one method of weight estimation. As now recommended in the 5th edition, ALSG advise that health professionals decide locally what method provides the easiest and best method for their own needs. We recommend use of population growth charts (which allows estimation of medians for any age, as well as 10th and 90th centiles), Sandell or Broselow tapes, or formulae. Regarding the latter, the traditional formula has been maintained for small children (1-5 years: [age+4]x2 = [agex2]+8 ), but the new one is used for older children. ALSG has previously made no recommendation for infants under 1 year, but a paper from the US shows that the formula [age x 0.5] + 4, may be used. In line with the above, APLS courses have been modified so that less time is spent on undertaking calculations. These are now done for the cardiac simulation alone, but provided ready calculated in subsequent simulation practices. Regarding children over 12, ALSG has never had a formula for this age group - the onset of puberty from 10 years onwards means that there is an even greater range of possible weights at any one age. A formula would therefore have a high likelihood of error. In addition, at this age, weights are approaching the maximum weight used to calculate doses and equipment sizes, ie weights of 40kg or 50kg. For inexperienced practitioners, we recommend using growth charts and estimating whether the child is small, medium or large for their age. Please see the following for associated reading: Appendix 1 - Luscombe, M & Owens B. 2007: Weight estimation in resuscitation: is the current formula still valid? Appendix 2 – Oakley, P. 2008: Paediatric Weight Estimation Appendix 3 – Marlow, R. et al. 2011: Accurate Paediatric Weight Estimation by Age: Mission Impossible?

Resuscitation and Clinical Skills Department 2013
APLS 5e: FAQ: Glucose Dose There is as expected a paucity of evidence for the bolus dose of glucose. The recommendation to change the dose came from the Inherited Metabolic Disease and Endocrinology Speciality Groups of RCPCH. The experts are less concerned about the size of bolus, but do feel that a follow-on infusion is a 'must'. Large boluses without follow-on infusion are commonly followed by rebound hypoglycaemia and do not encourage a smooth homeostasis. Experience shows that 2mls/kg is enough to treat induced hypoglycaemia and so should usually be sufficient to treat hypoglycaemia associated with illness or injury (provided there is an ongoing infusion). Remember 2mls/kg of 10% glucose = 200mg/kg (not an insignificant amount of glucose). Some international courses, especially in resource poor countries, are concerned about dropping the bolus dose from 2mls to 5mls, as WHO guidance is currently 5mls/kg - malnutrition is of course more common in these settings. Even though the evidence is only anecdotal, it is reasonable to use 2mls/kg. Ultimately, the recommendation could be 2 to 5 mls / kg (or 2 + 2 mls, or whatever), BUT it MUST be followed by an infusion.
Resuscitation and Clinical Skills Department 2013
Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013

Resuscitation and Clinical Skills Department 2013
Resuscitation and Clinical Skills Department 2013
Notes