apheresis reimbursement: guide to billing and … reimbursement: guide to billing and securing...
TRANSCRIPT

Apheresis Reimbursement: Guide to Billing and Securing
Appropriate Payment
May 24, 2013
Keith Berman, MPH, MBA
Health Research Associates
Pasadena, CA
(626) 564-0456

Disclaimer
Information and examples presented below are for
general educational purposes only. They do not
constitute advice for actual coding or billing by
physicians or hospitals.
Insurance billing codes, billing policies, coverage
policies and payment rates are subject to change.
Providers with questions should consult with
representatives of their third party payers before
submitting insurance claims.
Educational Objectives
Coding basics for therapeutic apheresis services
Medicare payment for hospital inpatient/outpatient apheresis
Physician apheresis supervision: billing rules and payment
Strategies for minimizing/addressing coverage denials
Special issues:
Plasma exchange and cytapheresis
Photopheresis
LDL apheresis

Codes: The Shorthand of Insurance Billing
• CPT codes. 5-digit codes used by physicians and hospitals to
bill insurers for outpatient procedures and services.
• ICD-9-CM procedure codes. Used by hospitals to identify
significant procedures during an inpatient stay.
• ICD-9-CM diagnosis codes. Used to identify diagnoses that
are both related and unrelated to the procedure or admission.
• Revenue codes. 3-digit codes that define the hospital
department or service category under which procedures or
products are billed.

Hospitals and Physicians Submit Separate Claims for Payment
Physicians: CMS-1500 Hospitals: UB-04
Health Insurer
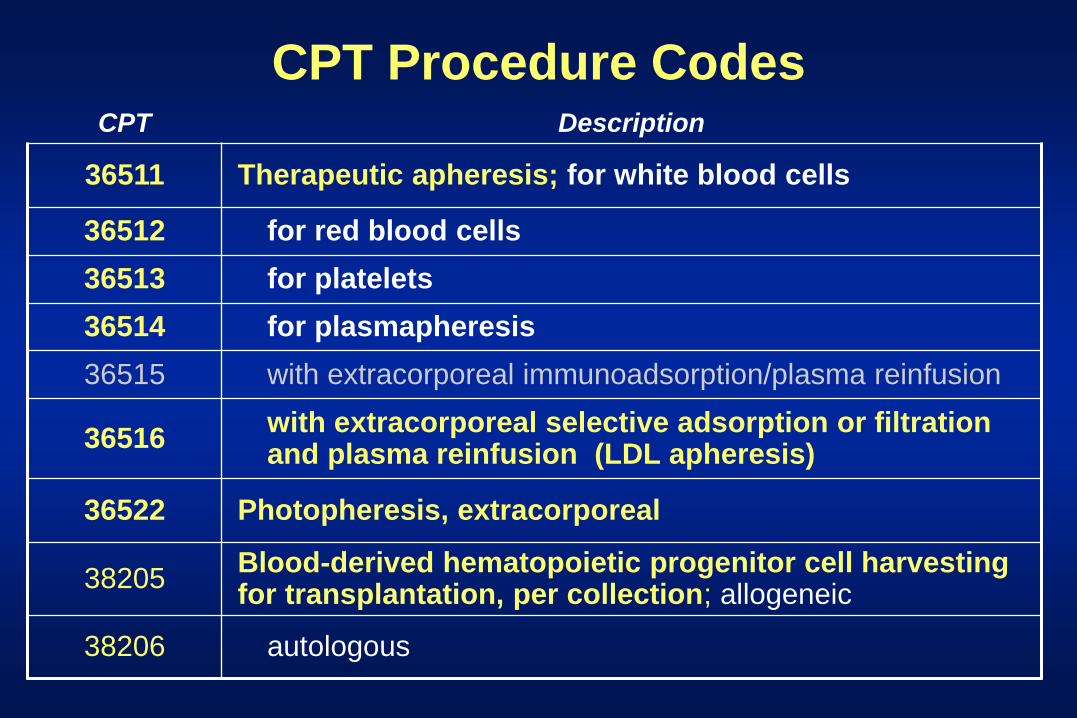
CPT Procedure Codes CPT Description
36511 Therapeutic apheresis; for white blood cells
36512 for red blood cells
36513 for platelets
36514 for plasmapheresis
36515 with extracorporeal immunoadsorption/plasma reinfusion
36516 with extracorporeal selective adsorption or filtration and plasma reinfusion (LDL apheresis)
36522 Photopheresis, extracorporeal
38205 Blood-derived hematopoietic progenitor cell harvesting for transplantation, per collection; allogeneic
38206 autologous
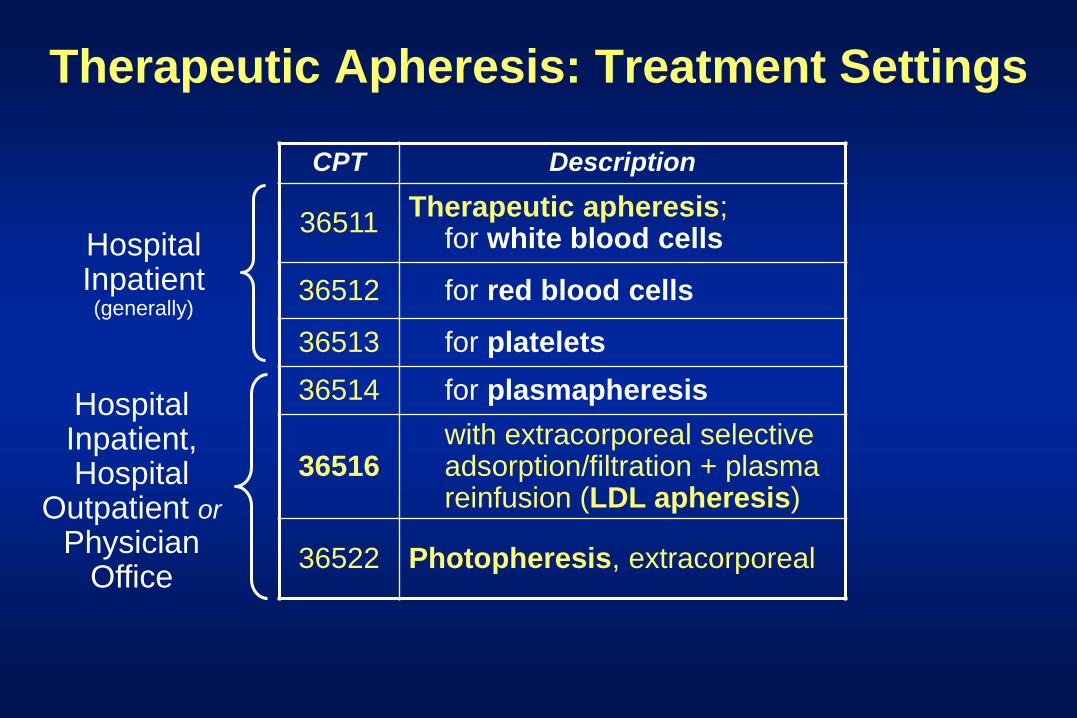
Therapeutic Apheresis: Treatment Settings
CPT Description
36511 Therapeutic apheresis;
for white blood cells
36512 for red blood cells
36513 for platelets
36514 for plasmapheresis
36516 with extracorporeal selective adsorption/filtration + plasma reinfusion (LDL apheresis)
36522 Photopheresis, extracorporeal
Hospital Inpatient (generally)
Hospital Inpatient, Hospital
Outpatient or Physician
Office
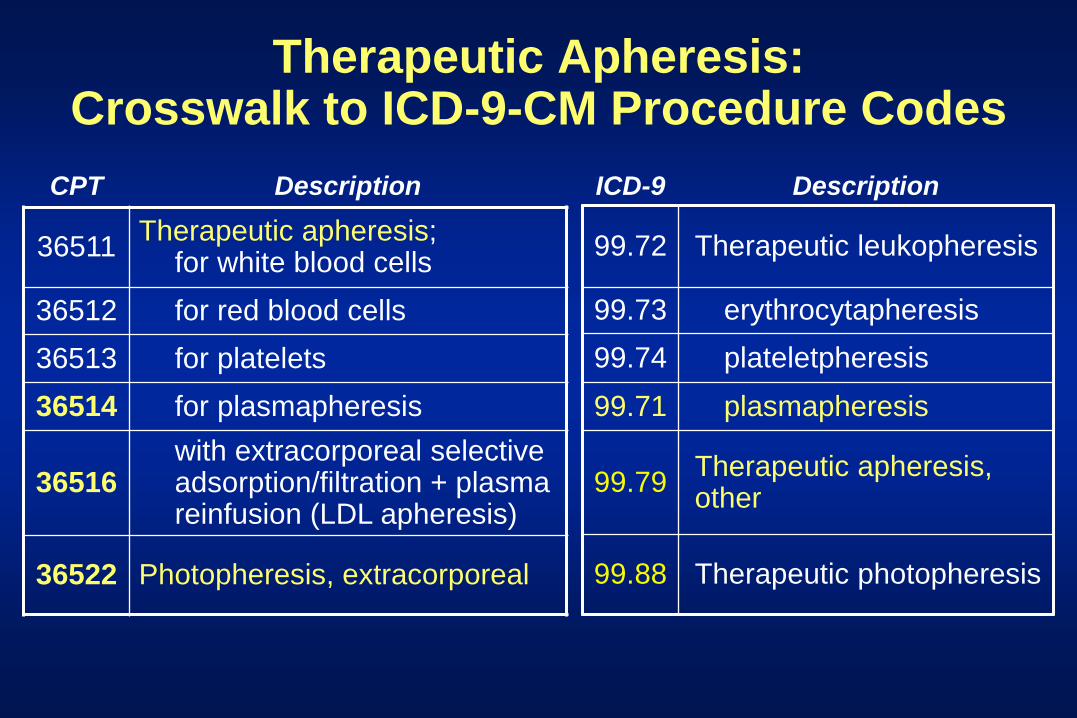
Therapeutic Apheresis: Crosswalk to ICD-9-CM Procedure Codes
CPT Description
36511 Therapeutic apheresis;
for white blood cells
36512 for red blood cells
36513 for platelets
36514 for plasmapheresis
36516 with extracorporeal selective adsorption/filtration + plasma reinfusion (LDL apheresis)
36522 Photopheresis, extracorporeal
ICD-9 Description
99.72 Therapeutic leukopheresis
99.73 erythrocytapheresis
99.74 plateletpheresis
99.71 plasmapheresis
99.79 Therapeutic apheresis, other
99.88 Therapeutic photopheresis
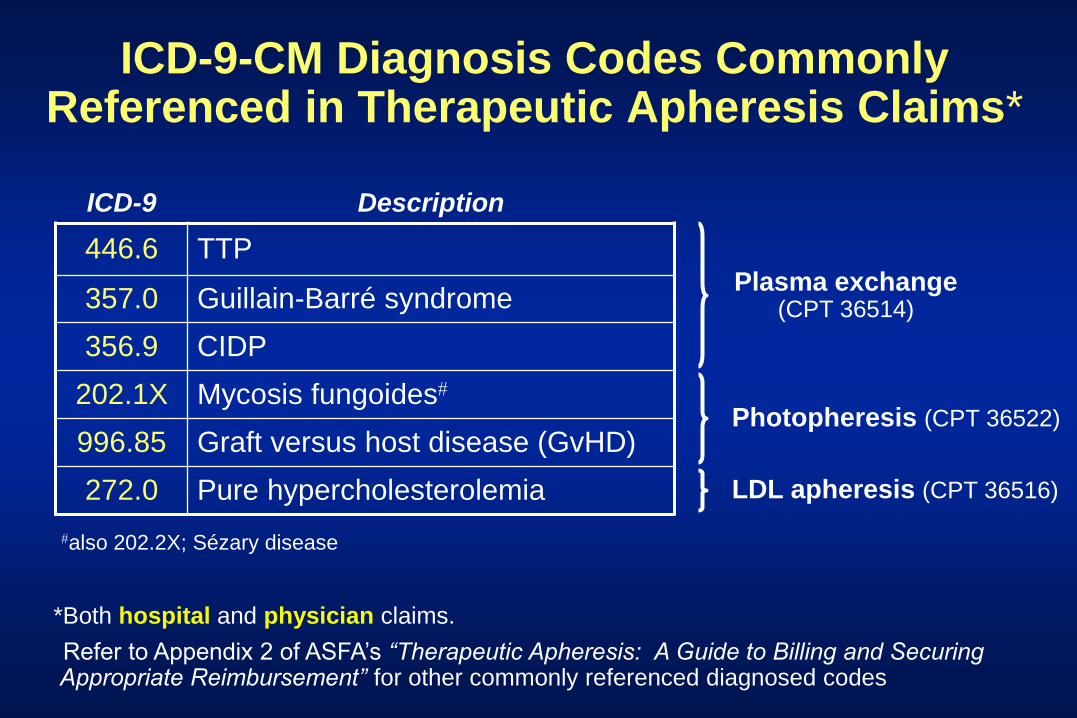
ICD-9-CM Diagnosis Codes Commonly Referenced in Therapeutic Apheresis Claims*
ICD-9 Description
446.6 TTP
357.0 Guillain-Barré syndrome
356.9 CIDP
202.1X Mycosis fungoides
996.85 Graft versus host disease (GvHD)
272.0 Pure hypercholesterolemia
*Both hospital and physician claims.
Refer to Appendix 2 of ASFA’s “Therapeutic Apheresis: A Guide to Billing and Securing Appropriate Reimbursement” for other commonly referenced diagnosed codes
also 202.2X; Sézary disease
Plasma exchange (CPT 36514)
Photopheresis (CPT 36522)
LDL apheresis (CPT 36516)
Medicare Hospital Outpatient Billing and Payment:
Ambulatory Payment Classifications (APCs)

Coding the UB-04 Hospital Claim Form for an Outpatient Plasma Exchange Procedure
Scenario: A myasthenic patient is exchanged on 5/11/2013
42 REV. CD. 43 DESCRIPTION 44 HCPCS 45 SERV
DATE 46 SERV UNITS
47 TOT CHARGES
949 OTHER THER SVS 36514 05/11/13 1 $2,475.00
67 PRIN. DIAG. CD.
68 CODE
69 CODE
OTHER DIAG.
70 CODE
202.14
80 PRINCIPAL
CODE
PROCEDURE
DATE
81 OTHER
CODE
PROCEDURE
DATE
OTHER
CODE
PROCED
DATE
99.88
A
B
Therapeutic plasma
exchange
CPT code
ICD-9-CM
procedure code
$990 cost x 2.5
charge-to-cost ratio
(in this example)
Myasthenia gravis ICD-9-CM
diagnosis code
Revenue
code

CPT Description
36511 Therapeutic apheresis; for white blood cells
36512 for red blood cells
36513 for platelets
36514 for plasmapheresis
38206 Blood-derived hematopoietic stem cell harvesting; autologous1
APC 0111 (blood
product exchange)
Medicare (Hospital Outpatients): 2013 Plasma/Cellular Apheresis Payment
$9512
(U.S. average)
1Allogeneic blood-derived hematopoietic stem cell harvesting is not covered by Medicare under the hospital outpatient prospective payment system (OPPS)
2Medicare payment rate varies by locality: e.g. about $1,140 in Manhattan; $870 in Pittsburgh
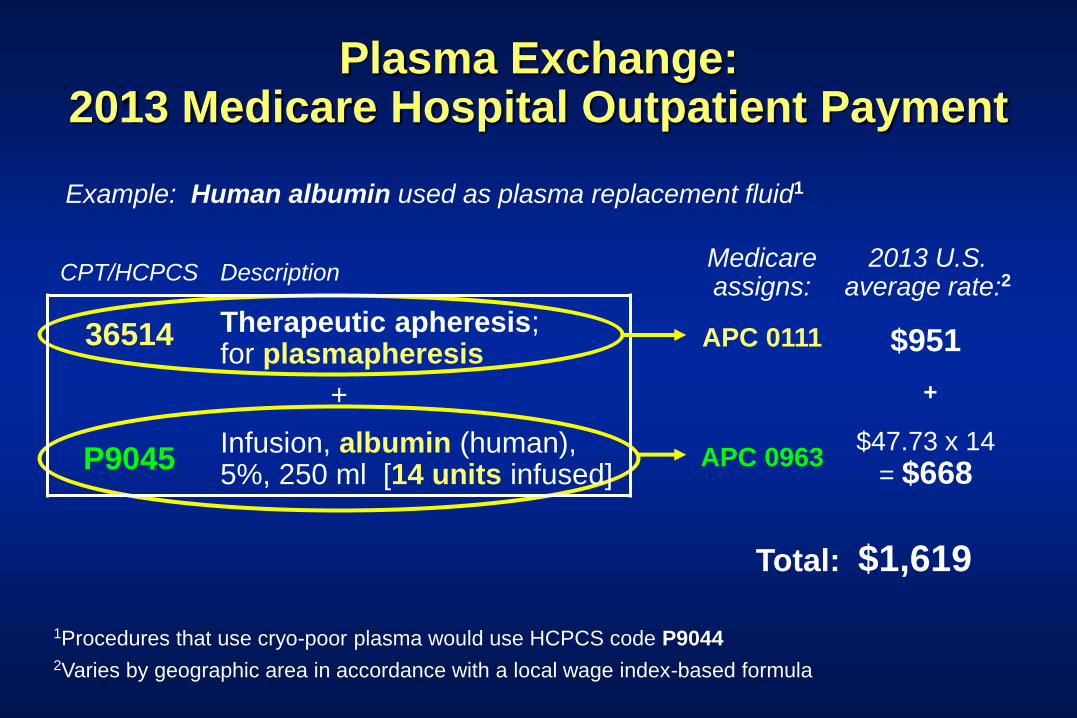
Plasma Exchange: 2013 Medicare Hospital Outpatient Payment
CPT/HCPCS Description
36514 Therapeutic apheresis; for plasmapheresis
+
P9045 Infusion, albumin (human), 5%, 250 ml [14 units infused]
Example: Human albumin used as plasma replacement fluid1
Medicare assigns:
2013 U.S. average rate:2
APC 0111 $951
APC 0963 $47.73 x 14
= $668
1Procedures that use cryo-poor plasma would use HCPCS code P9044 2Varies by geographic area in accordance with a local wage index-based formula
Total: $1,619
+
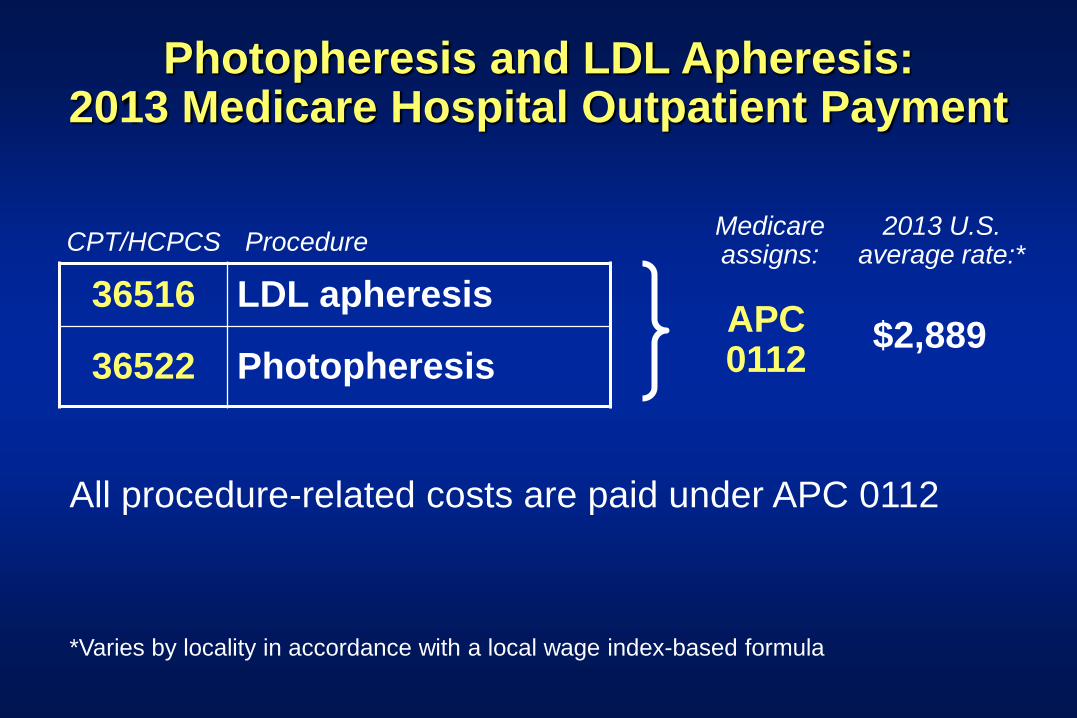
Photopheresis and LDL Apheresis: 2013 Medicare Hospital Outpatient Payment
CPT/HCPCS Procedure Medicare assigns:
2013 U.S. average rate:*
APC 0112
$2,889
*Varies by locality in accordance with a local wage index-based formula
36516 LDL apheresis
36522 Photopheresis
All procedure-related costs are paid under APC 0112
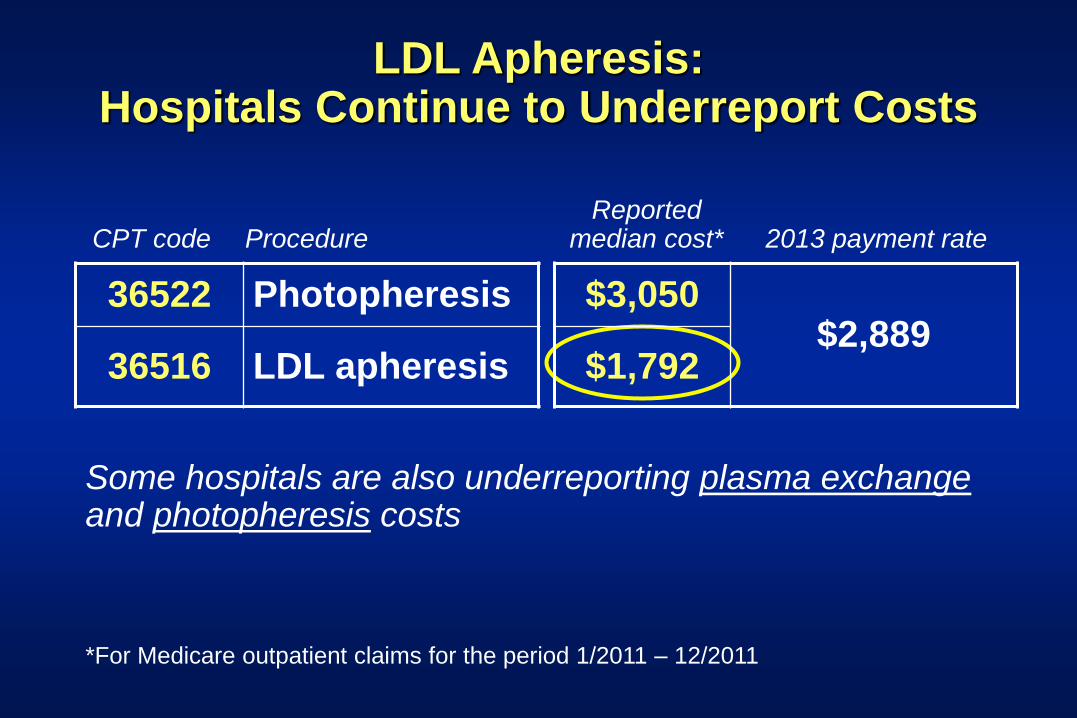
LDL Apheresis: Hospitals Continue to Underreport Costs
*For Medicare outpatient claims for the period 1/2011 – 12/2011
36522 Photopheresis
36516 LDL apheresis
$3,050 $2,889
$1,792
CPT code
Procedure
Reported median cost*
2013 payment rate
Some hospitals are also underreporting plasma exchange and photopheresis costs
Outpatient Apheresis: Commercial Insurers May Require Preauthorization
• Necessary documentation may include:
Detailed patient history
Examination findings
Treatment records
Laboratory records
Published evidence of clinical benefit
• Scope of coverage – the covered time period or number
of treatments – can vary by insurer
The Coverage Appeals Process: Get What the Patient Needs; Educate the Insurer
• Insurer coverage policies often lag behind or miss recent
published evidence in the clinical literature
• Don’t give up when an insurer denies coverage:
Ask for review on an individual consideration basis
Provide available published studies to document efficacy
As applicable, document failures with other treatment options
• Current examples:
Plasma exchange for treatment of NMO, relapsing MS
LDL apheresis for very high LP(a)
Photopheresis for drug-refractory post-lung transplant BOS

Medicare Hospital Inpatient Billing and Payment:
Ambulatory Payment Classifications (APCs)
Medicare Payment for Hospital Inpatients: All-Inclusive “MS-DRGs”
• 745 MS-DRGs (Medicare Severity-Adjusted Diagnosis-Related Groups)
• Presence of (1) complications and comorbidities (CCs), (2) major CCs or (3) no CCs can now dictate up to three MS-DRGs with differing payment rates
• Defining MS-DRGs with CCs and MCCs helps Medicare reimbursement on average better approximate actual costs of hospitalization
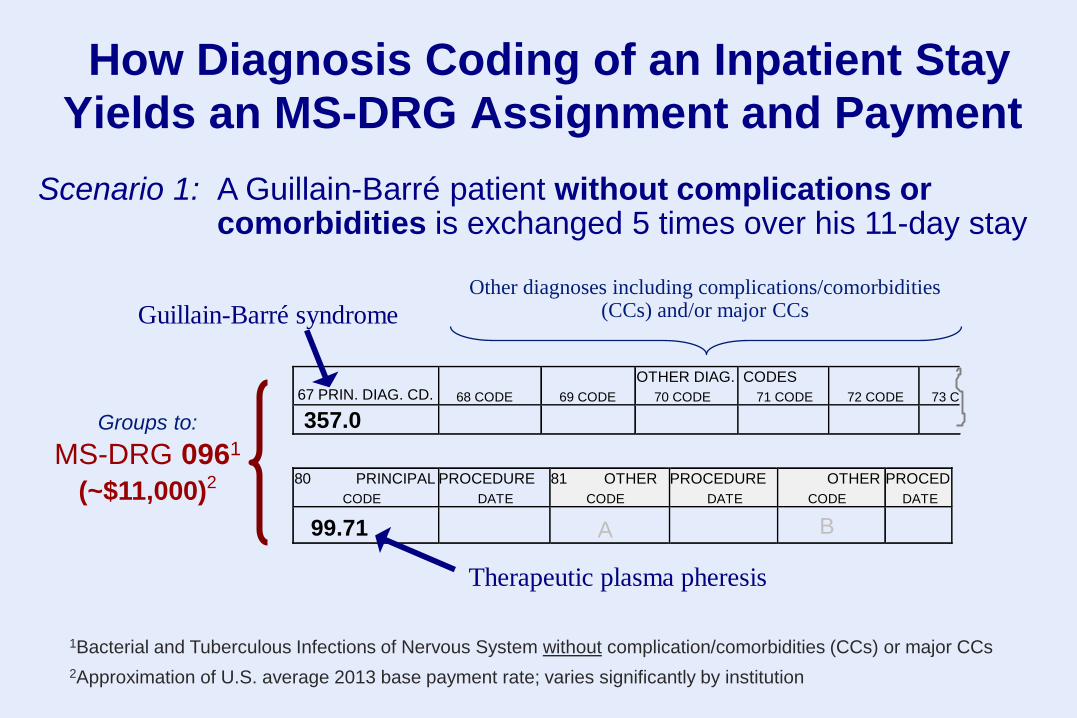
How Diagnosis Coding of an Inpatient Stay
Yields an MS-DRG Assignment and Payment
67 PRIN. DIAG. CD.
68 CODE
69 CODE
OTHER DIAG.
70 CODE
CODES
71 CODE
72 CODE
73 C
357.0
80 PRINCIPAL
CODE
PROCEDURE
DATE
81 OTHER
CODE
PROCEDURE
DATE
OTHER
CODE
PROCED
DATE
99.71
A
B
Guillain-Barré syndrome
Therapeutic plasma pheresis
Groups to:
MS-DRG 0961
(~$11,000)2
Scenario 1: A Guillain-Barré patient without complications or comorbidities is exchanged 5 times over his 11-day stay
1Bacterial and Tuberculous Infections of Nervous System without complication/comorbidities (CCs) or major CCs
2Approximation of U.S. average 2013 base payment rate; varies significantly by institution
Other diagnoses including complications/comorbidities (CCs) and/or major CCs

How Diagnosis Coding of an Inpatient Stay
Yields an MS-DRG Assignment and Payment
67 PRIN. DIAG. CD.
68 CODE
69 CODE
OTHER DIAG.
70 CODE
CODES
71 CODE
72 CODE
73 C
357.0 481
80 PRINCIPAL
CODE
PROCEDURE
DATE
81 OTHER
CODE
PROCEDURE
DATE
OTHER
CODE
PROCED
DATE
99.71
A
B
Guillain-Barré syndrome
Therapeutic plasma pheresis
Pneumococcal pneumonia
Scenario 2: A Guillain-Barré patient with pneumococcal pneumonia is exchanged 5 times over his 19-day stay
Groups to:
MS-DRG 0941
(~$19,250)2
1Bacterial and Tuberculous Infections of Nervous System with major complication/comorbidities
2Approximation of U.S. average 2013 base payment rate; varies significantly by institution

Hospital Inpatients: Apheresis and Drug Costs Are NOT Separately Reimbursed
• Fixed prospective payment (MS-DRGs, per diems) creates a powerful incentive to minimize costs
• This has generated interest in plasma exchange as a less costly alternative to IVIG in neurological disorders where shown similarly effective, e.g.:
Guillain-Barré syndrome
Moderate-severe MG with worsening weakness
Physician Billing for Apheresis Procedure
Supervision
(professional fee)
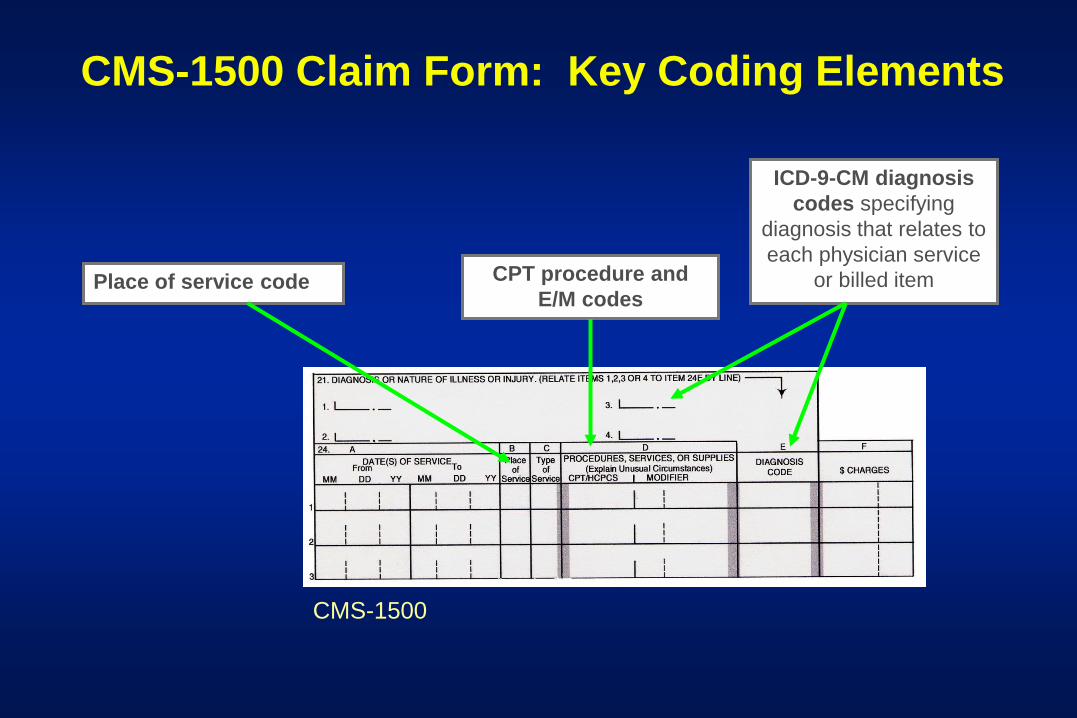
CPT procedure and
E/M codes
ICD-9-CM diagnosis
codes specifying
diagnosis that relates to
each physician service
or billed item Place of service code
CMS-1500 Claim Form: Key Coding Elements
CMS-1500

Correct Coding of “Place of Service” on the Apheresis Supervision Claim
Hospital outpatient: use “22”
Hospital inpatient: use “21”
Office-based procedure: use “11”
CMS-1500

CPT Procedure Codes for Apheresis Billing
CPT Description
36511 Therapeutic apheresis; for white blood cells
36512 for red blood cells
36513 for platelets
36514 for plasmapheresis
36515 with extracorporeal immunoadsorption/plasma reinfusion*
36516 with extracorporeal selective adsorption/filtration + plasma reinfusion (LDL apheresis)
36522 Photopheresis, extracorporeal

CPT Codes for Blood-Derived Stem Cell Harvesting
CPT Description
38205 Blood-derived hematopoietic progenitor cell
harvesting for transplantation; allogeneic
38206 autologous
The physician claim for supervision of stem cell harvesting should
identify the specific diagnosis (e.g. leukemia, lymphoma, aplastic
anemia) for which the planned transplantation procedure is
intended.
NOTE: Medicare pays for cytapheresis and stem cell harvesting
procedures in the hospital setting only
Apheresis Supervision: General Billing Principles
The physician:
Bills the CPT code applicable for that procedure
(e.g. CPT 36514 for plasma exchange)
Bills the professional fee for each date he/she
supervises an apheresis procedure
To bill an apheresis professional fee, the physician
must examine the patient and must be [immediately]
available during the procedure.*
*Gajewski JL, Simmons A, Weinstein R et al. Biol Blood Marrow Transplant 2005 Nov; 11(11):871-80.

Apheresis Supervision: More General Billing Principles
The physician should prepare a procedure note
documenting his/her services (consistent with the
institution’s standards)
Evaluation & management (E/M) codes should not be
used to bill for supervision of apheresis procedures.

Documenting the Apheresis Supervision
The physician is responsible for documenting supervision of the procedure in the patient record according to the institution’s standards.*
The procedure note should document that the physician:1
*ASFA Guidelines for Documentation of Therapeutic Apheresis Procedures in the Medical Record by Apheresis Physicians (www . apheresis.org)
1. Reviewed/evaluated clinical and lab data relevant to the treatment of the patient that day.
2. Made the decision to perform the procedure on that day.
3. Saw and evaluated the patient for the procedure.
4. Remained available throughout the duration of the procedure to respond in person to emergencies and other situations requiring his/her presence.

Understanding & Complying with Medicare’s “Direct, Personal Supervision” Requirement

Medicare Therapeutic Apheresis Coverage Policy Re: The Physician’s Role
A physician…is present to perform medical services and
to respond to medical emergencies at all times during
patient care hours;
Each patient is under the care of a physician; and
All nonphysician services are furnished under the
direct, personal supervision of a physician.
*Medicare National Coverage Determinations Manual, Chapter 1, Part 2, Section 110.14 (Apheresis [Therapeutic Pheresis]), effective 7/30/1992.
“Apheresis is covered…when the following conditions
are met:*

Clarifying Medicare’s “Direct, Personal Supervision” Requirement
2010: ASFA asks CMS to clarify the meaning of this term
CMS responds: “The intent of ‘direct, personal’…means
literally the regulatory definition of ‘direct’ supervision”1
“Direct supervision” defined by CMS for Medicare coverage:
“As of 1/1/2011, “direct supervision means that the
physician…must be immediately available to furnish
assistance and direction throughout the performance of the
procedure. It does not mean that the physician…must be
present in the room when the procedure is performed.”
1American Society for Apheresis. ASFA Announces the Clarification of 1992 National Medicare
Coverage Determination. Accessed at http://www.apheresis.org/apheresis_reimbursement.
242 CFR 410.27(a)(1)(iv).
Clarifying the Definition of “Immediately Available” for Medicare Apheresis Services
*Medicare Benefit Policy Manual, Chapter 6, Section 20.5.2 (Rev. 143, Effective 5/31/2011).
“Immediate availability requires the immediate physical
presence of the supervisory physician…practitioner.
CMS has not specifically defined the word ‘immediate’ in
terms of time or distance…
Examples of a lack of immediate availability would be
situations where the supervisory practitioner is
performing another procedure or service that he/she
could not interrupt, or where he/she is so physically far
away from the location where [apheresis] is being
furnished that he/he could not intervene right away...)”*
Clarifying the Definition of “Immediately Available” for Medicare Apheresis Services
“The…supervisory practitioner must judge [his/her]
relative location to ensure that he/she is immediately
available.
A supervisory practitioner may supervise from a
physician office or other nonhospital space that is not
officially part of the hospital campus where services are
being furnished as long as he/she remains immediately
available.”*
*Medicare Benefit Policy Manual, Chapter 6, Section 20.5.2 (Rev. 143, Effective 5/31/2011).

When to Bill and Not Bill Evaluation & Management
(E/M) Services
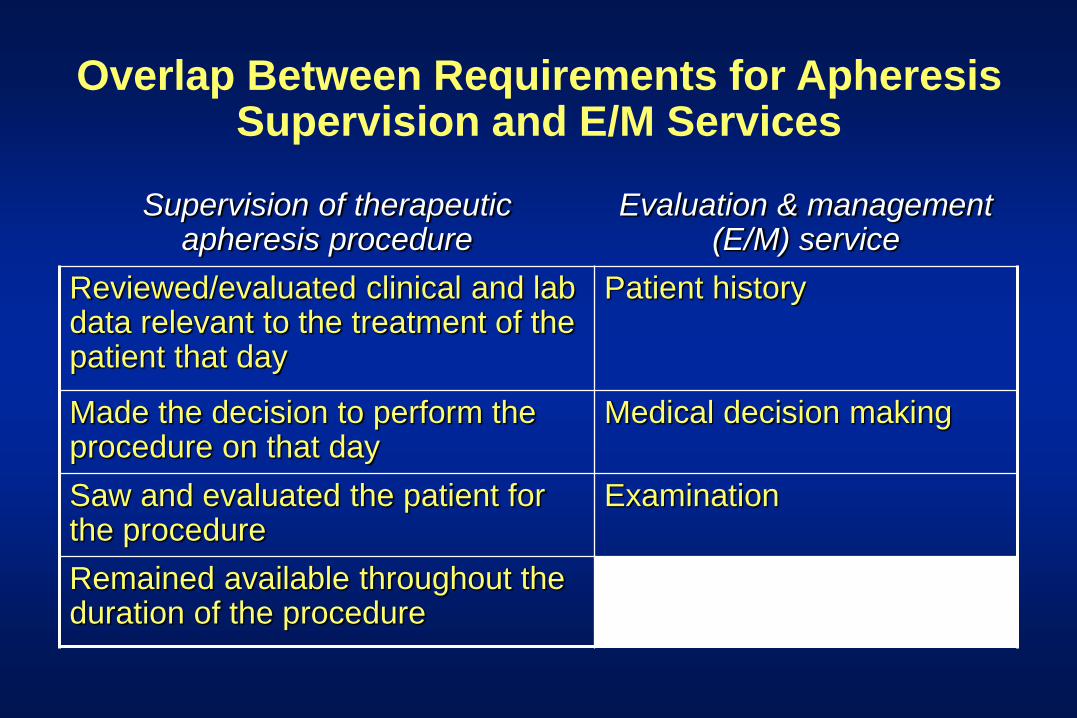
Overlap Between Requirements for Apheresis Supervision and E/M Services
Supervision of therapeutic apheresis procedure
Evaluation & management (E/M) service
Reviewed/evaluated clinical and lab data relevant to the treatment of the patient that day
Patient history
Made the decision to perform the procedure on that day
Medical decision making
Saw and evaluated the patient for the procedure
Examination
Remained available throughout the duration of the procedure

Billing the Apheresis Supervision and E/M Services on the Same Day by Same Physician
Source: AABB Billing Guide for Transfusion and Cellular Therapy Services. Edition Version 4.0 (October 2007).
Billing an E&M code in addition to an apheresis service may be appropriate only when the E&M code is a separately identifiable service that involves more than the evaluation and management portion of the apheresis service.
An E&M service must also involve a different diagnosis than the diagnosis for which the apheresis is being performed.
Add a “25” modifier* to the billed E&M code on this claim.
*Connotes a significant, separately identifiable E/M service by the same physician on the same day of the procedure.
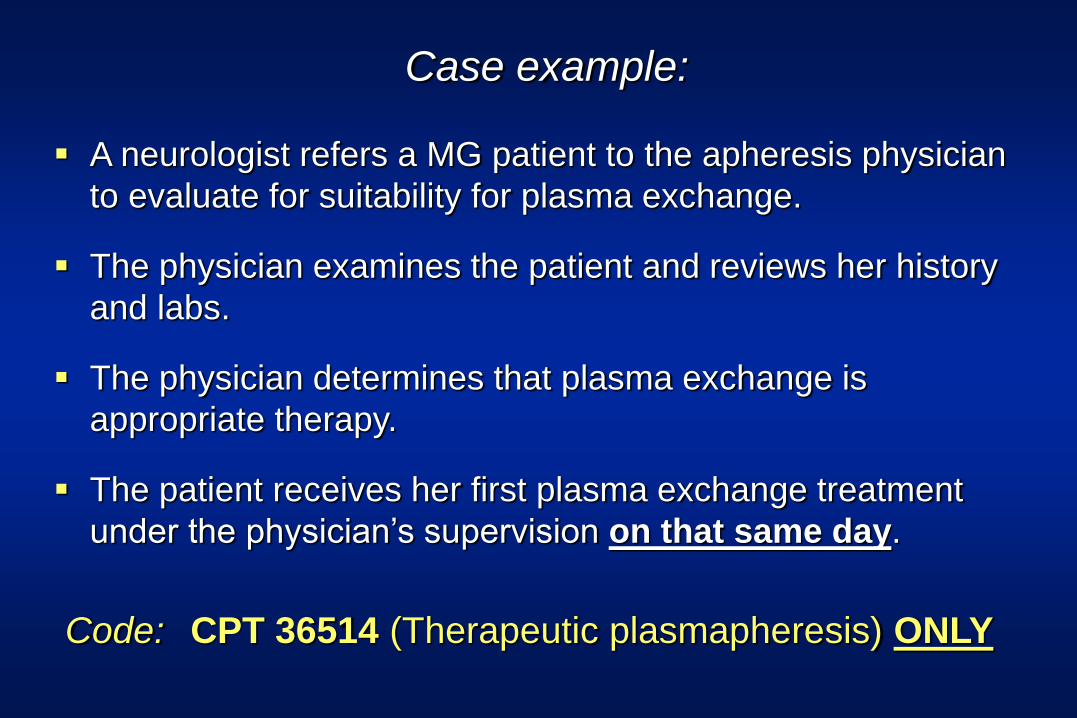
Case example:
Code: CPT 36514 (Therapeutic plasmapheresis) ONLY
A neurologist refers a MG patient to the apheresis physician
to evaluate for suitability for plasma exchange.
The physician examines the patient and reviews her history
and labs.
The physician determines that plasma exchange is
appropriate therapy.
The patient receives her first plasma exchange treatment
under the physician’s supervision on that same day.
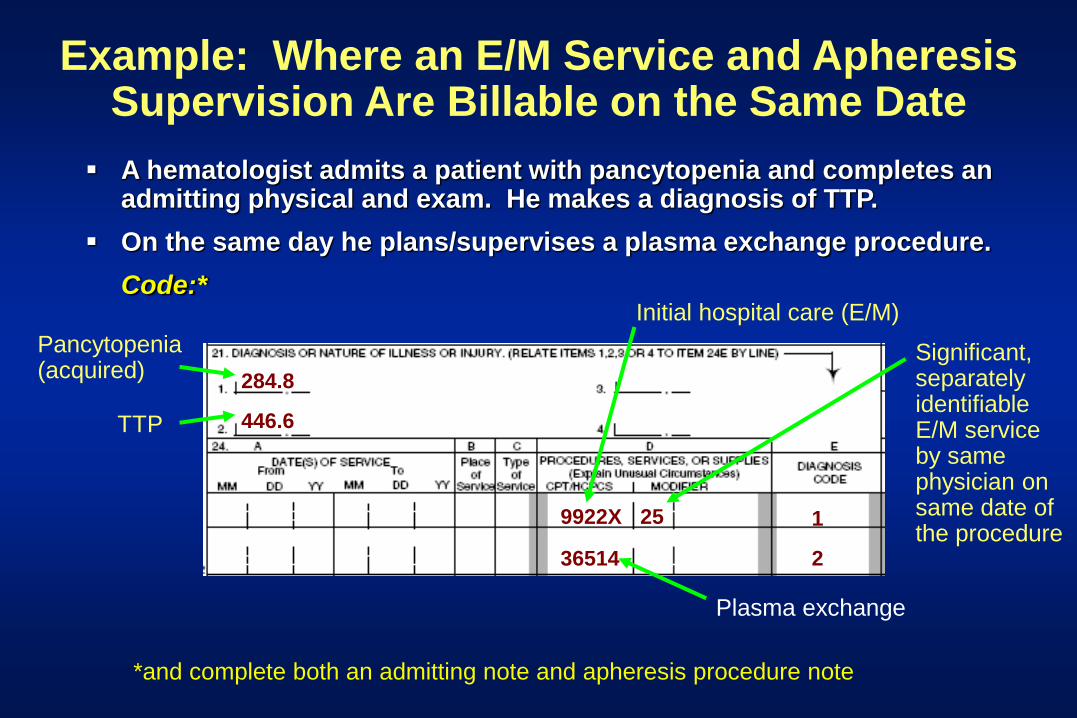
Example: Where an E/M Service and Apheresis Supervision Are Billable on the Same Date
A hematologist admits a patient with pancytopenia and completes an admitting physical and exam. He makes a diagnosis of TTP.
On the same day he plans/supervises a plasma exchange procedure.
Code:*
446.6
284.8
9922X
36514
25 1
2
Pancytopenia (acquired)
TTP
Initial hospital care (E/M)
Plasma exchange
Significant, separately identifiable E/M service by same physician on same date of the procedure
*and complete both an admitting note and apheresis procedure note


2013 Valuations for Physician Apheresis
Supervision
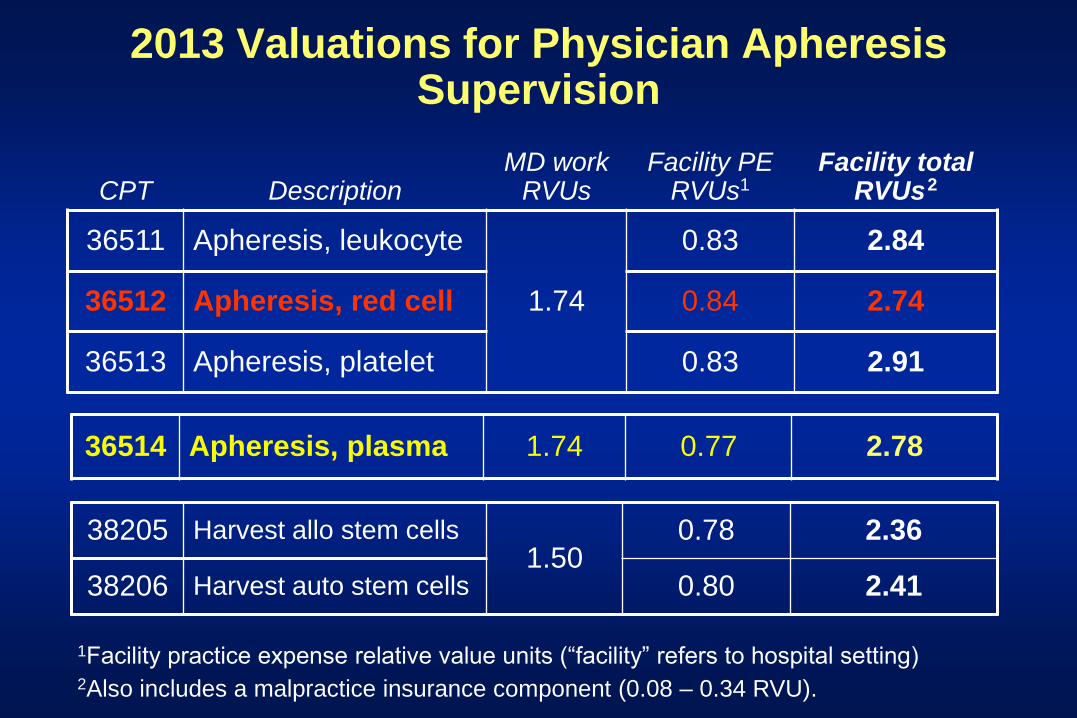
2013 Valuations for Physician Apheresis Supervision
38205 Harvest allo stem cells 1.50
0.78 2.36
38206 Harvest auto stem cells 0.80 2.41
CPT
Description
MD work RVUs
Facility PE RVUs1
Facility total RVUs
2
36511 Apheresis, leukocyte
1.74
0.83 2.84
36512 Apheresis, red cell 0.84 2.74
36513 Apheresis, platelet 0.83 2.91
1Facility practice expense relative value units (“facility” refers to hospital setting) 2Also includes a malpractice insurance component (0.08 – 0.34 RVU).
36514 Apheresis, plasma 1.74 0.77 2.78
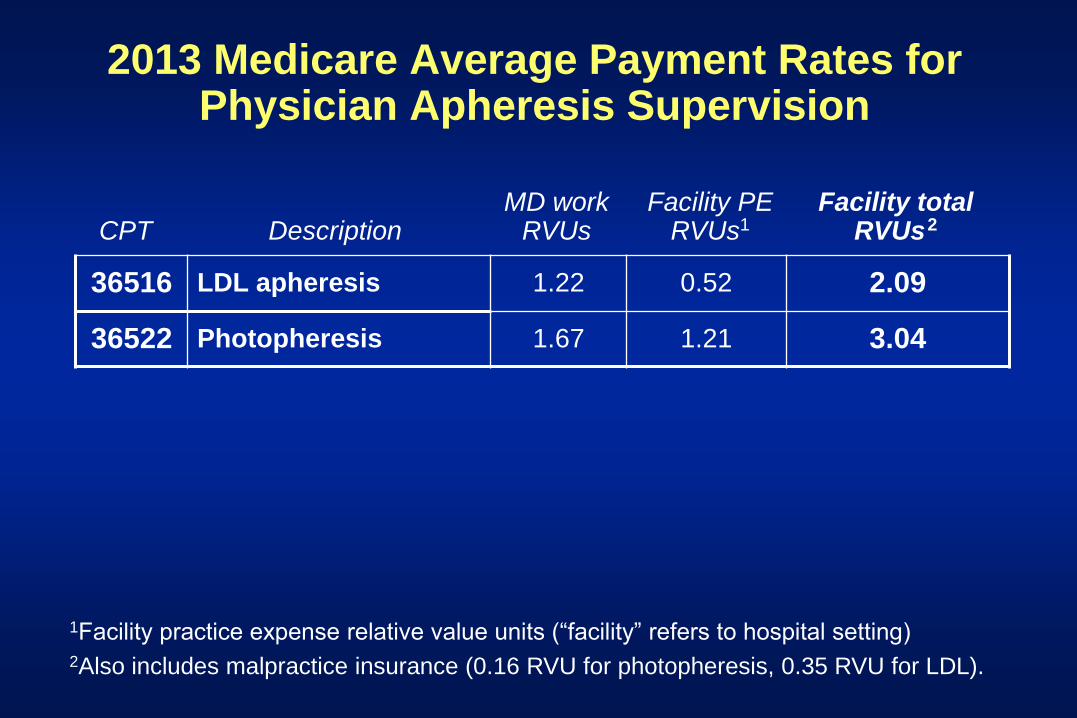
2013 Medicare Average Payment Rates for Physician Apheresis Supervision
36516 LDL apheresis 1.22 0.52 2.09
36522 Photopheresis 1.67 1.21 3.04
CPT
Description
MD work RVUs
Facility PE RVUs1
Facility total RVUs
2
1Facility practice expense relative value units (“facility” refers to hospital setting) 2Also includes malpractice insurance (0.16 RVU for photopheresis, 0.35 RVU for LDL).
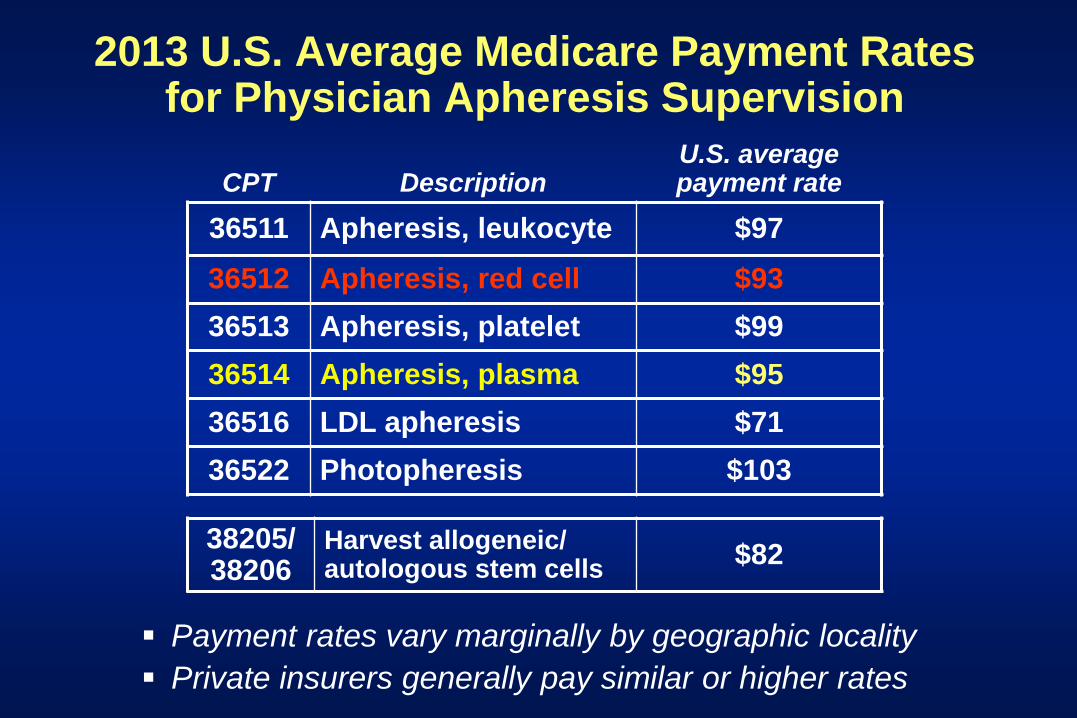
2013 U.S. Average Medicare Payment Rates for Physician Apheresis Supervision
CPT
Description
U.S. average payment rate
36511 Apheresis, leukocyte $97
36512 Apheresis, red cell $93
36513 Apheresis, platelet $99
36514 Apheresis, plasma $95
36516 LDL apheresis $71
36522 Photopheresis $103
Payment rates vary marginally by geographic locality
Private insurers generally pay similar or higher rates
38205/ 38206
Harvest allogeneic/ autologous stem cells
$82

Special Issues:
Plasma Exchange
Cytapheresis
Photopheresis
LDL Apheresis
Issue:
A number of state Medicaid
programs severely under-
reimburse hospitals for plasma
exchange and cytapheresis
procedures

Issue:
1992 Medicare National Coverage
Determination (NCD) for plasma
exchange and cytapheresis
procedures is 21 years out of date

Missing from the Current 1992-Vintage Medicare “Apheresis” National Coverage Determination:
Plasma exchange/plasmapheresis:
Missing numerous ASFA Category I and II indications
(e.g. antibody-mediated renal allograft rejection/HLA
desensitization; PANDAS; NMO; HUS; MS subtypes)
Includes improperly defined clinical uses (e.g. “acquired
myasthenia gravis;” “chronic relapsing polyneuropathy”)
Entirely missing covered uses for RBCX and platelet pheresis
Entirely missing LDL apheresis (and no separate NCD)
Issue:
Insurance coverage for LDL
apheresis still models ultra-
conservative indications for
devices licensed in the mid-1990s

LDL Apheresis: A Yawning Gap Between Insurance Coverage
Policies and Best Clinical Practice?
National Lipid Association Expert
Panel on FH:
For heterozygotes with familial hypercholesterolemia (FH) and very high risk characteristics (CHD, other CV disease, diabetes)
LDL cholesterol 160 mg/dL
Device indication and prevalent insurance coverage policies:
LDL cholesterol 200 mg/dL
Coming soon:
Extracorporeal Photopheresis (ECP):
Medicare Plans to Cover/Pay for ECP to Treat Bronchiolitis Obliterans Syndrome (BOS) in Post-Lung
Transplant Patients

Photopheresis: Medicare Coverage History
April 1988: Palliative treatment of skin manifestations
of CTCL that has not responded to other therapy.
Early 2006: Request submitted for reconsideration of
photopheresis NCD to add chronic GVHD
December 2006: Chronic GVHD refractory to standard
immunosuppressive drug treatment

August 4, 2011: CMS accepts written request for reconsideration of its NCD for ECP to add treatment for lung transplant patients who develop progressive bronchiolitis obliterans syndrome (BOS) refractory to drug treatment.
May 2, 2012: CMS posts final Decision Memo: Under its Coverage with Evidence
Development (CED) policy, CMS covers ECP for the treatment of BOS following
lung allograft transplantation only when ECP is provided under a clinical research
study that addresses one or more aspects of the following question:
Prospectively, do Medicare beneficiaries who have received lung allografts, developed BOS refractory to standard immunosuppressive therapy, and received ECP, experience improved patient-centered health outcomes as indicated by:
Improved FEV1, or decreased rate of decline of FEV1; Improved survival after transplant; and/or Improved quality of life.
September 22, 2012: Proposed registry study protocol is under review by CMS.
Photopheresis (ECP) for Post-Lung Transplant BOS: Status of Current Medicare Coverage Initiative
ECP/BOS: Proposed Registry Study Design
Multiple-center, single-arm study to evaluate the efficacy/tolerability of ECP to treat progressive BOS in adult Medicare-eligible lung allograft recipients experiencing declining FEV1 despite treatment with at least one of the following: high-dose steroid, azithromycin, anti-thymocyte globulin or sirolimus. Patients will receive 24 treatments over a 6-month period, with additional treatments thereafter at the discretion of the supervising physician. Spirometric testing data will be captured to assess a single primary endpoint: change in rate of decline in FEV1 over the 6-month period prior to initiation of ECP treatment, and over the 6- and 12-month period following initiation of ECP. Participating study sites will also report all serious adverse events believed to be directly related to ECP therapy. To document a minimum 50% reduction in the rate of decline in FEV1 versus baseline, the study will enroll a minimum of 136 patients over three years.

Questions & discussion
