anxiety understanding people who experience anxiety problems after stroke
TRANSCRIPT

AnxietyUnderstanding people who experience anxiety problems after stroke
Aims of the session• There are two sessions on anxiety. The first session
aims to introduce the topic of anxiety problems which may affect a person we are working with after a stroke.
• It sets out to describe anxiety as a normal human emotion and looks to explain how a person may feel when they feel anxious. You will learn how many people may have clinical levels of anxiety and who may benefit from help. Helpful questions and tools to measure and make sense of the anxiety are considered.
• The second session on anxiety looks at how to manage anxiety using psychological techniques.

Anxiety
• Anxiety is a normal human emotion that everyone experiences at times throughout their lives. Many people feel anxious or nervous, for example when faced with an important decision, going for a job interview or hearing a noise in the house at night. It often has to do with dealing with uncertainty or the unknown.
• Having an experience such as a stroke can be very difficult for people and their families and throws many challenges in their way. People who experience a stroke may benefit from talking through their anxiety and from receiving information and help to assist them.

Exercise: understanding the experience of someone who is feeling anxious
• It is important to understand how someone may feel when they are anxious. By being able to “step in to someone’s shoes” and understand the feelings of anxiety at that time we can begin to help them.
• Think about a time when you (or someone you know) felt anxious. What were you feeling at the time? Did you notice any changes in your body? What were you thinking? Also, how did this affect how you acted at that time?

The experience of anxiety: a framework to help• As you will have demonstrated in your example, when
people feel anxious there is a chain of feelings that they will experience.
• For most people, when anxiety is triggered they will experience a range of symptoms: they may get a rush of physical symptoms, their thoughts may change and their behaviour may change too.
• These things happen for reason; they are aimed at survival.
Starting to make sense of anxiety
• Often people worry about having physical anxiety responses, such as a faster heartbeat. This in itself might cause further anxiety.
• Explaining why our bodies and minds work in a certain way can help people understand the basics about anxiety. This can also open up conversations and give us the opportunity to help.
Explaining the basics about anxiety
• Anxiety is the response that our body produces in order to aid our survival when we feel threatened. This is a very helpful mechanism if we are in a situation where our life is threatened, such as when we are crossing the road and a car comes towards us at high speed.
• Our brain assesses situations very quickly to see if we are in danger. If it flicks the switch indicating danger, it automatically gives the signal to release hormones such as adrenaline into the bloodstream in order to maximise survival. This sets off the “fight or flight” response, preparing the body to either fight or to run away.

The basics about anxiety
• This fight/flight is an excellent response to help us in dangerous situations when we do not really have the time to think about what to do – it gets us ready for action quickly. In the case of the speeding car, this response will help us to move more quickly than usual and get us to safety.
• Unfortunately, in order for this to work quickly, the response does not discriminate between different kinds of danger. For example, our body responds in the same way when our life is threatened, when we are in hospital or when we are in an uncomfortable social situation. Some adrenaline may be helpful at these times but when our body has too many bodily symptoms we may struggle and may have to work on ways to manage the anxiety.

Biological response continued
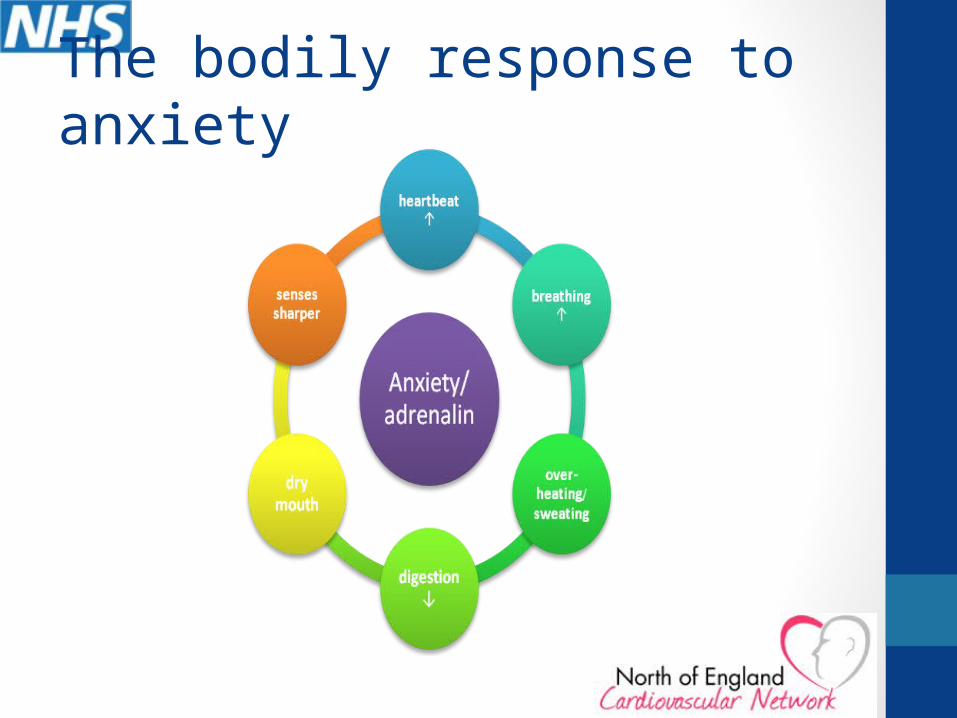
• When the body’s fight/flight response is activated people will experience symptoms such as sweating, heart rate increase, palpitations, nausea, dry mouth. This is because:
• Adrenaline causes the heart to beat faster. This helps to increase blood flow in the areas where it is most needed.
• Our breathing will increase to provide extra oxygen for the necessary energy. As our body works harder, we will feel warmer and start to sweat to cool us down.
• The mouth becomes dry, and we may notice butterflies in the tummy as the digestion slows down – the blood is being diverted to the areas where it is needed most, the muscles in arms and legs.
• Senses become sharper, and we seem to be thinking more quickly.
The bodily response to anxiety
Psychological Symptoms• In addition to the biological symptoms of anxiety, our feelings
and thoughts can change when the brain detects danger.
• When the anxiety response is triggered a person may worry
about what may happen to them, or that things will go wrong. Some people might think of a “worst case” scenario, for example that they are having a heart attack.
• Unhelpful belief systems may also come in to play when we are anxious. People who experience anxiety frequently tend to consider themselves as more vulnerable and less able to cope. They may see their future as unpredictable and their environment as rather chaotic. Such beliefs will add to the person not feeling in control, and can increase the anxiety.

The cognitive triad of anxiety

Changes in behaviour
• When people feel anxious they often change the way they behave:
• We often want to escape from a situation or wish to avoid it as we do not think we can cope with it. As we doubt our own coping, we may rely on others more, seeking “safety”.
• When a person avoids or “escapes” from a situation, or has reassurance by the presence of another (when not absolutely necessary) they will notice that the apprehension they experienced will reduce pretty quickly. While this is a relief in the short-term, this is actually unhelpful: the person does not learn that what they worried about does not happen, or that they can cope with the situation.

Anxiety disorders: in general population and after stroke
• Some people will develop “clinical levels of anxiety”. This is when the symptoms become difficult to cope with or our response to a certain situation is “excessive” or not appropriate. When anxiety interferes with a person’s day to day life, this can be called an anxiety disorder.
• Anxiety disorders are actually quite common in the general population. Mixed anxiety and depression is the most common mental health disorder in Britain, with almost 9% of people meeting criteria for diagnosis (The Office for National Statistics Psychiatric Morbidity report, 2001). This means that nearly one in ten of our patients have some sort of anxiety problem before they had their stroke.

Anxiety after stroke
• Rates for clinical anxiety symptoms following stroke have been estimated to be around 25% in the acute stage and at follow-up, although the estimates can be higher. That means at least one in four patients are anxious.
• It is important for us to identify, and help, those patients with anxiety. Stroke poses many challenges for people and if anxiety becomes a problem this will impact on a person’s rehabilitation and affect their quality of life. They may become dependent with regard to their activities of daily living and eventually have a reduced social network due to the anxiety and avoidance (Anstrom, 1996).
The many types of anxiety problems
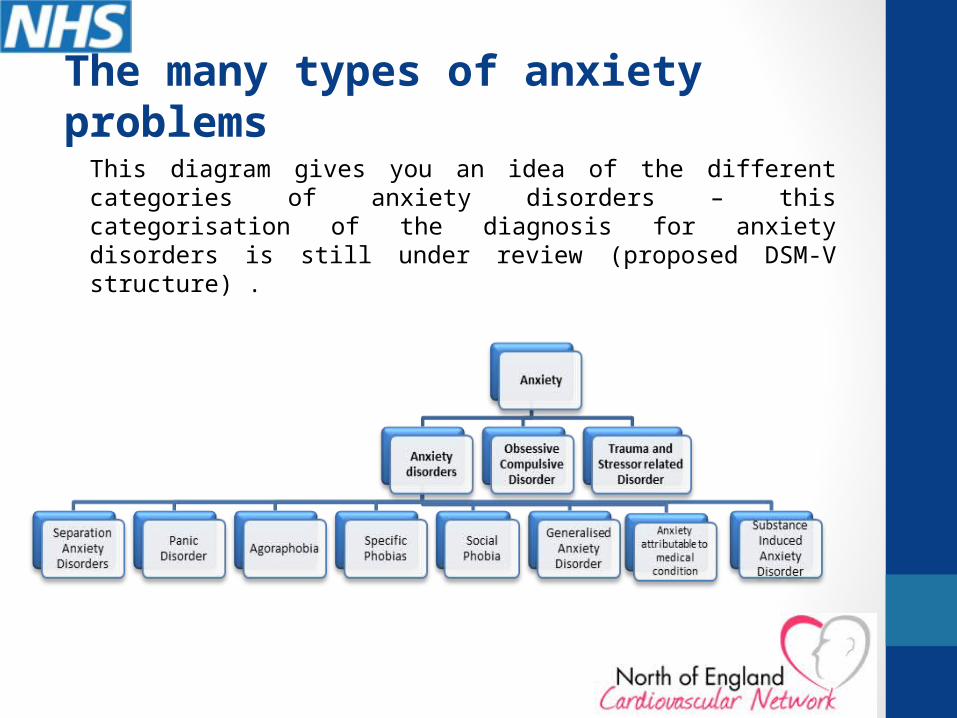
This diagram gives you an idea of the different categories of anxiety disorders – this categorisation of the diagnosis for anxiety disorders is still under review (proposed DSM-V structure) .

Helping people with anxiety
• Mostly you will be asked to help people with straight forward anxiety problems. You possibly will refer on those with other / more complex anxiety disorders.
• This is because treatment for the different anxiety problems can vary, for example treatment for panic attacks is different to treatment for obsessive compulsive problems.
• The next slide takes an example of a patient who is anxious in hospital and looks at how a nurse broaching the issue began to help her.
• Following that we look at tools (including our questions) which may help to make sense of someone’s anxiety.
Conversations about anxiety: Kate• Kate experienced a stroke whilst she was at home. She could not remember
much about the event but her family told her about it when she was in hospital. Kate had lots of worries after the stroke: worries about whether she would get better, worries about her abilities (for example her walking), worries about the stroke itself and about not remembering what had happened. She had previously been quite a private person and hated burdening others so she tried to keep her worries to herself.
• Nighttimes were bad for Kate. She felt unsettled in herself, had butterflies in her stomach and could not get off to sleep. Worrying thoughts went through her mind and she cried at times. She tried to avoid the nurses seeing her like this but one night a nurse came to her and asked if she would like to talk about how she was feeling. The nurse seemed to be able to understand how Kate may be feeling. She asked about Kate’s worries, how she was feeling in herself when she was anxious and about what might help her. The nurse suggested not keeping everything to herself and she also suggested a technique for getting off to sleep.
• The conversation helped Kate to begin to understand that anxiety was a common response after stroke and that there were ways to begin to manage it.
The Challenges after Stroke
• Clearly, for Kate, and for all people who have suffered a stroke, they face many challenges: coping with changes in the body and having to rely on others. Being in hospital and out of their usual environment is also difficult. Being separated from our family can also make us feel more vulnerable.
• Learning about the person’s stroke, and their emotional response, including anxiety reactions is important for all patients. We need to look at when their anxiety occurs and how does it feel for them and what is going through their mind to try to understand how to help.
• It is also useful to ask the person if they have been anxious prior to their stroke, and what helped them. We may also want to measure the severity of the anxiety.
• As a first point of call, ask the person how they are feeling, and what is going on for them. If the person seems a little uncomfortable, just check with them what is happening to them just now. Remember: a person who is anxious tends to feel vulnerable and often they do not think they are able to cope with a situation. Examples of questions are:
• Question them about it :“You just looked really worried. Can you tell me what went through your mind?”
• Try to get to the physical sensations: “ when you just had that thought of…..did you notice anything about your body or your feelings? Are there any times that you particularly anxious and experience these symptoms?”
• “Does anything help?” “What makes you feel better?”
Assessment & screening tools

Screening tools for anxiety?
• NICE & RCP recommend routine mood assessment which can include assessment of anxiety symptoms
• There are a number of tools that can be used which cover anxiety, for example:
• Hospital Anxiety & Depression Scale (HADS-A);• Beck Anxiety Scale (BAI);• Behavioural Outcome of Anxiety (BOA): for those who have
cognitive or communication problems.
• Check what assessments are used in your service, whether they cover anxiety of if you need to buy an assessment tool.

Screening tools
The Hospital Anxiety and Depression Scale–Anxiety (HADS-A) is validated for stroke patients. Seven of the items relate to anxiety (HAD-A) and seven relate to depression (HAD-D).
The items on the questionnaire that relate to anxiety are:• I feel tense and wound up• I get a sort of frightened feeling as if something is going to happen• Worrying thoughts go through my mind• I can sit at ease and feel relaxed• I get a sort of frightened feeling like butterflies in the stomach• I feel restless and have to be on the move• I get sudden feelings of panic
Each item on the questionnaire is scored from 0-3 and this means that a person can score between 0 and 21 for either anxiety or depression. Bjelland et al (2002) suggest if someone scores 8 or more, this indicates depression or anxiety, respectively.

A new measure to assess anxiety for those with communication problems is the Behavioural Outcomes of Anxiety (BOA), Kneebone et al, 2010. There are no norms available yet, but it is a good starting point to assess anxiety. It is completed with the primary carer. If it indicates significant anxiety, collect further information, e.g. through observation, in order to determine the cause of the anxiety.• Does he/she appear particularly tense or on edge?• Does he /she have a strained face?• Does he/she avoid activities or social engagements without good reason?• Does he/she appear fearful of falling?• Does he/she have trouble falling or staying asleep?• Is he/she jumpy or easily startled?• Is he/she restless or constantly on the move (e.g. do they pace)?• Does he/she appear to panic, or have unusual episodes of breathlessness or hyperventilation? • Is he/she easily tired?• Does he/she appear anxious?
Screening for those with Cognitive or Communication Problems
Process of using the questionnaires and results• Measuring the severity of anxiety (or type of anxiety problem)
can be used to get people talking about how they are feeling. It also helps to plan an intervention.
• Remember to use core therapeutic listening skills (warmth, genuineness and empathy) when asking a patient about their feelings. Leave sufficient time to have an honest conversation about how someone may truly be feeling. This is particularly important if we are working with someone who has communication problems and needs more time and props (e.g. pictures) to help them explain what they may be anxious about.
• The result of your assessment should be discussed with the multidisciplinary team. This will lead to an action plan to help with the anxiety.
• Reviews as to whether an intervention is working also need to be scheduled.
Observations and Information from others:
• Family members can often tell us helpful information. Is the person usually anxious? What makes them tense? Is there anything that helps them to feel calmer?
• In the case of someone with communication difficulties it is helpful to discuss possible reasons for anxiety based on observing the person.
• Also bear in mind: physical problems such as pain can lead people to be more anxious about being touched for example.
Anxiety Diaries• Diaries can also be a helpful tool to assess and monitor
when the anxiety is occurring and what is happening for the individual at particular times, often highlighting patterns of anxiety (for example are they anxious in physiotherapy, are they anxious at night time?)
Date and time
Situation
(describe where you were and who you were with)
Describe how you felt, and what was going through your mind
Describe any bodily sensations
Say what you or others tried to do to help and whether this helped.
Sunday, 8am
Bedroom, by myself, could not get out of bed
I was really anxious, thought I would wet myself
Had a dry mouth and my heart was racing
Helen gave me a hand, she reminded me how to get up

Pulling it all together: Assessment and Formulation of anxiety problems• The following section looks again at the case of Kate who is
experiencing anxiety in hospital. She has recently become more withdrawn:
• Kate, has come into the physiotherapy session. She is a little unsteady on her legs, and is notably nervous. After only 5 minutes of standing practice, she asks whether she can return to her room. She seems visibly relieved when you bring her back. Next time you come to take her to the session, she declines. You are worried that she is unable to make sufficient progress to return to independent living.
• What do you think is going on with Kate and how would you begin to assess her anxiety? Write some ideas down.

Understanding of Kate’s Problems 1
• Kate could talk about her anxiety. When asked what happened in the physio session, and if anything made her uneasy, Kate told us she noticed how wobbly she is. She said that she is afraid of falling and fracturing her hip. Her family tell us she is usually quite a laid back person.
• Kate’s problem involved her noticing a number of sensations, such as her heart racing, becoming sweaty, and her legs were starting to shake a little.
• While we know that this is a normal physiological response, that it is the effect of the adrenalin, Kate became worried about these symptoms. Her anxiety increased, and the symptoms got worse.

Understanding of Kate’s Problems 2
• Kate found a way to end her anxiety: she avoided further physiotherapy sessions. The effect was pretty immediate. The anxiety reduced, and she felt better. Unfortunately, this meant that Kate continued to hold on to the belief that she would fall if trying to stand.
• This means that avoidance was maintaining the anxiety.
• Some people may chose other behaviours to help them cope with their anxiety. They might rely on friends or family to come with them, or use a Zimmer frame even when they could manage with a stick. The effect is the same as with avoiding a situation: the person does not learn that they can cope with the situation, and therefore the anxiety is maintained.

Kate- understanding her problems
Situation
Thought
Feeling
Physical sensation
Behaviour
In the gym, being unsteady on her legs
I might fall and break my hip! The physio doesn’t look like
she could catch me…
Anxiety
Palpitations, sweating, shaky legs
Oh no, it is getting worse, I will fall for sure! ANXIETY increases!
Asking to be brought back to the room
ANXIETY decreases

How Kate was helped by the staff
• Staff engaged Kate in a discussion and helped her to express her feelings and worst fears. They learnt what helped her, and what did not, and together they started to work on the problem.
• Kate had felt “silly” about her feelings and had tried to hide her thoughts. When asked directly in a supportive way she was able to be honest.
• Good communication skills from the staff helped with the assessment. A screening measure also opened up the conversation and provided a measure as to how anxious Kate was and what her anxiety related to. It also helped Kate to see that anxiety is so common, they even had a questionnaire for it.

Summary
• Anxiety is a normal human emotion.
• When we are anxious we experience changes in our bodies, feelings (emotions), thoughts and often behaviour.
• Anxiety symptoms can be difficult for the person and can impact on rehabilitation.
• Identifying anxiety, when and where it occurs, and how severe it feels is important.
• From that we can begin to look approaches for helping.
• Approaches for helping are considered in the next presentation.