antimicrobial steward call february 11, 2019
TRANSCRIPT
Antimicrobial Steward Call February 11, 2019
Tennessee Department of Health Healthcare Associated Infections and Antimicrobial Resistance Program

Welcome

Adobe Connect Housekeeping
• All lines have been muted • Press *6 to unmute your line • Also can use the chat box to ask questions/comment

Announcements

C. auris Tabletop Exercises
• PARTICIPANTS WILL LEARN HOW TO: – Define plans for C. auris containment across the continuum of care – Access resources for response – Engage stakeholders and promote collaboration between lab scientists, epidemiologists,
healthcare facility staff and other key players – Understand how C. auris is misidentified in clinical laboratories

Containment of Candida auris
Save the Date for the 2019 Tabletop Exercise!
• Columbia - Wednesday, January 9th
• Brentwood - Thursday, January 10th
• Jackson - Wednesday, January 23rd
• Memphis - Thursday, January 24th
• Bristol - Wednesday, February 6th
• Knoxville - Thursday, February 7th, 2019
• Chattanooga - Thursday, February 21st
• Cookeville - Friday, February 22nd
Tentative Run Time: 9:00am – 2:30pm

2017 SAAR Rebaseline

Standardized Antimicrobial Administration Ration (SAAR)
• Expresses observed to predicted antibiotic use – Predicted use based on data being submitted to produce models using facility
characteristics • SAARs for different groups of antibiotics • SAARs for adult and pediatric locations • SAARs for ICU and non-ICU locations • Can be calculated at the unit or hospital wide level
SAAR Evolution
• 2014 baseline SAAR models were developed using AU Option data from: – 77 acute care hospitals (350 adult and 33 pediatric locations)
• 2017 baseline SAAR models were developed using AU Option data from:
– Adult models: 449 acute care hospitals, 2156 locations – Pediatric models 109 acute care hospitals, 170 locations
• Larger sample size enabled:
– Inclusion of new location types – Adult and pediatric patient populations modeled separately – Increased precision of estimates of predicted use

Changes from 2014 baseline
• Added SAARs for two new adult locations: stepdown and oncology • Added SAAR for antifungals • Added SAAR for agents posing high risk for CDI • Added azithromycin SAAR for pediatrics • Added rate distribution for agents commonly used to treat highly
resistant pathogens

Adult SAARs

Pediatric SAARs

New Antimicrobial Therapies

Whitney J. Nesbitt, PharmD, BCPS, BCIDP Antimicrobial Stewardship Clinical Specialist
Vanderbilt University Medical Center
When Bugs Go Bad: Antimicrobial Stewardship Practices for Multidrug-
Resistant Gram-Negatives

• None
DISCLOSURES

OBJECTIVES
• Identify the newer antibiotics able to treat multidrug-resistant gram-negative pathogens
• Determine potential applications of the recently introduced antibiotics
• Discuss stewardship principles applied to antibiotic selection

Antimicrobial Resistance
CDC Threat Report 2013 > 2 million illnesses
23,000 deaths Urgent threat level
Carbapenem-resistant Enterobacteriaceae (CRE) Serious threat level
Multidrug-resistant (MDR) Acinetobacter Extended spectrum β-lactamase (ESBL) producing
Enterobacteriaceae MDR P. aeruginosa
Attributable Costs Excess direct healthcare costs up to $20
billion Loss of productivity up to $35 billion per year Leading cause of death by 2050
ANTIBIOTIC RESISTANCE THREATS, UNITED STATES 2013
CDC. Antimicrobial resistance threats in the US, 2013.

CAUSATIVE PATHOGENS IN HEALTHCARE-ASSOCIATED INFECTIONS
NEJM 2014;370:1198-208.
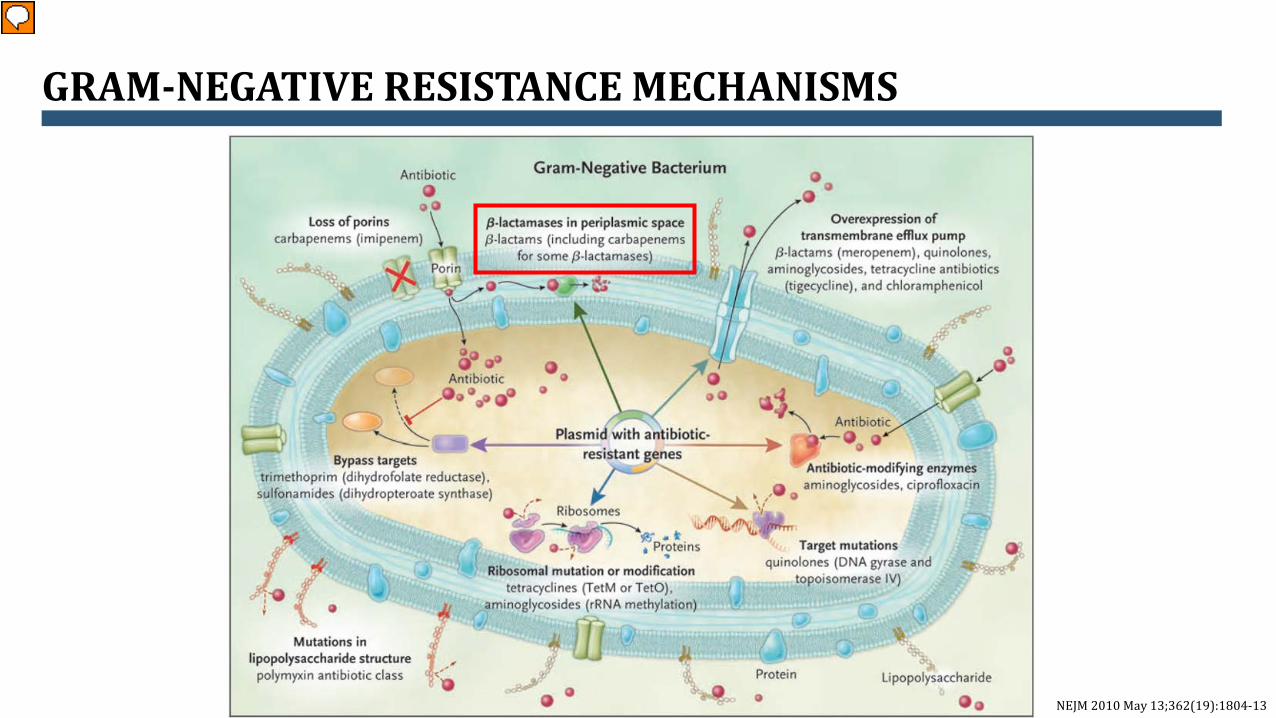
GRAM-NEGATIVE RESISTANCE MECHANISMS
NEJM 2010 May 13;362(19):1804-13

• >1000 β-Lactamases described • Increasing prevalence
ΒETA-LACTAMASES
Antimicrob Agents Chemother 2010:969. http://www.lahey.org/Studies/
Ambler Class Mechanism Enzyme Substrates
A (ESBL, carbapenemases)
Serine residue at active site
TEM-1 TEM-2 SHV-1 CTX-M KPC-2
Penicillins, cephalosporins, +/- carbapenems
B Zinc cofactor (metallo-enzyme)
IMP-1 VIM-1 NDM-1
Most beta-lactams, including carbapenems
C (amp-C)
Serine AmpC CMY-2 ACT-1
Cephalosporins
D (OXA) oxacillinases
Serine OXA-1 OXA-10 OXA-48
Pencillins, cephalosporins, carbapenems

Antibiotic Enterobacteriaceae CR
P. aeruginosa
CR Acinetobacter
spp. ESBLs
AmpC KPC NDM-1 OXA-48 TEM SHV CTX-M
Ceftolozane-tazobactam
Partial Partial Partial Variable None None None Yes None
Ceftazidime- avibactam
Yes Yes Yes Yes Yes None Yes Variable None
Meropenem-vaborbactam
Yes Yes Yes Yes Yes None None
None None
Plazomicin Yes Yes Yes Yes Yes None Yes Variable Variable
MDR GRAM-NEGATIVE TREATMENT
Intl J Infect Dis 2017; 62:39. Clin Infect Dis 2018; 68:519.
CR = Carbapenem-resistant

EXTENDED SPECTRUM BETA-LACTAMASE (ESBL)

ESBL TREATMENT
• Resistant to: • Penicillins • 3rd generation cephalosporins • Monobactam (aztreonam)
• When susceptibilities are known • Fluoroquinolones due to different resistance mechanisms • Cefepime has mixed data
• Higher treatment failures when MIC >2
Antimicrob Agents Chemother 2016; epub Clin Infect Dis 2013:488-95. Antimicrob Agents Chemother 2015: 7558-63 J Agents Chemother 2014:871-880 Lancet Infect Dis 2015:475-85 OFID 2016, 20;3(3) OFID. 2017. 4(2):ofx099

PIPERACILLIN-TAZOBACTAM FOR TREATMENT OF ESBLS • MIC matters for site of infection
• Piperacillin-tazobactam versus meropenem for treatment of ESBL-producers (MERINO Trial) • Mortality at 30 days
• 12.3% piperacillin-tazobactam versus 3.7% meropenem (p=0.002)
Clin Infect Dis 2012;15:167-74.
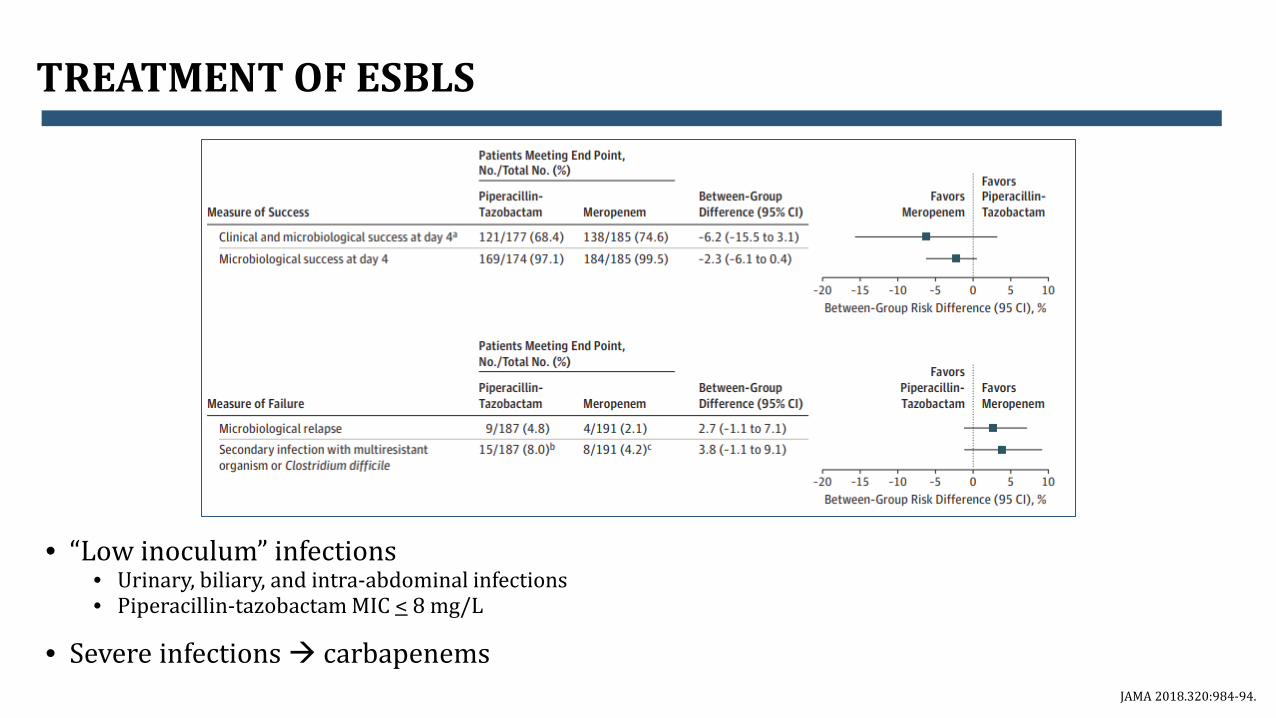
TREATMENT OF ESBLS
• “Low inoculum” infections • Urinary, biliary, and intra-abdominal infections • Piperacillin-tazobactam MIC < 8 mg/L
• Severe infections carbapenems JAMA 2018.320:984-94.
CARBAPENEM-RESISTANT ENTEROBACTERIACEAE (CRE)

• Aminoglycosides • Bactericidal • Nephrotoxicity, ototoxicity • Worse outcomes with monotherapy
• Tigecycline
• Bacteriostatic • Large volume of distribution poor for bacteremia (and maybe pneumonia)
• Polymixins (colistimethate, polymixin B)
• Nephrotoxicity, neurotoxicity, hepatotoxicity • Multiple formulations dose confusion/potential for error
• Combination therapy with polymixin + carbapenem
CRE TREATMENT HISTORY
Diagn Microbiol Infect Dis. 2013 February ; 75(2): 115–120.

• 89% isolates resistant to meropenem with MIC ≥ 4
• 30-day mortality • Monotherapy 54.3% • Combination 34.1% P=0.02
COMBINATION THERAPY FOR CRE

CEFTAZIDIME-AVIBACTAM
• Avibactam • First non beta-lactam beta-
lactamase inhibitor • Inhibits class A and C ESBLs (some D)
• Greater activity against KPC and ampC than others
• No activity against class B (MBL)
• Avibactam reduces MIC against Enterobacteriaceae 4-1024 fold
• 4-fold against Pseudomonas
• Lacks adequate anaerobic coverage
Drugs 2013; 73:159.

CEFTAZIDIME-AVIBACTAM VERSUS BEST AVAILABLE THERAPY
Lancet Infect Dis 2016; 16: 661–73
REPRISE
• Complicated intra-abdominal infections and UTIs
• Pathogens − Enterobacteriaceae (94%) − Pseudomonas (7%)
• Median treatment duration: 10 days
• No difference in clinical cure at TOC
visit: 91% vs. 91%

CEFTAZIDIME-AVIBACTAM VERSUS BEST AVAILABLE THERAPY FOR CRE K. PNEUMONIAE BACTEREMIA
Antimicrob Agents Chemother 2017; 61:e00883-17

CEFTAZIDIME-AVIBACTAM VERSUS CEFTOLOZANE-TAZOBACTAM FOR MULTIDRUG-RESISTANT GRAM-NEGATIVES
• Comparison of activity against 120 MDR bacterial strains
Int J Infect Dis. 2017; 62: 39–43
96.5
10
97 100
45
94
0
10
20
30
40
50
60
70
80
90
100
ESBL (n=29) CRE (n=60) Pseudomonas (n=31)
Sens
itivi
ty (%
)
C/TC/A
P=0.00002
CEFTAZIDIME-AVIBACTAM SUMMARY
• Potent activity against CRE • Avibactam reduces MIC 4-1024 fold in
Enterobacteriaceae • ESBL class A, C, D • Better outcomes than best available
therapy
• Not active against metallo-beta-lactamases
• Class B ESBLs: NDM, IMP, VIM
• Need metronidazole to cover anaerobes

• First in class, cyclic boronic acid beta-lactamase inhibitor • Lacks in vitro antibacterial activity • Potent inhibitor of:
• Class A (KPC, CTX-M, SHV, TEM) • Class C (P99, MIR, FOX)
• Most effective in inhibiting KPC when combined with meropenem
MEROPENEM-VABORBACTAM
Antimicrob Agents Chemother. 2017 Oct 24;61(11). Antimicrob Agents Chemother. 2016 Aug 22;60(9):5454-8

MEROPENEM-VABORBACTAM AND KPC ENTEROBACTERIACEAE
Antimicrob Agents Chemother. 2016 Aug 22;60(9):5454-8 Antimicrob Agents Chemother. 2017 Dec 21;62(1)

MEROPENEM-VABORBACTAM VERSUS BEST AVAILABLE THERAPY
TANGO-II
M/V BAT HAP/VAP or bacteremia
All-cause mortality 4/16(25%)
4/9 (44.4%)
Bacteremia EOT Overall Success 6/12
(50%) 3/8
(37.5%) TOC Overall Success 6/12
(50%) 2/8
(25%) cUTI/AP
EOT Overall Success 8/11 (73%)
2/4 (50%)
TOC Overall Success 3/7 (43%)
2/4 (50%)
Infect Dis Ther 2018; 7:439–455

MEROPENEM-VABORBACTAM SUMMARY
• First in class carbapenem + BLI with novel MOA
• Potent activity against CRE with significant reduction of meropenem MIC
• ESBL Class A, C
• Not active against metallo-beta-lactamases
• Class B ESBLs: NDM, IMP, VIM
• Given over 3 hours every 8 hours and renal dosing

• Semisynthetic aminoglycoside derived from sisomicin
• Aminoglycoside modifying enzymes (AMEs) can exist concurrently with carbapenemases
• Plazomicin not inhibited by most AMEs
PLAZOMICIN

CARE STUDY

PLAZOMICIN SUMMARY
• Not inhibited by most AMEs
• Did not receiving FDA approval for treatment of bacteremia
• Synergy with meropenem

Omadacycline • FDA approved for ABSSSI and
and CABP • More active than doxycycline and
minocycline against Enterobacteriaceae and Acinetobacter
• Less active against ESBL and CRE-producing Enterobacteriaceae
Ervacycline • Also classified as a fluorocycline
• FDA approved for complicated
intra-abdominal infections • Did not gain approval for UTIs
• Improved activity against
carbapenem-resistant Acinetobacter and Stenotrophomonas
NEWLY APPROVED TETRACYCLINES
New Engl J Med 2019;380:588.

MDR PSEUDOMONAS

• Plethora of resistance mechanisms
PSEUDOMONAS RESISTANCE
CID. 2002;34(5),: 634–640

THE RISE OF MDR PSEUDOMONAS
Clin Microbiol Rev. 2009 Oct; 22(4): 582–610
• Aminoglycosides • Bactericidal • Nephrotoxicity, ototoxicity • Worse outcomes with monotherapy
• Polymixins (colistimethate, polymixin B)
• Nephrotoxicity, neurotoxicity, hepatotoxicity • Multiple formulations dose confusion/potential for error
• Combination therapy with polymixin + carbapenem
PSEUDOMONAL TREATMENT HISTORY
Diagn Microbiol Infect Dis. 2013 February ; 75(2): 115–120.

• Potent anti-pseudomonal activity • Improved outer membrane permeability and stability against ampCs • Retains activity against Pseudomonas with efflux pump upregulation or loss of
OMP
• Enterobacteriaceae coverage similar to 3rd generation cephalosporins
• Lacks some coverage against • ESBL • Meropenem-resistant
• No metallo-beta-lactamase
CEFTOLOZANE-TAZOBACTAM
Antimicrob Agents Chemother. 2010 Sep;54(9):3933-7 Antimicrob Agents Chemother. 2007 Mar;51(3):826-30

CEFTAZIDIME-AVIBACTAM VERSUS CEFTOLOZANE-TAZOBACTAM FOR MULTIDRUG-RESISTANT GRAM-NEGATIVES
• Comparison of activity against 120 MDR bacterial strains
Int J Infect Dis. 2017; 62: 39–43
96.5
10
97 100
45
94
0
10
20
30
40
50
60
70
80
90
100
ESBL (n=29) CRE (n=60) Pseudomonas (n=31)
Sens
itivi
ty (%
)
C/TC/A

• 290 Pseudomonas isolates resistant to meropenem
• MIC at breakpoint: • 9% Ceftolozane-tazobactam • 30% Ceftazidime-avibactam • P > 0.0001
CEFTOLOZANE-TAZOBACTAM VERSUS CEFTAZIDIME-AVIBACTAM FOR PSEUDOMONAS
Beta-lactam susceptibility profile Cefepime 42%
Ceftazidime 46
Piperacillin-tazobactam 36%
Aztreonam 37%
Ceftolozane-tazobactam 91%
Ceftazidime-avibactam 81%
Antimicrob Agents Chemother 61:e00875-17.

• Ceftolozane-tazobactam • Increased activity
• Ceftazidime-avibactam
• May not be much benefit in Pseudomonal infections (MIC reduction only 4-fold) when compared to ceftolozane-tazobactam
• Meropenem-vaborbactam • Unclear benefit over ceftolozane-tazobatam
• Plazomicin
• Variable activity
SUMMARY OF PSEUDOMONAL THERAPIES
49

• Fosfomycin IV • Higher rates of cure and eradication compared to piperacillin-tazobactam
• ESBLs, aminoglycoside –resistant, and carbapenem-resistant Enterobacteriaceae, Pseudomonas, and Acinetobacter
• Cefiderocol
• “Trojan horse” mimicking natural siderophore iron complexes • Broad spectrum activity against MDR gram-negatives • Phase III trials for treatment of carbapenem-resistant gram-negatives underway
• Imipenem/cilastatin-relebactam
• Overcomes Pseudomonal resistance due to porin loss and ampC overexpression • Enterobacteriaceae activity (ESBLs, KPCs, and ampCs)
EMERGING ANTIBIOTICS
• Institutional pathogen prevalence and rates of resistance
• Causes of infection
• Formulary needs
• Creation of pathogen-specific algorithms
ANTIMICROBIAL STEWARDSHIP EVALUATION

REGIONAL CRE PREVALENCE
Antimicrob Agents Chemother. 2017 Jul 25;61(8)

REGIONAL CRE PREVALENCE
NE Central ICU Klebsiella: 12% CRE SE Central (TN) non-ICU E.coli: 0.2%
Take home: Need local data (hospital/unit>regional>national)
Account for patient population (ICU vs not), infection type (HAP vs other) Need decision support tools/risk stratification
Antimicrob Agents Chemother. 2017 Jul 25;61(8)
• Institutional pathogen prevalence and rates of resistance
• Causes of infection
• Formulary needs
• Creation of pathogen-specific algorithms
ANTIMICROBIAL STEWARDSHIP EVALUATION

Whitney J. Nesbitt, PharmD, BCPS, BCIDP Antimicrobial Stewardship Clinical Specialist
Vanderbilt University Medical Center
When Bugs Go Bad: Antimicrobial Stewardship Practices for Multidrug-
Resistant Gram-Negatives

Final Announcements
• TDH AU PP Survey • Q4 2018 Packets are complete and ready to be disseminated
• Next Call
• April 9 at 2pm Eastern/1pm Central Time • Effects of Data Suppression for Antibiotic Susceptibility Testing
• Opportunities for involvement
• Speaker or Topic for future call • Antibiotic Use Reporting into NHSN and TDH AU Point Prevalence Survey
• Feedback always appreciated