antihyperlipidemic agents.ppt
DESCRIPTION
antihyperlipidemic agentsTRANSCRIPT
Antihyperlipidemic Agents

Triglycerides and cholesterol
• essential constituents of the organism
• Triglycerides – – a form of energy store
Triglycerides and cholesterol
• Cholesterol – essential component of mammalian cell
membranes – for proper membrane permeability and fluidity
– important precursor molecule for the biosynthesis of bile acids, steroid hormones, and several fat-soluble vitamins
Triglycerides and cholesterol
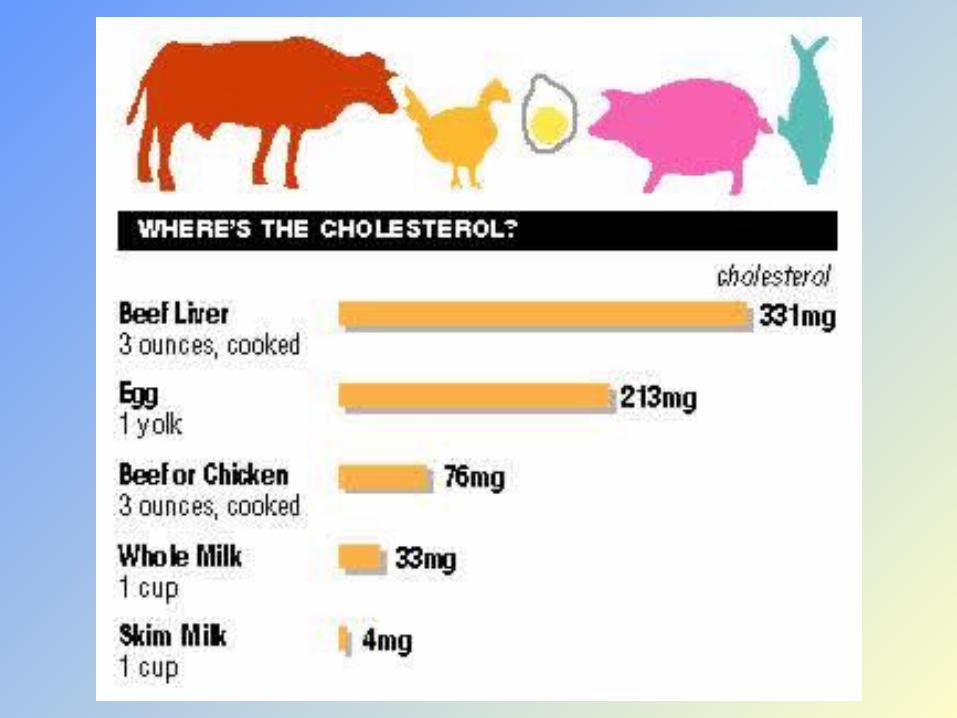
• Cholesterol – major dietary sources: cheese, egg yolks,
beef, pork, poultry, and shrimp• total fat intake, especially saturated fat and
trans fat, plays a larger role in blood cholesterol than intake of cholesterol itself

Cholesterol Synthesis
• 20–25% of total daily cholesterol production occurs in the liver– other sites of high synthesis rates: intestines,
adrenal glands, and reproductive organs
Cholesterol Synthesis
• one molecule of acetyl CoA and one molecule of acetoacetyl-CoA, are dehydrated to form 3-hydroxy-3-methylglutaryl CoA (HMG-CoA)– HMG-CoA is then reduced to mevalonate by
the enzyme HMG-CoA reductase• irreversible step • site of action for the statins

Cholesterol Synthesis• directly regulated by the cholesterol levels
present– higher intake from food - leads to a net
decrease in endogenous production– lower intake from food – increase in
endogenous production
Cholesterol Synthesis• main regulatory mechanism: sensing of
intracellular cholesterol in the endoplasmic reticulum by the protein SREBP (sterol regulatory element-binding protein 1 and 2)
• when cholesterol levels are low:– LDL receptor - scavenges circulating LDL from
the bloodstream, and – HMG-CoA reductase – lead to an increase of
endogenous production of cholesterol

Plasma Transport
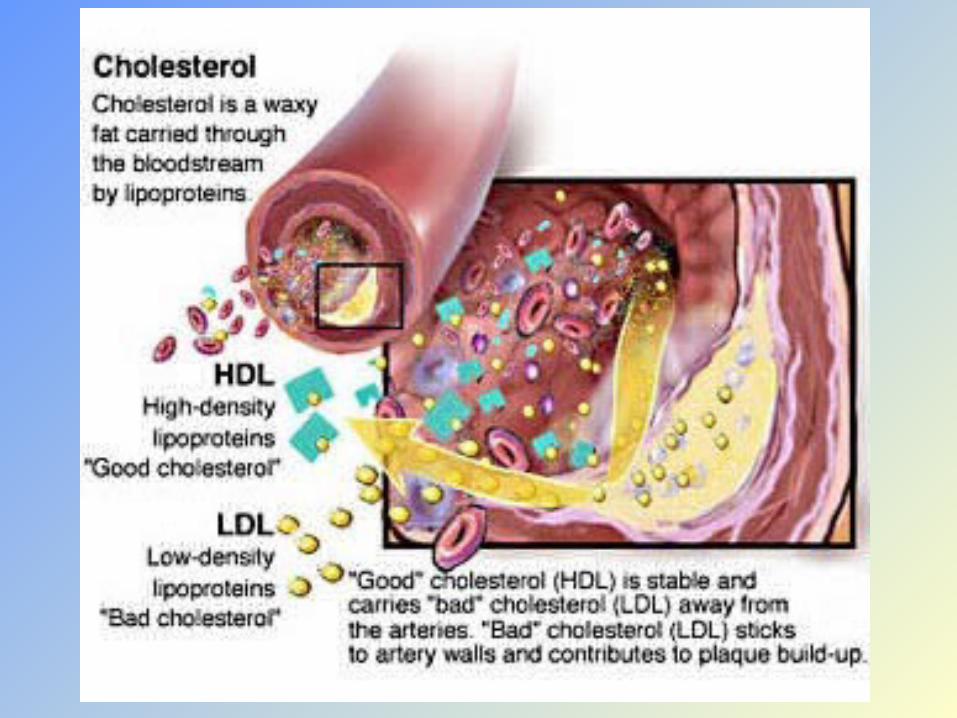
• Cholesterol is insoluble in blood
• Transport of cholesterol in circulatory system: within lipoproteins– complex spherical particles:
• exterior composed of amphiphilic proteins and lipids• inward-facing surfaces - lipid-soluble
(triglycerides and cholesterol esters are carried
internally)
– have cell-targeting signals that direct the lipids they carry to certain tissues
Triglycerides and cholesterol
• small amounts of lipid are coated with a layer of phospholipids, embedded in which are additional proteins—the apolipoproteins– Apolipoproteins serve as ligands for specific
receptors on cell membranes

Lipoprotein
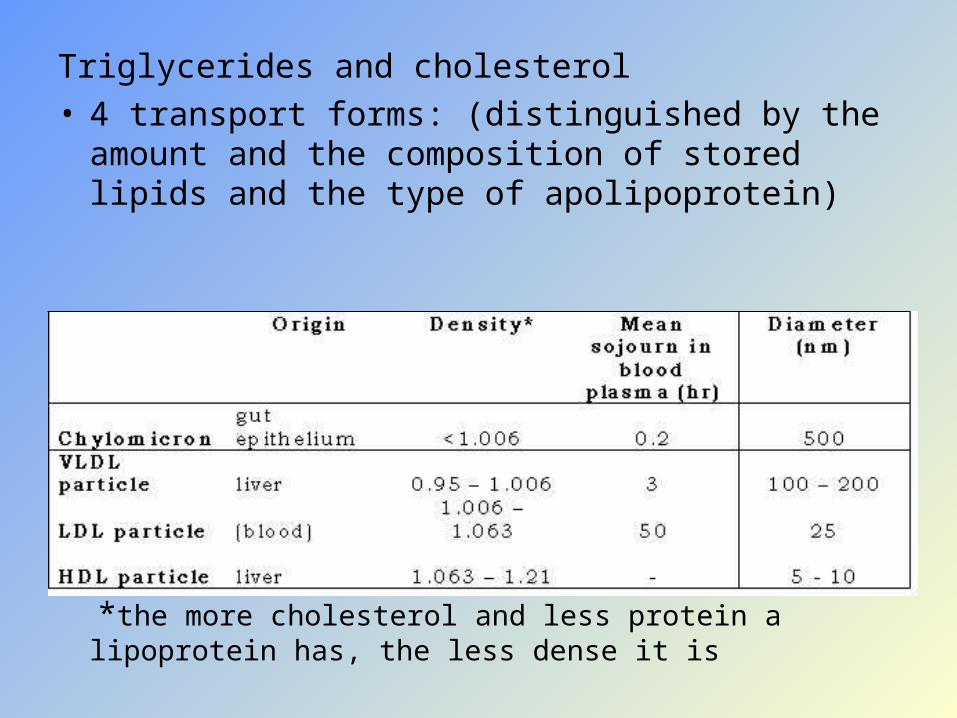
Triglycerides and cholesterol • 4 transport forms: (distinguished by the amount
and the composition of stored lipids and the type of apolipoprotein)
*the more cholesterol and less protein a lipoprotein has, the less dense it is


Plasma Transport
• Chylomicrons – transporters fats from the intestine to muscle
and other tissues that need fatty acids for energy or fat production.
– Cholesterol• is not used by muscles• remains in more cholesterol-rich chylomicron
remnants, which are taken up from the bloodstream by the liver
Plasma Transport
• VLDL molecules– produced by the liver– contain excess triacylglycerol and cholesterol
that is not required by the liver for synthesis of bile acids
– in the bloodstream, the blood vessels cleave and absorb more triacylglycerol to leave IDL molecules
Plasma Transport
• IDL molecules– contain an even higher percentage of
cholesterol – two possible fates:
• half are taken up by the liver for metabolism into other biomolecules
• half continue to lose triacylglycerols in the bloodstream until they form LDL molecules, which have the highest percentage of cholesterol within them
Plasma Transport
• LDL molecules – have the highest percentage of cholesterol
within them– major carriers of cholesterol in the blood– LDL-apolipoprotein B complex - recognized by
the LDL receptor in peripheral tissues
Plasma Transport
• LDL molecules synthesis of the LDL receptor is regulated by SREBP*– abundant cholesterol in cell LDL receptor
synthesis blocked– cell is deficient in cholesterol more LDL
receptors made
sterol regulatory element-binding protein
Plasma Transport
• when the SREBP system is deregulated:– many LDL molecules appear in the blood
without receptors on the peripheral tissues– LDL molecules are oxidized and taken up by
macrophages, which become engorged and form foam cells

Plasma Transport
• when the SREBP system is deregulated:– foam cells often become trapped in the walls
of blood vessels and contribute to artherosclerotic plaque formation
– hence, the association of LDL cholesterol (actually a lipoprotein) with "bad" cholesterol

Plasma Transport
• HDL particles – transport cholesterol: back to the liver
• for excretion to other tissues that use cholesterol to synthesize hormones
• process known as reverse cholesterol transport (RCT)
– having large numbers of large HDL particles – correlates with better health outcomes

Metabolism and Excretion
• Cholesterol is oxidized by the liver into a variety of bile acids
• Cholesterol is the major constituent of most gallstones, although lecithin and bilirubin gallstones also occur less frequently
Metabolism and Excretion
• Bile acids – conjugated with glycine, taurine, glucuronic
acid, or sulfate = bile salts: • solubilize fats in the digestive tract• aid in the intestinal absorption of fat molecules • aid in the intestinal absorption of the fat-soluble
vitamins, A, D, E, and K.

Metabolism and Excretion
• Bile acids– a mixture of conjugated and non-conjugated
bile acids along with cholesterol itself is excreted from the liver into the bile
– approximately 95% of the bile acids reabsorbed from the intestines
– essential for the digestion and absorption of dietary fats
– when more concentrated (as in the gallbladder) cholesterol crystallizes
Hyperlipoproteinemias
• primary – genetic– various drugs are available
• secondary – in obesity and metabolic disorders– immediate goal: lower lipoprotein levels by
diet and treatment of primary disease
Elevated LDL-cholesterol serum concentrations:
• associated with an increased risk of atherosclerosis– especially when there is a concomitant decline
in HDL concentration (increase in LDL:HDL quotient).


Total Fat Intake
• plays a larger role in blood cholesterol than intake of cholesterol itself
• Saturated fat intake - present in full fat dairy products, animal fats, several types of oil and chocolate
• Trans fats intake - derived from the partial hydrogenation of unsaturated fats– margarine and hydrogenated vegetable fat– consequently in many fast foods, snack foods,
and fried or baked goods

Studies have shown that:
1. Higher values of LDL cholesterol (4.5-7.5 mmol/L) were more common in CAD (coronary artery) patients
2. Lower values of HDL cholesterol (0.2-0.8 mmol/L) were more common in CAD patients. 3. High baseline levels of cholesterol correlated
with an increased risk of subsequent coronary heart disease (CHD) after 40 years of follow-up
4. Hyperlipidemia was by far the most important risk factor for CHD

Major Independent Risk Factors for Coronary Heart Disease
a. High serum cholesterol
b. Hypertension
c. Cigarette smoking
d. Diabetes mellitus

Major Modifiable Risk Factors for Coronary Heart Disease
a. Physical inactivity
b. Obesity
c. Atherogenic diet


Exercise
• elevates HDL levels to an extent
dependent on the level of aerobic
exercise
Diet
1. high saturated fat diet:
• increases levels of VLDL & LDL
2. low fat diet
• reduces LDL & HDL levels
3. alcohol
• increases VLDL levels

Major Non-Modifiable (Independent)
Risk Factors for Coronary Heart Disease
a. Advancing age
b. Male sex
c. Positive family history in a first
degree relative
Secondary hyperlipidemias
- may be due to: a. Hypothyroidism b. Nephrotic syndrome c. Diabetes mellitus (NIDDM) d. Chronic renal failure

Hormones
1. Thyroxine
• reduces LDL levels
2. Androgens
• reduce HDL levels
3. Estrogens
• increase LDL receptor function
• help keep LDL levels down in
premenopausal women

Antihyperlipidemic Agents

HMG CoA reductase inhibitors
(Statins)First isolated from cultures of Penicillium sp.
MOA:
competitive inhibition of HMG CoA reductase,
the enzyme that catalyzes the rate-limiting step
in cholesterol synthesis in the in the liver
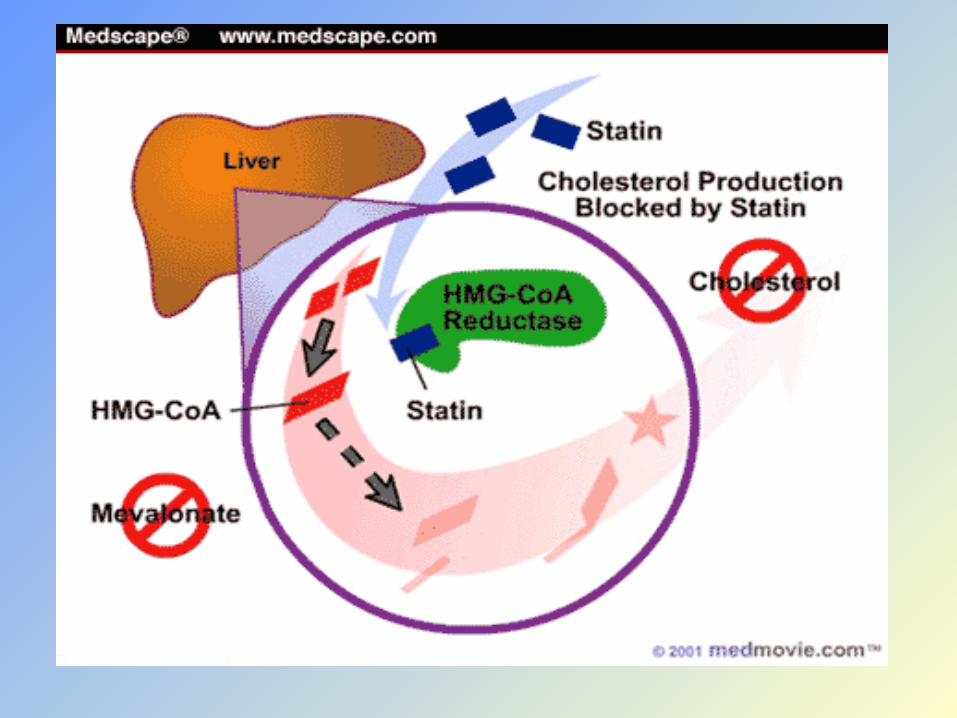

MOA Contd.
• Reduction in synthesis of Cholesterol
• Compensatory increase in LDL receptor on Liver cells
• Increased receptor mediated uptake and catabolism of LDL
Important HMG-CoA reductase inhibitor drugs:
• Atorovastatin(A)
• Lovastatin(L)
• Simavastatin(S)
• Pravastatin(P)
• Fluvastatin(F)
HMG CoA reductase inhibitors
(Statins)• active group of L, S, P, and F (or their
metabolites) resembles that of the physiological
substrate of the enzyme– P and F represent the active acidic forms :
Hydrophilic– L and S are lactones
HMG CoA reductase inhibitors
(Statins)• Atorvastatin has the longest duration of
action and highest LDL-CH lowering capacity
• Additional antioxidant property
HMG CoA reductase inhibitors
(Statins)Lipid Profile Effects:
• reduces total cholesterol, LDL, & triglycerides
• increases HDL cholesterol
Clinical Efficacy:
• powerful LDL-lowering drugs:
- reduces coronary risks in both primary
and secondary prevention
- reduces risk for stroke in
secondary prevention

HMG CoA reductase inhibitorsSignificant Pharmacokinetic Properties:
• extensive first-pass effect
• converted to hydroxy acids, which are
highly protein bound
• major route of excretion: liver
HMG CoA reductase inhibitors
outstanding record of patient acceptance and safety
HMG CoA reductase inhibitorsMost Important ADRs:
muscle pain/myopathy/rhabdomyolitis
– most serious
liver enzyme abnormalities
– increase transaminases, but liver damage is rare
Other Adverse Effects:
nausea
insomnia/fatigue/headache
skin rashes
Fibrates(Gemfibrozil, Fenofibrate)
MOA: unclear increases catabolism of triglyceride-rich lipoproteins brought about by an increased lipoprotein lipase activityLipid-Profile Effects: • for modifying atherogenic dyslipidemia particularly for lowering triglycerides • moderately elevates HDL-cholesterol • mild lowering of LDL-cholesterol
FibratesGenerally well-toleratedSide effects: nausea/abdominal pain/diarrhea – most common liver enzyme abnormalities gallstones skin flushes myalgiasDrug Interactions: potentiates oral anticoagulants

Omega-3 Fatty Acids(Linolenic Acid, DHA, EPA)
MOA:
reduce hepatic secretion of triglyceride-rich
lipoproteins
Clinical Efficacy:
• alternatives to fibrates or nicotinic acid for
treatment of hypertriglyceridemia
• reduce risk for major coronary events in
patients with established CHD
• recommended only as an option at present

Fibrates(Gemfibrozil, Fenofibrate)
MOA: unclear increases catabolism of triglyceride-rich lipoproteins brought about by an increased lipoprotein lipase activityLipid-Profile Effects: • for modifying atherogenic dyslipidemia particularly for lowering triglycerides • moderately elevates HDL-cholesterol • mild lowering of LDL-cholesterol
FibratesGenerally well-toleratedSide effects: nausea/abdominal pain/diarrhea – most common liver enzyme abnormalities gallstones skin flushes myalgiasDrug Interactions: potentiates oral anticoagulants

Fibrates(Gemfibrozil, Fenofibrate)
MOA: unclear increases catabolism of triglyceride-rich lipoproteins brought about by an increased lipoprotein lipase activityLipid-Profile Effects: • for modifying atherogenic dyslipidemia particularly for lowering triglycerides • moderately elevates HDL-cholesterol • mild lowering of LDL-cholesterol

FibratesGenerally well-toleratedSide effects: nausea/abdominal pain/diarrhea – most common liver enzyme abnormalities gallstones skin flushes myalgiasDrug Interactions: potentiates oral anticoagulants

Omega-3 Fatty Acids(Linolenic Acid, DHA, EPA)
• Also results in:
decreased synthesis of VLDL and
apolipoprotein B
improved clearance of remnant particles
• Total and LDL cholesterol are not decreased or are even increased
Nicotinic acidMOA: • mechanism uncertain• activate endothelial lipoprotein lipase and thereby
lower triglyceride levels– reduces triglyceride & hepatic synthesis of
apolipoprotein B-100, an essential component of VLDL
Other Lipid Profile Effects:
• increases HDL cholesterol
- the most effective among the lipid
lowering agents
• moderate reduction in LDL cholesterol

Nicotinic acidClinical Efficacy:
• recommended:
- for higher-risk persons with atherogenic
dislipidemia with moderate increase in
LDL-cholesterol levels
- in combination, for higher risk persons
with atherogenic dislipidemia and elevated
LDL-cholesterol
Nicotinic acidCaution:
active liver disease
recent peptic ulcer
hyperuricemia and gout
type 2 diabetes
Availability:
100 mg tablets
Daily dose: 2-6 grams per day!!!
Bile acid sequestrants Cholestyramine and Colestipol
Originally designed to control pruritus in
obstructive liver disease
MOA:
- anion exchange resins: exchange
chloride for the negatively charged acid
→ excretion of bile acids → increase
hepatocyte cholesterol content →
- increases removal of LDL from the
blood by hepatic LDL receptors
Bile acid sequestrants (Cholestyramine and Colestipol)
• by virtue of binding bile acids, they promote consumption of cholesterol for the synthesis of bile acids
• non-absorbable– no systemic toxicity
• gritty texture makes ingestion an unpleasant experience

Bile acid sequestrants (Cholestyramine and Colestipol)
Clinical Efficacy:
produce moderate reductions in LDL
cholesterol
• for persons with moderate elevations
in LDL cholesterol, younger patients,
women considering pregnancy
• for very high LDL - combine with statins
Bile acid sequestrants (Cholestyramine and Colestipol)
Side effects:
• dose-dependent; limits their widespread use– at the required dosage, the resins cause diverse GIT
disturbances
intestinal bloating/obstruction
nausea/flatulence/constipation - more
common

Bile acid sequestrants (Cholestyramine and Colestipol)
Drug Interaction:• adsorb and decrease the absorption of
such drugs as digitoxin, vitamin K antagonists, and diuretics
ProbucolMOA: uncertain
may enhance conversion of cholesterol to
bile acids followed by increased fecal
sterol secretion or inhibitory effects on
the synthesis of lipoproteins or
cholesterol

ProbucolProblems: • erratic ability to lower LDL • potent and persistent ability to lower HDL - no longer a first line lipid-lowering agent - appears effective in reducing atherogenesis, possibly by reducing LDL oxidation
Side effects: abdominal pain/nausea fetid perspiration flatulence/diarrhea angioneurotic edema hyperhydrosis prolonged Q-T interval


Plasma Expanders
• They are high molecular weight substances which exert colloidal osmotic pressure, and when infused i.v. retain fluid in the vascular compartment.
Desirable Properties
• Should exert osmotic pressure comparabe to plasma.
• Should remain in circulation and not leak out in the tissues.
• Should be pharmacodynamically inert.
• Should not be pyrogenic or antigenic.
• Should not interfere with grouping and cross matching of blood.
• Should be stable, easily sterilizable and cheap.
Egs.
• Human albumin
• Dextran
• Degraded gelatin
• Hydroxy ethyl starch (HES)
• Polyvinyl pyrrolidone (PVP)

Uses
• As substitutes for plasma in conditions where plasma has been lost or moved to extravascular compartments-
• Burns
• Hypovolemia
• Endotoxin shock
• Severe trauma
• Extensive tissue damage.
Contraindications
• Severe anaemia
• Cardiac failure
• Pulmonary edema
• Renal insuffiency.