antibody responses and fc gamma receptor iia polymorphism in
TRANSCRIPT


A
DThe
Antibopoly
Doctoral thWenner-G
dy respymorp
Nnae
hesis fromGren Insti
ponseshism infalcip
emeka C
St
m the Depaitute, Stoc
s and Fn relat
parum m
hukwuk
tockholm
artment ofkholm Un
Fc gammtion to Pmalari
kaelo Irie
2009
f Immunolniversity, S
ma recPlasmoia
emenam
logy, Sweden
ceptor odium
m
IIa

ii
Cover illustration: © Palle Ryde Figure 1, 2, 11 © Palle Ryde All previously published papers were reproduced with permission from the publishers. Distributed by Stockholm University Library Printed in Sweden by Universitetsservice AB, Stockholm 2009 © Nnaemeka Chukwukaelo Iriemenam, Stockholm 2009 ISBN 978-91-7155-894-7

iii
‘‘If I haven’t seen further, it is by standing in the footprints of giants’’ Ketil Malde
To my parents, Jonathan Iriemenam Okonkwo and Monica Chinwa Okonkwo And to my lovely wife, Chizube Iriemenam and my wonderful baby
Chikamdabere Iriemenam

iv
‘‘Try not to become a man of success but rather to become a man of value’’ Albert Einstein
Above the cover The picture depicts a cartoon of a plausible mechanism by which antibodies mediate their parasite clearance of infected erythrocytes by binding to free merozoites or to antigens on the surface of infected erythrocytes.
v
SUMMARY Immunity to asexual blood-stage of Plasmodium falciparum malaria is believed to be associated with protective antibodies of certain immunoglobulin classes and subclasses. This thesis addressed the importance of antibodies in relation to malaria infection and their effective interactions with Fc gamma receptor IIa (FcγRIIa) polymorphisms in individuals residing where malaria is endemic. Our data indicate that the frequency of FcγRIIa-R/R131 genotype was significantly higher in Sudanese patients with severe malaria when compared to patients with mild malaria, while the FcγRIIa-H/H131 genotype showed a significant association with mild malaria. The levels of IgG1 and IgG3 subclass antibodies were statistically significantly higher in the mild malaria patients when compared with the severe malaria patients. A reduced risk of severe malaria with IgG3 antibodies in combination with H/H131 genotype was also observed. Our data suggest the importance of cytophilic antibodies in parasite-neutralising immune mechanisms and also signify that the H/H131 genotype, which binds IgG3 more efficiently, is less likely to be associated with severe malaria while R/R131 genotype was associated with severe malaria in this population. The Fulani ethnic group in West Africa has been shown to be relatively resistant to malaria. We investigated the possible impact of FcγRIIa polymorphisms in the ethnic differences in malaria susceptibility seen between Fulani and non-Fulani in Mali and Sudan, and also analysed their malaria reactive IgG subclass profiles. The H131 allele was associated with the Fulani ethnic group, and the R131 allele with the Dogon in Mali and the FcγRIIa-H/H131 genotype and H131 allele were also found to be significantly more prevalent in the Fulani of Sudan as compared to the non-Fulani ethnic groups. The Fulani had higher serum levels of IgG1-3, with higher proportion of IgG2 than the Dogon in Mali while IgG1 and IgG3 were relatively lower among the Fulani in Sudan with a higher proportion of IgG2 than the non-Fulani. The higher IgG2 antibody levels seen in the Fulani individuals may be due to the relatively high prevalence for the H/H131 genotype in this population. Most clinico-epidemiology studies have been in areas with holo- and hyper-malaria endemicity. We have analysed antibody responses to a panel of six blood-stage antigens in relation to clinical malaria outcome in a hospital-based study in Sudan. The pattern of the IgG subclasses towards the different antigens varied but the IgG1 and IgG3 subclasses were the most prominent. Our results revealed a linear association with anti-AMA-1 IgG1 antibodies and reduced risk of severe malaria while a non-linear relationship with IgG3 antibodies was observed for MSP-2, MSP-3 and GLURP. In the combined final model, the highest levels of IgG1 subclass antibodies to AMA-1, GLURP-R0, and the highest levels of IgG3 subclass antibodies reactive to 3D7 MSP-2 were independently associated with a reduced risk of clinical malaria. The results further indicated that for most of the antigens, IgG3 antibodies, with their shorter half-life, may be more efficient than IgG1 in limiting parasitaemia in individuals with clinical malaria, probably due to its structurally biological function. Taken together, these data suggest the importance of the studied merozoite antigens as targets for parasite neutralising antibody responses of the IgG1 and IgG3 subclasses. Furthermore, our results suggest a possible association between FcγRIIa-R/H131 and anti-malarial antibody responses in the clinical outcome of malaria.

vi
TABLE OF CONTENTS SUMMARY.......................................................................................................................V TABLE OF CONTENTS................................................................................................VI LIST OF INCLUDED PAPERS.................................................................................VIII LIST OF ABBREVIATIONS.........................................................................................IX INTRODUCTION.............................................................................................................1 THE IMMUNE SYSTEM...............................................................................................1 Innate Immunity...........................................................................................................1 Cells involved in innate immunity.............................................................................3 Adaptive (Specific) Immunity........................................................................................6 T lymphocytes..............................................................................................................7 Antigen presentation....................................................................................................8 B lymphocytes.............................................................................................................8 Plasma cells................................................................................................................10 Cytokines...................................................................................................................10 Immunoglobulins..........................................................................................................11 Immunoglobulin classes.............................................................................................13 Effector functions mediated by antibodies................................................................16 Fc receptors.................................................................................................................17 FcγRIIa.......................................................................................................................19 MALARIA.....................................................................................................................20 The life cycle of Plasmodium malaria.......................................................................21 Clinical features of malaria.......................................................................................22 Malaria endemicity....................................................................................................26 MALARIA IMMUNOLOGY.......................................................................................29 The pre-erythrocytic stage.........................................................................................29 The erythrocytic stage...............................................................................................29 The importance of antibodies in P. falciparum immunity.........................................31 Target blood-stage antigens.....................................................................................33 B-cell memory in malaria..........................................................................................35 The haemoglobinopathies..........................................................................................36 Haemoglobin variant...............................................................................................37 The ABO blood group system...................................................................................39 RELATED BACKGROUND.........................................................................................40 Epidemiology of malaria in stable and unstable malaria transmissions........................40 Ethnicity.........................................................................................................................41 Antibody reactivities to blood-stage antigens in relation to malaria disease.................42 FcγRIIa and malaria.......................................................................................................43 THE PRESENT STUDY.................................................................................................45 AIM OF THE THESIS..................................................................................................45 SUDAN..........................................................................................................................46 Country profile...........................................................................................................46 Daraweesh project......................................................................................................46 MALI.............................................................................................................................48 Country profile...........................................................................................................48

vii
Study area...................................................................................................................48 METHODOLOGY........................................................................................................50 Ethical permissions....................................................................................................51 RESULTS AND DISCUSSION....................................................................................52 FcγRIIa polymorphism and antibody responses in clinical malaria outcome...........52 FcγRIIa polymorphism and IgG subclasses in relation to malaria............................54 FcγRIIa polymorphism on the IgG subclass patterns of antibodies...........................55 IgG subclass responses to different asexual blood-stage malaria antigens................57 CONCLUDING REMARKS AND FUTURE PERSPECTIVES................................61 ACKNOWLEDGMENTS...............................................................................................64 REFERENCES.................................................................................................................68

viii
LIST OF INCLUDED PAPERS This doctoral thesis is based on the following original papers, which are referred to by their Roman numerals in the text:
I. Nasr A*, Iriemenam NC*, Troye-Blomberg M, Giha HA, Balogun HA, Osman OF, Montgomery SM, ElGhazali G, Berzins K. Fc gamma receptor IIa (CD32) polymorphism and antibody responses to asexual blood-stage antigens of Plasmodium falciparum malaria in Sudanese patients. Scand J Immunol 2007; 66:87-96.
*The authors A. Nasr and N. C. Iriemenam contributed equally to this article.
II. Israelsson E, Vafa M, Bakary M, Lysén A, Iriemenam NC, Dolo A, Doumbo
OK, Troye-Blomberg M, Berzins K. Differences in Fcγ receptor IIa genotypes and IgG subclass pattern of anti-malarial antibodies between sympatric ethnic groups in Mali. Malar J 2008; 7:175.
III. Nasr A, Iriemenam NC, Giha HA, Balogun HA, Anders RF, Troye-Blomberg M,
ElGhazali G, Berzins K. FcγRIIa (CD32) polymorphism and anti-malarial IgG subclass pattern among Fulani and their sympatric tribes in eastern Sudan. Malar J 2009; 8:43.
IV. Iriemenam NC, Khirelsied AH, Nasr A, ElGhazali G, Giha HA, Elhassan TM,
Agab-Aldour AA, Montgomery SM, Anders RF, Theisen M, Troye-Blomberg M, Elbashir MI, Berzins K. Antibody responses to a panel of Plasmodium falciparum malaria blood-stage antigens in relation to clinical disease outcome in Sudan. Vaccine 2009; 27:62-71.

ix
LIST OF ABBREVIATIONS
ADCC Antibody-dependent cell cytoxicity ADCI Antibody-dependent cell-mediated inhibition APC Antigen presenting cell BCR B-cell receptor CLRs C-type lectin-like receptor CNS Central nervous system CR1 Complement receptor 1 CRP C-reactive protein CSA Chondroitin sulphate A CTL Cytotoxic T-cell DBL Duffy-Binding-like DC Dendritic cell DN Double negative DP Double positive EIR Entomological inoculation rate FcγR Fc gamma receptors H Histidine IFN Interferon IL Interleukin ITAM Immunoreceptor-tyrosine-based activation motif ITIM Immunoreceptor-tyrosine-based inhibitory motif KIR Killer-cell immunoglobulin-like receptors MBL Mannose-binding lectin MHC Major histocompatible complex NK cell Natural-killer NKT cell Natural-killer T cell NO Nitric oxide NOD Nucleotide binding and oligomerization domains PAM Pregnancy-associated malaria PAMPs Pathogen-associated molecular patterns PCR Polymerase-chain reaction PfEMP1 Plasmodium falciparum erythrocyte membrane protein 1 PPRs Pattern recognition receptors R Arginine RBC Red blood cell RIG-1 Retinoid acid-inducible gene-1 SNP Single-nucleated polymorphism SRs Scavenger receptors TCR T-cell receptor Th T helper cell TLRs Toll-like receptors TNF Tumour necrotic factor Treg Regulatory T cells VSA Variant surface antigen

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
1
INTRODUCTION
The immune system
The immune system is an organisation of cells and molecules with specialized roles in
defending against infection [1]. Its complex structure helps to detect a wide variety of
infectious agents, (viruses, bacteria, fungi, parasites) and distinguishes them from the
organism’s own healthy cells and tissues. The immune system can be classified into two
fundamental different types, the innate (natural) and adaptive (acquired) immune system
[1, 2].
Innate immunity
The innate immune system provides the frontline host defence to any microbial invader,
in a non-specific manner. It provides the immediate host defence against infection and is
found in all classes on plants and animals. It comprises four types of defensive barriers:
anatomic (skin, mucous membrane), physiologic (temperature, low pH, chemical
mediators), phagocytic (internalization), and inflammatory (tissue damage). Microbial
invaders/intruders that manage to escape these mechanisms, encounter a number of innate
cellular mediators with variant host defensive capabilities like tissue macrophages,
neutrophils, natural-killer cells (NK), and dendritic cells (DC) [3]. The innate immunity
signals plays a critical role in initiating and instructing the development of adaptive
effector mechanisms when it fails to successfully eliminate the pathogen and this process
requires several days to produce armed effector cells.
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
2
The innate immune system recognises pathogen through an array of soluble and
membrane bound sensors called pattern-recognition receptors (PRRs) that bind pathogen-
associated molecular patterns (PAMPs), found in a broad type of organisms [4].
Scavenger receptors (SRs) represent a large family of structurally unrelated distinct gene
products, expressed by myeloid cells, selected endothelial cells and some epithelial cells
and recognise different ligands including microbial pathogens as well as endogenous and
modified host-derived molecules [5, 6]. SRs are classified into eight different classes
(Class A-H) [6]. The nucleotide binding and oligomerization domains (NOD)-like
receptors (NLRs), which are intracellular, cytoplasmic sensors; and the retinoid acid-
inducible gene-1 (RIG-1)-like receptors (RLRs), which are cytosolic helicases are
additional classes of PRRs [7]. Other members of PRRs family include C-type lectin-like
receptor (CLRs), cytoplasmic double-stranded RNA [8], cytoplasmic-dsDNA receptor
[9], C-reactive protein (CRP), mannose-binding lectin (MBL) and complement proteins.
Of the PRRs, Toll-like receptors (TLRs) are the most studied. TLRs are evolutionary
conserved proteins that have a highly conserved intracellular Toll/IL-1R domain involved
in protein-protein interactions and signalling activation [10]. In humans, 11 TLRs have
been identified and based on their cellular localization, they are classified into two major
groups: TLR 3, 7, 8, and 9 are expressed in endosomes, while TLR 1, 2, 4, 5, and 6 are
present on the surface of many different cells [11]. Upon activation, these sensors trigger
response pathways to form an alarm system critical to the activation of myeloid lineage
cells (macrophages and DCs) that phagocytose and degrade pathogens, migrate to
secondary lymphoid tissue and present antigen to T cells [12]. TLRs control DC

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
3
functions, activate signals involved in the initiation of the adaptive immune response
[13], and thus may contribute directly to the perpetuation and activation of long term T-
cell memory [14]. B-cell intrinsic TLR signals are not required for antibody production or
maintenance [15]. Members of the TLR family recognise bacteria, viruses, fungi and
protozoa; NLRs detect bacteria, and RLRs detect viruses. The interplay between these
families ensures the efficient co-ordination of innate immune responses, through either
synergistic or co-operative signalling [16].
Cells involved in innate immunity
Mammalian species possess linked cluster of genes, the major histocompatible complex
(MHC), which play a role in inter-cellular recognition and discrimination of self and non-
self. MHCs are glycoproteins found on the surface of cells and are categorized into three
classes; Class I, II and III. Class I is expressed on the surface of all nucleated cells, while
Class II is expressed by professional antigen-presenting cells (APCs) [macrophages, DCs,
B cells], and Class III encodes molecules critical in immune function.
Monocytes and macrophages belong to the mononuclear phagocyte system. They are
phagocytes whose functions are non-specific. They help to phagocytose (engulf and
digest) debris and pathogens and stimulate lymphocytes to respond to the pathogen.
Monocytes are known to originate from the bone marrow through the common myeloid
progenitor (shared with neutrophils) and are released into the peripheral blood, where
they circulate for several days before entering the tissues and differentiate into tissue
macrophages, contributing to local trophy interactions and tissue homeostasis [17].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
4
Monocytes also have the capacity to differentiate into DCs and therefore play an
important role in innate and adaptive immunity, due to their microbicidal potential,
capacity to stimulate CD4+ and CD8+ T-cell responses and ability to regulate
immunoglobulin production by B cells [18]. Monocytes express PRR such as TLRs, and
Fc gamma receptors (FcγR) I-III and may contribute to the shaping of memory-T cell
responses [19]. The heterogeneity of macrophages reflects their specialized functions in
different anatomical locations, including the following; alveolar macrophages in the
lungs, macrophages in the central nervous system (CNS) [17], splenic macrophages,
tangible-body macrophages [20], Kupffer cells present in the liver, mesangial cells in the
kidney, etc. Activated macrophages have more effective phagocytic activities because
they express higher levels of MHC Class II molecules and the co-stimulatory B7
membrane molecule thereby allowing them to function more effectively as APCs.
DCs are the most effective APCs because they express high level of MHC class II
molecules and co-stimulatory molecules. They are able to activate naïve T cells and are
critical for the development of the adaptive immune system [21]. DCs are sentinels, able
to capture, process and present antigens and to migrate to lymphoid tissues to select rare,
antigen-reactive T-cell clones [22]. Two DCs subsets, in humans have been described;
myeloid DC which originates from the monocytes arising from the myeloid pathway, and
the plasmacytoid DC which originates from the lymphoid pathway. These subsets differ
slightly in their expression of TLRs but are both effective in the stimulation of naïve T
cells [13, 23]. A new novel subset of cytotoxic DCs has recently been described, with

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
5
functions of NK cells and DC cells, called killer DC [24, 25], that is believed to
participate in the control of tumour progression [25, 26].
NK cells are large granular lymphocytes with natural cytotoxicity that constitute a major
part of the innate immune system. They kill target cell through the release of cytoplasmic
granules of proteins (perforin and granzyme) that cause the target cell to die through
apoptosis or necrosis [27]. Unlike cytotoxic-T lymphocytes, which need to be activated
before granules appear, NK cells are constitutively cytotoxic. NK cells discriminate
between target cells and healthy self cells by a variety of cell surface activating and
inhibitory receptors and their interactions with DC cells shape innate and adaptive
immunity [28]. They express the surface markers CD16 (FcγRIII) and CD56 in humans,
and NK1.1/NK1.2 in certain strains of mice, enabling them to detect antibody-coated
target cells and to exert antibody-dependent cell cytoxicity (ADCC) [27]. Activating
receptors detect the presence of ligands on cells in distress by NKG2D (humans) as well
as RAE1 (mouse) while they use the inhibitory receptors (killer-cell immunoglobulin-like
receptors – KIR) to gauge the absence of self molecules on susceptible target cells [29].
By interacting with MHC Class 1 molecules that are expressed by most healthy cells,
inhibitory MHC Class 1 receptors provide a way for NK cells to ensure tolerance to self
while allowing toxicity towards stressed cells [27]. Two major subsets of NK cells are
distinguished based on their low and high expression of CD56 (CD56bright and CD56dim
respectively). About 90% of human NK cells are CD56dim/CD56bright, found in the blood,
spleen and display stronger cytotoxic functions while the remaining 10% are
CD56bright/CD56dim, found in the lymph nodes, with less cytotoxicty [30].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
6
Adaptive (Specific) Immunity
Unlike the innate immune response, the adaptive immune response provides the immune
system with the ability to recognize and remember specific pathogens, and to mount
stronger attacks each time the pathogen is encountered. This is done through four
different attributes; antigenic specificity (distinguishes between different antigens),
diversity (recognizes different structures on foreign antigens), immunologic memory
(second encounter of the same antigen produces a heightened reactivity) and self/non-self
recognition (distinguishes between self and non-self). Adaptive immune responses are
mediated by lymphocytes. Lymphocytes are one of the many types of white blood cells
produced in the bone marrow by the process of haematopoiesis. These cells recognize
individual pathogens specifically and possess memory.
Two major populations of lymphocytes are known – T lymphocytes (T cells) and B
lymphocytes (B cells). T cells and B cells recognize antigens through the specificity of
their antigen receptors, T- and B-cell receptors (TCR and BCR) respectively. B cells
respond to pathogens by producing large quantities of antibodies which then can
neutralize foreign objects like bacteria, viruses, etc. In response to pathogens some T
cells, called helper-T cells produce cytokines that direct the immune response while other
T cells, called cytotoxic-T cells, produce toxic granules that induce the death of pathogen
infected cells. Following activation, B cells and T cells leave a lasting legacy of the
antigens they have encountered, in the form of memory cells. Through the lifetime of an
animal, these memory cells will remember each specific pathogen encountered, and are
able to mount a strong response if the pathogen is detected again.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
7
T lymphocytes
T cells are generated in the thymus throughout adult life [31] and play central role in cell-
mediated immunity. Two lineages of T cells, αβ and γδ, generated in thymus are defined
by their expression of αβ- and γδ- TCR complexes [32]. The most immature subsets lack
the expression of the CD4 and CD8 molecule, thus called double negative (DN). Later,
the αβ lineage progresses to a CD4 CD8 double positive (DP) stage, during which they
undergo further positive and negative selection to generate MHC-restricted and self-
tolerant CD4 and CD8 single positive T cells [33]. The resulting mature γδ T cells, and
αβ T cells comprise; the CD8+ cytotoxic, CD4+ helper and regulatory lineages that form
the basis of cellular immunity [32]. CD4+ T cells regulate cellular and humoral immunity
while CD8+ T cells show cytotoxic activity towards intracellular pathogens. Both CD4+
and CD8+ T cells develop into memory-T cells which increase the specificity of the
adaptive immune responses. CD4+ T cells can differentiate into Th1, Th2, Th17 and Treg
subsets depending on the nature of the cytokine milieu [34].
Th1 cells drive the type-1 pathway, the cellular pathway, mediated by interferon gamma
(IFN-γ) and fight against intracellular pathogens, while Th2 cells drive the type-2
pathway, the humoral immunity pathway, mediated by interleukin-4 (IL-4), IL-5, IL-13
and helps in antibody production and fights against extracellular pathogens [35]. Th17
cells are characterized by their production of IL-17 and may have evolved for host
protection against microbes that Th1 or Th2 immunity are not well suited for, such as
extracellular bacteria and fungi. The effector cytokines produced by Th17 cells are
IL17A, IL17F, TNF-α, IL-22, IL-26 and IFN-γ [36]. Tregs are crucial for the

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
8
maintenance of immunological tolerance. Naturally occurring Tregs,
CD4+CD25+FoxP3+, arise in the thymus, while the induced Tregs (Tr1 and Tr3) may
originate during an immune response. Natural-killer T cells (NKT cells) share similar
characteristics with NK cell markers by the expression of αβ-TCR. Unlike the T cells
that recognize antigens presented by MHC molecules, NKT cells recognize glycolipid
antigen presented by CD1d. Upon activation, NKT cells can function as either Th or CTL
cells.
Antigen presentation
Antigen processing and presentation are major requirements of the immune response. B
cells can bind directly to the naïve antigen while T cells identify and destroy infected
cells through recognition of foreign determinants associated to self components. These
self components are MHC molecules expressed on the surface of APC and encoded by
the MHC-gene located on chromosome 6 in humans. MHC class I molecules bind to
peptidic fragments which are generated in the cytosol of the cell (endogenous processing
pathway), e.g. viral-infected cell, while MHC class II molecules bind peptidic fragments
that have been internalised by phagocytosis (exogenous processing pathway) and
degraded in the endocytic compartment.
B lymphocytes
B cells are lymphocytes that play a major role in the humoral immune response. Their
primary function is the production of antibodies against antigens, to function as APC and
develop into memory-B cells after antigen stimulation. Many B cells are produced in the

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
9
bone marrow throughout life. B-cell development occurs through several stages:
generation of mature immunocompetent B cells (stage of maturation), activation of
mature B cells (stage of antigen interaction), and differentiation of activated B cells into
memory-B cells and plasma cells (Figure 1). B-cell activation often proceeds through two
different routes: thymus-dependent antigens that require direct contact with Th cells, eg
proteins while thymus-independent antigens can activate B cells in the absence of Th
cells, eg lipopolysaccharide, peptidoglycan.
Figure 1. B-cell development. During antigen-independent maturation phase, immunocompetent B cells express membrane IgM and IgD. When activated by Th cells, B cells proliferate and differentiate into high-affinity mIg memory-B cells and plasma cells, which may express different isotypes due to class switching.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
10
Plasma cells
Conventional models postulate that the maintenance of serum antibodies requires the
continuous proliferation and differentiation of memory-B cells into antibody-secreting
plasma cells [37-39]. Plasma cells typically represent less than 1% of the cells in the
lymphoid organs, yet they are responsible for all antibodies in circulation [40]. An early
study [41] had suggested that some plasma cells have a half-life of only a few days [42-
43] to at most few weeks [44]. However, accumulating evidence, from this last decade,
suggest that plasma cells have the potential to be very long lived, maintaining persisting
antibody production in the event of re-infection [45-47]. The bone marrow is believed to
be a major site of long-term antibody production [47]. Two populations of plasma cells
have been described; long-lived and short-lived [48]. Long-lived plasma cells are a
central part of immune memory, as these cells are largely responsible for the long term
continuous secretion of antibodies. The possible explanation of plasma cell survival in
vivo could be that antibody levels are maintained by the continuous development of
short-lived plasma cells from memory cells, or that plasma cells themselves are long-
lived and maintained independently of memory-B cells and antigen [40].
Cytokines
Cytokines are low molecular weight regulatory polypeptides secreted by white blood
cells and various other cells in response to a number of stimuli. Cytokines bind to specific
receptors on the membrane of target cells triggering signal-transduction pathways that
alter gene expression in the target cell. Cytokines can bind to receptors on the membrane
of the same cell that is producing them (autocrine actions), bind to receptors on the target
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
11
cell in immediacy (paracrine action), or bind to target cells in distant (endocrine action).
Cytokines are involved in the regulation of the innate and adaptive immunity and
depending on the effect of the immune response; cytokines can be classified as Th1 (pro-
inflammatory) or Th2 (anti-inflammatory) cytokines. The cytokines secreted by the Th1
subset act primarily in cell-mediated responses, whereas those secreted by the Th2 subset
function mostly in B-cell activation and humoral responses.
Immunoglobulins
Immunoglobulins (Ig) are antigen-binding proteins present on the B-cell membrane and
secreted by plasma cells. When bound on the cell surface, the Ig functions as a receptor
involved in differentiation, activation and apoptosis, while the secreted form can
neutralize foreign antigens and recruit other effector components [49]. The Ig molecule
consists of two identical light (L) chains and two identical heavy (H) chains associated in
the form of a Y-shape (Figure 2). It consists of the antigen-binding site (Fab) and the
crystallisable fragment (Fc). Each light chain is bound to a heavy chain by disulfide
bonds and noncovalent interactions, forming the antigen-binding sites. The two heavy
chains are linked to each other by disulfide bonds to form the Ig molecule. The tail of the
Fc part interacts with receptors present on neutrophils, monocytes, macrophages, etc, and
complements. Based on the structure of their heavy chain constant regions, Igs are
classed into classes which may further be divided into subclasses. There are five classes
of heavy chains, δ, µ, γ, α and ε which form the five antibody isotypes IgD, IgM, IgG,
IgA and IgE. The different isotypes perform different functions, and help in directing the
appropriate immune response.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
12
Figure 2. Structure of the Ig molecule and the five different Ig isotypes.
The antibody interacts with antigenic determinants, or epitopes, via antigen-combining
sites present in the hyper-variable regions of the Ig molecule. The antigenic determinants
on Ig molecules fall into three categories: isotypic, allotypic, and idiotypic determinants.
Isotypes are antigenic determinants that characterize classes and subclasses of heavy-
chains and types and subtypes of light-chains. They are constant-region determinants that
distinguish each Ig class and subclass within a species. Allotypes are antigenic
determinants specified by allelic forms of the Ig. Allotypes are determined by the amino
acid sequence and corresponding three-dimensional structure of the constant region of the
Ig molecule and reflect genetic differences between members of the same species. This
signifies that not all members of the same species will have any particular allotype.
Idiotypes are unique antigenic determinants present on individual antibody molecules or
on molecules of identical specificity. Idiotypes are determined by the amino acid

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
13
sequence and corresponding three-dimensional structure of the variable region of the Ig
molecule. It reflects the antigen-binding specificity of any particular antibody molecule.
The individual determinant is called indiotope, and the sum of the individual idiotopes is
the idiotype.
Immunoglobulin classes
Five classes of Ig are described based on their ability to carry out various effector
functions, their average serum concentrations, and their half-life.
IgM predominates in early immune responses, and can exist as monomeric IgM
(expressed as a membrane-bound antibody on the B-cell) or pentameric IgM together
with a J chain. IgM is found in the blood and lymph fluid and is the first antibody
produced in a primary response to an antigen by the neonate, naïve B cells, and during a
primary immune response. Because of its high valency, pentameric IgM is more effective
than the other classes in neutralizing pathogens, agglutination and activation of
complement [50]. IgM does not cross the placenta.
IgG is the most abundant class in serum (75% of serum Ig), important in clearing antigen,
and is the only class that crosses the placenta (Table 1). Maternal IgG, from the placental
transport, protects the child during its early months of life. IgG fixes complement and
binding of IgG to Fc receptors on phagocytic cells (monocytes, macrophages) results in
their opsonisation. The IgG subclasses in humans differ in the number of disulfide bonds
and length of the hinge region, and are named IgG1, IgG2, IgG3 and IgG4. IgG1 makes

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
14
up most of the total IgG (66%), followed by IgG2 (24%), IgG3 (7%) and IgG4 (3%) [51].
IgG1, IgG3 and IgG4 cross the placenta and play an important role in protecting the new
born from infection. IgG3, however, is the dominant complement activator followed by
IgG1 and IgG2. One prominent feature of IgG3 is its 11 interchain disulfide bonds. IgG4
does not activate complement. Furthermore, IgG1 and IgG3 bind Fc receptors on
phagocytic cells with high affinity, thus mediate opsonisation while IgG4 has an
intermediate affinity, and IgG2 low affinity (Table 1).
Table 1. Selected functional properties of human immunoglobulins
+ to +++, increasing activity. – No activity. ? Questionable
IgA is predominant in external secretions; breast milk, mucous, saliva, tears,
genitourinary and digestive tract. It is important in mucosal immunity. In humans, two
subclasses are known; IgA1 and IgA2. IgA1 is monomeric while IgA2 can polymerize

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
15
into multimers. While serum IgA is predominantly monomeric in nature, secretory IgA is
polymeric, exists as a dimer or tetramer linked by disulfide bonds to the J chain and
secretory components. Secretory IgA is found on mucosal surfaces (lining of the
respiratory, gastrointestinal, genitourinary tracts) and can be considered an important first
line of defence against invading pathogens [52]. Human colostrum and milk contain a
very high concentration of secretory IgA and therefore, mother’s milk (which contains
secretory IgA against a wide range of microbial antigens) is able to protect the child
against mucosal pathogens [52].
IgD and IgE are the least abundant in the serum. IgD, as IgM, is the major membrane-
bound antibody on mature B cells. IgD does not bind complement and its exact role in
serum is uncertain.
IgE mediates mast-cell degranulation. It binds tightly to Fc receptors on basophils and
mast cells, and as a result, is involved in allergic reactions. IgE mediates the immediate
hypersensitivity reactions that are responsible for the symptoms of hay fever, allergy,
hives, asthma, and anaphylactic shock. IgE also plays a role in parasitic diseases.
Eosinophils have Fc receptors for IgE and binding of eosinophils to IgE-coated helminths
results in killing of the parasite. Mast cells are needed to clear intestinal helminthic
infections [53] and, when infected, IgE-deficient mice have higher burdens of
Schistosoma mansoni [54]. Elevation of P. falciparum-specific and total IgE in severe
malaria disease had been reported [55-56] while P. falciparum-specific IgE response also
seems to contribute to the control of parasites [57-58].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
16
Effector functions mediated by antibodies
Antibodies, generally, do not kill pathogens by binding to them. They recognize
pathogens and invoke responses (effector functions) that remove or kill pathogens. The
variable region of the molecule (Fab) helps to bind to antigens while the H chain region
(Fc) is responsible for its interaction with other cells that results in the effector functions
of the humoral response. Antigen binding by the antibodies is the primary function of
antibodies. The binding of Ig to various cell types (phagocytic cells, lymphocytes), which
have Ig receptors can activate the cells to perform effector functions. There are four
major effector functions that enable antibodies to remove or kill pathogens:
Opsonisation promotes antigen phagocytosis by monocytes, macrophages and
neutrophils. Neutralization or blocking – antibodies can prevent pathogen adherence.
Blocking of viral and bacterial adherence to mucous membrane is the major defensive
role of IgA in secretions. Complement activation – the important by-product of the
complement system is a protein fragment called c3b, which binds non-specifically to cell-
and antibody-complexes near the site at which the complement was activated. The
collaboration between antibody and the complement system is important to the
inactivation and removal of antigens and in the killing of pathogens. Antibody-
dependent cell mediated cytoxicity (ADCC) – linking of antibody bound to target cells
with the Fc receptors of a number of cell types particularly NK cells, can direct the
cytotoxic activities of the effector cell against the target cell.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
17
Fc receptors
BCR and TCR are the receptors involved in antigen recognition by cells of the immune
system. Fc receptors (FcR) bind the Fc part of the antibodies [59] and thus play a role in
immune regulation as they serve to link antibody-mediated immune responses with
cellular effector functions. FcR exist in every Ig class, FcγR bind IgG, FcαR bind IgA,
FcεR bind IgE, FcµR bind IgM, and FcδR bind IgD [59]. There are two different classes
of FcγRs, categorized according to the receptors’ affinity for specific IgG subclasses and
the type of signalling pathway they trigger [60-61]. The activating receptor contains
intracytoplasmic activation motifs called immunoreceptor-tyrosine-based activation motif
(ITAM) involved in triggering activating signalling while the inhibitory receptor
transmits their signals through an immunoreceptor-tyrosine-based inhibitory motif
(ITIM) involved in down-regulating signalling [61]. Innate immune effector cells
(monocytes, macrophages, DCs, basophils and mast cells) express both activating and
inhibitory FcγRs. Activating FcR trigger innate immune functions resulting in the release
of pro-inflammatory cytokines and an increased phagocytic capacity; in contrast anti-
inflammatory cytokines downregulate the activating FcR expression by increasing
FcγRIIb, and thus creating a balance between the activating and inhibiting receptors [62].
Since FcR are important players in regulating immunity, they are at the forefront of
immunological research [63] and are new targets for new immunotherapeutic design [64].
In all mammalian species studied to date, four different classes of Fc receptors have been
defined known as FcγRI (CD64), FcγRII (CD32), FcγRIII (CD16) and FcγRIV (Figure 3)
the latter only found in mice [61]. The genes encoding the Fc-binding chains of each of

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
18
the FcγRs are located on chromosome 1q21-24. FcγRI is expressed on monocytes,
macrophages, neutrophils and has the highest affinity for IgG and is the only FcR that
binds monomeric IgG. FcγRII and FcγRIII have low intrinsic affinity for monomeric IgG,
binds IgG in the form of immune complexes and due to their polymorphisms; they
increase the IgG binding affinity. Both FcγRII and FcγRIII interact with human IgG1 and
IgG3, whereas FcγRII is the sole FcγR class capable of binding human IgG2 complexes
[65]. FcγRIIIb exhibits the genetic polymorphisms FcγRIIIb-NA1/NA2, coded for
different capacities of IgG binding and phagocytosis [66]. Both FcγRII and FcγRIII have
been demonstrated on neutrophils, eosinophils, monocytes and macrophages. Signalling
through FcγRIII on NK cells and monocytes triggers ADCC and the production of IFN-γ
[67].
Figure 3. The family of Fc receptors for IgG. Both human and mice FcRs can be distinguished by their affinity for antibody Fc fragment and the signalling pathways induced. Adapted from Nimmerjahn and Ravetch [61].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
19
FcγRIIa
The human FcγRII is a 40 kDa glycoprotein expressed on monocytes, macrophages,
basophils, endothelial cells in placenta, platelets, and B cells and initiates phagocytosis,
ADCC and cellular activation [66]. At least six human FcγRII isoforms have been
identified which are encoded by a total of three genes, FcγRIIa, FcγRIIb, and FcγRIIc,
located at chromosome 1q23 [66]. The FcγRIIa gene has two single-nucleated
polymorphisms (SNPs) at position 27 and 131 on the amino acid sequence.
The SNP in the FcγRIIa gene (G494A) (rs1801274) is of interest because of its functional
consequences. A SNP at amino acid position 131 of the mature protein results in either
histidine (His131) or arginine (Arg131). These alleles are codominantly expressed;
therefore, an individual might phenotypically express RR, HR, or HH. This change alters
the ability of the receptor to bind certain IgG subclasses. FcγRIIa-H131 has a higher
affinity for human IgG3 and is the only human FcγR that efficiently binds IgG2, whereas
FcγRIIa-R131 binds IgG2 weakly. The clinical importance of FcγRIIa polymorphism has
been evaluated for encapsulated bacterial infections, which showed an association
between FcγRIIa-His/His131 and protection, whereas the poorly IgG2-binding allotype
FcγRIIa-Arg/Arg131 is associated with increased susceptibility to bacteraemia [68-69].
However, FcγRIIa polymorphism could constitute additional factor that might influence
the clinical manifestation of systemic lupus erythematosus [70-71]. Furthermore, IgG
may act via the activating FcγRIIa to regulate the CD1 expression profile of DCs [72].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
20
Malaria
The name malaria is derived from the Italian ‘mal’aria’, which means ‘bad air’ from the
early association of the disease with marshy surroundings [73]. Malaria is the most
widespread and persistent parasitic disease, which affects human populations throughout
the world and especially in tropical and sub-tropical countries. Each year, an estimated
300-500 million clinical cases occur, and between 1-3 million deaths, primarily among
children and pregnant women [74-75]. Every 30 second, a child dies of malaria
somewhere in the world [76], resulting in a daily loss of more than 2000 young lives
worldwide [77].
Malaria is caused by the intracellular parasitic protozoa of the genus Plasmodium and is
transmitted by the bite of an infected female Anopheles species mosquito [78]. Infection
can also occur through blood transfusion or congenital transmission. There are four
species of malaria parasites that infect humans: P. falciparum, P. vivax, P. ovale and P.
malariae. Recently, the discovery of P. knowlesi malaria in humans [79] suggests a
probable fifth human malaria parasite [80-82]. Accumulating evidence (from Malaysia,
Singapore and Philippines) suggest a potential public health importance due to
misdiagnosis of P. knowlesi malaria, short-term travel, immigration and zoonotic
transmission [82-88]. Further evidence shows that P. knowlesi infections in humans are
widely distributed in Malaysian Borneo and not newly emergent [89]. The most severe
form of human malaria is caused by P. falciparum. Malaria is a devastating infectious
disease that not only affects the health system, but also slows the rate of long-term
economic growth and development. The emergence of drug-resistant strains of the
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
21
parasite has exacerbated the situation, and global climate change, disintegration of health
services; human migration and population displacement have also contributed. Recently,
evidence of artemisinin-resistant malaria report from Western Cambodia confirm fears
that artemisinin is losing its effectiveness in the area [90-91].
The life cycle of Plasmodium malaria
The malaria parasite life cycle is complex involving the sexual stage and the asexual
stages both in the mosquito and vertebrate host respectively. At the time the female
infected mosquito takes a blood meal, sporozoites are injected into the blood stream
(Figure 4). Sporozoites migrate to the liver within 2-30 minutes, invade hepatocytes and
multiply into exo-erythrocytic merozoites. Each sporozoite gives rise to thousands of
merozoites which are released into the blood stream at hepatocyte rupture. The released
merozoites invade other erythrocytes, starting a new cycle of schizogony. After several
cycles, some merozoites develop into gametocytes, the sexual stages, which cause no
symptoms but are infective to the mosquitoes [78]. Cyclical fevers are the hallmark of
malaria, and typically occur shortly before or at the time of red blood cell (RBC) lysis, as
schizonts rupture to release new infectious merozoites. This occurs every 48h in P. vivax,
P. ovale and P. falciparum and every 72h in P. malariae infections. Intense fever is
accompanied by nausea, headaches and muscular pain, amongst other symptoms. In
patients infected with P. vivax and P. ovale, relapse may recur months to years after
initial infection. This is caused by re-activation of the silent liver-stage form of the
parasite (hypnozoites).

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
22
Figure 4. Life cycle of the malaria parasite. Adapted from Lozano and Patarroyo [92].
Clinical features of malaria
The erythrocytic cycle represents the only stage of the malaria life cycle that is
responsible for the clinical manifestation of malaria. Clinical manifestation of malaria can
be summed into mild (uncomplicated) and severe (complicated) malaria according to the
World Health Organisation set criteria (WHO) [93-94]. Mild malaria is defined with
headache, cough, diarrhoea, fever, muscular pain, nausea and no signs of severe
manifestation. Renal failure, hypoglycaemia, hepatic dysfunction, severe malarial
anaemia (haemoglobin <5 g/dL or haematocrit <15%), pulmonary oedema, convulsions

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
23
and shock are complications in severe malaria (Table 2). Cerebral malaria is a frequent
presentation of severe P. falciparum infection and has been attributed in part of the
unique ability of the parasite to alter the surface of infected red blood cell (iRBC) so that
they can bind to endothelial surfaces causing obstruction of cerebral blood flow, leading
to coma or other neurological phenomena, such as seizures and elevated intracranial
pressure [95]. Observations suggest that pro-inflammatory cytokines such as tumour
necrosis factor α (TNF-α) and nitric oxide (NO) induced by parasite material may also
contribute to the pathogenesis of cerebral malaria [96-97].
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
24
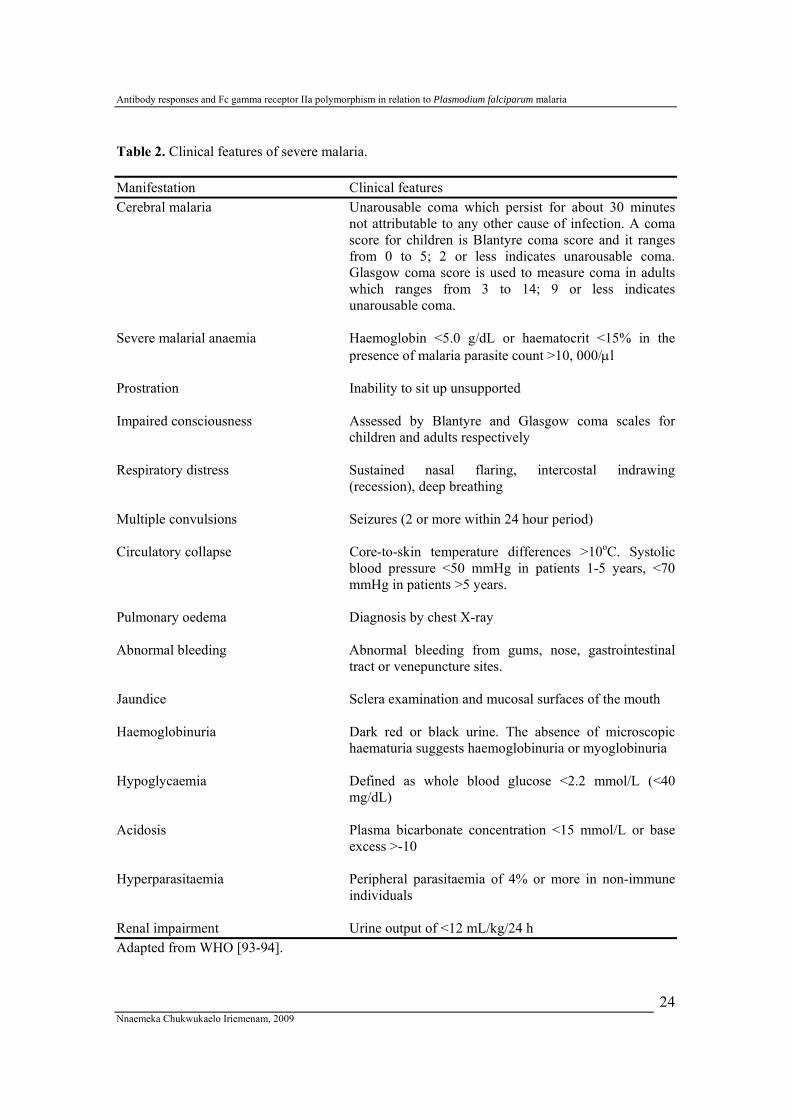
Table 2. Clinical features of severe malaria. Manifestation Clinical features Cerebral malaria Unarousable coma which persist for about 30 minutes
not attributable to any other cause of infection. A coma score for children is Blantyre coma score and it ranges from 0 to 5; 2 or less indicates unarousable coma. Glasgow coma score is used to measure coma in adults which ranges from 3 to 14; 9 or less indicates unarousable coma.
Severe malarial anaemia Haemoglobin <5.0 g/dL or haematocrit <15% in the
presence of malaria parasite count >10, 000/µl Prostration Inability to sit up unsupported Impaired consciousness Assessed by Blantyre and Glasgow coma scales for
children and adults respectively Respiratory distress Sustained nasal flaring, intercostal indrawing
(recession), deep breathing Multiple convulsions Seizures (2 or more within 24 hour period) Circulatory collapse Core-to-skin temperature differences >10oC. Systolic
blood pressure <50 mmHg in patients 1-5 years, <70 mmHg in patients >5 years.
Pulmonary oedema Diagnosis by chest X-ray Abnormal bleeding Abnormal bleeding from gums, nose, gastrointestinal
tract or venepuncture sites. Jaundice Sclera examination and mucosal surfaces of the mouth Haemoglobinuria Dark red or black urine. The absence of microscopic
haematuria suggests haemoglobinuria or myoglobinuria Hypoglycaemia Defined as whole blood glucose <2.2 mmol/L (<40
mg/dL) Acidosis Plasma bicarbonate concentration <15 mmol/L or base
excess >-10 Hyperparasitaemia Peripheral parasitaemia of 4% or more in non-immune
individuals Renal impairment Urine output of <12 mL/kg/24 h Adapted from WHO [93-94].
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
25
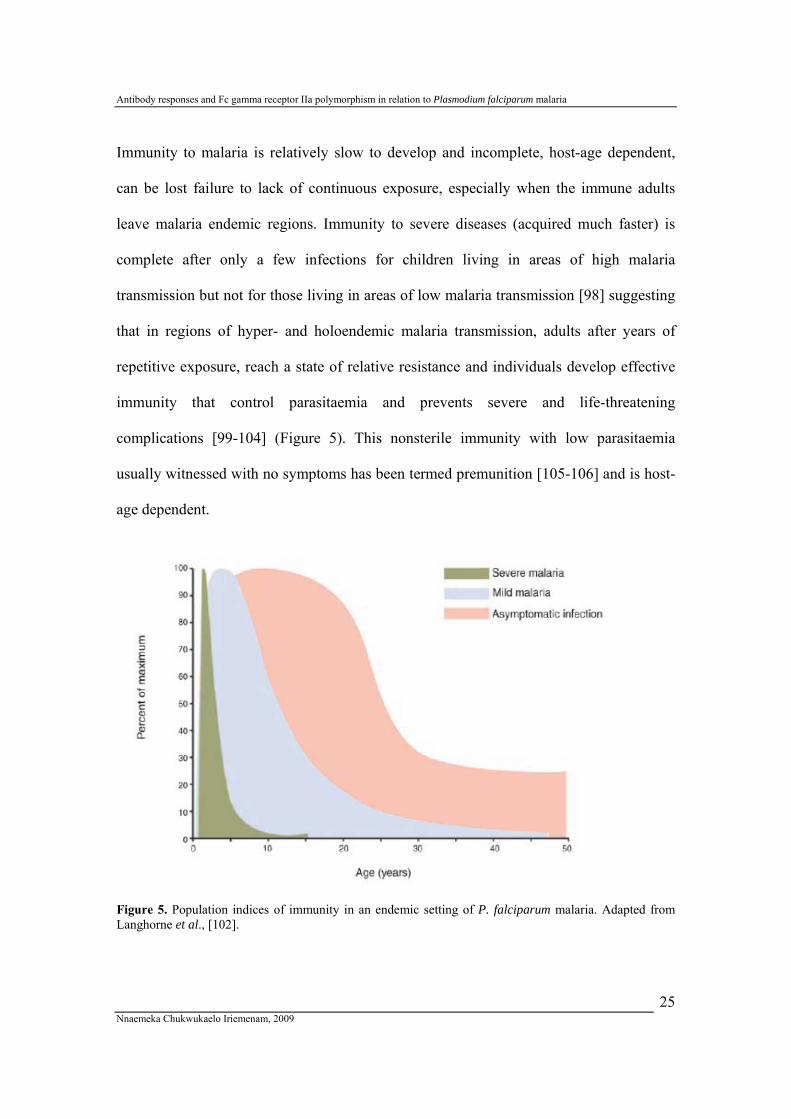
Immunity to malaria is relatively slow to develop and incomplete, host-age dependent,
can be lost failure to lack of continuous exposure, especially when the immune adults
leave malaria endemic regions. Immunity to severe diseases (acquired much faster) is
complete after only a few infections for children living in areas of high malaria
transmission but not for those living in areas of low malaria transmission [98] suggesting
that in regions of hyper- and holoendemic malaria transmission, adults after years of
repetitive exposure, reach a state of relative resistance and individuals develop effective
immunity that control parasitaemia and prevents severe and life-threatening
complications [99-104] (Figure 5). This nonsterile immunity with low parasitaemia
usually witnessed with no symptoms has been termed premunition [105-106] and is host-
age dependent.
Figure 5. Population indices of immunity in an endemic setting of P. falciparum malaria. Adapted from Langhorne et al., [102].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
26
In holoendemic areas, a small proportion of infections progresses to severe malaria (life-
threatening complications like severe malarial anaemia and cerebral malaria) while a
larger population become ill with fever when infected, but eventually recovers [107]
(Figure 6). The presence of P. falciparum parasitaemia at any given time therefore may
not correlate well with clinical disease in areas of holoendemicity as children may
harbour high parasite loads with no malarial symptoms [104].
Figure 6. Progression of malaria disease in a malaria-endemic region. Adapted from MalariaGEN [107].
Malaria endemicity
Malaria endemicity is classified on the basis of frequency of infection of individuals with
the parasite (parasite rate) and the frequency of enlarged spleen in children (spleen rate)
[108]. Four groups have been identified namely:
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
27
• Holoendemic – these areas/regions have intense all-year round malaria
transmission. The parasite rate in the one-year group is over 75% during the peak
transmission season. The spleen rate in adults is either high or low and the
population is relatively immune. Parasite density decreases with increase in age.
• Hyperendemic – these areas/regions have seasonal transmission. The parasite rate
and spleen rate in 2-9 years is between 51-75% during the transmission season.
The population’s immunity does not confer adequate immunity irrespective of the
age.
• Mesoedemic – these areas/regions have some malaria transmission. Occasional
epidemics could constitute a public burden due to low immunity acquisition. The
parasite rate and spleen rate in 2-9 years is 11-50% during transmission seasons.
• Hypoendemic – these areas/regions have limited or little transmission. The
population have little or no immunity to malarial disease. The parasite rate and
spleen rate in 2-9 years is <10%.
Malaria is also commonly classified epidemiologically as stables or unstable (Figure 7)
[109-110]. Stable malaria has the characteristics seen in holo-and hyperendemic areas
while unstable malaria has the characteristics seen in meso-and hypoendemic areas. In
stable malaria the level of immunity is high after childhood and a form of equilibrium is
maintained throughout life if the individual do not live outside the region. In unstable
malaria, equilibrium is not attained in the population and epidemics therefore occur when
mosquito breeding becomes seasonally prolific.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
28
Figure 7. P. falciparum malaria risk defined by annual parasite incidence with temperature and aridity. Dark grey areas represents stable transmission, middle grey areas (unstable transmission) while light grey represents no risk. The data shown are age-standardized (PfPR2–10) and shown as a continuum from 0–100%. Adapted from Tatem et al. and Guerra et al. [110-111].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
29
Malaria Immunology
The exact mechanism by which immunity to malaria is achieved remains a subject of
discussion. The complex life cycle of Plasmodium sp that involves two different hosts
and different stages makes it more complicated. However, it is believed that both cell-
mediated and humoral immune responses are involved.
The pre-erythrocytic stage
Immunity to pre-erythrocytic stages is believed to be mediated by both antibodies and
cellular mechanisms [112]. Antibodies directed against sporozoite surface proteins could
potentially protect either through opsonisation leading to clearance before reaching the
hepatocyte, or through interfering with the process of hepatocyte invasion [113]. Both
CD8+ T cells and CD4+ T cells are involved in protective immunity against malaria but in
different stages. In rodent models, CD8+ T cells have been implicated as the principal
effector cells, and IFN-γ as a critical effector molecule. IL-4 secreting CD4+ T cells are
required for induction of the CD8+ T-cell responses, and Th1 CD4+ T cells provide help
for optimal CD8+ T-cell effector activity. γδT cells, NK cells and NKT cells also play a
role [114].
The erythrocytic stage
CD4+ T cells are crucial in immunity against asexual stage, producing cytokines involved
in the activation of innate immunity and help activated B cells to produce antibodies
essential for parasite clearance. Although blood-stage protection is mediated by
antibodies other protective mechanisms are also used including innate immunity, IFN-γ

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
30
and CD4+ T cells [115-116]. IFN-γ produced by CD4+ T cells to specific blood-stage
antigens has been shown to be associated with protection against re-infection [117].
CD4+ T cells secretion of IFN-γ might also help to induce cytophilic IgG blood-stage-
specific antibodies and assist in the clearance of infected RBCs [118]. The absence of
MHC molecules on RBC indicates the importance of humoral immune responses against
the erythrocytic stages. The role of B cells in immunity against malaria was established in
mice lacking B cells, which were unable to eliminate blood stage malaria infections [119]
while one study showed that B cells are not required for the control of early acute
parasitaemias, but appear to be important for the final clearance of the infection, probably
by producing specific antibodies against the parasite [120].
Invasion of RBCs by merozoites is a key step in the establishment of malaria infection
and therefore is likely to be an important target of protective immune responses [113].
The process involves a complex cascade of events involving interactions between the
RBC and parasite proteins (Figure 8) including merozoite surface proteins (MSP-1 to 11)
[92, 121-126], RBC surface (PfEMP1, Pf332, PfAARP1, RIFINS, SURFINS) [122, 124,
127-129], parasitophorous vacuole (GLURP) [122, 124, 127, 130], EBA and AMA-1
[122, 124, 127, 131], etc. Given the short time that many of these proteins are exposed to
the host immune system, it is likely that antibodies are the main stay of immunity against
merozoites [113].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
31
Figure 8. The erythrocytic cycle with some merozoite representation describing the main proteins expressed. Adapted from Bolad and Berzins [124] and Patarroyo [121].
The importance of antibodies in P. falciparum malaria immunity
Not only are antibodies markers of exposure but also they are effectors of protection. The
classic example of the importance of antibodies in protective immunity against P.
falciparum infection was established by Cohen et al. [132] in which passive transfer of
immunoglobulins by the intramuscular route contributed to the control of parasite density
and protection against P. falciparum clinical malaria. In a similar study, gamma globulin
from adult West Africans was administered to East African subjects with severe P.
falciparum infections which led to abrupt reduction in parasite density and recovery from
clinical illness [133]. In Thai patients, the protective effect of African IgG antibodies
against P. falciparum malaria was also shown by passive transfer [134] and antibodies
from immune Africans were able to control asexual blood parasites in Saimiri monkeys
SURFINS

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
32
[135]. To date, the exact mechanisms by which malaria specific antibodies interfere with
the development and/or multiplication of the asexual stages of P. falciparum in protection
is still unclear, and the actual target antigens of protective antibodies remain uncertain.
Several seroepidemiological studies in different malaria endemic areas have supported
and also confirmed the association of IgG antibodies especially of the cytophilic
subclasses (IgG1 and IgG3) in protection [136-141]. Accumulating results from different
populations have also suggested a protective role of IgG2 antibodies in malaria infection
probably through its binding to the FcγRIIa-H131 [142-144]. Uncertainty remains as to
which IgG subclass antibody is more important in protective immunity against malaria.
However, in clinically protected individuals, the cytophilic antibodies were more
pronounced [136] and binding of antibodies to infected RBCs results in their opsonisation
facilitating their phagocytosis by monocytes/macrophages [145-147]. A number of
potential mechanisms has been suggested by which antibodies mediate parasite
neutralisation [122-124] including complement-mediated lysis of infected RBC,
preventing processing of invasion proteins or blocking their erythrocyte-binding sites
[113]. Inhibitory antibodies are thought to act by inhibiting erythrocyte invasion through
targeting merozoite surface antigens [148]. Children can acquire growth-inhibitory
antibodies at young age [149], and a correlation of plasma antibody-mediated growth
inhibition of blood stage P. falciparum with age has been shown [150]. The major
mechanism for antibody-mediated parasite neutralisation is thought to involve monocytes
or other leukocytes as effector cells [118, 124, 151], through antibody-dependent cell-
mediated inhibition (ADCI). In corporation with monocytes, the soluble factors (TNF-α,

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
33
NO) are released by the monocytes upon uptake of opsonised merozoites. But antibodies
by themselves neutralise parasites by interference with the merozoite invasion [152].
Target blood-stage antigens
The clinical symptoms of malaria manifest only during the blood-stage and much
attention has been given to the parasite molecules that interact with the host cells during
RBC invasion as potential targets of host immune responses (reviewed by Berzins and
Anders [122]). The important antigens of parasite neutralising antibodies are expressed
during the merozoite and trophozoite stages (Figure 8) [153-154] that play a role in RBC
invasion and are thought to be targets of immunity (Table 3). While antibodies to AMA-
1, Pf155/RESA and Pf332 inhibit merozoite invasion and parasite growth on their own
[131, 155-156], antibodies to MSP-3 and GLURP appears to be dependent on their
interaction with Fcγ receptors on monocytes or other effector cells [157-158].
Table 3. Selected asexual blood-stage targets of P. falciparum malaria
Adapted from Bolad and Berzins [124] and Taylor-Robinson [154].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
34
P. falciparum, the most virulent of the four malaria parasites of humans, adheres to a
molecule called chondroitin sulphate A (CSA) on the surface of syncytiotrophoblasts
[159-160], and women with higher levels of anti-adhesion antibodies against CSA-
binding parasites are protected from malaria infection during pregnancy [159-162] by
blocking parasite adhesion to placental CSA [163]. One important feature of P.
falciparum malaria is the switching of its variant surface antigens (VSA) [164]. The
mechanism of this is still not known but believed to be one way the parasite avoid the
immune response. The importance of VSA in naturally acquired protective immunity to
P. falciparum malaria has been shown and parasites causing clinical disease express
VSA to which the patient has no pre-existing antibody response. Thus, the immune
system responds to a clinical disease episode by mounting an antibody response with
specificity for the VSA expressed by the parasites causing it [165].
Antibodies specific for the VSA are of critical importance to protection [166] and VSA
expressed by parasites causing pregnancy-associated malaria (PMA), characterised by the
accumulation of iRBC in the placenta, are fundamentally different from all other VSA
(reviewed by Hviid [167]). These parasites express a P. falciparum erythrocyte
membrane protein 1 (PfEMP1) VSAPAM that binds to CSA. The identification of a
distinct PfEMP1 variant (VAR2CSA) as the dominant variant surface antigen and shown
to be a clinically important target for protective immune response to PAM raises interest
in developing preventive strategies [168]. VAR2CSA is a large polymorphic protein (350
kD) consisting of six Duffy-Binding-like (DBL) domains and several inter-domain
regions, expressed on the surface of infected erythrocyte on CSA from infected placentas

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
35
[168-169]. In areas of intense malaria transmission, antibody levels to VSACSA increase
with gravidity, block adhesion of iRBC to CSA [170] and protect against low-birth
weight and maternal anaemia while in regions of low endemicity, the antibody levels did
not appear to confer protection against placental malaria infection [171]. However,
despite the structure and interclonal conservation of VAR2CSA among other PfEMP1,
and with constraints on recombinant protein production, significant challenges still exist
concerning the development of a VAR2CSA-based vaccine [172]. Defining smaller parts
of the molecule which will induce antibodies against DBL domain may inhibit CSA
binding of the parasite [173].
B-cell memory in malaria
The short-lived nature of immune responses to P. falciparum blood-stage antigens in
malaria endemic regions questions the durability of memory-B cell [174]. A previous
study suggested that B-cell memory is a potential determinant of levels of antibodies to
malarial antigens in many individuals [175] and a relationship between memory-B cell
frequencies and serum antibody levels to P. falciparum extract had been reported [176].
A prior study in children indicates that antibodies against merozoite antigens have very
short half-live [177] and individuals with malaria have profound disturbances in B-cell
homeostasis [178]. Furthermore, a recent study denotes that children most likely have
short-lived plasma cells, thus, experience a rapid decline in antibody levels while older
children have longer-lasting antibody responses that depend on long-lived plasma cells
[179]. When malaria remerged in Madagascar after a long period of complete control,
people present 30 years earlier during malaria exposure were much more resistant to
clinical disease than the children [180]. Data from mice malaria study suggests that B-cell

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
36
response to a second infection is more efficient than the primary response, generating
long-lived plasma cells making the second encounter with parasite more efficient [181].
Acquired immunity to falciparum malaria is believed to be lost without repeated exposure
[102, 104]. However, repeated exposure to malaria may not result in long-lasting B-cell
memory [175]; perhaps it may result in specific memory-B cells being converted into
effector cells and the persistence of effector mechanisms [182]. The ability of the
immune environment to support long-lived plasma cells may gradually increase with age,
such that older individuals have higher proportion of long-lived plasma cells, enabling
antibodies to be continually produced without restimulation by persistent antigen [179].
Obviously, more studies of memory-B cell responses to human malaria are needed to
elucidate the inadequate understanding of naturally acquired immunity [102, 104].
The haemoglobinopathies
The haemoglobinopathies, disorders of haemoglobin structure production, were the first
genetically determined conditions to be implicated in malaria protection [183]. The
haemoglobinopathies can be divided into two categories: those associated with the
production of structurally variant forms of haemoglobin (HbS, C, E), and those caused by
the reduced production of normal α-and β-globin – the α-thalassaemias and β-
thalassaemias respectively [184-185]. The clinical effects of these conditions are highly
variable.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
37
Haemoglobin variant
Haemoglobin S
Sickle-cell disease is a blood disorder characterized by red-blood cells that assume an
abnormal, rigid, sickle shape. Mutation of the β-chain of the globin due to single base
pair gene and its substitution of a single amino acid (Glu→Val) results in reduced
solubility of the deoxyhaemoglobin molecule and erythrocytes assume irregular shapes
[186]. The homozygous (HbSS) are associated with severe sequelae and reduced life
expectancy while the heterozygous have a protective advantage over clinical malaria
episodes [187-190]. The mechanism whereby HbAS mediates protection remains unclear
though studies have described a reduced parasite growth and density [191], enhanced
phagocytosis of ring-parasitized mutant erythrocytes [192], an impaired cytoadherence of
falciparum-infected erythrocytes containing sickle haemoglobin [193] and higher titres of
IgG antibodies [194].
Haemoglobin C
Haemoglobin C is abnormal haemoglobin with substitution of a lysine residue for
glutamic acid residue at the 6th position of the β-globin chain. This mutated form reduces
the normal plasticity of host erythrocytes causing a haemoglobinopathy. Although HbAC
is asymptomatic, HbCC causes mild haemolysis, splenomegaly, or gallstones [195].
Recent studies appear to show selected advantage of homozygous HbCC [195-197].
Modiano et al. showed that the protective effect of HbAC was only 30% as compared to
>90% in HbCC [197]. The extent to which HbC reduces the risk of severe malaria and of
its variable symptoms in areas of different endemicity is yet to be established. However,

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
38
it is believed that regarding HbC, there is reduced ability of P. falciparum parasites to
grow and multiply in variant RBCs [198] and HbC-containing red-blood cells have
modified displays of malaria surface proteins that reduce parasite adhesiveness which
could reduce the risk of severe disease [199].
Haemoglobin E
Haemoglobin E, resulting from a single point mutation (Glu→Lys) at codon 26 of the -
globin gene, is common in Southeast Asia. Like HbC, the homozygous HbE is relatively
benign. A genetic analysis from Thai population revealed that HbE β26 Glu→lys, the
most frequent variant in Southeast Asia, has reached its current frequency in less than
5000 years [200]. Chotivanich et al. cultured P. falciparum parasites in media containing
various mixtures of normal and variant RBCs at relatively high parasite densities
designed to reflect progression to heavy parasitaemias and severe infection. Only 25% of
HbAE were susceptible to invasion suggesting the possibility that HbAE might protect
against severe malaria by limiting the ability of infections to achieve higher parasite
densities [201].
The thalassaemias
The thalassaemias are classified according to which chain of the haemoglobin molecule is
affected. In α thalassaemias, production of the α globin chain is affected, while in β
thalassaemia production of the β globin chain is affected. Thalassaemia produces a
deficiency of α or β globin. β globin chains are encoded by a single gene on chromosome
11 while α globin chains are encoded by two closely linked genes on chromosome 16.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
39
Few studies suggest a protective advantage of α thalassaemia over mild clinical disease
[202-203]. Unlike HbAS, which protects against all forms of disease, the effect of α
thalassaemia appears to be relatively specific for severe malarial anaemia [203-204]. α
thalassaemia is associated with complement receptor 1 (CR1) production [205], and
could protect against malaria anaemia via reduction in CR1-mediated rosetting.
The ABO blood group system
The ABO blood group system is the most mysterious, genetic polymorphism in humans
[206]. Relationship between ABO blood groups and susceptibility to malaria is
controversial due to contradictory results [206-207]. However, parasitized erythrocytes
form rosettes more readily with RBCs of A, B or AB groups than with O group [208-209]
and are associated with severity of clinical disease [210] with the development of
cerebral malaria [211]. Furthermore, recent data reveals that blood group O protects
against severe P. falciparum malaria through the mechanism of reduced rosetting [212].
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
40
Related background
Epidemiology of malaria in stable and unstable malaria transmissions
The transmission pattern of malaria normally governs the development of clinical
immunity to malaria. In stable malaria endemic area, a high entomological inoculation
rate (EIR) is often associated with increase in the incidence of parasitaemia and fever
[213], and parasitaemia is most common in young children, with the incidence of
parasitaemia decreasing steadily with age. Adults, however, have latent parasitaemia but
hardly develop clinical malaria. In unstable transmission settings, malaria transmission is
very seasonal and fluctuating, while in stable transmission settings it is stable over the
seasons or years. Children less than 5 years and especially primigravidae are known to be
more at risk to malaria disease due to inadequate acquisition of immunity. In stable
endemic areas, the most frequent manifestation of malaria is severe malarial anaemia
[214] which peaks at 6-12 months after trans-placental maternal immunity has faded
while cerebral malaria (the most fatal complication) peaks at 2-3 years, and by 5 years,
malaria morbidity declines [215-216]. In areas of unstable malaria transmission, like in
Sudan, the whole population is highly vulnerable. The mean age for severe malarial
anaemia is 5 years, cerebral malaria is about 14 years and the risk of clinical attack is
twice as high in the 5-20 age group and declines markedly after the age of 20 years [217-
219]. This decline has been suggested to be due to development of partial immunity after
having experienced a number of both symptomatic and asymptomatic infections [218].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
41
Ethnicity
Differences in susceptibility to malaria between ethnic groups suggest that host genetic
factors might have a role in resistance/susceptibility to malaria. Different studies have
reported differences in susceptibility to malaria between ethnic groups living in sympatry.
In Malaysia, the Orang Asli (aborigine) showed a lower susceptibility to malaria as
compared to other ethnic groups from the same region [220]. In Nepal, decreased malaria
morbidity in the Tharu people have been reported when compared to their sympatric
populations [221]. In Gambia, the Fulani showed lower incidence of malaria and higher
frequency of splenomegaly when compared to other sympatric groups albeit no apparent
socio-cultural differences and same exposure to malaria [222]. Other studies also
established lower parasite density and prevalence of malaria in the Fulani group [223-
224]. Studies from Burkina Faso, Mali and Sudan have also confirmed significant inter-
ethnic variation in susceptibility to malaria with the Fulani tribe developing less frequent
clinical malaria when compared to other ethnic groups living in sympatry (Mossi and
Rimaibé in Burkina Faso, Dogon in Mali and Masaleit in Sudan) [225-227].
In general, the Fulani have higher anti-malarial antibodies against liver-stage antigens
[228-229], blood-stage antigens [229-230] as well as crude P. falciparum blood-stage
extract [226, 231-232]. Increased numbers of specific IL-4- and IFN-gamma-producing
cells in the Fulani’s have also been suggested as contributing factor to the lower
susceptibility [232]. The mechanism behind the lower susceptibility to malaria by the
Fulani group remains unknown and studies continue to elucidate the unknown immuno-
genetic markers. A study from Sudan revealed a higher frequency of HbAS in non-Fulani

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
42
(Masaleit) than the Fulani [233], while another study suggests that the higher resistance
to malaria of the Fulani tribe could be derived from the functional deficit T regulatory
cells [234]. However, the low proportion of individuals with known genetic malaria
resistant factors like HbS, HbC, α−thalassaemia, G6PDA, HLAB*5301 in Fulani group
suggests lack of association with classic malaria-resistance genes and protection against
malaria in this group [235].
Antibody reactivities to blood-stage antigens in relation to malaria disease
Several asexual blood-stage antigens have been identified as possible vaccine candidates
(Figure 8) and their recognition in immune sera have been documented. A number of
sero-epidemiological studies has reported differences in IgG subclass patterns to different
asexual blood-stage antigens. MSP-2 is believed to induce very strong IgG3 responses
[236-238] in contrast to MSP-119 which induces IgG1 or mixed IgG1/IgG3 response
[239]. The most abundant IgG subclass responses to MSP-3 were IgG3, followed by
IgG1 and the presence of IgG3 antibodies to MSP-3 is associated with reduced risk of
clinical malaria [240-241], and long-lasting natural protection against malaria [242].
AMA-1 was recognised by predominantly IgG1 subclass antibodies in young children
and adults [243], and high antibody levels (IgG1 and IgG3) against GLURP were
associated with reduction in clinical malaria episode [241, 244-246].
Studies on naturally acquired antibody-mediated immunity to clinical malaria have
largely focused on the presence of antibody responses to individual antigens and their
associations with decreased morbidity. In a cross-sectional study, at peak and end of
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
43
malaria transmission from two villages with different levels of malaria transmission,
children who were high antibody responders to the selected malaria antigens were at
lower risk of clinical malaria than their counterparts classified as non-responders [247].
In a population of adult individuals living in hyperendemic area of Senegal, no
differences were seen between IgG1 and IgG3 subclasses before the rainy season, but
there were a significant decrease in specific IgG after the rainy season that affected IgG3
more than IgG1 [248]. A recent study on breadth (number of important targets to which
antibodies were made) and magnitude (antibody level measured in a random serum
sample) suggest that immunity to malaria may result from high titres of antibodies to
multiple antigenic targets [249] which was further suggested in another study [250].
However, the fine specificity or function of antibody responses is believed to be more
critical for the protection than the magnitude of antibody responses [251].
FcγRIIa and malaria
The importance of FcγRIIa dimorphism in relation to malaria, which indicates R/H131
polymorphism in regulating the clinical outcome of the disease, has been suggested but
shown with conflicting observations. In the Gambia, the HH131 genotype was
significantly associated with susceptibility to severe malaria while the presence of the
R131 allele, rather than the RR131 genotype, appeared to be an important factor
protecting from malaria disease [252]. Omi et al. found that the FcγRIIa-H/H131
genotype in combination with the FcγRIIIb-NA2 allele were associated with
susceptibility to cerebral malaria in Thai patients [253]. In Kenyan infants, FcγRIIa-
R/R131 carriers were found to be at lower risk to succumb to severe disease than the

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
44
FcγRIIa-R/H131 carriers [254]. In a cross-sectional study in western Kenya,
homozygotes for the R131 alleles were protected against high-density parasitaemia while
the H131 alleles were mildly protective and the FcγRIIa-131 polymorphism did not
protect against malaria anaemia [255]. Conversely, recent studies have suggested a
protective role of the HH131 genotype rather than the RR131 genotype in clinical malaria
from different malaria endemic regions (Burkina Faso, India and Brazil) probably
through its interaction with IgG2 [142-144].

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
45
The present study
Aim of the thesis
This study addresses the importance of antibodies in relation to malaria infection and
their effective interactions with FcγRIIa in both symptomatic and asymptomatic
individuals. Papers I and IV focused on the pattern of antibody responses in clinical
malaria while papers II and III centred on FcγRIIa polymorphisms in sympatric ethnic
groups.
The specific objectives were:
• To investigate a possible association between FcγRIIa-R/H131 polymorphism and
anti-malarial antibody responses and clinical outcome of P. falciparum malaria
among Sudanese patients.
• To study the interethnic differences in malaria susceptibility seen between the
Fulani and Dogon in Mali if it could be attributed to their FcγRIIa-R/H131
polymorphism and IgG subclass pattern of anti-malarial antibodies.
• To examine the influence of FcγRIIa-R/H131 polymorphism and IgG subclass
pattern of antibodies among sympatric Fulani and non-Fulani in a dry savannah
area of sub-Saharan Sudan.
• To analyse immunoglobulin G profiles of six leading blood-stage vaccine
candidate antigens in relation to clinical malaria outcome.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
46
Sudan
Country profile
Sudan is the largest and one of the most diverse countries in Africa, home to deserts,
mountain ranges, swamps and rain forests. Sudan has a population of 39.4 million with
an area of 2.5 million sq km (966,757 sq miles). The northern part has a desert climate
and rainfall is very infrequent, daytime temperatures are very high. The rainy season
varies between regions; rare in the north and frequent in the south. The human
development report for Sudan is 0.526, which gives the country a rank of 147th out of
177 countries [256]. Male life expectancy is 55.4 years while female is 57.8 years and
adult literacy is 50% [257]. Sudanese children suffer an under-five mortality rate of 112
deaths per 1,000 live births, an infant mortality rate of 81 deaths per 1,000 live births and
a maternal mortality ratio of 1,107 deaths per 100,000 live births [258]. In Sudan, malaria
transmission is very unstable, seasonal and the duration varies between north and south
Sudan (Figure 9). Malaria transmission is low in the north while it is moderate with
seasonal epidemic outbreaks in the south.
Daraweesh project
The Daraweesh project started as a collaboration between the Universities of Khartoum
(Sudan), Edinburgh (UK), Copenhagen (Denmark), and Brigham Young University
(USA) [217]. Daraweesh is situated on the Sudanese savannah, at the altitude of 603 m
above sea level, 16 km from Gedaref town, 80 km from the Ethiopian border and is a
region characterized by seasonal and unstable malaria transmission. The cost-cutting
measure is built on agriculture, and is mostly inhabited by a population of Fulani group

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
47
originating from Burkina Faso whose relations settled in Sudan over 100 years ago [217].
Daraweesh is characterized by wet and dry periods. The rainy season is short followed by
a long dry season extending over 9 months. Malaria incidences during the dry season are
very rare, while during the wet seasons, 20-40% of the population suffer at least 1
malaria attack. The risk of clinical malaria is much higher in ages 5-20 years than
individuals more than 30 years of age though all age-groups are affected. Daraweesh is a
hypo-endemic malaria area. More details of the demographic and social descriptions of
the study area, epidemiological settings can be found in previous publications [217-219,
259].
Figure 9: Distribution of endemic malaria and duration of transmission season in Sudan. The areas where the studies were conducted are marked with a red circle. Adapted from MARA/ARMA (www.mara.org.za).

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
48
Mali
Country profile
Mali is the seventh largest country in Africa, bordering Algeria on the north, Niger on the
east, Burkina Faso and the Côte d'Ivoire on the south, Guinea on the south-west, and
Senegal and Mauritania on the west. Mali has a population of 12 million with an area of
1,240,000 km². Mali is one of the world’s poorest nations rated 173 out of the 177
countries. The under 5 mortality rate is 219 per 1, 000 live births, maternal mortality ratio
is 1200 deaths per 100, 000 live births and the infant mortality rate is 121 deaths per 1,
000 live births. The human development report for Mali is 0.391, which gives the country
a rank of 168th out of 179 countries with data [260]. Male life expectancy is 45 years
while female is 48 years and adult literacy is 24% [261]. Mali experiences three types of
malaria transmission each year: (i) 6 months of seasonal transmission in the south; (ii) 3
months of transmission in the Sahelian area; and (iii) irregular transmission with
epidemics in the north (Figure 10).
Study area
The study area is located in the Mopti area about 850 km northeast of Bamako, the
capital of Mali. Details of the study area, epidemiological settings can be found in
previous publications [226, 231-232]. The study took place in four rural villages
(Mantéourou, Naye, Binédama, and Anakédié) where Fulani and Dogon ethnic groups
live in sympatry. The Mantéourou and Naye are divided into two subdivisions,
Mantéourou Peulh/Mantéourou Dogon and Naye Peulh/Naye Dogon-Dinsogou. The two
subdivisions are separated by 300–500 meters and inhabited either by Fulani or Dogon.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
49
The other two villages, Binédama and Anakédié, are exclusively populated by either
Fulani or Dogon, respectively, and are located approximately 1 km apart. Malaria
transmission is meso-endemic, with P. falciparum as the main cause of infection.
Transmission is seasonal and EIR of 0.38 infective bites per person per night has been
previously reported [226].
Figure 10: Distribution of endemic malaria and duration of transmission season in Mali. The area where the study was conducted is marked with a red circle. Adapted from MARA/ARMA (www.mara.org.za).

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
50
Methodology
The materials and methods, briefly described below, are properly described accordingly
in the respective papers.
Paper I
A total of 256 individuals, comprising 115 patients with severe malaria, 85 with mild
malaria and 56 malaria-free controls, were enrolled in a prospective clinical study over
two successive malarial transmission seasons. Human genomic DNA was purified using a
commercial DNA purification kit QIAmp® DNA blood mini kit and polymerase-chain
reaction (PCR) was performed for FcγRIIa-R/H131 polymorphism. Plasma samples were
tested for malaria-specific IgE, IgM, IgG and IgG subclasses using ELISA.
Paper II
Randomly selected asymptomatic Fulani and Dogon (164 respectively) were included in
this study. Human genomic DNA was extracted from filter papers using Chelex-100 and
PCR was performed for FcγRIIa-R/H131 polymorphism. ELISA was used to determine
total IgG subclasses and malaria-specific IgG subclasses.
Paper III
Two hundred and fifty one Fulani and 101 non-Fulani were genotyped for FcγRIIa-
R/H131 polymorphism. Plasma antibodies to four malaria merozoites (AMA-1, MSP-
23D7 and FC27, Pf332-C231) were measured using ELISA.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
51
Paper IV
Five hundred and fourty five individuals, aged 6 months to 65 years, were consecutively
enrolled in the study. Plasma levels of IgG and IgG subclases against six malaria antigens
(AMA-1, 3D7 MSP-2, FC27 MSP-2, MSP-3, GLURP-R0 and GLURP-R2) were
determined by ELISA.
Ethical permissions
The studies received ethical clearance from the ethical committees at the Faculty of
Medicine, University of Khartoum, Sudan, and the National Research Directorate of the
Sudanese Federal Ministry of Health, ethical committee of the Faculty of Medicine and
Pharmacy of Mali and the ethical committee of Karolinska Institute, Sweden.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
52
Results and discussion
FcγRIIa polymorphism and antibody responses in clinical malaria outcome (Paper I)
Fc receptors are expressed on the surface of all types of cells of the immune system. They
bind the Fc portion of Ig, thereby bridging specific antigen recognition by antibodies with
cellular effector mechanisms. FcγRIIa (the low affinity receptor), one of the three
receptors for human IgG, is believed to play a major role in eliciting monocyte- and
macrophage-mediated effector responses against blood-stage malaria parasites. The
importance of FcγRIIa dimorphism in relation to malaria, which indicates R/H131
polymorphism in regulating the clinical outcome of the disease, has been shown with
conflicting observations (reviewed by Braga et al. [262]).
In this study, we investigated a possible association between the FcγRIIa-R/H131
polymorphism and anti-malarial antibody responses with clinical outcome of P.
falciparum malaria among Sudanese patients. Our data showed that the frequency of
FcγRIIa-R/R131 genotype was significantly associated with severe malaria when
compared with patients with mild malaria. Furthermore, the frequency of FcγRIIa-
H/H131 genotype was statistically significantly associated with mild malaria, suggesting
that the FcγRIIa-H/H131 genotype might be associated with a reduced risk of severe
malaria, or possibly have a protective role against severe malaria. Recent data from
different endemic regions have also confirmed this result [142-144]. However, our data
are in contrast to those of earlier studies [252-254] which showed an association between
FcγRIIa-H/H131 genotype and susceptibility to malaria. These discrepant results may
most likely be explained by genetic differences between the populations studied, as well

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
53
as differences in gene–environment interactions and differences in patterns of malaria
transmission in the different study areas.
Cytophilic antibodies (IgG1 and IgG3) are believed to be influential in protective
immunity against malaria while non-cytophilic antibodies (IgG2 and IgG4) compete
against the available epitopes recognised by the cytophilics [136, 145]. Evidence showed
that in clinically protected individuals, cytophilic antibodies are the most dominant [136].
Sero-epidemiological studies from hyper- and holoendemic regions have also confirmed
this association [136-138]. Our data, from a meso-endemic setting, are in line with
previous data [136-141] regarding the association between cytophilic antibodies and
protection against natural exposure to P. falciparum malaria. While the FcγRIIa-R131
molecule shows a similar binding of the cytophilic subclasses [263], the H131 receptor
which binds IgG3 more efficiently, is the only FcγR that binds IgG2 efficiently [65, 263-
264]. We showed that IgG3 antibodies were more associated with reduced risk of severe
malaria in individuals with H/H131 genotype than in individuals with R/R131 genotype.
We also found an association with low level of IgG2, although it was weak taking into
account confounding factors such as sex and age. The importance of FcγRIIa in parasite
neutralizing events mediated by monocytes was indicated by Tebo et al. using THP-1
cells transfected with the 131H or 131R allele of the receptor [265]. The cells expressing
the 131R allele showed enhanced phagocytosis of P. falciparum infected erythrocytes
with sera containing high levels of IgG1 antibodies, while phagocytosis by cells
expressing the 131H receptor showed preference for sera containing high IgG3 antibody
levels. In antibody-dependent cell-mediated inhibition of P. falciparum growth in vitro,

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
54
the optimal parasite neutralizing activity by human monocytes was dependent on the
cooperation between FcγRIIa and FcγRIII receptors and only cytophilic IgGs were
potent, in agreement with immunoepidemiological findings [266].
Taken together, our study signified that the H/H131 genotype, which binds IgG3 more
efficiently, is less likely to be associated with severe malaria, while the R/R131 genotype
was associated with severe malaria in this population. The ability to develop clinical
immunity, however, appears to correlate much stronger with cytophilic antibodies
suggesting that these antibodies may play significant roles in parasite-neutralizing
immune mechanisms.
FcγRIIa polymorphism and IgG subclasses in relation to malaria (Paper II)
Studies have reported differences in susceptibility to malaria between ethnic groups
living in sympatry [220-227]. In Gambia, the Fulani showed lower incidence of malaria
and higher frequency of splenomegaly rates [222]. Studies in Burkina Faso extended the
results implying that Fulani are less parasitized, less affected by malaria and have higher
anti-malarial immune responses than the sympatric Mossi and Rimaibé ethnic groups
[229]. A study of the Fulani ethnic group in Mali also has confirmed this similar result
[226] and this relative resistance seems to be pathogen related and not a general hyper-
reactive immune system [231]. It was expected that the conventional haemoglobinopathy
resistance factors will be high in Fulani but the reverse was found [235]. In view of these
differences, we investigated the possible impact of FcγRIIa polymorphism in the ethnic

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
55
differences in malaria susceptibility seen between Fulani and Dogon in Mali and also
analysed both their total and malaria reactive IgG subclass profiles.
Our data showed a statistically significant difference with regard to the frequency of
homozygotes carrying the R/R131 genotype, which dominated in the Dogon group, while
the homozygotes R/R131 and H/H131 genotypes were evenly distributed in the Fulani
group. The Fulani also showed significantly higher levels of anti-malarial IgG1, IgG2 and
IgG3 antibody subclasses when compared with the Dogon. However, in some Fulani
individuals, a higher proportion of IgG2 over IgG3 was seen. In the Fulani, the frequency
of the H/H131 genotype is common and H-allele carriers had higher anti-malarial IgG2
levels than R/R homozygotes. In line with this finding, the Fulani ethnic group in Sudan
have been shown to have higher frequencies of both H/H131 genotype and H131 allele
than the sympatric Masaleit [233], and other studies suggested that the H/H131 genotype
might contribute to this relative protection from malaria [142-144].
In conclusion, our results suggest that the FcγRIIa-H131 allele may be associated with
the lower susceptibility to malaria seen in the Fulani group, and that anti-malarial IgG2
antibodies may be important in this context.
FcγRIIa polymorphism on the IgG subclass patterns of antibodies (Paper III)
In view of understanding the differences seen in Fulani when compared with other ethnic
groups, we analysed the influence of FcγRIIa-R/H131 polymorphism on the IgG subclass
patterns of antibodies to four malaria antigens (AMA-1, 3D7 MSP-2, FC27 MSP-2 and

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
56
Pf332-C231) in the Fulani and their sympatric non-Fulani ethnic groups (Masaleit, Hausa
and Four) in eastern Sudan. Our results show that FcγRIIa-H/H131 genotype and H131
allele were significantly more prevalent in the Fulani as compared to the non-Fulani
ethnic groups. In contrast to our previous findings in Burkina Faso and Mali, the Fulani
in Sudan showed lower anti-malarial IgG1 and IgG3 antibody levels, but higher levels of
IgG2 subclass antibodies. These discrepant results seen in Sudan may most likely be
explained by differences in patterns of malaria transmission in the different study areas
(Burkina Faso, Mali and Sudan).
Sudan is a country characterized by hypo/meso-endemicity, with seasonal and unstable
malaria transmission, unlike Burkina Faso and Mali, characterized by hyper/holo-
endemic malaria transmission. In general, the serum levels of IgG1 and IgG3 subclass
antibodies were found to be at higher levels than IgG2 and IgG4 antibodies in both ethnic
groups. However, the antibody levels varied between the different antigens. In line with
our previous finding in Mali (Paper II), the Fulani showed a higher frequency of the
H131 allele and higher levels of anti-malarial IgG2 antibodies than the sympatric non-
Fulani ethnic groups.
In the presence of the FcγRIIa-H131 receptor, IgG2 antibody is essential for effective
IgG2-mediated cellular activation. We found that higher levels of IgG2 and IgG3
antibodies were associated with the H/H genotype, while higher levels of IgG1 antibodies
were associated with the R/R131 genotype. However, the higher IgG2 antibody levels
seen in these Fulani individuals may be due to the relatively high prevalence for the

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
57
H/H131 genotype in this population. Additional studies are further needed to explicate
this.
In brief, we showed that the FcγRIIa-H/H131 genotype and H131 allele is at higher
frequency in the Fulani ethnic group and the H/H131 genotype was consistently
associated with higher levels of anti-malarial IgG2 and IgG3 antibodies, while the
R/R131 genotype was associated with higher levels of IgG1 antibodies.
IgG subclass responses to different asexual blood-stage malaria antigens (Paper IV)
Evidence shows that antibodies to blood-stage antigens of P. falciparum play a role in
protection from malaria, although the precise targets and mechanisms mediating
immunity remain unclear. In this study, we have analysed antibody responses to a panel
of six blood-stage antigens in relation to clinical malaria outcome in a hospital-based
study in Sudan. We focused our analysis on asexual blood-stage antigens namely; AMA-
1, 3D7 and FC27 alleles of MSP-2, MSP-3, R0 and R2 regions of GLURP based on their
association with protection in both pre-clinical and clinical studies. Our results show that
the pattern of the IgG subclasses for the different antigens varied but IgG1 and IgG3
antibody subclasses were the most prominent. AMA-1 antibodies were predominately of
the IgG1 subclass while both alleles of MSP-2, MSP-3 were biased for IgG3. GLURP
showed a bias for the IgG3 subclass especially in individuals above 5 years of age. The
dominance of IgG3 antibodies in individuals above 5 years was observed with MSP-2,
MSP-3 and GLURP.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
58
To demonstrate the characteristics of our associations, we divided the distributions into
groups by ranking them into fifths of the distribution. All measures were coded as series
of binary dummy variable, including age. In other to maximise power, we examined the
linear association by modelling the antibody distributions as ordinal variables based on
the fifths of the distributions. Our results revealed a linear association with anti-AMA-1
IgG1 antibodies and the linearity was more pronounced in the combined final model.
However, in individuals above 5 years, a non-linear (inverted U-shaped) relationship with
IgG3 antibodies was observed for MSP-2, MSP-3 and GLURP. Furthermore, in the
combined final model, the highest levels of IgG1 subclass antibodies to AMA-1,
GLURP-R0, and the highest levels of IgG3 subclass antibodies reactive to 3D7 MSP-2
were independently associated with a reduced risk of clinical malaria both before and
after adjustment for confounding factors. For reasons not fully understood, the different
merozoite antigens induced different relative levels of IgG1 and IgG3 antibodies.
Probably, the intrinsic properties of the antigen itself and/or age (in the context of our
results) may play a major role in determining the subclass of the antibody response.
Antibodies have the capacity to bind antigens through its Fab part, but its effector role is
mediated by the antibody’s Fc portion [267-268]. IgG1 and IgG3 subclass antibodies are
the key components of FcγR-mediated effector responses, and they have the ability to
neutralise pathogens at ports of entry into the body [145]. It has been suggested that IgG3
is more efficient at mediating these processes [266, 269]. Malaria specific IgG1 and IgG3
isotypes are transferred to the offspring more often and more efficiently than IgG2 and
IgG4 [270]. Furthermore, individuals with no detectable level of malaria specific IgG3
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
59
antibodies had bleak prognostic chance of recovery from severe malaria [271] and in
patients with the most severe form of malaria, a very low level of antibodies were
detected [272]. Evidence also shows a protective role of high levels of IgG3 antibodies in
uninfected primigravidae without placental malaria infection at enrolment and delivery
[273]. Antibodies to merozoite antigens are thought to function in vivo by inhibition of
merozoite invasion of erythrocytes, opsonisation of merozoites for phagocytosis, ADCI
[118, 122, 124, 274-275]. The subclass of antibodies produced against antigens is
probably very important as IgG subclasses differ in their structures and mediate different
immune effector functions [61, 276]. High titres of antibodies to the combinations of
merozoite antigens were reported to be associated with protection from clinical malaria
[249] and enhance the likelihood of therapeutic success in malaria patients [277].
Furthermore, IgG subclass specific responses against merozoite antigens are associated
with protection from symptomatic malaria and high-density parasitaemia [278], while
anti-VSA antibodies were associated with acquiring asymptomatic infection rather than
febrile malaria [279]. However, while antibodies to AMA-1 may directly inhibit the
merozoite invasion of erythrocytes [131], parasite neutralization by antibodies to MSP-3
and GLURP is dependent on their interaction with Fcγ receptors on monocytes or other
effector cells [157-158, 241, 274]. Recently, antibodies to another merozoite antigen
(MSP-1) were also able to inhibit in vitro growth of P. falciparum only in cooperation
with human monocytes [280].
In conclusion, this study provides further evidence of the potential importance of the
studied merozoite antigens as targets for parasite neutralising antibody responses of the

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
60
IgG1 and IgG3 subclasses. The results further indicated that for most of the antigens,
IgG3 antibodies, with their shorter half-life, may be more efficient than IgG1 in limiting
parasitaemia in individuals with clinical malaria, probably due to its structurally
biological function.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
61
Concluding remarks and future perspectives
This study aimed at elucidating some probable mechanisms by which antibodies mediate
their effective functions in malaria infection. We have studied their interactions with
FcγRIIa genotype in both malaria patients and asymptomatic individuals (individuals
with or without malaria parasites but no malaria) from different endemic settings.
The data from this thesis concludes that FcγRIIa-R/H131 polymorphism may play a role
in regulating the clinical outcome of malaria disease. In the case of severe malaria, we
found that the R/R131 genotype was significantly associated with susceptibility to severe
malaria, while the presence of H131 allele and H/H131 genotype, which binds IgG3
antibodies more efficiently, appeared to be less likely to be associated with severe
malaria. The results also indicated that the Fulani ethnic group, who are less susceptible
to malaria, have higher spleen rate, lower parasite prevalence, have a higher frequency of
the FcγRIIa-H/H131-and H131 allele carriers.
Binding of antibodies to infected RBCs is believed to evoke their opsonisation involving
mainly the cytophilic antibodies (Figure 11). IgG1 and IgG3 antibodies, however, have
high affinity for Fc receptors on phagocytic cells. Our data indicated that the levels of
IgG1 and IgG3 antibodies were statistically significantly higher in mild (uncomplicated)
malaria patients when compared with the severe malaria patients. Our results also showed
that Fulani in Mali had significantly higher levels of IgG1 and IgG3 subclass antibodies.
However, the Fulani in Sudan had lower levels of IgG1 and IgG3 antibodies which could
be attributed to differences in malaria endemicity. Interestingly, both the Fulani in Mali

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
62
and Sudan had significant higher levels of IgG2 antibodies when compared with their
sympatric groups. In individuals carrying H/H131, these results suggest that the
protective role of IgG2 and IgG3 antibodies in malaria infection might be through the
activation of FcγRIIa-H131 (Figure 11). Furthermore, our data showed that the higher
IgG2 subclass antibody levels seen in Fulani group may be due to the relatively high
prevalence of H/H131 in this ethnic group.
High titres of antibodies to the combination of merozoite antigens are thought to be
associated with protection from clinical malaria. However, the magnitude of anti-malarial
responses may not necessarily be the key element involved in protection but the antibody
specificity and biological function. To our studied antigens (paper IV), we found a bias
towards IgG3 antibodies which dominated in individuals above 5 years of age. Although
IgG3 has a very short half-life, continuous exposure to malaria infection (especially in
adults) may maintain its circulation leading to complement-mediated lysis of infected
RBC.
Future prospects would include longitudinal studies, follow-up studies and case-control
studies to evaluate the influence of FcγRs during malaria infections. Consecutive
antibody responses during these studies might also facilitate the understanding of its
functional mechanisms in malaria outcome. Functional experiments with FcγR allotypes
on the circulating levels of antibody subclasses would be interesting to investigate in
view of elucidating mechanisms of susceptibility/resistance to malaria.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
63
Figure 11. Probable mechanisms of antibody-mediated clearance of infected erythrocytes. (a) Antibodies can bind to free merozoites or bind to antigens on the surface of infected erythrocytes, thereby inhibit merozoite entry into the erythrocyte by complement-mediated lysis; (b) Antibodies can bind to monocytes/macrophages and optimise parasite killing through the release of soluble factors (TNF-α, NO) upon uptake of opsonised merozoites; (c) IgG2 can participate in parasite clearance in individuals with higher frequency of FcγRIIa-H131 that bind IgG2 along with IgG3 subclass antibodies.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
64
Acknowledgements
The journey has been tough, knotty and strenuous. For years, I wondered how it would
come to an end with little or no resources to help maximise my potentials. I would like to
express my heartfelt gratitude to everyone who, one way or the other, have contributed
immeasurably in making this thesis a reality.
Klavs Berzins, my supervisor, for the opportunity to work with you and your advice,
constructive criticisms and suggestions. Thank you for sharing your vast knowledge with
me, nurturing my ideas and interests, and the interesting discussions we always have.
Marita Troye-Blomberg, the Head of Department and my second supervisor, for the
conducive intellectual micro-environment existing at the department. Tack så mycket!
The seniors at the department; Eva Severinson, Carmen Fernández, and Eva
Sverremark-Ekström. Thank you for the favourable environment for scientific
interactions.
I am indebted to my parents, Jonathan Iriemenam Okonkwo and Monica Chinwa
Okonkwo who fought very hard in making sure that every child of the family received
the priceless legacy – education. I am very proud of you all!!! My younger brothers,
Chukwudi, Onyekachukwu, Ginikanwa, Amaobichukwu and my only sister Adaobi,
for your continued support, encouragement, kind-heartedness and prayers. I cannot thank
you enough! Many thanks to Osita Chukwuma, Elonna Okonkwo, Nwanneka
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
65
Umeigbo, Richard Uche and Immaculata Uche for your love, understanding, support,
advice and encouragement. Ka onye nwe anyị bi n’igwe gọzie ụnụ niile mmaji pụrụ
mmaji!
Dr. Grace Adeoye who first introduced me to the field of Parasitology and Immunology
and Dr. Olubunmi Otubanjo who fostered the interest I have in medical research.
Professor Adetayo Fagbenro-Beyioku and Dr. Wellington Oyibo for the invaluable
support, advice, encouragement and help anytime it is needed.
Hedvig Perlmann, Margareta Hagstedt (Maggan) and Ann Sjölund for your
technical support whenever I had difficulties with practical issues. I am very grateful.
Gelana Yadeta and Anna-Leena Jarva for your superb administrative services that
helps the department to run smoothly without hitches. Keep it up!
I also appreciate the technical support I received from my friends Amre Nasr, Halima
Balogun, Dr. Salah Farouk, and Dr. Gehad ElGhazali.
Adeola Aderounmu who first introduced me to my supervisor and helped me at the
initial stage of my arrival in Sweden. Thank you so much for your wonderful support and
encouragement! It is very much appreciated.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
66
I am very grateful to the patients, Daraweesh community, volunteers and participants in
the study areas for their support. This study is a success because of you. The staff at New
Halfa Teaching Hospital, Halfa Sugar Factory, Gedaref Teaching Hospital, El-Obied
Teaching Hospital, are appreciated for their excellent assistance in the field and
laboratory.
Past and present colleagues at the Department of Immunology – Magdi M. Ali, John
Arko-Mensah, Ahmed Bolad, Salah Eldin Farouk, Jacob Minang, Alice Nyakeriga,
Valentina Mangano, Anna Tjärnlund, Khaleda Qazi Rahman, Manijeh Vafa
Homann, Nina-Maria Vasconcelos, Yvonne Sundström, Nora Bachmayer, Petra
Amoudruz, Amre Nasr, Elisabeth Israelsson, Halima Balogun, Nancy Awah, Pablo
Giusti, Jubayer Rahman, Ylva Sjögren, Stefania Varani, Shanie Saghafian-
Hedengren, Olivia Simone, Charles Arama, Maria Johansson, Luis Fernando
Tordoya, Bakary Maiga, Judith Anchang, Ebba Sohlberg, Christian Okafor, Olga
Flores, Jacqueline Calla, Gishanti Arambepola, Nicky Thrupp, Stephanie Boström
and Shahid Waseem for making the department a pleasant place for research. Thank you
for your friendship.
To all my wonderful friends in Sweden; Newlife, Newlife International Cell Group,
Newlife Worship Team, African Ministry, African Gospel Mass Choir (All Nations),
Benjamin Benson, Margaret Benson, John van Dinther, Dr. Diddy Antai, Samuel
Nweze, Mukasa’s family, Jeffrey Idumu, Evelyn Nde, Daniel Ekerieke, Jae Sung
Kim, Gawa Bidla, Adeola Aderounmu, Amani Kheir, Ernest Ampadu, Saliu

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
67
Amedu, Abbas Owoade, Ronke Adedeji, Divine Eke, Yetunde Amao, Ademola
Johnson and Ikechukwu Ohajekwe. Your friendship is highly treasured!
Finally, I cannot describe the joy and peace I have with my family. Chizube and
Chikamdabere, your smiles, encouragement, support and love keep me strong each day.
Thank you so much for your perfect understanding! Ọ bụ ụnụ n’enye m obi ụtọ ụbọchị ọ
bụla.
These studies were funded by ICSC World Laboratory, UNESCO-IUMS-SGM, Swedish Institute,
SIDA/SAREC and BioMalPar European Network of Excellence.
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
68
REFERENCES
1. Delves PD, Roitt IM. The immune system: first of two parts. N Engl J Med 2000; 343:37-49.
2. Vivoer E, Malissen B. Innate and adaptive immunity: specificities and signalling hierarchies revisited. Nat Immunol 2005; 6:17-21.
3. Dempsey PW, Vaidya SA, Cheng G. The art of war: innate and adaptive immune response. Cell Mol Life Sci 2003; 60:2604-2621.
4. Areshoug T, Gordon S. Pattern recognition receptors and their role in innate immunity: focus on microbial protein ligands. Contrib Microbiol 2008; 15:45-60.
5. Mukhopadhyay S, Gordon S. The role of scavenger receptors in pathogen recognition and innate immunity. Immunobiology 2004; 209:39-49.
6. Plüdddemann A, Neyen C, Gordon S. Macrophage scavenger receptors and host-derived ligands. Methods 2007; 43:207-217.
7. Chen G, Shaw MH, Kim Y, Nunez G. Nod-like Receptors: Role in innate immunity and inflammatory disease. Annu Rev Pathol 2009; 4:365-398.
8. van Vliet SJ, Dunnen J, Gringhuis SI, Geijtenbeek TB, van Kooyk Y. Innate signaling and regulation of dendritic cell immunity. Curr Opin Immunol 2007; 4:435-440.
9. Takaoka A, Wang Z, Choi MK, Yanai H, Negishi H, Ban T, Lu Y, Miyagishi M, Kodama T, Honda K, Ohba Y, Taniguchi T. DAI (DLM-1/ZBP1) is a cytosolic DNA sensor and an activator of innate immune response. Nature 2007; 448:501-505.
10. Arancibia SA, Beltran CJ, Auirre IM, Silva P, Peralta AL, Malinarich F, Hermoso MA. Toll-like receptors are key participants in innate immune responses. Biol Res 2007; 40:97-112.
11. Takeda K, Akira S. Toll-like receptors in innate immunity. Int Immunol 2005; 17:1-14.
12. Roy CR, Mocarski ES. Pathogen subversion of cell-intrinsic innate immunity. Nat Immunol 2007; 8:1179-1187.
13. Iwasaki A, Medzhitov R. Toll-like receptor control of the adaptive immune responses. Nat Immunol 2004; 5:987-995.
14. Xu D, Komai-Koma M, Liew FY. Expression and function of Toll-like receptor on T cells. Cell Immunol 2005; 233:85-89.
15. Meyer-Bahlburg A, Khim S, Rawlings DJ. B cell intrinsic TLR signals amplify but are not required for humoral immunity. J Exp Med 2007; 204:3095-3101.
16. Creagh EM, O’Neill LAJ. TLRs, NLRs and RLRs: a trinity of pathogen sensors that co-operate in innate immunity. Trends Immunol 2006; 27:352-357.
17. Gordon S, Taylor PR. Monocyte and macrophage heterogeneity. Nat Rev Immunol 2005; 5:953-964.
18. León B, Ardavín C. Monocyte-derived dendritic cells in innate and adaptive immunity. Immunol Cell Biol 2008; 86:320-324.
19. Geissmann F, Auffray C, Palframan R, Wirrig C, Ciocca A, Campisi L, Narni-Mancinelli E, Lauvau G. Blood monocytes: distinct subsets, how they relate to dendritic cells, and their possible roles in the regulation of T-cell responses. Immunol Cell Biol 2008; 86:398-408.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
69
20. Tabe H, Kawabata I, Koba R, Homma T. Cell dynamics in the germinal center of the human tonsil. Acta Otolaryngol Suppl 1996; 523:64-67.
21. Banchereau J, Briere F, Caux C, Davoust J, Lebecque S, Liu YJ, Pulendran B, Palucka K. Immunobiology of dendritic cells. Annu Rev Immunol 2000; 18:767-811.
22. Steinman RM. Linking innate to adaptive immunity through dendritic cells. Novartis Found Symp 2006; 279:101-9; discussion 109-13, 216-9.
23. Reschner A, Hubert P, Delvenne P, Boniver J, Jacobs N. Innate lymphocyte and dendritic cell cross-talk: a key factor in the regulation of the immune response. Clin Exp Immunol 2008; 152:219-226.
24. Ullrich E, Chaput N, Zitvogel L. Killer dendritic cells and their potential role in immunotherapy. Horm Metab Res 2008; 40:75-81.
25. Chen L, Calomeni E, Wen J, Ozato K, Shen R, Gao JX. Natural killer dendritic cells are an intermediate of developing dendritic cells. J Leukoc Biol 2007; 81:1422-1433.
26. Bonmort M, Dalod M, Mignot G, Ullrich E, Chaput N, Zitvogel L. Killer dendritic cells: IKDC and the others. Curr Opin Immunol 2008; 20:558-565.
27. Vivier E, Tomasello E, Baratin M, Walzer T, Ugolini S. Functions of natural killer cells. Nat Immunol 2008; 9:503-510.
28. Brilot F, Strowig T, Munz C. NK cells interactions with dendritic cells shape innate and adaptive immunity. Front Biosci 2008; 13:6443-6454.
29. Lanier LL. NK cell recognition. Annu Rev Immunol 2005; 23:225-274. 30. Grégoire C, Chasson L, Luci C, Tomasello E, Geissmann F, Vivier E, Walzer T.
The trafficking of natural killer cells. Immunol Rev 2007; 220:169-182. 31. Schwarz BA, Bhandoola A. Trafficking from the bone marrow to the thymus: a
prerequisite for thymopoiesis. Immunol Rev 2006; 209:47-57. 32. Ciofani M, Zúñiga-Pflücker JC. The thymus as an inductive site for T
lymphopoiesis. Annu Rev Cell Dev Biol 2007; 23:463-493. 33. Starr TK, Jameson SC, Hogquist KA. Positive and negative selection of T cells.
Annu Rev Immunol 2003; 21:139-176. 34. Chen Z, O’Shea JJ. Th17cells: a new fate for differentiating helper T cells.
Immunol Res 2008; 41:87-102. 35. Kidd P. Th1/Th2 balance: the hypothesis, its limitations, and implications for
health and disease. Altern Med Rev 2003; 8:223-246. 36. Tesmer LA, Lundy SK, Sarkar S, Fox DA. Th17 cells in human disease. Immunol
Rev 2008; 223:87-113. 37. Zinkernagel RM, Bachmann MF, Kündig TM, Oehen S, Pirchet H, Hengartner H.
On immunological memory. Annu Rev Immunol 1996; 14:333-367. 38. Gray D, Siepmann K, van Essen D, Poudrier J, Wykes M, Jainandunsing S,
Bergthorsdottir S, Dullforce P. B-T lymphocyte interactions in the generation and survival of memory cells. Immunol Rev 1996; 150:45-61.
39. Szakal AK, Kosco MH, Tew JG. Microanatomy of lymphoid tissue during humoral immune responses: structure function relationships. Annu Rev Immunol 1989; 7:91-109.
40. Fairfax KA, Kallies A, Nutt SL, Tarlinton DM. Plasma cell development: from B-cell subsets to long-term survival niches. Semin Immunol 2008; 20:49-58.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
70
41. Miller JJ. An autoradiographic study of plasma cell and lymphocyte survival in rat popliteal lymph nodes. J Immunol 1964; 92:673-681.
42. Cooper EH. Production of lymphocytes and plasma cells in the rat following immunization with human serum albumin. Immunology 1961; 4:219-231.
43. Lévy M, Vieira P, Coutinho A, Freitas A. The majority of "natural" immunoglobulin-secreting cells are short-lived and the progeny of cycling lymphocytes. Eur J Immunol 1987; 17:849-854.
44. Ho F, Lortan JE, MacLennan IC, Khan M. Distinct short-lived and long-lived antibody-producing cell populations. Eur J Immunol 1986; 16:1297-1301.
45. Slifka MK, Antia R, Whitmire JK, Ahmed R. Humoral immunity due to long-lived plasma cells. Immunity 1998; 8:363-372.
46. Slifka MK, Ahmed R. Long-lived plasma cells: a mechanism for maintaining persistent antibody production. Curr Opin Immunol 1998; 10:252-258.
47. Slifka MK, Matloubian M, Ahmed R. Bone marrow is a major site of long-term antibody production after acute viral infection. J Virol 1995; 69:1895-1902.
48. Crotty S, Ahmed R. Immunological memory in humans. Semin Immunol 2004; 16:197-203.
49. Martin NH. The immunoglobulins: a review. J Clin Pathol 1969; 22:117-131. 50. Heyman B, Pilström L, Shulman MJ. Complement activation is required for IgM-
mediated enhancement of the antibody response. J Exp Med 1988; 167:1999-2004.
51. Pan Q, Hammarström L. Molecular basis of IgG subclass deficiency. Immunol Rev 2000; 178:99-110.
52. Woof JM, Kerr MA. The function of immunoglobulin A in immunity. J Pathol 2006; 208:270-282.
53. Lantz CS, Boesiger J, Song CH, Mach N, Kobayashi T, Mulligan RC, Nawa Y, Dranoff G, Galli SJ. Role for interleukin-3 in mast-cell and basophil development and in immunity to parasites. Nature 1998; 392:90-93.
54. King CL, Xianli J, Malhotra I, Liu S, Mahmoud AA, Oettgen HC. Mice with a targeted deletion of the IgE gene have increased worm burdens and reduced granulomatous inflammation following primary infection with Schistosoma mansoni. J Immunol 1997; 158:294-300.
55. Perlmann P, Perlmann H, Looareesuwan S, Krudsood S, Kano S, Matsumoto Y, Brittenham G, Troye-Blomberg M, Aikawa M. Contrasting functions of IgG and IgE antimalarial antibodies in uncomplicated and severe Plasmodium falciparum malaria. Am J Trop Med Hyg 2000; 62:373-377.
56. Calissano C, Modiano D, Sirima BS, Konate A, Sanou I, Sawadogo A, Perlmann H, Troye-Blomberg M, Perlmann P. IgE antibodies to Plasmodium falciparum and severity of malaria in children of one ethnic group living in Burkina Faso. Am J Trop Med Hyg 2003; 69:31-35.
57. Bereczky S, Montgomery SM, Troye-Blomberg M, Rooth I, Shaw MA, Färnert A. Elevated anti-malarial IgE in asymptomatic individuals is associated with reduced risk for subsequent clinical malaria. Int J Parasitol 2004; 34:935-942.
58. Duarte J, Deshpande P, Guiyedi V, Mécheri S, Fesel C, Cazenave PA, Mishra GC, Kombila M, Pied S. Total and functional parasite specific IgE responses in
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
71
Plasmodium falciparum-infected patients exhibiting different clinical status. Malar J 2007; 6:1
59. Daëron M. Fc receptor biology. Annu Rev Immunol 1997; 15:203-234. 60. Nimmerjahn F, Ravetch JV. Fcgamma receptors: old friends and new family
members. Immunity 2006; 24:19-28. 61. Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators of immune
responses. Nat Rev Immunol 2008; 8:34-47. 62. Nimmerjahn F, Ravetch JV. Fc-receptors as regulators of immunity. Adv Immunol
2007; 96:179-204. 63. Pleass RJ, Woof JM. Fc receptors and immunity to parasites. Trends Parasitol
2001; 17:545-551. 64. Shi J, McIntosh RS, Pleass RJ. Antibody- and Fc-receptor-based therapeutics for
malaria. Clin Sci 2006; 110:11-19. 65. Warmerdam PA, van de Winkel JG, Vlug A, Westerdaal NA, Capel PJ. A single
amino acid in the second Ig-like domain of the human Fc gamma receptor II is critical for human IgG2 binding. J Immunol 1991; 147:1338-1343.
66. van de Winkel JG, Anderson CL. Biology of human immunoglobulin G Fc receptors. J Leukoc Biol 1991; 49:511-524.
67. Cassatella MA, Anegón I, Cuturi MC, Griskey P, Trinchieri G, Perussia B. Fc gamma R(CD16) interaction with ligand induces Ca2+ mobilization and phosphoinositide turnover in human natural killer cells. Role of Ca2+ in Fc gamma R (CD16)-induced transcription and expression of lymphokine genes. J Exp Med 1989; 169:549-567.
68. Yuan FF, Wong M, Pererva N, Keating J, Davis AR, Bryant JA, Sullivan JS. FcgammaRIIA polymorphisms in Streptococcus pneumoniae infection. Immunol Cell Biol 2003; 81:192-195.
69. Yee AM, Phan HM, Zuniga R, Salmon JE, Musher DM. Association between FcgammaRIIa-R131 allotype and bacteremic pneumococcal pneumonia. Clin Infect Dis 2000; 30:25-28.
70. Manger K, Repp R, Spriewald BM, Rascu A, Geiger A, Wassmuth R, Westerdaal NA, Wentz B, Manger B, Kalden JR, van de Winkel JG. Fcgamma receptor IIa polymorphism in Caucasian patients with systemic lupus erythematosus: association with clinical symptoms. Arthritis Rheum 1998; 41:1181-1189.
71. Yun HR, Koh HK, Kim SS, Chung WT, Kim DW, Hong KP, Song GG, Chang HK, Choe JY, Bae SC, Salmon JE, Yoo DH, Kim TY, Kim SY. FcgammaRIIa/IIIa polymorphism and its association with clinical manifestations in Korean lupus patients. Lupus 2001; 10:466-472.
72. Smed-Sörensen A, Moll M, Cheng TY, Loré K, Norlin AC, Perbeck L, Moody DB, Spetz AL, Sandberg JK. IgG regulates the CD1 expression profile and lipid antigen-presenting function in human dendritic cells via FcgammaRIIa. Blood 2008; 111:5037-5046.
73. Tuteja R. Malaria - an overview. FEBS J 2007; 274:4670-4679. 74. Greenwood B, Mutabingwa T. Malaria in 2002. Nature 2002; 415:670-672. 75. Greenwood BM, Bojang K, Whitty CJ, Targett GA. Malaria. Lancet 2005;
365:1487-1498.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
72
76. Alnwick D. Roll back malaria – what are the prospects? Bull World Health Organ 2000; 78:1377.
77. Breman JG. The ears of the hippopotamus: manifestations, determinants, and estimates of the malaria burden. Am J Trop Med Hyg 2001; 64(1-2 Suppl):1-11
78. Fujioka H, Masamichi A. The malaria parasite and its life cycle. In: Wahlgren M, Perlmann, P. (Eds) Malaria; Molecular and Clinical Aspects. Amsterdam: Harwood Academic Publishers; 1999. p.19-55.
79. Singh B, Kim Sung L, Matusop A, Radhakrishnan A, Shamsul SS, Cox-Singh J, Thomas A, Conway DJ. A large focus of naturally acquired Plasmodium knowlesi infections in human beings. Lancet 2004; 363:1017-1024.
80. White N. Plasmodium knowlesi: the fifth human malaria parasite. Clin Infect Dis 2008; 46:172-173.
81. Collins WE, Barnwell JW. Plasmodium knowlesi: Finally Being Recognized. J Infect Dis 2009; 199:1107-1108.
82. Cox-Singh J, Davis TM, Lee KS, Shamsul SS, Matusop A, Ratnam S, Rahman HA, Conway DJ, Singh B. Plasmodium knowlesi malaria in humans is widely distributed and potentially life threatening. Clin Infect Dis 2008; 46:165-171.
83. Kantele A, Marti H, Felger I, Müller D, Jokiranta TS. Monkey malaria in a European traveler returning from Malaysia. Emerg Infect Dis 2008; 14:1434-1436.
84. Cox-Singh J, Singh B. Knowlesi malaria: newly emergent and of public health importance? Trends Parasitol 2008; 24:406-410.
85. Vythilingam I, Noorazian YM, Huat TC, Jiram AI, Yusri YM, Azahari AH, Norparina I, Noorrain A, Lokmanhakim S. Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia. Parasit Vectors 2008; 1:26.
86. Ng OT, Ooi EE, Lee CC, Lee PJ, Ng LC, Pei SW, Tu TM, Loh JP, Leo YS. Naturally acquired human Plasmodium knowlesi infection, Singapore. Emerg Infect Dis 2008; 14:814-816.
87. Luchavez J, Espino F, Curameng P, Espina R, Bell D, Chiodini P, Nolder D, Sutherland C, Lee KS, Singh B. Human Infections with Plasmodium knowlesi, the Philippines. Emerg Infect Dis 2008; 14:811-813.
88. Bronner U, Divis PC, Farnert A, Singh B. Swedish traveller with Plasmodium knowlesi malaria after visiting Malaysian Borneo: a case report. Malar J 2009; 8:15.
89. Lee KS, Cox-Singh J, Brooke G, Matusop A, Singh B. Plasmodium knowlesi from archival blood films: Further evidence that human infections are widely distributed and not newly emergent in Malaysian Borneo. Int J Parasitol 2009; [Epub ahead of print].
90. Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM. Artemisinin Resistance in Cambodia 1 (ARC1) Study Consortium. Evidence of artemisinin-resistant malaria in western Cambodia. N Engl J Med 2008; 359:2619-2620.
91. Wongsrichanalai C, Meshnick SR. Declining artesunate-mefloquine efficacy against falciparum malaria on the Cambodia-Thailand border. Emerg Infect Dis 2008; 14:716-719.
92. Lozano JM, Patarroyo ME. A rational strategy for a malarial vaccine development. Microbes Infect 2007; 9:751-760.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
73
93. WHO. Severe and complicated malaria. World Health Organisation, communicable diseases cluster. Trans R Soc Trop Med Hyg 1990; 84:(Suppl 2)S1-65.
94. WHO. Severe falciparum malaria. World Health Organisation diseases cluster. Trans R Soc Trop Med Hyg 2000; 94:(Suppl 1)S1-90.
95. Dondorp AM, Kager PA, Vreeken J, White NJ. Abnormal blood flow and red blood cell deformability in severe malaria. Parasitol Today 2000; 16:228-232.
96. Miller LH, Good MF, Milon G. Malaria pathogenesis. Science 1994; 264:1878-1883.
97. Maitland K, Marsh K. Pathophysiology of severe malaria in children. Acta Trop 2004; 90:131-140.
98. Gupta S, Snow RW, Donnelly CA, Marsh K, Newbold C. Immunity to non-cerebral severe malaria is acquired after one or two infections. Nat Med 1999; 5:340-343.
99. Baird JK. Host age as a determinant of naturally acquired immunity to Plasmodium falciparum. Parasitol Today 1995; 11:105-111.
100. Perlmann P, Perlmann H, Berzins K, Troye-Blomberg M. Selected problems of malaria blood stage immunity. Tokai J Exp Clin Med 1998; 23:55-62.
101. Druilhe P, Perignon JL. Mechanisms of defence against Plasmodium falciparum asexual blood stages in humans. Immunol Lett 1994; 41:115-120.
102. Langhorne J, Ndungu FM, Sponaas AM, Marsh K. Immunity to malaria: more questions than answers. Nat Immunol 2008; 9:725-732.
103. Beeson JG, Osier FH, Engwerda CR. Recent insights into humoral and cellular immune responses against malaria. Trends Parasitol 2008; 24:578-584.
104. Doolan DL, Dobaño C, Baird JK. Acquired immunity to malaria. Clin Microbiol Rev 2009; 22:13-36.
105. Sergent E, Parrot L. L’immunite, la premonition et la resistancw innee. Arch Inst Pasteur Algerie 1935; 13:279-319.
106. Perignon JL, Druilhe P. Immune mechanisms underlying the premunition against Plasmodium falciparum malaria. Mem Inst Oswaldo Cruz 1994; 89(Suppl. 2):51-53.
107. Malaria Genomic Epidemiology Network. A global network for investigating the genomic epidemiology of malaria. Nature 2008; 456:732-737.
108. Molineaux L. The epidemiology of human malaria as an explanation of its distribution, including some implications for its control. W McGregor (Eds.) Malaria, Edinburgh, Churchill Livingston 1988. p.913-998.
109. Hay SI, Guerra CA, Tatem AJ, Noor AM, Snow RW. The global distribution and population at risk of malaria: past, present, and future. Lancet Infect Dis 2004; 4:327-336.
110. Tatem AJ, Guerra CA, Kabaria CW, Noor AM, Hay SI. Human population, urban settlement patterns and their impact on Plasmodium falciparum malaria endemicity. Malar J 2008; 7:218.
111. Guerra CA, Gikandi PW, Tatem AJ, Noor AM, Smith DL, Hay SI, Snow RW. The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med 2008; 5:e38.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
74
112. Ménard R, Heussler V, Yuda M, Nussenzweig V. Plasmodium pre-erythrocytic stages: what's new? Trends Parasitol 2008; 24:564-569.
113. Marsh K, Kinyanjui S. Immune effector mechanisms in malaria. Parasite Immunol 2006; 28:51-60.
114. Doolan DL, Martinez-Alier N. Immune response to pre-erythrocytic stages of malaria parasites. Curr Mol Med 2006; 6:169-185.
115. Stephens R, Langhorne J. Priming of CD4+ T cells and development of C4+ T cell memory; lessons for malaria. Parasite Immunol 2006; 28:25-30.
116. Plebanski M, Hill AVS. The immunology of malaria infection. Curr Opin Immunol 2000; 12:437-441.
117. Luty AJ, Lell B, Schmidt-Ott R, Lehman LG, Luckner D, Greve B, Matousek P, Herbich K, Schmid D, Migot-Nabias F, Deloron P, Nussenzweig RS, Kremsner PG. Interferon-gamma responses are associated with resistance to reinfection with Plasmodium falciparum in young African children. J Infect Dis 1999; 179:980-988.
118. Bouharoun-Tayoun H, Oeuvray C, Lunel F, Druilhe P. Mechanisms underlying the monocyte-mediated antibody-dependent killing of Plasmodium falciparum asexual blood stages. J Exp Med 1995; 182:409-418.
119. von der Weid T, Honarvar N, Langhorne J. Gene-targeted mice lacking B cells are unable to eliminate a blood stage malaria infection. J Immunol 1996; 156: 2510-2516.
120. von der Weid T, Kitamura D, Rajewsky K, Langhorne J. A dual role for B cells in Plasmodium chabaudi chabaudi (AS) infection? Res Immunol 1994; 145:412-419.
121. Patarroyo ME, Patarroyo MA. Emerging rules for subunit-based, multiantigenic, multistage chemically synthesized vaccines. Acc Chem Res 2008; 41:377-386.
122. Berzins K, Anders R. The malaria antigens. In: Wahlgren M, Perlmann P, editors. Malaria – molecular and clinical aspects. Harwood Academic Publishers; 1999. p.181-216.
123. Holder AA. Proteins on the surface of the malaria parasite and cell invasion. Parasitology 1994; 108(Suppl):S5-S18.
124. Bolad A, Berzins K. Antigenic diversity of Plasmodium falciparum and antibody-mediated parasite neutralization. Scand J Immunol 2000; 52:233-239.
125. Li X, Chen H, Oo TH, Daly TM, Bergman LW, Liu SC, Chishti AH, Oh SS. A co-ligand complex anchors Plasmodium falciparum merozoites to the erythrocyte invasion receptor band 3. J Biol Chem 2004; 279:5765-5771.
126. Oh SS, Chishti AH. Host receptors in malaria merozoite invasion. Curr Top Microbiol Immunol 2005; 295:203-232.
127. Taylor-Robinson AW. Vaccination against malaria: targets, strategies and potentiation of immunity to blood stage parasites. Front Biosci 2000; 5:E16-29.
128. Moll K, Chêne A, Ribacke U, Kaneko O, Nilsson S, Winter G, Haeggström M, Pan W, Berzins K, Wahlgren M, Chen Q. A novel DBL-domain of the P. falciparum 332 molecule possibly involved in erythrocyte adhesion. PLoS ONE 2007; 2:e477.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
75
129. Winter G, Kawai S, Haeggström M, Kaneko O, von Euler A, Kawazu S, Palm D, Fernandez V, Wahlgren M. SURFIN is a polymorphic antigen expressed on Plasmodium falciparum merozoites and infected erythrocytes. J Exp Med 2005; 201:1853-863.
130. Theisen M, Soe S, Oeuvray C, Thomas AW, Vuust J, Danielsen S, Jepsen S, Druilhe P. The glutamate-rich protein (GLURP) of Plasmodium falciparum is a target for antibody-dependent monocyte-mediated inhibition of parasite growth in vitro. Infect Immun 1998; 66:11-17.
131. Triglia T, Healer J, Caruana SR, Hodder AN, Anders RF, Crabb BS, Cowman AF. Apical membrane antigen 1 plays a central role in erythrocyte invasion by Plasmodium species. Mol Microbiol 2000; 38:706-718.
132. Cohen S, McGregor IA, Carrington S. Gamma globulin and acquired immunity to human malaria. Nature 1961; 192:733-737.
133. McGregor IA, Carrington SP, Cohen S. Treatment of East African P. falciparum malaria with West African human γ-globulin. Trans R Soc Trop Med Hyg 1963; 57:170-175.
134. Sabchareon A, Burnouf T, Ouattara D, Attanath P, Bouharoun-Tayoun H, Chantavanich P, Foucault C, Chongsuphajaisiddhi T, Druilhe P. Parasitologic and clinical human response to immunoglobulin administration in falciparum malaria. Am J Trop Med Hyg 1991; 45:297-308.
135. Gysin J, Moisson P, Pereira da Silva L, Druilhe P. Antibodies from immune African donors with a protective effect in Plasmodium falciparum human infection are also able to control asexual blood forms of the parasite in Saimiri monkeys. Res Immunol 1996; 147:397-401.
136. Bouharoun-Tayoun H, Druilhe P. Plasmodium falciparum malaria: Evidence of isotope imbalance which may be responsible for delayed acquisition of protective immunity. Infect Immun 1992; 60:1473-1481.
137. Aribot G, Rogier C, Sarthou JL, Trape JF, Balde AT, Druilhe P, Roussilhou C. Pattern of immunoglobulin isotype response to Plasmodium falciparum blood-stage antigens in individuals living in a holoendemic area of Senegal (Dielmo, West Africa). Am J Trop Med Hyg 1996; 54:449-457.
138. Taylor RR, Allen SJ, Greenwood BM, Riley EM. IgG3 antibodies to P. falciparum merozoite surface protein 2: increasing prevalence with age and association with clinical immunity to malaria. Am J Trop Med Hyg 1998; 58:406-413.
139. Garraud O, Perrant R, Diouf A, Nambei WS, Tall A, Spiegel A, Longacre S, Kaslow DC, Jouin H, Mattei D, Engler GM, Nutman TB, Riley EM, Mercereau-Puijalon O. Regulation of antigen specific IgG subclasses in responses to conserved and polymorphic P. falciparum antigens in an in vitro model. Infect Immun 2002; 70:2820-2827.
140. Høgh B. Clinical and parasitological studies on immunity to Plasmodium falciparum malaria in children. Scand J Infect Dis Suppl 1996; 102:1-53.
141. Ferreira MU, Kimura EA, Katzin AM, Santos-Neto LL, Ferrari JO, Villalobos JM, de Carvalho ME. The IgG-subclass distribution of naturally acquired antibodies to Plasmodium falciparum, in relation to malaria exposure and severity. Ann Trop Med Par 1998; 92:245-256.
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
76
142. Aucan C, Traore Y, Tall F, Nacro B, Traore-Leroux T, Fumoux F, Rihet P. High IgG2 and low IgG4 levels are associated with human resistance to P. falciparum malaria. Infect Immun 2000; 68:1251-1258.
143. Sinha S, Mishra SK, Sharma S, Patibandla PK, Mallick PK, Sharma SK, Mohanty S, Pati SS, Mishra SK, Ramteke BK, Bhatt R, Joshi H, Dash AP, Ahuja RC, Awasthi S, Indian Genome Variation Consortium, Venkatesh V, Habib S. Polymorphisms of TNF-enhancer and gene for FcgammaRIIa correlate with the severity of falciparum malaria in the ethnically diverse Indian population. Malar J 2008; 7:13.
144. Leoratti FM, Durlacher RR, Lacerda MV, Alecrim MG, Ferreira AW, Sanchez MC, Moraes SL. Pattern of humoral immune response to Plasmodium falciparum blood stages in individuals presenting different clinical expressions of malaria. Malar J 2008; 7:186.
145. Groux H, Gysin J. Opsonization as an effector mechanism in human protection against asexual blood stages of Plasmodium falciparum: functional role of IgG subclasses. Res Immunol 1990; 141:529-542.
146. Druilhe P, Khusmith S. Epidemiological correlation between levels of antibodies promoting merozoite phagocytosis of Plasmodium falciparum and malaria-immune status. Infect Immun 1987; 55:888-891.
147. Kumaratilake LM, Ferrante A. Opsonization and phagocytosis of Plasmodium falciparum merozoites measured by flow cytometry. Clin Diagn Lab Immunol 2000; 7:9-13.
148. Chappel JA, Holder AA. Monoclonal antibodies that inhibit Plasmodium falciparum invasion in vitro recognize the first growth factor-like domain of merozoite surface protein-1. Mol Biochem Parasitol 1993; 60:303-312.
149. McCallum FJ, Persson KE, Mugyenyi CK, Fowkes FJ, Simpson JA, Richards JS, Williams TN, Marsh K, Beeson JG. Acquisition of growth-inhibitory antibodies against blood-stage Plasmodium falciparum. PLoS ONE 2008; 3:e3571.
150. Dent AE, Bergmann-Leitner ES, Wilson DW, Tisch DJ, Kimmel R, Vulule J, Sumba PO, Beeson JG, Angov E, Moormann AM, Kazura JW. Antibody-mediated growth inhibition of Plasmodium falciparum: relationship to age and protection from parasitemia in Kenyan children and adults. PLoS ONE 2008; 3:e3557.
151. Ockenhouse CF, Schulman S, Shear HL. Induction of crisis forms in the human malaria parasite Plasmodium falciparum by gamma-interferon-activated, monocyte-derived macrophages. J Immunol 1984; 133:1601-1608.
152. Perkins ME. Approaches to study merozoite invasion of erythrocytes. Res Immunol 1991; 142:662-665.
153. Wipasa J, Elliott S, Xu H, Good MF. Immunity to asexual blood stage malaria and vaccine approaches. Immunol Cell Biol 2002; 80:401-414.
154. Taylor-Robinson AW. Vaccination against malaria: targets, strategies and potentiation of immunity to blood stage parasites. Front Biosci 2000; 5:E16-29.
155. Ahlborg N, Iqbal J, Björk L, Ståhl S, Perlmann P, Berzins K. Plasmodium falciparum: differential parasite growth inhibition mediated by antibodies to the antigens Pf332 and Pf155/RESA. Exp Parasitol 1996; 82:155-163.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
77
156. Collins CR, Withers-Martinez C, Hackett F, Blackman MJ. An inhibitory antibody blocks interactions between components of the malarial invasion machinery. PLoS Pathog 2009; 5:e1000273.
157. Oeuvray C, Bouharoun-Tayoun H, Gras-Masse H, Bottius E, Kaidoh T, Aikawa M, Filgueira MC, Tartar A, Druilhe P. Merozoite surface protein-3: a malaria protein inducing antibodies that promote Plasmodium falciparum killing by cooperation with blood monocytes. Blood 1994; 84:1594-1602.
158. Theisen M, Soe S, Oeuvray C, Thomas AW, Vuust J, Danielsen S, Jepsen S, Druilhe P. The glutamate-rich protein (GLURP) of Plasmodium falciparum is a target for antibody-dependent monocyte-mediated inhibition of parasite growth in vitro. Infect Immun 1998; 66:11-17.
159. Fried M, Nosten F, Brockman A, Brabin BJ, Duffy PE. Maternal antibodies block malaria. Nature 1998; 395:851-852.
160. Duffy PE, Fried M. Malaria during pregnancy: parasites, antibodies and chondroitin sulphate A. Biochem Soc Trans 1999; 27:478-482.
161. Khattab A, Reinhardt C, Staalsoe T, Fievet N, Kremsner PG, Deloron P, Hviid L, Klinkert MQ. Analysis of IgG with specificity for variant surface antigens expressed by placental Plasmodium falciparum isolates. Malar J 2004; 3:21.
162. Staalsoe T, Shulman CE, Bulmer JN, Kawuondo K, Marsh K, Hviid L. Variant surface antigen-specific IgG and protection against clinical consequences of pregnancy-associated Plasmodium falciparum malaria. Lancet 2004; 363:283-289.
163. Elliott SR, Brennan AK, Beeson JG, Tadesse E, Molyneux ME, Brown GV, Rogerson SJ. Placental malaria induces variant-specific antibodies of the cytophilic subtypes immunoglobulin G1 (IgG1) and IgG3 that correlate with adhesion inhibitory activity. Infect Immun 2005; 73:5903-5907.
164. Hommel M, David PH, Oligino LD. Surface alterations of erythrocytes in Plasmodium falciparum malaria. Antigenic variation, antigenic diversity, and the role of the spleen. J Exp Med 1983; 157:1137-1148.
165. Marsh K, Howard RJ. Antigens induced on erythrocytes by P. falciparum: expression of diverse and conserved determinants. Science 1986; 231:150-153.
166. Hviid L. Naturally acquired immunity to Plasmodium falciparum malaria in Africa. Acta Trop 2005; 95:270-275.
167. Hviid L. The immuno-epidemiology of pregnancy-associated Plasmodium falciparum malaria: a variant surface antigen-specific perspective. Parasite Immunol 2004; 26:477-486.
168. Salanti A, Dahlbäck M, Turner L, Nielsen MA, Barfod L, Magistrado P, Jensen AT, Lavstsen T, Ofori MF, Marsh K, Hviid L, Theander TG. Evidence for the involvement of VAR2CSA in pregnancy-associated malaria. J Exp Med 2004; 200:1197-1203.
169. Magistrado P, Salanti A, Tuikue Ndam NG, Mwakalinga SB, Resende M, Dahlbäck M, Hviid L, Lusingu J, Theander TG, Nielsen MA. VAR2CSA expression on the surface of placenta-derived Plasmodium falciparum-infected erythrocytes. J Infect Dis 2008; 198:1071-1074.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
78
170. Fried M, Duffy PE. Adherence of Plasmodium falciparum to chodroitin sulfate A in the human placenta. Science 1996; 272:1502-1502
171. Fievet N, Le Hesran JY, Cottrell G, Doucoure S, Diouf I, Ndiaye JL, Bertin G, Gaye O, Sow S, Deloron P. Acquisition of antibodies to variant antigens on the surface of Plasmodium falciparum-infected erythrocytes during pregnancy. Infect Genet Evol 2006; 6:459-463.
172. Tuikue Ndam N, Deloron P. Towards a vaccine against pregnancy-associated malaria. Parasite 2008; 15:515-521.
173. Nielsen MA, Pinto VV, Resende M, Dahlbäck M, Ditlev SB, Theander TG, Salanti A. Induction of adhesion-inhibitory antibodies against placental Plasmodium falciparum parasites using single domains of VAR2CSA. Infect Immun 2009; [Epub ahead of print].
174. Wykes M, Good MF. Memory B cell responses and malaria. Parasite Immunol 2006; 28:31-34.
175. Dorfman JR, Bejon P, Ndungu FM, Langhorne J, Kortok MM, Lowe BS, Mwangi TW, Williams TN, Marsh K. B cell memory to 3 Plasmodium falciparum blood-stage antigens in a malaria-endemic area. J Infect Dis 2005; 191:1623-1630.
176. Migot F, Chougnet C, Henzel D, Dubois B, Jambou R, Fievet N, Deloron P. Anti-malaria antibody-producing B cell frequencies in adults after a Plasmodium falciparum outbreak in Madagascar. Clin Exp Immunol 1995; 102:529-534.
177. Kinyanjui SM, Conway DJ, Lanar DE, Marsh K. IgG antibody responses to Plasmodium falciparum merozoite antigens in Kenyan children have a short half-life. Malar J 2007; 6:82.
178. Asito AS, Moormann AM, Kiprotich C, Ng'ang'a ZW, Ploutz-Snyder R, Rochford R. Alterations on peripheral B cell subsets following an acute uncomplicated clinical malaria infection in children. Malar J 2008; 7:238.
179. Akpogheneta OJ, Duah NO, Tetteh KK, Dunyo S, Lanar DE, Pinder M, Conway DJ. Duration of naturally acquired antibody responses to blood-stage Plasmodium falciparum is age dependent and antigen specific. Infect Immun 2008; 76:1748-1755.
180. Deloron P, Chougnet C. Is immunity to malaria really short-lived? Parasitol Today 1992; 8:375-378.
181. Stephens R, Ndungu FM, Langhorne J. Germinal centre and marginal zone B cells expand quickly in a second Plasmodium chabaudi malaria infection producing mature plasma cells. Parasite Immunol 2009; 31:20-31.
182. Campos M, Godson DL. The effectiveness and limitations of immune memory: understanding protective immune responses. Int J Parasitol 2003; 33:655-661.
183. Haldane JBS. The rate of mutation of human gene. Hereditas 1949; 35:267-273.
184. Williams TN. Red blood cell defects and malaria. Mol Biochem Parasitol 2006; 149:121-127.
185. Williams TN. Human red blood cell polymorphisms and malaria. Curr Opin Microbiol 2006; 9:388-394.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
79
186. Wu DY, Ugozzoli L, Pal BK, Wallace RB. Allele-specific enzymatic amplification of β-globin genomic DNA for diagnosis of sickle cell anemia. Proc Natl Ac. Sci 1989; 86:2757-2760.
187. Marsh K, Otoo L, Hayes RJ, Carson DC, Greenwood BM. Antibodies to blood stage antigens of Plasmodium falciparum in rural Gambians and their relation to protection against infection. Trans R Soc Trop Med 1989; 83:293-303.
188. Hill AV, Allsopp CE, Kwiatkowski D, Anstey NM, Twumasi P, Rowe PA, Bennett S, Brewster D, McMichael AJ, Greenwood BM. Common West African HLA antigens are associated with protection from severe malaria. Nature 1991; 352:595-600.
189. May J, Evans JA, Timmann C, Ehmen C, Busch W, Thye T, Agbenyega T, Horstmann RD. Hemoglobin variants and disease manifestations in severe falciparum malaria. JAMA 2007; 297:2220-2226.
190. Williams TN, Mwangi TW, Wambua S, Alexander ND, Kortok M, Snow RW, Marsh K. Sickle cell trait and the risk of Plasmodium falciparum malaria and other childhood diseases. J Infect Dis 2005; 192:178-186.
191. Aubouy A, Migot-Nabias F, Deloron P. Correlations between treatment outcome and both anti-MSP119 antibody response and erythrocyte-related genetic factors in Plasmodium falciparum malaria. Infect Gene Evol 2007; 7:147-154.
192. Ayi K, Turrini F, Piga A, Arese P. Enhanced phagocytosis of ring-parasitized mutant erythrocytes: a common mechanism that may explain protection against falciparum malaria in sickle trait and beta-thalassemia trait. Blood 2004; 104:3364-3371.
193. Cholera R, Brittain NJ, Gillrie MR, Lopera-Mesa TM, Diakite SAS, Arie T, Krause MA, Guidon A, Tubman A, Fujioka H, Diallo DA, Doumbo OK, Ho M, Wellems TE, Fairhurst RM. Impaired cytoadherence of Plasmodium falciparum-infected erythrocytes containing sickle haemoglobin. PNAS 2008; 105:991-996.
194. Cabrera G, Cot M, Migot-Nabias F, Kremsner PG, Deloron P, Luty AJ. The sickle cell trait is associated with enhanced immunoglobulin G antibody responses to Plasmodium falciparum variant surface antigens. J Infect Dis 2005; 191:1631-1638.
195. Mockenhaupt FP, Ehrhardt S, Cramer JP, Otchwemah RN, Anemana SD, Goltz K, Mylius F, Dietz E, Eggelte TA, Bienzle U. Hemoglobin C and resistance to severe malaria in Ghanaian children. J Infect Dis 2004; 190:1006-1009.
196. Agarwal A, Guindo A, Cissoko Y, Taylor JG, Coulibaly D, Koné A, Kayentao K, Djimde A, Plowe CV, Doumbo O, Wellems TE, Diallo D. Hemoglobin C associated with protection from severe malaria in the Dogon of Mali, a West African population with a low prevalence of hemoglobin S. Blood 2000; 96:2358-2363.
197. Modiano D, Luoni G, Sirima BS, Simporé J, Verra F, Konaté A, Rastrelli E, Olivieri A, Calissano C, Paganotti GM, D'Urbano L, Sanou I, Sawadogo A, Modiano G, Coluzzi M. Haemoglobin C protects against clinical Plasmodium falciparum malaria. Nature 2001; 414:305-308.
198. Fairhurst RM, Fujioka H, Hayton K, Collins KF, Wellems TE. Aberrant development of Plasmodium falciparum in hemoglobin CC red cells: implications

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
80
for the malaria protective effect of the homozygous state. Blood 2003; 101:3309-3315.
199. Duffy PE, Fried M. Red blood cells that do and red blood cells that don't: how to resist a persistent parasite. Trends Parasitol 2006; 22:99-101.
200. Ohashi J, Naka I, Patarapotikul J, Hananantachai H, Brittenham G, Looareesuwan S, Clark AG, Tokunaga K. Extended linkage disequilibrium surrounding the hemoglobin E variant due to malarial selection. Am J Hum Genet 2004; 74:1198-1208.
201. Chotivanich K, Udomsangpetch R, Pattanapanyasat K, Chierakul W, Simpson J, Looareesuwan S, White N. Hemoglobin E: a balanced polymorphism protective against high parasitemias and thus severe P. falciparum malaria. Blood 2002; 100:1172-1176.
202. Williams TN, Maitland K, Bennett S, Ganczakowski M, Peto TE, Newbold CI, Bowden DK, Weatherall DJ, Clegg JB. High incidence of malaria in alpha-thalassaemic children. Nature 1996; 383:522-525.
203. Wambua S, Mwangi TW, Kortok M, Uyoga SM, Macharia AW, Mwacharo JK, Weatherall DJ, Snow RW, Marsh K, Williams TN. The effect of alpha+-thalassaemia on the incidence of malaria and other diseases in children living on the coast of Kenya. PLoS Med 2006; 3:e158.
204. Williams TN, Wambua S, Uyoga S, Macharia A, Mwacharo JK, Newton CR, Maitland K. Both heterozygous and homozygous alpha+ thalassemias protect against severe and fatal Plasmodium falciparum malaria on the coast of Kenya. Blood 2005; 106:368-371.
205. Cockburn IA, Mackinnon MJ, O'Donnell A, Allen SJ, Moulds JM, Baisor M, Bockarie M, Reeder JC, Rowe JA. A human complement receptor 1 polymorphism that reduces Plasmodium falciparum rosetting confers protection against severe malaria. Proc Natl Acad Sci USA 2004; 101:272-277.
206. Cserti CM, Dzik WH. The ABO blood group system and Plasmodium falciparum malaria. Blood 2007; 110:2250-2258.
207. Uneke CJ. Plasmodium falciparum malaria and ABO blood group: is there any relationship? Parasitol Res 2007; 100:759-765.
208. Carlson J, Wahlgren M. Plasmodium falciparum erythrocyte rosetting is mediated by promiscuous lectin-like interactions. J Exp Med 1992; 176:1311-1317.
209. Barragan A, Kremsner PG, Wahlgren M, Carlson J. Blood group A antigen is a coreceptor in Plasmodium falciparum rosetting. Infect Immun 2000; 68:2971-2975.
210. Rowe A, Obeiro J, Newbold CI, Marsh K. Plasmodium falciparum rosetting is associated with malaria severity in Kenya. Infect Immun 1995; 63:2323-2326.
211. Chotivanich KT, Udomsangpetch R, Pipitaporn B, Angus B, Suputtamongkol Y, Pukrittayakamee S, White NJ. Rosetting characteristics of uninfected erythrocytes from healthy individuals and malaria patients. Ann Trop Med Parasitol 1998; 92:45-56.
212. Rowe JA, Handel IG, Thera MA, Deans AM, Lyke KE, Koné A, Diallo DA, Raza A, Kai O, Marsh K, Plowe CV, Doumbo OK, Moulds JM. Blood group

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
81
O protects against severe Plasmodium falciparum malaria through the mechanism of reduced rosetting. Proc Natl Acad Sci USA 2007; 104:17471-17476.
213. Smith T, Charlwood JD, Kitua AY, Masanja H, Mwankusye S, Alonso PL, Tanner M. Relationships of malaria morbidity with exposure to Plasmodium falciparum in young children in a highly endemic area. Am J Trop Med Hyg 1998; 59:252-257.
214. Snow RW, Bastos de Azevedo I, Lowe BS, Kabiru EW, Nevill CG, Mwankusye S, Kassiga G, Marsh K, Teuscher T. Severe childhood malaria in two areas of markedly different falciparum transmission in east Africa. Acta Trop 1994; 57:289-300.
215. Gupta S, Day KP. A theoretical framework for the immunoepidemiology of Plasmodium falciparum malaria. Parasite Immunol 1994; 16:361-370.
216. Brewster DR, Kwiatkowski D, White NJ. Neurological sequelae of cerebral malaria in children. Lancet 1990; 336:1039-1043.
217. Theander TG. Unstable malaria in Sudan: the influence of the dry season. Malaria in areas of unstable and seasonal transmission. Lessons from Daraweesh. Trans R Soc Trop Med Hyg 1998; 92:589-592.
218. Giha HA, Rosthoj S, Dodoo D, Hviid L, Satti GM, Scheike T, Arnot DE, Theander TG. The epidemiology of febrile malaria episodes in an area of unstable and seasonal transmission. Trans R Soc Trop Med Hyg 2000; 94:645-651.
219. Giha HA, Elghazali G, A-Elgadir TM, A-Elbasit IE, Eltahir EM, Baraka OZ, Khier MM, Adam I, Troye-Blomberg M, Theander TG, Elbashir MI. Clinical pattern of severe Plasmodium falciparum malaria in Sudan in an area characterized by seasonal and unstable malaria transmission. Trans R Soc Trop Med Hyg 2005; 99:243-251.
220. Mak JW, Lim PK, Tan MA, Lam PL, Noor Rain A, Selvadurai GD, Hanjeet K. Parasitological and serological surveys for malaria among the inhabitants of an aborigine village and an adjacent Malay village. Acta Trop 1987; 44:83-89.
221. Terrenato L, Shrestha S, Dixit KA, Luzzatto L, Modiano G, Morpurgo G, Arese P. Decreased malaria morbidity in the Tharu people compared to sympatric populations in Nepal. Ann Trop Med Parasitol 1988; 82:1-11.
222. Greenwood BM, Groenendaal F, Bradley AK, Greenwood AM, Shenton F, Tulloch S, Hayes R. Ethnic differences in the prevalence of splenomegaly and malaria in The Gambia. Ann Trop Med Parasitol 1987; 81:345-354.
223. Bryceson AD, Fleming AF, Edington GM. Splenomegaly in Northern Nigeria. Acta Trop 1976; 33:185-214.
224. Bereczky S, Dolo A, Maiga B, Hayano M, Granath F, Montgomery SM, Daou M, Arama C, Troye-Blomberg M, Doumbo OK, Färnert A. Spleen enlargement and genetic diversity of Plasmodium falciparum infection in two ethnic groups with different malaria susceptibility in Mali, West Africa. Trans R Soc Trop Med Hyg 2006; 100:248-257.
225. Modiano D, Petrarca V, Sirima BS, Bosman A, Nebié I, Diallo D, Lamizana L, Esposito F, Coluzzi M. Plasmodium falciparum malaria in sympatric ethnic groups of Burkina Faso, west Africa. Parassitologia 1995; 37:255-259.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
82
226. Dolo A, Modiano D, Maiga B, Daou M, Dolo G, Guindo H, Ba M, Maiga H, Coulibaly D, Perlman H, Blomberg MT, Touré YT, Coluzzi M, Doumbo O. Difference in susceptibility to malaria between two sympatric ethnic groups in Mali. Am J Trop Med Hyg 2005; 72:243-248.
227. Pandey JP, Nasr A, Rocca KM, Troye-Blomberg M, Elghazali G. Significant differences in GM allotype frequencies between two sympatric tribes with markedly differential susceptibility to malaria. Parasite Immunol 2007; 29:267-269.
228. Modiano D, Chiucchiuini A, Petrarca V, Sirima BS, Luoni G, Roggero MA, Corradin G, Coluzzi M, Esposito F. Interethnic differences in the humoral response to non-repetitive regions of the Plasmodium falciparum circumsporozoite protein. Am J Trop Med Hyg 1999; 61:663-667.
229. Modiano D, Petrarca V, Sirima BS, Nebié I, Diallo D, Esposito F, Coluzzi M. Different response to Plasmodium falciparum malaria in west African sympatric ethnic groups. Proc Natl Acad Sci USA 1996; 93:13206-13211.
230. Modiano D, Chiucchiuini A, Petrarca V, Sirima BS, Luoni G, Perlmann H, Esposito F, Coluzzi M. Humoral response to Plasmodium falciparum Pf155/ring-infected erythrocyte surface antigen and Pf332 in three sympatric ethnic groups of Burkina Faso. Am J Trop Med Hyg 1998; 58:220-224.
231. Bolad A, Farouk SE, Israelsson E, Dolo A, Doumbo OK, Nebié I, Maiga B, Kouriba B, Luoni G, Sirima BS, Modiano D, Berzins K, Troye-Blomberg M. Distinct interethnic differences in immunoglobulin G class/subclass and immunoglobulin M antibody responses to malaria antigens but not in immunoglobulin G responses to nonmalarial antigens in sympatric tribes living in West Africa. Scand J Immunol 2005; 61:380-386.
232. Farouk SE, Dolo A, Bereczky S, Kouriba B, Maiga B, Färnert A, Perlmann H, Hayano M, Montgomery SM, Doumbo OK, Troye-Blomberg M. Different antibody- and cytokine-mediated responses to Plasmodium falciparum parasite in two sympatric ethnic tribes living in Mali. Microbes Infect 2005; 7:110-117.
233. Nasr A, Elghazali G, Giha H, Troye-Blomberg M, Berzins K. Interethnic differences in carriage of haemoglobin AS and Fcgamma receptor IIa (CD32) genotypes in children living in eastern Sudan. Acta Trop 2008; 105:191-195.
234. Torcia MG, Santarlasci V, Cosmi L, Clemente A, Maggi L, Mangano VD, Verra F, Bancone G, Nebie I, Sirima BS, Liotta F, Frosali F, Angeli R, Severini C, Sannella AR, Bonini P, Lucibello M, Maggi E, Garaci E, Coluzzi M, Cozzolino F, Annunziato F, Romagnani S, Modiano D. Functional deficit of T regulatory cells in Fulani, an ethnic group with low susceptibility to Plasmodium falciparum malaria. Proc Natl Acad Sci USA 2008; 105:646-651.
235. Modiano D, Luoni G, Sirima BS, Lanfrancotti A, Petrarca V, Cruciani F, Simporé J, Ciminelli BM, Foglietta E, Grisanti P, Bianco I, Modiano G, Coluzzi M. The lower susceptibility to Plasmodium falciparum malaria of Fulani of Burkina Faso (West Africa) is associated with low frequencies of classic malaria-resistance genes. Trans R Soc Trop Med Hyg 2001; 95:149-152.
236. Rzepczyk CM, Hale K, Woodroffe N, Bobogare A, Csurhes P, Ishii A, Ferrante A. Humoral immune responses of Solomon Islanders to the merozoite

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
83
surface antigen 2 of Plasmodium falciparum show pronounced skewing towards antibodies of the immunoglobulin G3 subclass. Infect Immun 1997; 65:1098-1100.
237. Taylor RR, Smith DB, Robinson VJ, McBride JS, Riley EM. Human antibody response to Plasmodium falciparum merozoite surface protein 2 is serogroup specific and predominantly of the immunoglobulin G3 subclass. Infect Immun 1995; 63:4382-4388.
238. Taylor RR, Allen SJ, Greenwood BM, Riley EM. IgG3 antibodies to Plasmodium falciparum merozoite surface protein 2 (MSP2): increasing prevalence with age and association with clinical immunity to malaria. Am J Trop Med Hyg 1998; 58:406-413.
239. Branch OH, Oloo AJ, Nahlen BL, Kaslow D, Lal AA. Anti-merozoite surface protein-1 19-kDa IgG in mother-infant pairs naturally exposed to Plasmodium falciparum: subclass analysis with age, exposure to asexual parasitemia, and protection against malaria. V. The Asembo Bay Cohort Project. J Infect Dis 2000; 181:1746-1752.
240. Osier FH, Polley SD, Mwangi T, Lowe B, Conway DJ, Marsh K. Naturally acquired antibodies to polymorphic and conserved epitopes of Plasmodium falciparum merozoite surface protein 3. Parasite Immunol 2007; 29:387-394.
241. Soe S, Theisen M, Roussilhon C, Aye KS, Druilhe P. Association between protection against clinical malaria and antibodies to merozoite surface antigens in an area of hyperendemicity in Myanmar: complementarity between responses to merozoite surface protein 3 and the 220-kilodalton glutamate-rich protein. Infect Immun 2004; 72:247-252.
242. Roussilhon C, Oeuvray C, Müller-Graf C, Tall A, Rogier C, Trape JF, Theisen M, Balde A, Pérignon JL, Druilhe P. Long-term clinical protection from falciparum malaria is strongly associated with IgG3 antibodies to merozoite surface protein 3. PLoS Med 2007; 4:e320.
243. Tongren JE, Drakeley CJ, McDonald SL, Reyburn HG, Manjurano A, Nkya WM, Lemnge MM, Gowda CD, Todd JE, Corran PH, Riley EM. Target antigen, age, and duration of antigen exposure independently regulate immunoglobulin G subclass switching in malaria. Infect Immun 2006; 74:257-264.
244. Dodoo D, Theisen M, Kurtzhals JA, Akanmori BD, Koram KA, Jepsen S, Nkrumah FK, Theander TG, Hviid L. Naturally acquired antibodies to the glutamate-rich protein are associated with protection against Plasmodium falciparum malaria. J Infect Dis 2000; 181:1202-1205.
245. Oeuvray C, Theisen M, Rogier C, Trape JF, Jepsen S, Druilhe P. Cytophilic immunoglobulin responses to Plasmodium falciparum glutamate-rich protein are correlated with protection against clinical malaria in Dielmo, Senegal. Infect Immun 2000; 68:2617-2620.
246. Lusingu JP, Vestergaard LS, Alifrangis M, Mmbando BP, Theisen M, Kitua AY, Lemnge MM, Theander TG. Cytophilic antibodies to Plasmodium falciparum glutamate rich protein are associated with malaria protection in an area of holoendemic transmission. Malar J 2005; 4:48.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
84
247. Nebie I, Tiono AB, Diallo DA, Samandoulougou S, Diarra A, Konate AT, Cuzin-Ouattara N, Theisen M, Corradin G, Cousens S, Ouattara AS, Ilboudo-Sanogo E, Sirima BS. Do antibody responses to malaria vaccine candidates influenced by the level of malaria transmission protect from malaria? Trop Med Int Health 2008; 13:229-237.
248. Diallo TO, Spiegel A, Diouf A, Lochouarn L, Kaslow DC, Tall A, Perraut R, Garraud O. Short report: differential evolution of immunoglobulin G1/G3 antibody responses to Plasmodium falciparum MSP119 over time in malaria-immune adult Senegalese patients. Am J Trop Med Hyg 2002; 66:137-139.
249. Osier FH, Fegan G, Polley SD, Murungi L, Verra F, Tetteh KK, Lowe B, Mwangi T, Bull PC, Thomas AW, Cavanagh DR, McBride JS, Lanar DE, Mackinnon MJ, Conway DJ, Marsh K. Breadth and magnitude of antibody responses to multiple Plasmodium falciparum merozoite antigens are associated with protection from clinical malaria. Infect Immun 2008; 76:2240-2248.
250. Gray JC, Corran PH, Mangia E, Gaunt MW, Li Q, Tetteh KK, Polley SD, Conway DJ, Holder AA, Bacarese-Hamilton T, Riley EM, Crisanti A. Profiling the antibody immune response against blood stage malaria vaccine candidates. Clin Chem 2007; 53:1244-1253.
251. Vafa M, Israelsson E, Maiga B, Dolo A, Doumbo OK, Troye-Blomberg M. Relationship between immunoglobulin isotype response to Plasmodium falciparum blood stage antigens and parasitological indexes as well as splenomegaly in sympatric ethnic groups living in Mali. Acta Trop 2009; 109:12-16.
252. Cooke GS, Aucan C, Walley AJ, Segal S, Greenwood BM, Kwiatkowski DP, Hill AV. Association of Fcgamma receptor IIa (CD32) polymorphism with severe malaria in West Africa. Am J Trop Med Hyg 2003; 69:565-568.
253. Omi K, Ohashi J, Patarapotikul J, Hananantachai H, Naka I, Looareesuwan S, Tokunaga K. Fcgamma receptor IIA and IIIB polymorphisms are associated with susceptibility to cerebral malaria. Parasitol Int 2002; 51:361-366.
254. Shi YP, Nahlen BL, Kariuki S, Urdahl KB, McElroy PD, Roberts JM, Lal AA. Fcgamma receptor IIa (CD32) polymorphism is associated with protection of infants against high-density Plasmodium falciparum infection. VII. Asembo Bay Cohort Project. J Infect Dis 2001; 184:107-111.
255. Ouma C, Keller CC, Opondo DA, Were T, Otieno RO, Otieno MF, Orago AS, Ong'Echa JM, Vulule JM, Ferrell RE, Perkins DJ. Association of FCgamma receptor IIA (CD32) polymorphism with malarial anemia and high-density parasitemia in infants and young children. Am J Trop Med Hyg 2006; 74:573-577.
256. Human Development Report 2007/2008. The Human Development Index - going beyond income, Sudan. (http://hdrstats.undp.org/countries/country_fact_sheets/cty_fs_SDN.html). Accessed on February 17, 2009.
257. World Health Organization (WHO/EMRO) Country profile, Sudan. (http://www.emro.who.int/sudan/countryprofile.htm). Accessed on February 17, 2009.

Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
85
258. UNICEF Sudan Background. (http://www.unicef.org/infobycountry/sudan_background.html). Accessed on February 17, 2009.
259. Hamad AA, Nugud Ael H, Arnot DE, Giha HA, Abdel-Muhsin AM, Satti GM, Theander TG, Creasey AM, Babiker HA, Elnaiem DE. A marked seasonality of malaria transmission in two rural sites in eastern Sudan. Acta Trop 2002; 83:71-82.
260. The Human Development Index - going beyond income. 2008 Statistical Update, Mali. (http://hdrstats.undp.org/2008/countries/country_fact_sheets/cty_fs_MLI.html). Accessed on February 17, 2009.
261. World Health Organization Statistical Information System (WHOSIS). (http://www.who.int/whosis/en/index.html). Accessed on February 17, 2009.
262. Braga ÉM, Gorza Scopel KG, Komatsu NT, Silva NM, Ferreira MU. Polymorphism of the Fcγ receptor IIA and malaria morbidity. J Mol Genet Med 2005; 1:5-10.
263. Parren PW, Warmerdam PA, Boeije LC, Arts J, Westerdaal NA, Vlug A, Capel PJ, Aarden LA, van de Winkel JG. On the interaction of IgG subclasses with the low affinity Fc gamma RIIa (CD32) on human monocytes, neutrophils, and platelets. Analysis of a functional polymorphism to human IgG2. J Clin Invest 1992; 90:1537-1546.
264. Sanders LA, Feldman RG, Voorhorst-Ogink MM, de Haas M, Rijkers GT, Capel PJ, Zegers BJ, van de Winkel JG. Human immunoglobulin G (IgG) Fc receptor IIA (CD32) polymorphism and IgG2-mediated bacterial phagocytosis by neutrophils. Infect Immun 1995; 63:73-81.
265. Tebo AE, Kremsner PG, Luty AJ. Fcgamma receptor-mediated phagocytosis of Plasmodium falciparum-infected erythrocytes in vitro. Clin Exp Immunol 2002; 130:300-6.
266. Jafarshad A, Dziegiel MH, Lundquist R, Nielsen LK, Singh S, Druilhe PL. A novel antibody-dependent cellular cytotoxicity mechanism involved in defense against malaria requires costimulation of monocytes FcgammaRII and FcgammaRIII. J Immunol 2007; 178:3099-106.
267. Wentworth AD, Jones LH, Wentworth P Jr, Janda KD, Lerner RA. Antibodies have the intrinsic capacity to destroy antigens. Proc Natl Acad Sci USA 2000; 97:10930-10935.
268. Garraud O, Perraut R, Riveau G, Nutman TB. Class and subclass selection in parasite-specific antibody responses. Trends Parasitol 2003; 19:300-304.
269. Bredius RG, Fijen CA, De Haas M, Kuijper EJ, Weening RS, Van de Winkel JG, Out TA. Role of neutrophil Fc gamma RIIa (CD32) and Fc gamma RIIIb (CD16) polymorphic forms in phagocytosis of human IgG1- and IgG3-opsonized bacteria and erythrocytes. Immunology 1994; 83:624-630.
270. Deloron P, Dubois B, Le Hesran JY, Riche D, Fievet N, Cornet M, Ringwald P, Cot M. Isotypic analysis of maternally transmitted Plasmodium falciparum-specific antibodies in Cameroon, and relationship with risk of P. falciparum infection. Clin Exp Immunol 1997; 110:212-218.
Antibody responses and Fc gamma receptor IIa polymorphism in relation to Plasmodium falciparum malaria
Nnaemeka Chukwukaelo Iriemenam, 2009
86
271. Sarthou JL, Angel G, Aribot G, Rogier C, Dieye A, Toure Balde A, Diatta B, Seignot P, Roussilhon C. Prognostic value of anti-Plasmodium falciparum-specific immunoglobulin G3, cytokines, and their soluble receptors in West African patients with severe malaria. Infect Immun 1997; 65:3271-3276.
272. Brasseur P, Ballet JJ, Druilhe P. Impairment of Plasmodium falciparum-specific antibody response in severe malaria. J Clin Microbiol 1990; 28:265-268.
273. Guitard J, Cottrell G, Magnouha NM, Salanti A, Li T, Sow S, Deloron P, Tuikue Ndam N. Differential evolution of anti-VAR2CSA- IgG3 in primigravidae and multigravidae pregnant women infected by Plasmodium falciparum. Malar J 2008; 7:10.
274. Khusmith S, Druilhe P, Gentilini M. Enhanced Plasmodium falciparum merozoite phagocytosis by monocytes from immune individuals. Infect Immun 1982; 35:874-879.
275. Druilhe P, Spertini F, Soesoe D, Corradin G, Mejia P, Singh S, Audran R, Bouzidi A, Oeuvray C, Roussilhon C. A malaria vaccine that elicits in humans antibodies able to kill Plasmodium falciparum. PLoS Med 2005; 2:e344.
276. Garraud O, Mahanty S, Perraut R. Malaria-specific antibody subclasses in immune individuals: a key source of information for vaccine design. Trends Immunol 2003; 24:30-35.
277. Pinder M, Sutherland CJ, Sisay-Joof F, Ismaili J, McCall MB, Ord R, Hallett R, Holder AA, Milligan P. Immunoglobulin G antibodies to merozoite surface antigens are associated with recovery from chloroquine-resistant Plasmodium falciparum in Gambian children. Infect Immun 2006; 74:2887-2893.
278. Stanisic DI, Richards JS, McCallum FJ, Michon P, King CL, Schoepflin S, Gilson PR, Murphy VJ, Anders RF, Mueller I, Beeson JG. Immunoglobulin G subclass-specific responses against Plasmodium falciparum merozoite antigens are associated with control of parasitemia and protection from symptomatic illness. Infect Immun 2009; 77:1165-1174.
279. Bejon P, Warimwe G, Mackintosh CL, Mackinnon MJ, Kinyanjui SM, Musyoki JN, Bull P, Marsh K. Analysis of immunity to febrile malaria in children that distinguishes immunity from lack of exposure. Infect Immun 2009; 77:1917-1923.
280. Galamo CD, Jafarshad A, Blanc C, Druilhe P. Anti-MSP1 Block 2 Antibodies Are Effective at Parasite Killing in an Allele-Specific Manner by Monocyte-Mediated Antibody-Dependent Cellular Inhibition. J Infect Dis 2009; 199:1151-1154.
