antibiotic review (80% of the knowledge, 80% of the time) dr roland halil, bsc(hon), bscpharm, acpr,...
TRANSCRIPT
Antibiotic Review(80% of the knowledge, 80% of the time)
Dr Roland Halil, BSc(Hon), BScPharm, ACPR, PharmDPharmacist, Bruyere Academic FHT
Assistant Professor, Dept Family Medicine, UottawaTwitter: @RolandHalil
Feb, 2015

Objectives
• Review clinically relevant pathogens in human disease in an ambulatory care setting
• Review antibiotic classes and spectra of activity– Focus on bread and butter examples of each
• Review treatment recommendations for common infections in primary care
Process
1. Map the Bugs– “Know your enemy”
2. Map the Drugs– “Save your ammo”
3. Map the Battlefield

Part 1 - Map the (Clinically Important) Bugs“Know your enemy”
Aerobic
β-Lactamase Negative
β-Lactamase Positive
Bacilli (rods)
Cocci (spheres)
Gram Negative
Gram Positive
Anaerobic
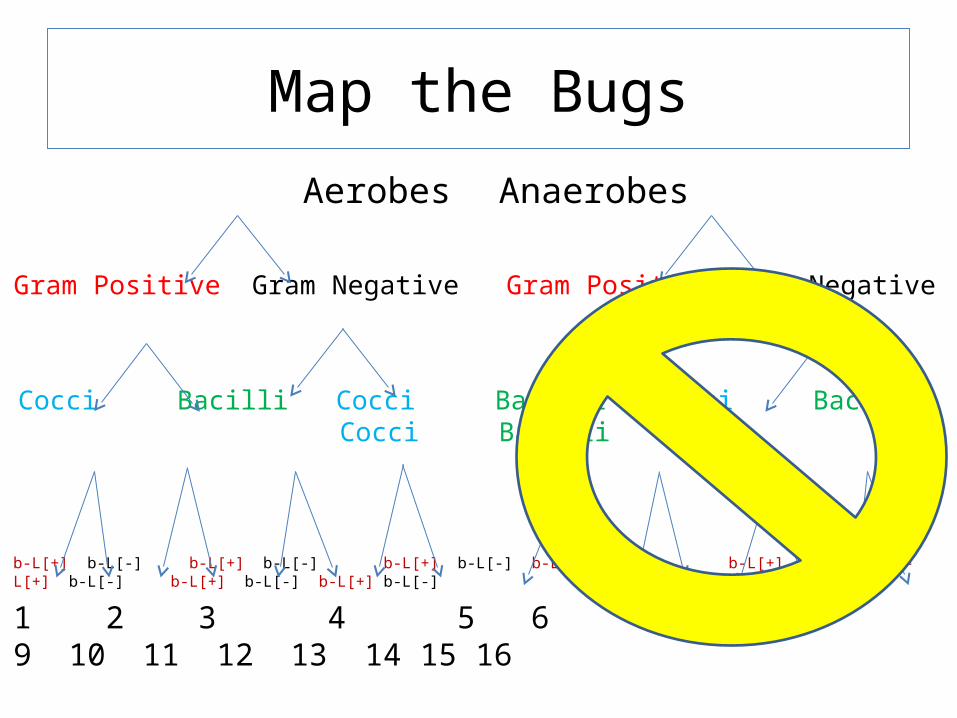
Aerobes Anaerobes
Gram Positive Gram Negative Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli Cocci Bacilli Cocci Bacilli
b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-]
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Map the Bugs

AnaerobesAbove & below the diaphragm
Oral•Simple organisms•Easily handled by penicillins (beta-lactams)– Eg. Actinomyces
Bifidobacterium Fusobacterium Lactobacillus Peptococcus Peptostreptococcus Propionibacterium
etc
Gut•Approx the same, except:
•Human pathogens:• Bacteroides fragilis
(B.frag)• Clostridium difficile
(C.diff)
–More virulent bugs requiring ‘bigger guns’…

Aerobes
Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli
b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-]
1 2 3 4 5 6 7 8
Map the Bugs
Anaerobes
Above & Belowdiaphragm
B.Frag C.Diff
9.

Aerobes
Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli
b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-] b-L[+] b-L[-]
1 2 3 4 5 6 7 8
Map the Bugs
Anaerobes
Belowdiaphragm
B.FragC.Diff
9.

Gram[+] Bacilli
• Not usually pathogenic– Major Exception: Listeria monocytogenes• Listeriosis – enteritis, sepsis, meningitis +/- encephalitis

Aerobes
Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli
(Listeria)
β-L[+] β-L[-] b-L[+] b-L[-] β-L[+] β-L[-]
1 2 3 4 5 6
Map the Bugs
Anaerobes
Belowdiaphragm
B.FragC.Diff
7.

Gm[-] Cocci
• Not usually pathogenic– Major Exceptions: • Neisseria gonorrhea• Neisseria meningitidis and• Moraxella catarrhalis
– (formerly thought to be a type of Neisseria)

Aerobes
Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli (Listeria) (Neisseria &
Moraxella)
β-L[+] β-L[-] β-L[+] β-L[-]
1 2 3 4
Map the Bugs
Anaerobes
Belowdiaphragm
B.FragC.Diff
5.

β-Lactamase Enzymes• First penicillinase described in 1940’s even
before penicillin was clinically available. • Most bugs produce some type of β-lactamase
enzyme that destroys β-lactam antibiotics (pen’s, ceph’s, carbapenems)
– Gm[+] cocci & β-lactamase [-]: Group A & B streps
give Penicillin

Aerobes
Gram Positive Gram Negative
Cocci Bacilli Cocci Bacilli (Listeria) (Neisseria &
Moraxella)
β-L[+] β-L[-] β-L[+] β-L[-]
1 (G.A.S.) 2 3
Map the Bugs
Anaerobes
Belowdiaphragm
B.FragC.Diff
4.

Aerobes
Gram Positive Gram Negative
Cocci Bacilli
β-L[+] both β-L[+]&[-]
1 2
Map the Bugs
Anaerobes
Belowdiaphragm
B.FragC.Diff
3.

Aerobes
Gram [+] Gram [-]
Cocci Bacilli
1 2
Map the Clinically Important Bugs
Anaerobes
(esp. Gut organisms)
Eg. C-Diff& B-frag
4.
Atypicals
1.Legionella pneumonia2.Chlamydia pneumonia3.Mycoplasma pneumonia
3.

1 - Gram [+] Cocci
Staphylococcus
•S. aureus– Methicillin resistant (MRSA)
– Methicillin sensitive (MSSA)
•S. epidermidis– Methicillin resistant (MRSE)
– Methicillin sensitive (MSSE)
– Skin commensal – Rarely pathogenic
Streptococcus•Group A (pyogenes) (β-Lact[-])
•Group B (agalactiae) (β-Lact[-])• Neonates, v. elderly, obstetrics
•S. pneumoniaetc. etc.
Enterococcus•(Formerly thought to be ‘Strep D’)
•E. faecalis•E. faecium
• A “mean” hospital organism

2 - Gram [-] Bacilli
“Easy” to Kill•Proteus mirabilis•Escherichia coli•Klebsiella pneumonia•Salmonella•Shigella•Haemophilus influenza– (Moraxella catarrhalis)
(actually a Gm[-] coccus)
PEcKSS-HiM
“Hard” to Kill•Serratia•Pseudomonas•Acinetobacter•Citrobacter•Enterobacter
SPACE bugs

2.5 - Gram [-] Bacilli“Easy” to Kill
•Proteus mirabilis•Escherichia coli•Klebsiella pneumonia•Salmonella•Shigella
PEcKSS bugs
“Hard” to Kill•Serratia•Pseudomonas•Acinetobacter•Citrobacter•Enterobacter
SPACE bugs
?“Moderate” To Kill• Haemophilus influenza–(Moraxella catarrhalis) (actually a Gm[-] coccus)
HiM bugs

Gram Negative vs Gram Positive Gm[-]: red on stain. (ie. Don’t retain stain) Gm[+]: blue-purple on stain;
Gm[-]: must pass through pores Gm[+]: molecules < 100kDa pass easily.
Gm[-]: b-lactamases concentrated in periplasmic space Gm[+]: b-lactamases diffuse outside cell;

Map the BugsSummary
• Gram positive aerobes:– Cocci
• Staph– Aureus
» MRSA (~8-10%)» MSSA
– Epiderimidis» MRSE (~65%)» MSSE
• Strep– Group A strep (pyogenes) – Group B strep (agalactiae) – Strep Viridans – Strep pneumo etc.
• Enterococcus– Faecalis– Faecium
– Bacilli• Listeria
• Gram negative aerobes:– Bacilli
• Easy to Kill– PEcKSS (Proteus, Ecoli,
Klebsiella, Salmonella, Shigella)– HiM (H.flu and Moraxella
(actually a Gm[-]coccus))
• Hard to Kill– SPACE bugs (Serratia,
Pseudomonas, Acinetobacter, Citrobacter, Enterobacter)
– Cocci• Neisseria
– gonorrhaea– meningitidis
• Moraxella catarhallis
Anaerobes:•Oral•Gut – Bfrag & Cdiff
Atypicals:•Mycoplasma pneumo•Chlamydia pneumo•Legionella pneumo

Map the Bugs - SummaryConjunctivitis: viral
Sinusitis: viral
Oral abscess: oral anaerobes
Pharyngitis: viral(Group A Strep)
Bronchitis: viral
Skin abscess: anaerobes, staph, strepN.B. Boils = Staph
H.pylori:Cdiff / Bfrag:
Otitis media: S.pneumo, Hi,M
AECOPD: S.pneumo, Hi,M
C.A.P: S.pneumo, atypicals –CAP+comorb./risk factors, or NHAP: also HiM bugs
Cellulitis: MSSA, GAS, GBS
UTI (Cystitis): PEcK
Pyelonephritis: PEcK
Traveller’s Diarrhea: (80% bacterial): EcSS, (camphlyobacter)

Part 2 - Map the Drugs(Save your Ammo)

Map the Drugs
• Arms race!– Remember: “Bigger guns
breed higher walls”
• Older drugs tend to be simpler drugs– More narrow spectrum– Broad spectrum drugs
breed resistance– Superbugs develop
• MRSA, VRE, ESBL, etc
• Older drugs have more safety data– Tend to be less toxic– Learn their history– Learn their
pharmacology

Part 2 - Map the Drugs“Save your Ammo”
Penicillins
Tetracyclines
Clindamycin
Vancomycin
Aminoglycosides
Fluoroquinolones
Macrolides
Cephalosporins
Metronidazole
Carbapenems

Antibiotics – Mechanisms of Action
From: http://commons.wikimedia.org/wiki/File:Antibiotics_Mechanisms_of_action.png Accessed Dec 28/12
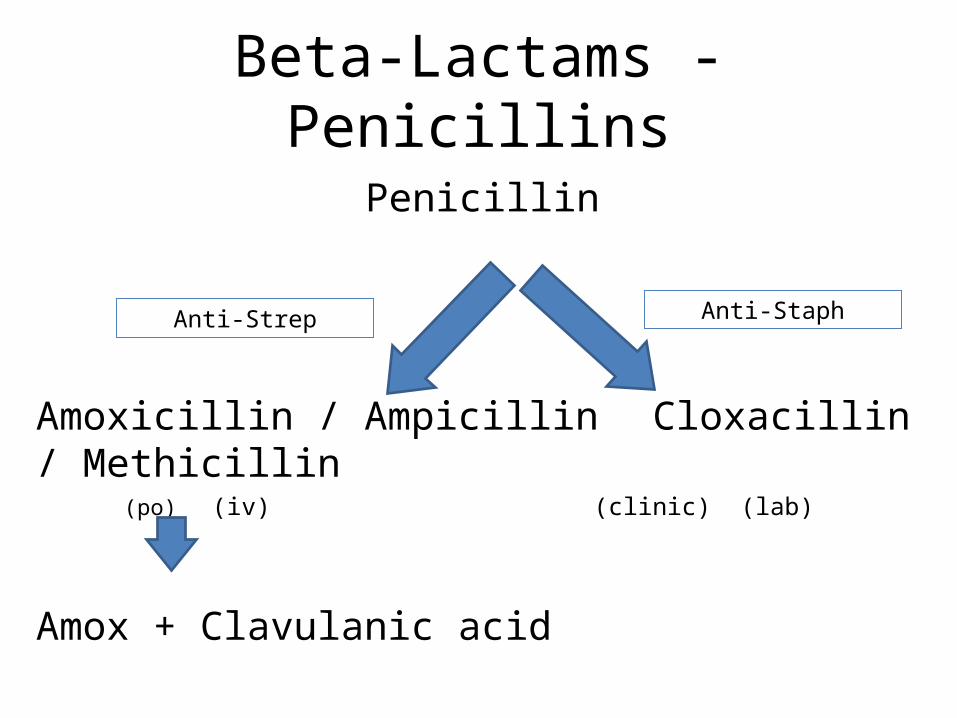
Beta-Lactams - Penicillins
Penicillin
Amoxicillin / Ampicillin Cloxacillin / Methicillin(po) (iv) (clinic) (lab)
Amox + Clavulanic acid
Anti-Strep Anti-Staph

Beta-Lactams - Cephalosporins• 1st Generation– Cephalexin (Keflex™)(or Cefadroxil) (po)– Cefazolin (Ancef™) (iv)
• 2nd Generation– Cefuroxime (po & iv)
• 3rd Generation– Ceftriaxone, Cefotaxime, Ceftazidime (iv)– Cefixime (Suprax™) (po)
• 4th Generation– Cefepime (iv) In
crea
sing
Gra
m[-]
cov
erag
e

Beta-Lactams – Other (FYI)(IV only, inpatient use only)
• Piperacillin (plus tazobactam)– big gun, tazo = suicide substrate, like clavulanic acid
• Carbapenems– Meropenem – Imipenem– Ertapenem
• Monobactams– Aztreonam
Broad spectrum, big gun antibiotics that cover Gm[+], both easy and hard to kill Gm[-] bugs, even some anaerobes.

Antibiotics – Mechanisms of Action
From: http://commons.wikimedia.org/wiki/File:Antibiotics_Mechanisms_of_action.png Accessed Dec 28/12

Fluoroquinolones• 2nd generation
– Ofloxacin– Ciprofloxacin– Norfloxacin
• 3rd generation– Levofloxacin
• 4th generation– Moxifloxacin
• Covers: Gm[-]’s– PEcKSS-HiM & SPACE bugs– 3rd and 4th gen. FQs cover
strep pneumo. well too
• Ofloxacin • Ciprofloxacin – Anti-pseudomonal – the
only PO option! – Norfloxacin
• Same spectrum as Cipro (even anti-Pseudomonal) – but only for cystitis UTI.
• Concentrates in the G.U. system only
• N.B. Not good enough for pyelonephritis or systemic infection

Fluoroquinolones• The “Respiratory FQs”– Concentrate in alveolar
macrophages – Greater than serum concn
1. Levofloxacin– the more active L-
enantiomer of Ofloxacin– Renal clearance
2. Moxifloxacin– Hepatic clearance
• Enhanced coverage of:1. Strep pneumo2. Oral Anaerobes3. Atypicals– N.B. only Moxi cover
B.frag– Neither covers C.diff
• (Both will cover Clostrium non-difficile strains)
• Both have 100% oral bioavailability– Therefore PO = IV dose

Antibiotics – Mechanisms of Action
From: http://commons.wikimedia.org/wiki/File:Antibiotics_Mechanisms_of_action.png Accessed Dec 28/12

Macrolides• Coverage of:– Atypicals, Strep pneumo, &
Hi.M. (Hflu & Mcat)• So, good for respiratory
infections!
– N.B. But doesn’t cover PEcKSS or SPACE bugs
• Erythromycin– Efficacy: Poorer coverage of
H.flu, MSSA– Toxicity:
• Prokinetic = diarrhea!• Worse for QTc prolongation
– Convenience: QID dosing
• Clarithromycin– Better Hflu &MSSA coverage– Less QTc prolongation vs E– Shorter half-life vs Azithro
• BID dosing x 7-10days
• New daily ‘XL’ formulation
• Azithromycin– An azalide, (not a macrolide)
• Same spectrum of activity• Less QTc prolongation vs E & C!
– Long t1/2 – QD dosing x 5d• BUT can breed resistant
S.pneumo (since below [MIC] for long periods of time)

Antibiotics – Mechanisms of Action
From: http://commons.wikimedia.org/wiki/File:Antibiotics_Mechanisms_of_action.png Accessed Dec 28/12

Aminoglycosides
1. Gentamicin2. Tobramycin– Reserved for Pseudomonas
aeruginosa
3. Amikacin
• All excellent Gram[-] coverage: – PEcKSS-HiM and SPACE
bugs
• Efficacy: excellent Gm[-]• Toxicity:– Nephrotoxicity– Ototoxicity– Less now with daily dosing
• Cost:– Cheap, old meds
• Convenience– Now Once daily IV/IM

PharmacodynamicsRelationship between Abx Concentration & Effect
Concentration Dependent Killing
• Higher the peak, better the kill
• i.e. Ratio of peak drug concentration and M.I.C. determines rate of kill.
• Eg. FQs, AGs
Time Dependent Killing• Time over MIC matters• i.e. Independent of peak
concentration. Determined by length of time over MIC
• Eg. B-lactams (Pen, Ceph etc)
Log [Conc]
Time (h)
Peak
MIC
Log [Conc]
Time (h)
MIC

PharmacodynamicsRelationship between Abx Concentration & Effect
Concentration Dependent Killing
• Higher the peak, better the kill
• i.e. Ratio of peak drug concentration and M.I.C. determines rate of kill.
• Eg. FQs, AGs
• With renal impairment:– Maintain the peak,
lengthen the interval– This ensures good rate of
killing while allowing enough time to eliminate the drug and avoid toxicities
– For eg: • If CrCL = 90mL/min -
Levofloxacin 750mg q24h po • If CrCL = 30mL/min –
Levofloxacin 750mg q48h po
Log [Conc]
Time (h)
Peak
MIC
Log [Conc]
Time (h)
Peak
MIC

PharmacodymamicsBactericidal vs Bacteriostatic
• Bactericidal Abx– B-lactams (Pen, Ceph)– Aminoglycosides (AGs)– Fluoroquinolones (FQs)– Rifampin– Metronidazole– Vancomycin
• Bacteriostatic Abx– Tetracyclines– Macrolides– Clindamycin– Chloramphenicol
Rarely a clinically important characteristic, unless the patient is immunocompromised or the risk of death with
delayed/incorrect therapy is high.

Combination Therapy
• Why?– Broaden spectrum • (eg. Mixed infection)
– Synergistic activity for hard to kill bugs • (eg. Enterococcus or pseudomonas)
– Prevent resistance• (eg. TB)
– Reduce dose and side effects

Map the DrugsPharmacology Summary
• Many antibiotic classes– Beta-lactams generally safest agents.• Even at high doses
– Some have overlapping mechanisms of action– Avoid combining similar mechanisms of action • Competing effects may reduce effectiveness of one agent• Eg. Penicillins + vancomycin – cell wall synthesis inhibitors• Eg. Tetracyclines + aminoglycosides –protein synthesis
inhibitors via 30-S subunit of the ribosome

Map the Drugs – Summary
From: http://commons.wikimedia.org/wiki/File:Antibiotics_Mechanisms_of_action.png Accessed Dec 28/12
For: TB, MRSA
For: skin, dental
infx (staph, strep, &
anaerobes)

Part 3 – Map the Battlefield

Map the BattlefieldRational Prescribing
Individual1.Efficacy
– Could be reduced, BUT:– Empiric tx still effective if
it is well chosen • (Lower risk infections,
properly dosed, clinically stable, true indication etc.)
2.Toxicity– Reduced with narrow
spectrum tx
3.Cost– Reduced with older tx
4.Convenience– Usually less convenient
Population1.Efficacy
– Maintained long term with lower resistance rates
2.Toxicity– Reduced since lifespan of
older drugs is maintained
3.Cost– Reduced insurance costs,
economic losses, hospital costs dealing with superbugs
4.Convenience
VS.

Map the Battlefield

Map the Bugs - SummaryConjunctivitis: viral
Sinusitis: viral
Oral abscess: oral anaerobes
Pharyngitis: viral(Group A Strep)
Bronchitis: viral
Skin abscess: anaerobes, staph, strep (GAS, GBS)N.B. boils = staph
H.pylori:Cdiff / Bfrag:
Otitis media: S.pneumo, Hi,M
AECOPD: S.pneumo, Hi,M
C.A.P: S.pneumo, atypicals –CAP+comorb./risk factors, or NHAP: also HiM bugs
Cellulitis: MSSA, GAS, GBS
UTI (Cystitis): PEcK
Pyelonephritis: PEcK
Traveller’s Diarrhea: (80% bacterial): EcSS, (campylobacter)

Map the BattlefieldConjunctivitis: viral – no tx
Sinusitis: viral – no tx
Oral anaerobes: abscess drainage +/- tx (Amox 2g – pre dental sx?)
Pharyngitis: viral – no tx (Group A Strep – Pen VK)
Bronchitis: viral – no tx
Skin abscess: drainage +/- tx
H.pylori: triple po tx PPI + (Clarithro +/- Amox +/- Metro)
Cdiff / Bfrag: Metro / po Vanco
Otitis media: S.pneumo, Hi,M (Amox +/- Clav, Cef2, Septra)
AECOPD: S.pneumo, Hi,M (Amox +/- Clav, Cef2, Septra)
C.A.P: S.pneumo, atypicals – (Amox, Macrolides (Clarithro/Azithro))CAP+comorb./risk factors, or NHAP: also HiM bugs (Combine AmoxClav or Cef2 + Macrolide (or use FQ))
Cellulitis: MSSA, GAS, GBS - (Clox, Cef1, & Clinda (more resistant)
UTI (Cystitis): PEcK – (Septra, Macrobid, Amox+/-Clav, Norflox)
Pyelonephritis: PEcK – (Septra, Amox-Clav, FQ (not Norflox)
Traveller’s Diarrhea: (80% bacterial): EcSS, (campylobacter) - Septra, FQ, (Azithro)

Map the Battlefield
Penicillin(Group A Strep, oral anaerobes, Neisseria)
Amoxicillin / Ampicillin Cloxacillin(Strep & Enterococcus plus (Staph aureus, Staph epi)Easy-to-Kill Gm[-](ie. PEcKSS))
Amox/Clav (Vancomycin)(for Strep & Entero & PEcKSS-HiM) (for MRSA / MRSE)(H.flu & Moraxella can be ~35% amox resistant) (~8-10% / ~ 65% resistant)

Beta-Lactams - Cephalosporins
• 1st Generation– Cephalexin (Keflex™) or Cefadroxil (po)– Cefazolin (Ancef™) (iv)
• 2nd Generation– Cefuroxime (po & iv)
• 3rd Generation– Ceftriaxone, Cefotaxime, Ceftazidime (iv)– Cefixime (Suprax™) (po)
• 4th Generation– Cefipime (iv)
Incr
easi
ng G
ram
[-] c
over
age
MSSA and Strep & PEcKSS (same as Amox)
N.B. never Enterococcus!
To boost: for PEcKSS-HiM(same as Amox/Clav)
SPACE bugs: The Big Guns

SPACE bugs
• The Big Guns:– 3rd and 4th generation Cephalosporins– Carbapenems (Meropenem)– Piperacillin/Tazobactam– Aminoglycosides (Gentamicin, Tobramicin)– Fluoroquinolones (Levofloxacin, Moxi, Cipro)

Reserved for Pseudomonas
• Ciprofloxacin (FQ)– The only PO agent! – (Use Norfloxacin for UTI if a FQ is needed)
• Ceftazidime (Cef3)• Cefipime (Cef4)• Tobramycin (AG)• Piperacillin/Tazobactam• Meropenem

Need for Bigger guns
• There is a higher risk of Gram negative SPACE bugs with:
– More risk factors / comorbidities– COPD, HIV, Diabetes, CKD etc
– More institutionalized settings• Community Retirement Home Nursing Home
Hospital ward ICU ventilated pt in ICU.
Map the Battlefield• PEN – for b-lact[-] Gm[+] cocci (GAS, GBS), oral anaerobes, Neisseria (meningitidis)• ?What to do for Strep pneumo /Enterococcus?
– Amox po / Amp iv (also good for PEcKSS)– How to boost? Amox/Clav (for HiM-PEcKSS)
• ?What to do for Staph?– Clox (MSSA, MSSE); Else Vanco (MRSA, MRSE)
• What about Cef1? (cephalexin / cefadroxil po or cefazolin iv)– Maps to Amox/Amp for PEcKSS and strep
• N.B. NOT Enterococcus (Cef’s never cover enterococcus!)
– How to boost? Cef2 (cefuroxime) for HiM-PEcKSS
• What about SPACE bugs?– FQs, AGs, Cef3, Cef4, Pip/Tazo, Meropenem)– Reserved for Ps aureginosa:(cipro, tobra, ceftazidime, cefipime, pip/tazo, meropenem)
• What about gut anaerobes? (Metro/PO Vanco)• What about atypicals? (Macrolides, Tetracyclines (doxy))• Where does Septra fit? (analogous with Amox/Clav and Cef2)

Summary
• This is far from an exhaustive review• Some parts have been highly simplified for use
in clinical practice• Some memorization is needed with regular
review of the material to retain this knowledge
• Doing so will allow you to choose empiric antibiotics with greater comfort in difficult situations and unfamiliar settings.

Case 1
• Mr. PT• 68 y.o. smoker with AE-COPD
– Vitals stable; ambulatory; fever, productive cough, phlegm is green – PMHx: HTN, COPD– Allergies: penicillin– Meds: Tiotropium 18mcg qd, Ramipril 10mg qd
– Expected pathogens?– Rx options? – Management of allergy status?
• Rx: ________ ?

Allergy status1. Severe diarrhea, pain2. Rash at age of 5 y.o.3. Rash 2 weeks post Rx
– involved hives (raised, intensely itchy spots that come and go over hours), with wheezing & swelling of the skin & throat
4. Major rash 3 yrs ago– flat, blotchy, spread over days but did not
change by the hour
5. Anaphylaxis
1. .2. .3. .
1. .
2. .

BL+ Aerobic GPCAerobic GNB
95% of Staph. species are BL +ve
Penicillin:BL-ve aerobic GPC
oral anaerobesN.meningitidis
Isoxazoyl PCNs:eg. Cloxacillin, Nafcillin
Gut anaerobes(B. fragilis)
Ampicillin/Amoxicillin:HiPEELSS
Easy to Kill GNB
Lacking Activity Vs.
TMP/SMX
Atypical Organisms
MSSA/MSSE
Macrolides:ErythromycinClarithromycinAzithromycin
TMP/SMXTetracyclines
Respiratory FluoroquinolonesGatifloxacinLevofloxacinMoxifloxacin
MRSA(7%)/ MRSE (>65%)
VancomycinRifampin
Fusidic AcidLinezolidSynercid
Amoxicillin/Clavulanic acidAmpicillin/Sulbactam
Second Generation Cephs
1st Generation Cephs:(Cefazolin iv / Cephalexin po)
PEcKSS
H. influenzaeB. fragilis
CefotetanCefoxitin
Metronidazole
Clindamycin
3rd Generation Cephs.
CeftriaxoneCefotaxime
Ceftazidime
4th Generation Cephs:Cefepime
Piperacillin:(P.aeruginosa, Enterobacter)
Never Use Alone!
Piperacillin/TazobactamTicarcillin/Clavulanic Acid
Carbapenems:Imipenem
Meropenem
AMGs:GentamicinTobramycin
Amikacin
CefuroximeCefuroxime axetil
Cefaclor
No Cephalosporin covers:MRSA / MRSE
enterococcus sp.Listeria monocytogenes
Difficult to Kill GNB
FQs:ciprofloxacinofloxacinnorfloxacin
Adapted from: Winslade N. On Continuing Practice 1990-1, volumes 17-18.Prepared By:Sandra A.N. Tailor, Pharm.D.Clinical Coordinator - Infectious DiseasesSunnybrook Health Science CentreDepartment of Pharmacy11/11/02