antibiotic guardian london workshop 2016
TRANSCRIPT

Welcome to the Antibiotic Guardian London Workshop
#antibioticguardian

National actions to tackle antimicrobial
resistance (AMR)
Antibiotic Guardian Roadshow
23 November 2016
Dr Diane Ashiru-Oredope
Pharmacist Lead;
Antimicrobial Resistance Programme
Public Health England
Twitter - @DrDianeAshiru
#AntibioticGuardian

The future if we do not act now
3
By 2050: more deaths from
resistant infections compared to
e.g. cancer
http://amr-review.org/
Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

AMR and Antibiotic Use
4 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Tackling AMR:
• The government
• Professional bodies/organisations/Public health agencies and leads
• Healthcare professionals – human and animal health
• The public
• Pharmaceutical companies
Antimicrobial Resistance
Dr Diane Ashiru-Oredope5 AMR; WLMHT Physical Health Conference Dr Diane Ashiru-Oredope
EVERYONE HAS A ROLE:
5 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Global action on AMR
• WHA 2014 resolution
• WHO Global AMR Action Plan 2015 – framework for
action
• Global Health Security Agenda: AMR action package
- mechanism and collaboration to accelerate
implementation
• United Nations Declaration – September 2016 (193
countries)
http://www.un.org/pga/71/2016/09/21/press-release-hl-meeting-on-antimicrobial-resistance/
6 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

UK 5-year AMR Strategy 2013-18:
Seven key areas for action
PHEHuman health
DH – High Level Steering Group (cross government)
DefraAnimal health
DH
1. Improving infection prevention and control
2. Optimising prescribing practice
3. Improving professional education, training
and public engagement
4. Better access to and use of surveillance
data
• Improving the evidence
base through research
• Developing new drugs,
vaccines and other
diagnostics and treatments
• Strengthening UK and
international collaboration
Impact of EAAD and Antibiotic Guardian Dr Diane Ashiru-Oredope & Ms Katerina (Aikaterini) ChaintarliEAAD and Antibiotic Guardian Dr Diane Ashiru-OredopeAntimicrobial Resistance Dr Diane Ashiru-Oredope7 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Non-susceptibility (%) among (a) E. coli, (b) Klebsiella spp. and (c) Enterobacter spp. from
bacteraemias in England, Wales and Northern Ireland, as reported to PHE-LabBase.
Livermore D M et al. J. Antimicrob. Chemother.
2013;jac.dkt212
© The Author 2013. Published by Oxford University Press on behalf of the British Society for
Antimicrobial Chemotherapy. All rights reserved. For Permissions, please e-mail:
Cephalosporins, diamonds;
ciprofloxacin, squares;
gentamicin, triangles Antimicrobial Use
is a driver for
resistance
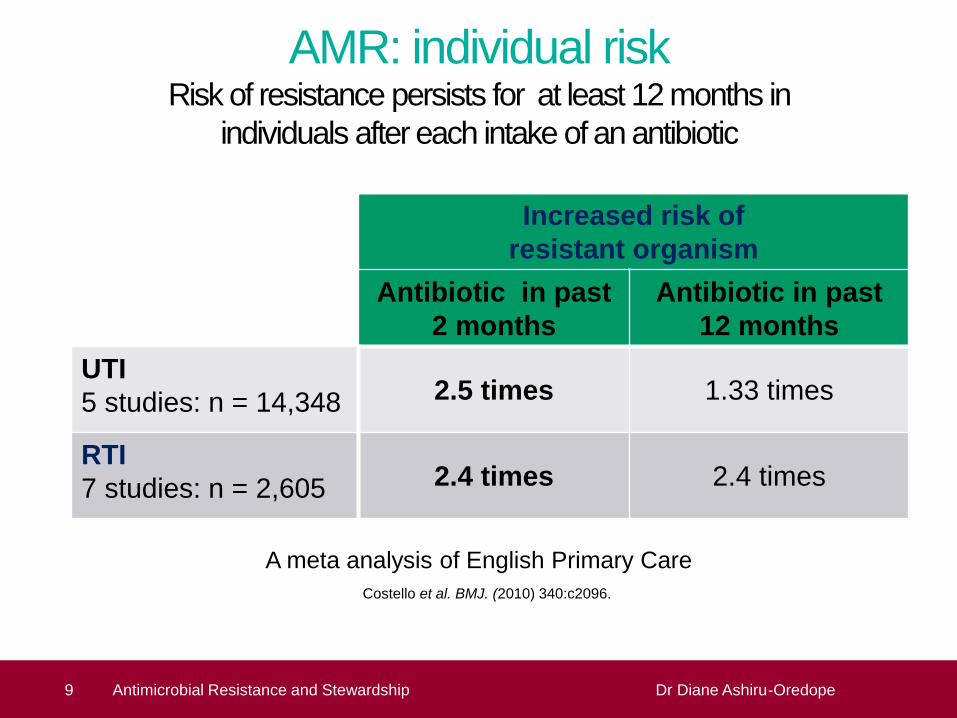
AMR: individual riskRisk of resistance persists for at least 12 months in
individuals after each intake of an antibiotic
Increased risk of
resistant organism
Antibiotic in past
2 months
Antibiotic in past
12 months
UTI
5 studies: n = 14,348 2.5 times 1.33 times
RTI
7 studies: n = 2,605 2.4 times 2.4 times
A meta analysis of English Primary Care
Costello et al. BMJ. (2010) 340:c2096.
9 Antimicrobial Resistance Dr Diane Ashiru-Oredope9 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
10 Antimicrobial Resistance Dr Diane Ashiru-Oredope
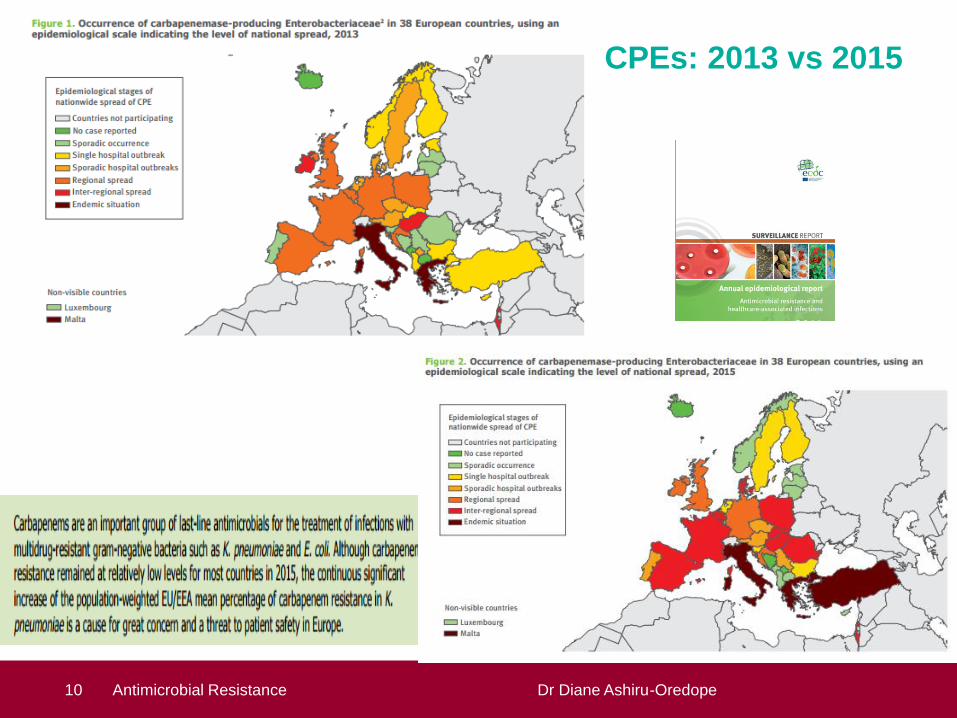
CPEs: 2013 vs 2015
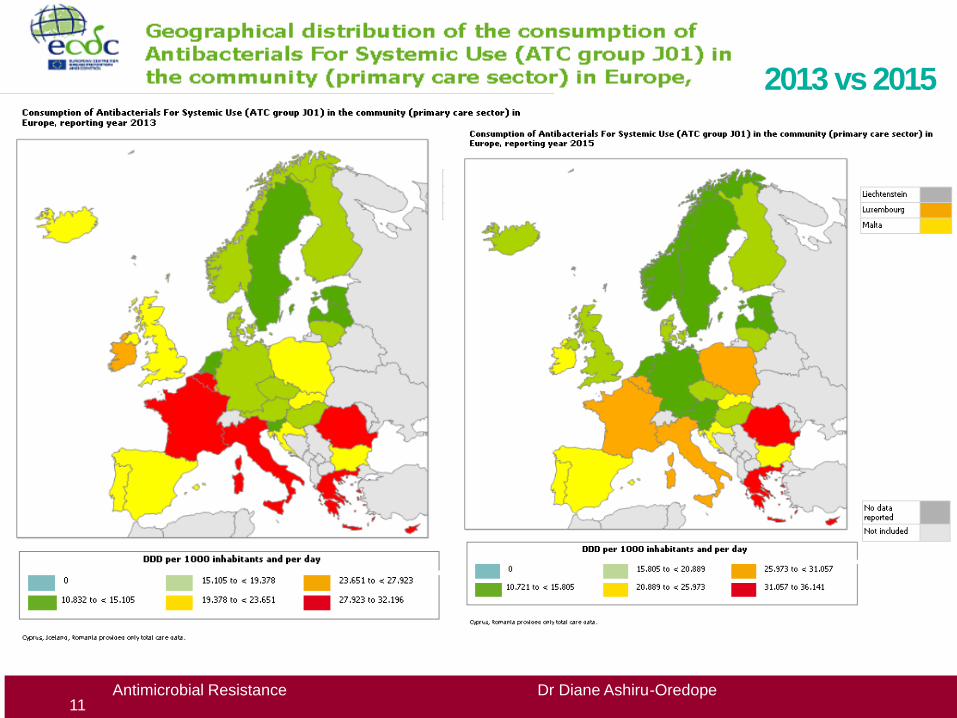
2013 vs 2015
11Antimicrobial Resistance Dr Diane Ashiru-Oredope

England: AMR and AMU surveillance
12 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

14 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
National Surveillance: Antibiotic use and
resistance in England 2015
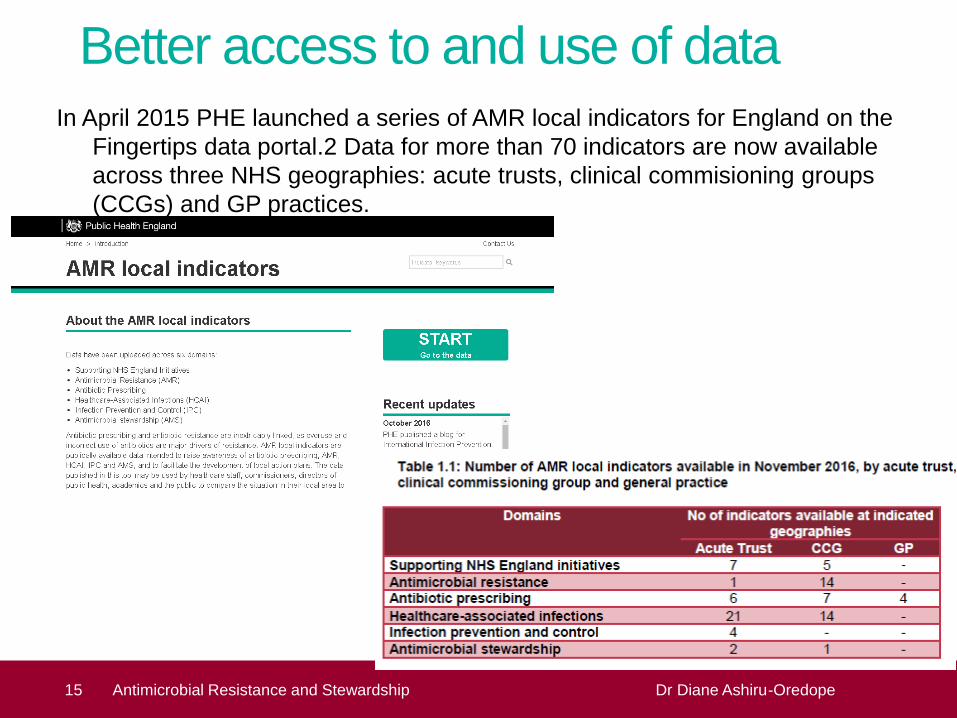
Better access to and use of dataIn April 2015 PHE launched a series of AMR local indicators for England on the
Fingertips data portal.2 Data for more than 70 indicators are now available
across three NHS geographies: acute trusts, clinical commisioning groups
(CCGs) and GP practices.
15 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Other clinical syndromes: E. coli UTI
ESPAUR 2010-2014: Year 2 Report
Improved AMR surveillance and drug-bug
outputs
Secular trends: Bloodstream E. coli AMR
Increased coverage from NHS
laboratories from 30% to 98%
Increased daily reporting from
10% to 82%
Increased automated reporting
from 0% to 78%
16 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Developed Enhanced Surveillance for
Emerging Critical Resistance
CPE* in the UK, 2000-2014 Developed Enhanced
Surveillance
Develop
toolkits for
healthcare
settings*Carbapenemase Producing
Enterobacteriaceae
17Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
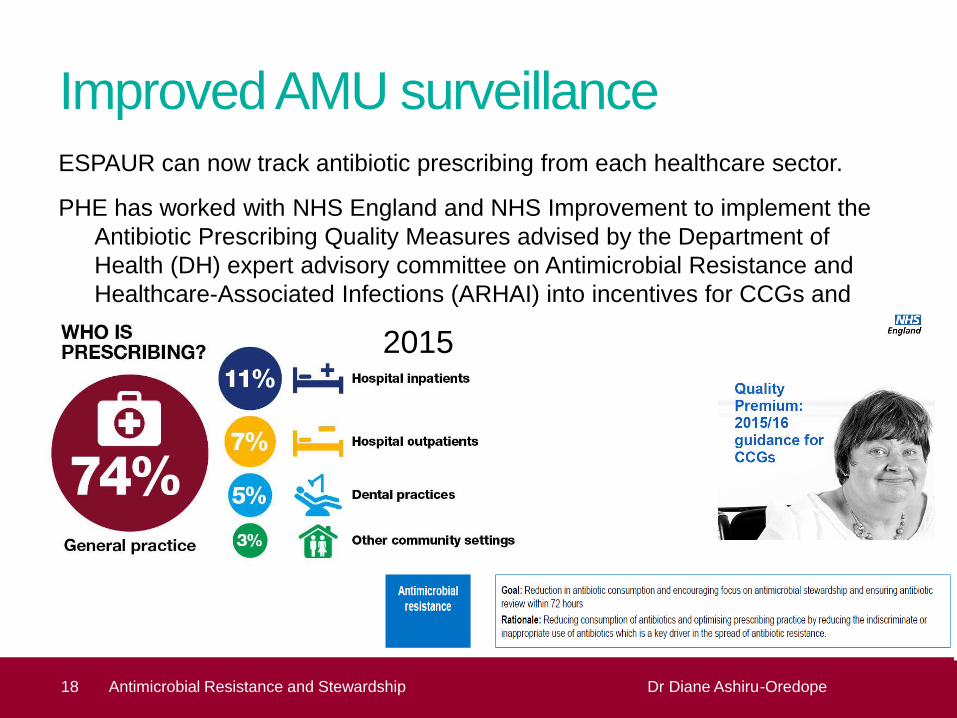
Improved AMU surveillanceESPAUR can now track antibiotic prescribing from each healthcare sector.
PHE has worked with NHS England and NHS Improvement to implement the
Antibiotic Prescribing Quality Measures advised by the Department of
Health (DH) expert advisory committee on Antimicrobial Resistance and
Healthcare-Associated Infections (ARHAI) into incentives for CCGs and
acute trusts.
18 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
2015
18 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

19 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
Improved antimicrobial stewardship
20 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Improved antimicrobial stewardship2014 to 2015: assessment of AMS activities and implementation of national AMS
toolkits in primary and secondary care – TARGET and Start Smart then Focus
(SSTF) respectively – Published in JAC
2015: Assessing the implementation of recommended antimicrobial stewardship
interventions in community healthcare trusts (77% response rate)
21 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Improved antimicrobial stewardshipdeveloped an antimicrobial stewardship surveillance system including tools to
support stewardship audits in acute trusts and these are being used as part
of the CQUIN (Commissioning for Quality and Innovation) in 2016/17.
23 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Antimicrobial Stewardship Surveillance:
CQUIN - data collection and submission
tools
ESPAUR and AMS Tools PHE CSPHDG Professional meeting Dr Diane Ashiru-Oredope24 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

25 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

Improved antimicrobial stewardshipDental antimicrobial stewardship toolkit has been developed and rolled out by
the dental subgroup of ESPAUR in collaboration with Faculty of General
Dental Practice and British Dental Association
https://www.gov.uk/guidance/dental-antimicrobial-stewardship-toolkit:
• Resources
• Guidance
• Education and training tools
• Audit tool and action planning
26 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
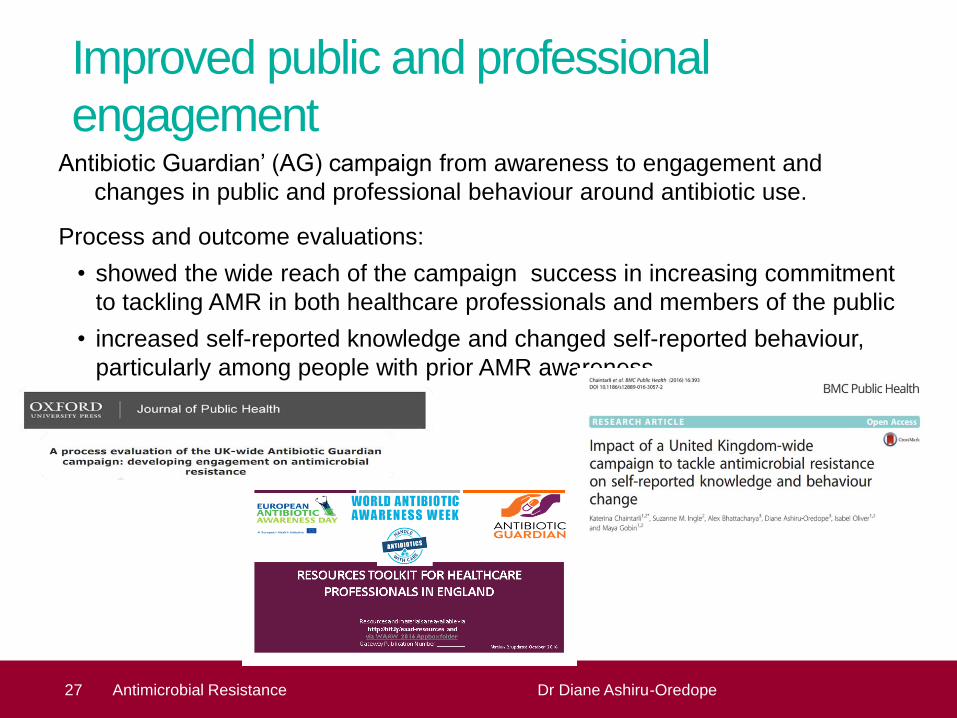
Improved public and professional
engagementAntibiotic Guardian’ (AG) campaign from awareness to engagement and
changes in public and professional behaviour around antibiotic use.
Process and outcome evaluations:
• showed the wide reach of the campaign success in increasing commitment
to tackling AMR in both healthcare professionals and members of the public
• increased self-reported knowledge and changed self-reported behaviour,
particularly among people with prior AMR awareness
27 Antimicrobial Resistance Dr Diane Ashiru-Oredope

Improved public and professional
engagementWorked with Health Education England to scope and develop implementation
options related to education and training of healthcare professionals for
antimicrobial prescribing and stewardship competencies in undergraduate
and postgraduate education and for continuing professional development.
28 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
August 2016

29 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

4. Improved public and professional
engagement
30 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
The PHE Primary Care Unit has continued to work with schools to provide
education about the spread, prevention and treatment of infection through
the ongoing development and delivery e-Bug, a free educational resource
for use in the classroom and at home.

New work on fungal resistance,
surveillance and stewardship
ESPAUR have also increased outputs to look at fungal resistance, antifungal
consumption and stewardship as this is an area of emerging concern
31 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
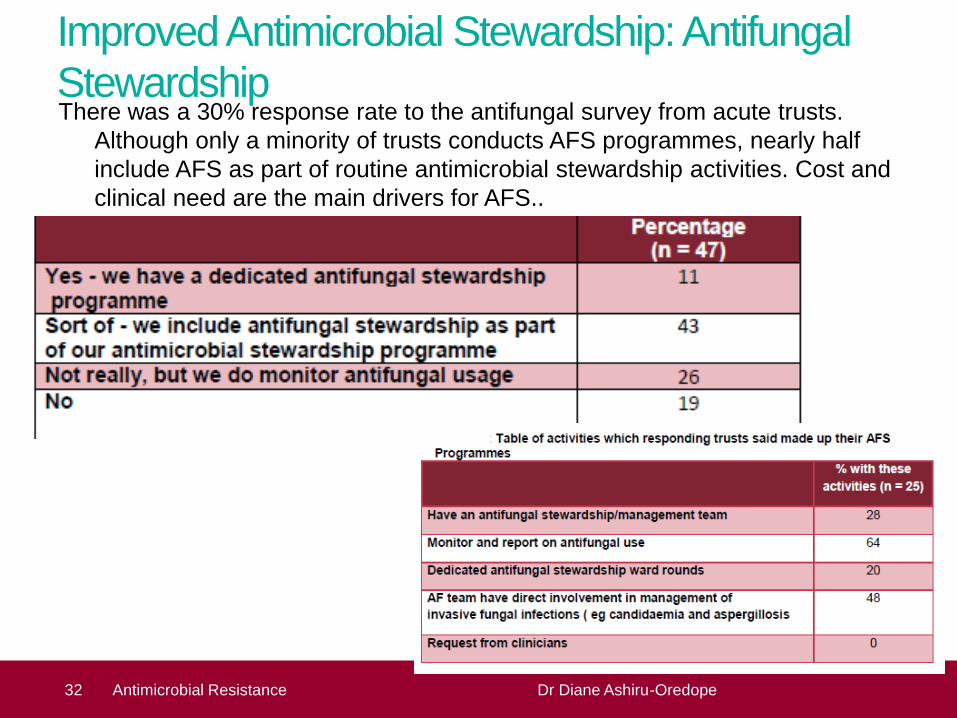
Improved Antimicrobial Stewardship: Antifungal
StewardshipThere was a 30% response rate to the antifungal survey from acute trusts.
Although only a minority of trusts conducts AFS programmes, nearly half
include AFS as part of routine antimicrobial stewardship activities. Cost and
clinical need are the main drivers for AFS..
32 Antimicrobial Resistance Dr Diane Ashiru-Oredope

Launch of the national point prevalence
survey on healthcare-associated infections
and antimicrobial use in acute hospitals
33 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope

34 Antimicrobial Resistance and Stewardship Dr Diane Ashiru-Oredope
• National actions to tackle AMR
• Local Implementation to tackle AMR in the North/Local AMR Action plans/STP
• One Health Initiative - uniting human and veterinary medicine
• Strengthening infection prevention and control practices
• Real world experience of a targeted, narrow spectrum antibiotic for the treatment of
CDI
• Evaluation of the feasibility of using point-of-care C-reactive protein to optimise
primary care prescribing for respiratory tract infections in Scotland
• Antimicrobial Stewardship - national update on CQUIN and QP
• Local – how are we doing towards achieving our AMR CQUIN part a and b
objectives
• Tackling AMR: Engaging with Patients and the Public
• Local examples of engagement with public/patient
• Engaging with students
• BANES – engaging with schools and combining flu campaign and Antibiotic
Awareness
• Engaging with community pharmacies

Antimicrobial Resistance Dr Diane Ashiru-Oredope
You are invited to become an Antibiotic
Guardian today (available via mobiles)
40 Antimicrobial Resistance Dr Diane Ashiru-Oredope
Addressing
AMR, IPC & HCAI
in London
Dr Tania Misra
AMR / IPC/ HCAI lead for PHE London
Consultant in Communicable Disease ControlNE & NC London Health Protection Team

Overview
• Role of PHE in AMR & HCAI
• London AMR & HCAI work – timeline
• AMR work done in London by FES,
Microbiology services and HPTs
• London AMR work plan 2016-2017
• London CRO Action Group
• Future plans
AMR, IPC & HCAI - The PHE role
at the frontline
• Working with partners to assist in the prevention of avoidable
HCAIs through proactive encouragement and promotion
of best practice in IP&C and AMR by providers and
commissioners
• Surveillance and timely feedback of AMR and HCAI-
related risk assessments and information to support actions
to reduce preventable HCAIs, including those due to
resistant organisms, and their consequences
• Support, coordination and expert advice in relation to
preservation of antibiotic effectiveness, HCAI and AMR-
related outbreaks and other situations

AMR Targets
Two new government ambitions
following the publication of the
O’Neill review
• Halving inappropriate
antimicrobial prescribing by 2020
• Halving healthcare acquired
Gram negative bloodstream
infections by 2020.
CQUIN for secondary care
• Reduction in antibiotic consumption per 1,000 admissions
• Empiric review of antibiotic prescriptions
Quality premium for primary care
• reduction in the number of antibiotics prescribed in primary care.
• number of co-amoxiclav, cephalosporins and quinolones as a proportion of the total number of selected antibiotics prescribed in primary care

London centre
AMR activity and timeline
Field Epidemiology
Services
Microbiology
Health Protection
Teams
Engagement with NHS
London since 2006
London DIPC Forum set
up in ~ 2010
Engagement with NHSE since 2012-13
Specialist Advice to Acute and Community Trusts
Building links with private providers
since 2014
Workshops, Study Days,
Training
Research projects
London CRO Action
Group - May 2016

London DIPC forum
Dissemination of key
messages
Collaborative Research /
Projects
Data requests
Communication between trusts,
PHE, NHSE, NHSI
Work done by PHL London for
AMR, IPC & HCAI
PHLL
Microbiology
Services in
London
Post Infection Reviews
– monthlyC difficile PII support Support NHS Trusts to
manage HCAI/ AMR
outbreaks / incidents
Education & Training
On going support to HPTs and NHS
providers on AMR and HCAI related topics

Work done by Field Epidemiology
Services for AMR, IPC & HCAI
Monthly Teleconference held at the centre – organised by FES (provide data, chair the meeting)
Quarterly report on mandatory surveillance data (MRSA, Cdiff, MSSA, E.coli) and other useful HCAI related data – e.g. CRO reports
AMR workbooks
Flagging outliers to relevant HPT
Expert epidemiological advice and support to large / complex outbreaks in hospitals, where requested or necessary
Supporting labs to adopt the Electronic Reporting System (ERS) for CRO samples through training and awareness
Training provided to HPT HCAI leads on data tools
- Fingertips
- HCAI DCS
- DET for Norovirus outbreaks
Work done by Health Protection
Teams for AMR, IPC & HCAI
Developing Positive Working
Relationships
Advice on IPC and AMR issues to linked
trusts / providers proactively through
IPCCs, Health Protection Committees
Useful link between IPC and AMR work in acute and community/ primary care – have an overview of the “patch”
Ensuring Surveillance
Information is Used for Action
Examination and dissemination of HCAI
and AMR data on a monthly basis
Raise concerns about outliers with relevant
provider/s
Support and Advice to Providers
Support and advice for transmission incidents
and outbreak management
Be the link for access to national experts
within PHE and the NIS for complex incidents
Workshops and Study Days
held in London over the last 5 years
• HCAI Study Day – July 2012
• IPC workshops with NHSE – July & Dec 2013
• CPE Workshop, March 2013
• CPE Toolkit Launch event – July 2014
• AMR Study Day – July 2016

Various research projects related to
AMR done in London
• The VIM Pseudomonas pilot study in London, 2012
• The Mupirocin Resistance - data analysis, 2012
• The E coli bacteraemia analysis, 2012
• Retrospective CRO review of London Hospitals, 2013
• The C.difficile in the community analysis, 2014
• The CPE toolkit audit study, 2015
• MSSA data analysis, 2015
• CPE toolkit audit of SL HPT

The London AMR plan for 2016-17
• AMR Study day
• HPT Geo leads to ensure in the acute
and community trusts they cover:
• AMR Audits
• AMR steering / stewardship group
• Process of disseminating the AMR
workbooks
• Encourage use of AMR data and
Fingertips
• HPT HCAI and Geo leads to
familiarise themselves with the
Fingertips tool
• Encourage providers to use the AMR
data to focus resources and effort

The AMR Fingertips Tool
• Antibiotic prescribing and antibiotic
resistance are inextricably linked
• AMR local indicators are publicly
available
• Intended to raise awareness of
antibiotic prescribing, AMR, HCAI,
IPC and AMS
• To facilitate the development of local
action plans

The AMR Fingertips Tool
• Antimicrobial Resistance data is
available by Acute trust (MRSA) and
by CCG
• Antimicrobial Resistance - new data
available by CCG - Rolling quarterly
average proportion of E. coli blood
specimens non-susceptible to the
following antibiotics: 3rd generation
cephalosporins, ciprofloxacin,
gentamicin, piperacillin/ tazobactam

The AMR Fingertips Tool
Antibiotic Prescribing data is available
by Acute Trust, CCG and GP practice
The “compare areas” and “area profiles” functions
enable a picture of antibiotic prescribing at CCG level

London CRO Action Group
• Established July 2016
• Chaired by DDHP
• Representatives from
acute trusts with an interest in CRO
• Quarterly meetings
• Troubleshooting
• Sharing good practice and data

Looking ahead
• Working with community partners on the Gram-
negative bacteraemia target
• Opportunities to engage with new local NHS
planning arrangements in the Sustainability and
Transformation Plans (STPs)
Acknowledgements
– the fab London Team
Microbiology
• Dr Bharat Patel
Field Epidemiology Services
• Shamma Mumtaz
• Geraldine Leong
• Dr James Sedgwick
Health Protection
• Dr Rachel Heathcock
• Dr Anita Bell
• Dr Deborah Turbitt, DDHP
One Health Initiative -
uniting human and
veterinary medicine
Presented by: Professor Peter Borriello
Date: 23rd November 2016 #1086086
ESBLs and food:
disinformation for mass consumption

1. Improving infection prevention and control
2. Optimising prescribing
3. Improving professional education, training, public engagement.
4. Developing new drugs, treatments, diagnostics.
5. Increased access to/use of surveillance data.
6. Identification and prioritisation of AMR research needs.
7. Strengthened international collaboration
UK 5 year AMR strategy:

62
63
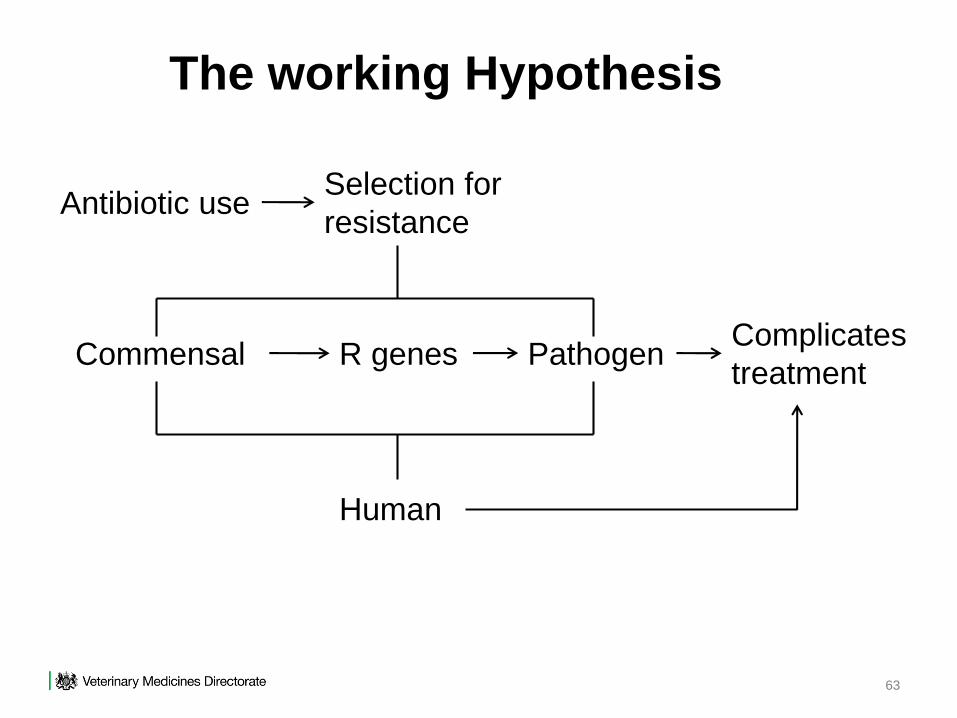
The working Hypothesis
Antibiotic useSelection for
resistance
Commensal R genes PathogenComplicates
treatment
Human

Antibiotic useSelection for
resistance
Commensal R genes PathogenComplicates
treatment
Human
The working Hypothesis
Alternatives
Improve
Infection control
• Food Hygiene
• Zonoses control
Prevent

65
AMRAssumptions which areMostlyReasonable

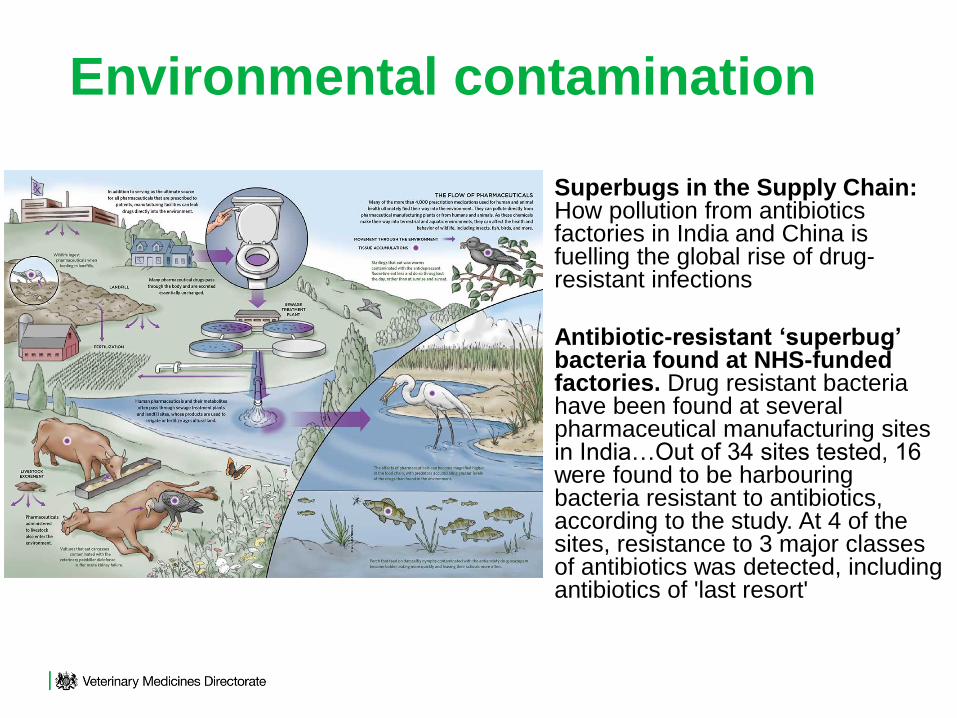
Superbugs in the Supply Chain: How pollution from antibiotics factories in India and China is fuelling the global rise of drug-resistant infections
Antibiotic-resistant ‘superbug’ bacteria found at NHS-funded factories. Drug resistant bacteria have been found at several pharmaceutical manufacturing sites in India…Out of 34 sites tested, 16 were found to be harbouring bacteria resistant to antibiotics, according to the study. At 4 of the sites, resistance to 3 major classes of antibiotics was detected, including antibiotics of 'last resort'
Environmental contamination

“Beaucoup de
germes nous voient
nous et les animaux
comme part du
même
environnement dans
lequel on vit.
Commes ces germes
nous voient comme
part d’un monde
unifié, nous devont
avoir une réponse
unifiée”.
S.P. Borriello, launch of Med Vet Net Association
October 2009

Article 2
70
The Three Key Pillars of National and
International Strategies
1.Optimal Stewardship to prolong
active life of what we have
2.Prevention of spread of resistance
3.Develop alternatives
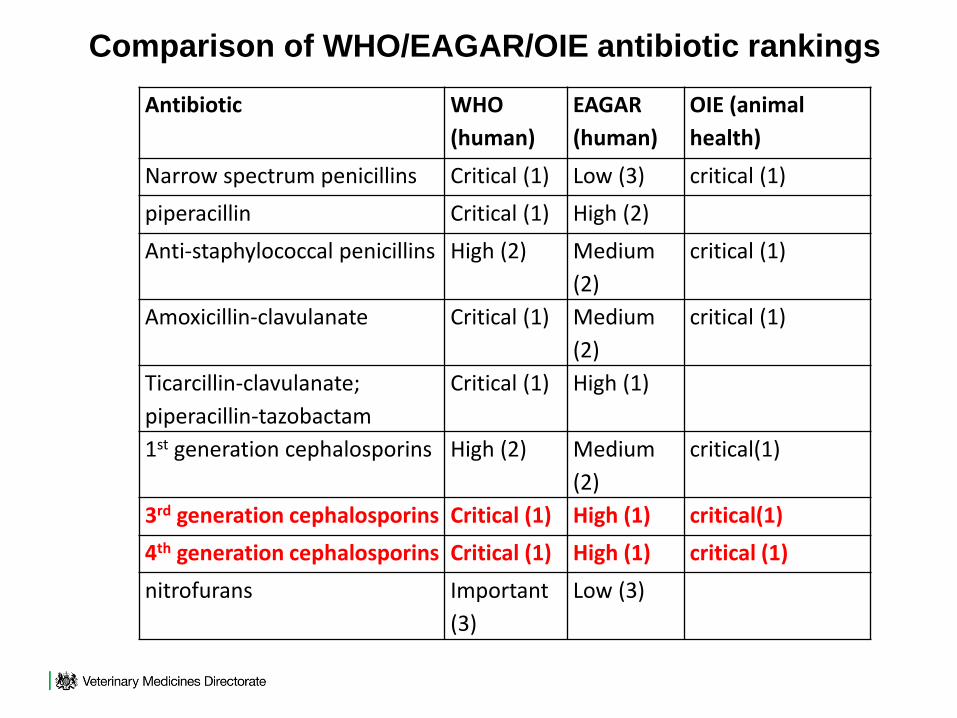
Antibiotic WHO
(human)
EAGAR
(human)
OIE (animal
health)
Narrow spectrum penicillins Critical (1) Low (3) critical (1)
piperacillin Critical (1) High (2)
Anti-staphylococcal penicillins High (2) Medium
(2)
critical (1)
Amoxicillin-clavulanate Critical (1) Medium
(2)
critical (1)
Ticarcillin-clavulanate;
piperacillin-tazobactam
Critical (1) High (1)
1st generation cephalosporins High (2) Medium
(2)
critical(1)
3rd generation cephalosporins Critical (1) High (1) critical(1)
4th generation cephalosporins Critical (1) High (1) critical (1)
nitrofurans Important
(3)
Low (3)
Comparison of WHO/EAGAR/OIE antibiotic rankings
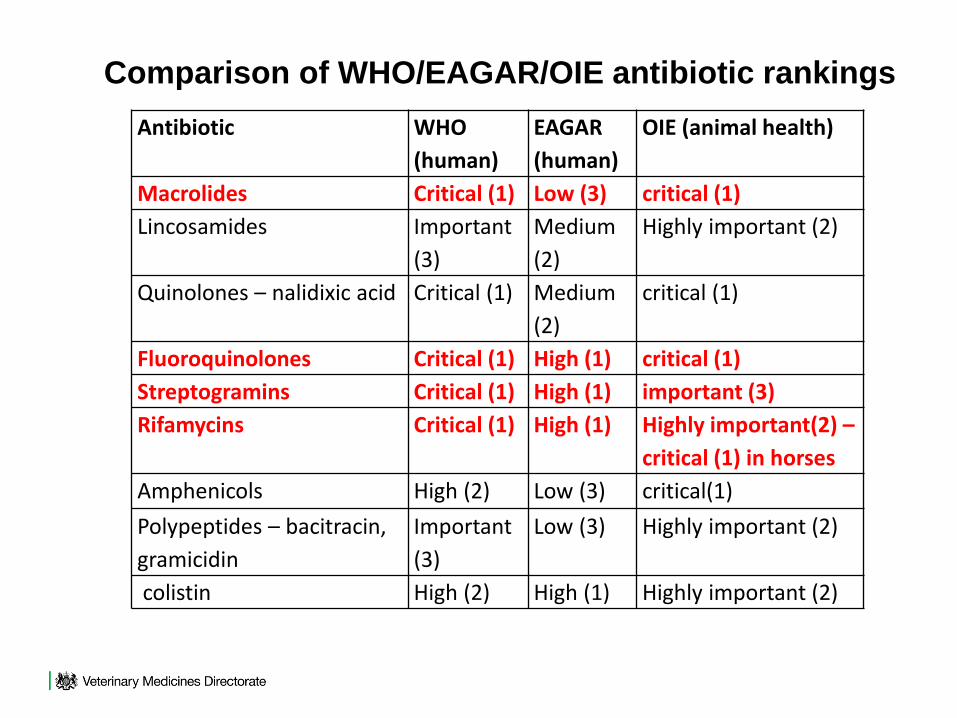
Antibiotic WHO
(human)
EAGAR
(human)
OIE (animal health)
Macrolides Critical (1) Low (3) critical (1)
Lincosamides Important
(3)
Medium
(2)
Highly important (2)
Quinolones – nalidixic acid Critical (1) Medium
(2)
critical (1)
Fluoroquinolones Critical (1) High (1) critical (1)
Streptogramins Critical (1) High (1) important (3)
Rifamycins Critical (1) High (1) Highly important(2) –
critical (1) in horses
Amphenicols High (2) Low (3) critical(1)
Polypeptides – bacitracin,
gramicidin
Important
(3)
Low (3) Highly important (2)
colistin High (2) High (1) Highly important (2)
Comparison of WHO/EAGAR/OIE antibiotic rankings

Antibiotic WHO
(human)
EAGAR (human) OIE (animal
health)
Tetracyclines High (2) Low (3) critical (1)
Glycylcylines - tigecycline Critical (1) High (1)
Aminoglycosides – neomycin, High (2) Low (3) critical (1)
streptomycin Critical (1) Low (3) critical (1)
Gentamicin, tobramycin Critical (1) Medium (2) critical (1)
spectinomycin High (2) Medium (2) critical (1)
Netilimycin, amikacin Critical (1) High (1) critical (1)
Sulfadiazine, trimethoprim High (2) Low (3) critical (1)
Trimethoprim-sulphamethoxazole (co-
rimoxazole)
High (2) Medium (2) critical (1)
Fusidanes – fusidic acid Important
(3)
High (1) important (3)
Comparison of WHO/EAGAR/OIE antibiotic rankings

74
High-Level comparison of veterinary
and human use of antibiotics.
Animal Human
Highest Use
Lowest Use
Livestock
(farm)GP
(Community)
Companion
animals
(Community)
Hospitals

Sales / Use
Human Animal
Sales
Prescription
All ATC Codes

76
Drivers of Enhanced Selection and
Maintenance of Antibiotic Resistance
Poor prescribing
Counterfeits
Globalisation
Inappropriate dosing
Slow diagnostics
Market disincentives
Variable
regulation/guidance/education
77
Key Issues Within and Between
Disciplines
Methodology Degree of Speciation
Break-points Source of Isolates
ECoFFs Drug-bug Combinations

MARAN: Salmonella CipR
2004 0.3%
2005 10.1%

MARAN: Salmonella CipR
2004 0.3% CBp>2µg/ml
2005 10.1% ECV 0.06µg/ml

80

Article 2
82
One Health Reports
E.coli, salmonella, campylobacters.
Issues:
Sample size Incomplete speciation
Methodology Dose data (human)
Definition of R Sales data (animals)

83
Escherichia coli and Resistance to
Key Antibiotic Classes
Cefotaxime/Ceftazidime 10% -
Cefotaxime - 11%
Ceftazidime - 6%
Fluoroquinolones 18% 6%
Gentamicin 9% 3%
Antibiotic Human Animal

84
Salmonella and Resistance to Key
Antibiotic Classes
Humans 2% 16%
Cattle 0% 0%
Chickens* 0% 1% (0%)
Turkeys* 0% 7% (0%)
Pigs* <1% (2%) 0%
Sheep 0% 0%
Cefotaxime Fluoroquinolones

85
Campylobacter and Resistance to
key Antibiotic Classes
Fluoroquinolones Erythromycin
Humans (c.jejuni) 47% 2.5%
Chickens (c.jejuni) 31% 0%
Humans (c.coli) 47% 8%
Chickens (c.coli) 42% 3%
Pigs (c.coli) 13% 28%

One Health and Susceptibility Testing
Campylobacter
Routine lab (h) : Campylobacter spp; disc
Reference lab (h): C.jejuni / coli ; diln
Animal: C.jejuni / coli ; disc

Large animal MRSA- LA-MRSA
animal MRSA- LA-MRSAanimal
MRSA- LA-MRSA• Generally multi-resistant – tetracycline and macrolide
(erythromycin, tylosin) resistance particularly common
• Note that ST398 less virulent than other MRSA strains
(lacks virulence genes)
• Large animal MRSA no longer just ST398 or ST9 –
also ST541 and ST692 (South Korea), ST5 (Korea,
USA), ST1, ST8 (Switzerland)
• Some of the non-ST398 strains carry PVL (Japan,
Korea)
• Pig ST9 strains ex China – 16/100 – reduced
vancomycin susceptibility (Kwok et al, 2013)

MRSA in companion animals
companion animals• Animal link first suspected late 80s–
Scott et al (J Hosp Infect 12:29-34) –
geriatric ward – nursing staff -
resident cat
• Same hospital strain found in pet
dog as in nurse owners – repeated
colonisation (Cefai et al Lancet,
1994, 344:539-540)
• From then on exponential increase
in reported cases – all hospital
strains
• Carriage in veterinarians and staff
reported
• Many cat and dog isolates from
healthy animals (ie carriage) but
some wound infections

89
Most commonly used Antibiotics
Human Animals
1. Penicillins 64% 1. Tetracylines 43.5%
2. Tetracylines 10% 2. Penicillins 22%
3. Macrolides 9.5% 3. Sulph/Trimeth 14.5%
4. Sulph/Trimeth 3% 4. Macrolides 10%
5. Other 13.5% 5. Other 10%



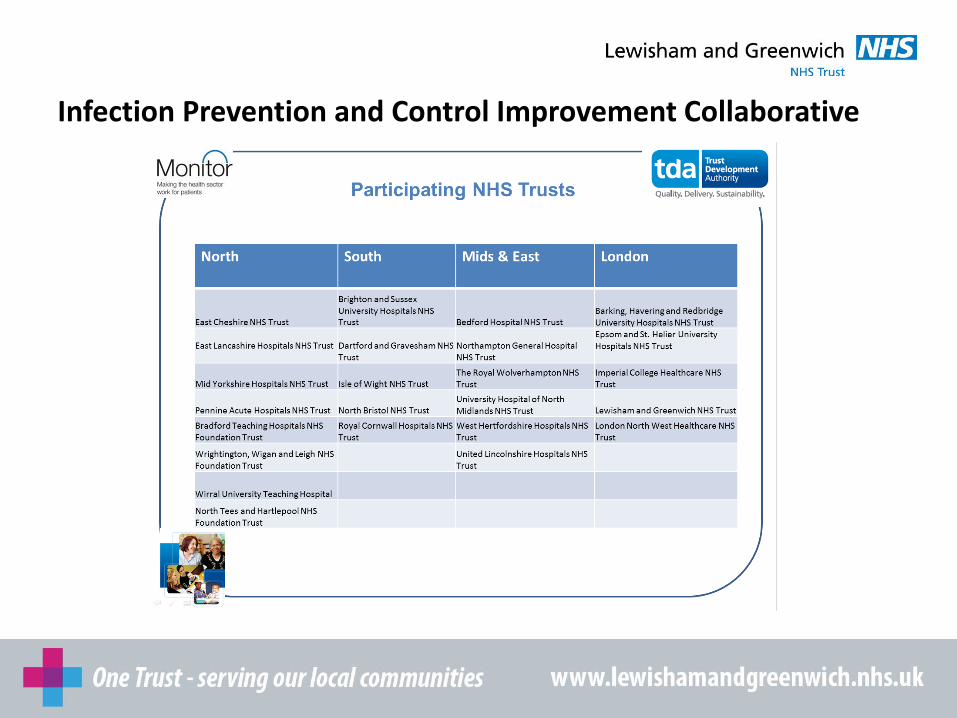
Lewisham and Greenwich NHS
Trust
NHS Improvements -
Infection Prevention and Control
Improvement Collaborative
Chris Wood – Lead Antimicrobial
Pharmacist (QEH)

Feb 2016Visit from TDA

Invitation to participate:
Infection Prevention and Control Improvement Collaborative

Infection Prevention and Control Improvement Collaborative
Better patient outcomes by improving IPC practice by September 2016
Infection Prevention and Control Improvement Collaborative

• Builds on the work many trusts are already undertaking to improve their processes for IPC
• 90 day cycle rapid improvement programme
• Start small in a defined area
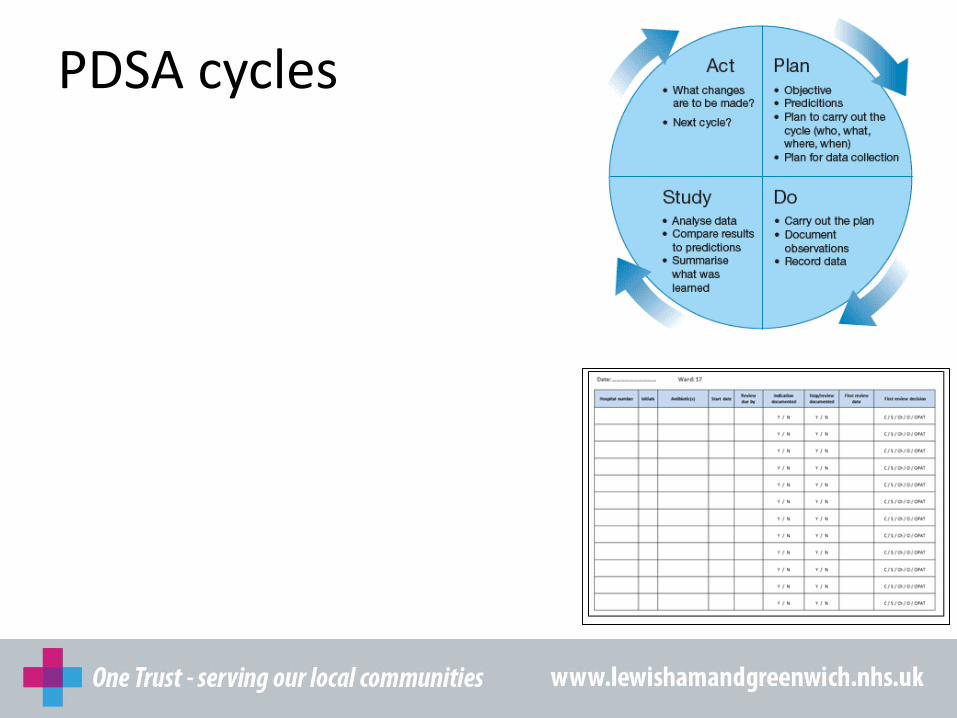
• Undertake early testing (PDSA cycles)
• Use the learning gathered in these areas to choose the interventions with the greatest impact
• Scale-up to full implementation across the organisation
PDSA cycles

Project ideas
• Recording of stool charts
• Stool sampling process
• Antimicrobial prescribing
Why focus on 72 hour review of antibiotics?
“Antimicrobial resistance poses a catastrophic threat. If we don’t act now, any one of us could go into hospital in 20 years for minor surgery and die because of an ordinary infection that can’t be treated by antibiotics. And routine operations like hip replacements or organ transplants could be deadly because of the risk of infection.”
Chief Medical Officer - Dame Sally Davies

Why focus on 72 hour review of antibiotics?
• Threat of antimicrobial resistance

Why focus on 72 hour review of antibiotics?
• Threat of antimicrobial resistance
• Evidence of lapses contributing to C diff cases

Why focus on 72 hour review of antibiotics?
• Threat of antimicrobial resistance
• Evidence of lapses contributing to C diff cases
• Local antibiotic prescribing audit results


Why focus on 72 hour review of antibiotics?
• Threat of antimicrobial resistance
• Evidence of lapses contributing to C diff cases
• Local antibiotic prescribing audit results
• National initiatives (Start Smart then Focus, Antibiotic Guardian)
Why focus on 72 hour review of antibiotics?
• Threat of antimicrobial resistance
• Evidence of lapses contributing to C diff cases
• Local antibiotic prescribing audit results
• National initiatives (Start Smart then Focus, Antibiotic Guardian)
• CQUINs

Aim Primary Drivers Secondary Drivers
Within 90 days increase the
percentage of patients on
antibiotics with a documented
antibiotic review decision within 72 hours
Medical leadership
Divisional Director and consultant engagement
Junior doctor involvement in change process
Junior doctor involvement in auditing
Empowering staff to challenge prescribing
Co-ordinated education of doctors, nurses and pharmacy team
Communication points between pharmacy and medical team
Communication points between nursing and medical team
Tools in place to support process
Materials in place on ward as reminders
Educational materials in place for new staff

Selecting the area
• Team with existing links to the microbiology team
• Area with below average performance in audits
• Engaged junior doctors
• Engaged senior nursing team
• Pharmacy team involvement

Left to right: Alok Khanna (Orthopaedic SHO), Jeanette Baverstock (ward 17 manager), Chris Wood (antimicrobial pharmacist), Juliet Uwagwu (consultant microbiologist), Debbie Flaxman (Deputy director infection prevention and control), Sheila Howard (Infection prevention and control matron)
PDSA cycles


PDSA cycles
• Doctors education programme
• Promotion of Start Smart then Focus principles

• Doctors education programme
• Promotion of Start Smart then Focus
principles

PDSA cycles
• Doctors education programme
• Promotion of Start Smart then Focus principles
• Nurse ward round prompt sheet
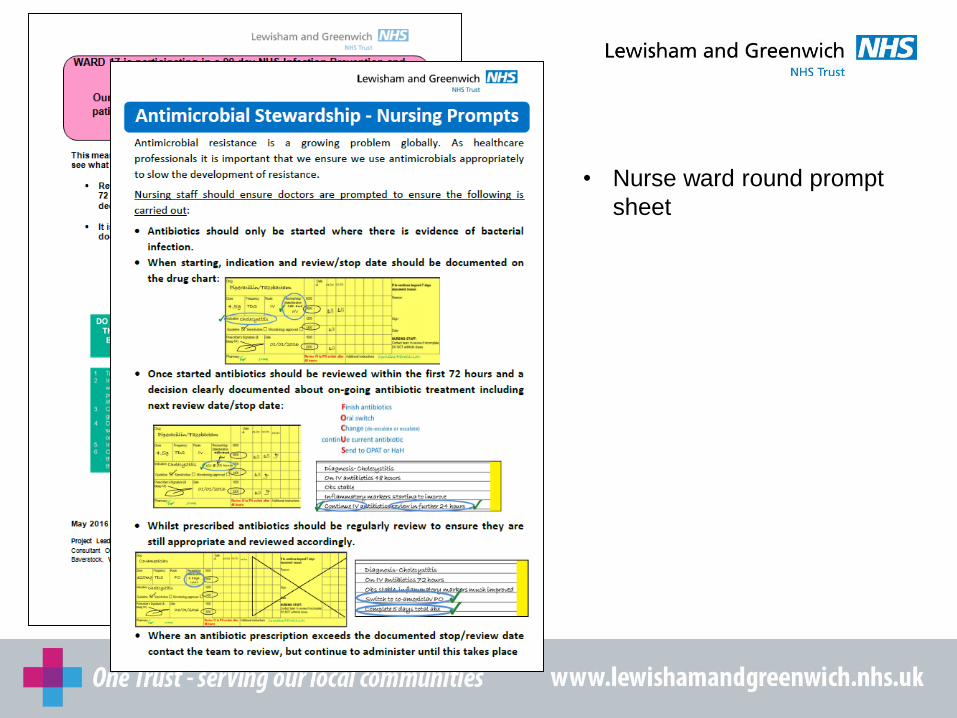
• Nurse ward round prompt
sheet

PDSA cycles
• Doctors education programme
• Promotion of Start Smart then Focus principles
• Nurse ward round prompt sheet
• Ward pharmacist engagement


Challenges
• Small number of patients for auditing
• Time consuming processes
• Maintaining motivation within the team
• Slow speed of generating and testing new ideas
• Roll out not yet completed

Benefits
• Creation of multi-disciplinary team with different approaches
• Trial of different interventions over short period
• Production of new resources which can be used to promote Antimicrobial Stewardship within the Trust
• Learnt new rapid methods of making change

Next steps
• Scaling up
• Working with general surgical team
• Recruit “change champions” - consultant, junior doctor, senior nurse, practice development nurse, pharmacist
• Roll out pack of materials
• Antimicrobial Stewardship introduction video

Antimicrobial Stewardship introduction video
https://www.youtube.com/watch?v=ykvl9ArctvI&t


Evaluation of C-reactive protein in
primary care settings to support
reduction of antibiotic prescribing
for self-limiting respiratory infections
Dr Jacqueline Sneddon,
Project Lead for SAPG

• Patient expectations
• Diagnostic uncertainty
• Decision fatigue
• Targets to reduce unnecessary antibiotic
use
ISSUES WITH MANAGING RESPIRATORY TRACT
INFECTIONS IN PRIMARY CARE

For people presenting with symptoms of lower respiratory tract infection in
primary care, consider a point of care C-reactive protein test if after
clinical assessment a diagnosis of pneumonia has not been made and it is
not clear whether antibiotics should be prescribed.
Use the results of the C-reactive protein test to guide antibiotic prescribing in people
without a clinical diagnosis of pneumonia as follows:
• Do not routinely offer antibiotic therapy if the C-reactive protein concentration is less
than 20 mg/litre.
• Consider a delayed antibiotic prescription (a prescription for use at a later date if
symptoms worsen) if the C-reactive protein concentration is between 20 mg/litre and
100 mg/litre.
• Offer antibiotic therapy if the C-reactive protein concentration is greater than
100 mg/litre
PNEUMONIA IN ADULTS: DIAGNOSIS AND
MANAGEMENT – NICE CG191
https://www.nice.org.uk/guidance/cg191?unlid=3826569120162211655
• Biomarker of infection which is part of the acute phase response to acute tissue injury regardless of the aetiology (infection, trauma and inflammation)
Surrogate marker of infection
• Evidence supports the clinical and cost-effectiveness of CRP testing for management of lower respiratory tract infections in primary care
• CRP is standard of care in some European countries
• CRP testing also recommended in Public Health England (PHE) primary care guidance (May 2016) for acute cough bronchitis
• Test takes 3.5 minutes so can be utilised within GP consultations to inform clinical management
C-REACTIVE PROTEIN

• Jensen A R et al, Biomarkers as point-of-care tests to guide prescription of antibiotics in patients with acute respiratory infections in primary care (Review) Cochrane Collaboration 2014
• Cooke J et al, Narrative review of primary care point-of-care testing (POCT) and antibacterial use in respiratory tract infection (RTI). BMJ Open Resp Res 2015;2:e000086
• Cals J W L et al, Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial, Ann Fam Med 2010;8:124-133
• Oppong R et al. Cost-effectiveness of point-of-care C-reactive protein testing to inform antibiotic prescribing decisions Br J Gen Pract. 2013 Jul; 63(612): e465–e471
• Hunter R, Cost-Effectiveness of Point-of-Care C-Reactive Protein Tests for Respiratory Tract Infection in Primary Care in England. Adv Ther (2015) 32:69–85
• Andreeva A, Melbye H, Usefulness of C-reactive protein testing in acute cough/respiratory tract infection: an open cluster-randomized clinical trial with C-reactive protein testing in the intervention group, BMC Family Practice 2014, 15:80
• Howick J et al, Current and future use of point-of-care tests in primary care: an international survey in Australia, Belgium, The Netherlands, the UK and the USA, BMJ Open 2014;4:e005611
• Huddy J R et al, Point-of-care C reactive protein for the diagnosis of lower respiratory tract infection in NHS primary care: a qualitative study of barriers and facilitators to adoption, BMJ Open 2016;6:e00995
EVIDENCE FOR CRP TESTING
• Evidence base supports use in LRTI
• Work underway in children presenting to Out-of-hours settings
(mainly with URTI) and in patients with COPD exacerbations
(anticipatory care).
• Procalcitonin also useful biomarker for infection but evidence only
established in hospital practice – mainly in ICU to assess response to
treatment and inform when antibiotics can be stopped.
• Early trials in primary care underway.
• Test takes about 20 minutes for a result so logistics of use in primary
care would need different model to CRP
WHEN IS CRP USEFUL?
WHAT ABOUT USING PROCALCITONIN?

AIM - to evaluate the feasibility of using CRP to support clinical decision-making in lower
respiratory tract infections in GP practices in Scotland.
METHOD
• Study steering group established to advise on methodology and governance issues.
• Ten GP practices recruited across four NHS board areas to take part in study.
• Alere Afinion® instruments provided on loan and training provided within each practice.
• Test strips ordered by practices and funded by SAPG (£3.50 per test).
• CRP testing used with patients presenting with suspected LRTI for at least 4 weeks
during the period November 2015–February 2016. NICE CRP thresholds used.
• Data on patient demographics and decision to prescribed or not collected during
consultations.
• On-line survey used to gather feedback on practical aspects of how the test was used
and its perceived impact on GP decision-making and prescribing of antibiotics.
SAPG STUDY
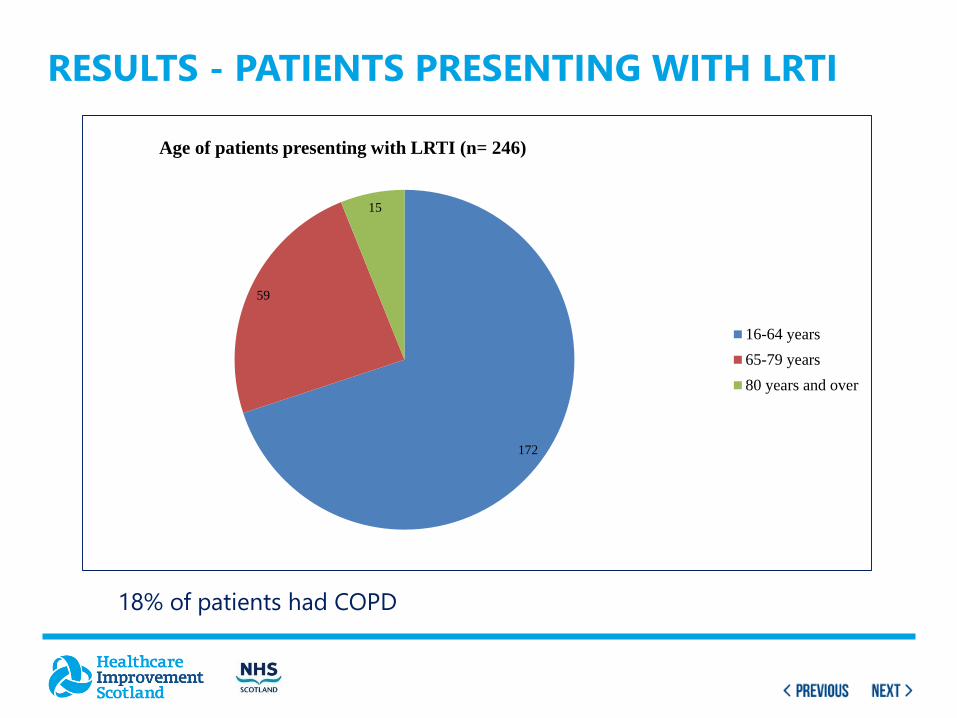
RESULTS - PATIENTS PRESENTING WITH LRTI
172
59
15
Age of patients presenting with LRTI (n= 246)
16-64 years
65-79 years
80 years and over
18% of patients had COPD

CRP TEST RESULTS
72%
24%
4%
0% 10% 20% 30% 40% 50% 60% 70% 80%
CRP result low (<20)
CRP result intermediate (20-100)
CRP result high (>100)
Percentage of patient tests
CRP results (n= 231)
For 15 patients (6%) there were problems with instrument error message so no result recorded

DID CRP TEST RESULT AFFECT DECISION MAKING?
74%
20%
6%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Yes
No
Unsure
Percentage of patients
Influence of CRP on prescribing decision (n=231)

HOW DID CRP INFLUENCE PRESCRIPTIONS?
64%
14%
22%
0% 10% 20% 30% 40% 50% 60% 70%
No prescription
Delayed prescription
Immediate prescription
Percentage of patients
Prescriptions for antibiotics (n=230)
One patient referred to hospital as high CRP

• Completed by 15 GPs.
• Training provided was sufficient but suggestion for a training DVD to provide a refresh on details of user technique.
• Most respondents found test easy to use.
• Three respondents reported having problems with user technique e.g. not using adequate blood sample, getting air bubble in cartridge.
• A few respondents suggested the need to switch on to warm up for 15 minutes and 3+ minute wait for result were potential barriers although this became easier with use.
• A variety of models were used; 4 GPs carried out tests themselves, 8 had test carried out by a practice nurse and 3 used a combination of both approaches.
FEEDBACK SURVEY – USING AFINION INSTRUMENT

• All respondents found it easy to identify patients with LRTI.
• Proportion of consultations where CRP test influenced the decision to not prescribe antibiotics
• Several respondents commented that using the test improved patient engagement and supported them in not prescribing to back up their assessment of clinical symptoms
IMPACT ON CLINICAL PRACTICE
Proportion of patients No. GPs (% GPs)
<25% 3 (20.0%)
25-50% 3 (20.0%)
51 – 75% 5 (33.3%)
>75% 4 (26.7%)

• Most respondents thought their patients found the results of
the CRP test an additional reassurance to their clinical
diagnosis
• Nine (60%) of respondents found the test helpful in dealing
with difficult patients who insisted on an antibiotic
• Other potential benefits identified by some respondents
were:
o increased use of delayed prescriptions for LRTI
o reduced number of patients seeking a second
appointment with the same symptoms
PERCEIVED IMPACT ON PATIENTS

• Overall respondents were positive about the benefits of using CRP testing.
• The main practical concern was the additional time that the test adds to a consultation, 3.5 minutes for the test plus time to explain test to patient is significant within a 10 minute consultation.
• A portable instrument would be of interest for home visits and in care homes, particularly for patients with COPD where exacerbations are often treated with antibiotics despite uncertainty about whether there is an infection.
• Patient experience of the test was positive as it provided reassurance when no antibiotic was required especially for ‘worried well’ patients.
• The majority of respondents would like to see CRP testing used routinely but there were some concerns about cost effectiveness.
SUMMARY OF EVALUATION

• Study results presented to Controlling Antimicrobial
Resistance in Scotland (CARS) group, chaired by CMO
discussions underway within Scottish
Government about further testing/roll out.
• Results shared with colleagues in other UK nations trialling
or implementing CRP testing.
• Results presented as poster at RCGP and FIS conferences
and as presentation at Antibiotic Guardian road show in
London.
WHAT HAPPENS NEXT?

RCGP conference
• Reduced antibiotic prescribing and unscheduled re-attendance by implementation of CRP point of care testing for acute LRTI in a nurse-led clinic - 67 patients (18-65 years)
• Near-patient CRP testing – a game changer antibiotic prescribing?– 3-month study in primary care using 606 tests resulted in 30% reduction in antibiotic prescriptions
Publications
• Should all acutely ill children in primary care be tested with point-of-care CRP: a cluster randomised trial? Restrict to those with high risk of serious infection. Verbakel et al. BMC Medicine (2016) 14:131
• Point-of-care C-reactive protein testing to reduce inappropriate use of antibiotics for non-severe acute respiratory infections in Vietnamese primary health care: a randomised controlled trial - 1028 children and 1009 adults. Lancet Global Health 2016; 4: e633–41
• Evaluating a point-of-care C-reactive protein test to support antibiotic prescribing decisions in a general practice – 94 patients. Clinical Pharmacist, October 2016, 309-318
RECENT STUDIES ON CRP
Point-of-care CRP testing in the diagnosis of pneumonia in adults
DRUG AND THERAPEUTICS BULLETIN OCTOBER 2016
The use of CRP testing may reduce unnecessary antibiotic prescribing while
targeting antibiotic therapy to patients most likely to benefit from it.
Rapid uptake of POC CRP testing in primary care seems unlikely in the absence
of a funded implementation programme.
• Scottish Government HAI Task Force (now SARHAI Strategy
Group) – for funding the study
• Alere Ltd – for supplying Afinion analysers
• Study reference group – for advice on study set up
• SAPG members – for recruiting GP Practices
• GP Practice staff in NHS GGC, Lothian, Tayside and Highland
ACKNOWLEDGEMENTS

THANK YOU
http://www.scottishmedicines.org.uk/files/sapg1/Executive_summary
_Evaluation_of_CRP_testing_in_primary_care_July_2016.pdf

Question and answers from the floor
#antibioticguardian

Lunch and networking
#antibioticguardian

Welcome back
Dr Diane Ashiru-Oredope, Pharmacist Lead, Public Health England
#antibioticguardian

Antimicrobial Stewardship - national
update on CQUIN and QPStuart Brown
Project Lead – AMR and HCAI
NHS Improvement
18th November 2016

Plan
• Background
• AMR CQUIN
• Quality Premium
• It is growing and spreading according to WHO
figures
– 5 of 6 regions show >50% resistance to 3rd gen
cephalosporins & fluoroquinolones in E.coli
– ALL SIX regions have >50% resistance in Kleb
pneumonia to 3rd gen cephalosporins & 2/5 show AMR
to carbapenems
• All antibiotics will be become resistant in time
• Antimicrobial resistance is generally irreversible
• AMR is directly linked to use at national level
• The antibiotic pipeline is dripping at best
Global AMR in 2014

UK Five Year AMR Strategy
Commissioning for Quality
and Innovation (CQUIN)
• CQUIN framework supports improvements
in the quality of hospital services and the
creation of new, improved patterns of care.
• National & local indicators
– 4 or 5 national priorities each year. Worth 2.5%
of income
– 2016-7 Clinical: Sepsis (2nd year), AMR,
Physical health of patient with severe mental
health

Commissioning for Quality and
Innovation (CQUIN) 2016-17
The CQUIN scheme is intended to deliver clinical quality
improvements and drive transformational change. These
will impact on reducing inequalities in access to services,
the experiences of using them and the outcomes
achieved

Part A – Reduction in antibiotic consumption per
1,000 admissions
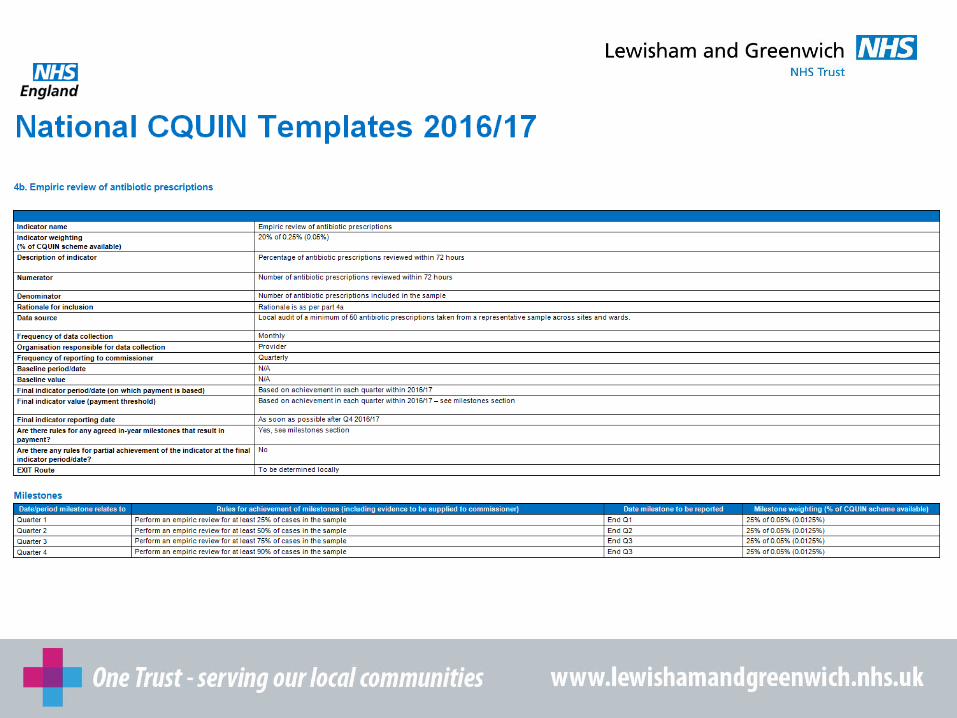
Part B – Empiric review of antibiotic prescriptions
156

AMR CQUIN 2016/17
Part A
• Reduction of 1% or more* in
– total antibiotic usage
– carbapenem usage
– piperacillin-tazobactam usage
• Submission of consumption data to PHE for years
2014/15 and 2015/16
Part B
• Percentage of antibiotics prescriptions reviewed within
72 hours
– Local audit of a minimum of 50 antibiotic prescriptions
* against baseline data 2013/14
Each indicator is worth 0.2% of the CQUIN scheme

AMR-CQUIN – what & why?
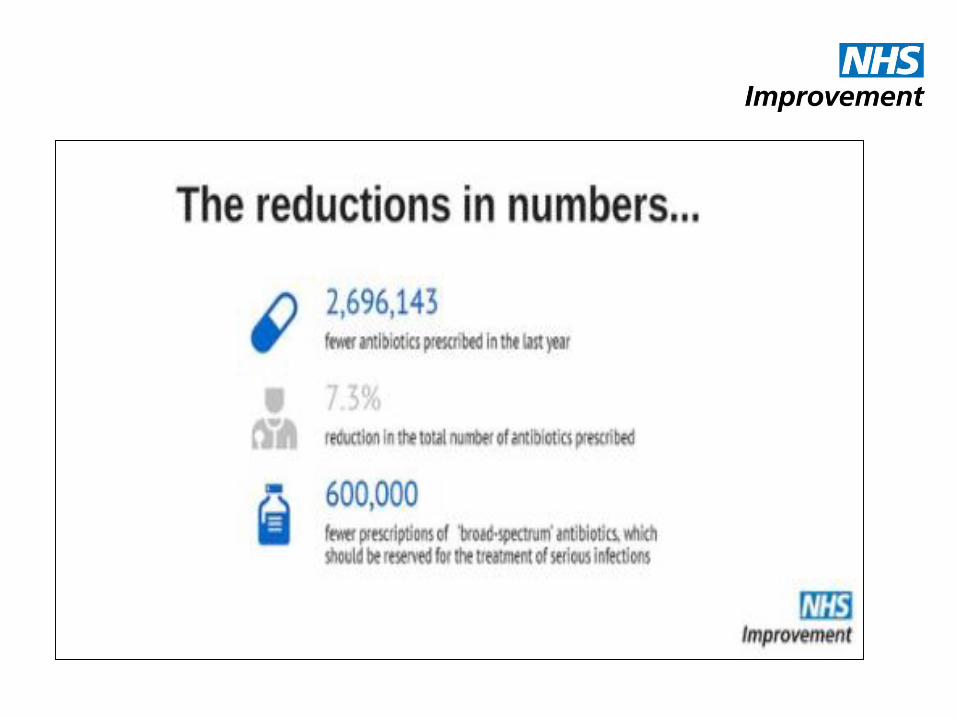
Requires 1% (DDD per admission) vs 2013-4
baseline for:
• Total (IP & OP): +6% over 4 years nationally
• Carbapenems: +36% & KPC outbreaks
• Piperacillin-tazo: +55% & K.pneum-R +36%
E.coli +31%
• 90%+ documentation of empiric antibiotics review
by day 3 (Q1 25%, Q2 50%, Q3 75%, Q4 90%): Only 10% of
Trusts could provide data though mandatory
Hospitals AMS Teams to use ££ to improve IT, staffing,
fund more expensive antibiotics or tests.

Summary: To meet the AMR and
Sepsis CQUINs
• Design systems to force better prescribing eg day 3 review for de-escalation AND IV to oral switch
• Review guidelines containing piperacillin-tazobactam and meropenem. Ensure they are followed through audit & feedback
• Quality improvement, not annual audit of AMS
• Merge sepsis and AMR CQUIN – start smart then focus
• Protected (restricted) antibiotic systems need to work
• Monitor & benchmark antibiotic usage
• Regular but varied communication on progress
• Local education & training at ward level
• Strong and effective multidisciplinary leadership (champions) at all levels

Start Smart – Then Focus
160

Progress So Far (as of October 2016)
Part A Consumption
2014/15 and 2015/16
Consumption data
Q1 2016/17
Number
Submitted
132 124
% of total 86% 81%
• Part B Empiric review of antibiotic prescriptions• 125 of 154 Trusts have submitted data via the PHE AMS online
submission tool
• Data indicates that 81.3% of prescriptions have evidence of review
within 72 hours (range 22-100%).
All data submitted is available on AMR Fingertips
http://fingertips.phe.org.uk/profile/amr-local-indicators

162

163

Quality Premium
2015/16 and 2016/17

Improved antibiotic prescribing in
primary and secondary care
The ‘quality premium’ is intended to reward
clinical commissioning groups (CCGs)
for improvements in the quality of the
services that they commission and for
associated improvements in health
outcomes and reductions in inequalities in
access and in health outcomes
This is a composite Quality Premium consisting
of three parts:
Part a) reduction in the number of antibiotics
prescribed in primary care
Part b) reduction in the proportion of broad
spectrum antibiotics prescribed in primary care
Part c) secondary care providers validating their
total antibiotic prescription data

NHS England Antibiotic Quality
Premium Dashboard

NHS England Antibiotic Quality Premium
Dashboard 2015-16


Antimicrobial resistance (AMR) Improving
antibiotic prescribing in primary care
Quality Premium Guidance for 2016/17
The two parts of the quality premium have specific thresholds as follows:
• Part a) reduction in the number of antibiotics prescribed in primary care. The required performance in 2016/17 must either be:
a 4% (or greater) reduction on 2013/14 performance
OR
equal to (or below) the England 2013/14 mean performance of 1.161 items per STAR-PU
• Part b) number of co-amoxiclav, cephalosporins and quinolones as a proportion of the total number of selected antibiotics prescribed in primary care to either:
to be equal to or lower than 10%, or
to reduce by 20% from each CCG’s 2014/15 value
So how do we continue to improve primary care
antibacterial prescribing in 2016-17?
Respiratory tract infections
• Delayed and No antibiotic prescription resources
• Bristol University NIHR funded research tools for use in
children
• Diagnostics – US Agency for Healthcare Research and Quality
• Vaccination
Urinary Tract Infections
• Link with the Think Kidney AKI programme
• Target nursing home residents
Education and Behavioural change
• Engage schools and universities
• Make every contact count – how can nurses help?
Local AMR Plans

Antimicrobial resistance (AMR)
Improving antibiotic prescribing in
primary care Quality Premium Guidance for 2016/17

Current Performance
173

2017-19 AMR incentives
174
Reducing the impact of serious
infection CQUIN
Reducing Gram Negative
Bloodstream Infections (GNBSIs)
and inappropriate antibiotic
prescribing in at risk groups
Quality Premium for CCGs
a) Timely identification and
treatment for sepsis in
emergency departments and
acute inpatient settings
b) Empiric review of antibiotic
prescriptions between 24-72
hours of patients with sepsis who
are still inpatients at 72 hours
c) Reduction in antibiotic usage
a) Reducing GNBSIs across the
whole health economy
b) Reduction of inappropriate
antibiotic prescribing for urinary
tract infections (UTI) in primary
care
c) Sustained reduction of
inappropriate prescribing in
primary care

175
Tackling AMR: Engaging with
Patients and the Public
Dr Diane Ashiru-Oredope
Pharmacist Lead;
Antimicrobial Resistance Programme
Public Health England
Twitter - @DrDianeAshiru
#AntibioticGuardian

UK 5-year AMR Strategy 2013-18:
Seven key areas for action
PHEHuman health
DH – High Level Steering Group (cross government)
DefraAnimal health
DH
1. Improving infection prevention and control
2. Optimising prescribing practice
3. Improving professional education,
training and public engagement
4. Better access to and use of surveillance
data
• Improving the evidence
base through research
• Developing new drugs,
vaccines and other
diagnostics and treatments
• Strengthening UK and
international collaboration
Impact of EAAD and Antibiotic Guardian Dr Diane Ashiru-Oredope & Ms Katerina (Aikaterini) Chaintarli
Tackling AMR: Engaging with Patients and the Public

Antibiotic resistance is poorly communicated and widely
misunderstood by UK public
“the body becomes resistant to antibiotics”
“If my symptoms have gone, I no longer
need to take antibiotics”
“It’s not my problem”
People have a better understanding when
AMR is presented in a way that is relatable
to them
“By getting antibiotics from the doctor, I
haven’t wasted their time”
Tackling AMR: Engaging with Patients and the Public

Every infection prevented
means less antibiotics
are used
AMR
Tackling AMR: Engaging with Patients and the Public

Tackling AMR: Engaging with Patients and the Public
2016 theme: chain of infection

Timeline of English Antibiotic
Awareness campaigns

1999: Andybiotic –
“Don’t wear me out”
• Press and magazines
• GP surgeries –
leaflets and postcards
• GP non-prescription
pads
• 1999, 2000, 2003,
2006
Educating the public: the value of awareness campaigns Dr Diane Ashiru-OredopeTackling AMR: Engaging with Patients and the Public
Sent to all GP surgeries and
independent pharmacies

Tackling AMR: Engaging with Patients and the Public

Developing plans for EAAD 2014• In previous years EAAD plans included creating educational materials
which healthcare professionals could use as part of local awareness
campaigns.
• Developed EAAD in 2014
• campaign that would be available all year round
• awareness raising engagement
• commitment from healthcare professionals and the public
• First year that the lead organisation aimed to directly engage the public
• Campaign developed by PHE in collaboration with all the UK devolved
administrations and also professional organisations
• Planning group is a multi-disciplinary group with public and third-sector
representation from human and animal health sector across the UK
Tackling AMR: Engaging with Patients and the Public

Educating the public
Moving from awareness to engagement:
Antibiotic Guardian calls on everyone in UK to become
Antibiotic Guardians – Behaviour change – ‘if-then’ approach
pledge system: http://antibioticguardian.com/
Tackling AMR: Engaging with Patients and the Public Combating AMR (CPC Conference) Dr Diane Ashiru-OredopeAntimicrobial Stewardship Dr Diane Ashiru-OredopeEAAD and Antibiotic Guardian Dr Diane Ashiru-OredopeTackling AMR: Engaging with Patients and the Public

Video created with TV doctorEducates on antibiotic resistance; suggests three steps that public can
take to help and a call to become an antibiotic guardian. Available for
download

Antimicrobial Stewardship Dr Diane Ashiru-OredopeTackling AMR: Engaging with Patients and the Public
Current website

Public Information should reflect One Health agenda –
VMD, Bella Moss
Tackling AMR: Engaging with Patients and the Public

Tackling AMR: Engaging with Patients and the Public

NEW GROUPS FOR WAAW/EAAD/AG 2016/17
• Increase local implementation and participation – can you help?
• Healthcare Students – seeking Antibiotic Guardian champions in healthcare schools
• Young families for children and families – Developing “Junior Antibiotic Guardian”
through the use of digital badges. This is in collaboration with PHE nursing directorate, eBug and Makewaves(https://www.makewav.es/).
• The Public through Community Pharmacy
Antimicrobial Stewardship in England Dr Diane Ashiru-Oredope 190 Implementing Antimicrobial Stewardship London AMR Study Day Dr Diane Ashiru-Oredope
Tackling AMR: Engaging with Patients and the Public
New resources for 2016

Tackling AMR: Engaging with Patients and the Public
New resources for 2016

World Antibiotic Awareness Week 2016
Tackling AMR: Engaging with Patients and the Public
#AGCStudents
BBC Doctors: EAAD/AG Replay
AMR Quiz on Playbuzz

Blogs posted duringWAAW 2016
Tackling AMR: Engaging with Patients and the Public

EAAD & Antibiotic Guardian: children
centres; hospitals; community pharmacies
University College London Hospitals
Awareness and engagement in Hospitals, community pharmacies,
universities, organisations in all UK Countries

Engagement via social media – e.g pictures tweeted with
#AntibioticGuardian
Tackling AMR: Engaging with Patients and the Public

World Antibiotic Awareness Week
Tackling AMR: Engaging with Patients and the Public
2016 Registration:
Organisation support: 157
Health School (dentistry, medicine, pharmacy, Vet): 48
Community Pharmacy: 238

#AntibioticGuardian
Tackling AMR: Engaging with Patients and the Public

#EAAD
Tackling AMR: Engaging with Patients and the Public

#AntibioticResistance
Tackling AMR: Engaging with Patients and the Public

Antibiotic Guardian – Russian & Dutch
French currently being developed
Tackling AMR: Engaging with Patients and the Public

Educating children – e-bug led by PHE
Primary Care Unit (Prof Cliodna McNulty)
Europe wide resource, led by Public Health England
e-Bug has
been
translated
into 22
different
languages,
including
most
European
languages,
Turkish
and Arabic
Free educational resource for classroom and home use and makes learning about micro-
organisms, the spread, prevention and treatment of infection fun and accessible for children and
young adults/students

AMR Public Involvement Forum • Engage with the public via strategic partners and other voluntary
organisations, PHE colleagues, lay members
• Representation from
• animal health, respiratory conditions, faith organisation, BME
organisation, home hygiene, various Healthwatch
• Raise awareness of the importance of AMR
• Encourage organisations to engage with the public to raise awareness
of AMR, especially during WAAW, IIPW
• Using resources and expertise to produce a public engagement toolkit
to support local Public Health England centres and Health Protection
teams
Tackling AMR: Engaging with Patients and the Public
Tackling AMR: Engaging with Patients and the Public
AMR Toolkit

Local
engagement
Tackling AMR: Engaging with Patients and the Public

Conclusion• Improving professional education, training and public engagement is
one of the seven key areas of the 5 year UK AMR strategy
• England has participated in EAAD activities since 2008, awareness
was increased but no evidence of increased knowledge and behaviour
change
• For the first time, using behaviour change strategies, the Antibiotic
Guardian campaign has shown evidence of moving from increasing
AWARENESS to ENGAGMENT and commitment from healthcare
professionals and the public
• Evaluation of the Antibiotic Guardian campaign highlighted that it is
an effective for increasing knowledge and changing behaviour (self
reported) particularly among members of public
Tackling AMR: Engaging with Patients and the Public

Antimicrobial Resistance Dr Diane Ashiru-Oredope
You are invited to become an Antibiotic
Guardian Champions today
208 Dr Diane Ashiru-Oredope

The Antibiotic Guardian Campaign
- At the Student End
Osenadia Joseph-Ebare & Lara-Turiya Seitz
Co-leads of the Antibiotic Guardian Health Students Planning Group
AG Health Students Planning Group
- Launched in April till November 2016
- Multidisciplinary team:
- Pharmacy
- Medicine
- Dentistry
- Nursing
- Veterinary medicine

Campaign Goals
Goal: 20 universities
Outcome:
20 universities and health student societies
66 nominated AG representatives
Communication:
- Facebook group
- AGC email account

Materials

How local networks are enabling Antimicrobial Stewardship activity in Bath & North East SomersetSchools & Vaccination
Elizabeth Beech 24th November 2016 Pharmacist - NHS Bath and North East Somerset CCGNational Project Lead Healthcare Acquired Infection and Antimicrobial Resistance - NHS [email protected] @elizbeech


Maximising flu vaccination to reduce unnecessary antibiotic use

Maximising vaccination
• Every contact counts – childhood immunisation sticker
• Book bagging in Key Stage 1
• 40% uptake vs 33% national
• Men ACWY reminder in A levels results
• Pharmacist at the University Freshers Week stall
• 52% uptake vs 35% national
• Flu Myth Busters for health & social care workforce 2016
• School Nurses flu vaccinating 2016

218


Bath & North East Somerset (B&NES)
Primary School Poster Competition• Launched in time for European Antibiotic Awareness Day 2016 and World
Antibiotic Awareness Week 2016
• Year 3 in all B&NES Primary Schools (50+)
• 4 key messages & lesson plans – delivered during WAAW
• Poster competition based on 4 key messages
• Judging & display of posters in community settings – GPs, Community
Pharmacies, local Hospital, Council locations
• Communications campaign – Get a conversation going! Collect and share
on twitter #AntibioticGuardian
220 e-Bug www.e-bug.eu

Bath & North East Somerset (B&NES)
Primary School Poster Competition
The children will design posters around these 4 key messages:
• Hand washing prevents infection
• Many common winter infections such as ear ache, sore throats, coughs and
colds are caused by viruses. Antibiotics do not work for viruses and can
give you side effects like diarrhoea and vomiting
• Vaccination prevents infection, particularly flu vaccination
• Using a tissue when coughing and sneezing can prevent sharing your
infection – Catch it, Bin it, Kill it!
221 e-Bug www.e-bug.eu

222 e-Bug www.e-bug.eu

Bath & North East Somerset 201522% of the whole population26% of children aged up to 10 years

Question and answers from the floor
#antibioticguardian

Concluding comments
Dr Diane Ashiru-Oredope, Pharmacist Lead, Public Health England
#antibioticguardian