anti-her2 epitope map herceptin (4d5) (aa 529-625) tk crd-2 crd-1 data from l. bald & b. fendly...
TRANSCRIPT


Anti-HER2 Epitope MapAnti-HER2 Epitope Map
Herceptin (4D5) (aa 529-625)
TK
CRD-2
CRD-1
data from L. Bald & B. Fendly
888888888888888888888888888888888888888888888888888
Extracellular Domain
Intracellular Domain
CB11


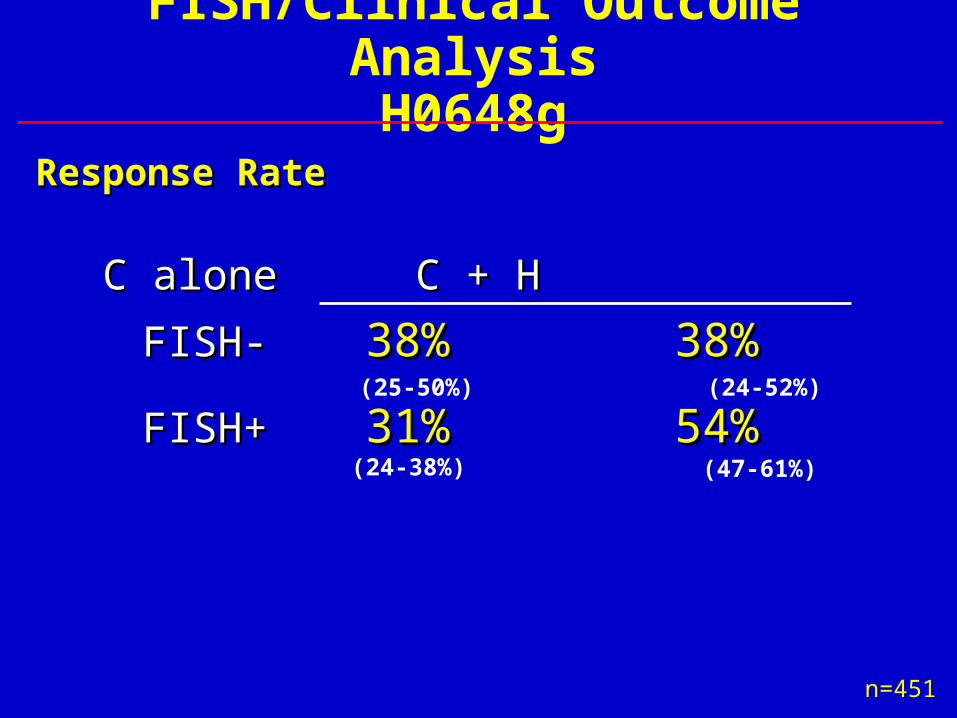
C aloneC alone C + H C + H
FISH-FISH- 38%38% 38% 38%
FISH+FISH+ 31%31% 54% 54%
n=451
(25-50%) (24-52%)
(24-38%) (47-61%)
FISH/Clinical Outcome AnalysisH0648g
Response RateResponse Rate

Number of Patients
FISH+ FISH-
Total patients evaluable 173 36
CR 8 0
PR 25 0
CR + PRCR + PR 33 (19%)33 (19%) 0 (0%)0 (0%)
(95% CI: 14%–26%) (95% CI: 0%–10%)
CR + PR + SD > 6 mo 41 (24%) 0 (0%)CR + PR + SD > 6 mo 41 (24%) 0 (0%)
FISH/Clinical Outcome AnalysisH0649g-Response Rate
IHC 2+/3+ combined IHC 2+/3+ combined
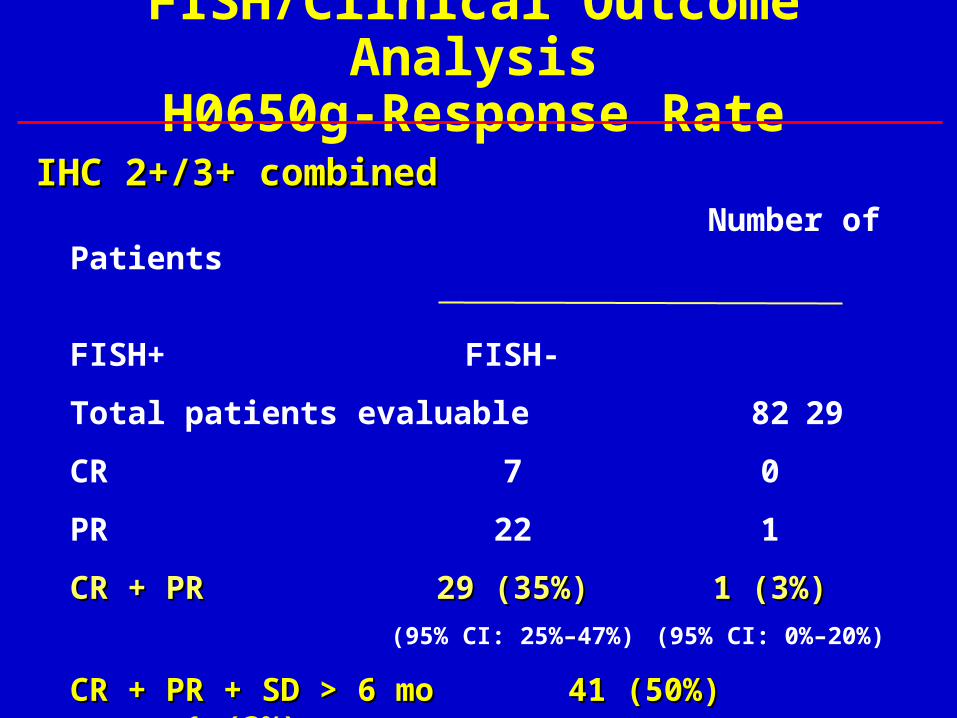
Number of Patients
FISH+ FISH-
Total patients evaluable 82 29
CR 7 0
PR 22 1
CR + PRCR + PR 29 (35%)29 (35%) 1 (3%)1 (3%)
(95% CI: 25%–47%) (95% CI: 0%–20%)
CR + PR + SD > 6 mo 41 (50%) 1 (3%)CR + PR + SD > 6 mo 41 (50%) 1 (3%)
FISH/Clinical Outcome AnalysisH0650g-Response Rate
IHC 2+/3+ combined IHC 2+/3+ combined

Use Herceptin® upfront
*2/3 subsequent Herceptin®
Initial therapyRR(%)
TTP(months)
Survival(months)
Paclitaxel* 17 3.0 18.4
Herceptin® + paclitaxel 49 7.1 25.0
Herceptin® monotherapy 35 3.5 24.4
Other Herceptin® salvage 18 3.2 16.4
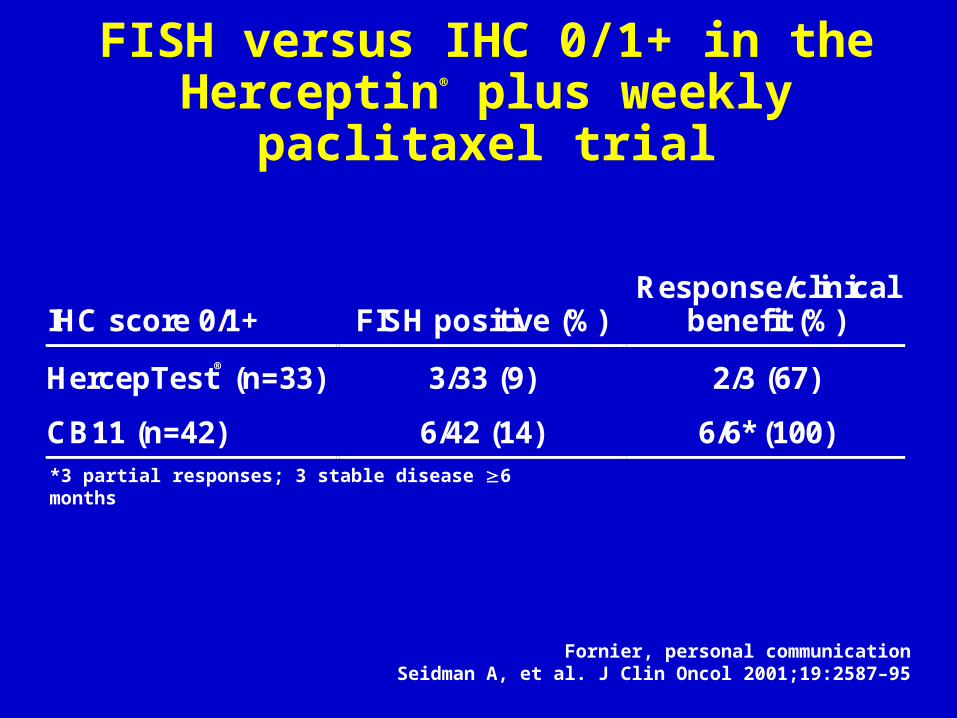
FISH versus IHC 0/1+ in the Herceptin® plus weekly paclitaxel trial
Fornier, personal communicationSeidman A, et al. J Clin Oncol 2001;19:2587–95
*3 partial responses; 3 stable disease 6 months
IHC score 0/1+ FISH positive (%)Response/clinical
benefit (%)
HercepTest® (n=33) 3/33 (9) 2/3 (67)
CB11 (n=42) 6/42 (14) 6/6* (100)

IntergroupReal World IHC vs Central Test
OUT = Outside Lab
% False (+)(3+) OUT vs Central 27
(3+) OUT vs FISH 31
(3+) Central vs FISH 7

NSABP B-31 Central Review(104 cases)
* cases whose eligibility was determined by FISH were excluded from analysis
ICH Test Type of Lab Central LabIHC Neg #of cases
Central LabIHC Neg %of cases
HercepTest 3+(n=80)
Non-ref
Ref
10/52
1/28
19%
4%Other IHCassay(n=24)
Non-ref
Ref
11/23
0/1
48%
0%

SummaryClinical outcomes data in patients with prospective FISH and IHC testingIHC 3+/FISH+IHC 2+/FISH+IHC 3+/FISH-IHC 0 and 1+/FISH+
Cardiac incidence in 1000 patients
Exploratory comparison of Herceptin plus Taxol vs Herceptin plus Taxotere
Gabriel N. Hortobagi, MD, FACP and Pamela N. Klein, MDHER-First



Recent Cardiac Data
H = Herceptin Pamela M. Klein, MDCardiac Dysfunction
Seldman et alTaxol + H
(n=95)
Burstein et alNavelbine + H
(n=40)
Vogel et alH monotherapy
(n=113)
Any cardiacdysfunction 10% 28% 3%Cardiactoxicity CTCgrade 3
3% 0% 3%

Doxorubicin 0.82 - 1.16Paclitaxel 0.91Epirubicin 0.99Vinblastine 1.09
Herceptin and Chemotherapy:In-vitro Activity
Pegram et al. Oncogene. 1999; 18:2241-51.Pietras et al. Oncogene. 1998; 17:2235-49.
Synergistic (CI < 1)
Vinorelbine 0.34Docetaxel / Carboplatin 0.34Docetaxel 0.41Etoposide 0.54Cyclophosphamide 0.57Paclitaxel / Carboplatin 0.64Thiotepa 0.67Cisplatin 0.67Liposomal doxorubicin 0.70
Additive (CI = 1)
Antagonistic (CI > 1)
Methotrexate 1.36Gemcitabine 1.25 - 5.34Fluorouracil 2.87


Taxotere + HerceptinAbstracts
Site Sched. No. RR% Kuzur 3 wk. 16 62 Nicholson Wkly 21 63 Germany Wkly 12 50 Italy Wkly 23 70

Weekly Docetaxel* + HerceptinMDACC ( First or 2nd Line)
(30 pts)
63% RR67% FISH (+)76% ECD (+)
9 mo Med. TTP
* 35 mg/m2/wk x 3/course (med D.I. = 24 mg/m2/wk)JCO 20: 1800, 2002
ToxicityWeekly Docetaxel + Herceptin
(30 pts)
Dexamethasone 4 mg x 3 doses23% DCd Tox
5 pleural effusion1 fatigue1 fungal infection1 bleeding ulcer
JCO 20: 1800, 2002

ToxicityWeekly Docetaxel + Herceptin
MDACC - 30 pts
93% Epiphora - Stenosis12 Pts Cannalicular Intubation10% Gr 1 LVEF16% Gr 2 LVEF1 case CHF (LVEF = 48%)
JCO 20: 1800, 2002
Clinical Activity of Trastuzumab and Vinorelbine in Women with Her2-Overexpressing Metastatic Breast
Cancer: JCO May 2001: Burstein et. Al

Response N RR (%)
CR 3 8PR 27 68CR + PR 30 75*SD > 6 m 2 5PD 8 20
*Conditional corrected 95% confidence interval 57%-89%.
Response Rates: Overall

Phase II Trial of Weekly Vinorelbine and Trastuzumab as First-Line Therapy in
Patients With HER2-Positive Metastatic Breast Cancer: SABCS 2001; Jahanzeb
et. Al.

Navelbine + Herceptin20 Pts.
RR = 60%
Jahanzeb - Asco 2001 - Abst 1986
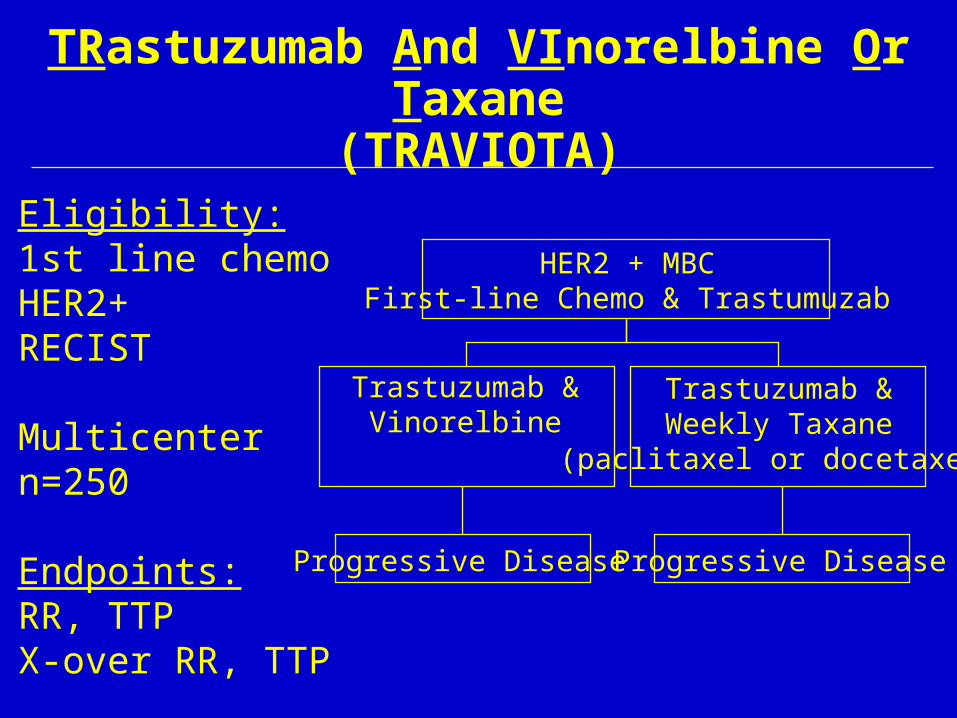
TRastuzumab And VInorelbine Or Taxane(TRAVIOTA)
Eligibility:1st line chemoHER2+RECIST
Multicentern=250
Endpoints:RR, TTPX-over RR, TTP
HER2 + MBCFirst-line Chemo & Trastumuzab
Trastuzumab &Vinorelbine
Trastuzumab &Weekly Taxane
(paclitaxel or docetaxel)
Progressive Disease Progressive Disease

Xeloda® plus Herceptin®: activity against BT474 breast cancer xenografts
Ouchi KF et al. Cancer Chemother Pharmacol (in press)
1,000
800
600
400
200
10020 25 30 35 40 45 50 55
***Tu
mo
ur
volu
me
(mm
3 )
ControlXelodaHerceptinXeloda + Herceptin
Days after inoculation
*p<0.05

Xeloda® plus Herceptin®:
the German
experience
• 18 patients with anthracycline and taxane-pretreated HER2+ MBC received 21-day cycle of
• standard-dose Herceptin, weekly
• Xeloda 1,125mg/m2 twice daily, days 1–14
• 47% ORR in 13 patients
• Median response duration of 10 months (range 7–18)
• Minimal side effectsBangemann N et al. Ann Oncol 2000; 11:143 (Abst 653P)
Gemzar + Herceptin3 + Overexpression
Population = HeavilyPretreated (64 Pts.)
R.R. = 45%
T.T.P (medium) = 5.8 mo.
San Antonio 2001 (Abst 523)

Coley (CpG 7909)(+) Herceptin
• Herceptin acts by modulating signaltransduction pathways and through ADCC
• CpG stimulates ADCC• In a mouse model
• CpG as active as Herceptin• Markedly synergistic
• Clin. Trial in Herceptin Resistant Pts.



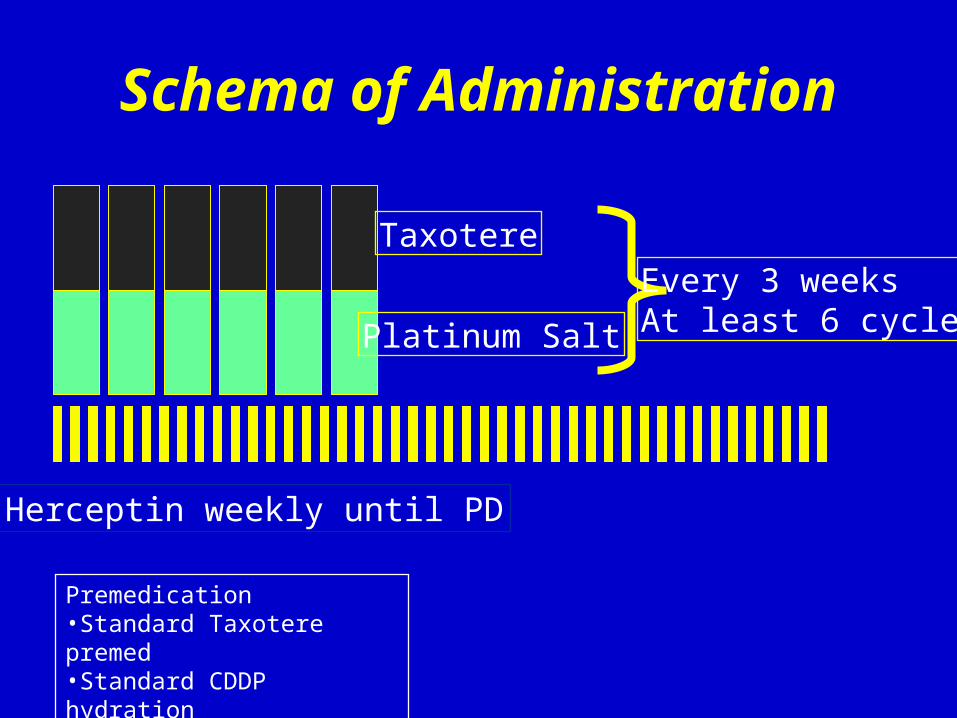
Schema of Administration
Taxotere
Platinum Salt
Every 3 weeks At least 6 cycles
Herceptin weekly until PD
Premedication•Standard Taxotere premed •Standard CDDP hydration

TCH - Response Rates First Line Patients
7/17 (41%) [19-67]
7/17 (41%) [19-67]
23/36 (64%)[46-79]
23/36 (64%)[46-79]
FISH negative**
FISH negative**
FISH positive**
FISH positive**OverallOverall
ORR95% CIORR95% CI
31/55 (56%) [40-69]
31/55 (56%) [40-69]
ORR95% CIORR95% CI
49/62 (79%)[66-88]
49/62 (79%)[66-88]
27/35 (77%)[59-90]
27/35 (77%)[59-90]
16/19 (84%)[60-96]
16/19 (84%)[60-96]
UCLAcarboUCLAcarbo
BCIRGcis
BCIRGcis
FISH Positive
FISH Negative
0 2 4 6 8 10 12 14 16 18 20Time to Disease Progression (months)
Number at Risk38 37 32 26 19 15 12 10 8 4 019 17 15 13 8 6 5 3 1 1 0
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n P
rog
ress
ion
Fre
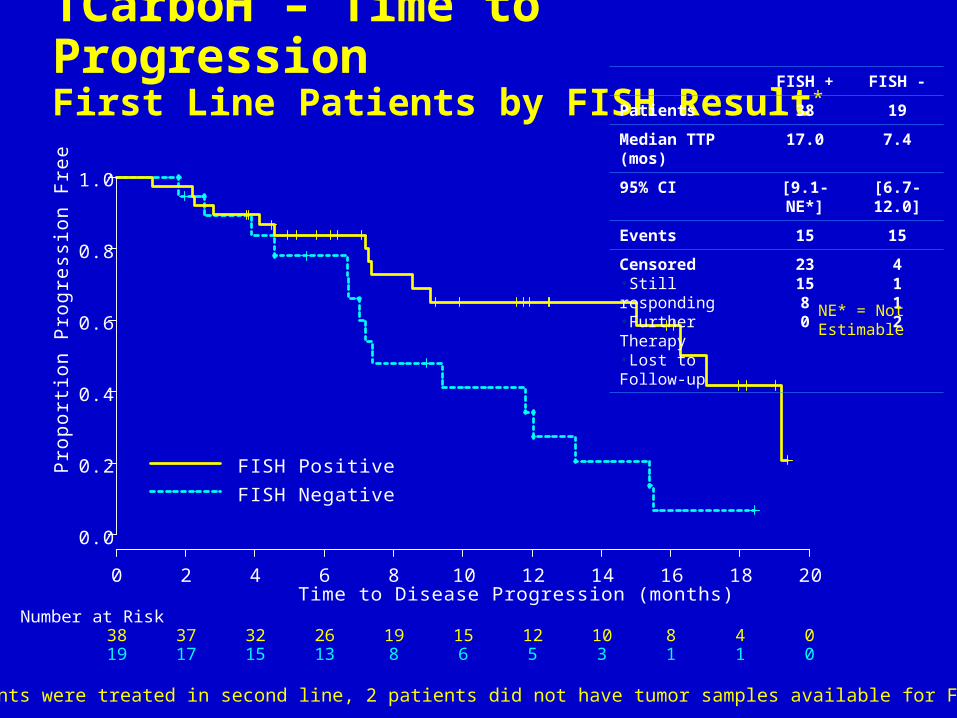
eTCarboH – Time to Progression First Line Patients by FISH Result* FISH + FISH -
Patients 38 19
Median TTP (mos) 17.0 7.4
95% CI [9.1-NE*] [6.7-12.0]
Events 15 15
Censored •Still responding•Further Therapy•Lost to Follow-up
231580
4112
NE* = Not Estimable
* 3 patients were treated in second line, 2 patients did not have tumor samples available for FISH testing


Dana - FarberPreoperative Trastuzumab &
Paclitaxel: Tumor Response Rates
No. cPR cCR pCR
Total 4017
43%12
30%7
18%
3+ 3216
50%11
34%6
19%
2+ 81
13%1
13%1
13%

SchemaSchema
Reevaluate Reevaluate
(Week 17)(Week 17)
Reevaluate Reevaluate
(Week 17)(Week 17)
ProgressionProgressionProgressionProgression
StableStableStableStable
Stop Herceptin Stop Herceptin Begin Pac / CarboBegin Pac / CarboStop Herceptin Stop Herceptin Begin Pac / CarboBegin Pac / Carbo
Continue Continue 8-week8-weekcourses courses until PD until PD or 12 or 12 monthsmonths
Continue Continue 8-week8-weekcourses courses until PD until PD or 12 or 12 monthsmonths
CR, PR, MRCR, PR, MRCR, PR, MRCR, PR, MR
Continue Weekly Continue Weekly Herceptin for 8 Herceptin for 8 addt’l weeks addt’l weeks (weeks 9-16)(weeks 9-16)
Continue Weekly Continue Weekly Herceptin for 8 Herceptin for 8 addt’l weeks addt’l weeks (weeks 9-16)(weeks 9-16)
Begin weeklyBegin weeklyHerceptin / Herceptin / Pac / Carbo ---Pac / Carbo ---Continue 8-wk Continue 8-wk courses until courses until progression or progression or total 12 mos. total 12 mos. treatmenttreatment
Begin weeklyBegin weeklyHerceptin / Herceptin / Pac / Carbo ---Pac / Carbo ---Continue 8-wk Continue 8-wk courses until courses until progression or progression or total 12 mos. total 12 mos. treatmenttreatment
HerceptinHerceptinWeeklyWeeklyx 8x 8
HerceptinHerceptinWeeklyWeeklyx 8x 8
ReevaluateReevaluateReevaluateReevaluate

Herceptin / Paclitaxel / Carboplatin
• Response to Herceptin induction (58 pts.)
¬ ORR 19%; SD or better 60%• Response to H / P / C (34 pts.)
¬ ORR 68%; SD or better 73%• Response to P/C (18 pts. with PD on Herceptin)
¬ ORR 50%
NeoadjuvantCisplat + Taxotere + Herceptin
U of Miami (16 Pts.)
PREHerceptin Std. Dose
T/C 70 mg/m2 each q 21 d
POSTAC x 4
Asco 2001 - Abst. 1871
100% RR25 % pCR
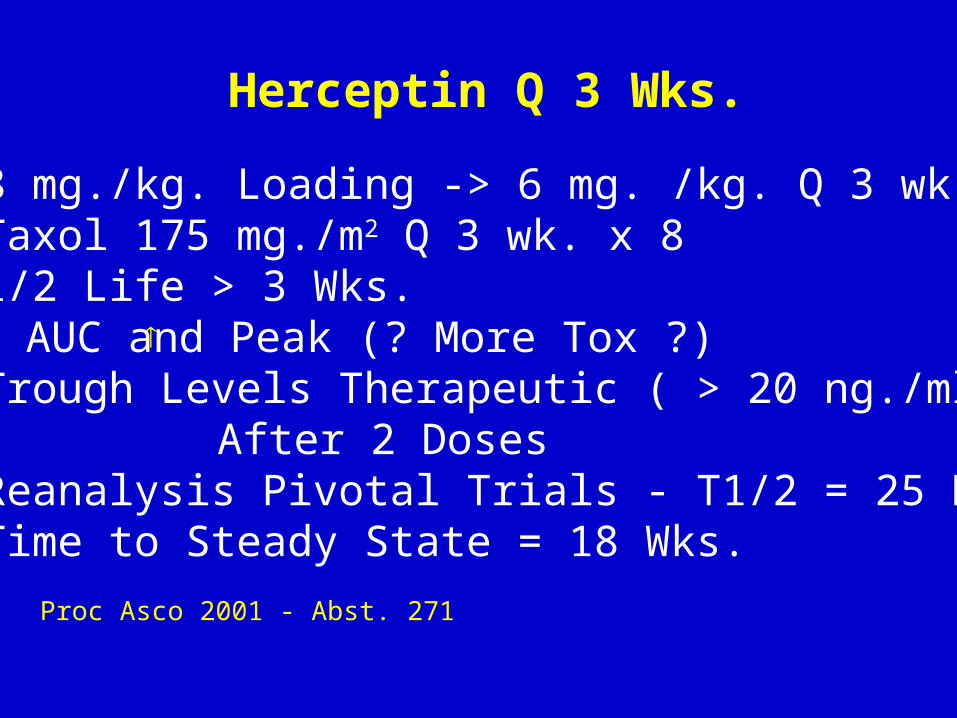
Herceptin Q 3 Wks.
• 8 mg./kg. Loading -> 6 mg. /kg. Q 3 wk. Taxol 175 mg./m2 Q 3 wk. x 8• 1/2 Life > 3 Wks.• AUC and Peak (? More Tox ?)• Trough Levels Therapeutic ( > 20 ng./ml )
After 2 Doses• Reanalysis Pivotal Trials - T1/2 = 25 Days Time to Steady State = 18 Wks.
Proc Asco 2001 - Abst. 271

Trough levels - weekly vs q3w
0
20
40
60
80
100
120
140
1 4 7 10 13 16 19 22 25 28 31 34
Week Number
Her
cep
tin
(u
g/m
L)
0
20
40
60
80
100
120
140
1 4 7 10 13 16 19 22 25 28 31 34
Week Number
Her
cep
tin
(u
g/m
L)
Weekly Administration Q-3 Weekly Administration

Summary• Herceptin administered q3w is safe with no
unexpected toxicity.• No interaction of Taxol and Herceptin
pharmacokinetics was observed.• Trough levels for q3w Herceptin were similar to
those seen with weekly dosing.• Peak and average serum concentrations were
higher than those seen with weekly Herceptin.• Half-life of Herceptin was 21 days.• This suggests that it could take approximately 18
weeks after discontinuing Herceptin to clear the drug from the body. Karen A. Gelmon, MD, FRCPC
Herceptin + Taxol q3w

Adjuvant HerceptinQ3 Wk 2001
HeraIntergroupBCIRG - Maintenance

Should Herceptin be continued in patients with disease progression on Herceptin?
Limited clinical data
Depends on mechanism of action of Herceptin- ? Alters sensitivity of breast cancer cells to
cytotoxic therapy- ? Interferes with anti-apoptotic pathways
Clinical anecdotes suggest some activity

Herceptin + VinorelbineStudy Design (MDACC)
Progressive disease after Herceptin + Taxane-based Therapy
(HER2 +)
Vinorelbine(Single Agent)
Vinorelbine +
Herceptin

(q3w x 4) (q3w x 4)
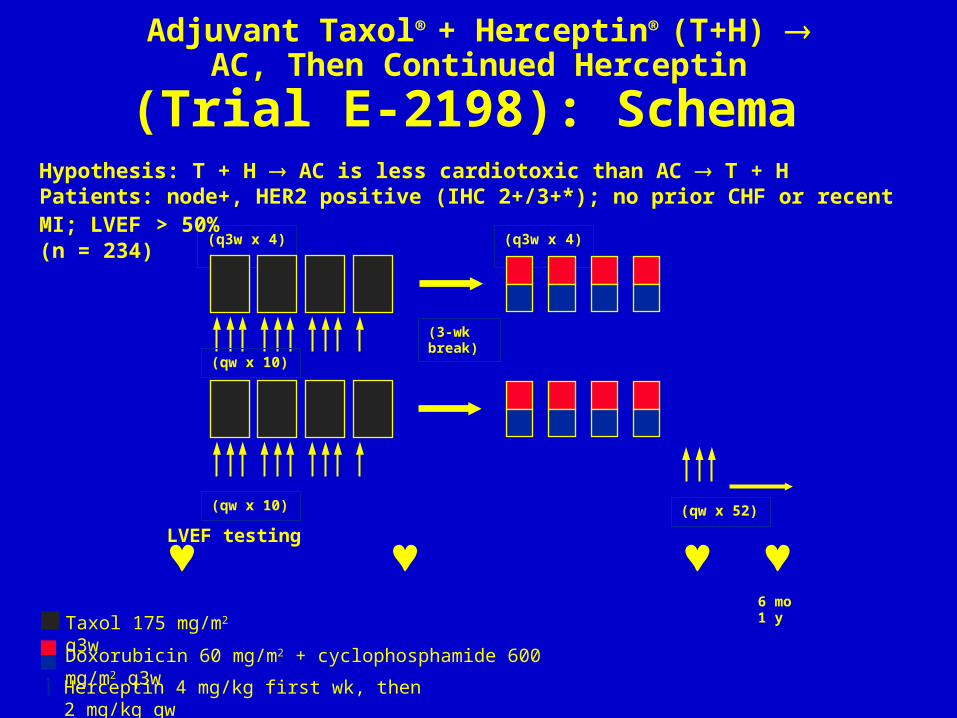
Adjuvant Taxol® + Herceptin® (T+H) AC, Then Continued Herceptin
(Trial E-2198): Schema Hypothesis: T + H AC is less cardiotoxic than AC T + H Patients: node+, HER2 positive (IHC 2+/3+*); no prior CHF or recent MI; LVEF > 50% (n = 234)
(qw x 10)
LVEF testing
Taxol 175 mg/m2 q3w
Herceptin 4 mg/kg first wk, then 2 mg/kg qw
Doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 q3w
(3-wkbreak)
(qw x 52)
6 mo1 y
(qw x 10)

Adjuvant Taxol + Herceptin (T + H) AC, Then Continued Herceptin
(E-2198): Cardiotoxicity • Primary end point: rate of clinical CHF• Secondary end point: > 10% absolute decrease
in LVEF from baseline Patients to go off Herceptin for LVEF drop of > 20%, LVEF drop below LLN, or CHF
• Results through immediate post-AC evaluation
CHF in 4 patients (< 2%), 3 post-AC
LVEF below LLN: 2.8% post-T + H, 6% post-AC
LVEF drop of > 10%: 9% post-T + H, 13.2% post-AC
Update of Sledge et al. Breast Cancer Res Treat. 2001;69:209. Abstract 4.

Adjuvant Therapy With Herceptin® in the NSABP B-31 Trial
Patient characteristics: node+, HER2 positive (IHC 3+* or FISH+†)
* HercepTestTM.† PathVysionTM or INFORM® (>5 copies/cell).
(q3w x 4)
Taxol® 175 mg/m2 q3wHerceptin 4 mg/kg first wk, then 2 mg/kg qw
Doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 q3w
Adjuvant tamoxifen for ER+ or PR+ patients.
Romond. Protocol NSABP-B-31.
Activation: March 2000
(n = 2700)
(q3w x 4)
(qw x 52)

(n = 3000)
(qw x 52)
Adjuvant Therapy With Herceptin® in the Intergroup Trial (N9831):
Schema• Patient characteristics: node+, HER2 IHC 3+ or FISH+ (> 5 copies/cell)
(q3w x 4)
(qw x 12)
(qw x 52)
Taxol® 80 mg/m2 qwHerceptin 4 mg/kg first wk, then 2 mg/kg qw
Doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 q3w
Radiotherapy for all pts 5 wks after Taxol, with tamoxifen for all ER+ pts at initiation of therapy.
Perez. Protocol NCCTG-N9831.Horton. Cancer Control. 2001;8:103.

(n = 3150)
Node+/High Risk
Node–/FISH+
Adjuvant Therapy With Herceptin®: Breast Cancer International Research
Group Trial (BCIRG 006)
(q3w x 4) (q3w x 4)
(qw x 12) (q3w x 14)(q3w x 6)
(q3w x 12)(qw x 18)
Herceptin 4 mg/kg first wk, then 2 mg/kg qw Herceptin 6 mg/kg q3w
Taxotere® 100 mg/m2 q3w
A 60 mg/m2 + C 600 mg/m2 q3w
Carboplatin AUC 6 + Taxotere 75 mg/m2 q3w

Randomize
Primary Management (chemotherapy, local or locoregional radiation)
Stratify
Surgery
Herceptin® q3w x 12 mo
N=1100
Herceptin q3w x 24 mo
N=1100
ObservationN=1100
HER2 Adjuvant (HERA) Trial: Schema
Patients HER2 IHC 3+/FISH+
Courtesy of Clifford Hudis.

Number of Patients in Adjuvant Herceptin Trials
Accrual(~June ’02)
Target
NSABP 720 (27%) 2700
Intergroup 781 (26%) 3000
BCIRG 006 679 (22%) 3150
HERA 50 (2%) 3300
Total 2230 (18%) 12150
