anti emesis
DESCRIPTION
muTRANSCRIPT
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 1/31
Antiemesis
Continue
NCCN Clinical Practice Guidelines in Oncology™
Antiemesis
V.2.2008
www.nccn.org

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 2/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008
NCCN®
NCCN Antiemesis Panel Members
Steve Kirkegaard, PharmDHuntsman Cancer Institute at the Universityof Utah
Mark G. Kris, MD †Memorial Sloan-Kettering Cancer Center
Dean Lim, MD †City of Hope
Michael Anne Markiewicz, PharmDUniversity of Alabama at BirminghamComprehensive Cancer Center
Lida Nabati, MD £ ÞDana-Farber/Brigham and Women's Cancer Center | Massachusetts General HospitalCancer Center
Dwight D. Kloth, PharmD, FCCP, BCOPFox Chase Cancer Center
Carli Nesheiwat, PharmD, BCOPSt. Jude Children's ResearchHospital/University of TennesseeCancer Institute
Hope S. Rugo, MD † ‡UCSF Helen Diller Family
Comprehensive Cancer Center
Steven M. Sorscher, MD †
Barbara Todaro, PharmDRoswell Park Cancer Institute
Susan Urba, MD † £University of MichiganComprehensive Cancer Center
Siteman Cancer Center at Barnes-Jewish Hospital and WashingtonUniversity School of Medicine
‡
Þ
†
#
£
*
Hematology/hematology oncology
Internal medicine
Medical Oncology
Nurse
Pharmacology
Supportive Care including Palliative, Pain management,Pastoral care and Oncology social work
Writing Committee member
*David S. Ettinger, MD/Chair †
The Sidney Kimmel Comprehensive
Cancer Center at Johns Hopkins
Duke Comprehensive Cancer Center
Michael J. Berger, PharmD, BCOPArthur G. James & Richard J. Solove
Research Institute at The Ohio State
University
Sally Barbour, PharmD, BCOP † ‡
Philip J. Bierman, MD † ‡
UNMC Eppley Cancer Center at The
Nebraska Medical Center
Bob Bradbury, BCPSH. Lee Moffitt Cancer Center & ResearchInstitute at the University of South Florida
Georgianna Ellis, MD †Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance
*
*
Continue

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 3/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008
NCCN®
Table of Contents
CHEMOTHERAPY INDUCED:
RADIATION-INDUCED:
ANTICIPATORY:
NCCN Antiemesis Panel Members
High Emetic Risk Chemotherapy - Emesis Prevention (AE-2)
Moderate Emetic Risk Chemotherapy - Emesis Prevention (AE-3)Low and Minimal Emetic Risk Chemotherapy - Emesis Prevention (AE-4)
Breakthrough Treatment for Chemotherapy Induced Nausea and Vomiting (AE-5)
Emetogenic Potential of Antineoplastic Agents (AE-6)
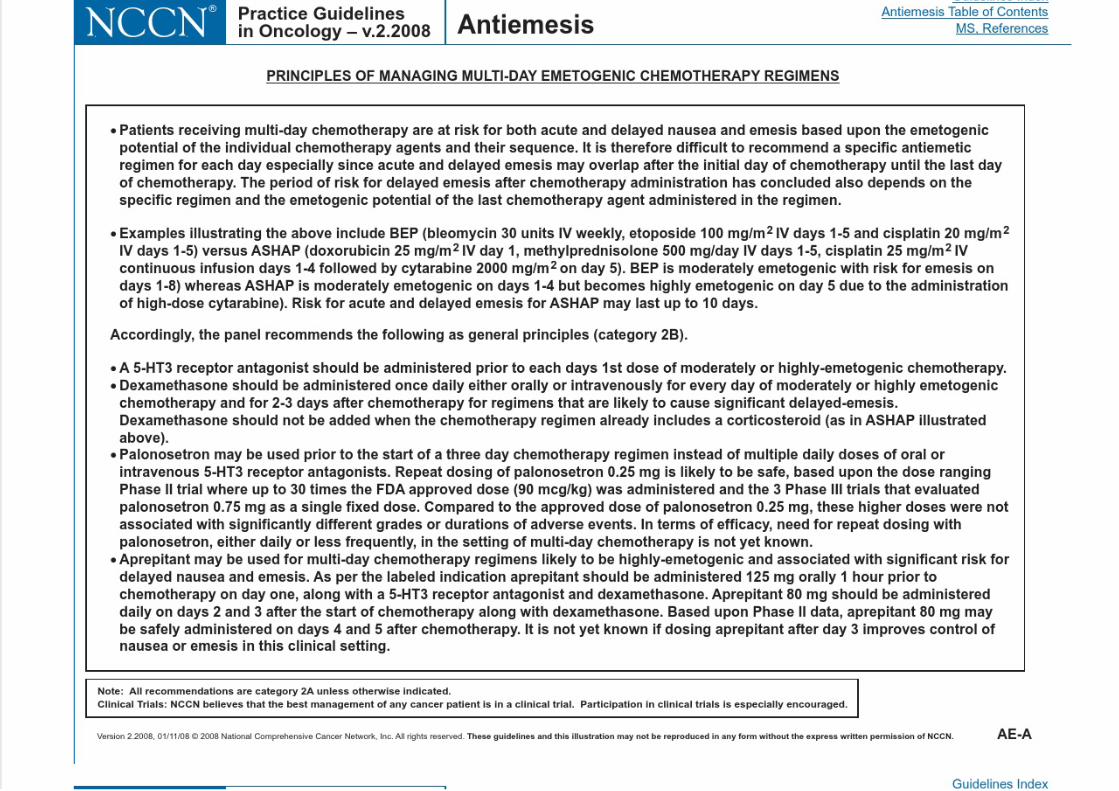
Principles of Managing Multi-Day Emetogenic Chemotherapy Regimens (AE-A)
Principles For Managing Breakthrough Emesis (AE-B)
Radiation-induced nausea and vomiting (AE-8)
Anticipatory nausea and vomiting (AE-9)
Summary Of Guidelines Updates
Priniciples Of Emesis Control (AE-1)
Guidelines IndexPrint the Antiemesis Guideline
Order the Patient Version of the Antiemesis Guideline
These guidelines are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult these guidelines is expected to use independent medical judgment in the context of individual clinicalcircumstances to determine any patient's care or treatment. The National Comprehensive Cancer Network makes no representations nor warrantiesof any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. Theseguidelines are copyrighted by National Comprehensive Cancer Network. All rights reserved. These guidelines and the illustrations herein may notbe reproduced in any form without the express written permission of NCCN. ©2008.
For help using thesedocuments, please click here
Manuscript
References
Clinical Trials:
Categories of Evidence andConsensus:NCCN
Thebelieves that the best managementfor any cancer patient is in a clinicaltrial. Participation in clinical trials isespecially encouraged.
To find clinical trials online at NCCNmember institutions,
All recommendationsare Category 2A unless otherwisespecified.
See
NCCN
click here:nccn.org/clinical_trials/physician.html
NCCN Categories of Evidence
and Consensus

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 4/31Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
SUMMARY OF GUIDELINES UPDATES
Change in the 2.2008 version of the NCCN Antiemesis Guidelines from the 1.2008 version is the addition of the 2008 manuscript.
Deleted recommendation prochlorperazine for 15 mg Spansule PO every 8 or every 12 h throughout the guidelines.
Added Vorinostat to the list of agents with low emetic risk.
Added Cetuximab, Lapatinib, Panitumumab, and Temsirolimus to the list of agents with minimal emetic risk.
The general principle of breakthrough treatment is to give an additional agent from a different drug class. Added the following
statement: No one treatment is better than the other for managing breakthrough emesis.
Multiple concurrent agents, perhaps in alternating schedules or by alternating routes, may be necessary. Added the following
statement: Dopamine antagonists (eg, metoclopramide), haloperidol, corticosteroids and agents such as lorazepam may be required.
Summary of changes in the 1.2008 version of the NCCN Antiemesis Guidelines from the 1.2007 version include:
Added footnote g: "Monitor for dystonic reactions; use diphenhydramine for dystonic reactions."
General
AE-4
AE-7
AE-B Principles for Managing Breakthrough Emesis
UPDATES
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 5/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
PRINCIPLES OF EMESIS CONTROL IN THE CANCER PATIENT
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
AE-1
Prevention of nausea/vomiting is the goal.
The risk of emesis and nausea for persons receiving chemotherapy of high
and moderate emetic risk lasts for at least 4 days. Patients need to be
protected throughout the full period of risk.
Oral and IV antiemetic formulations have equivalent efficacy.
Consider the toxicity of the specific antiemetic(s) .Choice of antiemetic(s) used should be based on the emetic risk of the
therapy, prior experience with antiemetics, as well as patient factors.
There are other potential causes of emesis in cancer patients.
These may include:Partial or complete bowel obstruction Vestibular dysfunctionBrain metastases
Electrolyte imbalance: hypercalcemia, hyperglycemia, hyponatremiaUremiaConcomitant drug treatments including opiatesGastroparesis, tumor or chemotherapy (vincristine etc) induced.Psychophysiologic:
AnxietyAnticipatory nausea and vomiting
For use of antiemetics for nausea and vomiting that is not related to
radiation and/or chemotherapy, See NCCN Palliative Care Guidelines

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 6/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
AE-2
HIGH EMETIC RISK CHEMOTHERAPY - EMESIS PREVENTION b,c
Higha
Start before chemotherapyAprepitant 125 mg PO day 1, 80 mg PO daily days 2-3
andDexamethasone 12 mg PO or IV day 1, 8 mg PO or IV daily days 2-4
and
± Lorazepam 0.5-2 mg PO or IV or sublingual either every 4 or every 6 h days 1-4
b,c
5-HT3 antagonist:
Ondansetron 16-24 mg PO or 8-12 mg (maximum 32 mg) IV day 1
or
Granisetron 2 mg PO or 1 mg PO bid or 0.01 mg/kg (maximum 1 mg) IV day 1
or
Dolasetron 100 mg PO or 1.8 mg/kg IV or 100 mg IV day 1or
Palonosetron 0.25 mg IV day 1
and
d
a
d
Data for post-cisplatin ( 50 mg/m ) emesis prevention are category 1, others are category 2A.
Order of listed antiemetics does not reflect preference.
2
b Antiemetic regimens should be chosen based on emetogenic potential of the chemotherapy regimen as well as patient specific risk factors.cSee Principles for Managing Multi-day Emetogenic Chemotherapy Regimens (AE-A).
See Principles of Emesis Control (AE-1)
(category 1, for combined regimen)
SeeBreakthroughTreatment(AE-5)

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 7/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
MODERATE EMETIC RISK CHEMOTHERAPY - EMESIS PREVENTION b,c
Day 1 Days 2-3
Moderate e
Aprepitant 80 mg PO days 2-3 if used on Day 1Dexamethasone 8 mg PO or IV daily
or
Dexamethasone 8 mg PO or IV daily or 4 mg POor IV bidor 5-HT3 antagonist:
±
e
Ondansetron 8 mg PO bid or 16 mg PO daily or
8 mg (maximum 32 mg/day) IV
or
Granisetron 1-2 mg PO daily or 1 mg PO bid or
0.01 mg/kg (maximum 1 mg) IV
or
Dolasetron 100 mg PO daily or 1.8 mg/kg IV or ± Lorazepam 0.5-2 mg PO or IV or sublingual
either every 4 or every 6 h
Start before chemotherapyAprepitant 125 mg PO in select patientsDexamethasone 12 mg PO or IV
and
5-HT3 antagonist:Palonosetron 0.25 mg IV (category 1)
or
Ondansetron 16-24 mg PO or 8-12 mg
(maximum 32 mg/day) IV (category 1)
or
± Lorazepam 0.5-2 mg PO or IV or sublingual
either every 4 or every 6 h
b,c
f
d
Granisetron 1-2 mg PO or 1 mg PO bid
(category 1) or 0.01 mg/kg (maximum 1 mg) IV
or Dolasetron 100 mg PO or 1.8 mg/kg or
100 mg IV (category 1)
and
e 2 2
2
f
Data for post-carboplatin 300 mg/m , cyclophosphamide 600-1000 mg/m ,
doxorubicin 50 mg/m emesis prevention are category 1.
Aprepitant should be added (to dexamethasone and a 5-HT3 antagonist regimen)for patients receiving the combination of an anthracycline and cyclophosphamideand select patients receiving other chemotherapies of moderate emetic risk (for example, carboplatin, cisplatin, doxorubicin, epirubicin, ifosfamide, irinotecan or
methotrexate).
AE-3
b Antiemetic regimens should be chosen based on emetogenic potential of thechemotherapy regimen as well as patient specific risk factors.
Order of listed antiemetics does not reflect preference.
c
dSee Principles for Managing Multi-day Emetogenic Chemotherapy Regimens (AE-A).
SeeBreakthroughTreatment(AE-5)

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 8/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Low
Minimal
Start before chemotherapy
Dexamethasone 12 mg PO or IV daily
or
b,c
Repeat daily for fractionated doses of chemotherapy
Prochlorperazine 10 mg PO or IV every 4 or every 6 h
or Metoclopramide 10-40 mg PO or IV either every 4 or every 6 h
± Diphenhydramine 25-50 mg PO or IV either every 4 or every 6 h± Lorazepam, 0.5-2 mg PO or IV either every 4 or every 6 h
g
Nausea/emesis
(0–24 h)
Consider using antiemetics listed under primaryprophylaxis as treatment for low emetogenic-potential drugs
AE-4
LOW AND MINIMAL EMETIC RISK CHEMOTHERAPY - EMESIS PREVENTION b,c
b
c Antiemetic regimens should be chosen based on emetogenic potential of the chemotherapy regimen as well as patient specific risk factors.
Monitor for dystonic reactions; use diphenhydramine for dystonic reactions.
gSee Principles for Managing Multi-day Emetogenic Chemotherapy Regimens (AE-A).
See Principles of Emesis Control (AE-1)
No routine
prophylaxis
Breakthrough Treatment For Chemotherapy InducedNausea/vomiting (AE-5)

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 9/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
No nausea/
emesis
Any nausea/
emesis
No change in antiemetic regimen
General principle of breakthrough treatment is to give an
additional agent from a different drug class prnProchlorperazine 25 mg supp pr every 12 h or 10 mg PO or IV
every 4 or every 6 h
or Metoclopramide 10-40 mg PO or IV either every 4 or every 6 h
± Diphenhydramine 25-50 mg PO or IV either every 4 or every
6 h
or Lorazepam 0.5-2 mg PO either every 4 or every 6 h
or
Ondansetron 16 mg PO or 8 mg IV daily
or Granisetron 1-2 mg PO daily or 1 mg PO bid or 0.01 mg/kg
(maximum 1 mg) IV
or
Dolasetron 100 mg PO daily or 1.8 mg/kg IV or 100 mg IVor Haloperidol 1-2 mg PO every 4-6 h prn
or Dronabinol 5-10 mg PO either every 3 or every 6 h
or Nabilone 1-2 mg PO bid
or
Dexamethasone 12 mg PO or IV daily, if not previously givenor Olanzapine 2.5-5 mg PO bid (category 2B)
or Promethazine 12.5-25 mg PO or IV every 4 h
i
Continue breakthroughmedications, on aschedule, not prn
Consider changingantiemetic therapy tohigher-level primarytreatment
SUBSEQUENTCYCLES
RESPONSE TOBREAKTHROUGHANTIEMETIC TREATMENT
AE-5
See Principles of Emesis Control (AE-1)
BREAKTHROUGH TREATMENT FOR CHEMOTHERAPY INDUCED NAUSEA/VOMITINGc,h
Nausea andemesis controlled
Nausea and/or emesis uncontrolled
c
gMonitor for dystonic reactions; use diphenhydramine for dystonic reactions.h
i
See blackbox warning/label indication regarding type II diabetes and hyperglycemia.
See Principles for Managing Multi-day Emetogenic Chemotherapy Regimens (AE-A).
See Principles of Managing Breakthrough Treatment (AE-B).

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 10/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
EMETOGENIC POTENTIAL OF ANTINEOPLASTIC AGENTS
AC combination defined as either doxorubicin
or epirubicin with cyclophosphamide
Altretamine
Cyclophosphamide > 1,500 mg/m
Carmustine > 250 mg/m
Cisplatin 50 mg/m
2
2
2
AGENTLEVEL
j
kProportion of patients who experience emesis in the absence of effective antiemetic prophylaxis
Daily use of antiemetics is not recommended based on clinical experience.
Low emetic risk,level 2 (See AE-7)
Minimal emetic risk,
level 1 (See AE-7)
AE-6
Adapted with permission from:Hesketh PJ, et al. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J. Clin Onc 15: 103-9, 1997.Grunberg SM, Osoba D, Hesketh PJ, et al. Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity---an update. Support Care Cancer 2005;13:80-84.
Epub 2004 Dec 14.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
High emetic risk(> 90 % frequency of emesis) j
Moderate emetic risk
(30- 90 % frequency of emesis j
Dacarbazine
Mechlorethamine
Procarbazine (oral)
Streptozocin
Aldesleukin > 12-15 million units/mAmifostine > 300 mg/m
Arsenic trioxide
Azacitidine
Busulfan > 4 mg/d
Carboplatin
Carmustine 250 mg/m
Cisplatin < 50 mg/m
Cyclophosphamide 1,500 mg/mCyclophosphamide (oral)
Cytarabine > 1 g/m
Dactinomycin
Daunorubicin
Doxorubicin
2
2
2
2
2
2
EpirubicinEtoposide (oral)
Idarubicin
Ifosfamide
Imatinib (oral)
Irinotecan
Lomustine
Melphalan > 50 mg/m
Methotrexate 250 - > 1,000 mg/mOxaliplatin > 75 mg/m
Temozolomide (oral)
Vinorelbine (oral)
k
2
22
G id li I d

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 11/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
AE-7
EMETOGENIC POTENTIAL OF ANTINEOPLASTIC AGENTS
AGENTLEVEL
Low emetic risk(10-30 % frequency of emesis) j
Amifostine 300 mgBexarotene
Capecitabine
Cytarabine (low dose) 100-200 mg/m
Docetaxel
Doxorubicin (liposomal)
Etoposide
Fludarabine (oral)
5-Fluorouracil
2
GemcitabineMethotrexate > 50 mg/m < 250 mg/m
Mitomycin
Mitoxantrone
Paclitaxel
Paclitaxel-albumin
Pemetrexed
Topotecan
Vorinostat
2 2
Minimal emetic risk(< 10 % frequency of emesis) j
Lapatinib
Lenalidomide
Melphalan (oral low-dose)
Methotrexate 50 mg/m
Nelarabine
Panitumumab
Pentostatin
RituximabSorafenib
Sunitinib
Temsirolimus
Thalidomide
Thioguanine (oral)
Trastuzumab
Valrubicin
Vinblastine Vincristine
Vinorelbine
2
Alemtuzumab
Alpha Interferon
Asparaginase
Bevacizumab
Bleomycin
Bortezomib
Busulfan
CetuximabChlorambucil (oral)
Cladribine (2-chlorodeoxyadenosine)
Decitabine
Denileukin diftitox
Dasatinib
Dexrazoxane
Erlotinib
FludarabineGefitinib
Gemtuzumab ozogamicin
Hydroxyurea (oral)
jProportion of patients who experience emesis in the absence of effective antiemetic prophylaxis
Adapted with permission from:Hesketh PJ, et al. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J. Clin Onc 15: 103-9, 1997.Grunberg SM, Osoba D, Hesketh PJ, et al. Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity---an update. Support Care Cancer 2005;13:80-84.
Epub 2004 Dec 14.
Guidelines Index
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 12/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
EMETOGENIC
POTENTIAL
TYPE OF RADIATION
THERAPYEMESIS PREVENTION BREAKTHROUGH TREATMENT
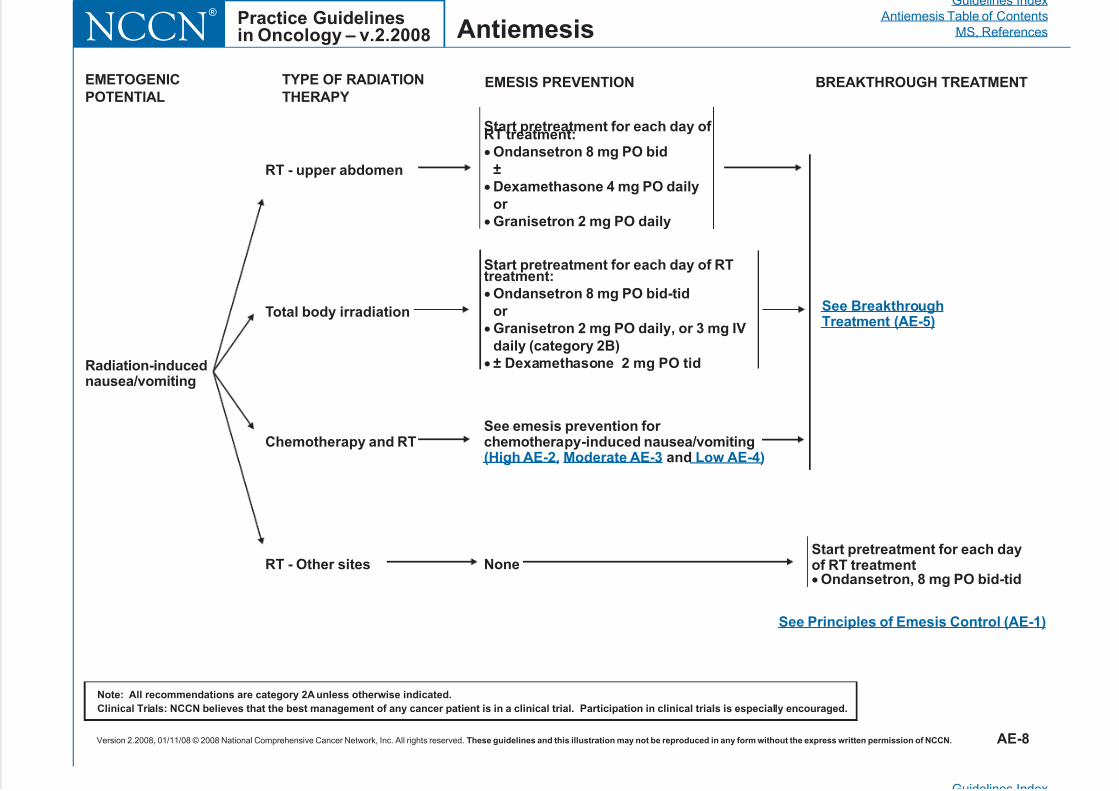
Radiation-inducednausea/vomiting
RT - upper abdomen
RT - Other sites
Chemotherapy and RT
Total body irradiation
None
Start pretreatment for each day of RT treatment:
Dexamethasone 4 mg PO daily
or
Granisetron 2 mg PO daily
Ondansetron 8 mg PO bid
±
Start pretreatment for each day of RTtreatment:
Granisetron 2 mg PO daily, or 3 mg IV
daily (category 2B)
± Dexamethasone 2 mg PO tid
Ondansetron 8 mg PO bid-tid
or See BreakthroughTreatment (AE-5)
Start pretreatment for each dayof RT treatment
Ondansetron, 8 mg PO bid-tid
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
AE-8
See Principles of Emesis Control (AE-1)
See emesis prevention for chemotherapy-induced nausea/vomiting
and(High AE-2, Moderate AE-3 Low AE-4)
Guidelines Index
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 13/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesAntiemesisPractice Guidelinesin Oncology – v.2.2008NCCN
®
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
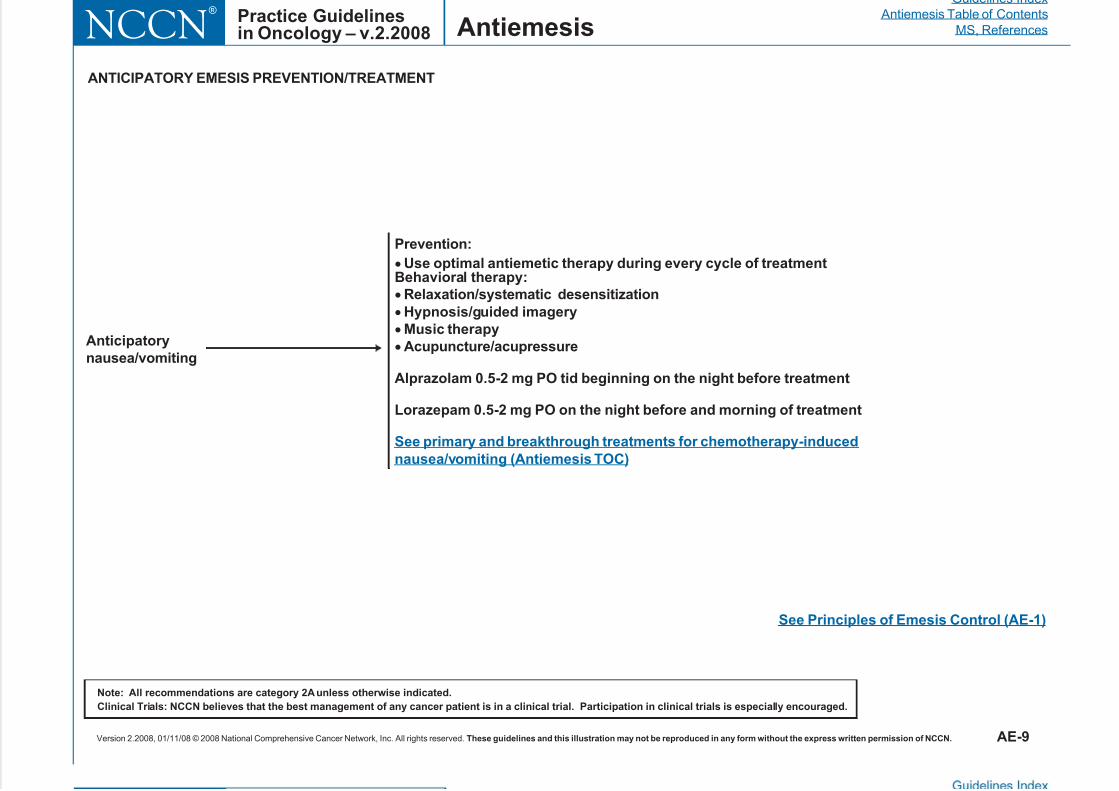
ANTICIPATORY EMESIS PREVENTION/TREATMENT
Anticipatory
nausea/vomiting
Prevention:
Behavioral therapy:
Hypnosis/guided imagery
Music therapy
Acupuncture/acupressure
Alprazolam 0.5-2 mg PO tid beginning on the night before treatment
Lorazepam 0.5-2 mg PO on the night before and morning of treatment
Use optimal antiemetic therapy during every cycle of treatment
Relaxation/systematic desensitization
See primary and breakthrough treatments for chemotherapy-induced
nausea/vomiting (Antiemesis TOC)
AE-9
See Principles of Emesis Control (AE-1)
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 14/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 15/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 16/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 17/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 18/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 19/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 20/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 21/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 22/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 23/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 24/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 25/31
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 26/31
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 27/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 28/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 29/31

7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 30/31
Antiemesis
Guidelines Index
Antiemesis Table of Contents
MS, ReferencesPractice Guidelinesin Oncology – v 2 2008NCCN
®
7/21/2019 Anti Emesis
http://slidepdf.com/reader/full/anti-emesis-56dbd01d899d7 31/31
Version 2.2008, 01/11/08 © 2008 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this i llustration may not be reproduced in any form w ithout the express writt en permission of NCCN. REF-7
Antiemesis ,in Oncology – v.2.2008 NCCN
108. Redd WH, Andrykowski MA. Behavioral intervention in cancertreatment: Controlling aversion reactions to chemotherapy. J ConsultClin Psychol 1982;50:1018-1029.
109. Razavi D, Delvaux N, Farvacques C, et al. Prevention ofadjustment disorders and anticipatory nausea secondary to adjuvantchemotherapy: A double-blind, placebo-controlled study of assessingthe usefulness of alprazolam. J Clin Oncol 1993;11:1384-1390.