anti-coagulants principles and practice gary greenberg, md, mph open door clinic urban ministries of...
TRANSCRIPT

Anti-coagulantsAnti-coagulantsPrinciples and practicePrinciples and practice
Gary Greenberg, MD, MPHOpen Door Clinic
Urban Ministries of Wake Co. NC Assoc. Free Clinics
May, 2011
1
Disclaimer / AlertsDisclaimer / Alerts
• I’m an internist at Urban Ministries Wake Co, and once-upon-a-time, a faculty practitioner at Duke Med. Ctr. x 18 years
• Only I am responsible for recommendations, and your mileage may vary
• Topics do include off-label and non-guideline-based care.
• Talk stresses new ideas, so potential truth-flux• I have no conflicts of interest to disclose.
2

Aims & LimitationsAims & Limitations
• Mechanisms (briefly)• Clinical, evidence-based, logistical, tactical• Website: tinyurl.com/AntiCoag or
www.OpenDoorDocs.org/AntiCoag.htmlDocumentsReferencesCalculatorsTools
3

Platelet Activation BlockersPlatelet Activation Blockers
• Clinical use is for arterial effects, preventing “white” emboli, arising across rapid flow
• Stroke prevention, not venous thrombosis prevention (or treatment)
• Effect can be irreversible for the individual platelet (aspirin) or dose-related (others)
4
Platelet Activation BlockersPlatelet Activation Blockers
Useful / Common• Aspirin
High (325 mg) v low (81 mg) dose
• Clopidogril (Plavix®)• Ticlopidine (Ticlid®)• Prasugrel (Effient®)• Cilostazol (Pletal®)• Aggrenox® (combines aspirin
with dipyridamole)
Narrow use, show-off list• Tirofiban (Aggrastat®)• Dipyridamole (Persantine®)• Anagrelide (Agrylin®)• Eptifibatide (Integrilin®, IV
only)
5

Uses for platelet aggregation Uses for platelet aggregation antagonistsantagonists
• CNS / embolic protection Threatened stroke / TIA Post-stroke secondary prevention Atrial fibrillation
• Coronary, direct thrombosis protection Interrupt an MI Post MI Post coronary re-vascularization (esp. stent placement) High vascular risk status (DM+ or P.A.D.) Primary prevention
6

PharmacologyPharmacologyDrug Class Evidence-
based UsesComment Interactions
Aspirin Cyclo-oxygenase inhibitor (COX-I)
Native CADStent protectionCVAPAD
Permanently acetylates cyclooxygenase prostaglandin synthetase
Action blocked by non-acetylated salicylates (maybe Pepto), maybe ibuprofen, but not naproxen
Plavix® Clopidogril
ADP receptor P2Y12 inhibitor
Stent protectionCVAPAD (for CAD/CVA risk)
Metabolic activation blocked by proton-pump inhibitors (except pantoprazole = Protonix)No effect in aggregated clinical trials
Ticlid® Ticlopidine
ADP receptor P2Y12 inhibitor
Stent protection First platelet agent to show effectiveness in women
Prasugrel Effient®
ADP receptor P2Y12 inhibitor
Stent protection No interaction with PPI’s
Dipyridamole (in Aggrenox® and Persantine®)
Thromboxane inhibitor
CVAPAD (direct effect)
Also vasodilator, used for ‘stress’ coronary testing
7

AspirinAspirin
• Cheap, well accepted• “Children’s aspirin” 81 is never for children!
Aspirinita • Duration of effect is life of platelet• Direct gastric irritant may make it riskier• Relative efficacy/ safety for 325 v 81 is unclear,
maybe even paradoxical• Ibuprofen, other salicylates may block effect
8

Plavix® ClopidogrilPlavix® Clopidogril• 75 mg daily = $170 / month• Required for stents, especially drug-eluting stents, for at least
a year• Demonstrable reduction in CVA & MI for patients with PAD (as
seen on TV)• Altered activation with co-administration of • No generic (now). But: both previous & soon (November,
2011) • Pt-Assistance requires Social Security Number (but Bristol-
Myers Squibb/Sanofi website says only: “Must live in the U.S.”
9

Ticlopidine (used to be Ticlid®)Ticlopidine (used to be Ticlid®)
• 250 mg BID = $80 / month• Earliest aspirin replacement, now only generic• Proven efficacy for stent protection• In addition to TTP & hemorrhage
Bone marrow effects include aplastic anemia Requires q 2 week CBC monitoring for prompt
discontinuation, for at least 3 months Needs informed consent regarding unique risks and
additional lab responsibilities
10

Effient® PrasugrelEffient® Prasugrel
• 10 mg daily = $187 / mo• New competitor to Plavix®• Equally effective for stent protection• Patient Assistance Program seems not to require SSN
(“must be a US resident”)• No evidence for CAD or CVA prophylaxis in PAD pts• May be sampling, since a new agent• No salicylate or ibuprofen or PPI interactions
11

Aggrenox®Aggrenox®
• Combination capsule: i BID = $200 / mo Aspirin 25 mg, Dipyridamole 200 mg,
• Demonstrably effective CVA prevention (esp. used for patients who stroked while on ASA)
• Pkg: “not interchangeable” with separate ingredients Combination is brand-name only Generic dipyridamole comes in 75 mg tab, so
“replacement” is iii BID, #180/mo = $155
12

PharmacologyPharmacologyDrug Class Evidence-
based UsesComment Interactions
Aspirin Cyclo-oxygenase inhibitor (COX-I)
Native CADStent protectionCVAPAD
Permanently acetylates cyclooxygenase prostaglandin synthetase
Action blocked by non-acetylated salicylates (maybe Pepto), maybe ibuprofen, but not naproxen
Plavix® Clopidogril
ADP receptor P2Y12 inhibitor
Stent protectionCVAPAD (for CAD/CVA risk)
Metabolic activation blocked by proton-pump inhibitors (except pantoprazole = Protonix)No effect in aggregated clinical trials
Ticlid® Ticlopidine
ADP receptor P2Y12 inhibitor
Stent protection First platelet agent to show effectiveness in women
Prasugrel Effient®
ADP receptor P2Y12 inhibitor
Stent protection No interaction with PPI’s
Dipyridamole (in Aggrenox® and Persantine®)
Thromboxane inhibitor
CVAPAD (direct effect)
Also vasodilator, used for ‘stress’ coronary testing
13

Atrial FibrillationAtrial Fibrillation
• Effects Embolic stroke is main risk Congestive failure (“10%” of cardiac output) Syncope Palpitations
• Treatment to rate or correction of rhythm seems nearly equally effective (or ineffective)
• Intermittent is not necessarily safer than continuous
14

Anticoagulation DecisionAnticoagulation Decision
CHADS-2
Risk for embolic event, if no treatment:1-2: aspirin, 3+ consider ‘full’ anticoagulation
15
Criterion Score
History of Congestive Heart Failure 1
History of Hypertension 1
Age over 75 y/o 1
History of Diabetes 1
Stroke or TIA history 2
Total
Chest. 2008 Jun;133(6 Suppl):546S-592S. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition).
http://www.vhpharmsci.com/sparc/
Score Risk / year
1 2.8%
2 4.0%
3 5.9%
4 8.5%
5 12.5
6 18.2%
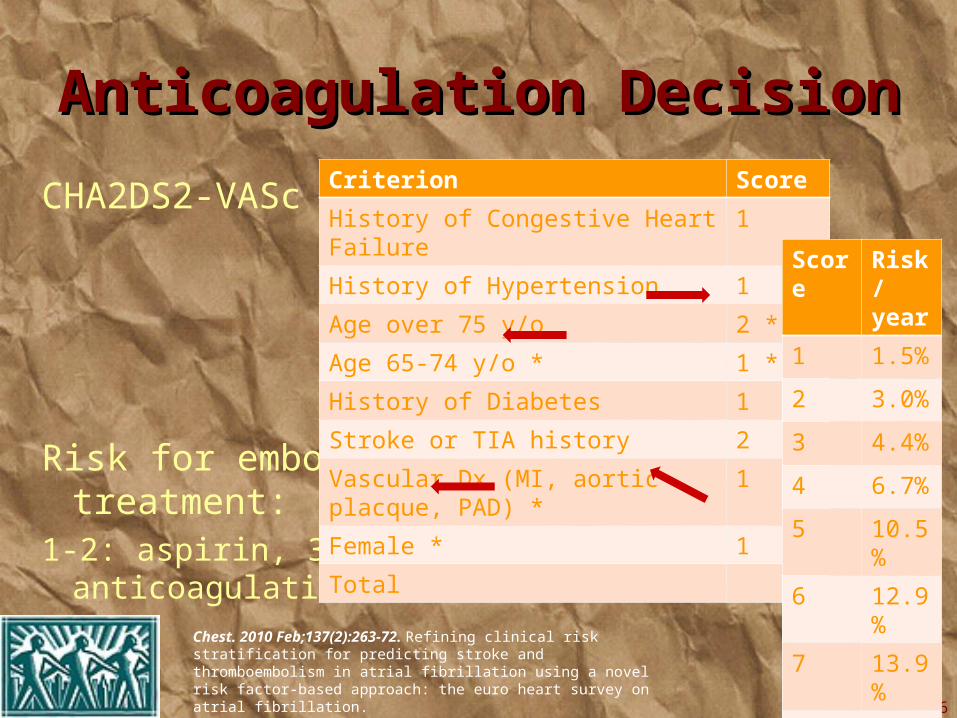
Anticoagulation DecisionAnticoagulation Decision
CHA2DS2-VASc
Risk for embolic event, if no treatment:1-2: aspirin, 3+ consider ‘full’ anticoagulation
16
Criterion Score
History of Congestive Heart Failure 1
History of Hypertension 1
Age over 75 y/o 2 *
Age 65-74 y/o * 1 *
History of Diabetes 1
Stroke or TIA history 2
Vascular Dx (MI, aortic placque, PAD) * 1
Female * 1
Total
Chest. 2010 Feb;137(2):263-72. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation.
http://www.vhpharmsci.com/sparc/
Score Risk / year
1 1.5%
2 3.0%
3 4.4%
4 6.7%
5 10.5%
6 12.9%
7 13.9%
8 14.1%
9 16.1%

Warfarin IssuesWarfarin Issues• Myths about “thinning”, so I say “clot-blocking”
Tired, cold-sensitive, pale, low-flow• Delayed onset is not pharmacological “loading”, it’s earlier
Factor VII wearing out• Evening dosing allows more rapid dose adjustment• Medical Mutual of NC provides an informed consent contract
and a tracking flow-sheet• Every patient needs to have a phone, good literacy (or
designate someone to supervise both medication use and communication)
• 7-day pill organizers help
17
Warfarin IssuesWarfarin Issues
Drug interactions include many mechanisms• Metabolic breakdown of warfarin (EtOH, macrolides, St.
John’s wort)• Enteral kinetics for vitamin K (antibiotics)• Protein binding for warfarin (salsalate)• Increased risk for GI irritation (NSAIDs, EtOH)• Platelet inhibition (NSAIDs)
Dietary issues are about vitamin K• Outrageous fear, where education is for total avoidance
18

About Vitamin KAbout Vitamin K
• 1st reported in German as Koagulationsvitamin• Necessary for manufacture of hepatic-sourced
clotting factors. Longest-lived of these is VII• Sources are vegetables (green, leafy) spinach,
broccoli, but also onions, spices• Patients learn to fear these, resulting in
occasional intake with increased variability
19
SUPPLEMENTINGSUPPLEMENTING Vitamin K?! Vitamin K?! • Patient’s dietary variability is reduced in proportionate impact• Warfarin dose will need to be increased to measurable effect• Patients need to understand that skipping or stopping the
vitamin pill predictably causes dangerous warfarin overdose• To synchronize compliance, needs to be taken together• CostCo “Premium” multivitamins have 100% RDA (80
microgram daily). Studies used 100, 150, 200 μg• Patients need to understand that this is NOT a common
clinical practice
20
Vitamin K supplementation can improve stability of anticoagulation for patients with unexplained variability in response to warfarin Blood, 2007 109:2419-2423
Vitamin K1 supplementation to improve the stability of anticoagulation therapy with vitamin K antagonists: a dose-finding study Haematologica, 2011 96: 583-589

Modified Warfarin Tracking PageModified Warfarin Tracking Page
21
Located at TinyUrl/AntiCoag
Warfarin Dose CalculationsWarfarin Dose Calculations
• Use proportionate intervals (small steps for small doses, bigger steps for larger ones)
• Use just one pill-size• Smoothe the regimen across the week• Patient reads back their regimen• Calculator and tracking form and contract are
all at tinyurl.com/AntiCoag
22

Warfarin DoseWarfarin DoseAdjustment CalculatorAdjustment Calculator
23
Located at TinyUrl/AntiCoag
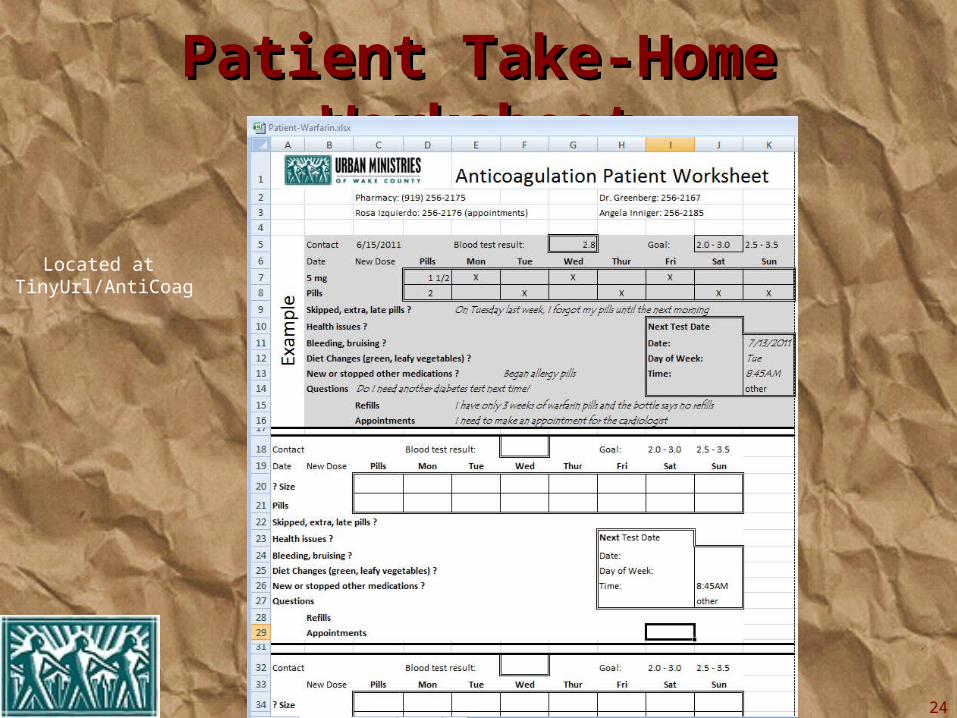
Patient Take-Home WorksheetPatient Take-Home Worksheet
24
Located at TinyUrl/AntiCoag

Duration of TherapyDuration of Therapy
• Atrial Fibrillation, until need to stop
• Pulmonary emboli or venous thrombosis (VTE) Single episode, Reversible cause: at least 3-6 months
Injury, immobility, pregnancy, medication (BCP’s), hospitalization Recurrent VTE: at least 12 months Idiopathic: unknown, perhaps 12 months Both recurrent and idiopathic (or irreversible): indefinite
25

Intensity of TherapyIntensity of Therapy
Usual case, INR 2.0 – 3.0• Venous thromboembolism• Atrial Fibrillation
High intensity, INR 2.5 – 3.5• Mechanical prosthetic valve
Low intensity (soft recommendation), INR 1.5 – 2.0• High risk patient, recurrent VTE
26

Other options: Other options: Enoxaparin (Lovenox®)Enoxaparin (Lovenox®)
Advantages• Compared to heparin drip
Out-patient Intermittent, calculated dose Rarer platelet antibodies No monitoring
• Compared to warfarin Instantly on, quickly gone No monitoring Predictable dose More effective in cancer pts
Disadvantages• Injectable, local bruising• Cost:
100 mg BID, $3,400/mo 60 mg BID, $2,050/mo But: Pt Assistance available
27
Other options: Other options: Vena Cava Filter (“umbrella”)Vena Cava Filter (“umbrella”)
• Only for prevention of pulmonary emboli, not for cardiac valves or atrial fibrillation Patients still have clots in their legs, with pain, edema
• Effective immediately, but invasively• Need to discuss if permanent is desired, many are
permanent (or require open, surgical removal)• Allows discontinuation of anticoagulation during GI
bleed or stroke urgency
28
Other options: Other options: Dabigaltran Pradaxa®Dabigaltran Pradaxa®
• Direct thrombin inhibitor, licensed 10/20/10• Effective in 12 hours• No monitoring, no dose-calculation, no injection, no
dietary issues, (almost) no interactions• Only licensed for Atrial Fibrillation, but published
articles show advantages for venous thrombo-embolism, too
• Usual dose: 150 BID, $220/mo (renal dose reduction)• Patient assistance is available
29

Other options: Other options: Rivaroxaban (soon more?)Rivaroxaban (soon more?)
• Direct thrombin (factor Xa) inhibitor• Derived from 2 Mexican leach anticoagulants• New class of agent, several collectively called
“xabans” (get it?)• Daily flat oral dosing, without monitoring, dietary
effects, many drug interactions (except statins via cytochrome CYP3A4)
30

ReferencesReferences
Online sites• ePocrates.com• DestinationRx.com• NeedyMeds.com• DailyMed.nlm.nih.gov• Guidelines.gov
Peer-reviewed Publications (avail online)• Mgmt of VTE: A Clinical Practice
Guideline from Amer. Coll. of Physicians & Amer. Acad. of Fam. Physicians (2007) Ann Intern Med 2007 146:204-210
• New Anticoagulants and the Future of Cardiology Rev Esp Cardiol. 2010; 63 :1223-9
31

I’m not just a speaker / doctor…I’m not just a speaker / doctor…
Just like Cy Sperling,President of the “Hair Club for Men” (& a member)
(no endorsement intended)
My personal medical history Remote ankle surgery, mild permanent venous insufficiency Ipsilateral distal DVT, 20 yrs later Pulmonary embolus 2 years later Negative thrombophilia evaluation, now (+) Family History spont DVT Lifelong “full” anticoagulation
32