anorectal anomaly(imperforate anus)
TRANSCRIPT
ANORECTAL ANOMALIES ANORECTAL ANOMALIES
(IMPERFORATE ANUS) (IMPERFORATE ANUS)
ANORECTAL ANOMALIES
Dr.B.SELVARAJ MS;Mch; FICS;
ASSOCIATE PROFESSOR IN PEDIATRIC SURGERY
MELAKA MANIPAL MEDICAL COLLEGE
MELAKA 75150 MALAYSIA
M
M
M
C
ANORECTAL ANOMALIES
Appropriate workup to confirm the type of anomaly
Able to identify associated anomalies
Objectives
1
2
3
4
5
Identify anomalies in male & female babies Identify anomalies in male & female babies
Proper postop care & followup Proper postop care & followup
Planning of surgical treatment for different types Planning of surgical treatment for different types
M
M
M
C
ANORECTAL ANOMALIES-Embryology
M
M
M
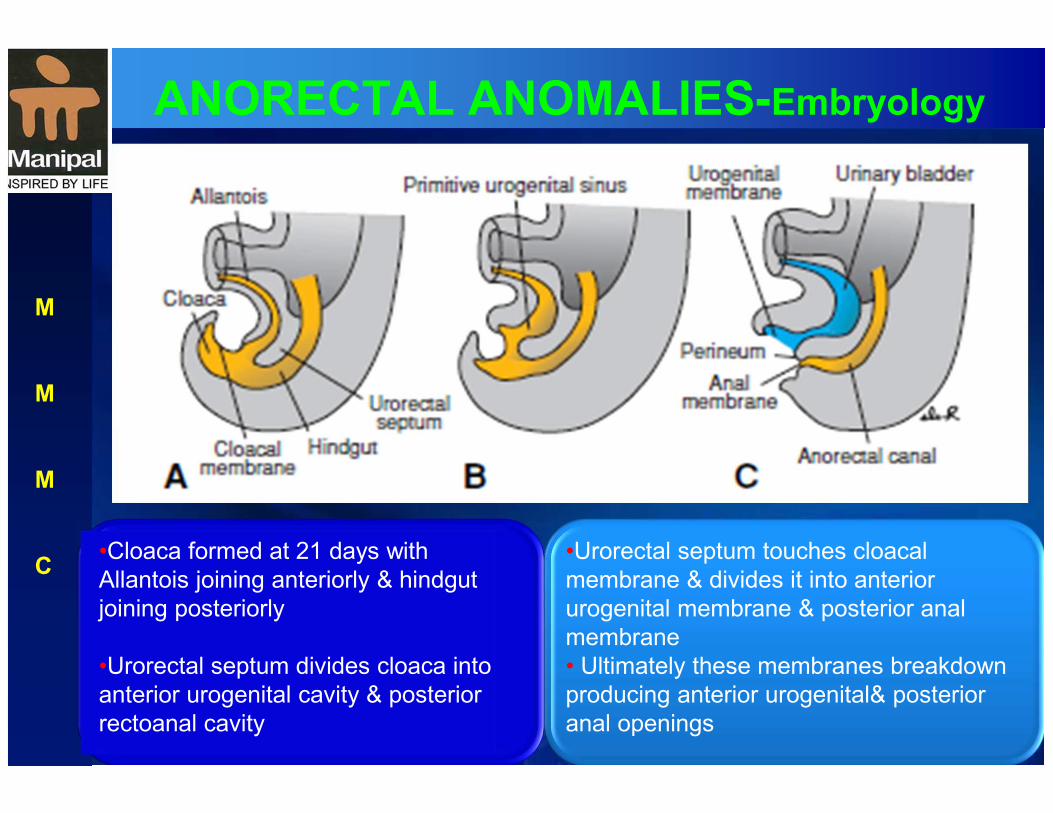
C •Cloaca formed at 21 days with
Allantois joining anteriorly & hindgut
joining posteriorly
•Urorectal septum divides cloaca into
anterior urogenital cavity & posterior
rectoanal cavity
•Urorectal septum touches cloacal
membrane & divides it into anterior
urogenital membrane & posterior anal
membrane
• Ultimately these membranes breakdown
producing anterior urogenital& posterior
anal openings
ANORECTAL ANOMALIES-Embryology
Rectoanal atresias & fistulas occur 1/5000 livebirths due to defective cloacal formation
Decrease in size of posterior portion of cloaca & shortening of cloacal membrane results in ectopic anal opening into urogenital sinus
Depending on the size of posterior portion of cloaca the rectourethral fistula may be high or low
Defect is due to ectopic positioning of anal opening & not in any defect in urorectal septum
Imperforate anus: The anal canal fails to recanalise, leaving a diaphragm between the upper & lower portions of the anal canal
M
M
M
C
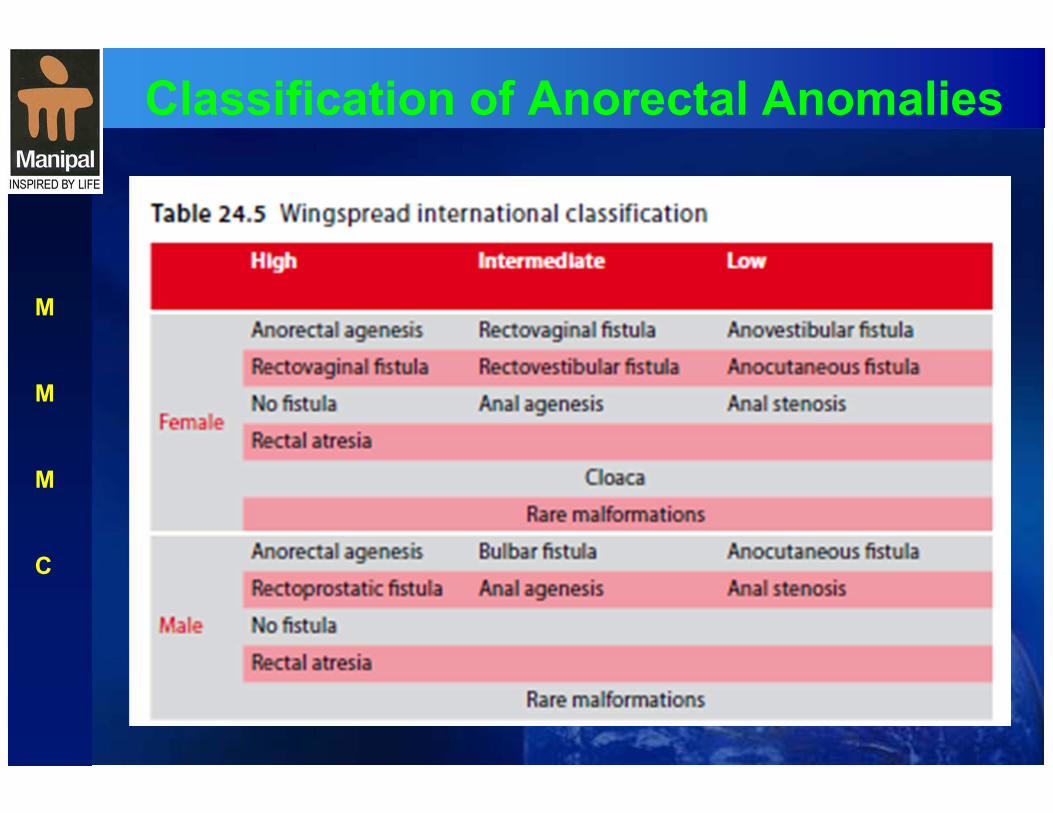
Classification of Anorectal Anomalies
M
M
M
C

Classification of Anorectal Anomalies
M
M
M
C
ANORECTAL ANOMALIES
Develop during first 2 months of life- but cause is unclear
Agents causing the anomaly have general noxious effects on the developing fetus- hence associated anomalies are common
Males are more affected with severe malformation
Incidence 1 in 5000 livebirths
M
M
M
C
ANORECTAL ANOMALIES
Present as absence of anus in it’s normal position
In mild forms bowel outlet opens in perineum outside the well developed muscle sphincter complex
In severe forms bowel outlet opens in urogenital tract in males & genital tract in females
Neonatal recoginition of type of anomaly is essential for planning the surgical management
M
M
M
C
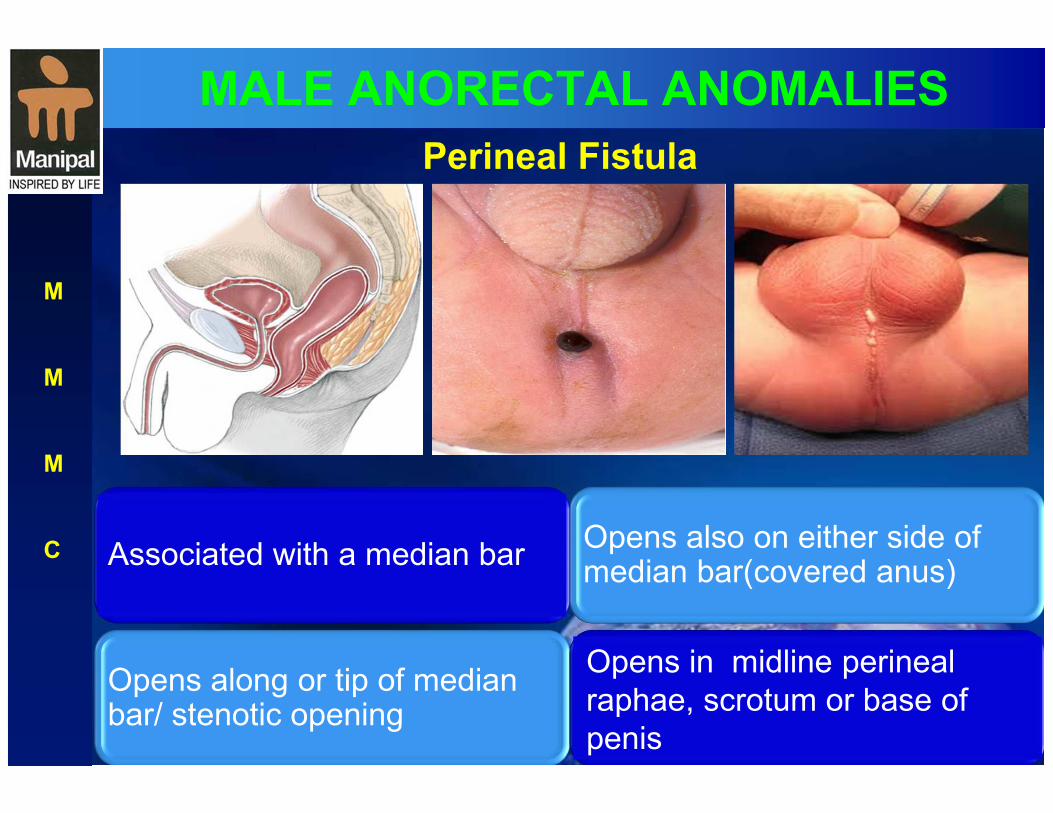
MALE ANORECTAL ANOMALIES
Perineal Fistula
M
M
M
C Associated with a median bar Opens also on either side of median bar(covered anus)
Opens along or tip of median bar/ stenotic opening
Opens in midline perineal
raphae, scrotum or base of
penis

MALE ANORECTAL ANOMALIES
Rectobulbar fistula
M
M
M
C
Rectum opens into the bulbar
urethra Presence of anal pit in perineum
Long common wall of rectum and urethra
Voluntary sphincter muscle
complex is well developed
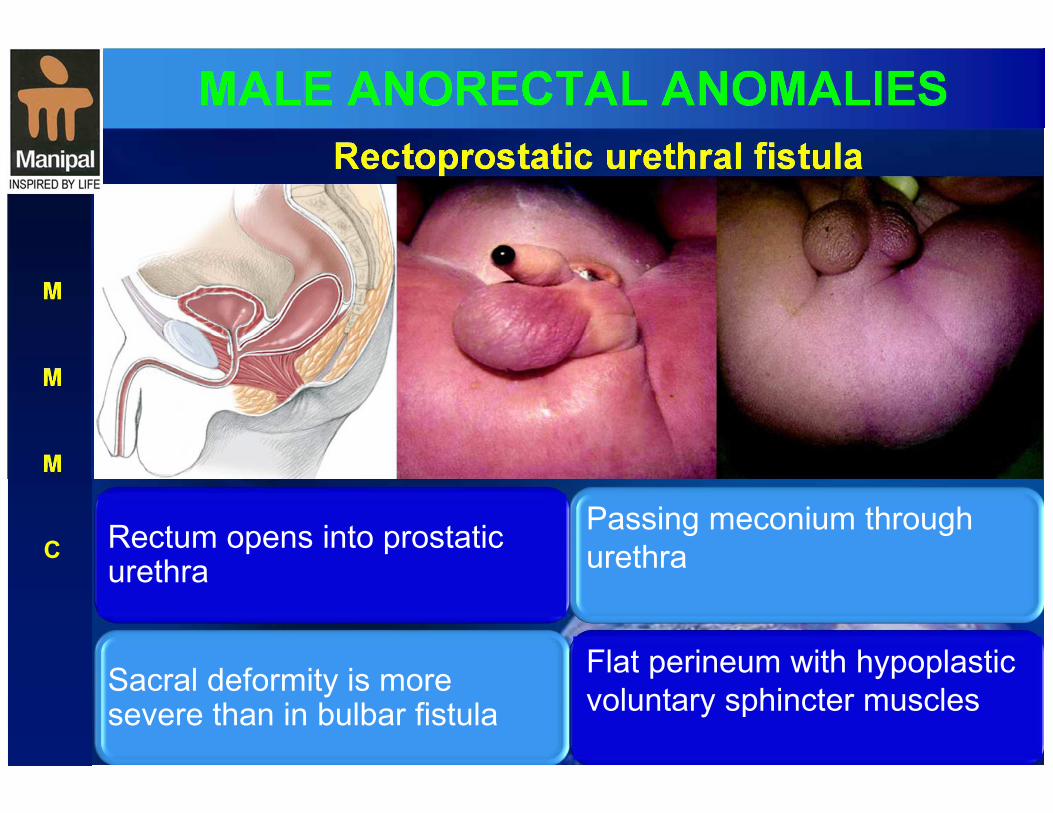
MALE ANORECTAL ANOMALIES
M
M
M
C Rectum opens into prostatic urethra
Passing meconium through
urethra
Sacral deformity is more severe than in bulbar fistula
Flat perineum with hypoplastic
voluntary sphincter muscles
Rectoprostatic urethral fistula
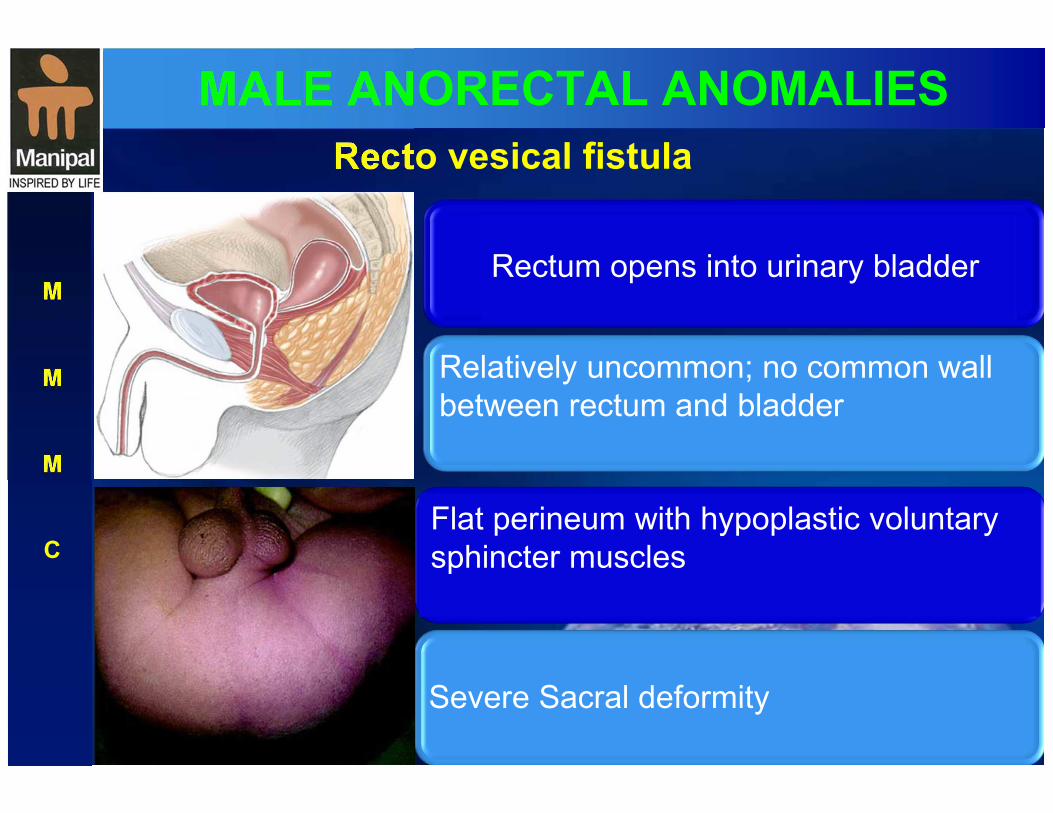
MALE ANORECTAL ANOMALIES
M
M
M
C
Rectum opens into urinary bladder
Relatively uncommon; no common wall
between rectum and bladder
Severe Sacral deformity
Flat perineum with hypoplastic voluntary
sphincter muscles
Recto vesical fistula
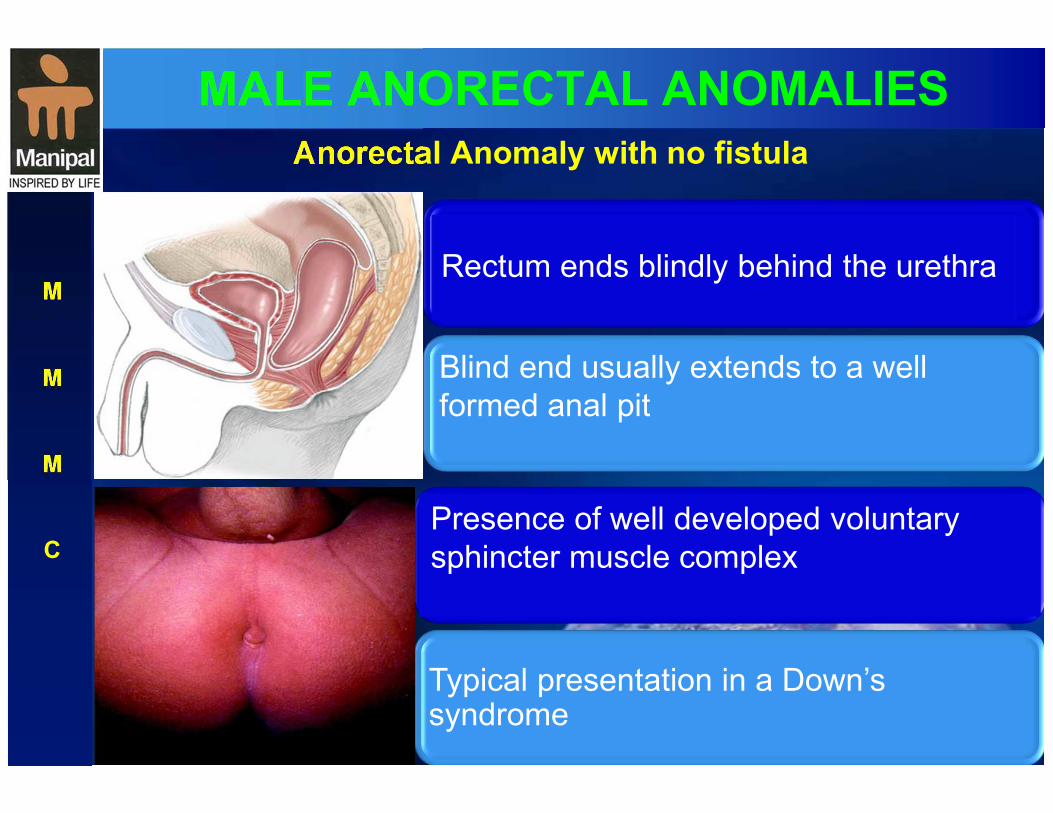
MALE ANORECTAL ANOMALIES
M
M
M
C
Rectum ends blindly behind the urethra
Blind end usually extends to a well
formed anal pit
Typical presentation in a Down’s syndrome
Presence of well developed voluntary
sphincter muscle complex
Anorectal Anomaly with no fistula
MALE ANORECTAL ANOMALIES
M
M
M
C
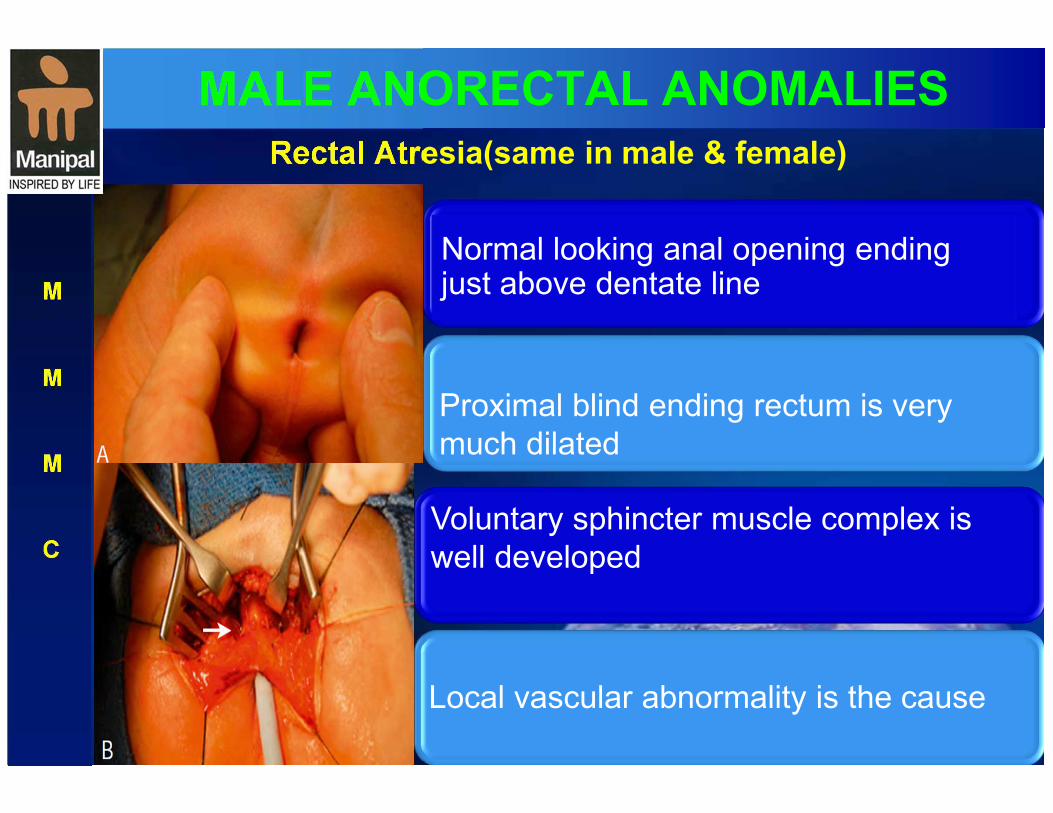
Normal looking anal opening ending just above dentate line
Proximal blind ending rectum is very
much dilated
Local vascular abnormality is the cause
Voluntary sphincter muscle complex is
well developed
Rectal Atresia(same in male & female)
FEMALE ANORECTAL ANOMALIES
M
M
M
C
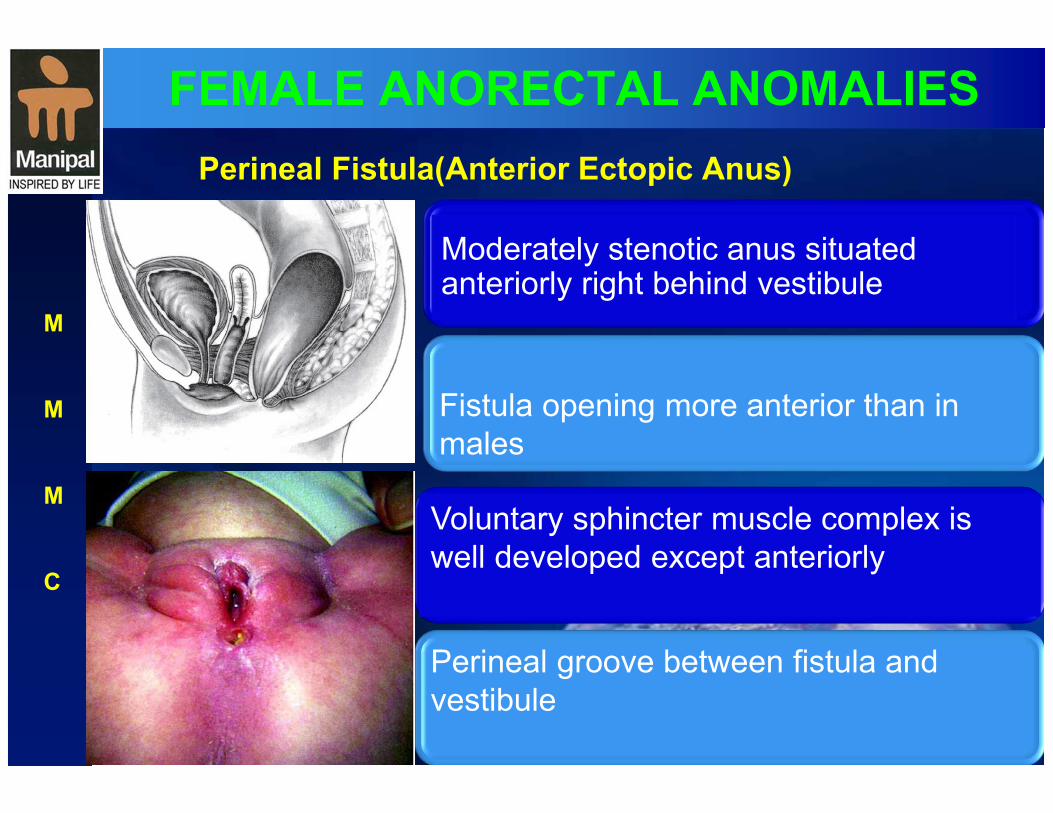
Moderately stenotic anus situated anteriorly right behind vestibule
Fistula opening more anterior than in
males
Perineal groove between fistula and
vestibule
Voluntary sphincter muscle complex is
well developed except anteriorly
Perineal Fistula(Anterior Ectopic Anus)
FEMALE ANORECTAL ANOMALIES
M
M
M
C
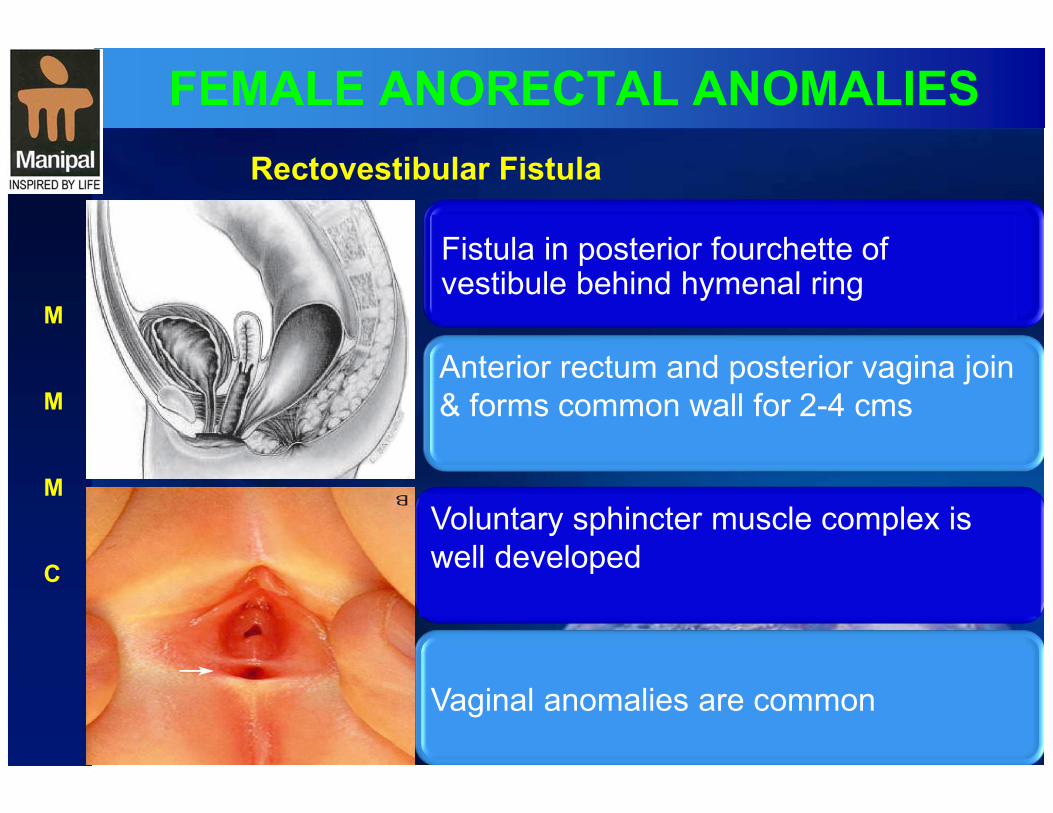
Fistula in posterior fourchette of vestibule behind hymenal ring
Anterior rectum and posterior vagina join
& forms common wall for 2-4 cms
Vaginal anomalies are common
Voluntary sphincter muscle complex is
well developed
Rectovestibular Fistula
FEMALE ANORECTAL ANOMALIES
M
M
M
C
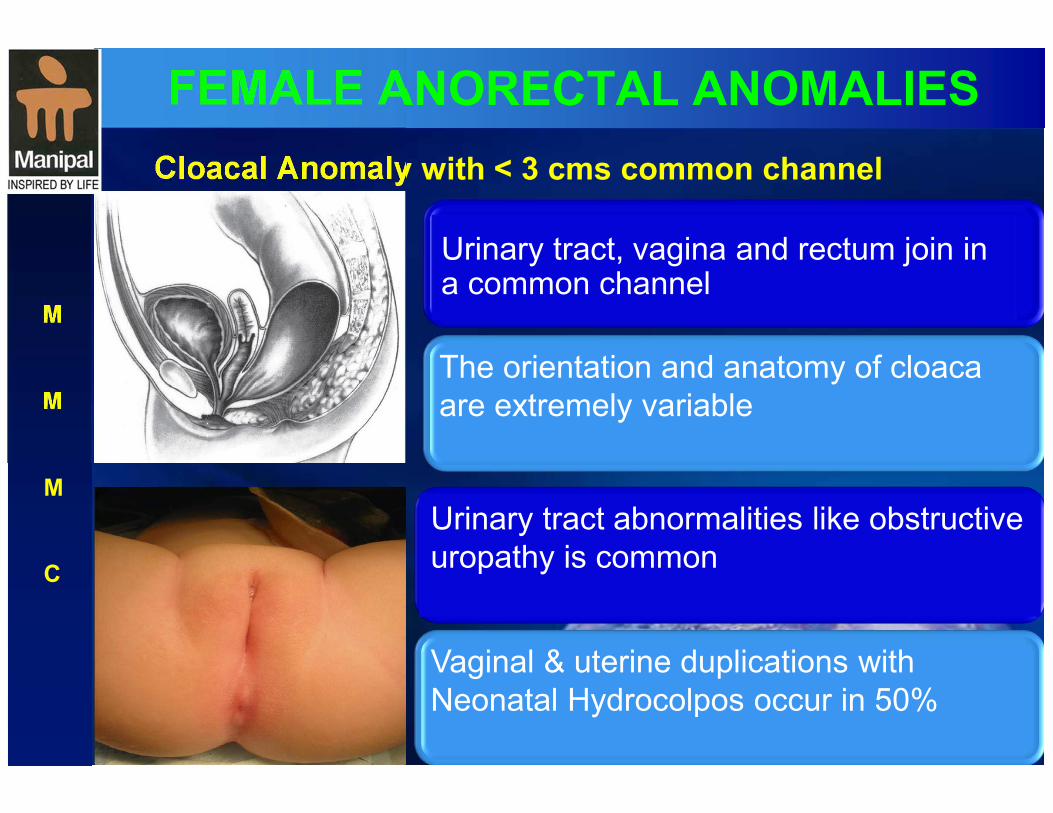
Urinary tract, vagina and rectum join in a common channel
The orientation and anatomy of cloaca
are extremely variable
Vaginal & uterine duplications with
Neonatal Hydrocolpos occur in 50%
Urinary tract abnormalities like obstructive
uropathy is common
Cloacal Anomaly with < 3 cms common channel
FEMALE ANORECTAL ANOMALIES
M
M
M
C
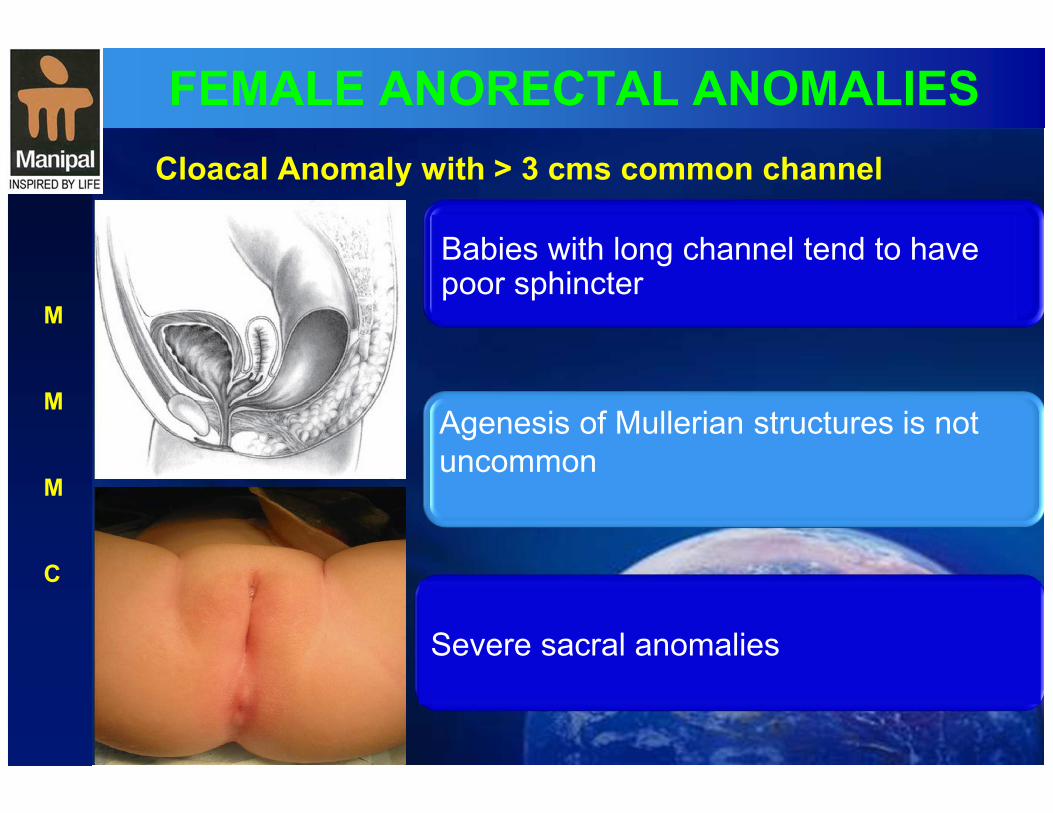
Babies with long channel tend to have poor sphincter
Agenesis of Mullerian structures is not
uncommon
Severe sacral anomalies
Cloacal Anomaly with > 3 cms common channel
FEMALE ANORECTAL ANOMALIES
M
M
M
C
Uncommon in females
Most babies have Down’s syndrome
Short distance between blind ending rectum and well
formed anal pit
Anorectal Anomaly with no fistula
Well-developed sphincters
ANORECTAL ANOMALIES
M
M
M
C
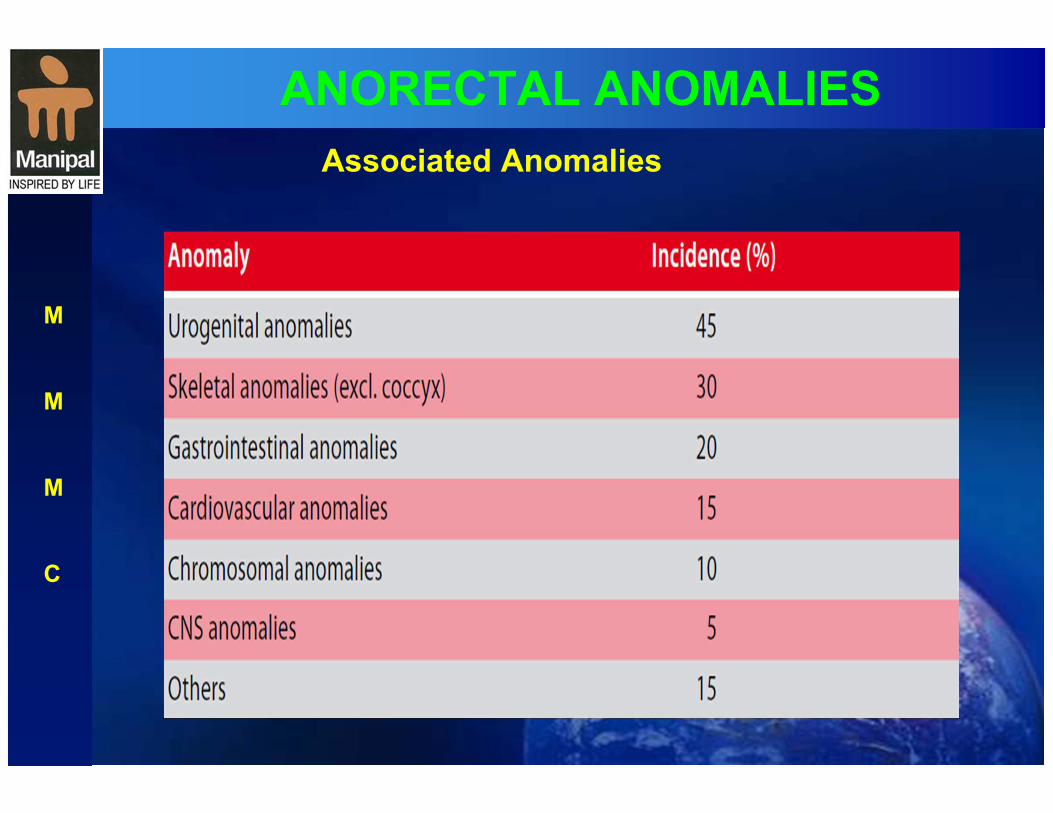
Associated Anomalies

ANORECTAL ANOMALIES- Preop workup
Clinical examination discloses the type of anomaly in majority of cases
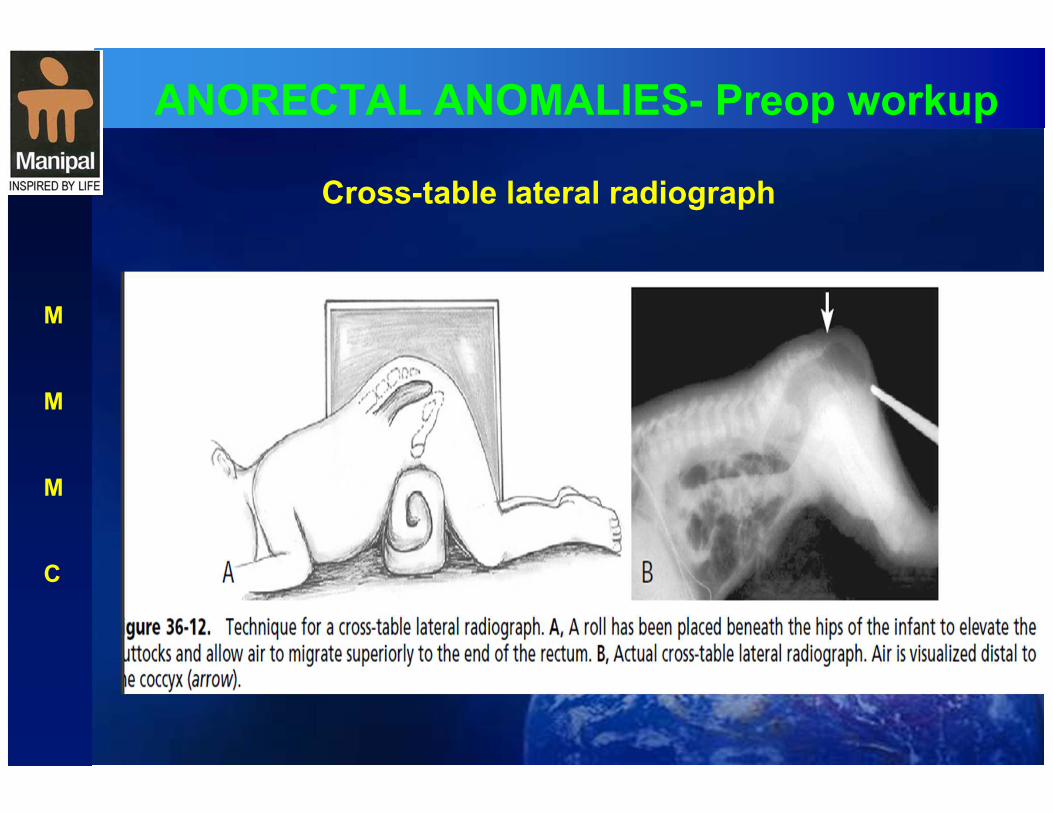
Cross-table lateral plain xray in doubtful cases to be done after 18-24 hrs
Early perineal USG to confirm type of anomaly
Abdominal USG& Echo to R/O associated anomalies
CT & MRI to reveal integrity of sphincter muscles
M
M
M
C
ANORECTAL ANOMALIES- Preop workup
M
M
M
C
Cross-table lateral radiograph

ANORECTAL ANOMALIES- Preop workup
M
M
M
C
Cross-table lateral radiograph
Low anomaly
Intermediate Anomaly
High anomaly

ANORECTAL ANOMALIES- Surgeries
M
M
M
C
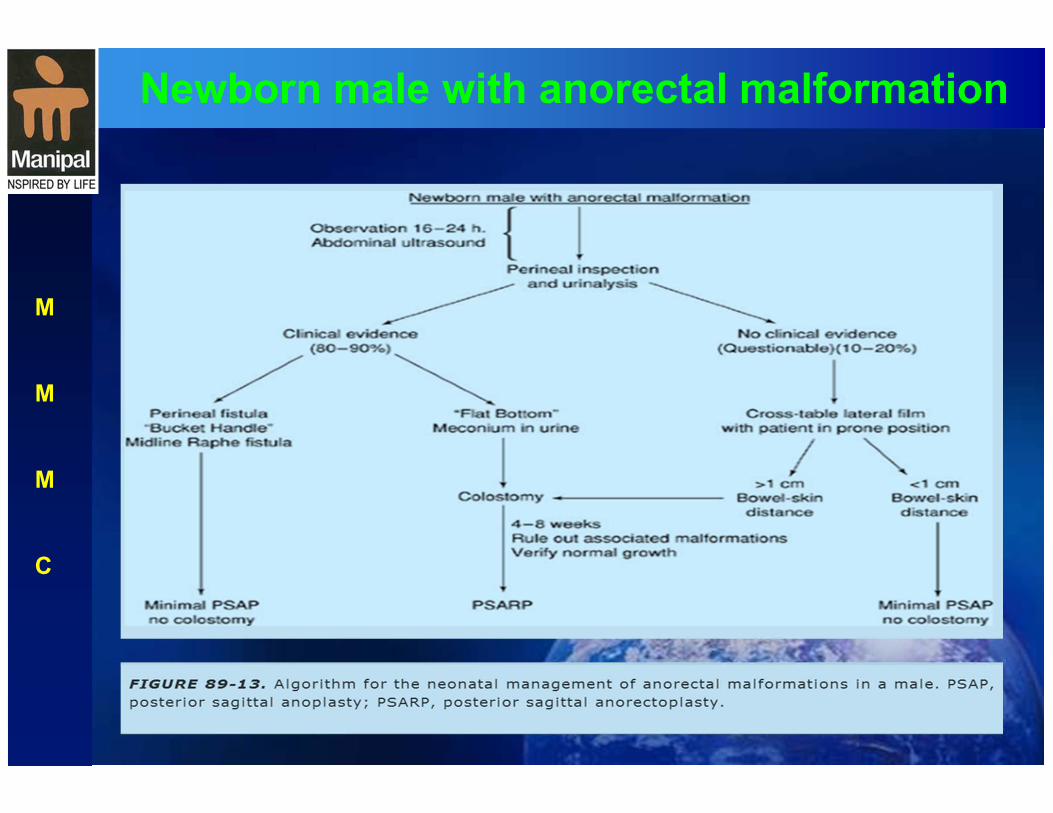
Newborn male with anorectal malformation
M
M
M
C
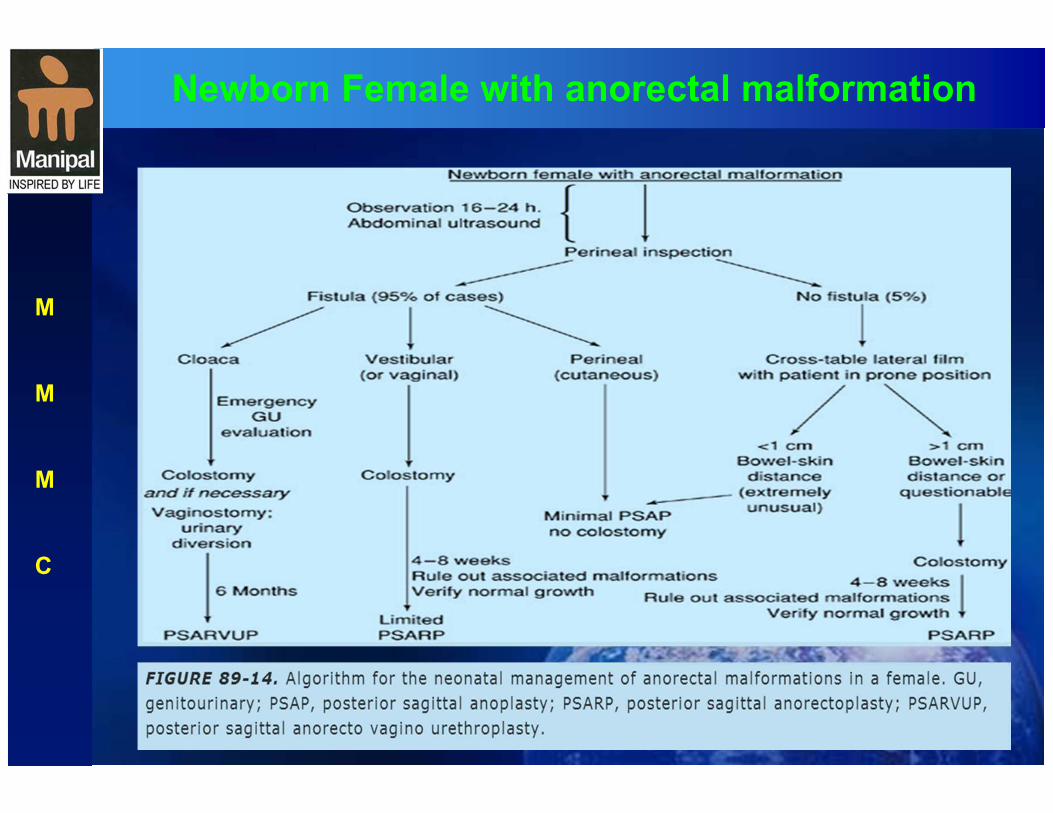
Newborn Female with anorectal malformation
M
M
M
C
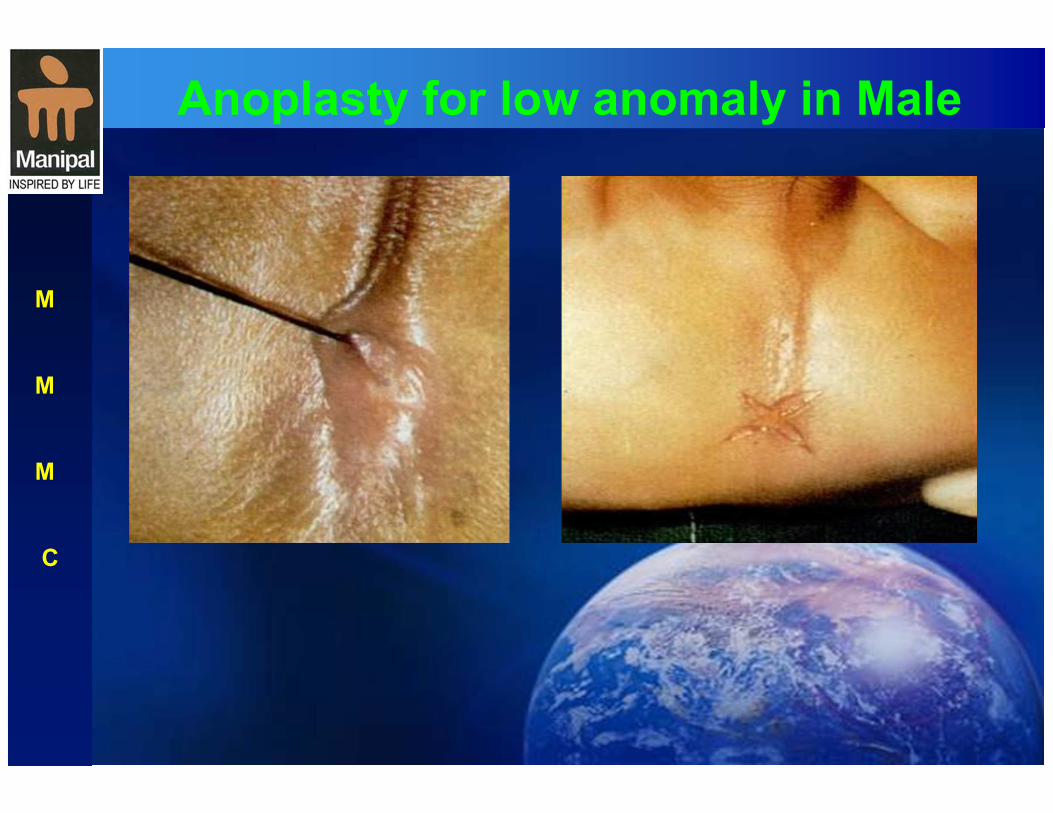
Anoplasty for low anomaly in Male
M
M
M
C
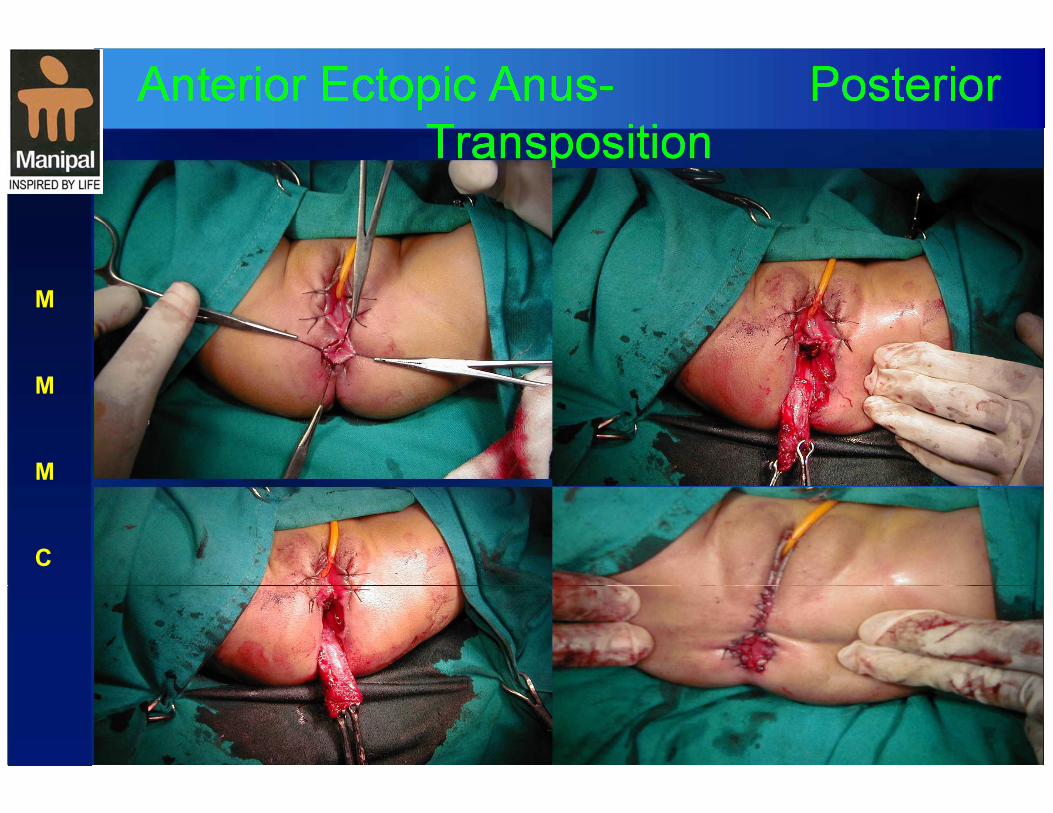
Anterior Ectopic Anus- Posterior
Transposition
M
M
M
C
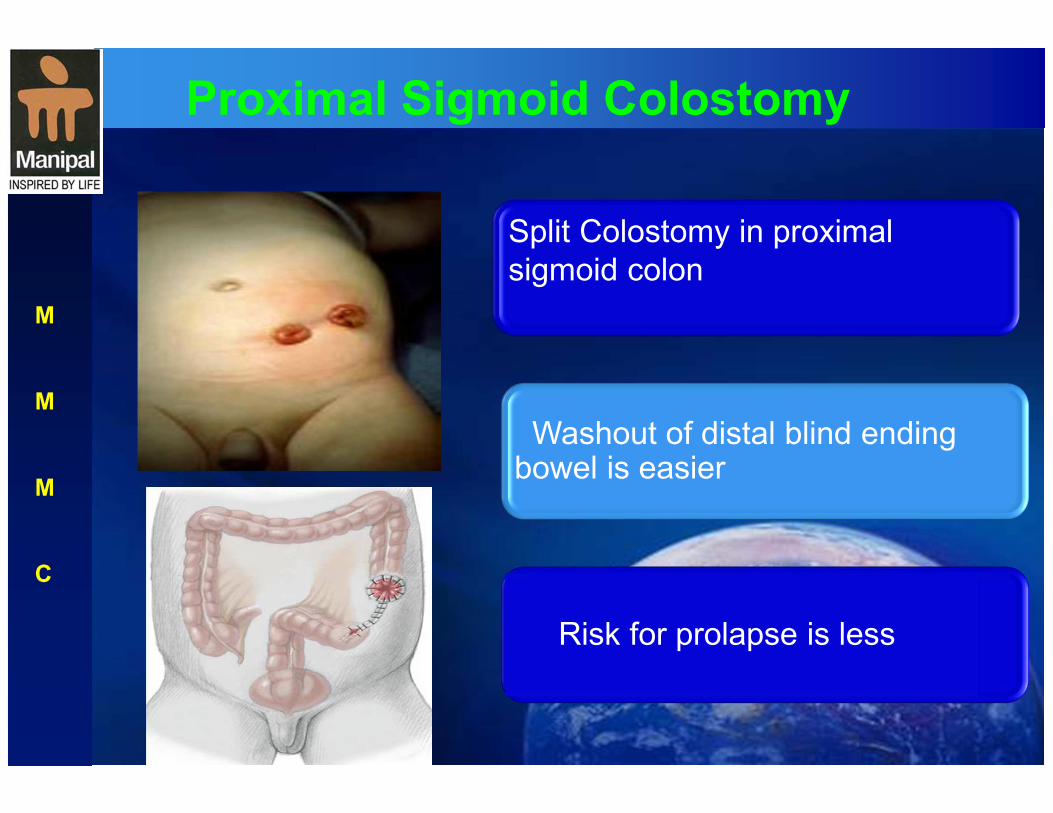
Proximal Sigmoid Colostomy
M
M
M
C
Split Colostomy in proximal
sigmoid colon
Washout of distal blind ending bowel is easier
Risk for prolapse is less

Distal Colostogram
M
M
M
C
Pressure distal colostogram
revealing the fistula
Dye fillsup both bladder and urethra

Posterior Saggital Anorectoplasty
M
M
M
C
Baby in prone position
Midline Saggital incision

Posterior Saggital Anorectoplasty
M
M
M
C
Opening Rectum
Identifying Fistula
Separating Fistula
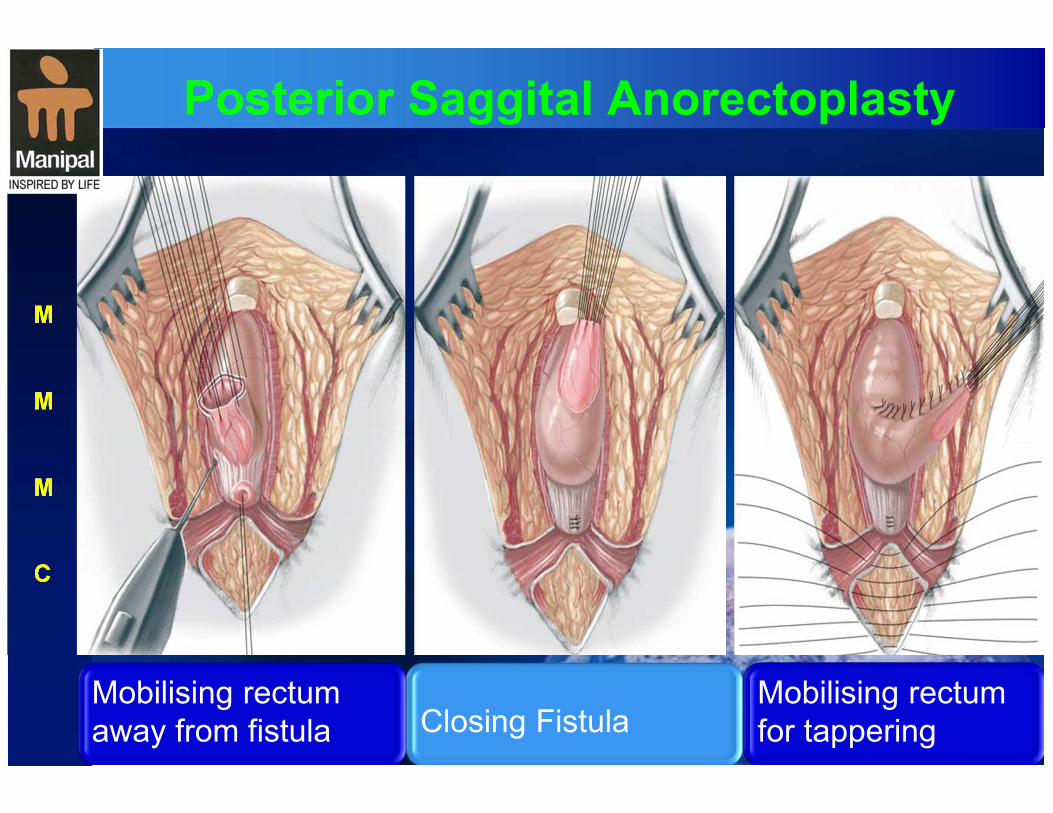
Posterior Saggital Anorectoplasty
M
M
M
C
Mobilising rectum
away from fistula
Closing Fistula
Mobilising rectum
for tappering

Posterior Saggital Anorectoplasty
M
M
M
C
Closing muscle
complex
Closing Sphincter
Closing skin
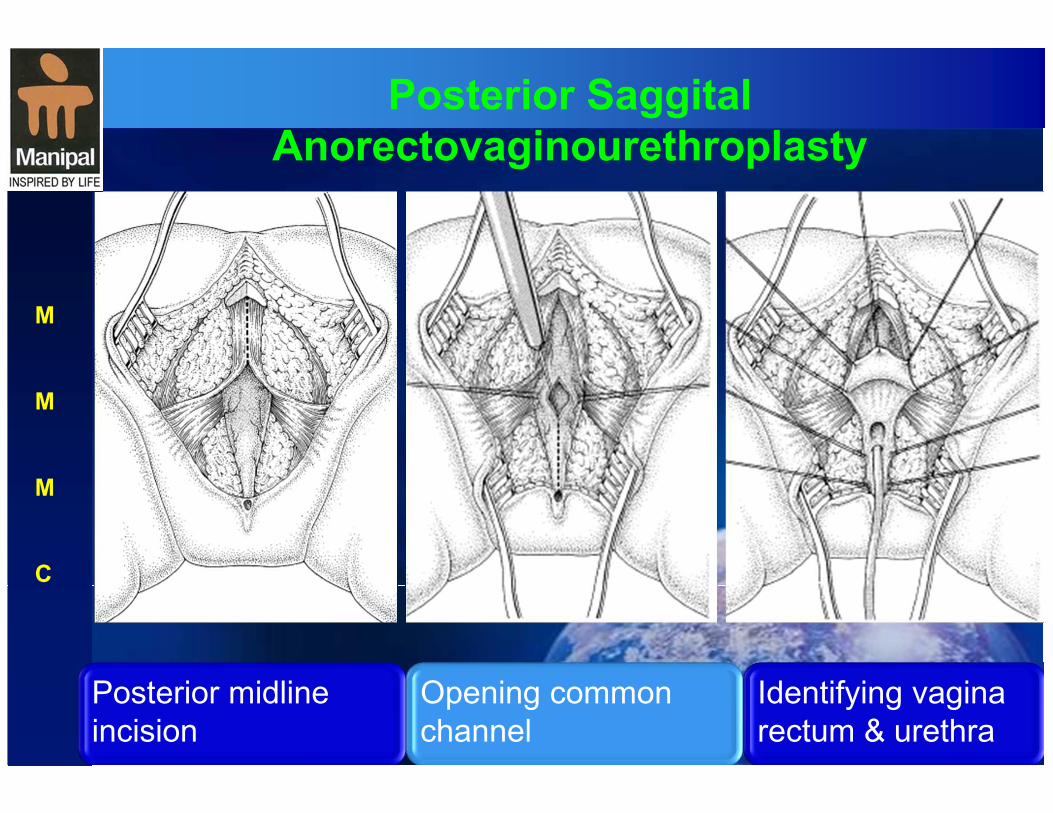
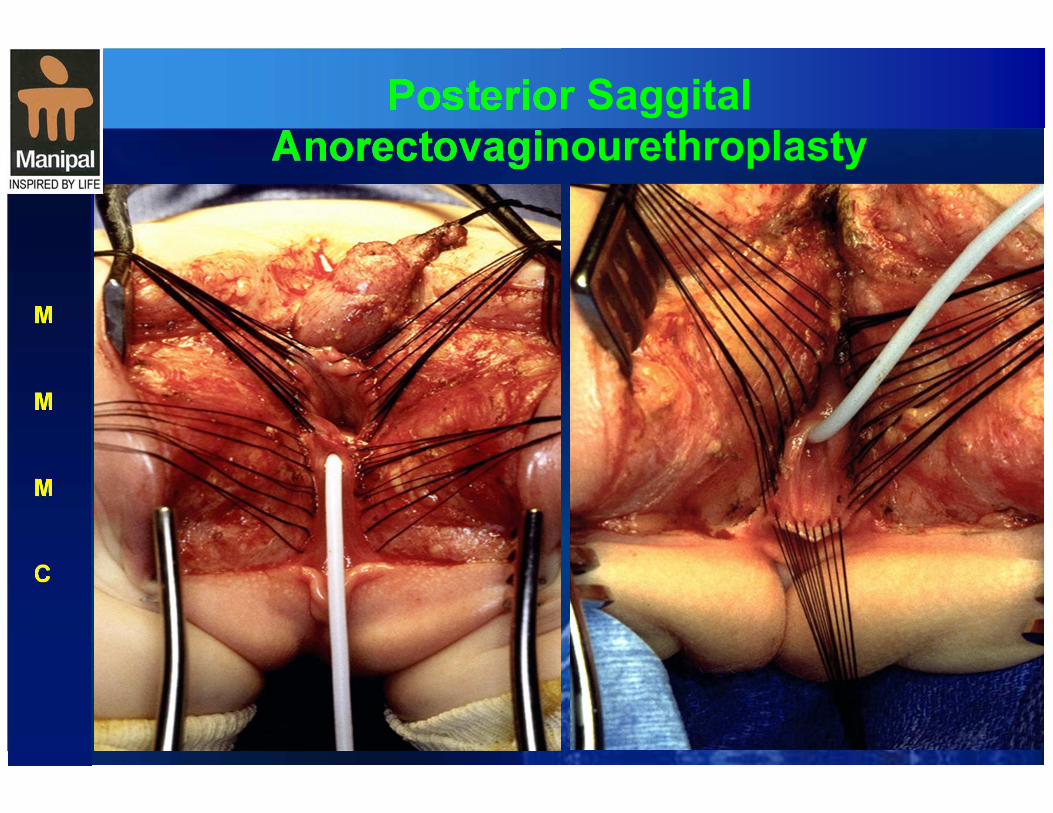
Posterior Saggital
Anorectovaginourethroplasty
M
M
M
C
Posterior midline
incision
Opening common
channel
Identifying vagina
rectum & urethra
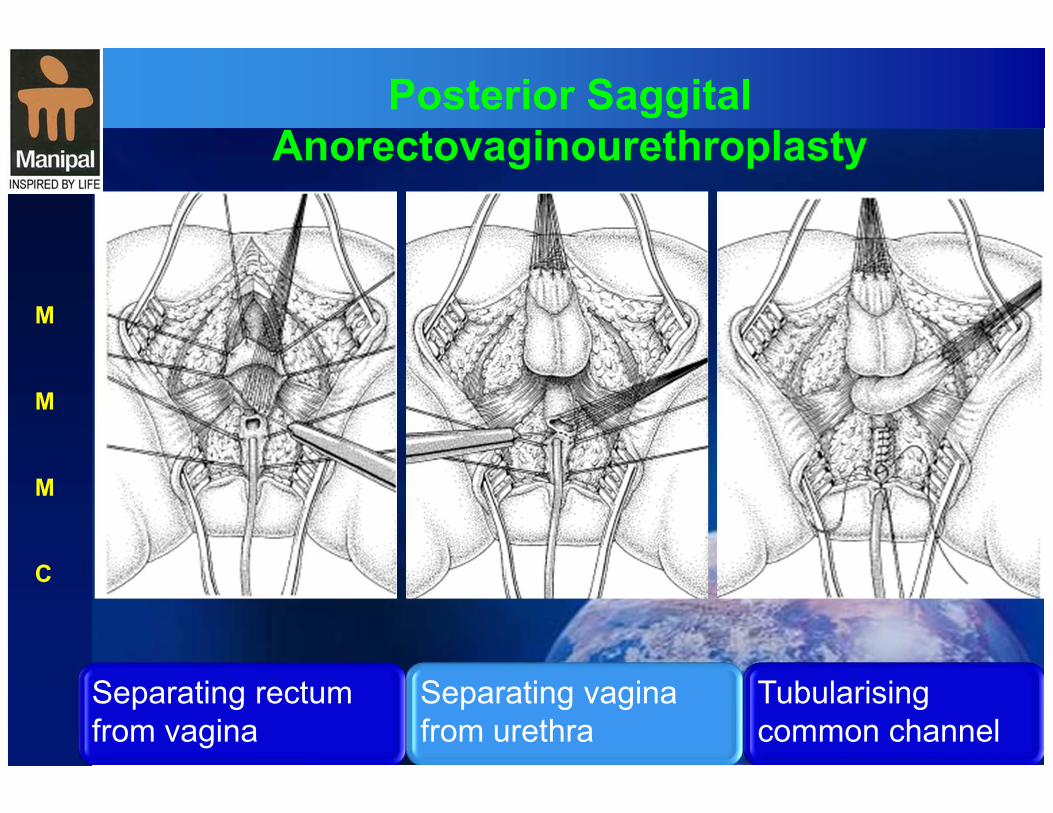
Posterior Saggital
Anorectovaginourethroplasty
M
M
M
C
Separating rectum
from vagina
Separating vagina
from urethra
Tubularising
common channel
Posterior Saggital
Anorectovaginourethroplasty
M
M
M
C
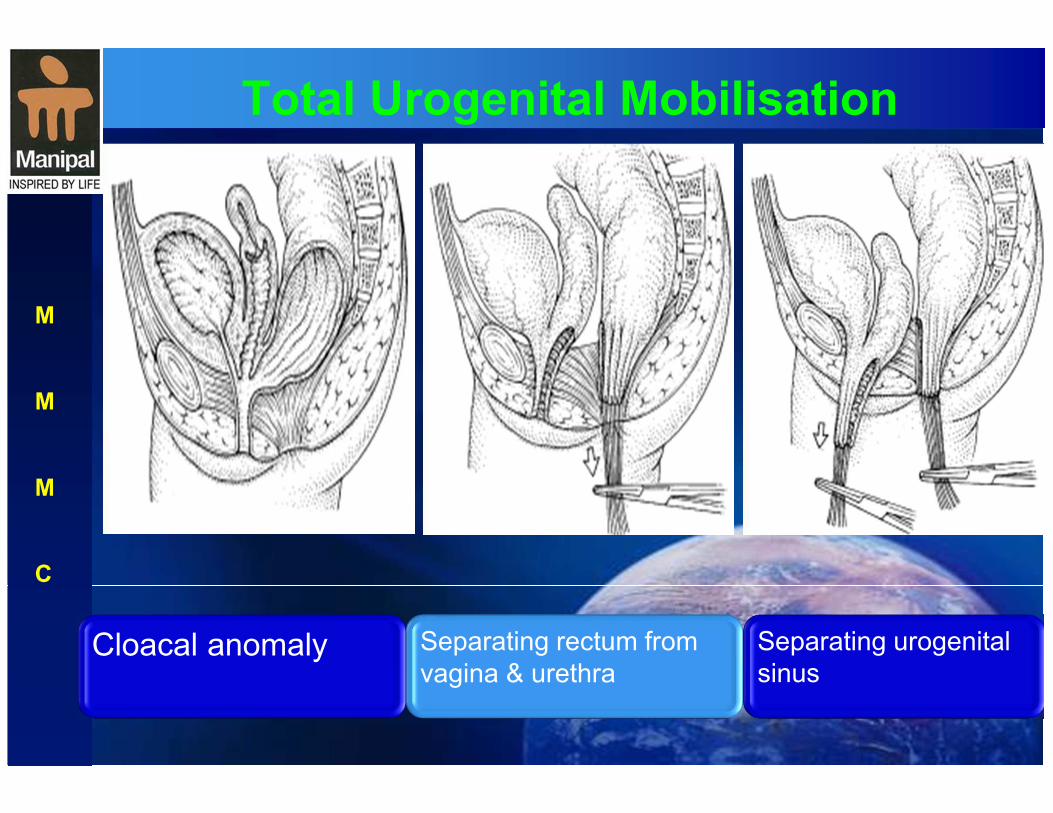
Total Urogenital Mobilisation
M
M
M
C
Cloacal anomaly
Separating rectum from
vagina & urethra
Separating urogenital
sinus
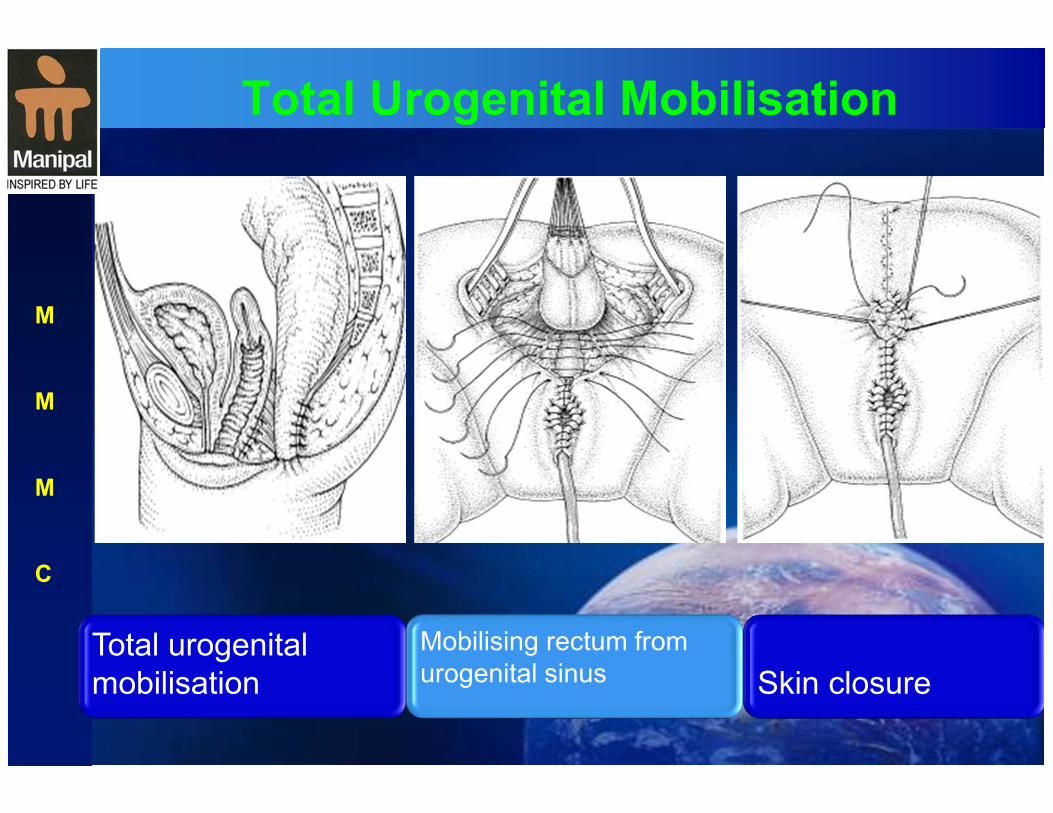
Total Urogenital Mobilisation
M
M
M
C
Total urogenital
mobilisation
Mobilising rectum from
urogenital sinus
Skin closure
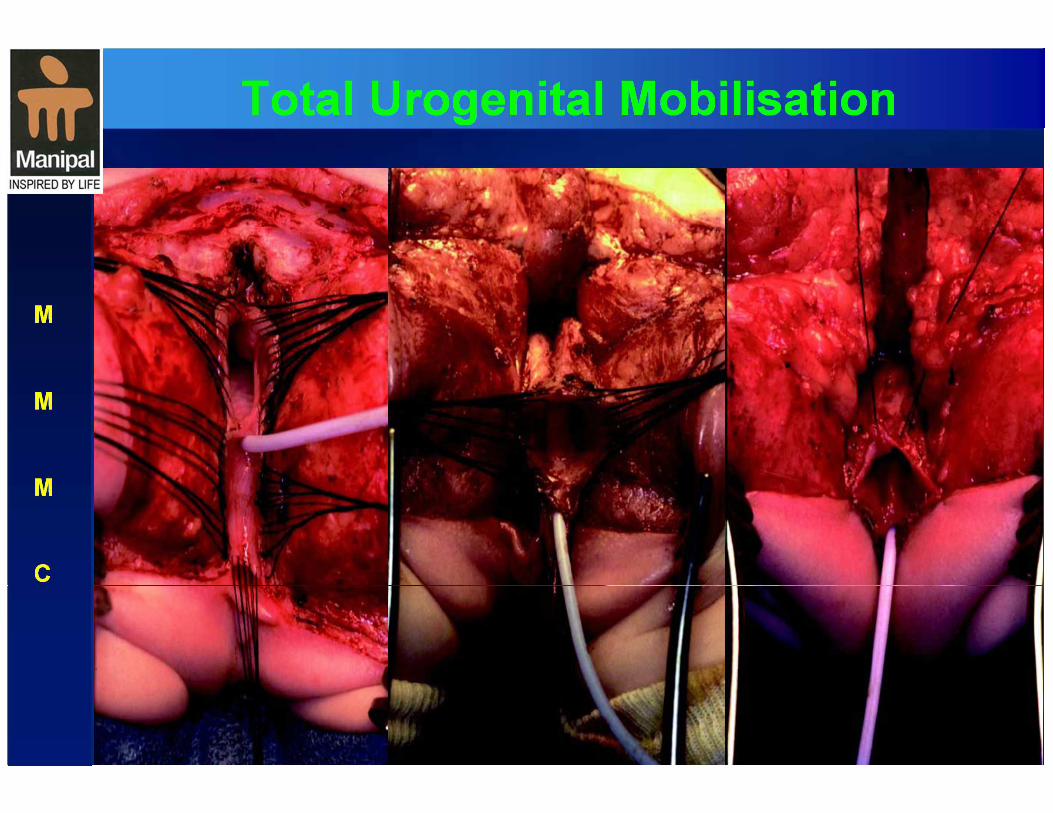
Total Urogenital Mobilisation
M
M
M
C
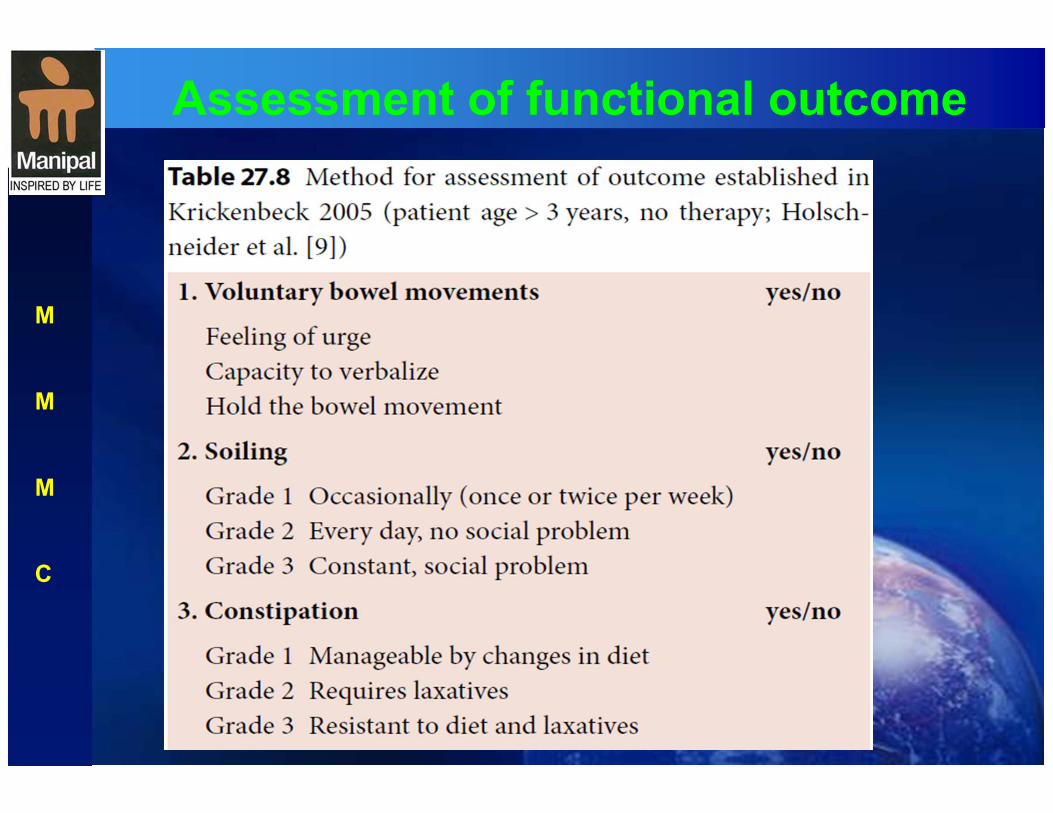
Assessment of functional outcome
M
M
M
C

Assessment of functional outcome
M
M
M
C
