annual report 1980 - lenus the irish health repository · annual report 1980 73, lower baggot...
TRANSCRIPT

Medico-Social Research Board annual report 1980 (1.98 MB)
Item type Report
Authors Medico-Social Research Board
Rights Medico-Social Research Board
Downloaded 31-May-2018 02:16:35
Link to item http://hdl.handle.net/10147/45741
Find this and similar works at - http://www.lenus.ie/hse

THE MEDICO-SOCIAL RESEARCH BOARD
An Bord Taighde Pobal-Liachta
ANNUAL REPORT 1980
73, Lower Baggot Street, Dublin 2 . Ireland.

THE MEDICO-SOCIAL RESEARCH BOARD
MICHAEL M. MACCOKMAC MA., M.Cornm.. FCCA., Professor of Business Administration. Univcrsity Col- lege Dublin.
Membrrs
GEOFFREY J. BOUKKE, MU., MA., FRCI'l., FFCM.(I)., DPH., DIH (Dundee), DCH., Profcssorof Community Medicine and Epidemiology, University College, Dub- lin and Dean of the Faculty of Community Medicine, Royal College of Physicians of Ireland.
JOHN P. CORRIUAN, MD., DPH., FFCM.(I)., DIH. (St.And.), Professor of Social Medicine, Yniversity College, Cork.
RISTEARD MULCAHY, MU., FRCP., FRCPI., Professor of Preventive Cardiology, University College, Dublin and Director, Cardiac Department, St. Vincent's Hospital, Dublin.
BARBARA STOKES, BA., FRCPI. Medical Director, St. Michael's House, Dublin.

Mcr;/cc! Il~~a11lz St~rdies: D. Walsh, MB.. DPM., FFCM.(I)., FRC:.I'syci1.
Congenitul A hnormuliries Register und Smdn'(w I,~lfufur~r D c ~ h Srudy:
A. Radic, MA., M R . , MFCMI.
Perinnfnl and Child Ileullh Studio.:: P . N . Kirke, MR., MI;CM.(I). , M.Sc., DC.'! I . . D . 0 h t .
Menti11 flundicup S~~cdies: M. Mulcahy, M B . , FKCPI.. MKC Psych., UPFI.
Medical Research As.sistunt.s lo the Director. ,
R. Hamili, MB.B.CI~. DCH.. E. Shelley, M B . R . C ~ I . M K C P I
Sociol0n.ists: A. O'Hare, M.Soc.Sc. (Senior Socioiogist), ?'. Brannick, M.Soc.Sc., B.Sc., A. O'Connor, B .Soc.Sc., S. O'Connor ,
M.Soc.Sc., J. Walsh, M.Soc.Sc.Dip.Stals.
Research und Admini~trution: H. McLoughlin (Personal Assistant to Director), G. O'Mahony (Assistant to Secretary), A.Purcell (Supervisor, Hospital In-Patient Enquiry Scheme), M. Griffin, RGN, A.
Kingston, B. McGrath, S. Starks, BA, 1I.Dip.
Secr~lurial: J . Murtagh, J . McCann, M. O'Dwycr, S. Riordan.
Clerical: R. Brady, Y . Dunne, R. Francis, H. Holden, N. McConnell,
M. Reade, M. Sheeran, A. Tobin, J. Woods, S. Woods.

Housekeeping: E. Roberts.
Maintenance: L. Johnson.
Staff working outside Head Office D. Carey, T . Cleary, M.Coffey, J. Colfer, B. Costelloe, E. Cox, C. Delaney, A. Dempsey, M. Giblin, U. Greaney, C. Lennon, A. Morrissey, D. Merrin, D. Murphy, M. McCau- ley, J. McLoughlin, M. McLoughlin, P. Rowe, J. Smith, C. Twomey, C. Tyrrell, A. Whelan.

ACTIVITIES OF THE MEDICO-SOCIAL RESEARCH BOARD 1980
Page 1 . Introduction ... ... . . . . . . . . . . . . 7
2. Hospital In-patient Enquiry Scheme. 13
3. Studies on Mental Health: (i) National Psychiatric In-patient Reporting
System ... ... . . . . . . . . . . - . 17 (ii) Determinants of Outcome of Severe Mcn-
tal Disorders .. . . . . . . . . . . . . . 18 (iii) Three-County Psychiatric Case Register 19 (iv) Three-County Schizophrenia Study . . . 20 (v) Mental Health Services in Pilot Study
Areas .. . . . . ... . . . . . . ... 21 (vi) The 1981 Psychiatric Hospital Census . . . 22 (vii) Alcohol-related problems . . . . . . ... 23
(viii) Unmarried Parents and their Children . . . 25 (ix) Suicide and Attempted Suicide . . . ... ,: 26 (x) Community Care of Discharged Psychiatric
Patients: An Evaluative Study of Aftercare. . . . . . . . . . ... ... 27
(xi) First Admissions to Psychiatric Hospitals in South-East England: Immigrants from Ireland. . . . . . . ... . . . ... 28
4. Studies on Mental Handicap: (i) Mental Handicap-Prevalence and Care. 30 (ii) Census of Mental Handicap ... ... 33
(iii) Survey of Adult Mentally Handicapped Persons living in the Community. ... ... 35
(iv) Register of females of childbearing age with phenylketonuria . . . ... ... ... 37
5. Perinatal Epidemiology: (i) Perinatal and Infant Mortality in Ireland
and Selected Countries . . . . . . ... 40

(ii) Socio-economic Group Differences in 1nf;int Mortality in Ireland . . . . . . ...
( I ) h e Characteristics of Mothers in thrce Dublin Maternity tiospitals . . . . . .
(iv) A Study of the Maternity and Infant Carc Scheme . . . . . . . . . . . . ...
( v ) The Dublin Neural 'Tube Defect Study.
6 . European Economic Community Studies: (i) C:onccrtcd Action Project on Congenital
Mdforniations and Multiple Births ... (ii) Accurate Certification and Registration of
Ilcaths ... . . . . . . . . . . . . . . . (iii) Respiratory Disorders in Agricultural
Workers ... . . . . . . . . . . . . (iv) Farmer's Lung in Coastal and Mountainous
Areas ... . . . . . . . . . . . . . . . (v) Evaluation of Farmer's Lung Campaign
(vi) Natural Background Radiation and Cancer Mortality in Ireland ... . . . . . . ...
7. The Sudden Infant Dcath Study
8. Sclf-discharge from Irish General ~ o s p i t a f s 1078 ... ... . . . . . . . . . . . . ...
9. Cancer of the Colon and Rectum
10. Multiple Sclerosis . . . . . . . . . . . .
11. Five Chinese Doctors visit Ireland . . . . . .
12. Conclusion
Publications 1980 . . . . . . . . . . . . ...
Expenditure
The total expenditure by the Medico-Social Research Board for year ending 31st December, 1980 was £503,000.
6

Many studies have shown that socio-economic factors play the principal role in health; the better off are healthier, suffer from fewer discascs and live longer than the poor. This is true of some of the major causes of ill-health in our society, such as heart attacks, a number of important cancers, for example lung cancer, high blood pressurc and stroke.
Despite the remarkable improvement in the stanciard of living of the Irish people during thc past 20 years the unequal distribution of wealth continues to be reflected in the notion's health. Good housing is a pre-requisite for healthy living and great strides have been made in the provision of local authority and private houses. A relatively high percentage of our people own their own houses. However, too many young and disadvantaged families still have to wait too long for a home of their own. The rcsulting overcrowding creates family and community stress. Certain sections of our society, such as the itinerants and some of the elderly, still experience real poverty. Unemployment, aggravated by the world recession, remains a national problem. Ironically, the greater involve- ment of the State in job provision has created an iinforcseen drawback. Those in secure, guaranteed employment now cost so much to maintain that little remains in the national purse for the unemployed and the unemployable.
After social inequality and the effects of relative poverty, perhaps our greatest and increasing problem is drug addic- tion. The amount of alcohol consumed in Ireland has doubled since 1970 and alcohol abuse causes an immense amount of misery and ill-health. Admissions to our psychiatric hospitals for alcoholic illness have increased from 619 in 1962 to 7,293 in 1978. So far wc have made little impression on cigarette consumption in Ireland which is, in fact, increasing in women and the young. It is a major cause of death below the age of 65.
The Hospital In-Patient Enquiry Scheme remains by far the largest part of the Board's work as far as staff and
7

expenditure are concerned. The projected coverage of the scheme is now almost 90% and in thc North-Eastern Health Board arca close to 97%. Over 91 research projects based on the information from this confidential scheme were under- taken in 1980. Complete confidentiality is maintained and no names or addresses go on thc computer. In this report, Mr. John O'Gorman, the Secrctary of the Board, who is in charge of the Hospital In-Paticnt Enquiry Scheme, gives an account of its progress.
Under the direction of Dr. Dermot Walsh, the scnior psychiatrist in the mental health section of the Board, many studies on mental health in Ireland are being undertaken. This section is responsible for the National Psychiatric In- Patient Reporting System which reports on all patients dis- charged from all psychiatric hospitals and units in the coun- try. Other studies include the three-county psychiatric case register, the three-county schizophrenia study, the study of the health services in pilot study areas and studies into special problems such as alcohol-related disorders, unmarried par- ents and their children, suicide and attempted suicide and the community care of discharged psychiatric patients. Dur- ing 1981 a census of all patients in psychiatric hospitals will be undertaken by the Board at the same time as the general census on April 5. i
A study of all first admissions to psychiatric hospitals in south-east England, comparing the United Kingdom-born with immigrants from Ireland and other immigrants was completed in 1980.' In the past studies on admissions to psychiatric hospitals in England have suffered from the prob- lem that in more than 30% of admissions birthplace was not noted. The Board undertook this study, in collaboration with the Department of Health and Social Security of the United Kindgom, based on all admissions to psychiatric hospitals in south-east England during 1976, that is in a population of 15 million people. A special effort was made to make sure that birthplace was noted and this was achieved in over 91% of admissions. A full report will be published in 1981 ."I At this stage it could be mentioned that the commonest reason for admission among Irish-born males in south-east England was alcoholic psychosis and alcoholism, although the admission rates for alcoholism were not as high as occur in the Republic of Ireland.
Dr. Michael Mulcahy continued studies on the major prob-
8

lem of mental handicap in Ireland. Thesc included studies on the prevalence and care of thc mentally handicapped, the preparation for a census of the mentally handicapped in 1981, and a survey of adult mentally handicapped persons living in the community. Nineteen eighty one is the year of the dis- abled and the Board will mark thc beginning of the year with a symposium on the care of the mcntally handicapped.
Dr. Peadar Kirke continues his studies on perinatal and child health. He has submitted reports for publication on perinatal and infant mortality in Ireland and other selected countries arid continues studies on the socio-economic group differences in infant mortality in Ireland, the characteristics of mothers in thrcc Dublin maternity hospitals and a study of the maternity and infant care scheme. Spina bifida and anencephalus are two of the most important congenital abnormalities occurring in ncwborn babies. These two con- ditions are more common in Ireland than in other countries. Recent research evidence suggests that it may be possible to reduce the chances of such abnormalities occurring by giving the mother certain vitamins before she becomes pregnant and during the first few months of pregnancy.' A group of Dublin doctors has estabfished a committee to undertake a study of this problem based on mothers at high risk of having a baby with a neural tube defect attending the four main Dublin maternity units. The Medico-Social Research Board ' is taking part in this study and Dr. Kirke has been asked by the committee to direct it.
At the request of the previous Minister for Health and Social Welfare and present Taoiseach, Mr. Charles J . Haughey, T .D. , the Board is undertaking a study on the very important problem of sudden infant death or cot death. Great interest in this problem has been stimulated in Ireland by the Irish Sudden Infant Death Association. Sudden infant deaths in Dublin city and county are the commonest cause of death between one week and one year and account for 38% of these deaths. They occur slightly more frequently in the winter months than in the summer. Each death is fully studied and autopsies are undertaken on all deaths, the majority by Dr. Seamus Cahalane of the Children's Hospital, Temple Street, Dublin. In 1981 the scope of the pathological inves- tigation into these deaths will be enlarged. Sudden infant deaths are also of great interest to the Committee for Medical Research of the European Economic Community and will be
9

included in the projected five-year programme of research by the Committee of Mcdical Rescarch (CRM).
In the 1979 Annual Report a description was given of the greater than expected nu~nbcr of deaths from cancer of the rectum that occurred in blue-collar workers at a Dublin brewcry. The study of thc brewcry workers has stimulated anothcr study comparing the background history. occupa- tion, diet, ctc. of patients with cancer of the colon and rectum with suitably chosen controls. This study is taking place, under the direction of the Director, in London by Dr. Kieran Moriarty and in Dublin by Dr. S h a m O'Neill and Dr. Kevin Ward and should be completed in 1981.
The Director of the Board has becn a member of the Specialised Working Group in Epidemiology of the Euro- pean Economic Community since 1973 and during 1980 he was elected Chairman. H c attends not only the meetings of this g~.oup but a number of other E E C research committees including the Committee for Medical Research (CRM) and has taken part in the planning of the five-year programme of E E C research for 1982-1987. The Board is taking part in a number of important E E C studies. These include a study to improve certification and registration of deaths in the coun- tries of the European Community. Death certification is the most important single source of information about hkalth that is available. A pilot study was undertakcn in 1981) in which 10 doctors in each of the countries of the E E C were asked to complete death certificates after studying 10 stories, or protocols, describing illnesses that lead to death. This was achieved in all the countries; in Ireland all 10 doctors asked to collaborate with the study did so. Some major differences were found in certification and coding between the countries of the Community. The Director is a member of a core committee of three, representing Ireland, England and France, which will organise a larger study on death certifi- cation in 1981 in which at least 50 doctors in the countries of the Community, chosen at random, will complete death certificates after studying 10 different stories of illnesses that lead to death.
The Medico-Social Research Board is taking part in a number of other E E C studies. For cxample, Dr . Alicja Radic is in charge of an EEC concerted action project to register all congenital abnormalities and multiple births. This is being undertaken in the Eastern Health Board area. Other E E C
10

studies are on respiratory diseases in agricultural workers, including farmer's lung, on the long-term effects of low dosage radiation and on multiple sclerosis.
Dr. David Nowlan, the medical correspondent of The Irish Times, suggested that a study should be undertaken on the reason why some patients discharge the~nsclves from hospital against medical advice. This study has bcen undertaken by Dr. Peadar Kirke and Ms. Teresa Brannick and a full report will be given in 1981.
In May 1980 the Board hosted a visit of five Chinese physicians led by Professor Deng Jia-dong, a hacmatologist and the Vice-President of the Chinese Academy of Medical Sciences. The group also included an orthopaedic surgeon, a general physician and two neurologists with a special inter- est in multiple sclerosis. This was a return visit following the invitation of the Chinese Academy of Medical Sciences to the Medico-Social Research Board to organise a visit by 10 Irish doctors to the People's Republic of China as guests of the Academy in 1976. The Chinese doctors visited the uni- versities and medical schools, hospitals, Guinness's Brewery and its medical centre and had a very full itinerary. They visited Dublin, Cork, Galway and rural areas of Ireland and gave a number of talks on medicine in China while they were, here. They were delightful guests.
The Director of the Board has long had his own personal, research interests and, in particular, he has continued research into the cause of multiple sclerosis, the commonest disease of the nervous system to affect men and women in the prime of their life. An account of these researches is described in this report.
It is not enough for the staff of the Board to undertake medico-social research into the major problems of Ireland. It is also of major importance that we collaborate with others in Ireland concerned with the medical and social health of our society, such as the Health Education Bureau, the Eco- nomic and Social Research Institute, the Irish Cancer Society and the Irish Heart Foundation. The members of the Board appointed by the Minister not only meet at the Board meet- ings with the Director to discuss and decide the various research projects of the Board but they also play a major part in facilitating the Board's research, representing as they do the major interests in medicine, economics and sociology in the country. The Board has bcen most fortunate in the
11

Chairmen chosen by the Ministers for Health since its foun- dation in 1965. The first Chairman. Professor Patrick Lynch, was the main inspiration of the Board in the early days. He was followed by two further outstanding Chairmen, Professor Thomas Murphy, now President of Univcrsity College, Duh- lin, and Professor Michael McCormac, Professor of Business Administration, University College, Dublin. No new Board members were appointed during 1980. The normal member- ship is 14 and it is hoped the Board will be brought up to strength in 1981.
It is the remit of the Medico-Social Research Board to study the most important medico-social problems of the country. This report describes some of the studies undertaken during the year.
R@rmces ' Dean. G. , Downing, H. and Shellcy, E. First admis\ians to psychiatric hc~rpitals
in South-East England. Immigrants from Ireland. Accepted for puhlicatim in the British Medical Journal.
Smithells, R.W. et al . Possible prevcritiun of neural~tuhs defects hy pr icon- ceptional vitamin supplementation. I.;!ncet, 1980,I. 339-340.

HOSPITAL IN-PATIENT ENQUIRY SCHEME
In our last report, coverage of the H.I .P.E. Scheme for 1980 was estimated at 353,000 discharges and at time of writing it seems likely that the target will be achieved or even slightly exceeded. During the year the Victoria and North Infirmary Hospitals in Cork, Shiel Hospital Ballyshannon and Doncgal District Hospital commenced participating in the H.I.P.E. Scheme and there was a significant improve- ment in the level of reporting in the South Eastern Health Board Area and to a lesser extent in the Midland Health Board Area. The overall performance in 1980 was satisfac- tory bearing in mind that because of economic stringency no additional clerical staff could be provided and shortages of clerical staff in other areas of hospital administration made it difficult to maintain the existing reporting structure for the H.I.P.E. Scheme.
The projccted coverage in 1981 is given in the following table.
TABLE I Estimated Coverag of H.I.P.E. Scheme 1981
Health Board
North Eastern Western North Western Eastern South Eastern Mid Wectern Southcrn Midland
NO. oi Estimetcd H.I .P.E.
Discharges* Surnmarics 1981 Expected % Covcmge
'Estimated discharges are based on 1977 data providcd by the Department of Health and 1979 data where available from other sources. District and Private Hospitals and maternity admissions are excluded.

We are now wcll on the way to full national coverage of the eligible hospitals and the only important areas which have still to be enrolled in the Scheme are the paediatric and gynaecologic;~l scctions of maternity hospitals and a small number of county and voluntary hospitals. Any additional staffiug resources which can be provided during thc coming year will he concentrated on these areas.
During the past year modification of our computer systems was completed in preparation for the introduction of the Ninth Kcvision of the International Classilication of Diseases on 1st January 1981. Another system development of interest is that from 1st January 1981 the Federated Dublin Voluntary Hospitals will produce the basic information required for the H.I.P.E. Schcmc as a by-product of thcir own computcrised hospital in-patient system. The data will be submitted to the Medico-Social Research Board on magnetic tape instead of on hand written summaries as heretofore. This development is of considcrable interest to the Board and the experience which will be gained from it will he invaluable whcn similar arrangements with tlealth Boards and other hospitals are being considered in due course.
As usual, diagnostic and surgical indices and other routine statistics were issued during 1980 to all participating hospitals and, in addition, special analyses were provided on request; to the following:
Hospitals 25 Individual Doctors 3 1 Department of Health 10 tlealth' Boards 4 Universities 2 Miscellaneous 19
-
91
The topics covered by these analyses included:
(a) An examination of the trend towards increase in hospitalisation
(b) Pattern of admissions of non-Dublin patients to Dublin hospitals

(c) Cross-checking of the incidence of hospitalised men- ingococcal meningitis as reported under the Inlec- tious Diseases Regulations.
(d) Incidence of various methods of prostaleclomy
(c) Reported incidence of aplastic anaemia and familial type malignant lymphomas.
We are very ple;~scd lo sce the I-1.I.P.E. Scheme being utilised in this way and we hope there will be increased use of thc data by doctors and administrators. The Board will gladly supply special analyscs on request and except where the cost involved in their preparation is significant they will normally be provided to users free of charge.
The processing of the 1979 H.I.P.E. tile is now almost completed and some of its main characteristics are givcn in the following tables.
TABLE 2 H.I.P.E. 197%l)ircharges hy Age, Sex and Avrragc Stay
A s -
< 1 1-14 15-24 25-44 45-64 65-74 75+
To ta l s -
Nu. olMalcs Av. Stay L No. of Females Av. Stay
I
TABLE 3
H.I.P.E. 1979-Discharges by Age and Marital Status
Married
Total 141,721
Widowed Oiher Unknown --CC
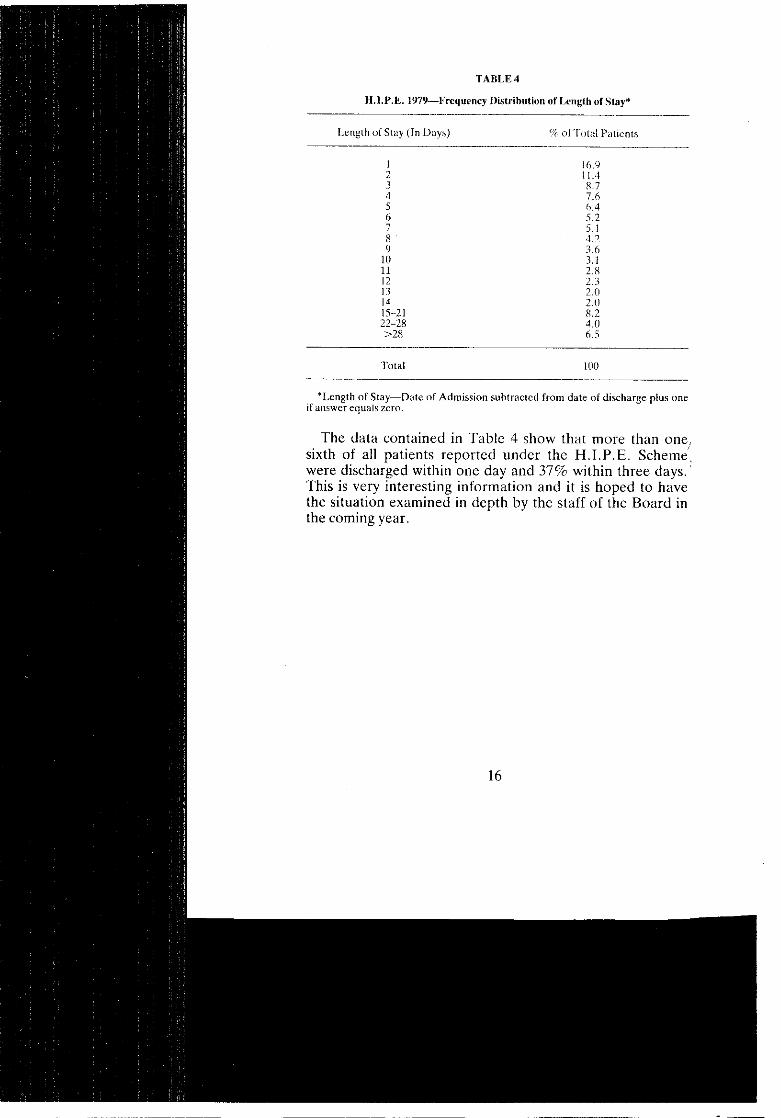
TABLE 4
H.I.P.E. IY7GFrcquency 1)istrihation of Length of Stay*
'Length of Stay-Date of Admission subtracted from date of discharge plus one if answer equals zcro.
The data contained in Table 4 show that more than one: sixth of all patients reported under the H.I.P.E. Scheme, were discharged within one day and 37% within three days. This is very interesting information and it is hoped to have the situation examined in depth by the staff of the Board in the coming year.

NATIONAL PSYCHIATRIC INI'ATIENT REPORTlNG SYSTEM
We continue to puhlish mni~al ly extensive data on in- patient ~novement in psychiatric 11ospitals and units. The latest in the series appeared towards the end of 1980. This was "Activities 01: Irish I'jychiatric Hospitals and Units 1978". As usual, in ndtliiion to ihc published data, more detailed infomr~tion I S been sent to individual liealth Boards and Iltrspitals wr~cerning their own activities.
We reported last year that the I977 data indicated a decrease in numhers of admissions over the preceding years. - . I his wab the lirst t i ~ i i c : rhis h x l happened since 1946 and we expressed the hope t h d i t was the beginning of a trend. if so, it would i~:ivc suggc\tCtl tlxrt the incrc;~sing provision of ccrn~munity ciltclm~tic~s 10 Impitalisation had succeeded in stemning the conti~iuing nurnhers of admissions. Unfortu- nately, thc 1978 report made ii clear ihat this was not the c s e , the numhcrs of :~ilinis<ions lor 1978 rose substantially over 1977 and more th,~n t.)llsct the decrease of the preceding year. I n 1078 there were 1.277 additional admissions repre- senting a 4.8% in~:se:isc 4nce 1977. Virtually all the increase in admissions WI:. ;iccounted !or by alcoholism (41% increase) and ncurusi.s (48% iricrc;~se). It is necessary to question wheiher sclrne of thcsc xirrlissions could not have been dealt with on an out-paiicrrt basis.
1;irst admissions ;rctu:~lly ciecl-eased in 1978 compared with 1977. All vf this dcc~-~; ise w x due to a fall in female first admissions while in;de firs! :idmissions increased very slightly.
As a result of the Increase in total adniissions in 1978 the number admitted to !rospit;~l, 27,662, was the highest ever recorded.

3 (ii)
DETERMINANTS OF OUTCOME OF SEVERE MENTAL DISORDERS
Since 1977 we have been participating in an international co-operative study entitled "Determinants of Outcome of Severe Mental Disorders". This project is being co-ordinated by the World Health Organisation and is being carried out simultaneously and with identical methodology in a number of psychiatric centres in the world. These are Nottingham in the United Kingdom, Moscow in the USSR, Prague in Czech- oslovakia, Aarhus in Denmark, Cali in Colon~bia, lbadan in Nigeria, Agra and Chandigarh both in India, Hawaii and Rochester in the United States, ~ a g a s a k i ' in Japan, and Dublin.
The study has a core element which is common to all participating centres. It is concerned with trying to establish with scientific reliability the incidence of schizophrenia in each of the centres. Associated with the core project are a 1
number of sub-studies in which one or more centres are : participating. The Irish centre is participating in what is entitled the "Disability Sub-study". This is concerned with measuring through the use of standardised schedules, the extent and quality of impairments and disablements as they arise over time.
From our base study population two annual cohorts of schizophrenic patients were selected, 1978 to 1979 and 1979 to 1980. Each of these group of patients is being followed-up for two years to study the extent of impairrncnt and disability in these groups and the factors responsible.
This study is of particular interest in the Irish context because of the suspicion that, compared to our European neighbours, recovery from schizophrenia is less complete in Ireland. It is, therefore, of importance for us that we study this matter in detail and identify the factors, social and otherwise that appear to inHuence the progress of this illness.

3 (iii)
THREE COUNTY PSYCHIATRIC CASE REGISTER
As detailed in earlier annual reports this register together with the St. Loman's psychiatric case register in Dublin, covers psychiatric services provided to over one-tenth of the Irish population. 'The data from the register complement the information available on inpatients from our annual "activi- ties" and our censuses. They provide the only reliable and detailed data concerning the activities of our psychiatric services outside the hospital and are: therefore, of consid- erable value to our national and local planners in thc health field. For this reason they should be continued. We are grateful for the support, financial and otherwise, afforded to us by the relevant Health Boards and their staffs to enable these joint endeavours to continue.
Some data from the registers have already been published on the treated prevalence of mental illness in Ireland.
/ "One-day prevalence" figures from the Three County Psy- chiatric Case Register were compared with similar data from the Camberwell Register. The findings showed much higher contact rates for Irish patients, particularly for schizophrenia. The first three year data on incidence and prevalence for the register will shortly be published. While we are aware that high prevalence rates in Ireland are partly explained by social, economic and demographic factors, we await with great interest the findings concerning incidence.

THREE COUNTY SCHIZOPHRENIA STUDY
As reported last year our earlier study of schizophrenia in three Irish counties has now been completed and we will shortly be publishing the results. It will be remembered that it was concerned to establish the incidence of mental illness and the incidence and prevalence of schizophrenia using standardised clinical and other techniques. It was also con- cerned with gathering social and cultural data concerning the early life experiences of patients and their performance in certain important areas of function compared with matched controls.

MENTAL HEALTH SERVICES IN PILOT STUDY AREAS (WHO STUDY)
Our participation in this collaborative international study was initiated at the instigation of and is being co-ordinated by the European Regional Office of WHO. The study, which is basically concerned with measuring the extent, usefulness and efficiency of psychiatric services has been carried out in our psychiatric case register area based on the St. Loman's catchment region of Dublin city and county. The first phase of the study which was completed in 1979 was concerned with a census of patients in care. The second phase was dedicated to the follow-up of a consecutive series of out- patients to establish the length of contact that they had with the psychiatric services following intake. This has now been completed and this group of patients is being followed for a further year.
/

3 (vi)
THE 1981 PSYCHIATRIC HOSPITAL CENSUS
In 1963 and 1971 censuses of patients resident in Irish psychiatric hospitals havc been carried out and the findings have been published.'.' Because it is now ten years since our last census, and because no detailed information has been available on resident patients since 1971, we have decided to carry out 'a census of these patients on the 31st March, 1981. This will coincide with the 1981 Census of Population. The main demographic parameters i.e. age, sex and area of residence will be available from the population census to enable us to publish the psychiatric census without undue delay. It seems clear however that such parameters as socio-economic group will not be available in time for the publication of our census. They will, therefore, have to be published separately.
Reference5 ' Walsh, D. (1971). The 1963 Irish Psychiatric Hospital Census. The Medico-
Social Research Board. ' O'Harr. A. and Walsh, D. (1974). The Irish Psychiatric Hospital Census 1971.
The Medico-Social Research Board.

3 (vii)
ALCOHOL-RELATED PROBLEMS Our activities in the ficld of alcohol consumption and
alcohol-related problems continue. These proceed on a very broad front and we have rccently joined the Irish National Council on Alcoholism and thc Health Education Bureau in a tripartite committee to disseminate accurate information concerning alcohol consumption and indicators of alcohol- related problems in this country. Bccausc of the considerable increase in alcohol consumption and in alcohol problems in recent years in Ireland the importance of providing reliable information as a basis for public education and prevention policies has been increasingly recognised.
The final meeting of the participants in the "International Study of Alcohol Control Experiences" takes place in Toronto in Spring 1981. From this meeting will come a joint publication on alcohol control experiences compiled by the Finnish Foundation for Alcohol Studies, The Addiction Foundation of Canada, The Social Research Group, School of Public Health of the University of California, The Neu- ropsychological Institute of Poland, The World Health Organisation, The Economic and Social Research Institute of Ireland and the Medico-Social Research Board. 1
Together with the coroners for Dublin city and county and County Kildare we are investigating the contribution of alco- hol to road accident fatalities.
It is hoped to obtain support for a study of children born to alcoholic mothers because of the recent reports of an increased incidence of congenital malformations among such children. Ireland 1967-1978. First and All Admissiuna fur Alcoholism and Alcoholic Psychosis
Year 1967 .. ... . . . . . . . . . 1968 . . . . . . . . . ... . . . 1969 . . . . . . . . . ... . . . 1970 . . . . . . . . . . , . . . . 1971 . . . . . . . . . . . . ... 1972 . . . . . . . . . . . . . 1973 . . . . . . . . . . . ... 1974 . . . . . . . . , . ... 1975 . . . . . . . . . . . . 1976 . . . . . . ... . . . ... 1977 . . . . . . ... . . . 1978 . . . . . . . ...

REPUBLIC OF IRELAND 1 9 6 1 - 1 9 8 0
CONSUMPTION O F BEER AND S P I R I T S PER PERSON
AGED 15 AND OVER. L I T R E S / 1 0 0 % ALCOHOL.
- BEER
6 - - - - - S P I R I T S 4 9 % increase 4
0 5 - C 0 U
N 4 4 -
do 0 0 4 3 - ,/-- \ _---_-- '- 1 1 7 % increase rn a, . .- - h * cl 2 - - _ - - - 4 4 - - - - - _ - - _ _ _ _ - - C

3 (viii)
UNMARRIED PARENTS AND THEIR CHILDREN
Our close association with the Federation of Services for Unmarried Parents and their Children continues. As indi- cated in the report for 1979 a study was published on a survey of children in residential care in the Eastern and North Western Health Boards who had not been placed for adop- tion. The reasons why this was so were highlighted and it was found that the most substantial was that these children were legitimate and, therefore, under our existing laws can- not be placed for adoption. We havc supported the Federa- tion in their demands for the removal of this legislative ban which effectively, and to no purpose, denies legitimate chil- dren. who are otherwise suitable, the benefit of a family home and upbringing.
Continuing our policy of student support a social science student was employed during the summer of 1980. The project this year was to enquire into the reasons why the children of umarricd n~others are given up for care by their natural parent. Preliminary findings suggest that a deficiency of serviccs i.e. such facilities as creche, day centres etc., are relevant factors. In addition, however, the findings indicated that a much more complex situation exists than simply lack of physical facilities. Illness in the mother, psychological stress and strain, and general inability to cope with a variety of demands, taken in conjunction with inadequate physical facilities, emerged as some of the intertwined and interlock- ing reasons for incapacity to cope with the child. A detailed report will be published shortly.

We are initiatine this vear a studv of suicide with the
&y" trend in the basic demographic and medical character- istics of those completing suicide. This is felt to be particularly relevant as data from other European countries indicate an increase in suicide rates among young people. Any preven-
We are c o n h i i n g our studies into the phenomenon that has developed during the last 20 years of deliberate self- poisoning. In the United Kingdom and Ireland this phenom- enon is twice as common in women as in men, particularly in
deliberate self-poisoning in a year, fortunately very few die because the drugs that they most frequently use are the tranquilisers and, luckily, it is difficult to achieve death with these drugs. Deliberate self-poisoning is generally a cry for help rather than a real attempt at committing suicide and
attacks.
from France, ~ e r m a n y and Italy that the; had the same Droblem of deliberate self-~oisonine as occurred in the
tion with Dr. A.M. Adelstein, the Chief statistician of the Office of Population Censuses and Surveys, London, and Dr. Johannes Mosbech, KAS Gentoffe, Hellerup, Denmark,

COMMUNITY CARE OF DISCHARGED PSYCHIATRIC PATIENTS:
AN EVALUATIVE STUDY OF AFTERCARE
This study is complete and has been submitted for publi- cation. It is a study of the aftercare received by psychiatric patients following their discharge from hospital. It involved not only study of the amount of care received by discharged patients but also of the pattern of usage of various aftercare facilities such as day-centres, outpatients clinics and hostels. It also looked at the work of community nurses and psychi- atric social workers.
The results show that the delivery of aftercare is not random but determined by various patient clinical/social characteristics. The results also raise questions concerning patterns of hospital admission, geographical planning of com- munity facilities, role of family doctor in aftercare and the comparative neglect of patients assigned to specific diagnostic groups, following their hospital discharge.

3 (xi)
FIRST ADMISSIONS TO PSYCHIATRIC HOSPITALS IN SOUTH-EAST ENGLAND:
IMMIGRANTS FROM IRELAND
The high admission rate to psychiatric hospitals of the Irish in lreland has prompted a study on first admissions to psy- chiatric hospitals of Irish immigrants in South-East England. This study has been undertaken in collaboration with the Department of Health and Social Security of the United Kingdom and with all the psychiatric hospitals and units in South-East England.
The 1971 census of population was used to calculate the Irish population at risk by age group. In 1971 there were 146,005 male and 173,450 female immigrants from the Republic of Ireland and Ireland, part not stated, resident in South-East England. Between 1971 and 1976 there was a slight fall in the Irish-born population because of diminished emigration from Ireland and because of an increase in the number who returned to Ireland as is shown by the Irish 1979 census.
An expected number of admissions to psychiatric hospitals was calculated for the Irish immigrants living in South-East England based on the United Kingdom-born admissions in each age-group, sex and diagnostic category. Expected admission figures, using the age and sex specific first admis- sions to psychiatric hospitals in Ireland, were also calculated. A similar theoretical number of expected first admissions was derived for males and females from Northern lreland based on the admissions of those born in any part of the United Kingdom and living in South-East England. In the past birthplace was omitted in more than 30% of all admissions to hospital in South-East England but as a result of a special effort in 1976 birthplace was included in over 91% of all first admissions.
This study has now been completed and is awaiting publi- cation. The largest diagnostic categories for the United King-
28

dom for males were personality and behaviour disorders and psychoneuroses and for females the highest first admission rates were for psychoneuroses and senile and pre-senile psychoses. Among the male immigrants from Ireland and migrants from Northern Ireland alcoholism and alcoholic psychosis was the largest category for first admissions. Admissions for schizophrenia for both males and females were also high among the Irish immigrants.
Rt,ference ' Dean, G., Downing, H. and Shelley, E. First adrnissionsto psychiatric hospitals
in South-East England: Immigrants from Ireland. British Medical Journal. In prcss.

MENTAL HANDICAP - PREVALENCE AND CARE
It is essential for rational planning of services for the mentally handicapped to consider whether the prevalence of severe and moderate mental handicap is increasing or decreasing. There are in fact two opposing theories as to changes in the prevalence of the lower categories of mental handicap. On the one hand is the steady state theory which postulates that there is a fairly constant overall prevalence rate which has been reported variously at between 2.9 to 3.4 per 1,000 of the total population.' The other theory is that there is a steady fall in prevalence due to modern advances in prevention.
Even small variations in prevalence, however, are impor- tant when one considers the implications both financial and in human terms of the birth, care and management of a severely handicapped child. An effort to estimate future trends was attempted by a Working Party set up by the , Department of Health which reported during 1980.2 The Medico-Social Research Board was represented on this Working Party which devoted considerable attention to the factors which were likely to increase the incidence and the prevalence of mental handicap and other factors which would have the opposite effect. The Working Party's conclusion was that there was 'a reasonable expectation of a considerable decrease in the number of mentally handicapped children, accompanied by an increase which will continue for some years in the number of mentally handicapped adults'. The reason for the relative increase in the adult population is chiefly that the mentally handicapped now live longer because of better care. The Working Party was influenced in its expectations that there would be a fall in the number of mentally handicapped children by the supposition that there would be a fall in the incidence of Down's syndrome. This should hopefully result from the fall in the mean maternal age at birth, which has been happening for some time, since the risk of Down's syndrome is increased in the case of older mothers and fathers. There is some evidence to suggest that
30

there may be an increase in the actual number of Down's syndrome children being born to younger mothers but this would have a smaller effect than the high risk in older mothers, and indeed, whether there is a true increase in younger women.
The Working Party also considered thc question of resi- dential care and the indications for it. Its conclusions were that there were many handicapped persons in residential centres who could be maintained in the community if ade- quate day care facilities were available. This conclusion would seem to be borne out by some comparisons with Sweden where day facilities have been developed in recent years at a fairly extensive level.' The disparity between the two countries is very evident if children under 16 are considered.
TABLE 1
Number of menlally handicapped children in special residential sehcmls and centres. Ireland and Sweden 1977.
'% under 16 in special
All mmtally residential All mentally handicapped schoolsand handicapped I I under16 1 a n m s /
Ireland . . . . . . . . . 4,751 2,403 50.0
It seems clear that adequate day facilities can prevent o r certainly postpone admission to residential care. Whether in fact the children are better off or even as well off at home is not as easy to decide. Whilst in theory a child who is accepted by his family should be better off at home it does not necessarily mean that he o r she will be so. A t the clinical level one is familiar with some families who do not accept their handicapped child even when a comprehensive range of day services and other support facilities are available. However, the majority of severely handicapped children are accepted by their families and they benefit accordingly.
In the event the increased use of community care will probably be decided on financial grounds. There is an assumption, still also unproven, that residential care is much
3 1

more cxpensiw then community carc. As long as this assump- tion prevails health planners are likely to continue to foster the notion of community carc and the provision of every encouragement to enable ;I family to keep their handicapped child, and indeed adult. at home.
7'0 discuss these and other matters arising from the Work- ing Party's Report the Medico-Social Research Board pro- pose to hold a sernirlar entitled "Caring fol- Mentally FIand- icapped Persons - thc Way Forward'' early in 1981. At this seminar the rescarch work of the Hoard's section on mental handicap will be discussed and the implications of such research for the future will be con!;idercd.

4 (ii)
CENSUS OF THE MENTALLY HANDICAPPED
Thc standardised record system for mentally handicappcd persons was established in almost every Comrnortity Care Area of the country during 1980. Thanks to the enthusiasm and energy of staff at community care level the work pro- ceeded throughout the year. The willing assistance of the public health nurses ensured that the records for children were completed at en early stage. In this respcct considerable help was forthcoming from those public hcalth nurses who have assumed special responsibility for the counselling of parents of young handicapped children.
The returns from special residential centres were relatively easily obtained through the willing co-operation of the staff of those centres. With the exception of returns from one special rcsidential school for mildly mentally handicapped children the returns are now complete.
The main and continuing difficulty with the census lies with the problem of the adult mentally handicapped in the com- munity. Aside from the fact that many of these adults are receiving the:Disahled Persons Maintenance Allowance and a proportion:of them are attending a day service for the mentally handicapped little else is known of their condition and their level of functioning. Consequently it is likely that once again, as in 1974, the Census of 1981 will provide a relatively complete picture as regards children but gaps will still remain in our knowledge of the mentally handicapped adult.
During the year some Health Boards were concerned with producing their own reports on mental handicap services within their Board area. Whilst in general the figures from the 1974 Census' are still being used, in some Boards updated figures, provided by the setting up of the Record System are already becoming available. The recently published report by the South-Eastern Health Board on Services for the Mentally Handicapped is of interest in this regard.2 The figure quoted for moderately, severely and profoundly hand- icapped children, aged 5-19, is 616; using population figures from the 1979 Censusi this yields a rate of 5.5 per 1,000. In 1974 the equivalent figures were 554 children which yielded
33

a prevalence rate of 5.6 per 1.000 based on the 1971 Census of Popul;ilion."'l'l~ese preliminary findings lend weight to the theory that there is a fairly constant prevalerm rate for modck~te , severe and profound handicap and that observa- tions over a prolonged period will be necessary to detect important ch;~ngcs.
The last source of inhlrrnation for the record systcm will be returns l'rom psychiatric hospitals, residential homes and geriatric homes. These sources provide a significant number of nrcnlally handicapped persons. In 1974 33.7% of nlentally handicapped persons in residential care were accommodated in psychiatric hospitds and 2.1% and 7.0% respectively were found in residential homes and geriatric homes. During 1980 evcry psychiatric hospi~al was either visited or contacted and returns from many are already available. Returns from many uesidenti:rl homes are still awaitcd. All such homeshave been rcquestcd lo identify evcry mentally handicapped child within their population. Since geriatric homes arc well known to the local Dircctor of Community Care, the Directors have been asked to assess and record the number of mentally hrtntlicappcd placed in the geriatric homes in their area.
It is planned that the projected Census will take place in May and June of 1981. Indications arc that it will be fully comprehe&sive in most areas and offer interesting compari- sons betwekn urban and rural areas in different parts of the country.
Krjcrrtirm ' Mulcahy. M. The Pre\,nlencc of Mcntal Handicap in the Republic of lrelimd.
1974. The Mcdlcu-Social Research Board, Duhlio. Senices fur the Mentally Handicapped in the South-Eastern Health Board
Area South~Enslcm Health Ro:rd Rcsmnal Mcntal Handicap Cammittce, March 1980.
I Census of Popuialim of Ireland, 1'179. Govcrnmcnt Publications. Duhlin. ' Census of Population of Ireland, 1971. Government Publications. Dublin.

SURVEY OF ADULT MENTALLY HANDICAPPED PERSONS LIVING IN THE COMMUNITY
A survey of adult mentally handicapped persons living a home in two community care areas in the Eastern Board has been completed. The population in thls were mentally handicapped or suspected mentally capped persons, aged 15-64 years, who were resident m the areas at the time of interviewing and were attending a mental handicap, psych~atric or rehabilitation service or in receipt of a welfare allowance within the two year time span 1979- 1980. Every attempt was made to identify all mentally hand- icapped persons in the areas studied and a number of sources of information were used. A total number of 562 persons was identified (3.9 per 1,000 population). An ~nterview schedule of approximately three-quarters of an hour duration was completed with the primary caring person in 374 cases.
A recorded dia nosis was available for 92% of the survey B population; 73% had a diagnosis which included mental handicap while 19% had a recorded diagnosis other than mental handicap e.g. epilepsy, cerebral palsy, quadriplegia, paraplegia, hydrocephalus or visual and hearing disabilities. On the basis of level of skills and independence in salient areas of functioning measured in the survey, the population was subdivided into three groups; those functionmg at high levels of ability 2976, these persons had little difficulty in communicating with others, were able to look after their personal needs and were relatively independent; those func- tioning at low levels of ability 20%, this group was generally very dependent on others, had difficulty in communicating with others and needed assistance with personal needs and feeding or whose profile of ability was variable; 52% who subdivided into persons who needed assistance with their personal needs and those with interpersonal difficulties.
It is clear from the findings of this survey that we must develop our community based services further if we are to provide the necessary supports to mentally handicapped per- sons and their families to live a satisfactory life within the

ct)n~munity. Information collected on day services revealed that a high propol-tion (60%) were not attending day services or proti~~ctively occupied at thc timc of the survey. Some were happy to continue like this, for various reasons, while othcl-s wcrc looking for ;I tliffercnt day placctnent. 7'he findings point to the nccd for more apprtrpriatc day service provision for otlults liviug in the cotnmunity and in particular for those Functioning at high levels of ability many of whom wcrc looking for ci t l~cr short-term training or open employ- rnent hut who needed soi i~e supports to achieve this. At the social level. we need to look seriously at thc quality of life of mcntally handic:~ppcd pel-sons and at ways of involving them in social liCe outside of work and outside of the home envi- ronment. Inlormation collcctcd on survcy population's rec- reational activities showcd a dcarth of activities and a lack of integration within the local community. Long-term residen- tial care provision will or may be nccessary for 47% of the su:-vcy population and in 5 % of cases it was ~irgcntly required. Those requiring residential care can be subdivided into var- ious ability levels, also in terms of the type of care they would he rcquiring. As would he expected, thc majority of the low ability group (53%) anticipate the need for residential care whereas only 16% of the high ability group do so. In the high ability g o d p it was hoped that 30% would get a job and maintain themselves; this contrasted with 19t of the low ability group. Short-term or crisis care in times of illness or to give ;I family member ;I hrcak would be nvailcd of by 29% of rcspondents were i t available.
The findings of this study will bc published under the following titles:
Walsh, J . and Mulcahy, M. Service Kcquirements of Adult Mentally Handicapped Persons Living in the Community. In preparation.
McConkcy. R. and Walsh J. An Index of Social Conipe- tencc for Use in Determining the Scrvice Needs of Mentally Handicapped Adults. In preparation.
Walsh, J . and McConkcy, K. The Recreational Pursuits of Mentally Handicapped Adults. In preparation.
Walsh, J. and Mulcahy, M. Kesidential Care Require- ments of Adult Mentally Handicapped Persons Living in the Conmunity. In preparation.

4 (iv)
KEGIS'I'EK OF FEMALES OF CIIILDUEARING AGE WITH PHENYLKETONUKIA
Since 1957 when Dent' reported the birth of non-phenyl- ketonuric mentally handicapped offspring to a phenylketon- uric mother there has been consistently increasing evidence that persistent maternal hyperphenylalaninemia during preg- nancy is harmful to the foetus in the majority of cases.'
A study on the prevalence of phenylketunuria (PKU) in the Republic of Ireland in 1974, which was conducted by the h4edico-Soci;1l Kesearch Board' highlighted the prohle~ns posed by the increasing number of PKU females at risk of having a child with congenital abnormalities andlor brain damage. In view of this risk it was decided, in 1978, to establish a Register of Females of Childbearing Age with PKU. Such a register is particularly relevant in Ireland because uf the known high prevalence of PKU.' The proce- dures involved in the setting up of this register have already been reported.'
Arrangcments were completed at the end of 1980 for the transfer of the Register to the Children's Hospital, Temple Street. At thc time of transfer 35 females with PKU, born prior to the commencement of the National Screening Pro- gramme in 1966 and living in the community, had been identified. Since nine of these were severely or profoundly mentally handicapped the remaining 26 were identified as the population at risk for maternal PKU. At the request of the treating paediatricians four of this group were not con- tacted and, therefore. at the time of transfer of the Register to the Children's Hospital, Temple Street, 22 persons in the at risk age group had been contacted. The dictary status and intellectual level of those contacted is presented in Table 1.

TABLE 1
MaLcr~tiil phenylkctm8uria population: Dietary stalwa at time of rentact rclated to intelleelual functioning.
(1) The ages of those contacted ranged from 12 to 30 years when first contacted (1978)
(2) Of the nine girls on dict at the time of contact, six were being treated at thc Children's Hospital, Temple Street, two at the National Children's Hospital, Ilar- court Street and one at Our Lady of Lourdes Hospital, Drogheda.
I (3) Five girls had bcen on diet in the past, two up to the
age of I 8 and the other three up to the age of five or six.
(1) Eight girls had never been on diet.
Of the 13 who were not on diet when contacted, three were moderately mentally handicapped and on evaluation of their social and familial situations were not considered to be at risk of pregnancy. Five of the remaining ten had started diet at the time of transfer. In four cases the diet was introduced for the first time and in the other diet was resumed at the age of 20 after a break of 14 years. The ages of the persons commencing the diet were 13, 16, 20 and 22 at the time of commencement. Of the five persuns who did not start diet, two had previously been on diet and the others had siblings who had been or are still on diet. With all of them the crucial importance of commencement of the diet prior to pregnancy has been discussed on a regular basis. In two cases
38

it is confictently expected that the special diet would be commenced prior to pregnancy. Ijowever, in the other three it is fclt that commencement of the diet may present problems and that regular contact with these families will be esscnti;il.
For the Suture it is proposed that contact will he maintained with tlie women concerned and h e i r families hy :I social worker from the Children's Hospital, Temple Stret'! w o r k i ~ g in co-operation with Dr. Doreen Murphy and the mztaholic unit attached to the hospital.
K ~ J L ~ ~ w c P , ~ ' l lent. C .E. Discussion of Armstrong MD: Kcliilmn 01 hiochemiciil :ibiio~m:tl~ty
to dcvclopmcot of mental defect in phcnylketuni~riit. E t i i ~ h ~ i c lactors in muntal ret;>ldalinn: Report oitwenty-third Ross PeJi:~tric Kescarch Crmicrcncc. Nwcmhcr 1416. Columbus, Ohio: Ross L.aboratortes. 1957.32-2.
-1.crikc. R.R. and Levy, H .L . (I9Nl). Matrrnal Phcnylkrlonuria and Hypcr- phcnylalaninaemia: An inlernation;d survcy of the outcome 01 u~~t rca lcd and treiilcd pregnancies. New England .Journal of Medicine, 303, 1202Xi
'Childwick, G. . Cahalane. S. and Molcahy. M. (14771. Phenylkctonuria in the Rrpublicuilrcli~nd, 1974. Irish Mzdic i Journal, 70,211.612,
'Cahalane, S. (1908). Archives of Disease in Childhood. 43,141 5Medico-Sorial Research Board. Annual Report, 1'179.

Perhaps tlw nmin featurc o l t h c last two decades in relation to malernity services has bcen the general recognition of the itnpor-t;rnce of pc-rinalal nlortality and morbidity. Interna- tional comp;~risons o f secular trends in perioatal and infant ~nor td i ty can he usel'ul as a starting point for evaluation studies of perinatal health and perinatal health services in a country. I'atterns of pcrinatal :lnd infant mortality were comparcd for Ireland and other countries in two papers'.? which have heen submitted fur publication.
In the first paper' present level5 and secular trends in perinatal and infant mortality in Ireland were considered in the light of the experience of other selected countries --Sweden. 1:iriland. Japan and the countries of the European Economic Community. Trends in infant mortality were con- sitlered for thc period 1960 to 1976; in the case of perinatal mortality the exarninarion was confined to the years 1966 to 1976 as national statistics o n late foetal mortality (a compo- nent of per-inatal mortality) ;Ire available for Ireland only since 1966.
There were ~nal-ked differences between the countries in pe r ina l~~ l mortality. The rates for Sweden, Finland, Den- niark, the Nctllerlilnds and J a p a ~ ~ were the lowest in the world. The Kcpublic of 1rcl;ind's rate of 19.7 per 1000 total births in 1976 was exceeded only by two of the fourteen countries in the study, Northern Ireland and Italy. Mortality in the Reput~lic of lrelmd Sell less rapidly between 1966 and 1976 than in most of the countries. The contrast was most marked between the Republic of Irelencl and Scandinavian countries. Between 19'70 and 1976, for example, perinatal rnort:ility fell by 19% in lreland compared with 35% in Swcden. i n Figure I the perinatal mortality ratcs for some of thcse countries are plotted on a vertical logarithmic scale to illustrate more clearly the rate of decline in mortality. Between 1956 and 1970 the rate of decline in perinatal
40

mortality in Ireland was similar to the Swedish experience and greater than the fall in Northern Ireland and England and Wales. In the Republic of Ireland the rate of decline slowed since 1970, the slope of the graph being less steep than for England and Wales, Japan and Sweden. The Figure illustrates the considerable difference in the rate of fall in mortality during this period between Japan and Sweden on the one hand and the Republic of Ireland, Northern Ireland and England and Wales on the other.
That trends in infant mortality in the study countries closely resembled those in perinatal mortality is not surprising in view of the fact that early neonatal deaths (deaths during the first week of life) account for approximately 50% of perinatal mortality and 60% of infant mortality in most of the coun- tries. Figure 2 illustrates how the infant mortality rate in Ireland fell steadily between 1962 and 1972 and more rapidly than in Northern Ireland, England and Wales and Sweden. The rates for Ireland and Northern Ireland remained almost static, however, between 1972 and 1975 while the downward trend continued in Japan and Sweden. The relatively slow rate of decline in mortality experienced by Northern Ireland and England and Wales between 1960 and 1975 is notable. As in the case of perinatal mortality (Figure I) , infant mor- tality fell considerabfy in Ireland and England and Wales in 1976. A strikmg feature is the rate at which mortality has fallen in Japan since 1960; the slope of the graph is steeper than for any other country.
In view of the slow rate of decline in perinatal and infant mortality in Britain and Ireland until 1975 relative to many other European countries, more recent trends merit com- ment. Between 1975 and 1978 perinatal mortality has fallen in England and Wales by 20% while infant mortality has fallen by 16% to 13.2 per 1,000 births in 1978. Provisional data on infant mortality only are available for Ireland since 1977 (the most recent perinatal mortality statistics relate to 1976) and on the basis of the rate of 14.9 per 1,000 in 1978, infant mortality has fallen by 15% since 1975, a rate of decline similar to that for England and Wales. The provi- sional Irish infant mortality rate of 12.4 per 1,000 for 1979 represents a dramatic 17% decline in mortality since the previous year. So while one must he cautious in interpreting the provisional Irish statistics, we may well he sharing the
41

recent British expcriencc of acceleration in the rate of decline in perinatal and infant mortality.
The perinatal and infant mortality rates for 1976 for the fourteen countries studied showed considerable diversity. The second papcr' attemptcd to identify rcasons for this diversity by examining inter-country differences in the main factors which influence rcproductivc health with spccial emphasis on biological and socio-economic factors.
Perinatal mortality rates arc oftcn incorrectly cited as if they were sensitive measures of the quality of perinatal health serviccs. It is tempting to attribute international variations in perinatal and infant mortality to variations between countries in the quality of perinatal and child health serviccs but many other factors require consideration first. The level of peri- natal and infant mortality in a country reflects a wide range of biological, socio-economic and environmental influences extending over the entire lifetime of the maternity population as well as the effect of health services. As doctors, we are particularly interested in the latter but the other influences may have a greater bearing on outcome. Due account must be taken of all such factors when the mortality experiences of different populations are compared.
Mothers aged 35 years or more, those having their fourth or later baby an& mothers with high levels of fertility have highcr than average risksof perinatal mortality. International studies show a strong correlation between the level of socio-economic devclopment and perinatal and infant mor- tality; the most developed countries tend to have the lowest mortality rates. Tables 1-4 (abstracts from more detailed tables in the papcr) illustrate Ireland's unfavourable position with regard to these factors. Congenital malformations pose a greater problem for Ireland than the other countries. For example, the first week death rate from congenital malfor- mations for the two year period 1974.1975 was 2.5 per 1,000 live births for Ireland, 1.9 per 1,000 for England and Wales and 1.4 per 1,000 for Sweden. Pcrinatal care around the time of birth car1 do very little to reduce mortality and morbidity from congenital malformations. Ireland is also at a consid- erable disadvantage with regard to other causes of perinatal and infant mortality in which socio-economic influences are believed to be important, for example. anoxic and hypoxic conditions, prematurity and respiratory diseases.
The unfavourable pattern of these factors in Ireland com-
42

pared with the other countries helps to put our relatively high perinatal and infant mortality rates in perspective. Thus it is likely that a sizeable proportion of perinatal and infant mortality in Ireland is determined by socio-economic and environmental factors and is, therefore, to a considerable cxtent beyond the scope of traditional medical care. Aware- ness of this situation is important, firstly, to prevent false expectations by both the profession and the public of what can he attained realistically in terms of reduction of mortality and morbidity by hcalth services alone and secondly, in order to allow the health and related scrviccs to he developed in the most appropriate manner to meet the particular needs of Irish mothers and their babies.
Assessing thc outcome of perinatal care is a complex exercise. Due account must be taken of the wide range of socio-economic, biological and environmental influences before the specific effect of medical care can be identified. The level of perinatal mortality depends greatly on the inci- dence of low birthweight and of congenital malformations both of which are determined by factors largely outside the scope of clinical intervention. It follows that if we wish to look at the performance of perinatal health services for different counrries or regions, we must compare birthweight - specific perinatall mortality ratcs for non-malformed babies. Such adjustments of perinatal mortality rates are precluded for Ireland by the absence of any population- based data on birthweight distribution at either the regional or national level.
The inadequacies of the routinely collected perinatal sta- tistics in Ireland are well known. The new Birth Notification System which is being introduced by the Department of Health is an important step in the right direction and it is hoped that this information system will cover all births in the country in the near future. The Director of the Hoard is a member of the Committee, chaired by Mr. Shaun Trant, which is responsible for introducing this new notification system. When full coverage is achieved, important basic infortnation such as population birthweight distribution will become available for the first time. The successful develop- ment of this information system is clearly an urgent priority for the obstetric and paediatric services. The studies ' .?have shown how unique Ireland is in many aspects of perinatal epidemiology. If the data collected by the Birth Notification
43

System prove to be complete and reliable, we may begin to understand the complex inter-relationships between socio- economic, biological, environmental and medical care factors and perinatal health as they opcrate in Ireland.
HeJer-c,,m I K i c k P. Rrannick 'r. Perinatirl and infant mmtality in Ircland and selected
countlies: prsscnt icvcls ;lnd sccuhr trends. (Submitted iorpuhlicntion Lrkh Mrdical Journal). ' Kiikc P. Pcrinat;il and infant mort;dity in Iceland and sclected countries:
variations in undcrlyinp T,iciur\. (Submitted far puhlication Irish Medical Joulnal) .
Pep. of
j C , - i'l. Lreland I. l r e i a n d - aJ - m 40 { ... I.. Enql rnd b - S w e d e n 0 10 Wales
F i g . 1: Per inate l mortali ty
r a t e s i n s e l e c t e d c o u n t r i e s ,
1966 - 1976.

Rep. of a-c-. Northern I r e l and lac I r e l and
- - - - - E n g l a n d & Wales - Sweden m
F ig .2 : I n f a n t mor ta l i ty r a t e s i n s e l e c t e d
c o u n t r i e s , 196b - 1976.

TABLE l
Percentage of live hirtlls to mothers aged 33 years sr mere in selected countries, 1971.
--- -- Rcpuirlic uf lrciimd .. Italy (1'174) ... . . 16.5 Wcst Gcrrnitny
12.6 . .
Deornaik . . 1 1 . 1
... . . . . . Sweden
5.1 ... . . . . . . .
Japan ... . . . ... 5.5
. . . ... ... 3.8 --
TABLE 2
Pcrccntage of live hirths of fourth or higher ordrr in seleetcd countries, 1975.
Republic of
Sweden (19- Japan [ " '7*
TABLE 3
Total fertility rates (average number of live births per I00 wumcn) for *elected eounlries, 1975.
, Republic of Ireland Nurthcrn Ire. '
Su West ti
I
Source: Pichat JB. Popululion 1976;31, 1041-97.
TABLE 4
Real Gross Domestic Product per capila* for srlcrted countries, I974 (L1.S.A. - 100).
France De 7..
'Real Gross Domestic Product (GDP) per capita=GDP per capita convcrtrd to dollars at purchasing power parity and exprrsscd as a ratio of U S A . GDP per capita.
Source: Kravis IB, Heston AW. Summers R. EcononiicJour,toi 1978; 88: 215~42

5 (ii)
SOCIO-ECONOMIC GROUP DIFFERENCES IN INFANT MORTA1,ITY IN IRELAND
Last year wc reported that we had commenced a study of thc association between infant mortality and socio-economic group (SEG) in Ircland for all births in the Irish Republic during 1976 based on the vital statistics birth and (first year) death registration data. Allocation to SEG is based on the occupation of the parent or guardian. One of the problems which we encountered was the large number of infant deaths, 212 of the 1052 (20'%), where it was no1 possible to allocate SEG due to the fact that parent's occupation was not recorded o n the death registration form. In contrast, SEG was known for all but 5 % of births, so we decided to try to trace the birth certificates or birth registration forms for the infant deaths where SEG was unknown in order t o establish the occupation of the parent whcre this was recorded. With the considerable help of the Central Statistics Office and the Registrar General's Office a birth certificate or birth regis- tration form was eventually traced for 196 of the 212 babies and parent's occupation was recorded for 135 o f these. Thus we now have the socio-economic group for 93% of the infant deaths during 1976.
The study is restricted to information recorded on the birth and death registration forms. From the death registration forms it is possible to study variations between the SEGs in neonatal, post-neonatal and infant mortality rates and in the causes of infant mortality. Birth registration data for 1976 allow us to examine soeio-economic group differences in maternal age and parity and - a particularly interesting variable - the proportion of previous children who were born alive but who died before the time of registering the baby born in 1976. These data are bcing currently analyscd and the findings will be published in 1981.
This is the first time that the association between infant mortality and socio-economic factors has been explored for the entire population of the Irish Republic. The study would not have been possible without the help of the Central Statistics Office and the General Register Office for which we are especially grateful.

5 (iii)
THE CHARACTERISTICS OF MOTHERS IN 'I'HKEE DUBLIN MATERNITY HOSPITALS
The three largc Dublin maternity hospitals, thc Cnomhc, National Maternity and Rotunda. occupy a prominent place on the Irish obstetric scene. Important among the reasons for this is the fact that some 22,000 births or 31% of the total births in the country currently takc place in these hospitals. In vicw of the dearth of basic, relevant and up-to-date statis- tics relating to perinatal health in Ireland, the Annual Reports of thcse hospitals which are generally published within nine months of the end of the ycar to which thcy refcr, provide much useful information for those interested in the health of pregnant mothers and their babies.
Thc level of perinatal mortality and morbidity in a hospital population or a geographically defined population rcsnlts from a wide variety of interacting influences including socio-economic, biolo/gical and mcdical care factors. Diffcr- cnccs between hospitals in pcrinatal mortality and morbidity rates might be due to differenccs between the hospital p o p ulations in such factors as socio-economic status, maternal age and parity, marital status, previous obstetric history, incidence of congenital malformations etc. and due account must be taken of thcse differences before examining hospital variations in the pattern of perinatal care.
With the co-operation of the Masters of the hospitals, we decided to carry out a descriptive study to determine the extent to which the maternity populations of the three hos- pitals were comparable in terms of certain socio-economic and biological characteristics known to influence reproduc- tive performance. The study is particularly concerncd with the socio-economic group distribution of the hospital popu- lations but we are also documenting the age, parity, marital status and area of residcncc (postal area for residents of Dublin city and county, and county for residents outside I Dublinj of the mothers.
A systematic sample of the mothers who gave birth in each
48

hospital during 1979 was taken and resulted in a total s;lmple size o f 900 mothcrs. Under the supervision of Ms. Teresa Brannick and Dr. Pcadar Kirke, the required information was abstracted from the charts of these mothers by two social science students, Ms. Moira Leydon and Ms. Clodagh O'licilly.
The opportunity was taken to collect information on the following variables: birthweight, gestation, previous history of pregnancy loss (abortion, miscarriage, perinatal death); maternal height, smoking during pregnancy, method of infant feeding, duration of marriage, and stage of pregnancy at first visit to the hospital antenatal clinic. The differences between the hospitals in these variables and also in the association hctween these factors and socio-economic group are being studied.
Because of the paucity of published informatior1 on the extent to which Irish mothers utilize antenatal care services, the use of antenatal care by mothers who had their babies in one of the Dublin hospitals, the National Maternity, during 1979 is being cxamincd. The aim of this small study is to describe and relate the mothers' socio-economic, dcmo- graphic and medical characteristics to their use of antenatal care in terms of stage of pregnancy at first antenatal visit to their general practitioner o r (he hospital and the total number of antenatal visits. We are particularly interested in looking at the characteristics of mothers who underutilized the serv- ice, i.e., mothers who attended late in pregnancy for their first antenatal visit and those who frequently missed sched- uled antenatal visits.
A one in twenty systematic random sample of 416 mothers was selected from the 8,361 mothers who had their babies in the hospital during 1979. The relevant information was abstracted from the mothers' charts and these data are cur- rently being analysed.
A sturly of the Malelliily and Inl'anL ( h e Schci~re (essen- tially th;it p r l 01. ohb i~ t r i c a n d ntm~:itnl care whicil is pro- vitlcd by gcner;11 {iract i t ionc~s for mothers eligible for the service) is at prcrclit 1)t:iiig untie~tal ten jointly by the Depart-
I merit o f IJcalth ; u d the Medico-Soci:~l Rese;~rch Board. T h e study is being supervised by a stceririg cornmittec which is reprewital ive o f the Dcl )ar tn~ent , the Medico-Social Research Board (Dr. Gcolfrey Dean). health boards and the medical and nursing professions. The 1n;lilr work of the study is being carried i)ol by Mr. Ronnie O'Srtllivnn from the Department of 1le:dth and Dr . Pc;~dar Kirke from the Medico-Social 1iese:trc.h Uu;rrd. The p u ~ p o s c of the study is I t o review the present operation of the Sclreme iticll~ding the objectives and in the light of the findings t o make recom- mendations for t11c future ~lrvelopincnt of this scrvice.
The corninittee wa.; fircccl with ;I very conlmim problem in such health service cv;lluation exercises - lack of basic relevant information. To assist the cornmittee in its deliber- ;~t ions, i t was decidtd t o k w d u c t ;I survey of all mothers who had give11 birth during a:specitied week. The items of infor- mation in the short siirvcy qucstionn;rire can be considered under three general 1ie;rdings: the characteristics of the rnother influencing her reproductive performance (e.g. age, parity, previous obstetric history), standards of care (e.g. gestation at first nntcnatal visit), and the mothers' views of their care (c.g. prefei-eirce for antenatal care from general practitioner o r hospital). 'This information will he examined for three groups of rnofhcrs. those eligible for the Scheme wllo availed of it and tlrosc who did not use it and mothers who were not eligible for the Scheme.
All mothers in the lrisli Republic who gave birth dwing the week 24th-30th Novcrnber, 1980 (expected to be approx- imately 1,390 inofhers) will be interviewed about 12 weeks after delivery by public healtti nurses who will complete a questionnaire for cnch mother. The main findings of this survey will be incorporated in the report of the steering committee and it is intentled at a later stage to report more detailed ;rspect5 of the studv.
50

Ncural trthe tiefccls (N7'I ) ) (mainly ancncephalus and spiu;~ iririti;~) arc ;I m;!jor cmrse of rnortalily and inott~itlity in infancy ;lnd bcc;ir~ee of the Iiigl~ indidcnce of tllcsc i t l l~~or- n~alitics in ircl;\n<l ielative to uthcr countries, we have a special 01-digatioi! to pursue any possibility of reducing this great I~urtlrm. ' l l ~ c r e i s ;I growingliody of evidence suggesting that ;I dietary int:ch;ruism may be inlportant iu the actiology of these congcuihl t~~il lfor~ri;~ti i)r~s and vit:~nrin deficiency iu the maternal ilict is curl-cutly receivir~g much attention. Lhr- ing the year a group of 1:)ul)lin doctors (Dr. I . 1)alrymple. I<crtuncla; Dr. N. J>uigrmn, (loomhe; Professor F,. C;uiuey, The Clrildl-en's liescarcl~ (:enlre, Crumlin; Dr. 7'. tlanr;~lty, St. Jarncs's; 1)s. 11. M;icDonald, National Maternity Hospi(al and Dr. P. Kirke, Medico-Social Rescirrch Bo;crd) came toeethe~- to consitlcr the cvicic!tcC iniplicating dietary factors
/ i n & rausatitrn of neural tobe defects (NTD) and to develop an appropriotc rcscarch strat'rgy. The group was joined by Dr. 1'. McC;irthy, a I-cse:~rch fellow with the National Keha- bilitation Board, Mr. L. Daly, a statistician from University College, Dublin and Professor H. Elwood from Queen's University, Belfast who is art authority on the epidemiology of NTDs.
After careful consideration the group has decided to con- duct a trial of vitamin supplementation in mothers at high risk of having a baby with a neural tube defect in order to test rigorously the hypothesis that vitamins significantly reduce the risk of recurrence of the condition. Mothers \vho have had one or more hahies with a neural tube defect are believed to have a one in twenty chance of having a recurr- ence of NTU in subsequent pregnancies. The proposal is to admit such mothers w h o intend to have auother baby into the study and t o randomize them iuto three groups, each of which would receive a particular combination of vitamins. The vitamins would he taken daily for at least until the date of the second missed period-i.e., until well after the t i n ~ e of
5 1

ncutal tuhc clowrc. 'The mothers would he lollowed until ctu!iplctiori 01' lhc s~~hseclucnt pl-cgnancy and thc recurrence r i~tc trC N1'1) will he cx~irnincd in each supplemented group :ifid iri ;I group 01 (:oillrol mothers. A t the conclusion of the study we hope to he in a position to establish whether vitamin s i r i~plcnic~~tai io~i ;IT-ound the time of conception reduces the - , . . L L U ~ T C I I C C rate of N ' I Ik ;ind i f such an effect is Sbund, it ii1;iy also hc posihlt. t o identify which p;irlicular vitamins are rcsporisihlc.
A mi~ior constrain^ in n study of this nature is the difficulty of d ta in ing :~dccl~ratc. numhcr-s o f mothers. To reach a sat- isfxtol-y conclusion 21s to the efficacy of vit;iniin supplemen- tation will rccluisc the study of about 500 mothers who previously Ii;~ve h x l one or more babies with a neural tube defect. Duhliii is prah:~hly the most suitable city in the world to pursue this question fir-stly because some 25,000 bil-ths rake place each year in illst four hospit:~ls (Coombe, National Maternity Iluspital, l<olunda and St. James's) and secondly, hcc;~use ol'thc high incidencc of neural tube dcfects (fivc pcr 1,000 in 1478) iri this population. During the period 1970- 1980 there were 237,500 births in the four Dublin hospitals of whom approximately 1,480 were NTDs. Allowing for those who have conipletcd their families and non-contacts, we esrimate that ahout $50 of these mothers will plan o further pregnancy and will agree to take part in the study. The remaining 150 mothers will be recruited prospectively from the expected 52,000 births in the four hospitals during I981 arid 1982. We expect that practically all of the study mothers will have completed their subsequent pregnancy by the enti of 1984. Thus, i f ;ill gocs according to plan. the results of the study would be wailable in early 1085.
Dr. Peadar Kirke is the director of the project and with the other members of the group he is currently involved in the planning and org;misation of the study. It is hoped to enter the first mothers into the study in mid-summer 1981. This is clearly ;I very large and ambitious project and a major effort will be scquired to bring it to a successful conclusion. The Medicn-Social Kesc:~rch Board is pleased to be involved in this co-opcrativc effort.

6 ( i ) CONCERTED ACTION I'RO.IHC1' ON CONGENITAI,
MA1,FOKMATIONS A N D MlJI~'I'Il'I,IS BIRTHS
1-hc purpose oftthis project known as EtII<OC'AT, is to establish a population hascd congenital nralforniatioll regis- ter and use it for monitoring environnlental factors, for instance, ncwly introduced drugs, that could be responsible for abnormalities. The register is also used fur testing differ- ent hypotheses and for specialiscd research on congenital abnormalities.
The register is based on the Community Care a r e a of the Eastern Ifealth Board (Dublin City and County, Co. Kildare and Co. Wicklow). In the year 1st Septernber 1979 to 3lst August I980 there were 25,950 babies born to nlothers I-esi- dent in the Eastern I-lealth Board area (Dublin City and County-21,372: Kildare--2,528 and Wicklow--2,OSO). Among those births there were 299 sets of twins and two sets of triplets. The twinning rate was 11.7 per 1,000 pregnancies.
In 1968 the twinning rate was 13.6 per 1,000 pregnancies (1). The fall in the twinning rave is due to a fall in the average age of mothers, The risk of having two egg (binovular) twins increases with the age of the mother.
T o ensure the complete coverage of the incidence of con- genital malformations several sources of ascertainment wcre used, including autopsy reports on periuatal deaths.
In the year 1st September 1979 to 31st August 1980 there were 673 babies born with one o r more congenital malfor- mations. The table shows the incidence of some of the more serious congenital malforn~ations.
Incidence of eonprnitnl malformations in the ilaslel-n Health h a r d area.
~ ~ (livc and stillbirths) --
Aneoccph;~ly with or without Spin:! Uilida Spim Bifid:, with o r without Rydroccph;ilur 0 t h c r C N . S . al~nnrnmalitiea I 1 h All C.N.S. ithnormal~tics 5 3 Congcnml I-lc;m Dlscaw 2 (1 Clcft lir, ;md "alate I i ... Down'; Syndmrnc 1 ..l Phcnylkelanurin 1 iq 11.2 --

'l'itc r:on&rnilal ~nalfor~nalic~ns of the central nervous system remain one o f t h t snajtn causes of perin:~lal nrort;~lity.
'['he rcgisicr llas a d i ~ c c t acrcss lo tlre c o i n n ~ ~ ~ n i t p through hi: I)iiectors of i 'o~irn~t~ni ty Care. This arrmgetr1cnt is very advmtagcrrus i ts the register may b2 used fur the urgent testing of hypottlcscs i f tI1e1.c arc sudden cI1angc.s in the i~rcitlcim of any group of congcnital inallorntatiotrs.
'l'l~cre w e ~ m ~ ~ x ~ s i l s for various slutlies in pl-eparalion tiaseil on the register. These studies will continue to he co- ortiinatcd by Bn~sscls until 1987.
A similar ElIKOC'AT study on cnngcnilal ahnormalitics, under the aegis of the Western Health D o a d , has been p~-op)+.xI for the Wcst of Ireland ccntrcd on Galway.
So [:it, three prthlications were produccd by EUKOCA1':
I . ECJKOCAT guide to Eponyms and Syndromes. Com- piled by J . A . C. Weatherall, Project Leader.
2. EUKOCAl'guide to the confirmation of zygosity diag- nosis of multiple births. By Robert F. Vlictinck and Herman Van der Berghe. Edited by J . A. C. Weath- erall. 19XO.
3. EIJIIOCAT guide to :i service in fetal and perinatal pathology. By John IL. Emery and Josephine A. C. Wcathcrnll.
/ { < p r e t r t
'TJean. G . and Keane, 'l. ( 1972). An investigation of thr high twiuning rate in rhc Rcpribl~c o( lrrl;md. Uritish Journal of I'revcntwc ;lnd Smial Medicine. 26.3, 186.

6 (ii)
ACCURATE CERTIFICATION AND REGISTRATION OF DEATH
Accuratc certification and registration of death is essential not only for legal purposes but also for making possible studies of the causes of death. In our 1979 Annual Report a study was described of registration and certification of death in 25 parishes in the West of Ireland for the years 1974 to 1977 inclusive. In this study, we found that more than 6% of deaths were unregister2d and almost 8 % of deaths were uncertified'.
It is not only important that deaths should be registered and certified it is also important that they should be certified and coded in such a way that comparisons are possible with other countries in western Europe. In 1980 we undertook a pilot study in collaboration with Professor Walter Holland, Department of Community Medicine, St. l'homas's Hospi- tal, London, and with Professor Rene Pariente of Paris, to ascertain how doctors certified non-rheumatic heart disease and respiratory diseases in Ireland, England and Wales, and France. For this study, 10 protocols were prepared describing case histories of patients leading to their death and 10 doctors in Ireland and in the other countries were asked if they would complete the death certificate for them. In Ireland 10 doctors were chosen at random and all of them kindly agreed to complete the death certificates, which were then coded by the Central Statistics Office, Dublin. The same exercise was undertaken in England and Wales and France and later in the year in the remaining countries of the European Eco- nomic Community. This pilot study proved most successful and showed some very major differences in certification and in codification of death between the countries ot the Com- munity. In 1981 a fullscale study will be undertaken using a random sample of at least 50 doctors in each of the countries of the Community. A comparison will then be made between the way deaths are certified and coded in the countries of the EEC and the results will be analysed and reported.
Reference 'Dean, G. and McLoughlin, H. The registratiorl and certification uf deaths in the
west of Ireland: A follow-upstudy. Irish Medical Journal. 1980, 73.7.269,
55

6 (iii)
RESPIRATORY DISORDERS IN AGRICULTURAL WORKERS
The present study is the continuation of the work under- taken with the European Economic Community aimed at defining, collecting and analysing data which appear neces- sary for determining the amounts of respiratory desease in rural workers.'
Despite the usual pattern of less respiratory disease among people in rural areas, a survey of a random sample of farmers in Ireland showed a relatively high prevalence of farmer's lung, an allergic alveolitis, caused by inhaling the spores of fungi occurring in mouldy hay.3 In Normandy, a survey by Professor Rene Pariente and his colleagues on agricultural workers showed that 30% had evidence of some degree of airway obstruction and 32% reported chronic cough. These findings indicated the need for further examination of the possible problems of occupationally induced respiratory dis- ease among agricultural workers.
Ireland has the highest proportion engaged in agriculture, 26% of its working population, of any of the countries of the European Economic Community and 87% of Irish farm workers are farmers working on their own account. Only Germany and Belgium where 8% and 4% respectively of the populations are engaged in agriculture, have a similarly high proportion of agricultural workers working on their own account. TABLE 1.
The expectation of life for men in Ireland is greater in rural areas than in other urban areas and greater in other urban areas than in Dublin city and county.' In women, on the other hand, this difference does not occur. Some causes of death are more common in women in urban areas and others in rural areas.

TABLE 1
AGRICULTURAL WORKERS IN THE EEC
proportion of (a) The working population engaged in agriculture (It) Employer and own account farmers, by country in 1971
p~~
O/o of working pop. Employers and awn engaged in agricult. account farmers as a %
uf all agricult. workers
Belgium Denmark Endand and Wales ~inance Germany Ireland Italy 19 66 Netherlands 7 77
A study of factors related to respiratory symptoms in Irish men showed that although rural dwellers had smoked con- siderably less than those living in Dublin and other urban areas, a higher proportion of rural dwellers complained of breathlessness, 16%, than in Dublin or other urban areas and complaints of chronic cough, 19.6%, and phlegm, 21.4%, were about the same as for the total Irish population (18.6% and 22.5% re~pectively).~ This study showed that in Ireland cigarette smoking, lower social class and increasing age were strongly associated with these respiratory symp- toms. Farm workers in Ireland are also subject to particular respiratory problems related to their work, for instance allergic alveolitis, or farmer's lung, due to sensitivity to the fungus Micropolyspora faeni which flourishes in mouldy hay . 3
Farmers are also subject to respiratory symptoms caused by other fungi and protein, for instance aspergillus causing aspergilloma, and bird protein causing bird fancier's lung. Another study, described below, is being undertaken under the guidance of a steering committee (Professor Walter Hol- land, London, Professor Renk Pariente, Paris, and Dr. Geof- frey Dean, Dublin).
Representatives from each EEC country were asked to obtain mortality data in a common format and this was collected for five years. In Ireland this was for 1969 and 1971-1974 (1970 was not available). The codes used were (1) All causes of death, (2) Respiratory tuberculosis, (3) Lung cancer, (4) Non-rheumatic heart disease, (5) Influenza and pneumonia, (6) Bronchitis, emphysema and asthma and (7) Other respiratory disease. These codes were based on the
57

ICD codes A. The data has been analysed in five-year age groups, from 16 to 64 years, by sex, occupation (agricultural or other) and also by urban and rural residence. Standardised mortality ratios (SMRs) have been computed, using for ref- erence the population and the deaths for the combined EEC countries. Male and female ratios have been calculated sep- arately using separate sex-specific reference populations. In addition, the SMR for the seven diagnostic groupings have been calculated for Scotland.
Since the proportion of agricultural workers who are employers, or who are farmers on their own account, rather than employees, varies between the different countries, the data for agricultural workers has been examined wherever possible according to this division. In England and Wales and in Denmark, the mortality rates for all the members of the social class to which each type of agricultural worker belongs have been obtained for comparison. In France, mor- tality data for men of social classes equivalent to the agricnl- tural worker categories have been obtained.
A comparison of urbanlrural mortality data was available from all countries except Belgium, Italy and Germany. Ger- man data were available for two states.
Large between-country differences in each of the seven groups studied occur. The SMR for bronchitis, emphysema and asthma was highest in men in Ireland of all the countries studied and for influenza and pneumonia Ireland ranked second highest, just below England and Wales. Respiratory tuberculosis rates are low in the Netherlands, Denmark and England and Wales and the highest respiratory tuberculosis mortality is in Italy. A full report of the study will be puh- lished in 1981.
A survey was also undertaken of 121 young members of the farming community who were attending a Macra na Feirme conferene4 They worked on farms which were larger than average (mean size 132.0 acres) and prevalence of smoking was low (21.5% were current smokers). Silage was made on the majority of farms (78%), yet 62% of those interviewed had been in contact with mouldy hay within the previous two years. Many of the farms (69%) kept poultry, but in small numbers and frequently reared both indoors and outdoors. Little is known of the risk of developing extrinsic allergic alveolitis in thesecircumstances.
Prevalence of cough, phlegm, breathlessness and wheeze,
58

and a history of lower respiratory tract infection appeared high. Five per cent of those interviewed had a history of asthma, while 10% had breathlessness, chest tightness or wheeze while dealing with mouldy hay. More detailed study of the prevalence of asthma and extrinsic allergic alveolitis associated with mites and fungi in mouldy hay and in grain crops would be useful.

6 (iv)
FARMER'S LUNG IN COASTAL AND MOUNTAINOUS AREAS
Dr. John McHardy of Donegal is undertaking a study in collaboration with the Medico-Social Research Board and the Microbiology Department of Queen's University, Belfast (Mr. James Evans) to compare 50 farmers in the coastal area of Donegal with 50 farmers in the mountainous areas. The farmers were interviewed and a specially prepared question- naire has been used. Their respiratory function was estimated and blood was taken and sent to the microbiology laboratory at Queen's University so that a precipitin test could be undertaken for sensitivity to Micropolyspora faeni and other allergens that could cause farmer's lung. From the first 83 farmers studied, seven of them gave a strongly positive precipitin test to Micropolyspora faeni, the fungus usually responsible for farmer's lung, two gave doubtful reactions and one was positive for another fungus, aspergillus.
Nineteen eighty has been a very bad year for farmer's lung in Ireland. Many specimens of blood are sent to the labora- tory at Queen's University from the north-east of Ireland. In all, at this laboratory 1,200 specimens of blood were tested for sensitivity to Micropolyspora faeni and 116 of these were strongly positive, the highest number that has been found in any year until now. The increasing number of farmers diag- nosed as having farmer's lung is no doubt due to the wet summer of 1979 but it is also due to the greatly increasing awareness among doctors of the high frequency of farmer's lung among farmers who handle mouldy hay in Ireland.

EVALUATION OF FARMER'S LUNG CAMPAIGN
The North-Western Health Board, which includes the three counties of Donegal, Sligo and Leitrim, is undertaking a study in collaboration with the Medico-Social Research Board to ascertain how effective are the efforts to inform farmers about the special dangers of respiratory disease to which they are exposed, for instance, farmer's lung from handling mouldy hay, other forms of allergic alveolitis, allergy to bird protein, etc. This is an attempt to assess the effectiveness of an educational campaign to prevent farmer's lung and other respiratory diseases in farmers and to identify what further refinements should be undertaken in the strat- egy to ensure that the message is clearly understood.
A random sample was taken of 100 farmers from the 23,000 farms listed in the three counties of Donegal, Sligo and Leitrim with a rateable valuation of over £5 per year. Every 230th farm on the list was chosen to produce the 100 farms. Four specially chosen public health nurses interwewed every member on the farms over 16 years of age. A special questionnaire was prepared. The four nurses covered 25 households each. The field work was completed during October and November, 1980, and the processing and col- lating of the data is being undertaken at the Medico-Social Research Board and a report will then be prepared for publication.

6 (vi)
NATURALBACKGROUNDRADIATION ANDCANCER MORTALITY IN IRELAND
The primary aim of this study is to determine if variations in the very low levels of naturally occurring background radiation are associated with variations in cancer rates. The study was funded to the Medico-Social Research Board by the European Atomic Energy Community (EURATOM) and carried out by the Department of Community Health and the Department of Physics, Trinity College, Dublin. A similar study is being carried out at the same time in Brittany by the Ecole Nationale de la Sante Publique, Rennes, where similar methods are being used.
The radiation mapping produced in the first year of the study has enabled us to identify three counties of high average natural background radiation (Waterford, Wexford and Wicklow) and five counties of low average background (Meath, Westmeath, Kildare, Carlow and Kilkenny) for more detailed study.
Detailed radiation mapping of these eight counties has been completed and average radiation values for each Dis- trict Electoral Division (DED) within these counties have been calculated. (There are between 50 and 120 DED's per county).
All the cancer deaths that occurred in these eight counties between 1971 and 1976 (inclusive) have been assigned (by computer analysis of the home addresses of the deceased) to the appropriate DED. DED's are the smallest unit of area for which data are available for demographic analysis. Because the numbers of deaths occurring in individual DED's are small. DED's have been aggregated according to their average background radiation levels.
The age sex standardised cancer (total and type specific) mortality rates of these aggregates are presently being com- pared to see if they correlate with the variations in natural background radiation.
In order to assess the effect of building materials and of other factors on indoor radiation and in order to validate our mortality data, a house-to-house survey of 98 houses was completed in the summer of 1980. These data are presently being analysed.
62

7
THE SUDDEN INFANT DEATH STUDY
A pilot study on infant deaths in Dublin City and County was started on 1st April 1979. The causes of death in all babies aged between one week and one year were ascer- tained. There were 223 deaths of babies in this age group between April 1st 1979 and 31st December 1980.
TABLE l
Causes of death in babies aged one week to one year (Dublin City and County-Is1 April l979131sf December 1980)
Total 99.9 1 5.9
The commonest cause of death was "Cot Deathx---of which there were 85 babies, giving a total of 38%. There were 35% of deaths due to congenital malformations, 16% due to infections and, surprisingly, almost 6% due to accidents. The babies that died of Sudden Infant Death Syndrome were studied in detail.
Sex and Seasonal Variation of Sudden Infant Death There was a 1.5:l ratio of male to female deaths. A greater
number of deaths occurred in the cold months (55.5%, October-April) as compared to the warmer months (44.4%, May-October) but the variation was not very marked.
Birth Weight The birth weight ranged from 2,000-4,500 grams+. The

majority (63%) were 3,000-4,000 grams and when compared to babies born in Dublin hospitals this weight pattern is standard.
Age at Death There were no sudden infant deaths less than four weeks old. Most of them (53%) were eight to fifteen weeks old.
Mother's Age Seventy one per cent of sudden infant deaths were to
mothers aged 25-34 years, with 2% less than 20 years, and 6% over 35 years.
Feeding Over half (52%) of babies were bottle fed, and 34% were
i I
breast fed either completely or for a limited time after birth.
Socio-economic groups Most of the deaths (53%) fall into the "skilled manual"
and "other non-manual" groups, but as there is no informa- tion vet on births bv socio-economic erouD it is not ~ossible to diaw any concl;sions from this. siudy on births by socio-economic group is at present being undertaken by the Medico-Social Research Board.
Place o f baby in fanzily A small number (16%) of these were first babies, with the
greatest proportion (30%) being third babies. Whenever possible, a clinical conference is held on sudden
infant death babies. A full report on the baby is obtained from the parents and the family doctor and the public health personnel involved in the baby's care are invited to attend. These conferences are held in Temple St. Hospital under guidance of the Pathologist, Dr. Seamus Cahalane and they highlight the need for such a procedure to become standard practice on all home infant deaths, involving all those who deliver the primary care.
At present all sudden infant deaths in this study have an autopsy examination. In 1981 we propose enlarging greatly the depth of the pathological investigations that will be undertaken into these deaths. This will include detailed stud- ies of the neuro-anatomy and virology under the direction of Dr. Seamus Cahalane of Temple Street Children's Hospital.
64

SELF-DISCHARGE FROM IRISH GENERAL HOSPI- TALS, 1978.
Much has been written in recent years about non-compli- ance of patients with medical treatment. Discharge from hospital against medical advice (AMA) is perhaps the most extreme manifestation of non-compliance among hospital- ised patients but this phenomenon has not been considered. Discharge AMA is an unpleasant event for the patient, his family, his fellow-pntients and the staff. It can also represent a serious risk for the patient. We were prompted by Dr. David Nowlan (Irish Medical Journal, 1979.72, 39) to exam- ine the extent and nature of the problem in Ireland. "Self- discharged" is coded in the HIPE and our study is confined to the items of information which are included in this infor- mation system.
In 1978 there were 1,280 discharges AMA accounting for 0.4% of the total hospital discharges reported to the HIPE. Males were twice as likely as females to discharge themselves AMA and the problem was most marked in the 25-44 age group. Not surprisingly, patients who took their own dis- charge did not stay in hospital for as long as total discharges. The average length of stay was 10 days for total discharges and 6 days for discharges AMA; half of those discharged AMA spent just one day o r less in hospital. Emergency admission was more common among the self-discharges, 52%, than total discharges, 25%. Most "persons of no fixed abode", 93%. left hospital AMA and they were responsible for 20% of all discharges AMA.
The four main diagnostic categories where the percentage of patients discharging themselves AMA was greater than the ovcrall average of 0.4% are shown in table I. The two commonest causes of admission to general hospitals partici- pating in the HIPE in 1978 were "accidents, poisoning and violence" and "symptoms and ill-defined conditions" and discharge AMA was a particular problem among these patients. The self-discharge rate was also high for patients
65

with two Less common causes of hospital admission, "infective and parasitic diseases" and "mental disorders". Sixty-six per cent of the paticnts who discharged themselves AMA were in these four diagnostic categories which together accounted for just 29% of total hospital discharges.
An investigation of all discharges for accidents, poisoning and violence showed that the percentage of patients dis- charged AMA was more than 1 % for three main diagnostic subgroups: intra-cranial injury excluding skull fracture, unspecified lacerations of the head and adverse effects of medicinal agents. Intra-cranial injury was the largest group and accountcd for 9% of all discharges AMA. One in forty of all patients with a diagnosis of adverse effects of medicinal agents was dischargcd AMA. Pain in the chest and abdominal pain were two main diagnostic subgroups in the "symptoms and ill-defined conditions" category. Just over 2% of all palicnts with a diagnosis of "pain in the chest" were dis- charged AMA. The fact that this diagnostic group was class- ified under "symptoms referable t o the respiratory system" suggests that the hospital doctors felt that the chest pain was probably not cardiac in origin. In the group of infective and parasitic diseases, gastro-enteritis and tuberculosis were the notable diagnostic suhgroups. Of the 39 patients with gastro-enteritis who were discharged AMA, 21 were aged less than one year and 1 1 were between one and two years. Almost 5% of all patients with tuberculosis were discharged AMA and approximately half of these were in the 45-64 age-group. Drug dependence and alcoholism were the impor- tant diagnostic subgroups in the mental disorders category. A total of Y I patients had a discharge diagnosis of drug dcpendencc and 23% of these were discharged AMA. Alco- holism accounted for 47 of the 101 patients with mental disorders who discharged themselves AMA and all but one of these were male. The self-discharge rate was below the average for the other main causes of hospital admission, i.e. diseases of the respiratory, circulatory, disgestive, genito- urinary and nervous systems and neoplasms. An important finding relating to these diagnostic groups, however, was that some patients with serious illnesses discharged themselves AMA. For example I1 out of a total of 3,644 admissions (0.310) for acute n~yocardial infarction were discharged AMA as were 19 of 3,243 admissions (0.6%) for other forms of ischaemic heart disease.
66

A detailed diagnostic breakdown of discharges AMA revealed that the self-discharge rate was particularly high for a variety of conditions which share a common association with the excessive use of alcohol. The fact that the following alcohol related conditions--head injuries, adverse effects of medicinal agents, neuroses, alcoholism, drug dependence, pulmonary tuberculosis, alcoholic cirrhosis and pancreatitis -accounted for 27% of discharges AMA and just 5% of total discharges suggests that abuse of alcohol may be a common association with discharge AMA.
The findings of this study will be reported in full in 1981.
TABLE 1
Main diagnostic group for d ischarp AhlA and total hospital discharges, 1978.
I -
I
Group of diagnoses and ICD Code Number
Accidents, poisoning and violence (NRIM-999)
Sym toms and ill-defined con4tions (780-796)
Infective and parasitic dis- eases (OW-136)
Mental disorders (290-315)
All other diagnoses 439
All diagnoses 1280
% of all dkcharges
AM A
/ Patients discharged AMA Total
hospitill dischtp
discharges*
'Patients discharged AMA as percentage of total discharges f w specified diagnostic group.

In the Annual Report 1979 of the Medico-Social Research Board a study on the "Causes of death of blue-collar workers at a Dublin Brewery, 1954-1973" was reported and the results of the study have now been published.'The brewery workers had a greater than expected death risk from cancer of the rectum and, to a lesser extent, from cancer of the colon and they also had an increased risk of death from diabetes. Nevertheless, overall they had a better expectation of life than the general Dublin male population and their pattern of I death was not that expected of a population consuming large amounts of alcohol. i
The increased risk of death from cancer of the rectum and, to a not statistically significant amount, cancer of the colon among the brewery workers has prompted a study comparing the past occupational history, a detailed study of the diet and drinking habits, smoking habits and the leisure-time activities of 100 patients who have developed cancer of the rectum and 100 who have developed cancer of the colon in comparison with the same number in the same age group who did not develop these cancers. The study was undertaken by Dr. Kieran Moriarty of St. Leonard's Hospital, London, where the study has been completed and by Dr. Shane O'Neill and Dr. Kevin Ward of Sir Patrick Dun's Hospital, Dublin, where it is expected the study will be completed in 1981. The results will then be analysed and reported upon.
There is good evidence that dietary fibre, particularly the amount of fibre or roughage in the diet, is of great importance in diseases of the bowel, including bowel cancer. A naval surgeon, Capt. Cleave, perhaps more than anyone else, has shown the importance of not removing the fibre from our diet2 and he has brought the evidence together in his publi- cation of what he terms "sacharine diseases". A deficiency of fibre in the diet, for instance the use of white bread rather than wholemeal bread, often results in an excess of easily assimilated carbohydrates, leading to a premature onset of
68

obesity and diabetes. The importance of sufficient fibre in the diet is a concept which could prove to be one of the most important new ideas in this ~ e n t u r y . ~ It is hoped that the present studies comparing.the diet of patients with cancer of the colon and rectum with suitably chosen controls will throw further light on the aetiology of these important cancers.
References ' Dean, G . , MacLennan, R . , McLoughlio. H , and Shelley, E. Causes of death
of blue-collar workers at a Dublin brewery, 1954-73. British Journal of Cancer (1979). 40,581. ' Cleave, T.L. The ne lect of natural principles in current medical practice. Journal of the Royal ~ a v a f ~ e d i c a l Service, 1956: 42,SS. ' Avery Jones, F. The Emergenceof Gastroenterology. The Harveian Oration
of 1980. RoyalCollege of Physicians, London.

MULTIPLE SCLEROSIS
The Director of the Board has continued his research into his major personal research interest, the cause and preven- tion of multiple sclerosis (MS). He founded the Multiple Sclerosis Society of South Africa and is a member of the International Medical Advisory Board of the International Federation of Multiple Sclerosis Societies.
The epidemiology of multiple sclerosis appears to be a major clue to its causation and has to explain the following facts. Immigrants from northern Europe to South Africa and Israel keep their high risk of getting MS unless they migrate below the age of 15, when they have only one-quarter of the risk of those who migrate after this age.'.' On the other hand, immigrants from areas of the world where MS is uncommon, Asia, Africa and the West Indies, to England, a high MS prevalence area, keep their very low risk of MS particularly if they are ethnic Asians or Af~icans .~ This could, of course, be due to a great extent to a genetic factor which protects them against developing MS. Multiple sclerosis, contrary to the previous opinion of the Italians, has a rela- tively high prevalence in Sicily, over 40 per 100,000' but a very low prevalence in the neighbouring islands of Malta only 60 miles away, 4 per 100,000.5 In South Africa, immi- grants from the United Kingdom have 11 times the risk of developing MS of the Afrikaans-speaking white p~pu la t ion .~ In contrast, mortality from MS in Australia among the Australian-born is half of that of the reported mortality in England and Wales and immigrants from the United King- dom have the same risk of dying from MS as the Australian-born.' Campbell et al reported in 1947 that four out of seven research workers into a demyelinating disease of sheep, similar in many ways to multiple sclerosis, devel- oped multiple sclerosis.'
In Ireland, MS is slightly more common in the North than in the S o ~ t h . ~ In Scotland MS is more common than in England and the prevalence of MS is not significantly differ-
70

ent in the more celtic Outer Hebrides than in certain areas of North-East Scotland which has a larger Viking genetic component ."I
Multiple sclerosis almost certainly results from a combi- nation of genetic and environmental factors because it occurs more frequently than would be expected by chance in two members of a family. On the other hand, it is not inherited in the ordinary sense hut what is probably inherited is a genetic predisposition. That this is so is confirmed by the fact that certain blood factors, the HLA factors, are more com- mon in multiple sclerosis than in the general population, for example HLA A3, B7, Dw2. On the other hand, the fact that immigrants to South Africa and Israel develop MS much less frequently when they migrate in childhood than when they migrate as adults confirms that there must also be an environmental factor.
Given these facts, multiple sclerosis research is continuing along the following paths.
1. With assistance from the Committee for Medical Research of the European Economic Community a study is being undertaken to compare the genetic, the HLA factors, and environmental differences between Sicily and Malta; this consists of a comparison of the multiple sclerosis patients and their controls, those who do not have multiple sclerosis. In this way it is hoped to ascertain to what extent genetic factors contribute to the comparative absence of multiple sclerosis in Malta.
2. Multiple sclerosis does occur but it is extremely uncom- mon among the New Commonwealth immigrants. The genetic and environmental factors that could account for the small number of MS patients who do occur in this group are being investigated.
3. We are reviewing again what really happened to the four out of the seven research workers into swayback disease who developed MS. All four have died and two had autopsies of their brain and spinal cord, although these autopsies have not been reported upon. We managed to obtain the autopsy specimens of one of them and traced the relatives of all four so as to review fully the whole story. It seems a vital clue:
4. An acute form of MS, neuromyelitis optica, Devic syndrome, is more common in India, Japan and China than in Europe. In China it is much more common than multiple sclerosis which is very uncommon. Devic syndrome is very
71
uncommon in Europe but when it does occur it is often in an immigrant from Asia or Africa. The International Federation of Multiple Sclerosis Societies hopes to develop a study of Devic syndrome and MS in collaboration with Chinese neu- rologists in 1981.
5. The New Commonwealth immigrants, particularly the ethnic Asians and Africans, have a very low risk of MS and it will be interesting to see if their children who were born in Europe keep this low risk or have a risk which increases towards the high European level. It looks at present as if they keep the low risk of their parents.
6. Finally, it would be of great interest to compare the genetic and environmental factors where two siblings, that is brother and brother, sister and sister, or brother and sister, both have MS in comparison with adult siblings in a family who do not develop MS. In this way it would be possible to find out much more about the importance of the genetic predisposition to the disease.
The epidemiology of MS appears to offer the vital clue to its cause and present thinking suggests that multiple sclerosis results in all probability from some form of faulty immune reaction, due to a genetic predisposition, to some protein substance in the central nervous system, probably a virus, but so far no virus has been detected.
"-" Dean, G. and Kurtrkc, J. (1971). British MedicalJournal, 725.
' Alter, M. el al.{1962{: Archives ofNeurology (Chic.), 7,253. ' Dean, G. et al. 1976 Bntlsh Medical Journal. 1,861. Dean, G. el al. (1979). Journal of Epidemiology and Community Health. 33,
3. 107 ' -Vassallo, L. el al. (1979). Journal of Epidemiology and Community Health,
33,3,111. * Dean, G. (1967). Brmsh MI ' Australian Bureau of stat is^
rdical Journal. 2, 724 rics. 1981. Personal communication.
" Campbell, A.M.G. et al. (1947). Brain, 70,50. Br?dy,R.,-?ep_n,-:., Secerbegovic, S. and Secerbegovic, AM., Irish Medical
FIVE CHINESE DOCTORS VISIT IRELAND
In 1976, the Director of the Board received an invitation from Professor Huang Chia-ssu, the President of the Chinese Academy of Medical Sciences, to lead a group of 10 Irish doctors from the Republic of Ireland as guests of the Acad- emy. The delegation of doctors visited China for two weeks in September, 1976 and they were able to study Chinese medicine, both traditional and modern medicine, in the cities of Peking, Shanghai and Canton and also in rural areas. The visit was fully reported upon at the time. The Irish doctors were impressed at the Chinese application of the teachings of Chairman Mao to "serve the people". The achievements of Chinese preventive medicine were particularly impressive and also their care of children and of the aged.
In 1980 the Medico-Social Research Board invited the Chinese Academy of Medical Sciences to send five Chinese doctors to visit Ireland. The visit took place in June, 1980 and the leader of the group was Professor Deng Jia-dong, the Vice-president of the Chinese Academy of Medical Sci- ences. Among the group was Professor Feng Ying k'un, an orthopaedic surgeon, Dr. Wu Chung-hao, a general physi- cian, and two neurologists, Professor Wang Guisheng and Professor Zhao Baoxun. The Chinese physicians were received at Aras an Uachtarain by President Hillery and also by Dr. Michael Woods, T.D. Minister for Health and Social Welfare. They were delightful guests and gave a number of lectures while they were in Ireland at Trinity College and elsewhere.
The two neurologists were invited because of their partic- ular interest in multiple sclerosis and after visiting Ireland they spent a further three weeks as guests of the National Multiple Sclerosis Society of New York in the United States, followed by a week as guests of the Multiple Sclerosis Society of Great Britain and Northern Ireland in England. Multiple sclerosis is very uncommon in China but an acute form of the disease, Devic syndrome, is relatively common. It is hoped


that the visit of the Chinese neurologists to Ireland, the United States and England, will lead to a collaborative study between the neurologists of the western world and those of China on multiple sclerosis and Devic syndrome in China which could throw light on the aetiology of multiple sclerosis.
The Medico-Social Research Board would like to thank all those who helped make the visit of the Chinese physicians a success and who entertained them, in particular the President and staff of the universities, the medical schools, the hospitals they visited and those who offered hospitality, especially Mr. P.V.Doyle, Guinness's and The Irish Times.

CONCLUSION
In previous reports we have concluded with emphasis on the major causes of ill-health in Ireland, such as cigarette smoking, alcohol abuse, a diet too rich in animal fats and junk foods and not rich enough in fibre, and lack of exercise. Concluding the 1980 report and looking forward to 1981 during a time of economic recession with large numbers of our people unemployed we should give the highest priority to the significance of poverty in the causation of ill-health. It has been shown in many studies in the United Kingdom and elsewhere that there is a great difference in mortality and morbidity between the better-off-the upper socio-economic g r o u p a n d the poor-the lower socio-economic group. Such studies in Ireland have not been feasible in the past except for social class factors in psychiatric hospital admissions because they depend on accurate reporting of occupation not only in the census returns, which provide the populations at risk, but also on death certificates and returns of hospital admissions.
Unfortunately, in Ireland accurate information about occupation has frequently been omitted from the death cer- tificates and hospital admissions. In the case of married women, it is important to have an exact description of the work of the husband whether it is before or after retirement. The Director of the Central Statistics Office, Dublin, is assisting these studies by making sure that occupation is recorded as accurately as possible on death certificates so that the causes of death can be studied by social class. A preliminary study has already been undertaken by the Direc- tor of the Board among males aged 15 to 64 resident in Dublin, a group at present with the best codingof occupation. This study shows that among these men the difference in socio-economic group mortality which occurs in England is also occurring in Ireland.
In our modern society it is possible to produce sufficient basic wealth by employing relatively few people but unless
76

some form of occupation is available to adults so that their life has purpose, lack of employment can be completely destructive of personal self-respect. Perhaps people would prefer to work for a modest wage to improve the environment than to be unemployed.
The Board hopes to undertake a number of studies based on socio-economic group, on mortality and morbidity in infants and also the effects of poverty on life expectancy, the causes of death and hospitalised morbidity. It has already been shown that socio-economic group is a big factor in influencing recovery from psychiatric illness; the unskilled are greatly over-represented among psychiatric hospital residents.
During 1980 the Medico-Social Research Board encour- aged two of its staff to take higher degrees, Dr. Emer Shelley who is taking the degree in M.Sc. in Epidemiology at the London School of Hygiene and Tropical Medicine, and Dr. Rosemary Hamill, who was previously working with the Hospital In-Patient Enquiry Scheme, is taking the Diploma in Public Health at University College, Dublin. They will both be returning to work for the Board in the second half of 1981. The Board proposes to continue its policy of training young doctors in epidemiology and community health in collaboration with the Faculty of Community Medicine of the Royal College of Physicians of Ireland.
The Board has been responsible for a joint study under- taken by the Medico-Social Research Board, The Health Education Bureau and the Irish Cancer Society on leisure- time activities and attitudes and practices with regard to alcohol, cigarette smoking and drugs among post-primary schoolchildren. This study is under the Direction of Dr. Aengus O'Rourke of the Department of Community Medi- cine, Trinity College, Dublin, and the study in Dublin city and county should be completed in the first half of 1981 and will then be followed by a further study in the rest of the Republic of Ireland. The findings of the study will be com- pared with a similar study that was undertaken in 1970. It is planned and hoped that the study will then extend to North- ern Ireland, using the same questionnaire and technique, where it will be undertaken in collaboration with the Ulster Cancer Foundation.
Other collaborative studies are also taking place between the Republic and Northern Ireland, for instance on farmer's

lung and a study following the observation by Dr. Leonard Walby of the Department of Health and Social Security, Belfast, that the usual ratio of maleifemale births, normally about 1060:1000, changed suddenly in Northern Ireland in 1978 to 1007:1000. The same alteration in the sex ratio occurred in the Republic in 1978 but not to such a degree. The ratio in counties Donegal, Cavan and Monaghan, con- tingent to the six counties of Northern Ireland, was 1005:1000. A joint report between the Department of Health and Social Security, Belfast, and the Medico-Social Research Board about the sudden change in the sex ratio will be published in 1981.
The Committee for Medical Research (CRM) of the Euro- pean Economic Community, which the Director attends as Chairman of the Specialised Working Group in Epidemiol- ogy of the Community, is preparing a five-year programme for future research in the Community from 1982 to 1987. Many of the projects which are planned have stemmed from the Specialised Working Group in Epidemiology and from research ideas that have originated in Ireland. Dr. John Kevany of the Department of Social Medicine, Trinity Col- lege, Dublin, is also a member of the Specialised Working Group in Epidemiology. Professor Ciaran McCarthy and, on his retirement from the Committee: Professor John Scott, represent the Medical Research Council and Dr Tim O'Dwyer, the Department of Health, on the Committee for Medical Research of the EEC.
The CIBA Foundation for the promotion of international co-operation in medical research in London asked the Direc- tor of the Board to collaborate in the preparation of a book entitled "Collaboration in medical research in Europe". Dr. Emer Shelley, Dr. Dermot Walsh and the Director of the Board have contributed a chapter to this book, which will be published in 1981, on migration. We have also contributed a chapter on multiple sclerosis to a book, edited by Trowell and Burkitt, entitled "Western Diseases: their emergence and prevention". This book illustrates how many of the "western diseases" may result from a diet rich in refined carbohydrates, animal fats and protein and low in fibre.
During 1980 there has been greatly increased interest in the importance of diet on health. There is little doubt that our ancestors ate a more healthy diet than we do when they consumed a diet rich in fibre. Our diet of refined carbohy-
78

drates and high animal fat with an excess intake of salt and low in fibre probably makes a large contribution to some of our major diseases such as heart attacks, high blood pressure, diverticulitis, appendicitis and cancer of the colon.
How then can we best achieve a more healthy society in Ireland? This can be achieved by a fairer distribution of wealth, employment of all those willing and able to work, moderation in the use of alcohol and a move away from our pub culture towards drinking alcohol moderately with meals for those who wish to drink, stopping cigarette smoking, eating a sensible diet high in fibre and with a reduced amount of animal fats, i.e. butter, eggs and fatty meat, and refined carbohydrates and, lastly, taking more exercise.
With limited funds, and the amount spent on medico-social research in Ireland is still very small-in 1980 the budget of the Medico-Social Research was IRE503,000--the decisions as to what research will be undertaken by the Board depend on a variety of factors. They depend partly on the expertise of the staff available to the Board. They depend also on the ideas and concepts that come to the Board from its members and from a variety of sources such as the Department of Health, from the Dail representing public interests, from the medical profession and other groups, such as the Economic and Social Research Institute and The Health Education Bureau and very often they come as a result of meetings of overseas experts, for example the Committee for Medical Research in Brussels, or meetings at the CIBA Foundation in London. Some of the Board's projects are large, such as the Hospital In-Patient Enquiry Scheme and the National Psychiatric Reporting System, and some are small but every suggestion that comes to the Board for research is considered and those that can be undertaken where the staff and funds are available, and which are considered to have a high priority, will be undertaken.
During the 13 years of the Board's work there has been almost unlimited goodwill towards the activities of the Board.
It has been said that research consists of 1% inspiration and 99% perspiration and the members of the Board and the Directorate are well aware that many of those who take part in our studies never receive official acknowledgment, for instance, in the hospitals and at the office of the Board all those who are working so patiently on the Hospital in-Patient Enquiry Scheme on which so many research projects are
79

based and on the psychiatric reporting systems. We are well aware of the importance of their work and would like to thank them as we do all those who do not officially work for the Board and who contribute in so many ways to make the work of the Board a success.

ACKNOWLEDGMENTS
We would like to thank Dr. Michael Woods, T.D., Min- ister for Health and Social Welfare, for the great interest he has shown in our work and for the time he has spent with us discussing the medico-social problems of Ireland. We would also like to express our thanks to Dr. Brendan Hensey, Secretary of the Department of Health, and to members of the Departmental staff.
We have continued our work in the closest co-operation with the Irish Medical Association and the Medical Union. We would also like to acknowledge the close liaison we have had with the World Health Organisation, with the Committee for Medical Research of the European Economic Commu- nity, the Medical Research Council of Ireland, The Central Statistics Office, the Economic and Social Research Institute, the Irish Heart Foundation, the Irish Cancer Society, the Health Education Bureau, the Multiple Sclerosis Society, the Irish Blood Transfusion Service and many other boards,
: societies and institutes. Our work would not have been possible without the help
we have received from our many friends, medical and non- medical, who have assisted us in our various research projects.

PUBLICATIONS BY STAFF 1980
The Porphyrias. Conn's "Current G. Dean Therapy", 1980,316.
Factors related to respiratory symp- E. Shelley, toms in Irish men. Irish Medical G. Dean, Journal. 73,6,240. 1980. L. Daly,
and N. Hickey.
The registration and certification of G. Dean deaths in the West of Ireland: A and follow-up study. Irish Medical H. McLoughlin Journal. 73,7,269,. 1980.
Activities of Irish Psychiatric Hospi- A. O'Hare tals and Units 1977. The and Medico-Social Research Board, D. Walsh. Dublin, 1980.
Seasonality of schizophrenic births in A. O'Hare, Ireland. Brit. J. Psych. 137, 74, D. Walsh 1980. and
F. Torey.
Down's syndrome and hypothroid- M. W. Quinn. ism. Irish J. med. Sci. 149, 1 , 19, 1980.
Childhood accidents in Ireland. Irish T. Brannick Medical Journal. 73, 6, 220. and 1980. P. N. Kirke.
Mental Handicap-Ireland and Sweden M. Mulcahy, Compared. Irish Medical Jour- nal. 73,9,357. 1980.
82

The feasibility of price control in reducing alcoholism. Acta psy- chiat. scand., Suppl. 285, vol. 62, 1980.
Multiple sclerosis among immigrants to Britain and in the lslands of Sicily and Malta. Progress in Multiple Sclerosis Research. Springer-Verlag, Berlin, Heidel- berg, New York. 1980. p.465.
HLA groups in relation to epidemiol- ogy. Progress in Multiple Scle- rosis Research. Springer-Verlag, Berlin, Heidelberg, Ncw York. 1980. p.516.
Mothers' views of obstetric care. Br. J. Obst. and Gyn. 87,1029, 1980.
Mothers' views of care in labour. Br. J. Obst. and Gyn. 87, 1034.
1
The treated prevalence of mental ill- ness in the Republic of Ireland-The three county case register study. Psy- chol. med. 10,465, 1980.
Vocational Training and Employment of the Handicapped in Ireland. Vocational Training, No. 2, 1980. European Centre for the Development of Vocational Training, Berlin, pp.40-43.
Major issues in planning services for mentally handicapped persons. Impact, Brothers of Charity Journal on mental handicap, Dublin, December 1980. Vol. 12,5, pp. 2-4.
B. Walsh and D. Walsh
G . Dean.
G . Dean
P. N. Kirke. v
P. N. Kirke.
A . O'Harc, D. Walsh, B. Blake and J. V . Halpenny.
S. O'Connor and P. Faughnan.
S. O'Connor.