annual progress report 20081231 - europa
TRANSCRIPT

Partners
MASH
MASs-casualties and Health-care following the release of
toxic chemicals or radioactive materials
EU project 2007209

MASH: MASS-CASUALTIES AND HEALTH-CARE FOLLOWING THE RELEASE OF TOXIC CHEMICALS OR RADIOACTIVE MATERIALS
EU PROJECT NUMBER 2007209
ANNUAL PROGRESS REPORT 2008-12-31.
Commencement date: April 15th 2008. Contract number: 2007209 Duration: 30 months
Partners:
The European Centre for CBRNE, University of Umeå, Sweden;
Bundeswehr Institute of Radiobiology InstRadBio Bw, Germany;
Centro de Estudios e Investigaciones Técnicas de Guipúzcoa, CEIT, Spain;
Health Protection Agency, HPA, United Kingdom;
Karolinska Institutet, KI, Sweden;
SAMU de Paris, Assistance Publique Hopitaux de Paris, SAMU, France ;
Swedish Defence Research Agency, FOI, Sweden.
Brief summary of project activities 2008
Work package (WP) n° 1-3: Coordination of the project
Project leader: Dr. Åke Sellström
List of partners involved (lead in bold)
CBRNE Centre, CEIT, HPA, SAMU, KI, FOI, InstRadBio Bw
Objective
The objective of our active dissemination strategy is to relay information back to relevant end-users as well as to gain valuable input from all interested parties to obtain the most comprehensive overview of the state of preparedness for CR mass casualty incidents in Europe today.
Description of the work
The coordination of MASH will require use of normal tools and skills for management of an international project with relatively senior and independent partners. There are, however, two areas where the coordination will become critical to the over all performance:
The management of the project will be Dr Åke Sellström, coordinator and Dr Ann Göransson Nyberg, assistant to the coordinator
During 2008 following meetings have been performed:
• Mash Kick-Off Meeting, In Umeå, Sweden 080429 – 080430
• Telephone conference:
MASH 2nd Management meeting 22 September 2008
MASH 3rd Management meeting 20 November 2008
MASH 4th Management meeting 17 December 2008
• Åke Sellström was invited to European Commission DG SANCO 2008-12-10 for a presentation of the project. His presentation will be attached to the report.

Work package n° 4: CR(E) Scenarios
Project leader: Dr. Gudrun Cassel
List of partners involved (lead in bold)
FOI, CBRNE Centre, KI, HPA
Objective
Together with the reference group, the project will define standard scenarios from which the planning process may be discussed. Accordingly, the scenarios should result in a common understanding of the situation to be planned for, in mass emergencies following chemical or radioactive release.
Gudrun Cassel and her co-workers have now completed their report on our scenarios (D1), which will be attached to this report. Gudrun Cassel or Björn Sandström will have a presentation about the scenarios in a joint seminar taking place in Munich from February (10th) 11th-12th, 2009.
Description of the work
The document consists of a summary of each scenario in the form of a table followed by more detailed descriptions. The detailed description of each scenario has an introductory real event followed by the constructed scenario with an injury panorama. The description also contains information on possible technical counter-measures and a discussion of treatment possibilities. Finally there are some suggestions on what type of substances that could be involved in creating such a scenario.
The last part of the summary table of the different scenarios has been left empty concerning response management of each event. Those variables are aimed as support to the discussion on the particular needs of preparedness. The results from other WPs could, if preferred, be used to fill “best practice” into those parts of the tables to create complete summaries of the scenarios in the forthcoming final report.
Work package n° 5: Best practise of today - C mass casualties Project leader: Dr. David Baker
List of partners involved (lead in bold)
SAMU, CBRNE Centre, CEIT
Objective
A common understanding of the generic preparedness planning concept and its components in a C emergency.
Description of the work
1. SAMU, responsible for the chemical responses work package (WP5) has been working closely with Bundeswehr colleague’s occupied with the radiological survey in WP 6. Their
help is gratefully acknowledged. We shall continue to work closely in issuing invitations for the workshop meeting to be held in Munich on February 11th 2009. It will be more efficient if registration and bookings are made through a single channel and I shall liaise with Armin Riecke about this.
2. The chemical questionnaire is now posted on the MASH website and login codes and passwords have been issued to point of contact in the following EU 27 Member States:
Austria, Belgium, Finland, France, Hungary, Luxembourg, Lithuania, Malta, Poland, Portugal, Romania, Slovenia, Spain, United Kingdom.
Through HPA enquiries are being made to set up a point of contact in Eire. We are still looking for points of contact in the remaining States. You have kindly agreed to forward POC in Sweden and Denmark. Any help you could give with the other States would be appreciated. I shall try to complete sending the remaining questionnaire logins by the middle of next week.
3. Concerning finances, the first tranche of SAMU co - finance is still being held by you in Umea. I have had discussions with Professor Carli at SAMU who is now setting up a special account to hold and audit funds. You have kindly paid Dieter Graessle's invoice for setting up the chemical website and the sum of 2,700 Euro is owing to the Umea account from SAMU.
Work package n° 6: Best practise of today - R mass casualties
Project leader: Dr.Viktor Meineke
List of partners involved (lead in bold)
InstRadBio Bw, CBRNE Centre, CEIT
Objective
A common understanding of the generic preparedness planning concept and its components in an R emergency.
Description of the work
The work started in April 2008 with the establishment of the points of contacts in the EU 27.
Helpful information was offered by The Radiation Emergency Medical Preparedness and Assistance Network (REMPAN) of the WHO and by the International Atomic Energy Agency (IAEA).
To gather the information regarding the R/N mass casualty preparedness in the member states of the EU 27 we established questionnaire. This form is online available at
www.mash-online.de
29 institutions from 22 member states announced their active participation (date December 17th, 2008).

A test version of the form can be envisioned using the following data: username: testuser; password: radi9bul.
First results from the questionnaire will be discussed in a joint seminar taking place in Munich from February (10th) 11th-12th, 2009. This seminar will try to define a best practice model for dealing with R/N mass casualties of today. It is also aiming at coordinating further research and training activities as well as achieving exchange of scientists.
Besides the MASH participants about 150 clinical and research physicians, other scientists and representatives from national and international organisations will attend the symposium.
Work package n° 7: Contribution of modern bio-technology
Project leader: Dr. Leif Stenke.
List of partners involved (lead in bold)
KI, CBRNE Centre, FOI
Objective
To suggest biotechnologies that will improve the over-all effectiveness of the health system to handle C or R emergencies.
Description of the work
WP 7 will focus on methods and tools made available from recent advancements in biotechnology to triage in a mass emergency situation following exposure to toxic chemicals and/or to dangerous radioactive material. Current methods for early diagnostics and exposure assessment will be summarized giving particular attention to those methods ability to indicate probable health consequences, latent effects, and/or need for medical treatments. A horizon scan into the fields of molecular diagnostics, proteomics and genomics will also be made, highlighting particularly promising developments that should be of critical value to the mass emergency situation. The use of electronic, standardized medical algorithms to support the medical personnel in the triage situation will be reviewed in cooperation with WP 8.
Activities during 2008, plans for 2009
KI (through its main responsible person for WP 7, Dr Leif Stenke) has participated, as WP 7 leader and as a partner in other WPs, in common MASH group activities during the year. These have included a “kick-off” start meeting in Umeå on April 29-30, a WP 4 (“Scenarios”) focused meeting in Stockholm on September 22nd and several telephone conferences. Tasks also within non-WP 7 work packages have been performed between meetings, particularly related to WP4. Some administrative undertakings related to MASH have been dealt with during the year. A problem, still unsolved, is continued lack of full funding for KI MASH efforts from Swedish authorities, after an unexpected negative decision from the Swedish National Board of Health and Welfare (SoS) in late 2008. Through continued contacts with SoS and other organisations (incl KBM) we, with support from MASH leaders, aim at solving this financial problem as soon as possible.

Preparations for WP 7 activities have been commenced. Additional experts at Karolinska Biomics Centre and Dept of Clinical Genetics at Karolinska have been contacted and are planned to be involved in the radio nuclear aspects of WP 7, while skilled personnel at ICT and FOI have accepted to be consulted regarding the chemical aspects of this work package. Our plan is to deliver a final WP 7 report by the end of 2009.
Work package n° 8: Contribution of modern Information and Communication Technology
Project leader: Dr. Jon Legarda
List of partners involved (lead in bold)
CEIT, CBRNE Centre, SAMU, FOI, InstRadBio Bw
Objective
To suggest ICT technologies that will improve the over-all effectiveness of the health system to handle C or R emergencies.
Description of the work
The work in WP8 regarding ICT in mass casualty scenarios has been structured as follows:
1. A brief introduction with: a background analysis; the current use cases; European and National organisms.
2. Detection equipments related to field or hospital: type/model; technology on which are based; main features like connectivity, reliability, data processing; autonomy.
3. Communication systems: what type of transmission systems are used; what type of coverage they have; communication standards like GSM, WiFi, dedicated (ISM bands), military bands.
4. Information management: tag type; information flow; data bases (how, when and where the information is managed); security/protocols/encryption.
We have compiled lot of information about detection equipments and we are looking for how the communication systems work and how is done the data management. One of the main references is the WIISARD project (USA) but there are several EU projects so interesting that will provide key information in the final report. All information is general, not specific to the MASH scenarios but for all kind of Radiological and Chemical incidents. In the future we’ll have to particularize each equipment/solution to our scenarios.
We also have compiled some information about chemical, nuclear, radiological and biological agents, decontamination, etc. that could be reviewed by you and we are expecting to have it ready for the meeting in February.
Work package n° 9: Foresight into needs, possibilities and know-ledge gaps for the future
Project leader: Dr. Virginia Murray
List of partners involved (lead in bold)
HPA, CBRNE Centre, SAMU, KI, FOI
Objective
To forecast, prioritise and recommend future improvements of the generic emergency preparedness planning.
Description of the work
It aims to identify and further detail the gaps in scientific knowledge, specialist needs and the tools to support medical emergency responders and others in the area of hazard and risk assessment, triage assessments, decontamination and data collection in mass casualty incidents involving radiation and chemical releases.
A pan-European assessment of coordination actions for hazard and risk assessment, triage, decontamination, medical and fatality management will be made, including guides to decision making using modern technologies and documentation.
Further investigation will describe how cutting-edge advances in biotechnology and medical instrumentation, as well as communication technologies will be implemented in parallel to improve current abilities and minimize the impact of mass casualty incidents in order to suggest an updated and modernized standard for generic preparedness. The foresight will also identify knowledge gaps at a level that may support recommendations for future research.
This work package is built upon all other work; the scenario of interest (WP4), the capabilities and methods used today for handling such events (WP5 and 6), and the potential for biotechnology and ICT tools for addressing current limitations (WP7 and 8). WP9 will take all of this information and detail the way ahead for improved medical management of CR crises.

Mass-casualties and health care following the release of toxic chemicals or radioactive materials
Work Package (WP) 4 deliverable
Scenarios
Gudrun Cassel, Håkan Eriksson and Björn Sandström
Swedish Defence Research Agency, FOI Department of CBRN Defence and Security
901 82 Umeå, Sweden,
http://www.foi.se/ http://www.foi.se/kcc/ E-mail: [email protected]

2008-12-18
2

2008-12-18
3
Contents Background..................................................................................................................... 5 Progress of WP 4 deliverable ........................................................................................ 6 Summary of C-Scenarios ............................................................................................... 7 C-Scenarios .................................................................................................................. 15
Scenario 1: Dispersion of persistent agent in urban area................................................................15
Scenario 2: Release of toxic industrial chemical in semi-closed area .............................................19
Scenario 3: Release of toxic industrial chemical in open space ......................................................23
Scenario 4: Dispersion of unknown toxic liquid in enclosed area ....................................................27
Summary of R-Scenarios ............................................................................................. 31 R-Scenarios .................................................................................................................. 35
Scenario 5: Radiological dispersal in urban area ............................................................................35
Scenario 6: Improvised radiation device (IRD) in enclosed area.....................................................41
References ................................................................................................................... 45

2008-12-18
4

2008-12-18
5
Background Chemicals, that produce harmful effects on people, can spread over a large area after release from storage or transportation facilities. Release may be accidental or deliberate, as in a terrorist chemical attack. Effective management systems are needed to take care of the victims.
Mass emergencies involving toxic chemicals and harmful radiological material are likely to cause an overwhelming burden on pre-hospital care systems. This project deals with the early phases of care-taking process. Scenarios for training of situations that result in medical emergencies following the release of chemical or radiological agents are an important prerequisite for a successful handling of such an event.
Mass emergencies due to toxic chemicals or radioactive materials are complicated since exposures can result in deleterious effects which are not immediately obvious in the traditional triage and evaluation of patients immediately following the incident. Management of the incident scene and how victims will be taken care of varies in different countries throughout the world and is based more on dogma than scientific data (1, 2, 3, 4). The final outcome making early diagnostic assessments difficult due to symptoms correlation with exposures are not obvious. People acutely affected by toxic exposures or from radiation need early medical interventions and at the same time, decontamination of patients if relevant should be performed early in the response efforts, preferably on the scene, to prevent spreading of contamination in surrounding areas, transportation vehicles, and health care facilities. A large number of persons whether seriously affected or not will be seeking medical attention out of fear and anxiety, thus the local health system may be overwhelmed by numerous patients demanding attention. In the Tokyo incident involving the release of the nerve agent sarin into the underground, an estimated 688 of more than 4000 of the patients were transported by ambulance or first responders, the rest were self-evacuated, seeking care in hospital emergency departments (5).
Insufficient research has been conducted in addressing issues on management of mass casualty incidents, especially those involving chemical agents or radiological material. It can even be argued whether the term “mass casualty” has been properly defined. Mass casualty accidents require different approaches than those used in routine emergency response. A large number of affected persons present many logistical problems for both triage and decontamination, many of which impact and overlap the work required for each category of personnel.
For triage, a reliable scheme for categorizing patients according to urgency and type of care is required (6). However, no gold standard for mass casualty triage scheme is available to date. In fact, under normal circumstances, triage decisions are estimated to be only about 80 % accurate (7). There are no consensus triage systems today that include evaluation of CR-effects.
This project is intended to improve the knowledge concerning mass casualty management systems and health care after an incident with chemical agents and radioactive substances.
This part of the project (WP4) will describe scenarios reflecting the needs for competence and capability of medical emergency planners and operators at national and local levels of the member states and their critical efficiency in coping with a mass emergency.
The project is confined to situations where the mass casualties are caused by toxic chemicals and radioactive substances. From these scenarios careful preparedness planning will improve a state’s readiness to communicate with and to actively support the local level. Likewise,
2008-12-18
6
improved preparedness planning and improved methodologies at the local level will increase its efficiency in dealing with and communicating with others about the mass emergency at hand.
The objective is to create a common understanding of the mass emergency situation. The scenarios will serve as a support for the work conducted in following WPs. The scenarios describe situations with serious consequences for the medical management system. Thus it is vital that the resources needed for prioritizing, giving first-aid, decontaminating and transporting patients are accurately and concretely evaluated.
In order to define situations for mass emergencies following chemical release, the generic scenarios from the GSCT project (8; EU-agreement number – 2003217) were further developed and generic scenarios describing situations involving dangerous radioactive material (9) were developed to be used in discussions on generic preparedness planning in the member states.
Progress of WP 4 deliverable The objective of this deliverable is to create a common understanding of mass-casualty situations. It aims to support the response management in the planning of situations where the standard resources are insufficient or the cause of symptoms is difficult to explain. The presented scenarios are also aimed to serve as input to the continued work in other WPs of the project.
Document structure The document consists of a summary of each scenario in the form of a table followed by more detailed descriptions. The detailed description of each scenario has an introductory real event followed by the constructed scenario with an injury panorama. The description also contains information on possible technical counter-measures and a discussion of treatment possibilities. Finally there are some suggestions on what type of substances that could be involved in creating such a scenario.
The last part of the summary table, concerning response management of each event of the different scenarios, has been left unanswered. Those variables are aimed as support to the discussion on the particular needs of preparedness. The results from other WPs could, if preferred, be used to fill “best practice” into those parts of the tables to create complete summaries of the scenarios in the forthcoming final report.
2008-12-18
7
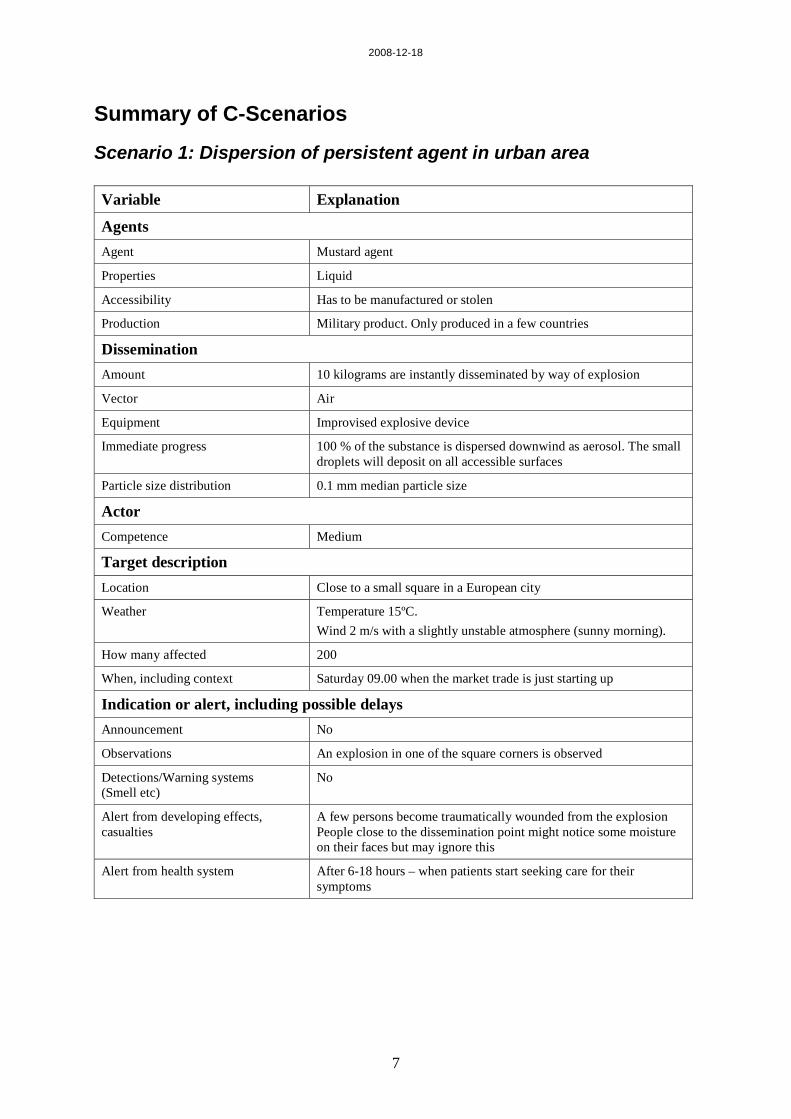
Summary of C-Scenarios
Scenario 1: Dispersion of persistent agent in urban area Variable Explanation
Agents Agent Mustard agent
Properties Liquid
Accessibility Has to be manufactured or stolen
Production Military product. Only produced in a few countries
Dissemination Amount 10 kilograms are instantly disseminated by way of explosion
Vector Air
Equipment Improvised explosive device
Immediate progress 100 % of the substance is dispersed downwind as aerosol. The small droplets will deposit on all accessible surfaces
Particle size distribution 0.1 mm median particle size
Actor Competence Medium
Target description Location Close to a small square in a European city
Weather Temperature 15ºC. Wind 2 m/s with a slightly unstable atmosphere (sunny morning).
How many affected 200
When, including context Saturday 09.00 when the market trade is just starting up
Indication or alert, including possible delays Announcement No
Observations An explosion in one of the square corners is observed
Detections/Warning systems (Smell etc)
No
Alert from developing effects, casualties
A few persons become traumatically wounded from the explosion People close to the dissemination point might notice some moisture on their faces but may ignore this
Alert from health system After 6-18 hours – when patients start seeking care for their symptoms
2008-12-18
8
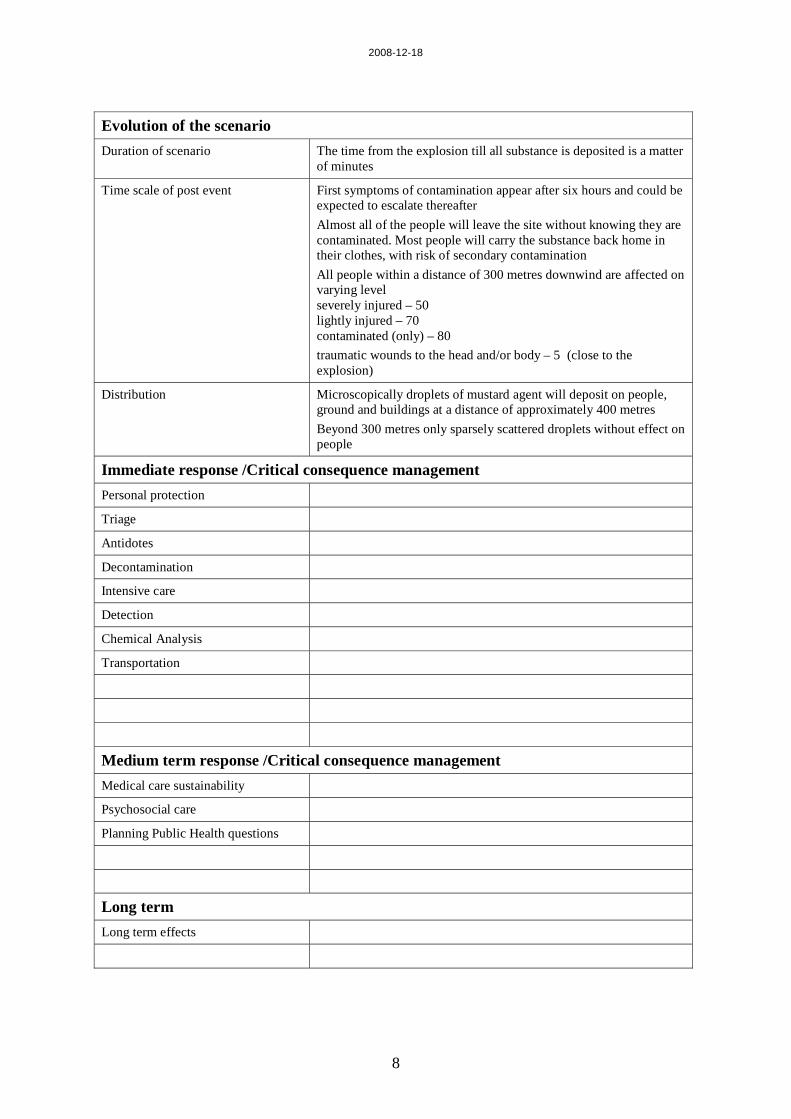
Evolution of the scenario Duration of scenario The time from the explosion till all substance is deposited is a matter
of minutes
Time scale of post event First symptoms of contamination appear after six hours and could be expected to escalate thereafter Almost all of the people will leave the site without knowing they are contaminated. Most people will carry the substance back home in their clothes, with risk of secondary contamination All people within a distance of 300 metres downwind are affected on varying level severely injured – 50 lightly injured – 70 contaminated (only) – 80 traumatic wounds to the head and/or body – 5 (close to the explosion)
Distribution Microscopically droplets of mustard agent will deposit on people, ground and buildings at a distance of approximately 400 metres Beyond 300 metres only sparsely scattered droplets without effect on people
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects

2008-12-18
9
Scenario 2: Release of toxic industrial chemical in semi closed area Variable Explanation
Agents Agent Sulphur dioxide
Properties Liquefied toxic gas Liquid, with low boiling point, stored and transported under pressure
Accessibility Daily transport by road
Production Common industrial chemical
Dissemination Amount 13.5 tons; Common amount in vehicle
Vector Air Vaporises spontaneously when temperature is above -10ºC
Equipment Technical knowledge
Immediate progress 100 % of the content will be spontaneously dispersed to the main part of the grandstand
Particle size distribution Gas
Actor Competence Low
Target description Location Sports arena
Weather Temperature 15ºC with an overcast sky. Wind 2 m/s.
How many affected Approximately 20 000. A major part of the crowd will be affected. Fatal or severe injuries on a large number of spectators. Irritation in eyes and breathing zone may even occur on people outside the arena.
When, including context Warm evening
Indication or alert, including possible delays Announcement No
Observations Some strange activity nearby the service entrance of the arena.
Detections/Warning systems (Smell etc)
Smell
Alert from developing effects, casualties
Fatalities and severe injuries will appear within minutes and will continue up to 24 hours Traumatic wounds fatalities – 1 000 severely injured – 8 000 lightly injured – 10 000 limb fractures – 50 wounds to the head and body – 1 000
Alert from health system No
2008-12-18
10
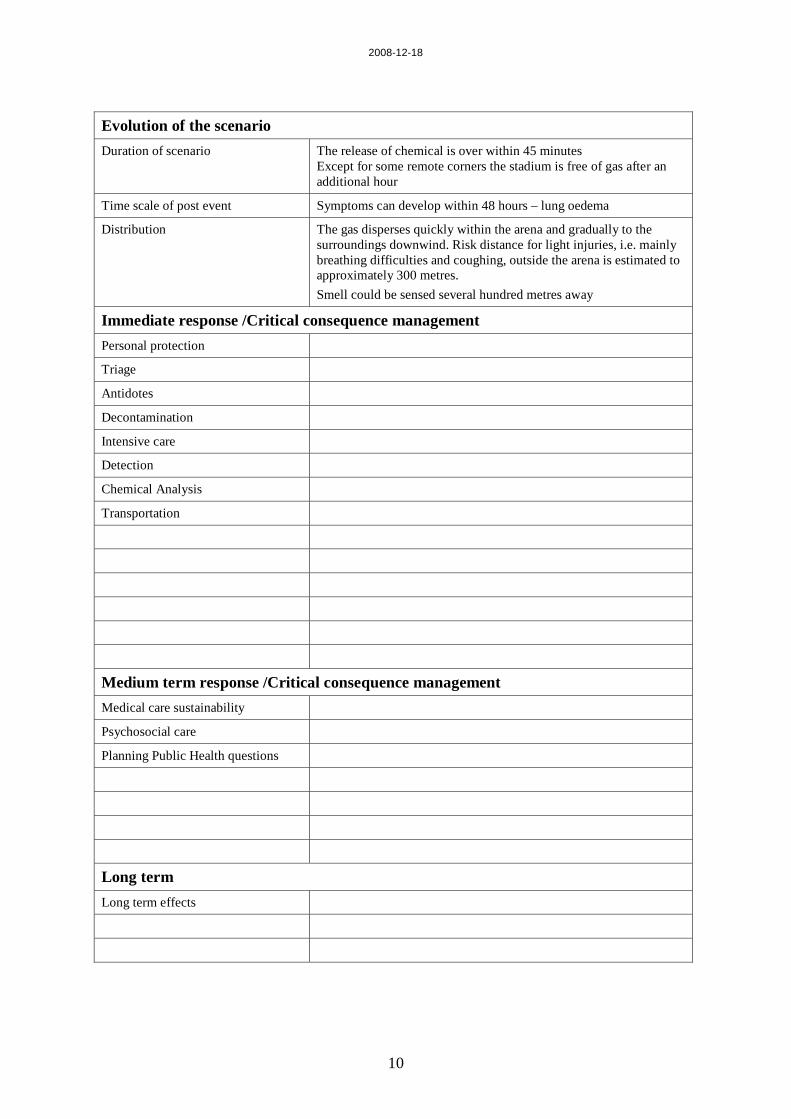
Evolution of the scenario Duration of scenario The release of chemical is over within 45 minutes
Except for some remote corners the stadium is free of gas after an additional hour
Time scale of post event Symptoms can develop within 48 hours – lung oedema
Distribution The gas disperses quickly within the arena and gradually to the surroundings downwind. Risk distance for light injuries, i.e. mainly breathing difficulties and coughing, outside the arena is estimated to approximately 300 metres. Smell could be sensed several hundred metres away
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects

2008-12-18
11
Scenario 3: Release of toxic industrial chemical in open space Variable Explanation
Agents Agent Chlorine
Properties Liquefied toxic gas Liquid, with low boiling point, stored and transported under pressure
Accessibility Daily transports on road and rail
Production Common industrial chemical
Dissemination Amount 33 tons from the total of 65 tons; Common amount in rail tank
Vector Air Vaporises spontaneously when temperature is above -34ºC
Equipment Accident
Immediate progress The content will be spontaneously dispersed into the air. Rescue operation stops the release after half an hour.
Particle size distribution Gas
Actor Competence Not applicable (scenario is an accident)
Target description Location Rail road entering a small town
Weather Temperature 15ºC with a covered sky. Wind 5 m/s.
How many affected 20 000 persons in the area of which 7 500 are directly affected. 90% of the residents are located indoors, 10% outdoors.
When, including context On a warm summer evening
Indication or alert, including possible delays Announcement No
Observations Derailed train, visible yellow gas cloud over the agricultural land close to the event
Detections/Warning systems (Smell etc)
Smell – recognisable by ordinary people
Alert from developing effects, casualties
Severely injuries will appear immediately when cloud passes developed area. fatalities – single (engineer on site) severely injured – 20 lightly injured – 100 irritated air pathways – 1 500
Alert from health system No
2008-12-18
12
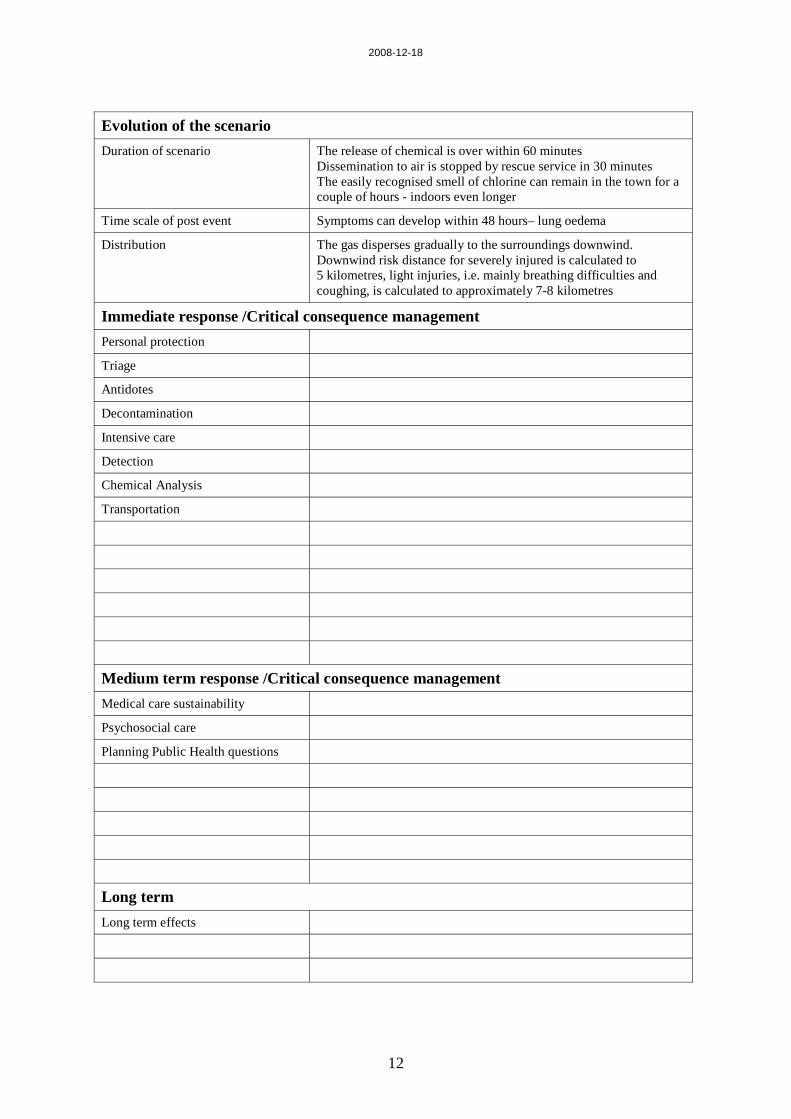
Evolution of the scenario Duration of scenario The release of chemical is over within 60 minutes
Dissemination to air is stopped by rescue service in 30 minutes The easily recognised smell of chlorine can remain in the town for a couple of hours - indoors even longer
Time scale of post event Symptoms can develop within 48 hours– lung oedema
Distribution The gas disperses gradually to the surroundings downwind. Downwind risk distance for severely injured is calculated to 5 kilometres, light injuries, i.e. mainly breathing difficulties and coughing, is calculated to approximately 7-8 kilometres
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects
2008-12-18
13
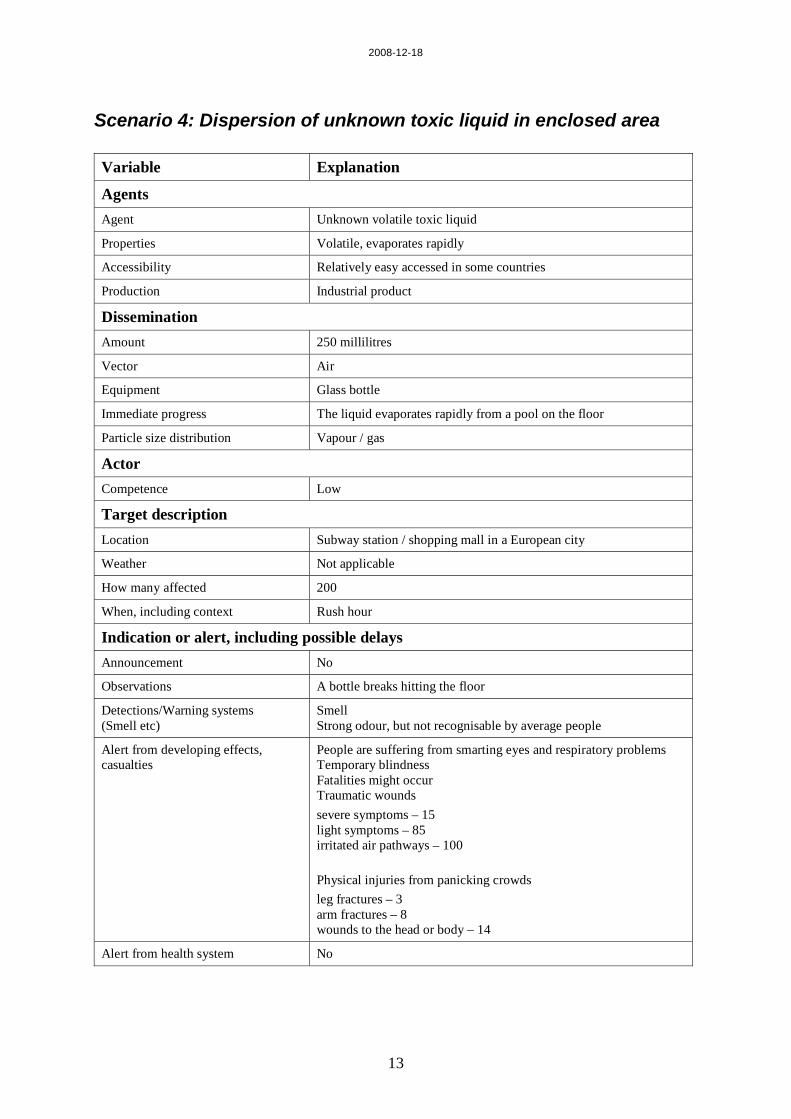
Scenario 4: Dispersion of unknown toxic liquid in enclosed area Variable Explanation
Agents Agent Unknown volatile toxic liquid
Properties Volatile, evaporates rapidly
Accessibility Relatively easy accessed in some countries
Production Industrial product
Dissemination Amount 250 millilitres
Vector Air
Equipment Glass bottle
Immediate progress The liquid evaporates rapidly from a pool on the floor
Particle size distribution Vapour / gas
Actor Competence Low
Target description Location Subway station / shopping mall in a European city
Weather Not applicable
How many affected 200
When, including context Rush hour
Indication or alert, including possible delays Announcement No
Observations A bottle breaks hitting the floor
Detections/Warning systems (Smell etc)
Smell Strong odour, but not recognisable by average people
Alert from developing effects, casualties
People are suffering from smarting eyes and respiratory problems Temporary blindness Fatalities might occur Traumatic wounds severe symptoms – 15 light symptoms – 85 irritated air pathways – 100 Physical injuries from panicking crowds leg fractures – 3 arm fractures – 8 wounds to the head or body – 14
Alert from health system No

2008-12-18
14
Evolution of the scenario Duration of scenario The liquid evaporates and is gone within 15 minutes
Time scale of post event Symptoms can develop within 48 hours – lung oedema
Distribution Gas concentrations in the air will gradually dilute to give only a slight smell within one hour and eventually disappear A slight smell might be sensed through the tunnel system to the nearby stations
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects
2008-12-18
15
C-Scenarios
Scenario 1: Dispersion of persistent agent in urban area
A bomb under a truck killed at least one person and wounded five in Istanbul yesterday, a day after 13 people died in an arson attack in the city. Explosive experts defused a second bomb planted inside a crowded Burger King restaurant on the outskirts of the city, the Anatolia news agency said. Since the capture of Kurdish rebel leader Abdullah Ocalan, Turkey has witnessed a sharp increase in violence, including a suicide bomb attack and violent street clashes.
Associated Press
What if…? The perpetrators are in possession of an appropriate amount of mustard agent and the knowledge of handling it…
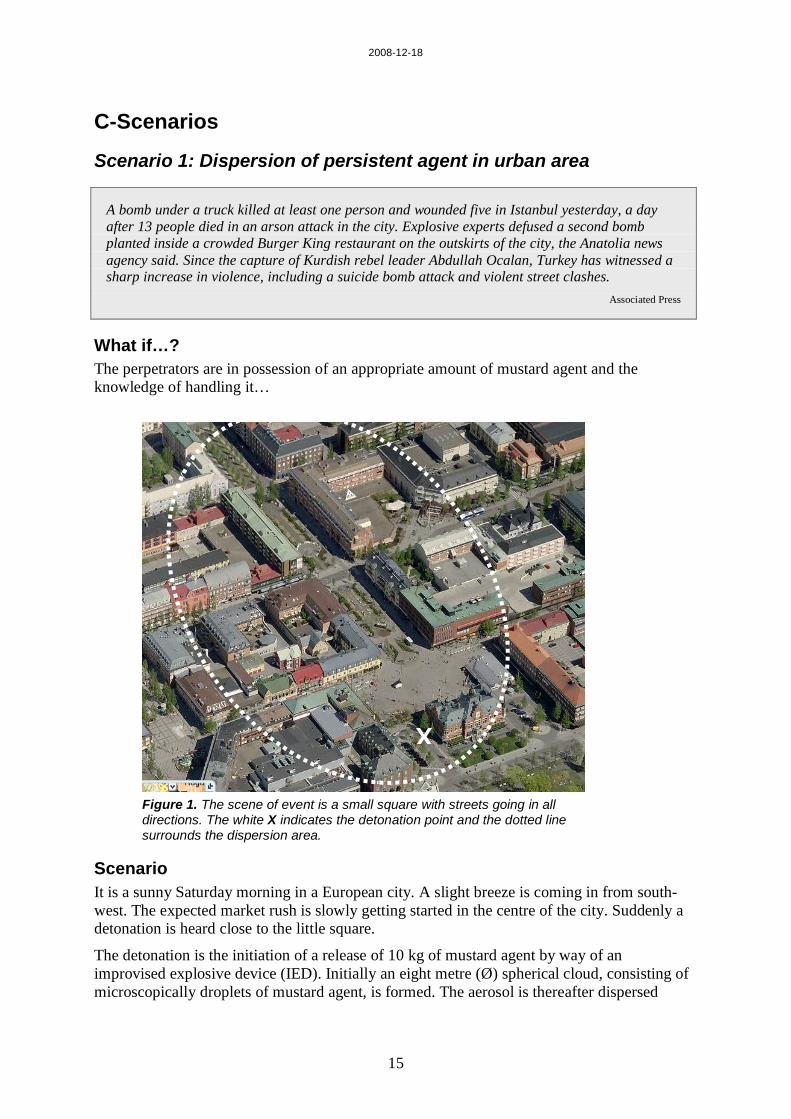
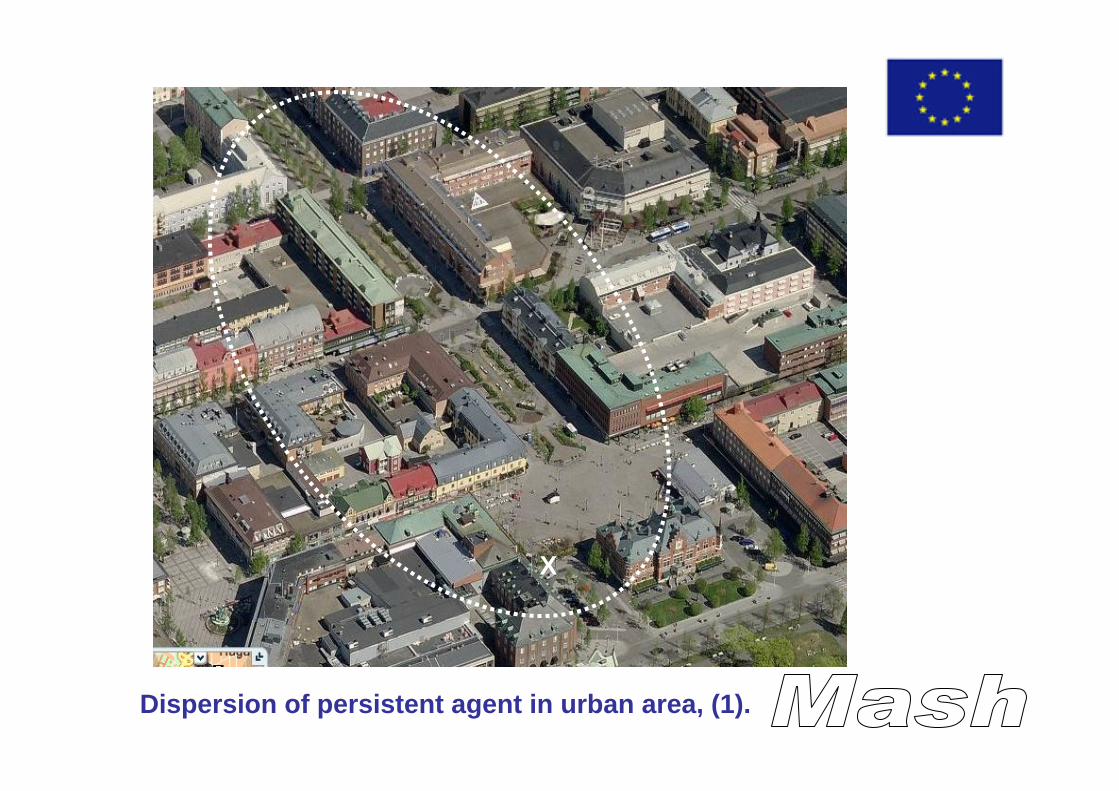
Figure 1. The scene of event is a small square with streets going in all directions. The white X indicates the detonation point and the dotted line surrounds the dispersion area.
Scenario It is a sunny Saturday morning in a European city. A slight breeze is coming in from south-west. The expected market rush is slowly getting started in the centre of the city. Suddenly a detonation is heard close to the little square.
The detonation is the initiation of a release of 10 kg of mustard agent by way of an improvised explosive device (IED). Initially an eight metre (Ø) spherical cloud, consisting of microscopically droplets of mustard agent, is formed. The aerosol is thereafter dispersed
X
2008-12-18
16
downwind. People outdoor will be exposed to the aerosol when it deposits on all accessible surfaces.
Assumptions The affected area is assumed to hold 60 persons in the little square and 140 persons on the avenue leading northerly from the square, equally distributed over the area.
Rescue service No technical counter-measures will be possible in such an event. The main tasks will be to find and help injured persons and to prevent people from entering the area.
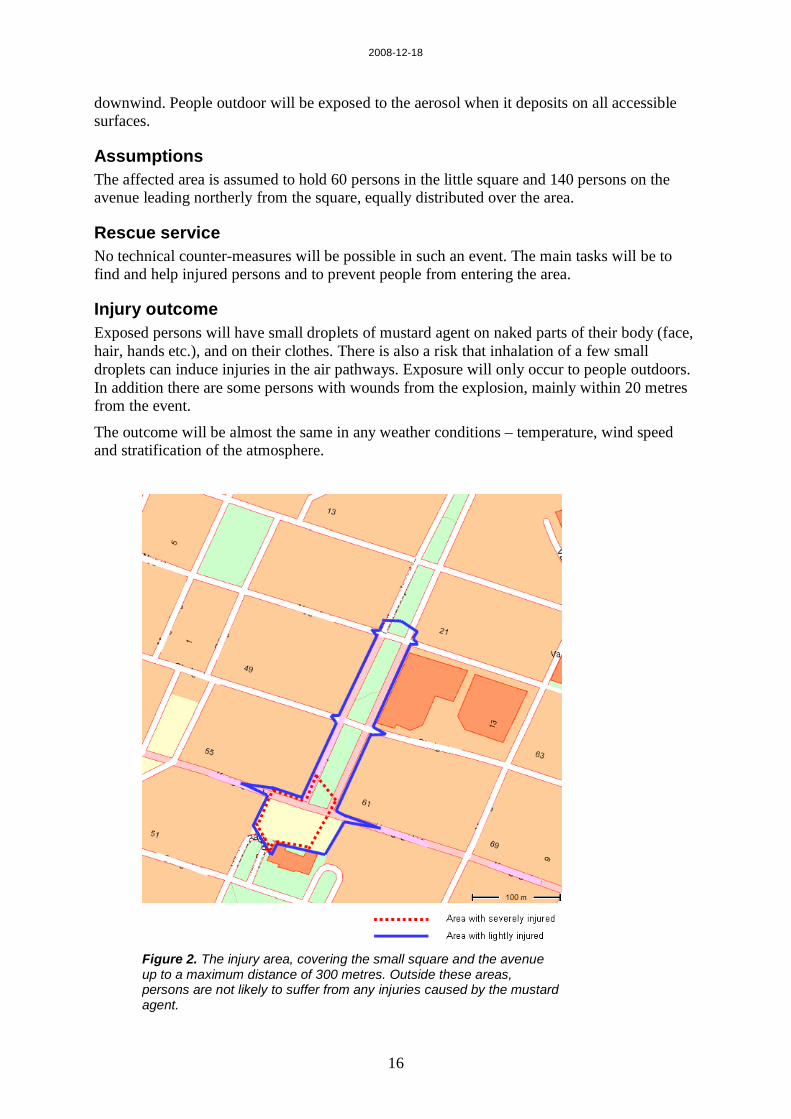
Injury outcome Exposed persons will have small droplets of mustard agent on naked parts of their body (face, hair, hands etc.), and on their clothes. There is also a risk that inhalation of a few small droplets can induce injuries in the air pathways. Exposure will only occur to people outdoors. In addition there are some persons with wounds from the explosion, mainly within 20 metres from the event.
The outcome will be almost the same in any weather conditions – temperature, wind speed and stratification of the atmosphere.
Figure 2. The injury area, covering the small square and the avenue up to a maximum distance of 300 metres. Outside these areas, persons are not likely to suffer from any injuries caused by the mustard agent.

2008-12-18
17
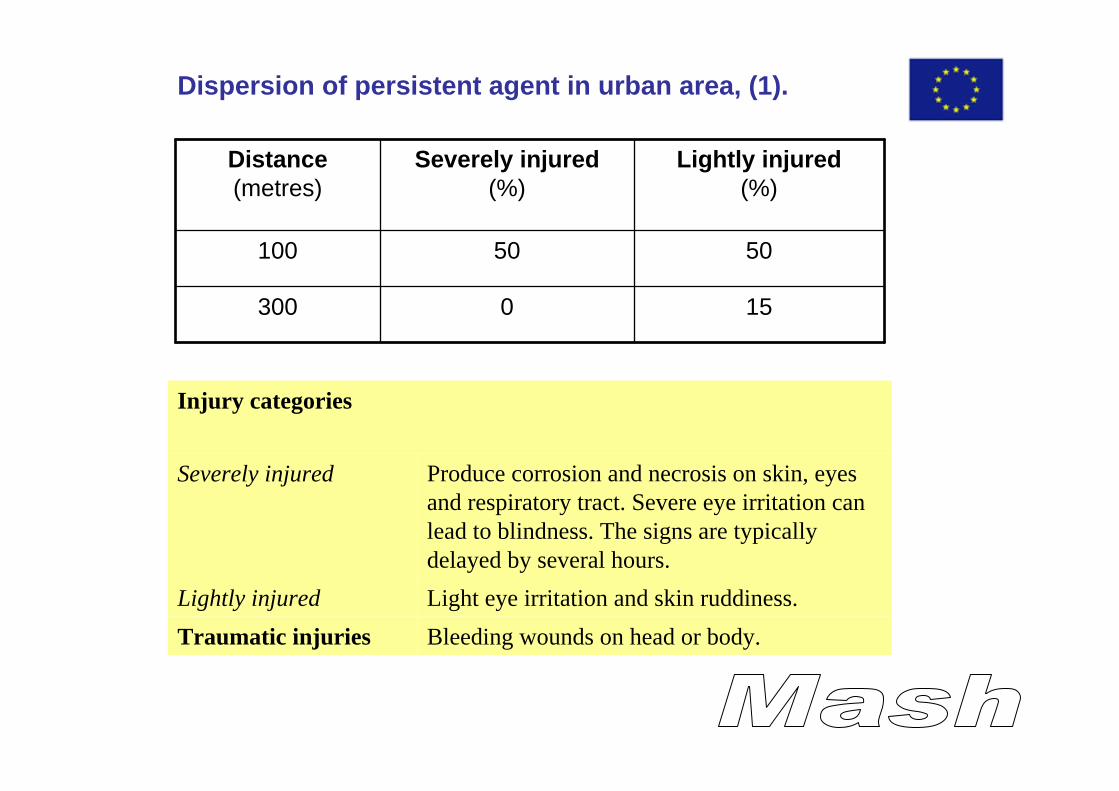
Table 1. Injury distribution downwind the release point. The distribution of severely injured will be higher at shorter distances and lower farther away from the event.
Distance (metres)
Severely injured (%)
Lightly injured (%)
100 50 50
300 0 15
Calculated for the number of persons present, there are 40 severely injured and 20 lightly injured in the square. In the avenue there are 10 severely, 50 lightly injured and 80 that are uninjured but slightly contaminated – by a few microscopic droplets.
Five persons are also suffering from additional wounds as a consequence of the detonation.
Injury categories
Severely injured Early upper respiratory prodromal symptoms – sneezing and rhinorrheoa
Eye irritation and conjunctivitis. Severe eye irritation can lead to blindness. Blisters appear on the skin and there may be inflammation and necrosis of the respiratory tract with severe cough and breathing difficulties. The symptoms and signs are typically delayed by several hours.
Lightly injured Slight conjunctivitis irritation and skin inflammation
Traumatic injuries
Bleeding wounds on head or body.
Treatment The main problem in a scenario like this is the prolonged period (latency) until the symptoms appear. This can last from six to eighteen hours before the first symptoms are revealed. In the best of worlds, the rescue service will detect the agent and the right measures will be accomplished, but a non-surprisingly outcome of this scenario might be that they just clean up after the explosion and consider the case closed.
If the agent is detected, the measures will be undressing, decontamination of exposed skin and thereafter symptomatic treatment for chemical burns. There are no available explicit methods for medical treatment of injuries caused by mustard agent.
If the agent not is detected the health care personnel have to be observant enough to solve the mystery when patients start to seek care. In that case there will be no effect of decontamination and the medical measures are symptomatic treatment for burns.
Additionally, recommendations to wash the clothes worn have to be announced to people who visited the site during the day.
In either case there is a need for treatment of the traumatic injuries due to the explosion. Doing so, attention has to be paid to the risk for secondary contamination to health care personnel. In the latter case the risk of injuries to caring personnel is imminent. A massive need for information to all anxious people has to be considered.

2008-12-18
18
Decontamination of ground and buildings might come into question.
Possible agents Possible substances for a scenario like this are persistent chemical warfare agents, persistent pesticides and other low-volatile highly toxic liquids.

2008-12-18
19
Scenario 2: Release of toxic industrial chemical in semi-closed area
In 1985, a disastrous fire at the Valley Parade Stadium in Bradford eventually claimed the lives of 56 football supporters. In addition, about 250 of the most injured overwhelmed resources at local hospitals. At least a further 200 persons needed first aid treatment at the ground. What started as a small fire in one point of the stand spread quickly and within three minutes the whole of the roof and the wooden stands below were on fire and police struggled to save those who were too stunned or weak to escape. BBC
What if…? It wasn’t an accidental fire but an ill-intentioned manoeuvre to create panic in the society and additionally injure a lot of people. Then it could give huge consequences to use an event with a big crowd gathered to celebrate a large sports event…
Figure 3. During the event the stadium is crowded, carrying its capacity of 20.000 spectators.
Scenario There is a warm evening in a major city. The city’s favourite football team is preparing for a European championship game against a team from another European city. The grand-stand of the stadium is being filled with enthusiastic supporters from both teams. The stadium has a capacity of 20 000 spectators.
At the same hour on the route leading through the city, there is a tanker lorry passing. The tanker contains sulphur dioxide. On a roadside parking area the lorry is stopped by two persons, dressed like policemen. The driver is drugged and put aside whilst the lorry is hi-jacked and driven towards the stadium. Just at the start of the game, the lorry forces itself into the stadium through the service entrance. The two men, wearing breathing protection, jump out of the lorry and quickly open the valves to release the contents of the tank. After doing so,
2008-12-18
20
they disappear the same way they arrived. The sulphur dioxide is released at a rate of approximately 5 kg/s, i.e. the tank will be emptied in approximately 45 minutes.
In the stands nobody has noticed the little episode in one corner of the stadium. The spectators start reacting when panic is breaking out in the south east corner of the stadium. After a couple of minutes the security organisation of the event realises that the situation is serious and orders evacuation of the stadium. Under orderly conditions the full stadium can be evacuated in 20 minutes. In this situation, with people stampeding, it will not be as quick.
Rescue service The rescue services manage to make relevant technical counter-measures to diminish the dispersion to air after 30 minutes. Such measures are theoretically possible, but demand a very well planned, educated, trained and equipped organisation. The hereafter released sulphur dioxide will be taken care of by the rescue services and is not of any further concern to the outcome of the event.
Injury outcome The main consequence from the event will be injuries in eyes and air pathways due to exposure to sulphur dioxide. Additionally, there will most certainly be a high number of traumatic injuries created by the panicking crowd.
The number of injured from inhaling the chemical is increasing during the whole course, but sulphur dioxide implies that the essential injury level is reached already within a few minutes. The reason is that the inhaled concentration is more significant than the exposure time. The phenomenon is indicated in figures 2-7, showing the distribution of injured by level of injury after 5 and 30 minutes, respectively.
After half an hour the death toll has reached 1 000 persons. As many as 8 000 persons are suffering from severe injuries and approximately 10 000 are lightly injured. Some of the lightly injured are located outside the stadium, at a maximum distance of 300 metres, but the great majority are inside the stadium.
In addition there are 50 persons suffering from limb fractures and 1 000 persons suffering from moderate to severe traumatic wounds to the head and body caused by collisions to other people or building parts and falling in staircases.
Injury categories
Fatally injured Rapidly lethal, serious lung oedema and suffocation.
Severely injured Severe effect on the eyes as corneal burns and vision loss, severe difficulties in breathing, chest pain and weakness. Risk for permanent pulmonary and eye injuries. Lung oedema, chemical induced pneumonia and pleurisy can occur up to a few days after the exposure. This category needs immediate emergency care.
Lightly injured Considerable irritation in eyes and breathing pathways with symptoms as cough and chest pain. The symptoms are so painful that persons are likely to seek medical care.
Irritation Moderate to severe irritation in eyes and upper air passages, irritating cough. The symptoms will subside shortly after exposure is terminated.
Traumatic injuries Limb fractures and bleeding wounds on head or other body parts
2008-12-18
21
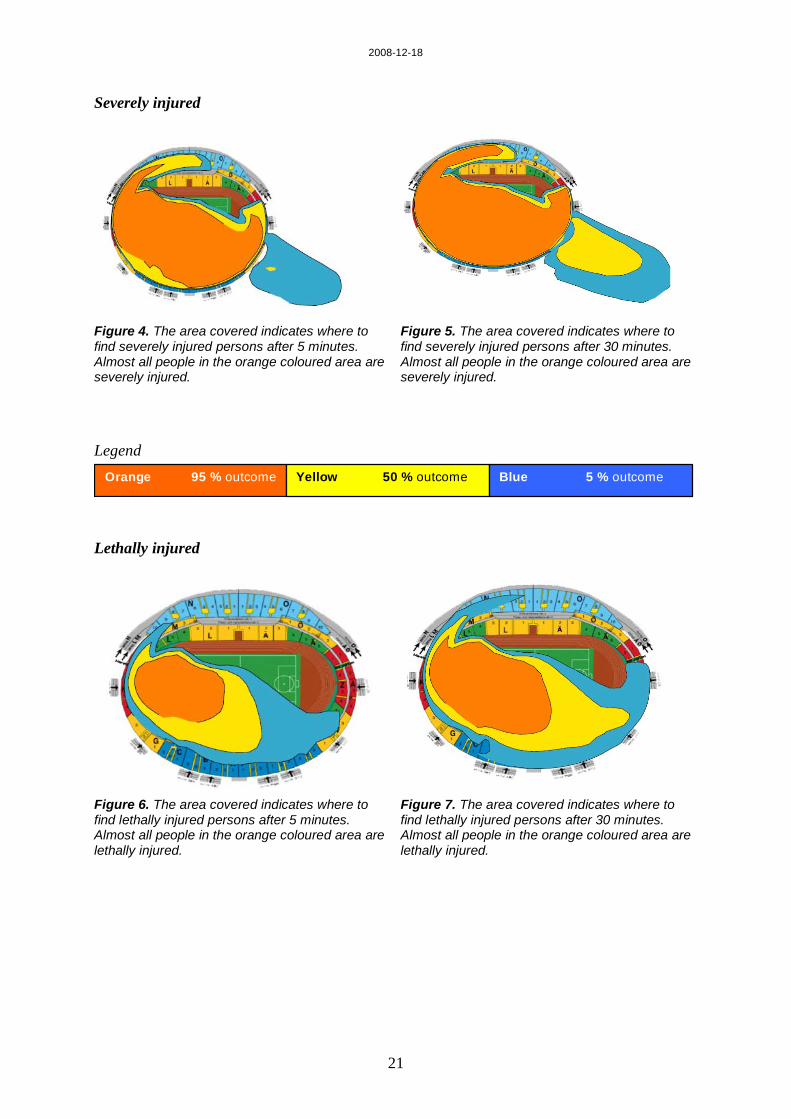
Severely injured
Figure 4. The area covered indicates where to find severely injured persons after 5 minutes. Almost all people in the orange coloured area are severely injured.
Figure 5. The area covered indicates where to find severely injured persons after 30 minutes. Almost all people in the orange coloured area are severely injured.
Legend
Lethally injured
Figure 6. The area covered indicates where to find lethally injured persons after 5 minutes. Almost all people in the orange coloured area are lethally injured.
Figure 7. The area covered indicates where to find lethally injured persons after 30 minutes. Almost all people in the orange coloured area are lethally injured.
Orange 95 % outcome Yellow 50 % outcome Blue 5 % outcome

2008-12-18
22
Lightly injured
Figure 8. The area covered indicates where to find lightly injured persons after 5 minutes. Almost all people in the orange coloured area are injured. The area reaches about 300 metres outside the stadium.
Figure 9. The area covered indicates where to find lightly injured persons after 30 minutes. Almost all people in the orange coloured area are injured. The area reaches about 300 metres outside the stadium.
Treatment Medical treatment for injuries caused by inhaling sulphur dioxide is exclusively symptomatic. Oxygen and medicines for treatment of asthmatic symptoms are relevant in this case. The corrosive effect on the eyes has to be interrupted by rinsing.
The need of acute life-saving decontamination is over all non-existing, regarding the type of chemical, gas, and positions of persons in relation to the location of the release. Undressing could be relevant for a few, but staying outdoors, in fresh air, for a few minutes will make most of the exposed persons harmless to medical first responders.
A massive information demand could be expected.
Possible agents Possible substances for a scenario like this are other liquefied toxic industrial gases such as chlorine, hydrogen chloride or ammonia. The injury outcome and treatment methods will be similar for many of the representatives of this type of chemicals, but the actual number of injured can be expected to vary with the substance.
Similar outcome could be expected from use of volatile nerve agents. In such cases a successful treatment is dependent on early life support and the rapid distribution of antidotes.

2008-12-18
23
Scenario 3: Release of toxic industrial chemical in open space
Just before 1.00 pm on Monday, February 28 in 2005, a freight train derailed in the vicinity of Kungsbacka, Sweden. The train carried 12 tank wagons, each of them containing 65 tons of chlorine. The cause of the accident was that the freight train went out on a blind track to await a meeting train. The attempts to stop the train failed and the engine and four of the wagons derailed into the surrounding field. Fortunately none of the tanks were damaged. Göteborgsposten
Figure 10. The derailed part of the train which has come to a halt, awaiting the rescue vehicles.
What if…? The event occurs on a summer evening and one chlorine tank is damaged…
Scenario A freight train derails about one kilometre before entering a small town. The train is carrying chlorine wagons – each containing 65 tons of chlorine. One vessel is punctured and the contents are continuously released into the air during one hour, corresponding to a hole of approximately 8 mm2. The continuous release creates a plume of gas downwind, which has relatively constant concentrations on given distances from the release. Some variations in gas concentrations will appear due to air turbulence. The main wind direction is straight towards the small town.
Due to the time of day (early evening) and the fine weather, most of the people are at their homes and approximately 10% of them are located outdoors, hence 90% are staying indoors. The nearest residential area, in the wind direction, is located at a distance of approximately two kilometres from the event.
Rescue service The rescue services manage to make relevant technical counter-measures to diminish the dispersion to air after 30 minutes. Such measures are theoretically possible, but demand a very well planned, educated, trained and equipped organisation. The chlorine released subsequently will be taken care of by the rescue services and is not of any further concern to the outcome of the event.

2008-12-18
24
Injury outcome The outcome, expressed in number of injured persons was one fatality (the train driver), approximately 20 severely injured and 100 lightly injured. In addition, it is expected that some 1 500 persons suffer from moderate to severe irritation in the respiratory pathways.
The distribution of the number of injured, outdoors and indoors respectively, is shown in table 2 below.
Figure 11. Areas representing different levels of injury outdoors after release of 33 tons of chlorine during 30 minutes. The various areas, in different colours, represent the areas where it could be expected to find persons suffering from injuries at the four levels indicated, from irritation to fatal injuries.
Figure 12. Areas representing different levels of injury indoors after release of 33 tons of chlorine during 30 minutes. The various areas, in different colours, represent the areas where it could be expected to find persons suffering from injuries at the four levels.
Table 2. Number of injured persons outdoors and indoors, distributed in four different injury levels.
Injury level Outdoors Indoors Total
Fatal 1 0 1
Severe 10 10 20
Light 50 50 100
Irritation 400 1100 1500
2008-12-18
25
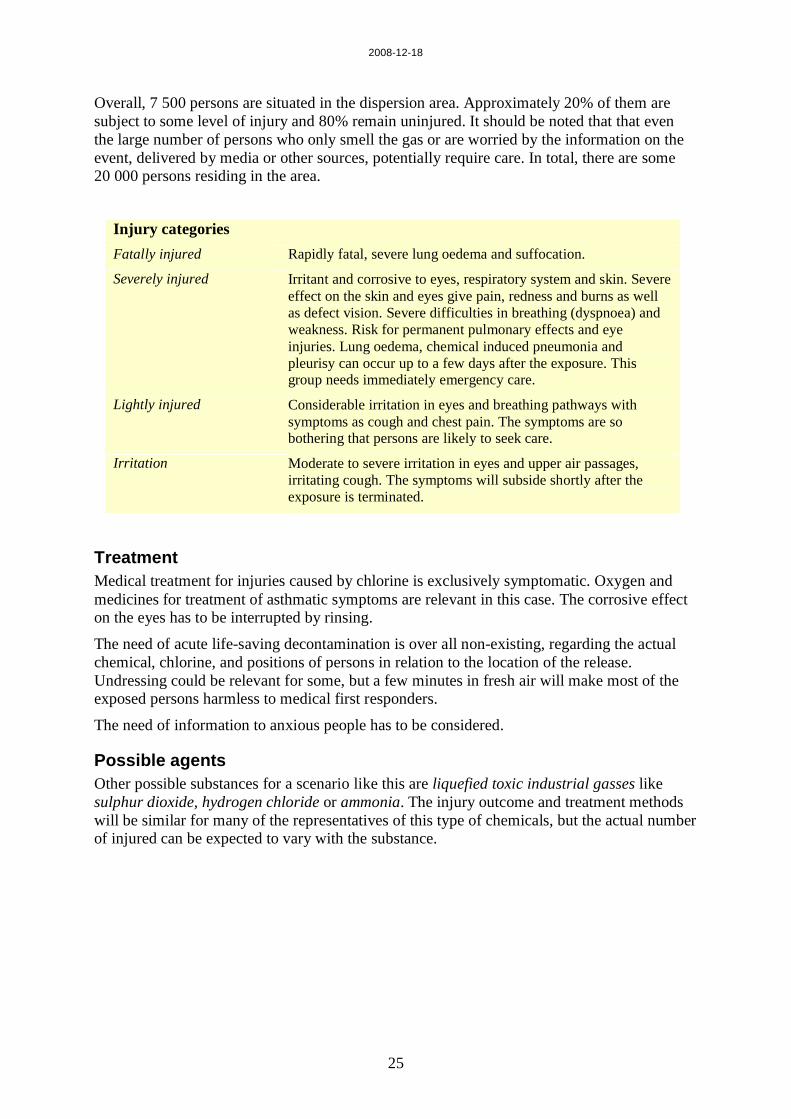
Overall, 7 500 persons are situated in the dispersion area. Approximately 20% of them are subject to some level of injury and 80% remain uninjured. It should be noted that that even the large number of persons who only smell the gas or are worried by the information on the event, delivered by media or other sources, potentially require care. In total, there are some 20 000 persons residing in the area.
Injury categories Fatally injured Rapidly fatal, severe lung oedema and suffocation.
Severely injured Irritant and corrosive to eyes, respiratory system and skin. Severe effect on the skin and eyes give pain, redness and burns as well as defect vision. Severe difficulties in breathing (dyspnoea) and weakness. Risk for permanent pulmonary effects and eye injuries. Lung oedema, chemical induced pneumonia and pleurisy can occur up to a few days after the exposure. This group needs immediately emergency care.
Lightly injured Considerable irritation in eyes and breathing pathways with symptoms as cough and chest pain. The symptoms are so bothering that persons are likely to seek care.
Irritation Moderate to severe irritation in eyes and upper air passages, irritating cough. The symptoms will subside shortly after the exposure is terminated.
Treatment Medical treatment for injuries caused by chlorine is exclusively symptomatic. Oxygen and medicines for treatment of asthmatic symptoms are relevant in this case. The corrosive effect on the eyes has to be interrupted by rinsing.
The need of acute life-saving decontamination is over all non-existing, regarding the actual chemical, chlorine, and positions of persons in relation to the location of the release. Undressing could be relevant for some, but a few minutes in fresh air will make most of the exposed persons harmless to medical first responders.
The need of information to anxious people has to be considered.
Possible agents Other possible substances for a scenario like this are liquefied toxic industrial gasses like sulphur dioxide, hydrogen chloride or ammonia. The injury outcome and treatment methods will be similar for many of the representatives of this type of chemicals, but the actual number of injured can be expected to vary with the substance.

2008-12-18
26
2008-12-18
27
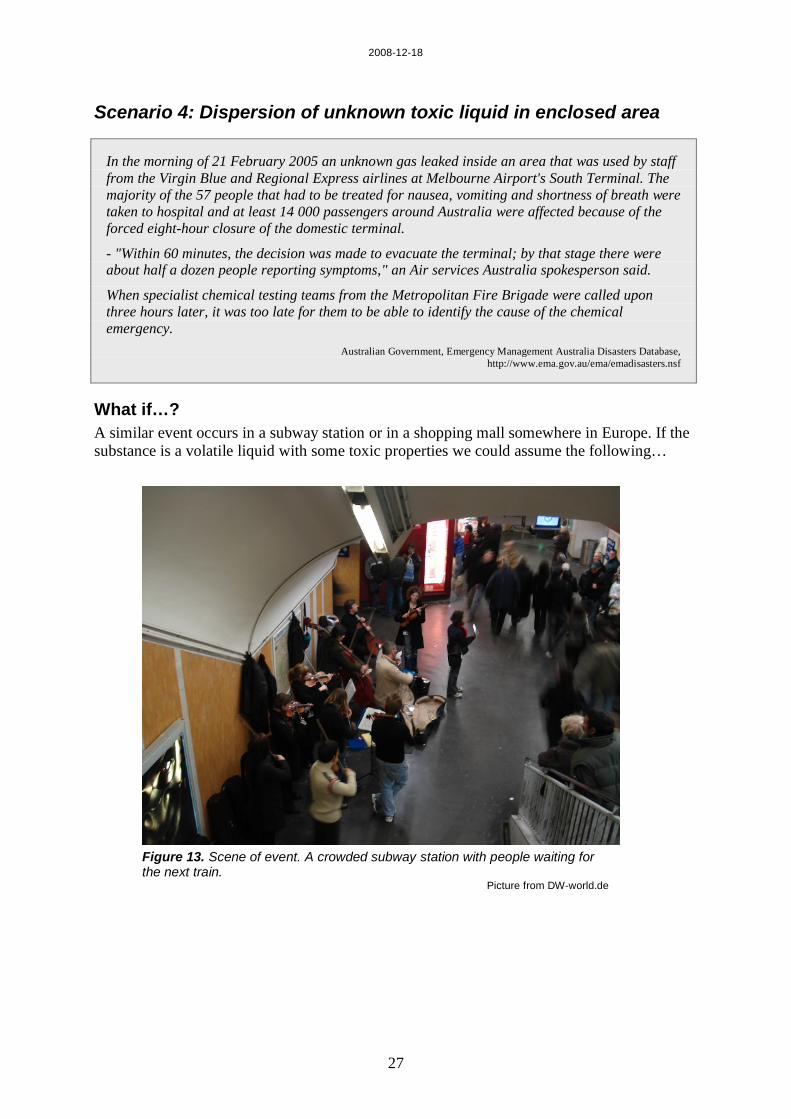
Scenario 4: Dispersion of unknown toxic liquid in enclosed area
In the morning of 21 February 2005 an unknown gas leaked inside an area that was used by staff from the Virgin Blue and Regional Express airlines at Melbourne Airport's South Terminal. The majority of the 57 people that had to be treated for nausea, vomiting and shortness of breath were taken to hospital and at least 14 000 passengers around Australia were affected because of the forced eight-hour closure of the domestic terminal.
- "Within 60 minutes, the decision was made to evacuate the terminal; by that stage there were about half a dozen people reporting symptoms," an Air services Australia spokesperson said.
When specialist chemical testing teams from the Metropolitan Fire Brigade were called upon three hours later, it was too late for them to be able to identify the cause of the chemical emergency. Australian Government, Emergency Management Australia Disasters Database, http://www.ema.gov.au/ema/emadisasters.nsf
What if…? A similar event occurs in a subway station or in a shopping mall somewhere in Europe. If the substance is a volatile liquid with some toxic properties we could assume the following…
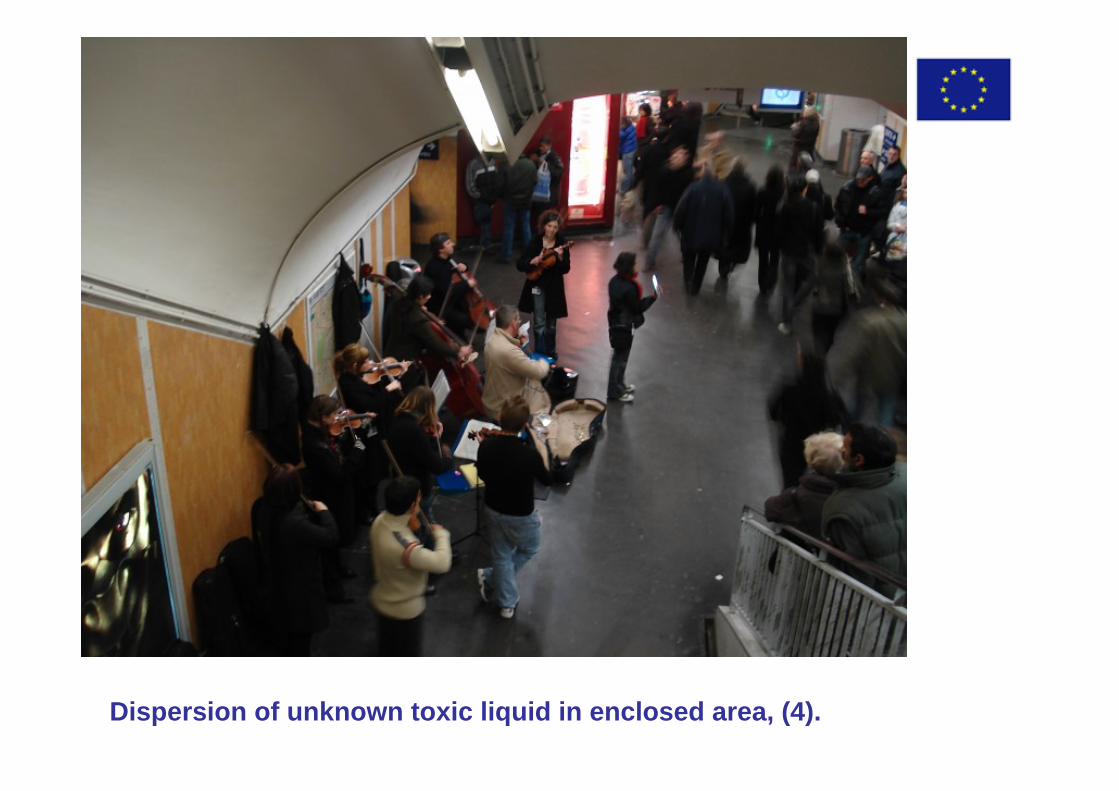
Figure 13. Scene of event. A crowded subway station with people waiting for the next train.
Picture from DW-world.de

2008-12-18
28
Scenario During the rush-hour, an assailant throws a small bottle down the staircase in a subway station. The bottle breaks, hitting the floor, and a liquid pool is formed. After a few seconds the first persons start coughing. Shortly, panic breaks out when people try to leave the station to reach fresh air.
The substance is volatile and evaporates spontaneously. The concentration of the substance is enough to make people instantly unable to help themselves, due to temporary blindness and severe difficulties to breath. The concentration dilutes by air movement and ventilation farther away from the event (see figure 14).
Assumptions The number of persons in the affected part of the station is 200.
Rescue service The substance is completely evaporated within 15 minutes. In such a short time no technical counter-measures will be possible. The main task for the rescue services will be to organise the evacuation of persons that can’t find the way out by their own.
Injury outcome Exposed persons react instantly with cough and tear-running eyes. Close to the event the symptoms are severe, with temporary blindness and severe difficulties in breathing. Problems with seeing make it, in addition to the panic, even harder to carry out a rapid evacuation. Persons remaining in the highest concentrations for a few minutes might develop pulmonary oedema within a couple of days.
In addition there are some traumatic injuries, due to the panic.
Due to air movements in the tunnel system, stations nearby might be object to the smell of the substance, which can cause some anxiety.
Table 3. Injury outcome after exposure to the vapour and additional traumatic wounds.
Injury level from exposure
Number of injured from
exposure
Number of arm fractures
Number of leg fractures
Number of wounded on head or body
Severely injured 15 3 2 7
Lightly injured 85 4 1 3
Irritation 100 1 4

2008-12-18
29
Figure 14. Affected area in the subway station. Train movements help to carry contaminated air onto the platforms.
Injury categories Severely injured Severe eye irritation, temporary blindness. Severely irritating effect
on breathing pathways. Risk of pulmonary oedema.
Lightly injured Lachrymation. Moderate to severe cough.
Irritation Slightly sore throat, light cough, lightly irritated eyes.
Traumatic injuries Fractures and bleeding wounds on head or other body parts caused by collisions with other people or building parts and falling in staircases.
Treatment Since the substance is unidentified it is impossible to decide any specific antidote. The measures will be to bring people out to fresh air and treat the symptoms. Oxygen treatment might be essential in severe cases. Treatment of traumatic injuries has to be considered.
The need for the provision information to anxious people is likely to be considerable.
Possible agents Possible substances for a scenario like this are volatile chemical warfare agents, volatile pesticides and other volatile highly toxic or incapacitating liquids. Depending of the actual agent the treatment methods can vary. For some chemicals it might be essential to provide early life support and to distribute antidotes rapidly while other chemicals only can be treated symptomatically.

2008-12-18
30
2008-12-18
31
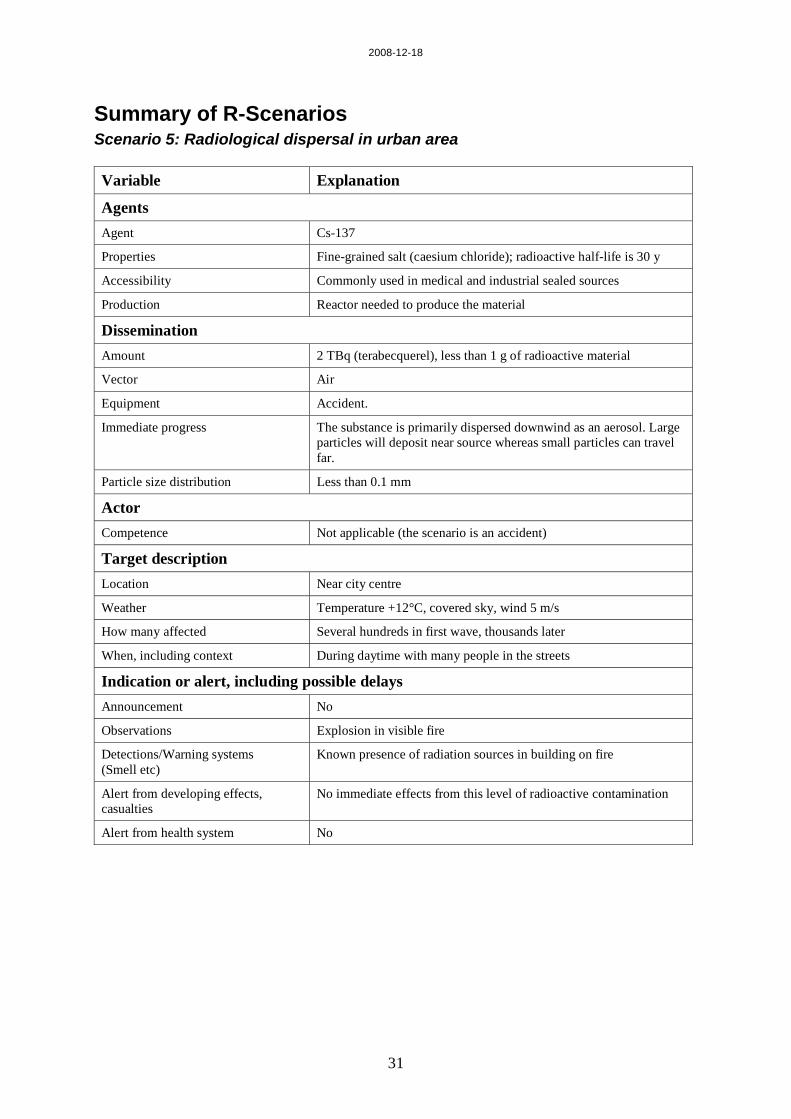
Summary of R-Scenarios Scenario 5: Radiological dispersal in urban area Variable Explanation
Agents Agent Cs-137
Properties Fine-grained salt (caesium chloride); radioactive half-life is 30 y
Accessibility Commonly used in medical and industrial sealed sources
Production Reactor needed to produce the material
Dissemination Amount 2 TBq (terabecquerel), less than 1 g of radioactive material
Vector Air
Equipment Accident.
Immediate progress The substance is primarily dispersed downwind as an aerosol. Large particles will deposit near source whereas small particles can travel far.
Particle size distribution Less than 0.1 mm
Actor Competence Not applicable (the scenario is an accident)
Target description Location Near city centre
Weather Temperature +12°C, covered sky, wind 5 m/s
How many affected Several hundreds in first wave, thousands later
When, including context During daytime with many people in the streets
Indication or alert, including possible delays Announcement No
Observations Explosion in visible fire
Detections/Warning systems (Smell etc)
Known presence of radiation sources in building on fire
Alert from developing effects, casualties
No immediate effects from this level of radioactive contamination
Alert from health system No
2008-12-18
32
Evolution of the scenario Duration of scenario Radioactive release follows immediately after the explosion.
Radioactive particles travel air-borne until deposited on the ground. Resuspension of particles may occur. Decontamination of people and environment will be needed – size of area necessary to decontaminate will be matter of discussion.
Time scale Depending on success of authorities to reassure the public that the situation is under control.
Distribution The radioactive fallout is primarily distributed downwind, but in urban areas activity will also travel sideways following direction of streets.
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects

2008-12-18
33
Scenario 6: Improvised radiation device (IRD) in enclosed area Variable Explanation
Agents Agent Ir-192
Properties Sealed source; small radioactive bars inside metal container. Radioactive half-life is 74 days.
Accessibility Commonly used in industrial and medical sources
Production Reactor or other powerful neutron generator needed to produce the material.
Dissemination Amount 5.5 TBq contact dose of ~100 Sv / min, at 1 m:
Vector Non-applicable
Equipment Non-specific, several methods to prevent direct handling of the source with fingers
Immediate progress Distance-to-source-dependent irradiation
Particle size distribution Non-applicable
Actor Competence Competent in handling radioactive source
Target description Location Public transport vehicle
Weather Non-important
How many affected Only a few on day 1, several hundreds – thousands from day 2
When, including context During daytime
Indication or alert, including possible delays Announcement No
Observations Passengers with local radiation damage on lower legs, cleaner with locally irradiated fingers
Detections/Warning systems (Smell etc)
Detection instrument
Alert from developing effects, casualties
Erythema on lower legs, nausea, vomiting
Alert from health system Yes

2008-12-18
34
Evolution of the scenario Duration of scenario Irradiation following deliberate positioning of radioactive source on
vehicle for public transport. Scenario ends when source is competently taken care of and put in lead shield. Decontamination of people or environment will NOT be needed if source is kept intact.
Time scale In the first stage depending on observant medical staff and later success of authorities to reassure the public that the situation is under control.
Distribution Radiation intensity follows the inverse-square law, which means that at any distance from the source the dose rate will be four times higher at half this distance.
Immediate response /Critical consequence management Personal protection
Triage
Antidotes
Decontamination
Intensive care
Detection
Chemical Analysis
Transportation
Medium term response /Critical consequence management Medical care sustainability
Psychosocial care
Planning Public Health questions
Long term Long term effects

2008-12-18
35
R-Scenarios
Scenario 5: Radiological dispersal in urban area
On 2 January 2008, a major fire broke out at the Royal Marsden Hospital in Chelsea in west London. In all, about 200 staff, 79 patients and an equal number of out-patients were evacuated. Several patients unable to walk by themselves had to be placed on mattresses in a nearby street while those in better condition could be led away.
About 25 fire vehicles, ten ambulances and a special hazardous area response team were sent to the scene after the alarm. Streets in the area were blocked off by volunteer police officers and the smoke was felt in a large are of London.
Royal Marsden Press Release, Fire at The Royal Marsden, and related news articles.
What if…? Royal Marsden Hospital is a world-renowned cancer treating hospital. As such, the hospital has an inventory of radiation sources. This inventory was not damaged by the fire in January 2008.
For scenario 5, we will assume that a medical clinic that keeps radiation sources is hit by an accidental fire. The high temperature leads to the destruction of lead shields covering sources. An explosion ruptures a source containing caesium-137 in the form of caesium chloride and the radioactive material is subsequently spread over the neighbourhood.
Scenario St. Peregrine Hospital is hit by an accidental and fast-spreading fire that starts in the Radiology Clinic on the ground floor. The risk of exploding gas tubes prevents proper fire-fighting and fifteen minutes later a violent explosion occurs. By this time the sky is filled with smoke and a slight wind moves the smoke to the east.
The heavy explosion has released a radioactive cloud. The radiation source that is blown up contains one of the worst possible radioactive materials, caesium-137 chloride. The fine-grained powder is dispersed over the neighbourhood according to figures 15-17.
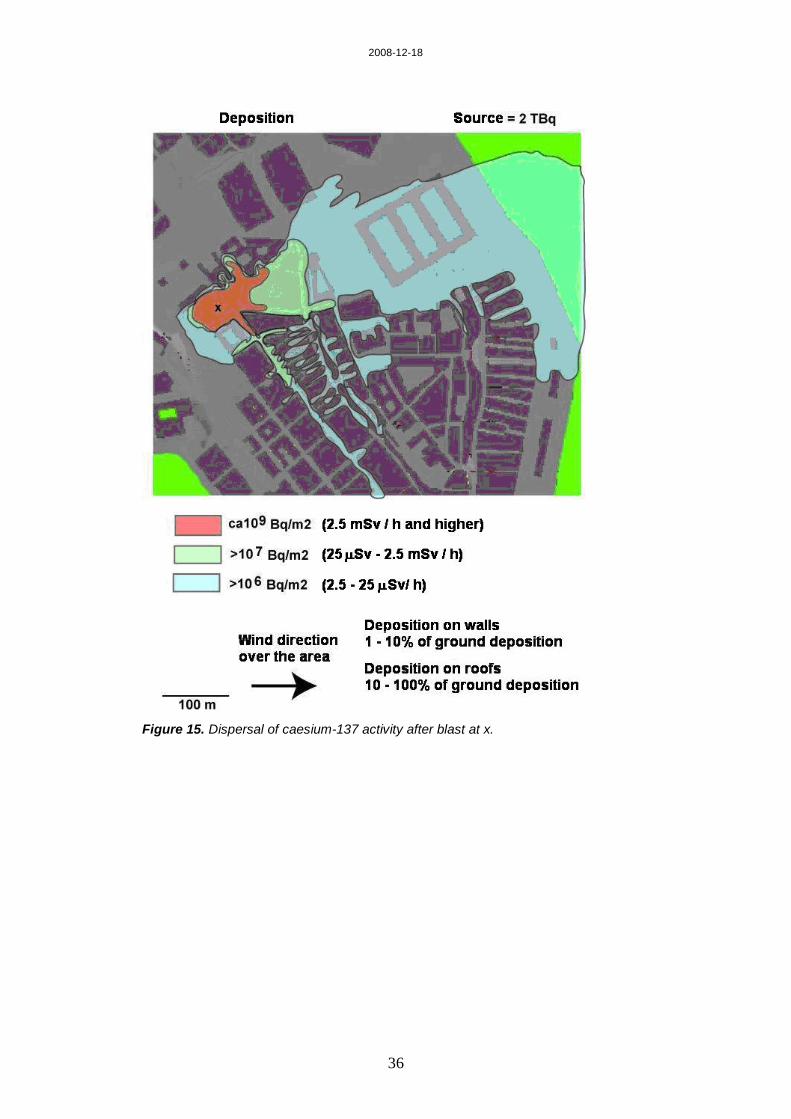
Dose-rates measured in the area with radiation detection instruments will be as indicated in figure 15.
2008-12-18
36
Figure 15. Dispersal of caesium-137 activity after blast at x.

2008-12-18
37
Persons within in the area of the dispersed radioactive caesium have inhaled significant amounts of activity as shown in figure 16.
Figure 16. Inhaled amounts of caesium-137 activity after blast at x.
2008-12-18
38
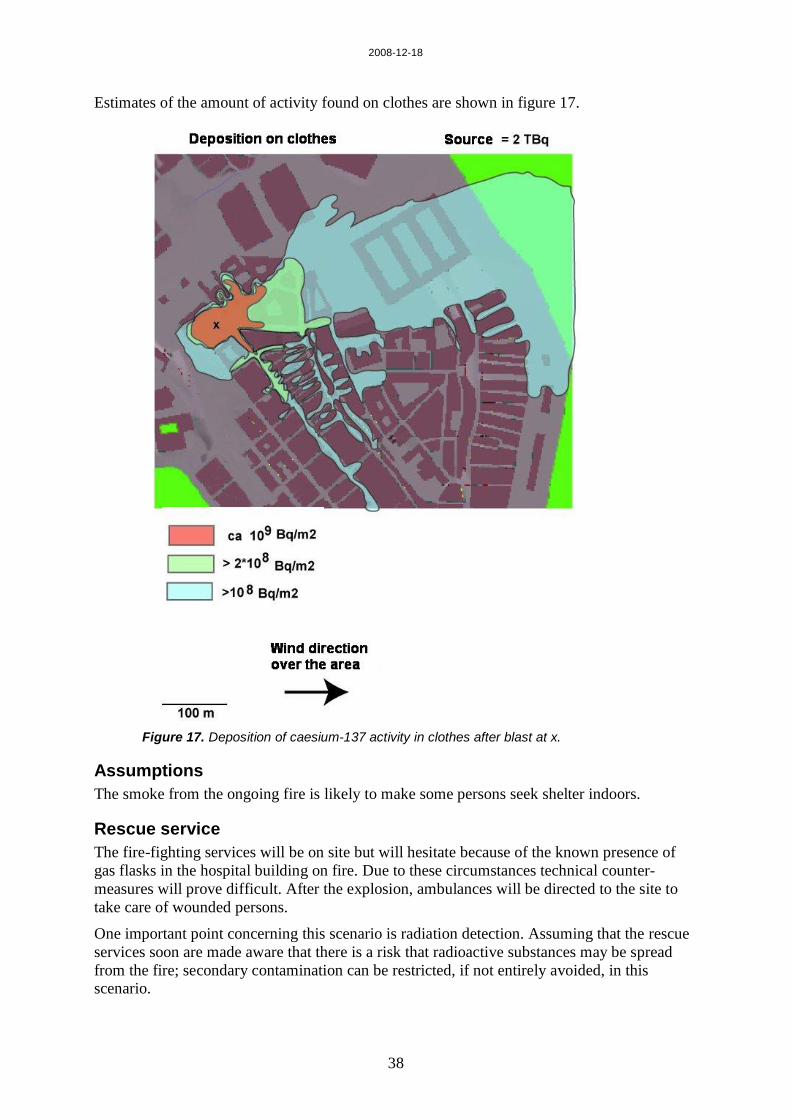
Estimates of the amount of activity found on clothes are shown in figure 17.
Figure 17. Deposition of caesium-137 activity in clothes after blast at x.
Assumptions The smoke from the ongoing fire is likely to make some persons seek shelter indoors.
Rescue service The fire-fighting services will be on site but will hesitate because of the known presence of gas flasks in the hospital building on fire. Due to these circumstances technical counter-measures will prove difficult. After the explosion, ambulances will be directed to the site to take care of wounded persons.
One important point concerning this scenario is radiation detection. Assuming that the rescue services soon are made aware that there is a risk that radioactive substances may be spread from the fire; secondary contamination can be restricted, if not entirely avoided, in this scenario.

2008-12-18
39
Injury outcome
Table 4. Number of affected persons distributed in different levels of effect.
Type of injury Internal contamination
Degree of contamination in
clothes
Number of persons
Severe wounds from blast – hospitalization required ~ 5 x 105 Bq ~ 109 Bq/m2 2
Wounds from blast – hospitalization required ~ 5 x 105 Bq ~ 109 Bq/m2 5
Slight wounds from blast – in need of medical aid, but hospitalization not required for wounds
~ 5 x 105 Bq ~ 109 Bq/m2 8
Severe contamination – in need of decontamination ~ 5 x 105 Bq ~ 109 Bq/m2 30
Moderate to severe contamination – in need of decontamination > 2 x 105 Bq > 2 x 108 Bq/m2 60
Slight to moderate contamination – in need of decontamination > 105 Bq > 108 Bq/m2 250
Injury categories Traumatic injuries Fractures and bleeding wounds on head or other body parts caused
by flying debris after blast.
Radiological injuries No acute effects. Slight increase in risk for late effects.
For exposed persons, there will be a dose-dependent, slight increase in risk for late radiation-induced effects, predominantly in the form of cancer.
Medical care The radiation doses in this scenario are too low to give any acute radiation effects. Depending on the way victims will respond to the situation, the medical treatment may vary. Whole body counting of Cs-137 can be used to determine levels of internal contamination and it may be decided to treat some of the highly-contaminated patients with decorporating agents, e.g. Prussian Blue, to shorten the biological half-life of Cs-137 in persons with high Cs-137 activities.

2008-12-18
40
2008-12-18
41
Scenario 6: Improvised radiation device (IRD) in enclosed area
This little-publicised event that was rated as a level-2-event on the IAEA INES-scale, took place in India in August 2005.
A mentally frustrated radiation worker, in the field of industrial radiography, stole a radioactive source from a business rival. The source contained about 2TBq iridium-192. Iridium-192 is a radioactive material with a half-life of 74 days. The source was removed with about 15 cm of the tubing from the radiography device. The removed parts did not weigh more than 70 g. The radiation worker then placed the source inside a folded umbrella and travelled by taxi to the nearest local railway station where he went on a local train. As the train passed a bridge the radiographer threw the source into the water.
The stolen source could never be located despite extensive radiation surveys. The Indian authorities therefore assumed that the source had drifted further out into the sea and was lying too deep to be detected. Since the source was judged unlikely to affect the public, the event was considered merely as an incident and thus rated at level 2 on the INES scale.
Ref: IAEA INES-NEWS Events, Theft of source pigtail containing Ir-192 radiography source http://www-news.iaea.org/news/, accessed: 2005-09-23
What if…? For scenario 6, let us assume that this event would have occurred somewhere in Europe and that the person with the radiation source instead of throwing it out of the window simply had left it on a local train, underground train, or a bus, and gone off at the next station leaving the source behind. Depending on the state in which it was left on the train, it could go unnoticed for as long as the remainder of the day. In the scenario, we will assume that the source is removed when the passenger car is cleaned at the end of its day shift.
Scenario A person with access to radiation sources has become mentally unstable after incidents in his personal life. For reasons that he later can’t explain, he leaves an unshielded radiation source (5.5 TBq Ir-192) on a local train early in the morning.
At distances longer than 50 cm, several hours of exposure to the source is needed to reach life-threatening doses, but attempts to handle the source with bare hands will result in local skin damage after only a few seconds.
Figure 18. The local train runs back and forth during the day.
2008-12-18
42
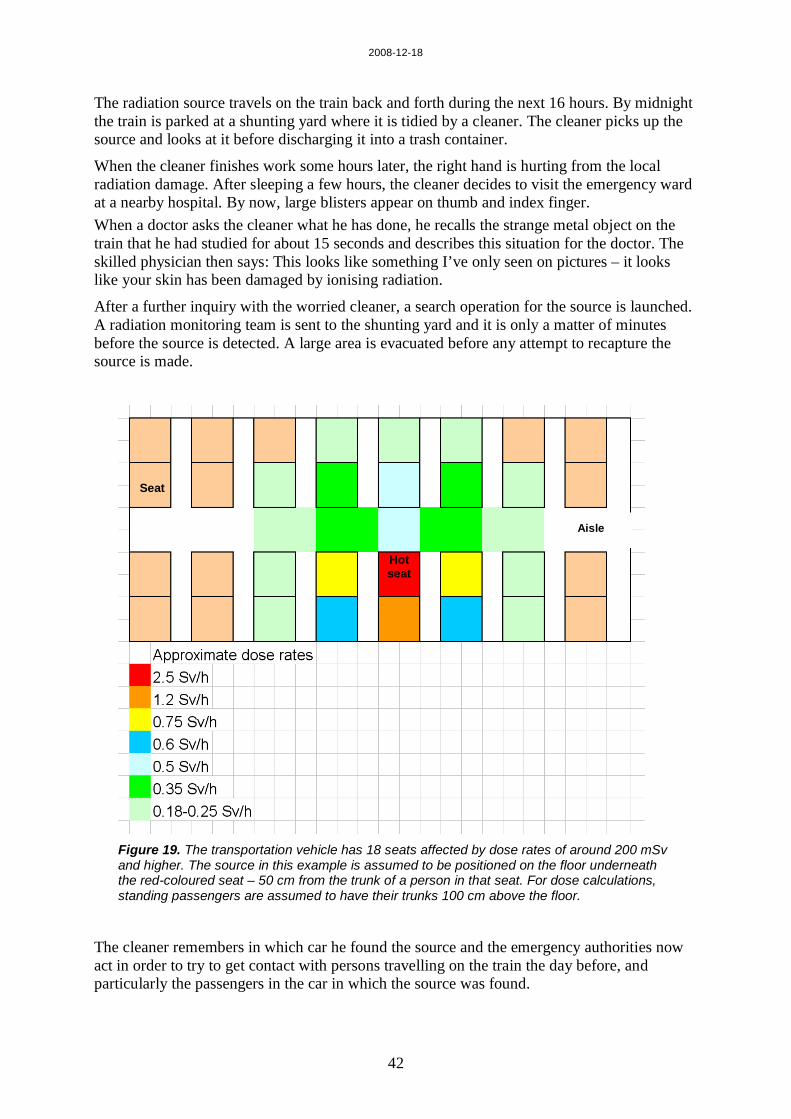
The radiation source travels on the train back and forth during the next 16 hours. By midnight the train is parked at a shunting yard where it is tidied by a cleaner. The cleaner picks up the source and looks at it before discharging it into a trash container.
When the cleaner finishes work some hours later, the right hand is hurting from the local radiation damage. After sleeping a few hours, the cleaner decides to visit the emergency ward at a nearby hospital. By now, large blisters appear on thumb and index finger. When a doctor asks the cleaner what he has done, he recalls the strange metal object on the train that he had studied for about 15 seconds and describes this situation for the doctor. The skilled physician then says: This looks like something I’ve only seen on pictures – it looks like your skin has been damaged by ionising radiation.
After a further inquiry with the worried cleaner, a search operation for the source is launched. A radiation monitoring team is sent to the shunting yard and it is only a matter of minutes before the source is detected. A large area is evacuated before any attempt to recapture the source is made.
Figure 19. The transportation vehicle has 18 seats affected by dose rates of around 200 mSv and higher. The source in this example is assumed to be positioned on the floor underneath the red-coloured seat – 50 cm from the trunk of a person in that seat. For dose calculations, standing passengers are assumed to have their trunks 100 cm above the floor.
The cleaner remembers in which car he found the source and the emergency authorities now act in order to try to get contact with persons travelling on the train the day before, and particularly the passengers in the car in which the source was found.
Seat
Hot seat
Aisle
2008-12-18
43
Rescue service The rescue service will have a limited role in this scenario. It will probably be called upon to assist in evacuation of area around the shunting yard. Radiation expertise will be necessary to shield off and take care of the radiation source. As the source in the scenario is a sealed and intact source, decontamination will not be necessary.
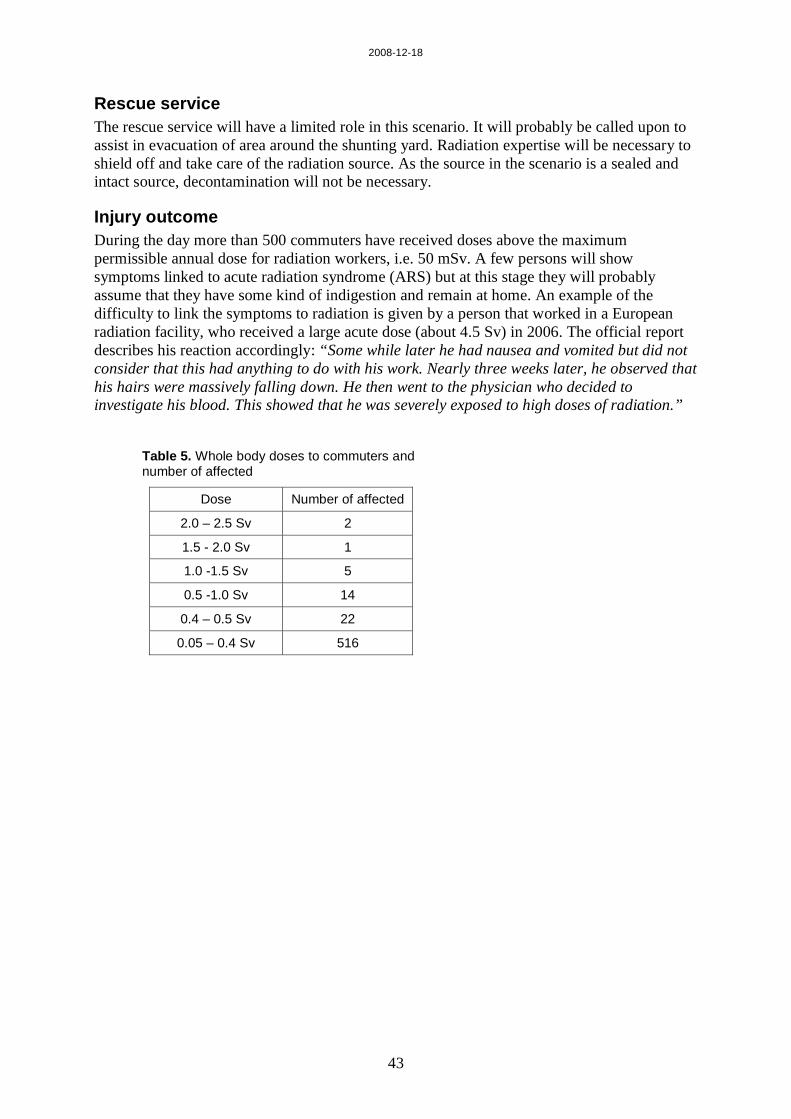
Injury outcome During the day more than 500 commuters have received doses above the maximum permissible annual dose for radiation workers, i.e. 50 mSv. A few persons will show symptoms linked to acute radiation syndrome (ARS) but at this stage they will probably assume that they have some kind of indigestion and remain at home. An example of the difficulty to link the symptoms to radiation is given by a person that worked in a European radiation facility, who received a large acute dose (about 4.5 Sv) in 2006. The official report describes his reaction accordingly: “Some while later he had nausea and vomited but did not consider that this had anything to do with his work. Nearly three weeks later, he observed that his hairs were massively falling down. He then went to the physician who decided to investigate his blood. This showed that he was severely exposed to high doses of radiation.”
Table 5. Whole body doses to commuters and number of affected
Dose Number of affected
2.0 – 2.5 Sv 2
1.5 - 2.0 Sv 1
1.0 -1.5 Sv 5
0.5 -1.0 Sv 14
0.4 – 0.5 Sv 22
0.05 – 0.4 Sv 516

2008-12-18
44
Injury categories for Radiological injuries 2.0-2.5 Sv Symptoms of nausea, vomiting and anorexia often appear within a
few hours and may persist for up to 48 hours. Drop in blood cells counts affecting granulocytes and platelets, and in particular, lymphocytes with slow recovery to normal levels over several weeks. Fever may occur after a few days. There is a very high probability of survival at this dose interval. Chromosome damage will be detectable
1.0-2.0 Sv Same type of symptoms as at the higher dose level, but all symptoms are less pronounced. The same is true for blood cell counts. Chromosome damage will be detectable.
0.5-1.0 Sv Some of the symptoms described for the higher dose levels may occur, but most will be asymptomatic. A slight drop in lymphocyte counts might be registered. Survival will be 100%. Chromosome damage will be detectable.
0.05-0.5 Sv Chromosome damage will be detectable, but will require analysis of large number of cells.
For all dose levels there will be a dose-dependent, slight increase in risk for late radiation-induced effects, predominantly in the form of cancer.
Medical care Medical surveillance and care will be needed for patients with signs of ARS. Dose estimation (biological dosimetry / dose simulation) will be needed for a very large number of persons.
2008-12-18
45
References 1. Levitin H., et al. Decontamination of mass casulties-Re-evaluating Existing Dogma.
Prehospital and disaster medicine Vol. 18 (3), 200-207, 2003.
2. Baker DJ., management of respiratory failure in toxic disaster. Resuscitation, 42, 125-131, 1999.
3. Laurent JF., et al. Management of victims of urban chemical attack: the French approach. Resuscitation, 42, 141-149, 1999.
4. Moles TM. & Baker DJ. Clinical analogies for management of toxic trauma. Resuscitation, 117-124, 1999.
5. Okumura T., et al. The Tokyo subway sarin attack: Management, Part 1: Community Emergency response. Aca Emerg Med, 5, (6), 613-617, 1998.
6. Garner, et al. Comparative Analysis of Multiple Casualty incident triage Algorithmes. Annals of Emergency Medicine, 38, 5, 2001.
7. D.C. Cone and Koenig, K.L. Mass casualty triage in the chemical, biological, radiological or nuclear environment. Eur.J.Emerg. Med. 12, 287-302, 2005.
8. Cassel G.E. et al. Development of Generic scenarios for release of chemicals by terrorists. FOI report, FOI-R--2272--SE, 2007.
9. F.A. Mettler Jr. Medical resources and requirements for responding to radiological terrorism. Health Phys.89, 488-493, 2005.

Åke Sellström, coordinator of Mash,[email protected]

Partners:
The European Centre for CBRNE, University of Umeå, Sweden;
Bundeswehr Institute of Radiobiology InstRadBio Bw, Germany;
Centro de Estudios e Investigaciones Técnicas de Guipúzcoa, CEIT, Spain;
Health Protection Agency, HPA, United Kingdom;
Karolinska Institutet, KI, Sweden;
SAMU de Paris, Assistance Publique Hopitaux de Paris, SAMU, France ;
Swedish Defence Research Agency, FOI, Sweden.
Scenarios (WP 4), FOI
Present practise following mass exposure to radioactivity (WP 5), InstRadBio Bw,
Present practise following mass exposure to toxic chemicals (WP 6), SAMU
Reviewing opportunities in biotechnology (WP 7), KI
Reviewing opportunities in ICT (WP 8), CEIT
Fore-sight of future European preparedness (WP 9),HPA
Coordination (WP 1 – 3),The European CBRNE Center
C-Scenarios
Dispersion of persistent agent in urban area, (1).
Release of toxic industrial chemical in semi-closed area, (2).
Release of toxic industrial chemical in open space, (3).
Dispersion of unknown toxic liquid in enclosed area, (4).
R-Scenarios
Radiological dispersion outdoors, (5).
Improvised radiation device in public area, (6).
X
Dispersion of persistent agent in urban area, (1).

Dispersion of persistent agent in urban area, (1).
150300
5050100
Lightly injured(%)
Severely injured(%)
Distance(metres)
Bleeding wounds on head or body. Traumatic injuriesLight eye irritation and skin ruddiness.Lightly injured
Produce corrosion and necrosis on skin, eyes and respiratory tract. Severe eye irritation can lead to blindness. The signs are typically delayed by several hours.
Severely injured
Injury categories
Dispersion of persistent agent in urban area, (1).

Release of toxic industrial chemical in semi-closed area, (2).

Dispersion of unknown toxic liquid in enclosed area, (4).
Dispersion of unknown toxic liquid in enclosed area, (4).

Radiological dispersion outdoors, (5).

Improvised radiation device in public area, (6).

1.1 Organizational structures
1.2 Competence - Performance
2. Health system
2.1. Pre-hospital triage/ Detection in case of a chemical agent release, Identification in case of a chemical agent releaseMonitoring in case of a chemical agent release
2.2. Decontamination
2.3 Clinical diagnosis
2.4 Therapy, aftercareCapacity for casualties of chemical agent releaseAftercare
3.0 Further comments
Qustionnere - Chemicals
1.1 Organizational structures
1.2 Competence
1.3 National Characteristics
2.0 Health system2.1 Pre-hospital triage/ Monitoring in case of a radiation accident2.2 Decontamination: 2.3 Clinical diagnosis2.4 Biological Dosimetry:
Dicentric chromosome definition: FISH-translocation determination:y-H2A.X-focus assay :CB-micro nuclei assay:COMET-assay: RTQ-PCR based biodosimetry:
2.5 Physical dose reconstruction methods2.6 Therapy, aftercare
Qustionnere - Radioactivity

www.mash-online.eu
username: testuserpassword: radi9bul