animal models of preeclampsia: insight into possible ... · pdf filewe could not find any...
TRANSCRIPT
Central Medical Journal of Obstetrics and Gynecology
Cite this article: Suzuki H, Ohkuchi A, Shirasuna K, Takahashi H, Usui R, et al. (2014) Animal Models of Preeclampsia: Insight into Possible Biomarker Can-didates for Predicting Preeclampsia. Med J Obstet Gynecol 2(2): 1031.
*Corresponding authorsAkihide Ohkuchi, Department of Obstetrics and Gynecology, Jichi Medical University School of Medicine, 3311-1 Yakushiji, Shimotsuke-shi, Tochigi, 329-0498, Japan,Tel: 81-285-58-7376; Fax: 81-285-44-8505; Email:
Submitted: 26 April 2014
Accepted: 09 June 2014
Published: 10 June 2014
ISSN: 2333-6439
Copyright© 2014 Ohkuchi et al.
OPEN ACCESS
Research Article
Animal Models of Preeclampsia: Insight into Possible Biomarker Candidates for Predicting PreeclampsiaHirotada Suzuki1, Akihide Ohkuchi1*, Koumei Shirasuna2,3, Hironori Takahashi1, Rie Usui1, Shigeki Matsubara1 and Mitsuaki Suzuki1
1Department of Obstetrics and Gynecology, Jichi Medical University School of Medicine, Japan2Division of Inflammation Research, Center of Molecular Medicine, Jichi Medical University, Japan3Department of Animal Science, Tokyo University of Agriculture, Japan
Keywords•Preeclampsia•Mouse•Rat•Animal model•Prediction
Abstract
Aim: Animal models of preeclampsia (PE) have been extensively developed. Angiogenic/angiostatic balance theory bysoluble fms-like tyrosine kinase 1 (sFlt-1), placental growth factor (PlGF) and soluble endoglin (sEng) for the genesis of PE is one of the most successful models of translational research from bench to bed. However, the balance theory of angiogenic/angiostatic factors does not explain the genesis of PE entirely. We attempted to list articles on animal models of PE and to gain insight into possible biomarker candidates for predicting PE.
Methods: We collected 64 articles animal models of PE, consisting of 25 different methods. For angiotensinogen/renin, complement component C1q, 2-methoxyoestradiol (2-ME)/catechol-O-methyltransferase (COMT), galectin-1 (Gal-1), heme oxygenase-1 (HO-1), interleukin (IL)-10, and asymmetric dimethylarginine (ADMA)/L-arginine, we searched for articles on the prediction of PE in PubMed.
Results: Angiotensinogen in the first trimester, prorenin at 8 weeks of gestation in women with type 1 diabetes, and plasma prorenin receptor in early pregnancy might predict the occurrence of PE. Low Gal-1 levels during the first trimester might predict the occurrence of PE during the second trimester. IL-10 levels did not change before the onset of PE. Maternal plasma ADMA in the second and third trimesters was higher in women with PE. We could not find any cohort or nested case-control studies on complement component C1q, 2-ME/COMT, and HO-1.
Conclusion: Clinically useful biomarkers other than angiogenesis-related factors were not found. Basic research using animal models will gain insight into possible biomarker candidates for predicting PE.
Special Issue on
Prediction of Preeclampsia
INTRODUCTIONPreeclampsia (PE) is associated with maternal and infantile
morbidity and mortality [1-3]. Recently, after the discovery of the roles of soluble fms-like tyrosine kinase 1 (sFlt-1) and soluble endoglin (sEng) in the genesis of a preeclamptic rodent model showing hypertension, proteinuria, and glomerular endotheliosis [4,5], several prospective cohort studies have elucidated that serum/plasma levels of placental growth factor (PlGF), sFlt-1, sEng, and the sFlt-1/PlGF ratio may be useful to
predict the occurrence of PE [6-12]. Recently, we showed that the onset threshold of plasma levels of the sFlt-1/PlGF ratio is a highly sensitive and specific screening method for detecting the imminent onset of PE within 4 weeks after blood sampling at 19–31 weeks [13,14]. Thus, angiogenic/angiostatic balance theory by sFlt-1, PlGF and sEng for the genesis of PE is one of the most successful models of translational research from bench to bed. However, the balance theory does not explain the genesis of PE entirely, because some women with PE did not show an increased level of sFlt-1 and/or sEng, or a decreased level of

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 2/12
PlGF, especially at ≥36 weeks of gestation [15,16]. Therefore, new candidates causing and/or facilitating the occurrence of PE have been searched for vigorously [17,18].
In this review, we attempted to list articles on animal models of PE and to gain insight into possible biomarker candidates for predicting PE.
METHODSH.S. searched for articles on animal models of PE in PubMed.
He found 7 articles using the angiotensinogen/renin system [19-25], 3 articles using BPH/5 [26-28], 1 article using complement component C1q [29], 1 article using a model by crossbreeding CBA and JXDBA/2 [30], 2 articles using 2-methoxyoestradiol (2-ME)/catechol-O-methyltransferase (COMT)deficiency [31,32], 1 article using an antagonist of galectin-1 (Gal-1) [33], 1 article using heme oxygenase-1 (HO-1) knockout (KO) mice [34], 1 article using chronic administration of the inhibitor of cystathionine γ-lyase (CSE, an enzyme responsible for the endogenous production of hydrogen sulfide [H2S]), DL-propargylglycine (PAG) [35], 1 article using indoleamine 2,3-dioxygenase (IDO) inhibitor, 1-methyl-L-tryptophan [36], 5 articles using IgG of human PE (angiotensin II type 1 [AT1] receptor agonistic autoantibody [AT1-AA]) [37-41], 1 article using interleukin (IL)-10 KO mice [42], 5 articles using N(omega)-nitro-L-arginine methyl ester (L-NAME) [43-47], 1 article using desoxycorticosterone acetate (DOCA), and marinobufagenin (MBG) [48], 1 article using matrix metalloproteinase-9 (MMP-9)KO mice [49], 1 article using ligand of the liver X receptor (LXR) oxygenated cholesterol derivatives (oxysterols) [50], 1 article using a model by crossbreeding p57kip heterozygous KOmice and p57kip heterozygous KO mice [51], 2 articles using phosphatidylserine/phosphatidylcholine (PSPC) [52,53], 10 articles using reduced uterine perfusion pressure (RUPP) models [54-63], 1 article using both adenovirus vector of sEng and adenovirus vector of sFlt-1 [5], 9 articles using adenovirus vector of sFlt-1 alone [4,64-71], 1 article using exogenous mouse vascular endothelial growth factor (VEGF) [72], 1 article on Storkhead box-1 (STOX1) transgenic (tg) mice [73], 2 articles using suramin [74,75], 2 articles using helper T cells type 1 (Th1) like splenocytes [76,77], and 3 articles by stimulation of Toll-like receptor (TLR)-3 or hyper-expression of TLR-3 [78-80] (Table 1).
As for angiotensinogen/renin, complement component C1q, 2-ME/COMT, Gal-1, HO-1, IL-10, and L-NAME, A.O. searched for articles on the prediction of PE using these markers in PubMed. The following combinations of key words were used: A AND B, where A was the key word of the target biomarker, and B was a constant key word. A was “angiotensinogen” OR “renin”, “C1q” AND “complement”, “2-methoxyoestradiol” OR “catechol-O-methyltransferase”, “galectin-1”, “heme oxygenase-1”, “IL-10”, or (“asymmetric dimethylarginine” OR ADMA OR L-arginine OR “nitric oxide”). B was ((preeclampsia OR “pregnancy-induced hypertension” OR “hypertension in pregnancy” OR “gestational hypertension” OR “EPH gestosis” OR “toxemia of pregnancy” OR eclampsia) AND (predict* OR predicting OR prediction OR ((cohort OR prospective OR retrospective OR “nested case-control”) AND study) OR “risk factor” OR “meta-analysis”OR “systematic review” OR combination OR multivariate OR “logistic regression”)).
RESULTS AND DISCUSSION
Angiotensinogen and renin
Increased angiotensinogen and renin in pregnant mice/rats caused PE-like changes (Table 1) [19-25], suggesting that increases of angiotensinogen and renin might be candidates for predicting PE. We searched for articles in PubMed using the key words of (“angiotensinogen” OR “renin”) AND B. Angiotensinogen in the first trimester [81], prorenin at 8 weeks of gestation in women with type 1 diabetes [82], and plasma prorenin receptor in early pregnancy [83] might predict the occurrence of PE.
Complement component C1q
Complement component C1q has an important role in trophoblast migration, spiral artery remodeling, and normal placentation [29]. Pregnant C1q-deficient (C1q-/-) mice developed PE-like changes and showed decreased placental VEGF and elevated levels of sFlt-1; treatment of C1q-/- mice with pravastatin restored angiogenic balance and reduced hypertension and albuminuria [29]. This study suggested that a decrease of C1q might be a candidate for predicting PE. We searched for articles in PubMed using the key words of (“C1q” AND complement) AND B. However, there were no hits.
COMT, 2-ME
2-ME, a natural metabolite of estradiol, is generated by COMT in the placenta and increases during pregnancy; however, placental COMT activity is suppressed in women with PE [31]. Kanasaki et al. [31] discovered that pregnant mice deficient in COMT develop PE-like changes; 2-ME ameliorated all symptoms and suppressed placental hypoxia, hypoxia-inducible factor-1α expression and sFlt-1 elevation (Table 1). In addition, the levels of COMT and 2-ME were significantly lower in women with PE [31], suggesting that the decreases of 2-ME and COMT might be candidates for predicting PE. We searched for articles in PubMed using the key words of (“2-methoxyoestradiol” OR “catechol-O-methyltransferase”) AND B. We could not find any studies on predicting PE using 2-ME and/or COMT.
Galectin-1 (Gal-1)
Gal-1, a member of a family of carbohydrate-binding proteins, is associated with placentation and the promotion of maternal tolerance toward fetal antigens [33]. Freitag et al. [33] discovered that Gal-1 exhibits proangiogenic functions during early stages of pregnancy, promoting decidual vascular expansion through VEGF receptor 2 signaling; blocking Gal-1-mediated angiogenesis results in PE-like changes in mice. In addition, low Gal-1 levels during the first trimester were associated with the occurrence of PE during the second trimester, suggesting that a low level of Gal-1 in early pregnancy might be a candidate for predicting PE (Table 1). We searched for articles in PubMed using the key words of “galectin-1” AND B, but we could not find any studies on predicting PE using Gal-1.
HO-1
HO-1 and its metabolite carbon monoxide (CO) exert protective effects against oxidative stimuli [34]. Cudmore et al. [34] discovered that adenoviral overexpression of HO-1 in

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 3/12
Mole-cles/
Strain
Author, year, [ref-
erence]Species Methods Classifi-cation Symptoms Treatment
Angiotensinogen/renin systemTakimoto E, 1996 [19]
mice Angiotensinogen tg renin tg PEHypertension, proteinuria myo-cardial hypertrophy, placental edema/necrosis.
Recovery of blood pressure af-ter delivery.
Bohlender J, 2000 [20]
rats Angiotensinogen tg♀ Xrenin tg♂ GH Hypertension. NR: proteinuria. Amelioration of hypertension
after birth.
Brosnihan KB, 2010 [21]
rats Angiotensinogen tg♀ Xrenin tg♂ PE
Increased blood pressure, pro-teinuria, and FGR, lower placen-tal weight.
Geusens N, 2010 [22]
rats Angiotensinogen tg♀ Xrenin tg♂ PE FGR.
Falcao S, 2009 [23] mice Angiotensinogen and renin dou-
ble tg pregnant mice sPE
Hypertension, proteinuria placental necrosis, reduced pup weight, reduced placental weight, heart hypertrophy.
Genest DS, 2013 [24] mice Angiotensinogen and renin dou-
ble tg pregnant mice sPEChronic hypertension, increased blood pressure during preg-nancy, proteinuria.
Exercise training ameliorated blood pressure, proteinuria.
Hering L, 2010 [25] rats Administration of angiotensinⅡ
to pregnant rat PE
Hypertension, proteinuria, re-duced placental weight, reduced fetal weight, reduced trophob-last invasion, increased uterine artery resistance.
BPH/5
Davisson RL, 2002 [26]
mice BPH/5 x BPH/5 PE
Hypertension, proteinuria, glomerulosclerosis, reduced pup weight, reduced litter size, impaired endothelium-depend-ent relaxation in resistance arteries.
Recovery of blood pressure af-ter delivery.
Woods AK, 2011 [27]
mice BPH/5 x BPH/5, administration of Ad-VEGF at 7.5 day. PE
Hypertension, proteinuria, fetal resorption. Reduced levels of free VEGF and PlGF; unchanged sFlt-1.
Amelioration of hypertension, proteinuria, and fetal resorp-tionby the administration of Ad-VEGF.
Hoffmann DS, 2008 [28]
mice
BPH/5 x BPH/5, administra-tion of Tempol (superoxide dismutase mimetic) throughout gestation
PEFGR, fetal absorption, hyperten-sion, proteinuria. Increased ROS.
Amelioration fetal growth and survival, hypertension, pro-teinuria by the administration of Tempol.
C1q
Singh J, 2011 [29] mice C1q KO x C1q KO PE
Hypertension, proteinuria, glomerular endotheliosis, re-duced litter size, increased sFlt-1, decreased VEGF, increased STAT-3.
Amelioration by the administra-tion of pravastatin.
CBA X JXDBA/2
Ahmed A, 2010 [30] mice i) CBA/J♀ x DBA/2♂
ii) Administration of AngII to i) PE
Hypertension, albuminuria, en-dotheliosis, decreased placental VEGFand elevated placental sFlt-1.
Restoration of trophoblast invasiveness, placental blood flow, and angiogenic balance, and prevention of the onset of PE by the administration of pravastatin.
COMT KO
Kanasaki K, 2008 [31]
mice COMT KO pregnant mice PE
Hypertension, proteinuria, en-dotheliosis, reduced placental weight, reduced littersize, in-creased sFlt-1.
Amelioration of all PE-like fea-tures by the administration of 2-ME.
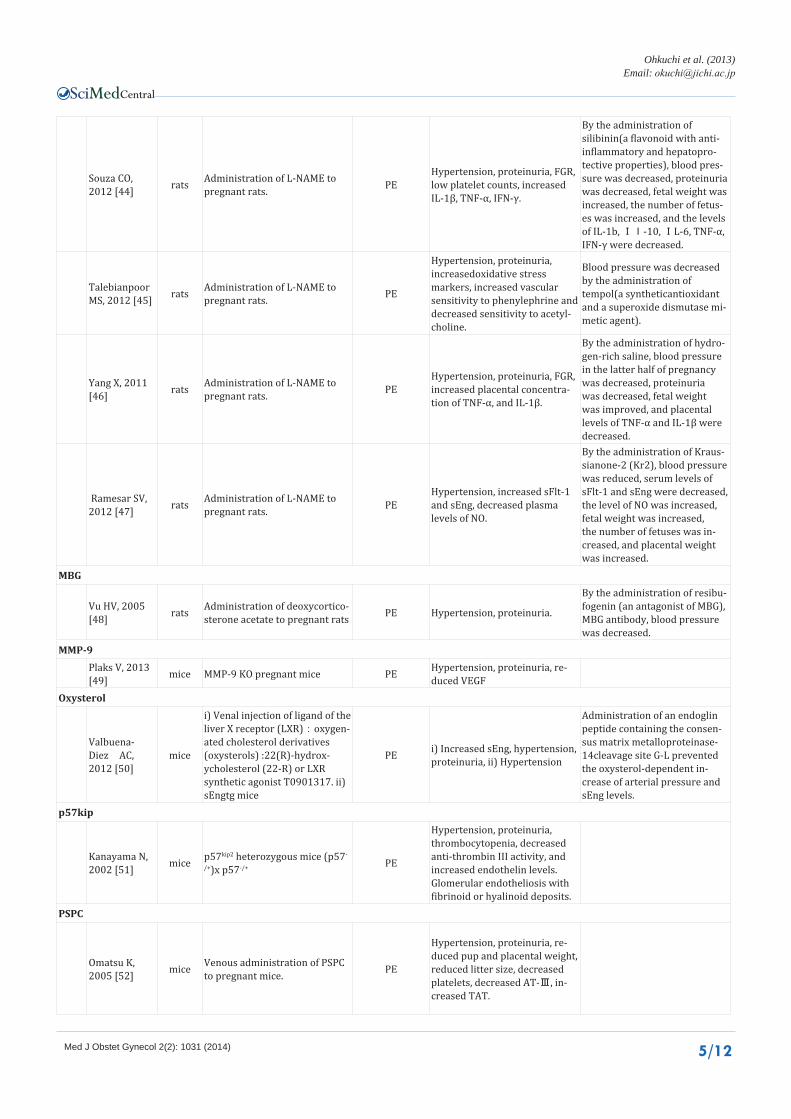
Table 1: Preeclampsia (PE) models (mouse/rat).

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 4/12
Stanley JL, 2012 [32] mice COMT KO pregnant mice PE
Hypertension, proteinuria, FGR, abnormal umbilical Doppler waveforms.
Administration of sildenafil cit-rate improved fetal growth, and notch on the umbilical artery.
Gal-1
Freitag N, 2013 [33] mice
i) administration of antagonist of gal-1 to pregnant mice. ii) Lgals1 KO mice.
PE
Hypertension, proteinuria, re-duced placental weight, reduced litter size, reduced pup weight, increased sEng, increased AT1-AA.
HO-1KOCudmore M, 2007 [34]
mice HO-1 KO pregnant mice Increased sFlt-1, increased sEng.
Hydrogen sulfide
Wang K, 2013 [35] mice
Administration of DL-propar-gylglycine, which inhibits activ-ity of cystathionineγ-lyase (CSE), which produces a gaseous messenger, H2S, to pregnant mice.
PE
Hypertension, proteinuria, reduced pup weight, increased sFlt-1, increased sEng, liver damage.
Amelioration of angiogenic balance, fetal growth by the administration of GYY4137 (H2S release).
IDONishizawa H, 2008 [36]
mice Administration of IDO inhibitor to pregnant mice. PE
Hypertension, proteinuria, placental circulation impairment.
IgG of human PE(AT1-AA)
Zhou CC, 2008 [37] mice
Administration of IgG antibody-obtained from human PE or AT1-AA to pregnant mice.
PE
Hypertension, proteinuria, glomerular endotheliosis, pla-cental abnormalities, reduced pup weight, increased sFlt-1.
Amelioration of symptoms by losartan, an AT1 receptorantagonist, antibody neutraliz-ing seven–amino-acid sequence on the second extracellular loop of AT1 receptor.
Siddiqui AH, 2013 [38] mice
Administration of IgG antibody obtained from human PE to pregnant mice.
PE
Hypertension, proteinuria, decreased aldosterone, cel-lular and vascular impairment of adrenal glands, increased sFlt-1.
Amelioration of symptoms by losartan, 7-aa epitope peptide, VEGF121 infusion.
Zhou CC, 2011 [39] mice
Administration of IgG antibody obtained from human PE to pregnant mice.
PE
Hypertension, proteinuria, and renal damage. PreproET-1 mRNA and IL-6 mRNA were increased in placenta and kidney, and serum level of IL-6 was increased.
Amelioration ofhypertension, proteinuria, and renal damage-by the administration of ET-A antagonist BQ123, and anti-IL-6 antibody.
Zhou CC, 2010 [40] mice
Administration of IgG antibody obtained from human PE to pregnant mice.
PE
Hypertension, proteinuria, and renal damage. Increased sEng, increased production of sEng in placenta, increased TNFα, increased production of TNFα in placenta.
Irani RA, 2010 [41] mice
Administration of IgG antibody obtained from human PE to pregnant mice.
PE
Hypertension, proteinuria, in-creased sFlt-1, increased sEng, increased production of TNFαin placenta.
IL-10 KO
Lai Z, 2011 [42] mice IL-10 KO pregnant miceunder
9.5% oxygen concentration. PE
Hypertension, proteinuria, glomerular endotheliosis, re-duced pup weight, increased sFlt-1.
Amelioration of symptoms by the administration of recom-binant IL-10.
L-NAME
Herraiz S, 2012 [43] rats Administration of L-NAME to
pregnant rats. PE Hypertension, proteinuria, FGR.
By the administration of silde-nafil citrate (SC), blood pressure was decreased, proteinuria was ameliorated, and fetal weight and survival rates were increased.
Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 5/12
Souza CO, 2012 [44] rats Administration of L-NAME to
pregnant rats. PEHypertension, proteinuria, FGR, low platelet counts, increased IL-1β, TNF-α, IFN-γ.
By the administration of silibinin(a flavonoid with anti-inflammatory and hepatopro-tective properties), blood pres-sure was decreased, proteinuria was decreased, fetal weight was increased, the number of fetus-es was increased, and the levels of IL-1b, Il-10, IL-6, TNF-α, IFN-γ were decreased.
Talebianpoor MS, 2012 [45] rats Administration of L-NAME to
pregnant rats. PE
Hypertension, proteinuria, increasedoxidative stress markers, increased vascular sensitivity to phenylephrine and decreased sensitivity to acetyl-choline.
Blood pressure was decreased by the administration of tempol(a syntheticantioxidant and a superoxide dismutase mi-metic agent).
Yang X, 2011 [46] rats Administration of L-NAME to
pregnant rats. PEHypertension, proteinuria, FGR, increased placental concentra-tion of TNF-α, and IL-1β.
By the administration of hydro-gen-rich saline, blood pressure in the latter half of pregnancy was decreased, proteinuria was decreased, fetal weight was improved, and placental levels of TNF-α and IL-1β were decreased.
Ramesar SV, 2012 [47] rats Administration of L-NAME to
pregnant rats. PEHypertension, increased sFlt-1 and sEng, decreased plasma levels of NO.
By the administration of Kraus-sianone-2 (Kr2), blood pressure was reduced, serum levels of sFlt-1 and sEng were decreased, the level of NO was increased, fetal weight was increased, the number of fetuses was in-creased, and placental weight was increased.
MBG
Vu HV, 2005 [48] rats Administration of deoxycortico-
sterone acetate to pregnant rats PE Hypertension, proteinuria.
By the administration of resibu-fogenin (an antagonist of MBG), MBG antibody, blood pressure was decreased.
MMP-9Plaks V, 2013 [49] mice MMP-9 KO pregnant mice PE Hypertension, proteinuria, re-
duced VEGF Oxysterol
Valbuena-Diez AC, 2012 [50]
mice
i) Venal injection of ligand of the liver X receptor (LXR):oxygen-ated cholesterol derivatives (oxysterols) :22(R)-hydrox-ycholesterol (22-R) or LXR synthetic agonist T0901317. ii) sEngtg mice
PE i) Increased sEng, hypertension, proteinuria, ii) Hypertension
Administration of an endoglin peptide containing the consen-sus matrix metalloproteinase-14cleavage site G-L prevented the oxysterol-dependent in-crease of arterial pressure and sEng levels.
p57kip
Kanayama N, 2002 [51] mice p57kip2 heterozygous mice (p57-
/+)x p57-/+ PE
Hypertension, proteinuria, thrombocytopenia, decreased anti-thrombin III activity, and increased endothelin levels. Glomerular endotheliosis with fibrinoid or hyalinoid deposits.
PSPC
Omatsu K, 2005 [52] mice Venous administration of PSPC
to pregnant mice. PE
Hypertension, proteinuria, re-duced pup and placental weight, reduced litter size, decreased platelets, decreased AT-Ⅲ, in-creased TAT.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 6/12
Zhang Y, 2009 [53] mice Venous administration of PSPC
to pregnant mice. PEElevated SBP, proteinuria, andreduction of AT III and blood platelets.
Amelioration of symptoms by annexineX, AND (a recom-binantpolypeptide that is composed of annexin V and hirudinby connecting Pro46-Gln65 of hirudin to the C-ter-minus (Asp320) of annexin V), heparin.
RUPPAlexander BT, 2001 [54] rats Clipping of Ao of pregnant rats. PE Hypertension, proteinuria.
George EM, 2011 [55] rats Clipping of Ao of pregnant rats. PE
Hypertension, reduced pup size, reduced placental weight, in-creased sFlt-1, decreased VEGF, increased superoxide, increased preproET-1 mRNA.
Cobalt protoporphyrin (HO-1 induced) i.p. caused a signifi-cant shift in the ratio to an ang-iogenic balance, and decreased preproET-1 mRNA.
Amaral LM, 2014 [56] rats Clipping of Ao of pregnant rats. PE Hypertension, increased iNOS.
By transcutaneous administra-tion of N-[3-(aminomethyl) benzyl] acetamidine (1400 W), hypertension was improved by inhibiting the production of iNOS
Lillegard KE, 2013 [57] rats Clipping of Ao of pregnant rats. PE Hypertension, increased C3a.
By administration of a soluble form of an endog-enouscomplement regulator, soluble complement receptor 1 (sCR1),hypertension was improved.
LaMarca B, 2011 [58] rats Clipping of Ao of pregnant rats. PE Hypertension, increased serum
AT1-AA, ET-1.
By the administration of rituxi-mab (B-lymphocyte-suppres-sive agent), blood pressure and ET-1 were decreased.
Tam Tam KB, 2011 [59] rats Clipping of Ao of pregnant rats. PE Hypertension, increased uterine
artery resistive index.
By the administration of en-dothelin typeA receptor an-tagonist, blood pressure was decreased, and uterine artery resistive index was decreased.
Morton JS, 2012 [60] rats Clipping of Ao of pregnant rats. PE
Significant increase in the ex-pression of the LOX-1 receptor, endothelial NO synthase, and superoxide in thoracic aorta.
Endothelial-dependent vasodi-lator function was modestly increased in the presence of both oxidized LDL and the LOX receptor inhibitor.
Walsh SK, 2012 [61] rats Clipping of Ao of pregnant rats. PE Hypertension, endothelial dys-
function.
By the administration of PARP inhibitor (PJ34)post RUPP sur-gery, blood pressure was not changed.
McCarthy, 2011 [62] rats Clipping of Ao of pregnant rats. PE Hypertension, proteinuria, de-
creased HO-1.
By the administration of PPAR-γ agonist, rosiglitazone, blood pressure was decreased, pro-teinuria was decreased, and HO-1 was increased.
Cornelius DC [63] rats Clipping of Ao of pregnant rats. PE
Hypertension, FGR, reduced placental weight, increased ROS and AT1-AA.
T-helper17 (TH17) suppression via IL-17 recombinant recep-tor C (IL-17RC). Blood pressure was decreased, fetal weight was increased, placental weight was increased, the production of ROS in the placenta was decreased, and AT1-AA was decreased.
sEng
Venkatesha S, 2006 [5] rats Administration of AdsEng and
AdsFlt-1 to pregnant rats. PE
Hypertension, proteinuria, glomerularendotheliosis, de-creased platelets, increased liver enzyme, reduced pup weight.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 7/12
sFlt-1Maynard SE, 2003 [4] rats Administration of AdsFlt-1 to
pregnant rats PE Hypertension, proteinuria, glomerular endotheliosis.
Lu F, 2007 [64] mice Administration of AdsFlt-1 to
pregnant mice PEHypertension, reduced pup weight, reduced litter size, de-creased platelets.
Suzuki H, 2009 [65] mice Administration of AdsFlt-1 to
pregnant mice PEHypertension, proteinuria, glomerular endotheliosis, de-creased VEGF.
By the administration of rhPlGF, rhVEGF-A, hypertension was improved.
Li Z, 2007 [66] rats Administration of AdsFlt-1 to pregnant rats PE Hypertension, proteinuria,
glomerular endotheliosis.
By the administration of rVEGF, hypertension, proteinuria, and glomerular endotheliosis were improved.
Bergmann, 2010 [67] mice Administration of AdsFlt-1 to
pregnant mice PE Hypertension, proteinuria, glomerular endotheliosis.
By the administration of AdVEGF, hypertension, proteinuria,and endotheliosis were improved.
Mateus J, 2011 [68] mice Administration of AdsFlt-1 to
pregnant mice PE Hypertension. By the administration of rVEGF, hypertension was improved.
Lu F, 2007 [69] mice Administration of AdsFlt-1 to
pregnant mice PE IUGR, blood pressure increased.BP was significantly higher in male offspring born to sFlt-1-treated mothers.
Kumasawa K, 2010 [70] mice Administration of LV-sFlt-1 to
embryonic cells. PE
Hypertension, proteinuria, re-duced placental weight, reduced pup weight, increased sEng, increased AT1-AA.
By the administration of prav-astatin, hypertension, and pro-teinuria were improved, the se-rum concentration of sFlt-1 was decreased, the serum level of PlGF was increased, fetal weight was improved, and placental weight was improved.
Fox KA, 2011 [71] mice Administration of Ad-sFlt-1 to
pregnant mice PE NR: BP, proteinuria.
By the administration of prav-astatin, the production of eNOS in the aorta and liver was in-creased, the production of HO-1 in the kidney was increased.
VEGF
Murakami Y, 2005 [72] mice Administration of exogenous
murine VEGF (164) PEHypercoagulation in the placental circulation and a significant ele-vation of systolic blood pressure.
By the administration of anti-VEGF neutralized antibody, symptoms were suppressed.
STOX1
Doridot L, 2013 [73] mice STOX1 tg ♂ x Wild type ♀ PE
Hypertension, proteinuria, glomerular endotheliosis, re-duced litter size, increased sFlt-1, increased sEng.
Amelioration by the administra-tion of aspirin.
Suramin
Nash P, 2005 [74] rats Suramin i.p. to pregnant rats. GH
Hypertension, decreased renal blood flow, decreased placental blood flow, fetal growth retarda-tion; increased isoprostane 8-epi-PGF2a, increased endothelin-1
Carlstrom M, 2009 [75] rats Suramin ip to pregnant rats. GH
Hypertension, fetal growth re-tardation. Smaller placentae, in-creased renin, decreased sFlt-1, decreasedplacental vessel area
Th1
Zenclussen AC, 2004 [76] mice Administration of Th1-like
splenocytes to pregnant mice. PE
Hypertension, proteinuria, glomerulonephritis, reduced lit-ter size; increased production of cytokine of uterine lymphocytes.
McRae JL, 2013 [77] mice
WT or CD39 tg ♀ x WT ♂, fol-lowed by the administration of Th1-like splenocytes.
PEHypertension, proteinuria, glomerulonephritis in WT x WT injected Th1-like splenocytes.
Amelioration of hypertension, proteinuria, and glomerulone-phritis in pregnant CD39 tg mice.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 8/12
TLR
Chatterjee P, 2012 [78] mice
TLR3-specific agonist poly I:C TLR7-specific agonist R-837 TLR7/8 agonist CLO97 i.p. to pregnant mice.
PEHypertension, proteinuria, FGR, early delivery, reduced placen-tal weight.
Chatterjee P, 2011 [79] mice
IL-10 KO, pregnant mice, Ad-ministration of TLR3 agonist polyinosinepolycytidylic acid (poly I:C)
PEHypertension, proteinuria, decreased number of pups per litter, increased demise.
Kopriva SE, 2012 [80] mice Pregnant mice treated with the
TLR3 agonist poly I:C (P-PIC). PE
Hypertension, proteinuria,increased miR-210, increased HIF1α, NFκB in placenta, decreased STAT6 in placenta.
Pregnant TLR3 KO mice treated by poly I:C did not develop hypertension, and placental HIF-1α, NF-kBp50, miR-210, and STAT6 were not changed compared with pregnant TLR3 KO mice.
Abbreviations: PE: Preeclampsia; GH: Gestational Hypertension; NR: Not Reported; FGR: Fetal Growth Restriction; sPE: superimposed Preeclampsia; Ad: Adenoviral vector; VEGF; Vascular Endothelial Growth Factor; PlGF: Placental Growth Factor; ROS: Reactive Oxygen Species; KO: Knockout; sFlt-1: soluble Fms-like tyrosine kinase 1;COMT: Catechol-O-MethylTransferase; 2-ME: 2-Methoxyoestradiol; Gal-1: Galectin-1; AT1-AA: Angiotensin II type 1 (AT1) receptor Agonistic Autoantibody; HO-1: Heme Oxygenase-1; CSE: Cystathionine γ-lyase; H2S: Hydrogen Sulfide; sEng: soluble Endoglin; IDO: Indoleamine 2,3-dioxygenase; ET-1: Endothelin 1; TNF-α: Tumor Necrotizing Factor alpha; IL-10: Interleukin-10; L-NAME: N(omega)-nitro-L-arginine methyl ester; IFN-γ: Interferon Gamma; NO: Nitric Oxide; DOCA: Desoxycorticosterone Acetate; MBG: Marinobufagenin; MMP-9: Matrix Metalloproteinase-9; LXR: Liver X Receptor; PSPC: Phosphatidylserine/Phosphatidylcholine; AT-III: Aanti-Thrombin III; TAT: Thrombin Anti-Thrombin complex; RUPP: Reduced Uterine Perfusion Pressure; Ao: Aorta; iNOS: Inducible Nitric Oxide Synthase; eNOS: endothelial Nitric Oxide Synthase; PGF: Prostaglandin F; Th1: helper T cells type 1 (Th1); TLR-3: Toll-like receptor 3.
endothelial cells inhibits VEGF-mediated sFlt-1 release and interferon (IFN)-γ- and tumor necrosis factor (TNF)-α–induced sEng release, whereas HO-1 inhibition results in sFlt-1 and sEng production from endothelial cells andplacental villous explants, and mice lacking HO-1 produce higher levels of sFlt-1 and sEng than wild-type mice (Table 1). These results suggested that a decrease of HO-1 might be a candidate for predicting PE-like changes. We searched for articles in PubMed using the key wordsof “heme oxygenase 1”AND B, but there were no reports on predicting PE using the circulating level of HO-1. However, Farina et al. [84] quantified mRNA expression in tissue samples from chorionic villous sampling (CVS) of normal and PE patients at 11 weeks of gestation. HO-1 was associated with the lowest degree of aberration in PE, indicating that circulating levels of mRNA levels of HO-1 might be used for the prediction of PE. Nakamura et al. [85] measured circulating mRNA in 24 women with PE and 24 controls; the mRNA level of HO-1 was significantly decreased in women with PE. Cohort studies using not only mRNA levels but also protein levels of HO-1 are warranted in the future.
IL-10
Hypoxia affects the cytokine balance by reducing IL-10 production and inducing IL-6 and IL-8 in placental explants and trophoblasts [34]. Lai et al. [34] discovered that exposure of pregnant wild-type and IL-10-/- mice to 9.5% oxygen results in PE-like changes, suggesting that a low concentration of IL-10 might be a biomarker for predicting PE (Table 1). We searched for articles in PubMed using the key words of “IL-10” AND B. PE was associated with elevated levels of IL-10 [86]. Kronborg et al. [87] collected blood samples during pregnancy from a cohort of 1631 women. Plasma levels of IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, TNF-α, IFN-γ and granulocyte macrophage colony-stimulating factor were measured at <25th, 26th-29th, 30th-35th, and >36th weeks in 32 women with PE and 67 normative pregnant women (controls). PE was associated with increased TNF-α between 26th and 29th
week and increased IL-6 after the 36th week, but other cytokines were comparable in women with PE and controls. Therefore, IL-10 might not be a biomarker candidate for predicting PE.
Nitric oxide (NO)
Administration of L-NAME as a nitric oxide synthase (NOS) inhibitor during mid- to late gestation results in PE-like changes [43-47], suggesting that the decrease of NO might be a candidate for predicting PE (Table 1). We searched for articles in PubMed using the following key words of (“asymmetric dimethylarginine” OR ADMA OR L-arginine OR “nitric oxide”) AND B. Asymmetric dimethylarginine (ADMA) and monomethylarginine (L-NMMA) compete with L-arginine, the substrate for nitric oxide synthase NOS [88]. Maternal plasma ADMA in the second and third trimesters has been reported to be higher in women with preeclampsia [88-92], although ADAM in the first trimester was not significantly different [93]. Kahlil [93] reported that L-arginine and L-homoarginine in the first trimester were significantly reduced in women with early-onset PE with delivery at <34 weeks of gestation than in unaffected controls. Therefore, the ADAM levels in the 2nd trimester might be a biomarker candidate for predicting PE.
Coagulation activation
Omatsu et al. [12] developed a murine PE model by injecting PS/PC microvesicles into Institute of Cancer Research (ICR) pregnant mice, and diffuse fibrin deposition was observed in the placentas, indicating that coagulation activation is one of the mechanisms for the development of PE (Table 1) [52, 53]. In a systematic review by Duckitt and Harrington [94], the presence of anticardiolipin antibodies or lupus anticoagulant or both significantly increased the risk of developing preeclampsia, suggesting that screening for coagulation activation might be useful to detect women at high risk forPE.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 9/12
Other
Mouse models of reduced uterine perfusion pressure (RUPP) [54-63] indicate the importance of normal physiological changes of the spiral artery in humans (Table 1). In another part of this Special Issue on the ‘Prediction of Preeclampsia’, Ohkuchi et al. discuss the role of uterine artery Doppler for predicting early-onset (EO)-PE.
Mouse models using sEng and sFlt-1 [4,5,64-71] indicate the role of increased levels of sFlt-1 and/or sEng before the onset of PE (Table 1). Elsewhere in this Special Issue, Hirashima et al. Discuss the role of angiogenesis-related factors for predicting EO-PE.
CONCLUSIONIn view of the animal models of PE, we can speculate that
several candidates remain to be elucidated in the future [26-28,30,35,37-41,48-51,72-80]. Recently, it has been reported that low-dose aspirin administered at <16 weeks of gestation might be useful to prevent the later occurrence of PE [95]. Therefore, screening women at high risk for PE at <16 weeks of gestation is very important. Not only circulating levels of protein, but also circulating levels of DNA, mRNA and micro RNA (miRNA) might be candidates for predicting PE in early pregnancy. Animal studies on the genesis of PE are very important tools for searching for biomarkers to predict PE in early pregnancy.
Angiogenic/angiostatic balance theory by sFlt-1, PlGF and sEng for the genesis of PE is one of the most successful models of translational research from bench to bed. However, the balance theory does not explain the genesis of PE entirely. Until now, clinically useful biomarkers other than angiogenesis-related factors have not been found. Basic research using animal models will gain insight into possible biomarker candidates for predicting PE.
CONTRIBUTORSH.S. and A.O. systematically searched for articles and selected
eligible articles, and A.O. wrote the manuscript. K.S, H.T, R.U, S.M. and M.S. critically reviewed the manuscript.
FINANCIAL DISCLOSUREThis work was supported by Grants-in-Aid (24390383 and
24592482 to A.O.) from the Ministry of Education, Culture, Sports, Science and Technology in Japan and a research grant (3-2417-011 to S.M.) from the Japan Association of Obstetricians and Gynecologists Ogyaa Donation Foundation.
REFERENCES1. Nagaya K, Fetters MD, Ishikawa M, Kubo T, Koyanagi T, Saito Y, et al.
Causes of maternal mortality in Japan. JAMA. 2000; 283: 2661-2667.
2. Hecher K, Campbell S, Doyle P, Harrington K, Nicolaides K. Assessment of fetal compromise by Doppler ultrasound investigation of the fetal circulation. Arterial, intracardiac, and venous blood flow velocity studies. Circulation. 1995; 91: 129-138.
3. Yamauchi A, Minakami H, Ohkuchi A, Usui R, Idei S, Sato I. Causes of stillbirth: an analysis of 77 cases. J Obstet Gynaecol Res. 1999; 25: 419-424.
4. Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, et al. Excess
placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003; 111: 649-658.
5. Venkatesha S, Toporsian M, Lam C, Hanai J, Mammoto T, Kim YM, et al. Soluble endoglin contributes to the pathogenesis of preeclampsia. Nat Med. 2006; 12: 642-649.
6. Krauss T, Pauer HU, Augustin HG. Prospective analysis of placenta growth factor (PlGF) concentrations in the plasma of women with normal pregnancy and pregnancies complicated by preeclampsia. Hypertens Pregnancy. 2004; 23: 101-111.
7. Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004; 350: 672– 683.
8. Levine RJ, Lam C, Qian C, Yu KF, Maynard SE, Sachs BP, et al. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia. N Engl J Med. 2006; 355: 992–1005.
9. Moore Simas TA, Crawford SL, Solitro MJ, Frost SC, Meyer BA, Maynard SE. Angiogenic factors for the prediction of preeclampsia in high-risk women. Am J Obstet Gynecol. 2007; 197: 244.e1– e8.
10. De Vivo A, Baviera G, Giordano D, Todarello G, Corrado F, D’anna R. Endoglin, PlGF and sFlt-1 as markers for predicting pre-eclampsia. Acta Obstet Gynecol Scand. 2008; 87: 837-842.
11. Lim JH, Kim SY, Park SY, Yang JH, Kim MY, Ryu HM. Effective prediction of preeclampsia by a combined ratio of angiogenesis-related factors. Obstet Gynecol. 2008; 111: 1403-1409.
12. Kusanovic JP, Romero R, Chaiworapongsa T, Erez O, Mittal P, Vaisbuch E, et al. A prospective cohort study of the value of maternal plasma concentrations of angiogenic and anti-angiogenic factors in early pregnancy and midtrimester in the identification of patients destined to develop preeclampsia. J Matern Fetal Neonatal Med. 2009; 22: 2021-1038.
13. Ohkuchi A, Hirashima C, Matsubara S, Takahashi K, Matsuda Y, Suzuki M . Threshold of soluble fms-like tyrosine kinase 1/placental growth factor ratio for the imminent onset of preeclampsia. Hypertension. 2011; 58: 859-866.
14. Ohkuchi A, Hirashima C, Takahashi K, Suzuki H, Matsubara S, Suzuki M. Onset threshold of the plasma levels of soluble fms-like tyrosine kinase 1/placental growth factor ratio for predicting the imminent onset of preeclampsia within 4 weeks after blood sampling at 19-31 weeks of gestation. Hypertens Res. 2013; 36: 1073-1080.
15. Ohkuchi A, Hirashima C, Matsubara S, Suzuki H, Takahashi K, Arai F, et al. Alterations in placental growth factor levels before and after the onset of preeclampsia are more pronounced in women with early onset severe preeclampsia. Hypertens Res. 2007; 30: 151-159.
16. Hirashima C, Ohkuchi A, Matsubara S, Suzuki H, Takahashi K, Usui R, et al. Alteration of serum soluble endoglin levels after the onset of preeclampsia is more pronounced in women with early-onset. Hypertens Res. 2008; 31: 1541-1548.
17. Ishibashi O, Ohkuchi A, Ali MM, Kurashina R, Luo SS, Ishikawa T,et al. Hydroxysteroid (17-b) dehydrogenase 1 is dysregulated by miR-210 and miR-518c that are aberrantly expressed in preeclamptic placentas: a novel marker for predicting preeclampsia. Hypertension. 2012; 59: 265-273.
18. Ohkuchi A, Ishibashi O, Hirashima C, Takahashi K, Matsubara S, Takizawa T, et al. Plasma level of hydroxysteroid (17-ß) dehydrogenase 1 in the second trimester is an independent risk factor for predicting preeclampsia after adjusting for the effects of mean blood pressure, bilateral notching and plasma level of soluble fms-like tyrosine kinase 1/placental growth factor ratio. Hypertens Res. 2012; 35: 1152-1158.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 10/12
19. Takimoto E, Ishida J, Sugiyama F, Horiguchi H, Murakami K, Fukamizu A. Hypertension induced in pregnant mice by placental renin and maternal angiotensinogen. Science 1996; 274: 995-998.
20. Bohlender J, Ganten D, Luft FC. Rats transgenic for human renin and human angiotensinogen as a model for gestational hypertension. J Am Soc Nephrol. 2000; 11: 2056-2061.
21. Brosnihan KB, Hering L, Dechend R, Chappell MC, Herse F. Increased angiotensin II in the mesometrial triangle of a transgenic rat model of preeclampsia. Hypertension. 2010; 55: 562-566.
22. Geusens N, Hering L, Verlohren S, Luyten C, Drijkoningen K, Taube M, et al. Changes in endovascular trophoblast invasion and spiral artery remodelling at term in a transgenic preeclamptic rat model. Placenta. 2010; 31: 320-326.
23. Falcao S, Stoyanova E, Cloutier G, Maurice RL, Gutkowska J, Lavoie JL. Mice overexpressing both human angiotensinogen and human renin as a model of superimposed preeclampsia on chronic hypertension. Hypertension. 2009; 54: 1401-1407.
24. Genest DS, Falcao S, Michel C, Kajla S, Germano MF, Lacasse AA, et al. Novel role of the renin-angiotensin system in preeclampsia superimposed on chronic hypertension and the effects of exercise in a mouse model. Hypertension. 2013; 62: 1055-1061.
25. Hering L, Herse F, Geusens N, Verlohren S, Wenzel K, Staff AC, et al. Effects of circulating and local uteroplacental angiotensin II in rat pregnancy. Hypertension 2010; 56: 311-318.
26. Davisson RL, Hoffmann DS, Butz GM, Aldape G, Schlager G, Merrill DC, et al. Discovery of a spontaneous genetic mouse model of preeclampsia. Hypertension. 2002; 39: 337-342.
27. Woods AK, Hoffmann DS, Weydert CJ, Butler SD, Zhou Y, Sharma RV, et al. Adenoviral delivery of VEGF121 early in pregnancy prevents spontaneous development of preeclampsia in BPH/5 mice. Hypertension. 2011; 57: 94-102.
28. Hoffmann DS, Weydert CJ, Lazartigues E, Kutschke WJ, Kienzle MF, Leach JE, et al. Chronic tempol prevents hypertension, proteinuria, and poor feto-placental outcomes in BPH/5 mouse model of preeclampsia. Hypertension. 2008; 51: 1058-1065.
29. Singh J, Ahmed A, Girardi G. Role of complement component C1q in the onset of preeclampsia in mice. Hypertension. 2011; 58: 716-724.
30. Ahmed A, Singh J, Khan Y, Seshan SV, Girardi G. A new mouse model to explore therapies for preeclampsia. PLoS One. 2010; 5: e13663.
31. Kanasaki K, Palmsten K, Sugimoto H, Ahmad S, Hamano Y, Xie L, et al. Deficiency in catechol-O-methyltransferase and 2-methoxyoestradiol is associated with pre-eclampsia. Nature. 2008; 453: 1117-1121.
32. Stanley JL, Andersson IJ, Poudel R, Rueda-Clausen CF, Sibley CP, Davidge ST, et al. Sildenafil citrate rescues fetal growth in the catechol-O-methyl transferase knockout mouse model. Hypertension. 2012; 59: 1021-1028.
33. Freitag N, Tirado-González I, Barrientos G, Herse F, Thijssen VL, Weedon-Fekjær SM, et al. Interfering with Gal-1-mediated angiogenesis contributes to the pathogenesis of preeclampsia. Proc Natl Acad Sci U S A. 2013; 110: 11451-11456.
34. Cudmore M, Ahmad S, Al-Ani B, Fujisawa T, Coxall H, Chudasama K, et al. Negative regulation of soluble Flt-1 and soluble endoglin release by heme oxygenase-1. Circulation. 2007; 115: 1789-1797.
35. Wang K, Ahmad S, Cai M, Rennie J, Fujisawa T, Crispi F, et al. Dysregulation of hydrogen sulfide producing enzyme cystathionine γ-lyase contributes to maternal hypertension and placental abnormalities in preeclampsia. Circulation. 2013; 127: 2514-2522.
36. Nishizawa H, Hasegawa K, Suzuki M, Achiwa Y, Kato T, Saito K,
et al. Mouse model for allogeneic immune reaction against fetus recapitulates human pre-eclampsia. J Obstet Gynaecol Res. 2008; 34: 1-6.
37. Zhou CC, Zhang Y, Irani RA, Zhang H, Mi T, Popek EJ, et al. Angiotensin receptor agonistic autoantibodies induce pre-eclampsia in pregnant mice. Nat Med. 2008; 14: 855-862.
38. Siddiqui AH, Irani RA, Zhang W, Wang W, Blackwell SC, Kellems RE, et al. Angiotensin receptor agonistic autoantibody-mediated soluble fms-like tyrosine kinase-1 induction contributes to impaired adrenal vasculature and decreased aldosterone production in preeclampsia. Hypertension. 2013; 61: 472-479.
39. Zhou CC, Irani RA, Dai Y, Blackwell SC, Hicks MJ, Ramin SM, et al. Autoantibody-mediated IL-6-dependent endothelin-1 elevation underlies pathogenesis in a mouse model of preeclampsia. J Immunol. 2011; 186: 6024-6034.
40. Zhou CC, Irani RA, Zhang Y, Blackwell SC, Mi T, Wen J, et al. Angiotensin receptor agonistic autoantibody-mediated tumor necrosis factor-alpha induction contributes to increased soluble endoglin production in preeclampsia. Circulation. 2010; 121: 436-444.
41. Irani RA, Zhang Y, Zhou CC, Blackwell SC, Hicks MJ, Ramin SM, et al. Autoantibody-mediated angiotensin receptor activation contributes to preeclampsia through tumor necrosis factor-alpha signaling. Hypertension. 2010; 55: 1246-1253.
42. Lai Z, Kalkunte S, Sharma S. A critical role of interleukin-10 in modulating hypoxia-induced preeclampsia-like disease in mice. Hypertension. 2011; 57: 505-514.
43. Herraiz S, Pellicer B, Serra V, Cauli O, Cortijo J, Felipo V, et al. Sildenafil citrate improves perinatal outcome in fetuses from pre-eclamptic rats. BJOG. 2012; 119: 1394-1402.
44. Souza CO, Peraçoli MT, Weel IC, Bannwart CF, Romão M, Nakaira-Takahagi E, et al. Hepatoprotective and anti-inflammatory effects of silibinin on experimental preeclampsia induced by L-NAME in rats. Life Sci. 2012; 91: 159-165.
45. Talebianpoor MS, Mirkhani H. The effect of tempol administration on the aortic contractile responses in rat preeclampsia model. ISRN Pharmacol. 2012; 2012: 187208.
46. Yang X, Guo L, Sun X, Chen X, Tong X. Protective effects of hydrogen-rich saline in preeclampsia rat model. Placenta. 2011; 32: 681-686.
47. Ramesar SV, Drewes SE, Gathiram P, Moodley J, Mackraj I. The effect of Kraussianone-2 (Kr2), a natural pyrano-isoflavone from Eriosema kraussianum, in an L-NAME- induced pre-eclamptic rat model. Phytother Res. 2012; 26: 1375-1380.
48. Vu HV, Ianosi-Irimie MR, Pridjian CA, Whitbred JM, Durst JM, Bagrov AY, et al. Involvement of marinobufagenin in a rat model of human preeclampsia. Am J Nephrol. 2005; 25: 520-528.
49. Plaks V, Rinkenberger J, Dai J, Flannery M, Sund M, Kanasaki K, et al. Matrix metalloproteinase-9 deficiency phenocopies features of preeclampsia and intrauterine growth restriction. Proc Natl Acad Sci U S A. 2013; 110: 11109-11114.
50. Valbuena-Diez AC, Blanco FJ, Oujo B, Langa C, Gonzalez-Nuñez M, Llano E, et al. Oxysterol-induced soluble endoglin release and its involvement in hypertension. Circulation. 2012; 126: 2612-2624.
51. Kanayama N, Takahashi K, Matsuura T, Sugimura M, Kobayashi T, Moniwa N, et al. Deficiency in p57Kip2 expression induces preeclampsia-like symptoms in mice. Mol Hum Reprod. 2002; 8: 1129-1135.
52. Omatsu K, Kobayashi T, Murakami Y, Suzuki M, Ohashi R, Sugimura

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 11/12
M, et al. Phosphatidylserine/phosphatidylcholine microvesicles can induce preeclampsia-like changes in pregnant mice. Semin Thromb Hemost. 2005; 31: 314-320.
53. Zhang Y, Hua Z, Zhang K, Meng K, Hu Y. Therapeutic effects of anticoagulant agents on preeclampsia in a murine model induced by phosphatidylserine/phosphatidylcholine microvesicles. Placenta. 2009; 30: 1065-1070.
54. Alexander BT, Cockrell K, Cline FD, Llinas MT, Sedeek M, Granger JP. Effect of angiotensin II synthesis blockade on the hypertensive response to chronic reductions in uterine perfusion pressure in pregnant rats. Hypertension. 2001; 38: 742-745.
55. George EM, Cockrell K, Aranay M, Csongradi E, Stec DE, Granger JP. Induction of heme oxygenase 1 attenuates placental ischemia-induced hypertension. Hypertension. 2011; 57: 941-948.
56. Amaral LM, Pinheiro LC, Guimaraes DA, Palei AC, Sertório JT, Portella RL, et al. Antihypertensive effects of inducible nitric oxide synthase inhibition in experimental pre-eclampsia. J Cell Mol Med. 2013; 17: 1300-1307.
57. Lillegard KE, Johnson AC, Lojovich SJ, Bauer AJ, Marsh HC, Gilbert JS, et al. Complement activation is critical for placental ischemia-induced hypertension in the rat. Mol Immunol. 2013; 56: 91-97.
58. LaMarca B, Wallace K, Herse F, Wallukat G, Martin JN Jr, Weimer A, et al. Hypertension in response to placental ischemia during pregnancy: role of B lymphocytes. Hypertension. 2011; 57: 865-871.
59. Tam Tam KB, George E, Cockrell K, Arany M, Speed J, Martin JN Jr, et al. Endothelin type A receptor antagonist attenuates placental ischemia-induced hypertension and uterine vascular resistance. Am J Obstet Gynecol. 2011; 204: 330.e1-4.
60. Morton JS, Abdalvand A, Jiang Y, Sawamura T, Uwiera RR, Davidge ST. Lectin-like oxidized low-density lipoprotein 1 receptor in a reduced uteroplacental perfusion pressure rat model of preeclampsia. Hypertension. 2012; 59: 1014-1020.
61. Walsh SK, English FA, Crocker IP, Johns EJ, Kenny LC . Contribution of PARP to endothelial dysfunction and hypertension in a rat model of pre-eclampsia. Br J Pharmacol. 2012; 166: 2109-2116.
62. McCarthy FP, Drewlo S, Kingdom J, Johns EJ, Walsh SK, Kenny LC. Peroxisome proliferator-activated receptor-γ as a potential therapeutic target in the treatment of preeclampsia. Hypertension. 2011; 58: 280-286.
63. Cornelius DC, Hogg JP, Scott J, Wallace K, Herse F, Moseley J, et al. Administration of interleukin-17 soluble receptor C suppresses TH17 cells, oxidative stress, and hypertension in response to placental ischemia during pregnancy. Hypertension. 2013; 62: 1068-1073.
64. Lu F, Longo M, Tamayo E, Maner W, Al-Hendy A, Anderson GD, et al. The effect of over-expression of sFlt-1 on blood pressure and the occurrence of other manifestations of preeclampsia in unrestrained conscious pregnant mice. Am J Obstet Gynecol. 2007; 196: 396.e1-7.
65. Suzuki H, Ohkuchi A, Matsubara S, Takei Y, Murakami M, Shibuya M, et al. Effect of recombinant placental growth factor 2 on hypertension induced by full-length mouse soluble fms-like tyrosine kinase 1 adenoviral vector in pregnant mice. Hypertension. 2009; 54: 1129-1135.
66. Li Z, Zhang Y, Ying Ma J, Kapoun AM, Shao Q, Kerr I, et al. Recombinant vascular endothelial growth factor 121 attenuates hypertension and improves kidney damage in a rat model of preeclampsia. Hypertension. 2007; 50: 686-692.
67. Bergmann A, Ahmad S, Cudmore M, Gruber AD, Wittschen P, Lindenmaier W, et al. Reduction of circulating soluble Flt-1 alleviates
preeclampsia-like symptoms in a mouse model. J Cell Mol Med. 2010; 14: 1857-1867.
68. Mateus J, Bytautiene E, Lu F, Tamayo EH, Betancourt A, Hankins GD, et al. Endothelial growth factor therapy improves preeclampsia-like manifestations in a murine model induced by overexpression of sVEGFR-1. Am J Physiol Heart Circ Physiol. 2011; 301: H1781-7.
69. Lu F, Bytautiene E, Tamayo E, Gamble P, Anderson GD, Hankins GD, et al. Gender-specific effect of overexpression of sFlt-1 in pregnant mice on fetal programming of blood pressure in the offspring later in life. Am J Obstet Gynecol. 2007; 197: 418.e1-5.
70. Kumasawa K, Ikawa M, Kidoya H, Hasuwa H, Saito-Fujita T, Morioka Y, et al. Pravastatin induces placental growth factor (PGF) and ameliorates preeclampsia in a mouse model. Proc Natl Acad Sci U S A. 2011; 108: 1451-1455.
71. Fox KA, Longo M, Tamayo E, Kechichian T, Bytautiene E, Hankins GD, et al. Effects of pravastatin on mediators of vascular function in a mouse model of soluble Fms-like tyrosine kinase-1-induced preeclampsia. Am J Obstet Gynecol. 2011; 205: 366.
72. Murakami Y, Kobayashi T, Omatsu K, Suzuki M, Ohashi R, Matsuura T, et al. Exogenous vascular endothelial growth factor can induce preeclampsia-like symptoms in pregnant mice. Semin Thromb Hemost. 2005; 31: 307-313.
73. Doridot L, Passet B, Méhats C, Rigourd V, Barbaux S, Ducat A, et al. Preeclampsia-like symptoms induced in mice by fetoplacental expression of STOX1 are reversed by aspirin treatment. Hypertension. 2013; 61: 662-668.
74. Nash P, Wentzel P, Lindeberg S, Naessén T, Jansson L, Olovsson M, et al. Placental dysfunction in Suramin-treated rats--a new model for pre-eclampsia. Placenta. 2005; 26: 410-418.
75. Carlström M, Wentzel P, Skøtt O, Persson AE, Eriksson UJ. Angiogenesis inhibition causes hypertension and placental dysfunction in a rat model of preeclampsia. J Hypertens. 2009; 27: 829-837.
76. Zenclussen AC, Fest S, Joachim R, Klapp BF, Arck PC. Introducing a mouse model for pre-eclampsia: adoptive transfer of activated Th1 cells leads to pre-eclampsia-like symptoms exclusively in pregnant mice. Eur J Immunol. 2004; 34: 377-387.
77. McRae JL, Russell PA, Chia JS, Dwyer KM. Overexpression of CD39 protects in a mouse model of preeclampsia. Nephrology (Carlton). 2013; 18: 351-355.
78. Chatterjee P, Weaver LE, Doersch KM, Kopriva SE, Chiasson VL, Allen SJ, et al. Placental Toll-like receptor 3 and Toll-like receptor 7/8 activation contributes to preeclampsia in humans and mice. PLoS One. 2012; 7: e41884.
79. Chatterjee P, Chiasson VL, Kopriva SE, Young KJ, Chatterjee V, Jones KA, et al. Interleukin 10 deficiency exacerbates toll-like receptor 3-induced preeclampsia-like symptoms in mice. Hypertension. 2011; 58: 489-496.
80. Kopriva SE, Chiasson VL, Mitchell BM, Chatterjee P. TLR3-induced placental miR-210 down-regulates the STAT6/interleukin-4 pathway. PLoS One. 2013; 8: e67760.
81. Kolla V, Jenö P, Moes S, Lapaire O, Hoesli I, Hahn S. Quantitative proteomic (iTRAQ) analysis of 1st trimester maternal plasma samples in pregnancies at risk for preeclampsia. J Biomed Biotechnol. 2012; 2012: 305964.
82. Ringholm L, Pedersen-Bjergaard U, Thorsteinsson B, Boomsma F, Damm P, Mathiesen ER. A high concentration of prorenin in early pregnancy is associated with development of pre-eclampsia in women with type 1 diabetes. Diabetologia. 2011; 54: 1615-1619.

Central
Ohkuchi et al. (2013)Email:
Med J Obstet Gynecol 2(2): 1031 (2014) 12/12
83. Watanabe N, Bokuda K, Fujiwara T, Suzuki T, Mito A, Morimoto S, et al. Soluble (pro)renin receptor and blood pressure during pregnancy: a prospective cohort study. Hypertension. 2012; 60: 1250-1256.
84. Farina A, Sekizawa A, De Sanctis P, Purwosunu Y, Okai T, Cha DH, et al. Gene expression in chorionic villous samples at 11 weeks’ gestation from women destined to develop preeclampsia. Prenat Diagn. 2008; 28: 956-961.
85. Nakamura M, Sekizawa A, Purwosunu Y, Okazaki S, Farina A, Wibowo N, et al. Cellular mRNA expressions of anti-oxidant factors in the blood of preeclamptic women. Prenat Diagn. 2009; 29: 691-696.
86. Lau SY, Guild SJ, Barrett CJ, Chen Q, McCowan L, Jordan V, et al. Tumor necrosis factor-alpha, interleukin-6, and interleukin-10 levels are altered in preeclampsia: a systematic review and meta-analysis. Am J Reprod Immunol. 2013; 70: 412-427.
87. Kronborg CS, Gjedsted J, Vittinghus E, Hansen TK, Allen J, Knudsen UB. Longitudinal measurement of cytokines in pre-eclamptic and normotensive pregnancies. Acta Obstet Gynecol Scand. 2011; 90: 791-796.
88. Speer PD, Powers RW, Frank MP, Harger G, Markovic N, Roberts JM. Elevated asymmetric dimethylarginine concentrations precede clinical preeclampsia, but not pregnancies with small-for-gestational-age infants. Am J Obstet Gynecol. 2008; 198: 112.
89. Fickling SA, Williams D, Vallance P, Nussey SS, Whitley GS. Plasma concentrations of endogenous inhibitor of nitric oxide synthesis in
normal pregnancy and pre-eclampsia. Lancet. 1993; 342: 242-243.
90. Holden DP, Fickling SA, Whitley GS, Nussey SS. Plasma concentrations of asymmetric dimethylarginine, a natural inhibitor of nitric oxide synthase, in normal pregnancy and preeclampsia. Am J Obstet Gynecol. 1998; 178: 551-556.
91. Pettersson A, Hedner T, Milsom I. Increased circulating concentrations of asymmetric dimethyl arginine (ADMA), an endogenous inhibitor of nitric oxide synthesis, in preeclampsia. Acta Obstet Gynecol Scand. 1998;77: 808-813.
92. Savvidou MD, Hingorani AD, Tsikas D, Frölich JC, Vallance P, Nicolaides KH. Endothelial dysfunction and raised plasma concentrations of asymmetric dimethylarginine in pregnant women who subsequently develop pre-eclampsia. Lancet. 2003; 361: 1511-1517.
93. Khalil AA, Tsikas D, Akolekar R, Jordan J, Nicolaides KH. Asymmetric dimethylarginine, arginine and homoarginine at 11-13 weeks’ gestation and preeclampsia: a case-control study. J Hum Hypertens. 2013; 27: 38-43.
94. Duckitt K, Harrington D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. BMJ. 2005; 330: 565.
95. Roberge S, Villa P, Nicolaides K, Giguère Y, Vainio M, Bakthi A, et al. Early administration of low-dose aspirin for the prevention of preterm and term preeclampsia: a systematic review and meta-analysis. Fetal Diagn Ther. 2012; 31: 141-146.
Suzuki H, Ohkuchi A, Shirasuna K, Takahashi H, Usui R, et al. (2014) Animal Models of Preeclampsia: Insight into Possible Biomarker Candidates for Predicting Preeclampsia. Med J Obstet Gynecol 2(2): 1031.
Cite this article