angiogenic factors as tumor markers
TRANSCRIPT

Investigational New Drugs 15: 29–37, 1997. 29c 1997 Kluwer Academic Publishers. Printed in the Netherlands.
Angiogenic factors as tumor markers
Mai NguyenAssistant Professor of Surgery, University of California, Los Angeles, USA
Key words: angiogenesis, angiogenic factor, tumor marker, serum, urine
Summary
The process of angiogenesis plays a critical role in tumor growth and metastasis. Recently, there has been muchinterest in the possible use of angiogenic growth factors as tumor markers. This paper will review the results thusfar of attempts at measuring various angiogenic factors in bodily fluids. In the future, angiogenic factors will mostlikely be useful as a monitor of therapy and/or a predictor of outcome after cancer has been diagnosed.
Introduction
In the past few decades, researchers have becomeincreasingly interested in the observation that tumorgrowth and metastasis are accompanied by signifi-cant new blood vessel formation i.e., angiogenesis.In the adult, the process of angiogenesis is normalduring menstruation and wound repair. When bloodvessels grow unabated and out of control, angiogene-sis becomes pathological and sustains the progressionof many neoplastic and non-neoplastic diseases. Thiswork, pioneered in large part by Dr. Judah Folkman,led to the hypothesis that tumors are “angiogenesis-dependent”. In the early prevascular phase, tumorsare usually thin and cell population is limited. Withthe onset of angiogenesis, the tumor cell populationrapidly expands and metastasizes. This hypothesis issupported by multiple animal experiments in whichtumors implanted in chicks, rodents and rabbits arerestricted in growth during the avascular phase, butrapid growth and metastasis occur shortly after vas-cularization. In addition, angiogenesis inhibitors thatare not cytostatic to tumor cells in vitro inhibit tumorgrowth and metastasis in the animals in vivo [1].
Angiogenesis is a complex multistep process whichincludes endothelial cell proliferation, migration anddifferentiation into tube-like structures. These stepsinvolve multiple growth factors and adhesion mole-cules among endothelial cells as well as those withother supporting cells. Up to now, approximate-
ly 15 angiogenic peptides have been identified andsequenced [2]. These include basic and acidic fibrob-last growth factor (bFGF and aFGF), vascular endothe-lial growth factor (VEGF), epidermal growth fac-tor (EGF), transforming growth factor-alpha and beta(TGF-� and TGF-�), hepatocyte growth factor (HGF),tumor necrosis factor-alpha (TNF-�), interleukin-8(IL-8), granulocyte colony stimulating factor (G-CSF),E-selectin, angiogenin, platelet-derived endothelialcell growth factor (PD-ECGF), placental growth fac-tor and pleiotrophin. These angiogenic molecules areeither released by the tumor cells themselves, or mobi-lized from extracellular matrix and/or released by hostcells such as macrophages recruited into the tumor.
Multiple clinical observations in human cancerhave added support to the hypothesis that tumors areangiogenesis-dependent. Angiogenesis, as determinedby the amount of vascularity in the tumor specimen,was first shown to have prognostic significance inbreast cancer by Weidner et al. in 1991 [3]. The num-ber of vessels in a tumor specimen correlates with thedisease stage and can add prognostic prediction inde-pendent of other routinely used markers. Since 1991,an overwhelming majority of published reports haveshown a significant correlation between the densityof intratumoral microvessels of invasive breast carci-noma and the incidence of metastases and/or patientsurvival. Similar associations have now been reportedfor patients with melanoma, prostate carcinoma, tes-ticular carcinoma, ovarian carcinoma, rectal carcino-

30
ma, bladder carcinoma, central nervous system tumors,multiple myeolma, non-small-cell lung carcinoma,andsquamous carcinoma of the head and neck [4].
The above vascular density, however, can only bedetermined in pathological specimens at the time oftumor resection or subsequent biopsies. We are inter-ested in finding a marker or multiple markers of angio-genesis which can be measured repeatedly withoutinvasive procedures. More than ten years ago, Chodaket al. demonstrated that the urine of patients withbladder and renal cancers stimulate the migration ofcapillary endothelial cells, an important component ofangiogenesis [5]. The endothelial chemokinetic activi-ty of urine samples was consistently reduced to normallevels after tumor removal, and the reappearance ofthis activity was associated with recurrence of tumorgrowth.
Since many angiogenic growth factors have nowbeen identified and sequenced, we asked whether thelevel of any of these factors could be detected in bodilyfluids, and whether their levels have any clinical rel-evance in cancer diagnostics and monitoring. Studiesfrom our laboratory and from other institutions haveshown that angiogenic growth factors can be signifi-cantly elevated in the serum and urine of patients witha wide variety of cancer types. The levels of certainangiogenic factors have been shown to correlate withdisease stage of the tumor. From the published dataso far, certain conclusions can be made regarding theuse of angiogenic factors as tumor markers. First, atumor type can be associated with multiple angiogenicfactors, and an angiogenic factor can be associatedwith multiple tumor types. Second, the measurementof angiogenic factors will most likely not be useful asdiagnostic or screening tools for cancer. Finally, thelevel of angiogenic factors may be used in the futureas a monitor of therapy and/or a predictor of outcomeafter cancer has been diagnosed.
This paper will review the results thus far ofattempts at measuring various angiogenic factors inbodily fluids, and will offer suggestions for the possi-ble future use of angiogenic factors as tumor markers.
Fibroblast growth factor
FGF, one of the most potent angiogenic factors, hasbeen reported to be widely distributed among nor-mal and neoplastic tissue [2]. However, a sensitiveimmunoassay for the detection of bFGF in bodily flu-ids was not reported until 1991. The immunoassay forbFGF developed by Watanabe et al. is specific for bio-
Table 1. Angiogenic factors in different tumor types
Angiogenic Tumor with Refer-factor abnormal levels ences
FGF Bladder, renal, prostate, testicular, breast,colon, lung, gastrointestinal, brain, ovarian,cervical, sarcoma, lymphoma, leukemia,MEN1
7–18
VEGF Breast, uterine, ovarian, lung 2, 19EGF Brain, liver, esophageal, gastric, colon,
lung, breast, cervical, ovarian, head & neck,lymphoma, leukemia, genitourinary
20–25
TGF Breast, liver, gastric, colon, esophageal,pancreatic, bladder
26–30
HGF Bladder 31Cytokines Ovarian, colon 32–33E-selectin Breast, ovarian, gastrointestinal, multiple
myeloma37
logically active bFGF and has a detection limit of 10pg/ml [6]. In serum, the detection limit is 30 pg/ml andin concentrated urine, the limit is 0.1 pg/ml.
The first clinical use of this bioassay was by Fuji-moto et al. 1991 [7]. These authors measured serumand urine levels of bFGF and aFGF in 31 patients withrenal cell carcinoma. In over 50% (16/31) of thesepatients, bFGF was elevated (> 30 pg/ml) in their sera.There was relatively good correlation between serumlevels of bFGF and tumor size, grade, and tumor inva-sion of the renal vein. These authors did not detectany bFGF in the urine of these patients. aFGF was notfound in any serum or urine samples. In 1995, Fuji-moto et al. extended their patient population to includepatients with renal cell carcinoma, renal pelvic andureteral cancer, bladder, prostate and testicular cancer.They found that renal cell carcinoma had a higher ten-dency toward increased serum levels of bFGF than anyof the other urogenital tumors [8].
We used the same bioassay but concentrated thecollected urine samples 100-fold by processes of dial-ysis and lyophilization. Because the hydration statusand urinary output of each subject varied, each urinebFGF value was normalized against urine creatininecontent. We collected urine samples from 950 patientshaving a wide variety of solid tumors, leukemia orlymphoma and from a control group consisting of 87healthy volunteers and 198 patients with non-cancer-related diseases [9]. Male control subjects had a medianbFGF level of 151 pg/g and female control subjects amedian of 237 pg/g, with a combined 90th percentile of619 pg/g. An elevated level of bFGF was found in theurine of some of the patients with virtually every type oftumor studied including kidney, bladder, prostate, tes-

31
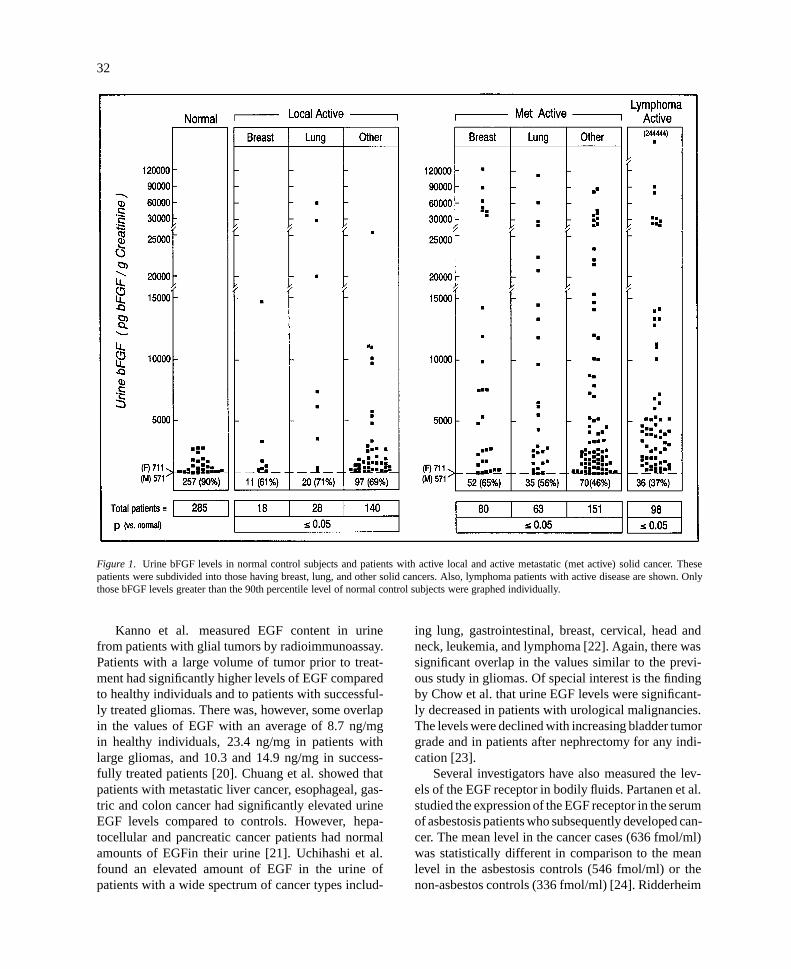
ticular, breast, colon, lung, brain, ovarian, sarcoma andlymphoma (Figure 1). In the solid cancer patients cate-gorized as having no evidence of disease, bFGF levelswere not significantly different from those in normalcontrol subjects. 31% of patients with active local and47% of patients with metastatic active cancers showedelevated bFGF levels. Survival among cancer patientsat the median follow-up time was 85–88% for thosewith “normal” and 71–72% for those with “elevated”urine bFGF levels. Urine levels of bFGF were not inde-pendently prognostic for survival over and above theprognostic effects of clinical status and disease stage.However, in a group of 39 patients with bladder can-cer, urine bFGF was found to be more sensitive thancytology for diagnostic purposes [10].
We also used the same bioassay in order to measurebFGF levels in patients’ serum. We found no detectablebFGF in the serum of 204 healthy blood donors. 6% of235 patients with breast cancer had detectable bFGF(> 30 pg/ml). An elevated bFGF level was associatedwith a 5.9 fold increase in mortality risk and a 2.7 foldincrease in recurrence of disease at 15 months com-pared to patients with undetectable serum bFGF lev-els. The increase in mortality risk predicted by bFGFin these patients was found to be independent of oth-er prognostic factors including disease stage and thepatient’s clinical status [11]. Zimering et al. founddetectable bFGF in the serum of patients with multi-ple endocrine neoplasia type 1 (MEN1) ranging from0.24 to 1.28 ng/ml, whereas normal controls had unde-tectable amount of bFGF (< 0.2 ng/ml) [12].
Since the publication of these studies, there hasbeen a technical improvement in the ELISA forFGF allowing a detection level of 1 pg/ml. Thisincreased sensitivity will hopefully improve on theabove 6% detection in breast cancer patients’ serum.The improved detection will also eliminate the need forconcentrating urine samples by dialysis and lyophiliza-tion and thereby greatly simplify FGF measurements.
Using this new improved assay, O’Brien et al. mea-sured urine bFGF from 38 patients with ongoing blad-der tumor, 21 with no residual bladder tumor, and 24control subjects. They found that urine bFGF was high-er in patients with active bladder cancer than in thosewith a clear cytoscopy. Using a threshold value of 4ng/g, the sensitivity of the test for detecting cancer was62% and specificity was 70% [13]. Lin et al. studiedurine by bFGF in patients with Wilms’ tumor. bFGFwas found to be elevated in 42% of preoperative sam-ples when compared to age-matched controls. Patientswith stage III, IV, and V disease had significantly high-
er levels of urinary bFGF compared to those with stageI and II disease [14]. aFGF levels in the urine wasstudied by Chopin et al. In this study, the majority ofpatients with advanced bladder cancer had detectableaFGF levels in their urine. Healthy controls did nothave any detectable aFGF in their urine [15].
The improved assay was also used by other inves-tigators to measure serum levels of bFGF. Sliutz etal. studied 20 patients suffering from cervical cancer,and found significantly higher bFGF levels in patientswith active disease compared with those in remission.When applying a cut-off level of 15 pg/ml, serum bFGFreached a sensitivity of 66% and a specificity of 92%[16]. Takei et al. measured serum bFGF in patientswith breast cancer and found significant elevations inall stages of disease. It is unclear why the assay used inthis study detected a few hundreds of pg/ml amount ofbFGF in the serum of even control subjects, which wassignificantly higher than previously reported amountsby other investigators [17].
Of note, bFGF has been detected in the cere-brospinal fluid (CSF). Li et al. tested CSF from 26patients with brain tumors and from 18 control sub-jects. These investigators detected bFGF in the CSF of62% (16/26) patients with brain tumors but in none ofthe controls. The level of bFGF also correlated withmitogenic activity in CSF in vitro and with density ofmicrovessels in histological sections [18].
Vascular endothelial growth factor
VEGF is a homodimeric 32–42 kDa heparin-bindingglycoprotein with potent angiogenic, endothelial cell-specific mitogenic and vascular permeabillity-enhanc-ing activities [2].
In preliminary studies and yet unpublished data,Folkman has found that VEGF is abnormally elevatedin the serum of breast cancer patients [2]. Kondo etal. have previously shown that serum VEGF levelsin patients with uterine, ovarian and lung cancer areelevated compared to those of normal controls [19].
Epidermal growth factor
EGF is a 52-amino acid polypeptide originally dis-covered in extracts of the male mouse submandibulargland. It has been shown that EGF stimulates DNAsynthesis and cell division in various tissues includingthe endothelium [2].
32
Figure 1. Urine bFGF levels in normal control subjects and patients with active local and active metastatic (met active) solid cancer. Thesepatients were subdivided into those having breast, lung, and other solid cancers. Also, lymphoma patients with active disease are shown. Onlythose bFGF levels greater than the 90th percentile level of normal control subjects were graphed individually.
Kanno et al. measured EGF content in urinefrom patients with glial tumors by radioimmunoassay.Patients with a large volume of tumor prior to treat-ment had significantly higher levels of EGF comparedto healthy individuals and to patients with successful-ly treated gliomas. There was, however, some overlapin the values of EGF with an average of 8.7 ng/mgin healthy individuals, 23.4 ng/mg in patients withlarge gliomas, and 10.3 and 14.9 ng/mg in success-fully treated patients [20]. Chuang et al. showed thatpatients with metastatic liver cancer, esophageal, gas-tric and colon cancer had significantly elevated urineEGF levels compared to controls. However, hepa-tocellular and pancreatic cancer patients had normalamounts of EGFin their urine [21]. Uchihashi et al.found an elevated amount of EGF in the urine ofpatients with a wide spectrum of cancer types includ-
ing lung, gastrointestinal, breast, cervical, head andneck, leukemia, and lymphoma [22]. Again, there wassignificant overlap in the values similar to the previ-ous study in gliomas. Of special interest is the findingby Chow et al. that urine EGF levels were significant-ly decreased in patients with urological malignancies.The levels were declined with increasing bladder tumorgrade and in patients after nephrectomy for any indi-cation [23].
Several investigators have also measured the lev-els of the EGF receptor in bodily fluids. Partanen et al.studied the expression of the EGF receptor in the serumof asbestosis patients who subsequently developed can-cer. The mean level in the cancer cases (636 fmol/ml)was statistically different in comparison to the meanlevel in the asbestosis controls (546 fmol/ml) or thenon-asbestos controls (336 fmol/ml) [24]. Ridderheim

33
et al. measured the level of EGF receptors in the urineof ovarian cancer patients, and found that radicallyoperated women excreted significantly less EGF recep-tors into urine than women with residual tumor mass.However, the authors reported that the highest levelswere found in normal premenopausal women and inwomen with non-ovarian malignancies [25].
Transforming growth factor
TGF’s are stable multifunctional polypeptide growthfactors, which recently have been found to be angio-genic as well [2].
Chakrabarty et al. found that patients with breastcancer have significantly elevated serum levels of TGF-� (mean 353 pg/ml) compared to healthy individuals(mean 144 pg/ml) [26]. Stromberg et al. measuredurinary levels of TGF-� in women with disseminatedbreast cancer and normal controls. The median TGF-� value for women with breast cancer was 981 ng/gcompared to 642 ng/g for healthy women. Althoughthe difference was statistically different, the overlap inthe levels was rather high [27]. Chuang et al. showedthat patients with hepatocellular, metastatic liver, gas-tric and colon cancer had elevated uringary TGF-�compared to controls. However, esophageal and pan-creatic cancer patients had normal amounts of TGF-�in their urine [21]. In contrast, Moskal et al. mea-sured serum TGF-� in patients with multiple types ofgastrointestinal cancer and found a mean of 269 pg/mlcompared with the normal mean of 147 pg/ml. The ele-vations were significant in esophageal and pancreaticcancer as well [28]. On the other hand, Fazekas-Mayet al. failed to find any significant elevations in urinaryTGF-� in patients with head and neck cancer [29].
Eder et al. found that patients with bladder cancerhad detectable levels of TGF-�1 and TGF-�2 in theirurine in comparison with undetectable levels in con-trol subjects. Serum TGF-�1 and TGF-�2 were alsosignificantly elevated in these patients compared withcontrols [30].
Hepatocyte growth factor
HGF is a protein secreted by stromal cells that inducesdisruption of intercellular junctions and stimulatesmotility and invasiveness of carcinoma cells. HGF isalso a potent inducer of angiogenesis [2].
Joseph et al. found that urinary HGF was signif-icantly elevated in patients with bladder carcinomaas compared with normal control subjects as well as
patients with prostate cancer. Interestingly, patientswith benign prostate conditions such as benign pro-static hypertrophy (BPH) and prostatitis had levels ofHGF similar to those with prostate cancer [31].
Cytokines
TNF-�, granulocyte colony-stimulating factor andinterleukin-8 are inflammatory cytokines which havealso been found to be angiogenic [2]. There has beenreport by Moradi et al. showing significantly elevatedlevels of TNF-� in the serum of patients with ovariancancer compared to normal controls [32]. Ueda et al.found elevated serum levels of IL-8 and GM-CSF inpatients with colorectal cancer. In this study, however,TNF-� was not detected in any of these patients [33].
E-selectin
E-selectin is an adhesion molecule expressed byendothelial cells which mediates endothelial-leukocyteinteractions during inflammation. Recently, cell sur-face E-selectin has been shown to be important inangiogenesis, and soluble E-selectin is an angiogenicgrowth factor [34, 35]. There has been one report fromBanks et al. which showed that E-selectin is elevated inthe serum of patients with breast, ovarian, gastrointesti-nal cancer and multiple myeloma. There was, however,a significant amount of overlap between the normal lev-els and the cancer patients’ levels of E-selectin. AlsoE-selectin was not elevated in patients with bladder,renal cancer and lymphoma [36].
Elevation of angiogenic factors in non-cancerconditions
Angiogenesis is a process which is not specific forcancer alone. In the healthy adult, angiogenesis occursin the female endometrium during the menstrual cycleand pregnancy. Angiogenesis is also important in theprocess of wound healing. In the neonate or infant,angiogenesis accompanies the normal growth anddevelopment. There are also non-malignant diseasesin the adult which are associated with new blood ves-sel growth, and these include diabetic retinopathy andrheumatoid arthritis.
In our previous studies, we have measured urinebFGF from 17 inpatients during the first week fol-lowing non-cancer related major surgery, and found

34
a significantly elevated bFGF median level of 1,351pg/g. We have also found that there was a statisticaldifference between healthy male and female controlsubjects. Male subjects had a median bFGF level of151 pg/g and female a level of 237 pg/g [9]. We mea-sured urine bFGF in 23 women during the first trimesterof pregnancy and found a median of 260 pg/g, whichwas not statistically different from non-pregnant wom-en. In contrast, four women in their last trimester ofpregnancy had a significantly elevated bFGF medianlevel of 1,587 pg/g. Hill et al. measured serum bFGFin pregnant women, and found that bFGF was presentfrom at least 18 weeks gestation. Serum bFGF roseto a maximum value at week 28–31 of gestation [37].Hill et al. also found that maternal serum bFGF wasmildly but significantly elevated in women who devel-op diabetes during pregnancy compared to those whodo not. Interestingly, women with pregestational dia-betes or women who only have glucose intolerance didnot have significantly higher serum bFGF compared toother pregnant women [38].
O’Brien et al. found that bFGF was elevated inthe urine of patients with benign prostatic hypertrophy(BPH median 4.52 ng/g, control median 2.08 ng/g)[13]. We measured urine bFGF in 24 patients with BPHand found no statistically significant difference (BPHmedian 198 pg/g versus 151 pg/g in male controls). Wealso observed no significant difference in three patientswith prostatitis (prostatitis median 146 pg/g). Josephet al. studied a different angiogenic factor, HGF, inthe urine and found a significant elevation in prostati-tis but not in BPH [31]. Chopin et al. found that 10%of patients with BPH or some inflammatory urolog-ical disease had elevated aFGF levels in their urine[15]. Further studies need to be carried out with largernumbers of subjects in order to definitively determinewhether benign diseases of the prostate are associatedwith an increase in angiogenic factors in the urine.
Of note, VEGF has been found in non-tumor dis-eases. Ocular fluid of patients with diabetic retinopathyand other retinal diseases involving neovascularizationcontained elevated levels of VEGF [39].
It is also important to recognize that many of theangiogenic growth factors have physiological func-tions other than in the process of capillary formation.Therefore, the level of these growth factors may be ele-vated in other disease processes. For example, TNF-�and E-selectin are involved in processes of infectionand inflammation and have been found to be elevatedin septic shock [40]. D’Amore et al. found that serumbFGF was elevated in some patients with Duchenne
Muscular Dystrophy, consistent with their hypothesisthat the instability of the muscle plasma membrane dueto dystrophin deficiency leads to leakage of bFGF [41].
The future of angiogenic growth factors as tumormarkers
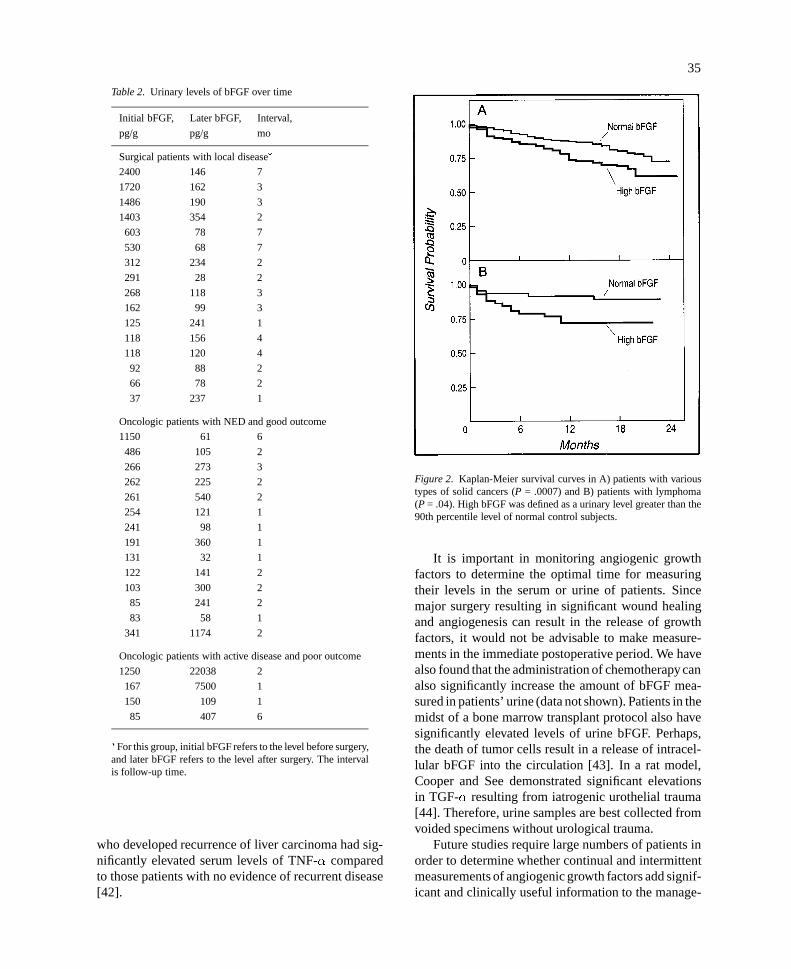
Based on the results from the above studies involv-ing different types of tumor, it appears that the mea-surement of angiogenic growth factors is not specificenough for screening or diagnosis of cancer. However,there seems to be much promise in the use of angio-genic factors as markers of therapeutic efficacy andas assessment of an individual patient’s prognosis. Inour previously published study, we have found that fol-lowing complete surgical removal of tumor, previouslyelevated urine bFGF levels decreased into the normalrange. In the vast majority of patients who had noevidence of disease following medical therapy, urinelevels of bFGF either decreased or remained withinthe normal range when measured again a few monthslater. Patients with progressive disease had increasedbFGF levels detected after repeat urine samples (Table2). In addition, taken as a group, survival among can-cer patients at the median follow-up time was 85–88%for those with “normal” and 71–72% for those with“elevated” urine bFGF levels (Figure 2).
Other investigators have also found that repeatedmeasurements of angiogenic growth factors correlatewith the individual’s clinical disease status. Fujimotoet al. found that patients with renal cell carcinomano longer had detectable bFGF in the serum followingcomplete removal of their tumors [8]. Lin et al. showedthat patients with relapse or persistent Wilms’ tumorhad significantly elevated late postoperative urinarybFGF levels when compared to disease-free patients[14]. Sliutz et al. studied serum bFGF in patients withcervical cancer. In these patients, a continuous increaseof bFGF serum levels before the clinical detection ofrelapse was seen in two out of four cases with a meanlead time of four months [16]. Zimering et al. showedthat successful surgery or bromocryptine treatment inpatients with pituitary tumor was associated with afall in serum bFGF levels [12]. One patient who hadincreased tumor size also had a coincident rise in bFGFlevel. Kanno et al. found that surgical intervention andirradation seemed to influence longitudinal fluctuationsof urinary EGF in patients with gliomas. At the termi-nal stage of the disease, urine EGF levels became sig-nificantly elevated [20]. Nakazaki showed that patients
35
Table 2. Urinary levels of bFGF over time
Initial bFGF, Later bFGF, Interval,
pg/g pg/g mo
Surgical patients with local disease�
2400 146 7
1720 162 3
1486 190 3
1403 354 2
603 78 7
530 68 7
312 234 2
291 28 2
268 118 3
162 99 3
125 241 1
118 156 4
118 120 4
92 88 2
66 78 2
37 237 1
Oncologic patients with NED and good outcome
1150 61 6
486 105 2
266 273 3
262 225 2
261 540 2
254 121 1
241 98 1
191 360 1
131 32 1
122 141 2
103 300 2
85 241 2
83 58 1
341 1174 2
Oncologic patients with active disease and poor outcome
1250 22038 2
167 7500 1
150 109 1
85 407 6
�For this group, initial bFGF refers to the level before surgery,and later bFGF refers to the level after surgery. The intervalis follow-up time.
who developed recurrence of liver carcinoma had sig-nificantly elevated serum levels of TNF-� comparedto those patients with no evidence of recurrent disease[42].
Figure 2. Kaplan-Meier survival curves in A) patients with varioustypes of solid cancers (P = .0007) and B) patients with lymphoma(P = .04). High bFGF was defined as a urinary level greater than the90th percentile level of normal control subjects.
It is important in monitoring angiogenic growthfactors to determine the optimal time for measuringtheir levels in the serum or urine of patients. Sincemajor surgery resulting in significant wound healingand angiogenesis can result in the release of growthfactors, it would not be advisable to make measure-ments in the immediate postoperative period. We havealso found that the administration of chemotherapy canalso significantly increase the amount of bFGF mea-sured in patients’ urine (data not shown). Patients in themidst of a bone marrow transplant protocol also havesignificantly elevated levels of urine bFGF. Perhaps,the death of tumor cells result in a release of intracel-lular bFGF into the circulation [43]. In a rat model,Cooper and See demonstrated significant elevationsin TGF-� resulting from iatrogenic urothelial trauma[44]. Therefore, urine samples are best collected fromvoided specimens without urological trauma.
Future studies require large numbers of patients inorder to determine whether continual and intermittentmeasurements of angiogenic growth factors add signif-icant and clinically useful information to the manage-

36
ment of patients with cancer. In addition, we need todetermine whether a complete profile with all knownangiogenic growth factors is important, or whether acertain growth factor is more appropriate for a specifictumor type. With the advent of multiple clinical trialsinvolving angiogenic inhibitors as anti-tumor agents,we may find that determination of the level of angio-genic factor(s) is particularly appropriate in order tomonitor therapeutic progress.
References
1. Folkman J: Angiogenesis in cancer, vascular, rheumatoid andother disease. Nature Med 1:27–31, 1995
2. Folkman J: Tumor angiogenesis. In: Mendelsohn J, HowleyPM, Israel MA, Liotta LA (eds). The molecular basis of cancer.WB Saunders, 1995, pp 206–232
3. Weidner N, Semple JP, Welch WR, Folkman J: Tumor angio-genesis and metastasis – correlation in invasive breast carcino-ma. New Engl J Med 324:1–8, 1991
4. Weidner N: Tumor angiogenesis: Review of current applica-tions in tumor prognostication. Presented at a national meetingon New cancer strategies: angiogenesis antagonists, Washing-ton DC, 1995
5. Chodak GW, Scheiner CJ, Zetter BR: Urine from patients withtransitional-cell carcinoma stimulates migration of capillaryendothelial cells. New Eng J Med 305:869–874, 1981
6. Watanabe H, Hori A, Seno M, Kozai Y, Igarashi K, IchimoriY, Kondo K: A sensitive enzyme immunoassay for humanbasic fibroblast growth factor. Biochem Biophys Res Comm175:229–235, 1991
7. Fujimoto K, Ichimori Y, Kakizoe T, Okajima E, SakamotoH, Sugimura T, Terada M: Increased serum levels of basicfibroblast growth factor in patients with renal cell carcinoma.Biochem Biophys Res Comm 180:386–392, 1991
8. Fujimoto K, Ichimori Y, Yamaguchi H, Arai K, Futami T,Ozono S, Hirao Y, Kakizoe T, Terada M, Okajima E: Basicfibroblast growth factor as a candidate tumor marker for renalcell carcinoma. Jpn J Cancer Res 86:182–186, 1995
9. Nguyen M, Watanabe H, Budson AE, Richie JP, Hayes DF,Folkman J: Elevated levels of an angiogenic peptide, basicfibroblast growth factor, in the urine of patients with a widespectrum of cancer. J Natl Cancer Inst 86: 356–361, 1994
10. Nguyen M, Watanabe H, Budson AE, Richie JP, FolkmanJ: Elevated levels of the angiogenic peptide basic fibroblastgrowth factor in urine of bladder cancer patients. J Nat CancerInst 85:241–242, 1993
11. Watanabe H, Nguyen M, Schizer M, Li V, Hayes D, Sallan S,Folkman J: Basic fibroblast growth factor in human serum –A prognostic test for breast cancer (Abstract). Molec Biol Cell3S:234a, 1992
12. Zimering MB, Katsumata N, Sato Y, Brandi ML, Aurbach GD,Marx SJ, Friesen HG: Increased basic fibroblast growth factorin plasma from multiple endocrine neoplasia type 1: Relationto pituitary tumor. J Clin Endocrin Metab 76:1182–1187, 1993
13. O’Brien TS, Smith K, Cranston D, Fuggle S, Bicknell R, HarrisAL: Urinary basic fibroblast growth factor in patients withbladder cancer and benign prostatic hypertrophy. Br J Urol76:311–314, 1995
14. Lin RY, Argenta PA, Sullivan KM, Adzick NS: Diagnosticand prognostic role of basic fibroblast growth factor in Wilms’tumor patients. Clin Cancer Res 1:327–331, 1995
15. Chopin DK, Caruelle JP, Colombel M, Palcy S, Ravery V,Caruelle D, Abbou CC, Barritault D: Increased immunode-tection of acidic fibroblast growth factor in bladder cancer,detectable in urine. J Urology 150:1126–1130, 1993
16. Sliutz G, Tempfer C, Obermair A, Reinthaller A, Gitsch G,Kainz C: Serum evaluation of basic fibroblast growth factor incervical cancer patients. Cancer Let 94:227–231, 1995
17. Takei Y, Kurobe M, Uchida A, Hayashi K: Serum concentra-tions of basic fibroblast growth factor in breast cancer. ClinChem 40:1980–1981, 1994
18. Li VW, Folkerth RD, Watanabe H, Yu C, Rupnick M, BarnesP, Scott RM, Black PM, Sallan SE, Folkman J: Microvesselcount and cerebrospinal fluid basic fibroblast growth factor inchildren with brain tumours. Lancet 344:82–86, 1994
19. Kondo S, Asano M, Matsuo K, Ohmori I, Suzui H: Vas-cular endothelial growth factor/vascular permeability factoris detectable in the sera of tumor-bearing mice and cancerpatients. Biochem Biophys Acta 1221:211–214, 1994
20. Kanno H, Chiba Y, Kyuma Y, Hayashi A, Abe H, TakadaH, Kim I, Yamamoto I: Urinary epidermal growth factor inpatients with gliomas: significance of the factor as a glial tumormarker. J Neurosurg 79:408–413, 1993
21. Chuang LY, Hung WC, Yang ML, Chang CC, Tsai JF: Uri-nary epidermal growth factor receptor-binding growth factorsin patients with cancers of the digestive tract. Clin Biochem27:485–489, 1994
22. Uchihashi M, Hirata Y, Nakajim H, Fujita T, Matsukura S:Urinary excretion of human epidermal growth factor (hEGF)in patients with malignant tumors. Horm Metab Res 15:261–262, 1983
23. Chow NH, Tzai TS, Cheng PE, Chang CJ, Lin JSN, Tang MJ:An assessment of immunoreactive epidermal growth factor inurine of patients with urological diseases. Urol Res 22:221–225, 1994
24. Partanen R, Hemminki K, Koskinen H, Luo JC, Carney WP,Brandt-Rauf PW: The detection of increased amounts of theextracellular domain of the epidermal growth factor receptorin serum during carcinogenesis in asbestosis patients. J OccMed 36:1324–1328, 1994
25. Ridderheim M, Cajander S, Tavelin B, Stendahl U, BackstromT: EGF/TGF-� and progesterone in urine of ovarian cancerpatients. Antic Res 14:2119–2124, 1994
26. Chakrabarty S, Huang S, Moskal TL, Fritsche HA: Elevatedserum levels of transforming growth factor-� in breast cancerpatients. Cancer Let 79:157–160, 1994
27. Stromberg K, Duffy M, Fritsch C, Hudgins R, Sharp ES, Mur-phy LD, Lippman ME, Bates SE: Comparison of urinary trans-forming growth factor-� in women with disseminated breastcancer and healthy control women. Cancer Det Prev 15:277–283, 1991
28. Moskal TL, Huang S, Ellis LM, Fritsche HA, Chakrabarty S:Serum levels of transforming growth factor � in gastrointesti-nal cancer patients. Cancer Epid Biom Prev 4:127–131, 1995
29. Fazekas-May M, Suen JY, Yeh YC, Yeh HW, Milligan LB:Investigation of urinary transforming growth factor alpha levelsas tumor markers in patients with advanced squamous cellcarcinoma of the head and neck. Head Neck 12:411–416, 1990
30. Eder IE, Stenzl A, Cronauer MV, Bartsch G, Klocker H: Trans-forming growth factor-�1 and -�2 and basic fibroblast growthfactor in serum and urine from patients with bladder cancer(Abstract). Proc Am Assoc Cancer Res 36:1461, 1995
37
31. Joseph A, Weiss GH, Jin L, Fuchs A, Chowdhury S, O’Shaug-nessy P, Goldberg ID, Rosen EM: Expression of scatter factorin human bladder carcinoma. J Nat Cancer Inst 87:372–377,1995
32. Moradi MM, Carson LF, Winberg JB, Haney AF, Twiggs LB,Ramakrishnan S: Serum and ascitic fluid levels of interleukin-1, interleukin-6, and tumor necrosis factor-alpha in patientswith ovarian epithelial cancer. Cancer 72:2433–2440, 1993
33. Ueda T, Shimada E, Urakawa T: Serum levels of cytokinesin patiets with colorectal cancer: Possible involvement ofinterleukin-6 and interleukin-8 in hematogenous metastasis.J Gastroenterol 29:423–429, 1994
34. Nguyen M, Strubel N, Bischoff J: A role for sialyl Lewis-X/Aglycoconjugates in capillary morphogenesis. Nature 365:267–269, 1993
35. Koch AE, Halloran MM, Haskell CJ, Shah MR, Polverini PJ:Angiogenesis mediated by soluble forms of E-selectin andvascular cell adhesion molecule-1. Nature 376:517–519, 1995
36. Banks RE, Gearing AJH, Hemingway IK, Norfolk DR, PerrenTJ, Selby PJ: Circulating intercellular adhesion molecule-1(ICAM-1), E-selectin and vascular cell adhesion molecule-1(VCAM-1) in human malignancies. Br J Cancer 68:122–124,1993
37. Hill DJ, Tevaarwerk GJM, Arany E, Kilkenny D, GregoryM, Langford KS, Miell J: Fibroblast growth factor 2 (FGF-2) is present in maternal and cord serum, and in the motheris associated with a binding protein immunologically relatedto the FGF receptor-1. J Clin Endocrin Metab 80:1822–1831,1995
38. Hill DJ, Tevaarwerk GJM, Caddell C, Arany E, Kilkenny D,Gregory M: Fibroblast growth factor 2 is elevated in term
maternal and cord serum and amniotic fluid in pregnanciescomplicated by diabetes: relationship to fetal and placentalsize. J Clin Endocrin Metab 80:2626–2632, 1995
39. Aiello LP, Avery RL, Arrigg PG, Keyt BA, Jampel HD, ShahST, Pasquale LR, Thieme H, Iwamoto MA, Park JE, NguyenHV, Aiello LM, Ferrara N, King GL: Vascular endothelialgrowth factor in ocular fluid of patients with diabetic retinopa-thy and other retinal disorders. New Engl J Med 331:1480–1487, 1994
40. Newman W, Beall LD, Carson CW, Hunter GG, Graben N,Rndhawa ZI, Gopal TV, Wiener-Kronish J, Matthay MA: Sol-uble E-selectin is found in supernatants of activated endothelialcells and is elevated in the serum of patients with septic shock.J Immunol 150(2):644–654, 1993
41. D’Amore PA, Brown RH, Ku PT, Hoffman EP, Watanabe H,Arahata K, Ishihara T, Folkman J: Elevated basic fibroblastgrowth factor in the serum of patients with Duchenne MuscularDystrophy. Ann Neurol 35:362–365, 1994
42. Nakazaki H: Preoperative and postoperative cytokines inpatients with cancer. Cancer 70:709–713, 1992
43. Soutter AD, Nguyen M, Watanabe H, Folkman J: Basic fibrob-last growth factor secreted by an animal tumor is detectable inurine. Cancer Res 53:5297–5299, 1993
44. Cooper CS, See WA: The impact of iatrogenic urothelial trau-ma on urinary levels of transforming growth factor-alpha. JUrol 147:1647–1649, 1992
Address for offprints: Mai Nguyen, UCLA Surgery/Oncology, CHS54-140, 10833 Leconte Avenue, Los Angeles, CA 90095, USA (Tel:310-206-2215; Fax: 310-825-7575)