anesthesie voor vaatheelkunde - website - uz leuven · 21-10-2016 4 carotid endarterectomie •...
TRANSCRIPT

21-10-2016
1
Dr. Danny HoogmaAnesthesiology
Anesthesia for vascular surgery
Overview
• Introduction
• Preoperative optimalization
• Monitoring
• Intra-operative management– Carotid endarterectomy– Aortic surgery
– Peripheral vascular surgery
• Conclusion
Leerdoelen:
• Atherosclerose is een systeem ziekte
• Carotis end-arterectomie– monitoring– complicaties
• Aorta chirurgie en cross-clamp
• Perifeer vasculaire chirurgie is high risk
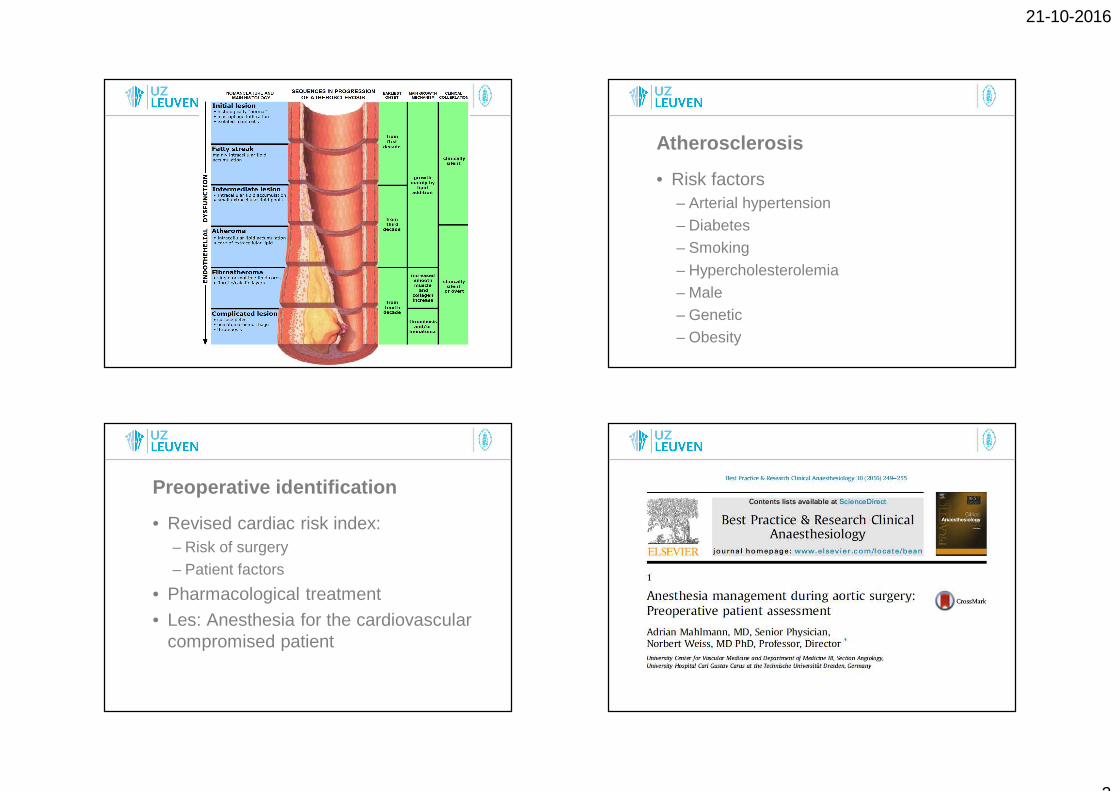
Introduction
• Atherosclerosis– Systemic disease
• Endothelial dysfunction• End-organ dysfunction possible
– Lipids accumulation– Inflammatory proces
21-10-2016
2
Atherosclerosis
• Risk factors– Arterial hypertension– Diabetes– Smoking
– Hypercholesterolemia– Male– Genetic– Obesity
Preoperative identification
• Revised cardiac risk index:– Risk of surgery– Patient factors
• Pharmacological treatment
• Les: Anesthesia for the cardiovascular compromised patient

21-10-2016
3
Clinical evaluation
• Cardiac, neurological, pulmonary, renal…
• Diabetes
• Smoking
• Bloodpressure– Bilateral measurement
Preoperative investigations
• Functional capacity
• ECG
• Cardiac stress testing
• …
Monitoring
• Hemodynamic:– Bloodpressure
– ECG, lead II en V– Centrale acces– TEE– Fore-sight / NIRS / Neurowave
• Neurological:– SSEP/MEP/EEG– Clinically
Perioperative management
• Carotid endarterectomy
• Aortic surgery
• Peripheral vascular surgery

21-10-2016
4
Carotid endarterectomie
• Symptoms: – Amaurosis fugax -> CVA
• Etiology– Progressieve occlusie door plaque
• Circulus van Willis
– Emboli
• Intervention?– Highly beneficial: symptomatisch / stenose 70-99%
– Moderately beneficial: 50-69% stenose (occulairplethysmografie)
Type of anaesthesia
• Regional?– Cervical blok C1-C4– Neuromonitoring +++
• General anesthesie?– Control (pulmonary and hemodynamic)
– Potential protective effect of anaesthetics
• Goal = maintain bloodpressure = perfussion
Cerebral circulation
• Aerobic metabolism
• Major part of cardiac output– CBF = 50 ml/100g/min
• Prone for irreversible ischaemia– Threshold = CBF < 20 ml/100g/min
• Blood brain barrier
• Rigid box

21-10-2016
5
CBF and brain tissue
Cerebral bloodflow
• Autonomic nervous system– Perfusion pressure = MAP-ICP
Cerebral bloodflow
• Metabolic regulation– Nerve activity (adenosin)– PaCO2
– pH CSV
– PaO2

21-10-2016
6
Monitoring• Carotid stump pressure?
– CBF not known– Low specificity (> shunts)
• Transcranial doppler?– A. Cerebri media
• Continuous, non invasive and detection of emboli possible• Only 1 vessel…, what about signal detection
• NIRS?– Evaluation delivery vs consumption– Only frontal cortex
• EEG en SSEP?– EEG: cerebral activity, SSEP: evalution of nerve fiber up to the cortex– Neuron evaluation: hibernation if CBF <16-18 ml/100g/min, cell necrosis if <10-12
ml/100g/min– Multifactorial interference
Carotid endarterectomie
• Perioperative events– Emboli 60-95%
• Manipulation carotis = surgeon
– Hypoperfusion = anaesthetist• Autoregulatory dysfunction (belang perfusie
druk)• Normal-high bloodpressure
– ‘light anesthesia’ + vasopressors
– Glycemia < 150 mg/dl
Carotid endarterectomie
• Perioperative events– Rhythm disturbances
• Glomus/vagus manipulation � atropin/lidocain
– Ventilation• Hypocapnia
– Decreased CBF
• Hypercapnia– Vasodilation in non-ischemic areas (steal
phenomenon)
Carotid endarterectomie
• Shunt needed?– Hypoperfusion (cave emboli)
• Lengthens procedure time

21-10-2016
7
Carotid endarterectomie
– Patient selection!• Preoperative
– occlusion/stenosis other vessels? – Recent ischemia = high risk for new perioperative event
• Clinical neurological evaluation • Hemodynamic evaluation
– Carotid stump pressure (insufficient specificity)– Transcranial doppler– NIRS
• Neurologic evaluation– EEG, SSEP, Neurowave– Effect anesthestics
CAS = carotid artery stenting
Carotid endarterectomie
• Postoperative– Neurologic evaluation
• Epileptic insult, nerve injury (surgical), TIA/CVA
– Hemodynamic instability• Baroreceptor dysfunction
– Hyperperfusion syndrome– Bleeding
• Cave difficult airway
– Cardiac morbidity (myocardial infarction)
Aortic surgery
• Dissection
• Rupture
• Aneurysm
• Occlusion

21-10-2016
8
Aortic surgery
• Cross-clampling– Major cardiovascular, humoral en metabolic
impact
• Artery of Adamkiewicz– Drainage of liquor?
• Deep hypothermic cooling with circulation stop or usage of the octopussystem
Impact of cross-clamping
Hemodynamic
Myocardial
Metabolic
Renal
Pulmonary
Spinal
Zammert M, Gelman S. The pathophysiology of aortic cross-clamping. Best Practice & Research Clinical Anaesthesiology. 2016 Sep;30(3):257–69.
Redistribution of blood volume
Geen examen-leerstof
Gelman S, Anesthesiology, 1995

21-10-2016
9
Systemic hemodynamic response
Geen examen-leerstof
Gelman S, Anesthesiology, 1995
Spinal cord blood flow
Geen examen-leerstof
Gelman S, Anesthesiology, 1995
Pathophysiology cross-clamp
Geen examen-leerstof
Peroperative management
• Afterload– Supra-coeliacus clamping (nitrates)
• Preload ↓(nitrates)
• Sympatic block (epidural)
• Shunting– Flow distal to clamp
– Individual organ perfusion

21-10-2016
10
Monitoring during TAA
• Periferal IV line/invasive ABP/CVC
• ABG/ACT
• Spinal catheter
• Bladder catheter
• Temperature
• TEE/MEP/SSEP/…
Removal of aortic cross-clamp
• Anticipation– Optimalization of intravascular volume– Vasopressors– Progressive declamping
– Pharmacological intervention (ie: bicarbonate, potassium,…)
Unclamping
Geen examen-leerstof
Gelman S, Anesthesiology, 1995
21-10-2016
11
Peripheral vascular surgery
• Inflow vs outflow procedure
• Ischemia– 5P: pain, pallor, pulseless, paresthesia,
paralyse
• Claudicatio � cave mobidity and mortality equals abdominal aortic aneurysm repair
Type of anesthesia
• Often general anesthesia
• Regional anesthesia if indicated– Neuraxial LRA often impossible– Peripheral LRA certainly possible
• Risk of perioperative myocardialinfarction no different
Endovascular procedure
• Thoracic and abdominal– EVAR since the ‘80
• Advantage of less surgical inducedstress reponse with a decreasedhemodynamic effects
• Decreased operative mortability andmorbidity but similar long-term outcome
Conclusion
• Hemodynamic stability– Know your pharmacology, the product isn’t
‘dangerous'!• Hypnotics, NMBA, opioid, fluids…
– Decreased tolerance to disturbances