anesthesiafor)achild)with)congenital)heart disease) • milrinone)(pdi)) _ increaseof...
TRANSCRIPT
Anesthesia for a child with congenital heart disease

Congenital heart disease
• CHD is the most common birth defect, occurring in approximately 1/125 births, 90% survive to adulthood.
• Extracardiac anomalies requiring surgery withing the first year of life are present in 30% of paIents.
• Children with CHD undergoing norcardiac surgery are at increased risk of perioperaIve morbidity and mortality compared with other children.

• Majority of cardiac arrest occur during noncardiac surgery.
• 75% of the paIents were under two years old.
• 75% of deaths accounted for by three disInct defects: aorIc stenosis, cardiomyopathy and single ventricle lesions.
PreoperaIve evaluaIon
• Dg: AV-‐VA discordace, PS, LPA stenosis, VSD, B-‐T shunt x 2
HOW DOES THE BLOOD FLOW?

ClassificaIon of concenital heart lesions
Classification Physiology Effect Examples Cyanotic: Normal pulmonary blood flow
Mixing of arterial and venous blood in common cardiac chambers
Cyanosis Polycythemia
Single venticles Double outlet RV TGA with ASD or VSD
Cyanotic: Decreased pulmonary blood flow
Obstruction of PBF leads to shunting at the atrial and/or ventricular level
Cyanosis+ CHF Polycythemia
TOF Severe pulmonary stenosis Pulmonary atresia
Acyanotic: Increased pulmonary blood flow
Left to right shunt at the atrial, ventricular or great vessel level leads to preferential flow to the low resistance pulmonary bed
PDA & ASD: Clinically normal AVSD / VSD: CHF if severe
ASD VSD AVSD PDA Aortopulmonary window
Acyanotic: Obstructed blood flow
No shunt, but blood flow is ostructed
CHF Mild pulmonary stenosis Aortic stenosis Coarctation of the aorta
PreoperaIve evaluaIon
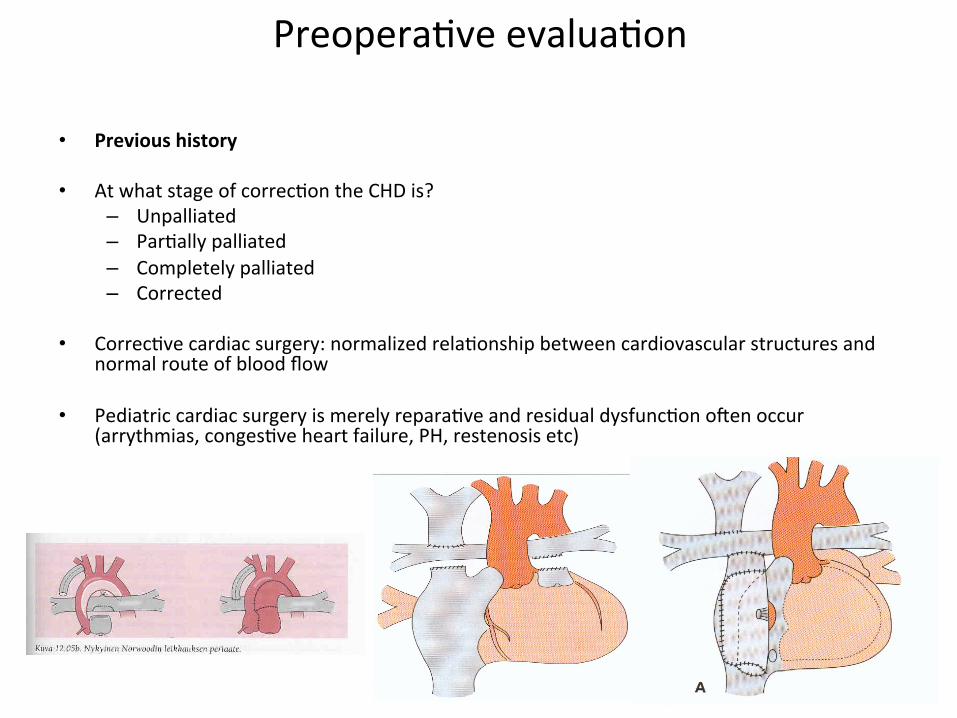
• Previous history
• At what stage of correcIon the CHD is? – Unpalliated – ParIally palliated – Completely palliated – Corrected
• CorrecIve cardiac surgery: normalized relaIonship between cardiovascular structures and normal route of blood flow
• Pediatric cardiac surgery is merely reparaIve and residual dysfuncIon o[en occur (arrythmias, congesIve heart failure, PH, restenosis etc)

PreoperaIve evaluaIon
• How does the blood flow?
• Echocardiography – Anatomic defects / shunts – Ventricular funcIon – Valve funcIon – Doppler and colour flow imaging -‐> direcIon of flow through defect/valves, velociIes/pressure
gradients • Latest cardiac cathethrizaIon
– Size and locaIon of defects – Degree of stenosis or shunt – Pressure cradients and sat02 in each chamber and great vessels – Mixed venous 02 saturaIon in SVC or proximal to area where shunt occurs – Low saturaIons in LA and LV -‐> right to le[ shunt – High saturaIons in RA and RV -‐> le[ to right shunt – RaIo of pumonary to systemic blood flow Qp / Qs

PreoperaIve evaluaIon
• FuncIonal status – Daily acIviIes and exercise tolerance – Tacyphnea, dyspnea, cyanosis – Infants; respiratory distress during feeding – Arrythmias, syncope, chest pain – Hypertension / hypotension – Murmurs / pulmonary auscultaIon – InfecIon
• 12 lead EKG – Chamber enlargement / hypertrophy – ConducIon defects / arrythmias – ConducIon defects – Arrythmias – Ischemia

PreoperaIve evaluaIon
• Chest x-‐ray – Heart size and shape – Prominence of pulmonary vascularity – InfecIon
• Pulse oximetry
• Blood tests – Electrolyte disturbaces (diureIc therapy, renal dysfuncIon) – Hemoglobin / hematocrit level is a good indicator of severity / chronicity of cyanosis – CoagulaIon tests – Arterial blood gases – Calcium and blood glucose especially newborns/neonates/criIcally ill children

PreoperaIve evaluaIon
• Drug history – Generally all cardiac medicaIons should be given on the morning of surgery – ACE inhibitors? – Aspirin therapy to prevent shunt thrombosis should usually be conInued – Children with warfarin therapy need to be admiged to hospital for anIcoagulant
monitoring and considering LMWH prior to elecIve surgery?
• PremedicaIon – Used to avoid distress, minimize oxygen consumpIon and maybe to reduce the amount
of inducIon agent. – -‐> less undesirable hemodynamic and respiratory symptoms before/during inducIon – midazolam 0.3-‐0.5 mg/kg, diazepam 0.3-‐0.5 mg/kg – monitoring of spO2
• EndocardiIs porphylaxis – Follow appropriate guidelines.

IntraoperaIve monitoring
• Depends a lot on complexity of the heart defect and surgery
• ECG, Sp02 x 1-‐2, ETCO2, NIBP are standard
• A-‐lines and CVP
• TEE
• NIRS
• Temperature (oesophagus, rectum, bladder)
• Diuresis

IntraoperaIve monitoring
• PDA – Pulse oximetry on right hand -‐> preductal saturaIon – Pulse oximetry on lower limb -‐> postductal saturaIon
• AorIc coarctaIon – Pulse oximetry on right upper limb – Arterial line on right upper limb – (Pre-‐ and post-‐coarctaIon blood pressure measuremaents )

AnestheIc techniques
• InducIon and maintenance
– Dependent on age and cardiac reserve – Cood cardiac funcIon -‐> inhalaIonal or i.v. inducIon and maintenance
– Poor funIon / cardiac reserve -‐> slow i.v. InducIon
– Neonates -‐> sevoflurane, S-‐ketamine, midazolame, dexmedetomidine, opiates
– Be careful with PVR changes during inhalaIonal inducIon due to changes in PaO2, PCO2 and intrathoracic presssure

InhalaIonal agents
• InducIon usually well toleratered
• Sevoflurane – Ligle effect on myocardial contracIlity or shunt fracIon – Don’t decrease heart rate – Decrease in SVR, decreases MAP, may improve systemic flow in L-‐>R shunts – CardioprotecIve effect
• Isoflurane – High insidence of laryngospasm -‐> not good for inducIon – Ligle effect on myocardial contacIlity or shunt fracIon – VasodilaIon -‐> decreases MAP -‐> increases HR
• Desflurane – High insidence of laryngospasm – Decreases SVR, increases HR
• Nitrous oxide – May enlarge intravascular air emboli and cause obstrucIon of blood flow in arteries and capillaries – In shunts possibility for bubbles to be shunted into systemic circulaIon – Don’t use in children with limited pulmonary blood flow or PHT – Is there a reason to use?

IV-‐anestheIcs
• S-‐Ketamine – SympatomimeIc effects helps to maintain HR, contracIlity, MAP – No effect on PAP or PVR – Useful with unstable hemodynamics, neonates – Well tolerated in children with pulmonary hypertension
• Propofol – Depress myocardial funcIon, decrease SVR, MAP – No effect on HR, PAP, PVR – Can be used for most paIents – Not for very unstable paIents or neonates
• Thiopental – Depress myocardial funcIon, decrease SVR, MAP – For inducIon, also for neonates, no pain – Not for very unstbale paIents
• Midazolam – Ligle effect on contracIlity, SVR and MAP – Useful for neonates and hemodynamically unstable paIents

IV-‐anestheIcs
• Opioids – No cardiodepressant effect if bradycardia avoided – High dose opioid anesthesia well tolerated in unstable paIents
• Etomidate – Don’t depress heart contracIly or decrease SVR, MAP – Adrenal gland depression – Rarely used – For inducIon of very unstable paIents?
• Dexmedetomidine – Hemodynamically stable anesthesia (adjuvant) – Can cause bradycardia – Can be useful in treaIng tachyarythmias – Not the best choice for paIents with AV-‐nodal conducIon defects

alfa1 alfa2 beeta1 beeta2 V1 V2
epinephrine +++ +++ +++ +++
norepinephrine +++ +++ ++ +
phenylephrine ++ ++ -‐ -‐
vasopressin -‐ -‐ -‐ -‐ +++ +++
Vasopressors
• Epinephrine – Beeta1 dominant with small doses, alfa1 effect increases with dose – Increases HR, coronary flow, CO, BP, oxygen consumpIon, – Tachyarytmias, pulmonary vasoconstricIon
• Norepinephrine – Alfa1 dominant – Increases SVR, weak beeta1 inotropic effect – High doses -‐> tachyarythmias, pulmonary vasoconstricIon
• Phenylephrine – Increases SVR with potent alfa acIvity, virtually no beeta effect – Primarely as a rapid bolus, bolus / infusion to decrease oullow track gradient – No direct heart rate effect, reflectory baroreceptor mediated rensponse a[er alteraIons in MAP
• Vasopressin – ConstricIon of vascular smooth muscle (V1) and increased SVR, water reabsoprIon in renal
collecIng duct (V2) – Increases vascular sensiIvity to cathecolamines, effects preserved during acidoIc condiIons

Inotropes
• Milrinone (PDI) -‐ Increase of intracellular cAMP and calcium by inhibiIon of cAMP breakdown in cardiac myocytes and vascular smooth muscle
-‐ Inotropic, lusitropic and vasodilaIve effect -‐ Decreases PBP and SVR -‐ Basic and well tolerated intropic infusion -‐ Loading dose 50 ug/kg during 0.5-‐2h, conIniuous infusion 0.375-‐0.75 ug/kg/min -‐ Side-‐effecs hypotension, ventricular arrythmias (rare)
• Levosimendan
– SensiIzaIon of contracIle protein troponin C to intracellular calcium – Openin of Kalium channels on vascular smooth muscle – Enhances ventricular contracIlity without increasing oxygen consumpIon – Pulmonary and systemic vasodilataIon – Decompensated HF – Loading dose 12-‐24 ug/kg during 10 min, conInious infusion 0.05-‐0.2 ug/kg/min during 24 hours – Combined to low-‐dose milrinone – Side-‐effects hypotension, tachycardia

Anesthesic management
• Q = Blood flow
• P = Pressure withing chamber or vessel
• R = Vascular resistance of pulmonary or systemic vasculature
RPQ =

L -‐> R shunts (ASD,VSD,AVSD,PDA,A-‐P window)
• Increased pulmonary blood flow
– Increased RV workload
– Pulmonary congesIon
– Longstanding L-‐>R -‐> PHT
– PVR > SVR -‐> R-‐>L shunt -‐>Sdr Eisenmenger
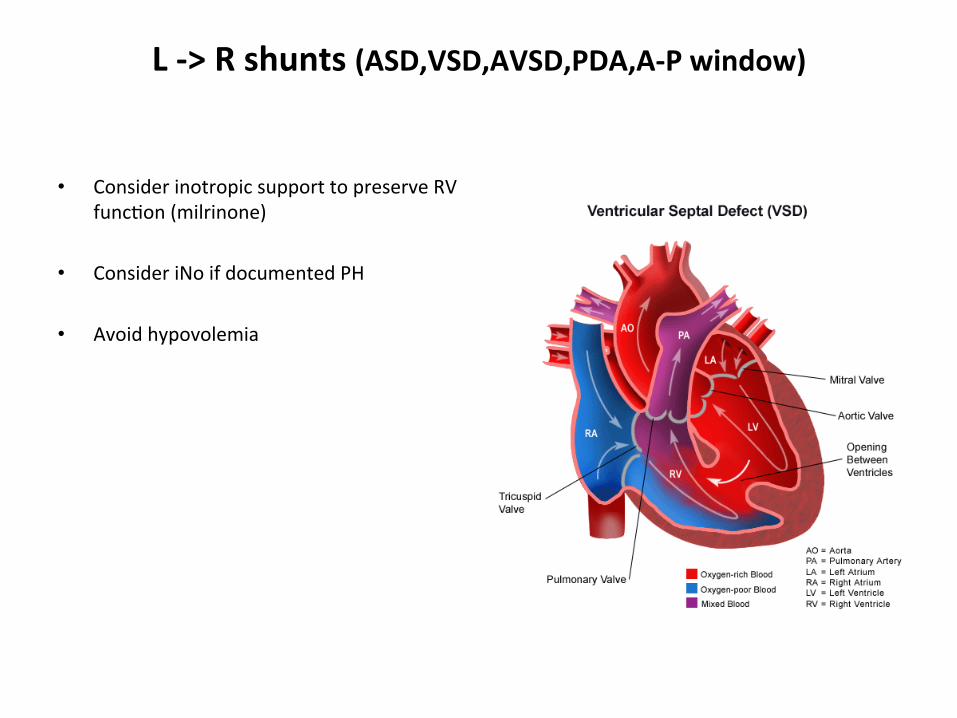
L -‐> R shunts (ASD,VSD,AVSD,PDA,A-‐P window)
• Consider inotropic support to preserve RV funcIon (milrinone)
• Consider iNo if documented PH
• Avoid hypovolemia
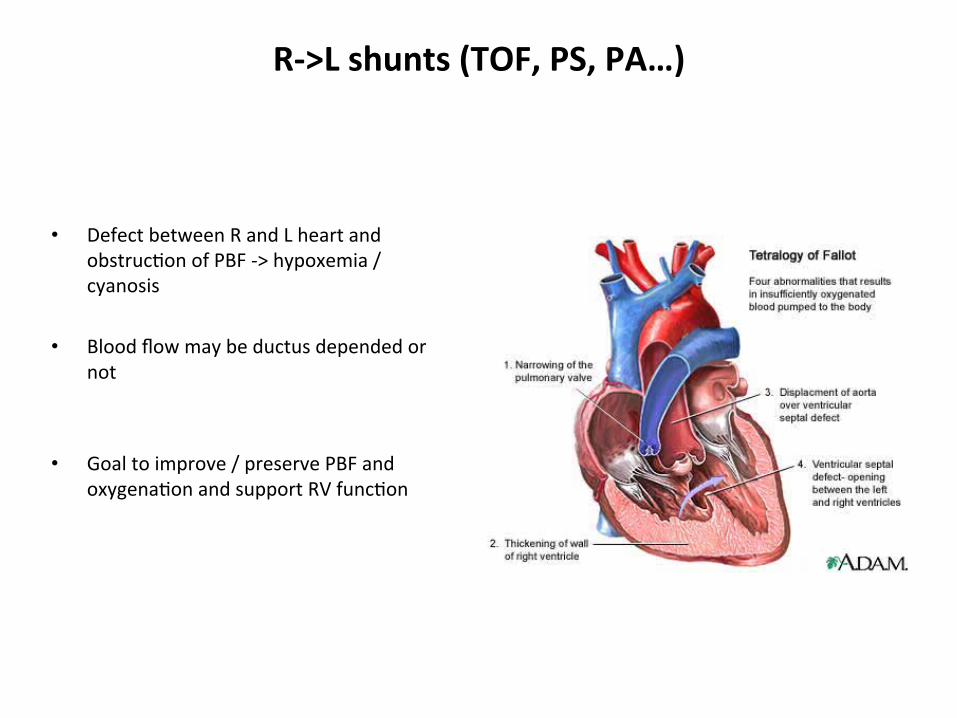
R-‐>L shunts (TOF, PS, PA…)
• Defect between R and L heart and obstrucIon of PBF -‐> hypoxemia / cyanosis
• Blood flow may be ductus depended or not
• Goal to improve / preserve PBF and oxygenaIon and support RV funcIon
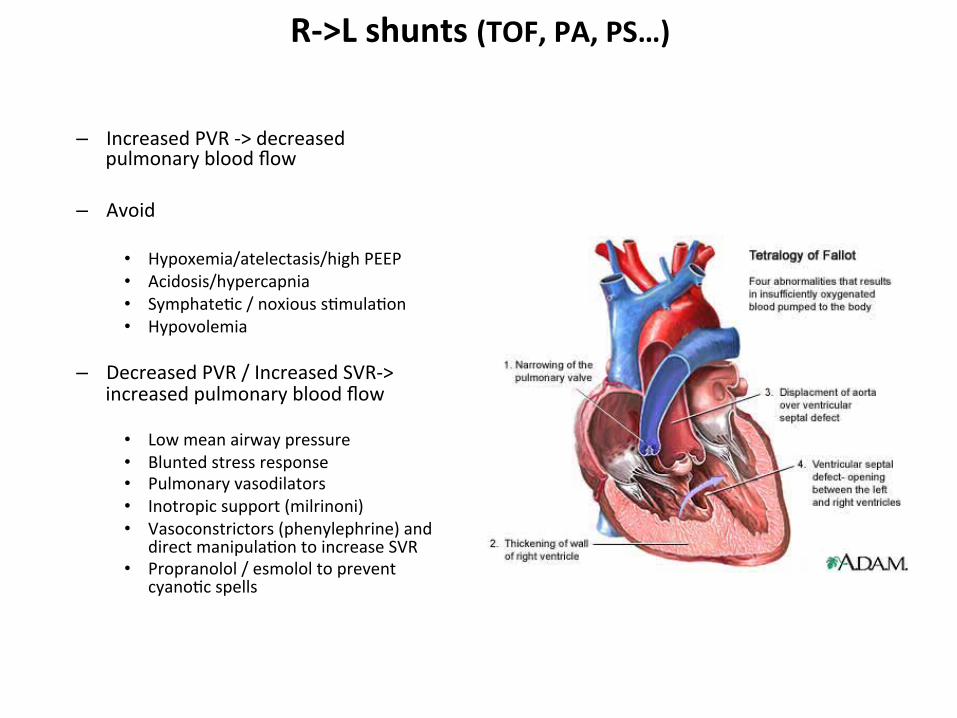
R-‐>L shunts (TOF, PA, PS…)
– Increased PVR -‐> decreased pulmonary blood flow
– Avoid
• Hypoxemia/atelectasis/high PEEP • Acidosis/hypercapnia • SymphateIc / noxious sImulaIon • Hypovolemia
– Decreased PVR / Increased SVR-‐> increased pulmonary blood flow • Low mean airway pressure • Blunted stress response • Pulmonary vasodilators • Inotropic support (milrinoni) • Vasoconstrictors (phenylephrine) and
direct manipulaIon to increase SVR • Propranolol / esmolol to prevent
cyanoIc spells

Complex shunts (UVH, TA, TGA, DORV…)
• Mixing of arterial and venous blood in common cardiac chambers
• Arterial blood saturaIon 75-‐85%
• Blood flow may be obstructed or not
• Blood flow can be ductus depended or not
• Both cyanosis and CHF

Complex shunts (UVH, TGA, TA…)
• Ductus depended flow-‐> conInue alprostadil
• Risk of both thrombosis and bleeding
• Increased PBF may steal blood from systemic circulaIon
• Don’t try to ”overoxygenate” – Doesn’t improve systemic oxygenaIon – Causes hypotension, coronary ischemia,
ventricular dysfuncIon
• Goal Qp / Qs = 1 – Qp / Qs = Sa02-‐Sv02/ 98-‐Sa02 – Sa02 75-‐85% – PaO2 and PaCO2 5,5-‐6 kPa
• Adjust Hb goal to preoperaIve value

Single ventricle paUent with a shunt
• AnIcoagulant therapy should be conIuned to avoid shunt trombosis
• During PPV the PBF during expiraIon – I : E = 1: 3 – 1:5 – Inspiratory Ime max 0,7 sec – Peep with cauIon – NormovenIlaIon and Qp : Qs =1 (0,7-‐1,5:1) – Don`t try to ”overoxygenate”
• Avoid hypovolemia, preserve low PVR, sr, consider inotropic support to maintain ventricular contracIlity (milrinone,levosimendan,epinephrine?)
• Consider increasing SVR to increase PBF
• Spontaneous breathing is preferable -‐> early ekstubaIon if possible

ObstrucUve lesions of systemic blood flow (AS, CoA)
• Icreased workload of LV
• Slow i.v. inducIon of anesthesia
• In severe obstrucIon avoid high doses of inhalaIon agents to prevent too low SVR and worse gradient?
• OpImize preload and volume status to get beger flow beyond lesion

Pulmonary arterial hypertension
• Systolic PAP > 50% of systemic systolic arterial blood pressure
• Pulmonary vascular remodelling, vasoconstricIon, RV hypertrophy, RA enlargement, TI, RV / biventricular heart failure
• PAH is significant risk factor for perioperaIve mortality

Pulmonary arterial hypertension
• PremedicaIon – Useful to avoid distres – Consider preoperaIve sildenafil
• Slow i.v. inducIon
• No single ideal anestheIc -‐> balanced anesthesia o[en preferred
• InfiltraIon of local anestheIc at the surgical site can offer benefit by reducing the need of opioids/sedaIve drugs
Pulmonary arterial hypertension
• Consider profylacIc inotropic support – Milrinone -‐> inotopic effect and pulmonary vasodilaIon – Levosimendan – Inhaled nitrix oxide
• SelecIve pulmonary vasodilaIon, radip onset, easy to use • Drug of choice to decrease PVR
• Control volume status to opImize preload and to avoid hypotension – Norepinephrine, phenylephrine, epinephrine if needed
• Be prepaired and have a plan to threat increasing PVR or PHT crisis

Pulmonary arterial hypertension
Robert et al Ped Anesth 2008

Discussion...

Koichi et al J Anesth 2011