and the related dementias multiple targets, multiple · pdf filesummary •the other or...
TRANSCRIPT

Jeffrey Kaye
Layton Professor of Neurology & Biomedical Engineering
ORCATECH - Oregon Center for Aging & Technology
NIA - Layton Aging & Alzheimer's Disease Center
"… and the Related Dementias" -Multiple Targets, Multiple Outcomes
September 26, 2017 – Bethesda, MD
2017 Annual Regulatory Science Workshop
Summary
• The ‘other’ or ‘related dementias’ are prevalent
• They have been recognized by typical, but not invariant signs and symptoms emergent at variable pace
• The pathologies associated with these dementias are heterogeneous
• A cornucopia of biomarkers (imaging, fluid, physiologic) identify pathologic states; their relevance to progression and functional change in different use cases is evolving
• Biometric or digital biomarkers may add to the ability to identify more precisely, objectively and rapidly, meaningful relevant change in at risk or cognitively impaired patients

Differential Diagnosis of Dementia
Dementia
More Rapidly Evolving
Dementias
VascularDementias
Dementia with
Lewy Bodies
FrontotemporalDementias
Alzheimer’s Disease
Me
mo
ry
Progressive cognitive decline affecting daily function
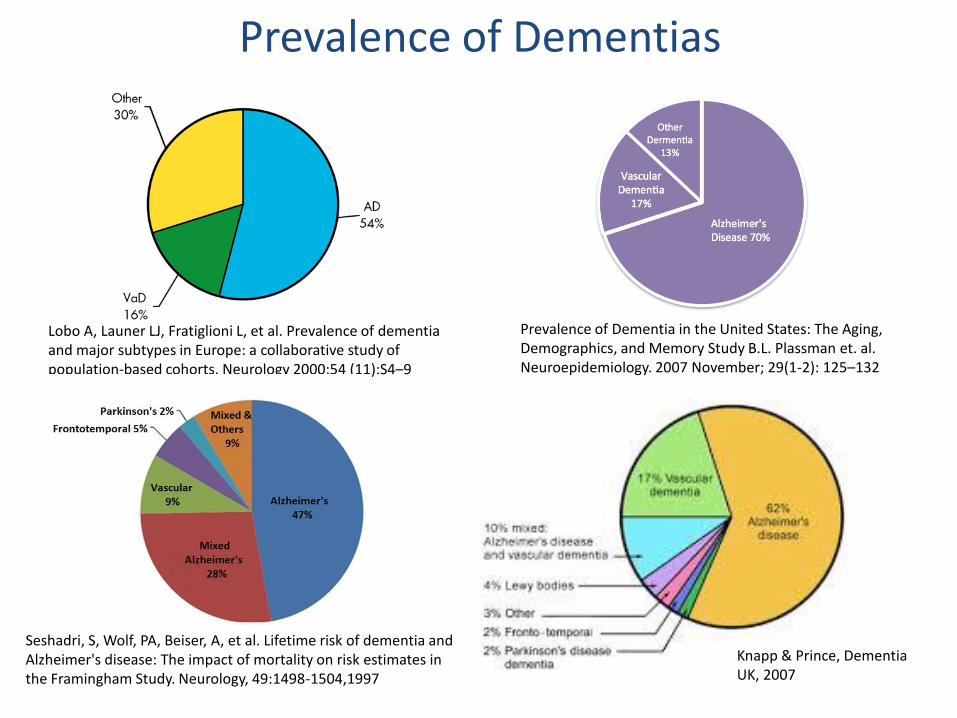
Prevalence of Dementias
Lobo A, Launer LJ, Fratiglioni L, et al. Prevalence of dementia and major subtypes in Europe: a collaborative study of population-based cohorts. Neurology 2000;54 (11):S4–9
Seshadri, S, Wolf, PA, Beiser, A, et al. Lifetime risk of dementia and Alzheimer's disease: The impact of mortality on risk estimates in the Framingham Study. Neurology, 49:1498-1504,1997
Knapp & Prince, Dementia UK, 2007
Prevalence of Dementia in the United States: The Aging, Demographics, and Memory Study B.L. Plassman et. al. Neuroepidemiology. 2007 November; 29(1-2): 125–132
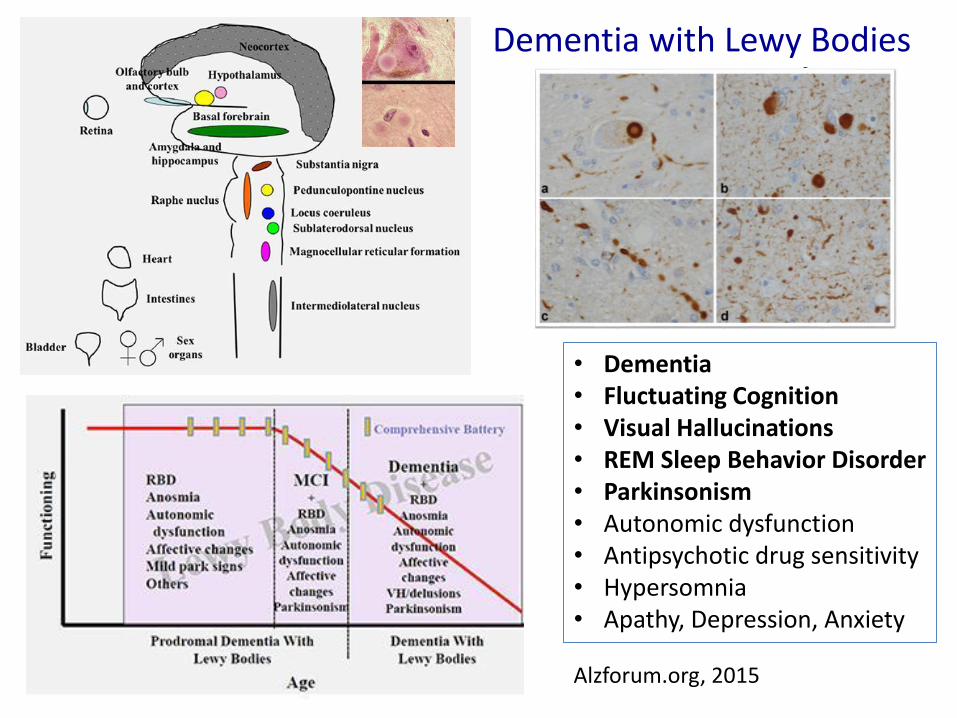
Dementia with Lewy Bodies
Alzforum.org, 2015
• Dementia• Fluctuating Cognition• Visual Hallucinations• REM Sleep Behavior Disorder• Parkinsonism• Autonomic dysfunction• Antipsychotic drug sensitivity• Hypersomnia• Apathy, Depression, Anxiety

McKeith, et al. Neurology, 2017, Diagnosis and management of dementia with Lewybodies. Fourth consensus report of the DLB Consortium
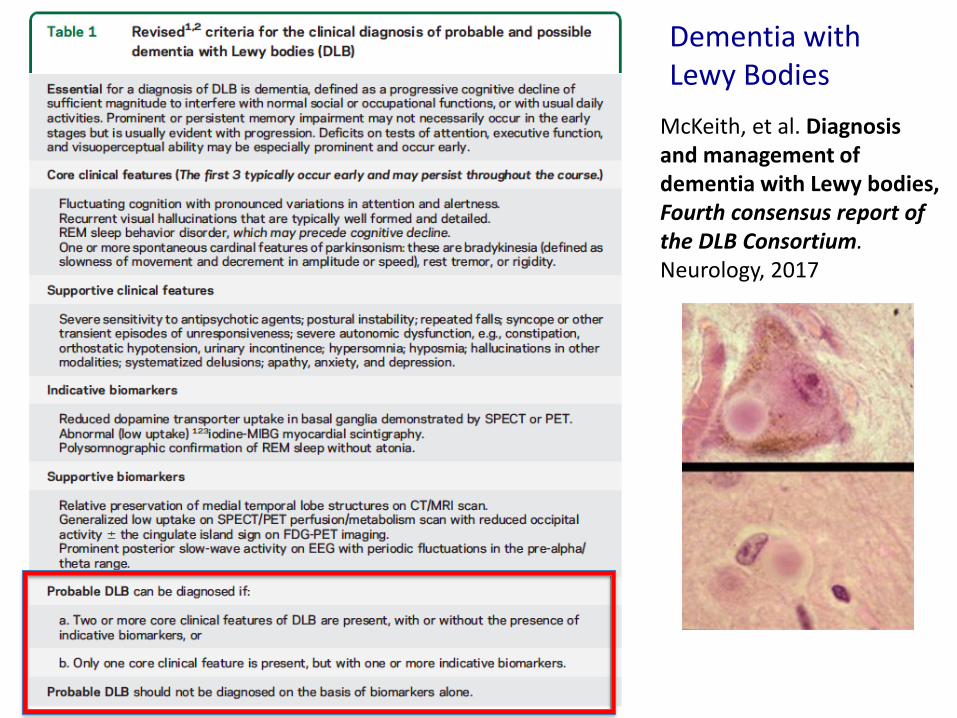
McKeith, et al. Diagnosis and management of dementia with Lewy bodies, Fourth consensus report of the DLB Consortium. Neurology, 2017
Dementia with Lewy Bodies
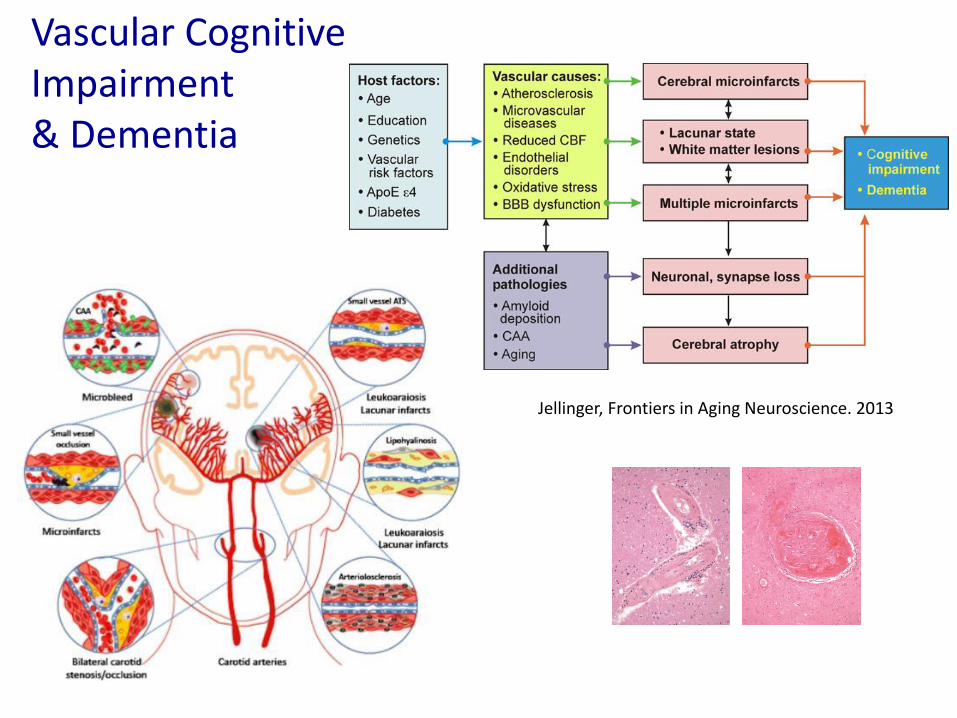
Vascular Cognitive Impairment & Dementia
Jellinger, Frontiers in Aging Neuroscience. 2013

Clinical Features of Vascular Dementia
CORTICAL SYNDROME• Medial frontal: executive dysfunction, abulia, apathy; akinetic mutism• Left parietal; aphasia, apraxia, agnosia• Right parietal: hemineglect (anosognosia, asomatognosia), confusion,
agitation, visuospatial, constructional difficulty• Medial temporal: anterograde amnesia
SUBCORTICAL SYNDROME• Focal motor signs• Early presence of gait disturbance, apraxic gait, parkinsonian gait• History of unsteadiness, falls• Urinary frequency, urgency,• Pseudobulbar palsy• Personality and mood changes (abulia, apathy, depression)• Cognitive disorder with relatively mild memory deficit, psychomotor
retardation, executive dysfunction

Vascular Dementia Criteria
1994 2013
DSM-5 Major Vascular Neurocognitive Disorder
PROBABLE IF Clinical features are consistent with vascular etiology:
• Onset related temporally to one or more cerebrovascular events
• Decline prominent in complex attention, processing speed, frontal-executive function
• Presence of cerebrovascular disease from history, exam, and/or neuroimaging accounting for deficits

O.A. Skrobot et al. / Alzheimer’s & Dementia 13 (2017) 624-633

Recent small subcortical
infarct
White matter hyper-
intensity LacunePerivascular
space
Cerebral microbleed
Modified from Wardlaw JM, Lancet Neurol. 2013
A B C D E F
MPRAGE T2* DTI FLAIR ASL rsfMRSilbert, Neuroimaging Core OHSU Aging & Alzheimer’s Center, 2017
Boespflug et al. Radiology, 2017
Imaging Markers of Vascular Disease or Damage

Westover et al., Estimating cerebral microinfarct burden from autopsy samples. Neurology, 2013
Based on in-depth examination (99 slides from 23 regions) of twobrains
The True Brain-Burden of Vascular Disease is Difficult to Estimate

Small vessel vascular disease & MCI prodrome
Carlson, et al., Neurology, 2008Silbert, et al., Neurology, 2012
Automated segmentation of WMH from FLAIR
Oregon Brain Aging Study
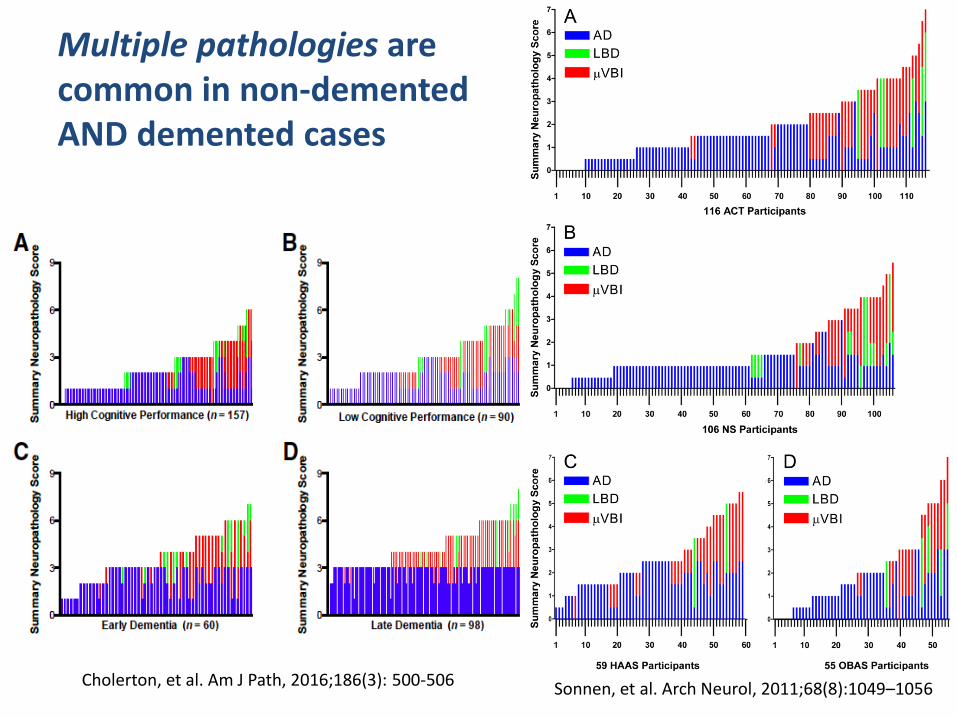
Multiple pathologies are common in non-demented AND demented cases
Cholerton, et al. Am J Path, 2016;186(3): 500-506 Sonnen, et al. Arch Neurol, 2011;68(8):1049–1056

RESIDUAL COGNITIVE DECLINE: 59%
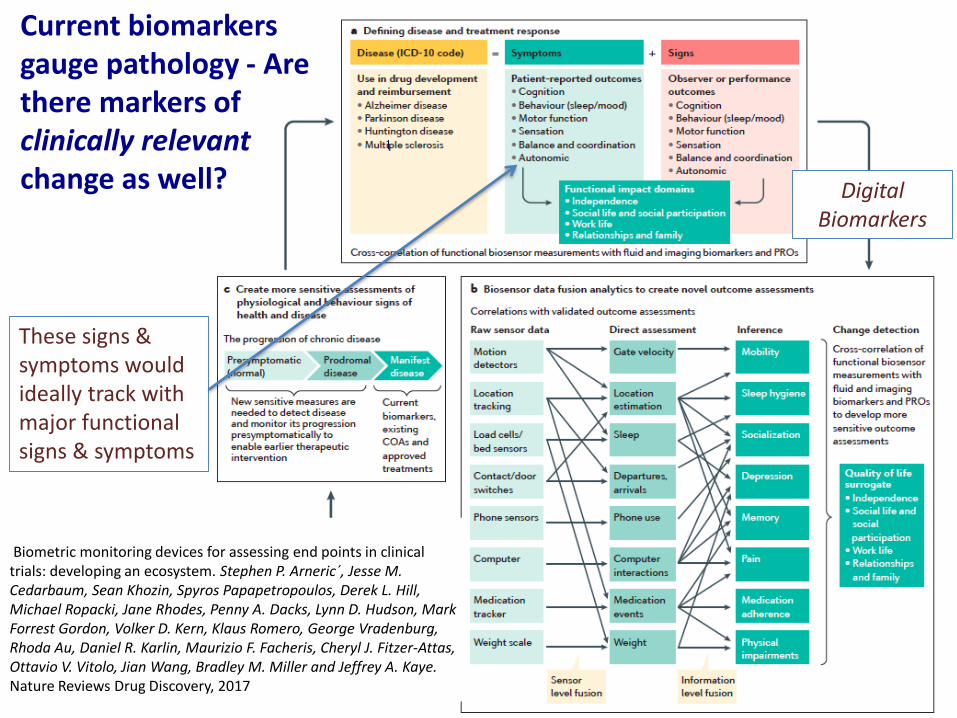
Current biomarkers gauge pathology - Are there markers of clinically relevant change as well?
Biometric monitoring devices for assessing end points in clinical trials: developing an ecosystem. Stephen P. Arneric´, Jesse M. Cedarbaum, Sean Khozin, Spyros Papapetropoulos, Derek L. Hill, Michael Ropacki, Jane Rhodes, Penny A. Dacks, Lynn D. Hudson, Mark Forrest Gordon, Volker D. Kern, Klaus Romero, George Vradenburg, Rhoda Au, Daniel R. Karlin, Maurizio F. Facheris, Cheryl J. Fitzer-Attas, Ottavio V. Vitolo, Jian Wang, Bradley M. Miller and Jeffrey A. Kaye. Nature Reviews Drug Discovery, 2017
These signs & symptoms would ideally track with major functional signs & symptoms
Digital Biomarkers

Buracchio et al. The Trajectory of Gait Speed Preceding Mild Cognitive Impairment Arch Neurol. 2010;67(8):980-986
Sabia, BMJ. 2017;; 357: j2709
Early MCI
Late MCI
Dodge et al. Trajectories of gait speed over time. Neurology, 2012
Physical Activity Walking
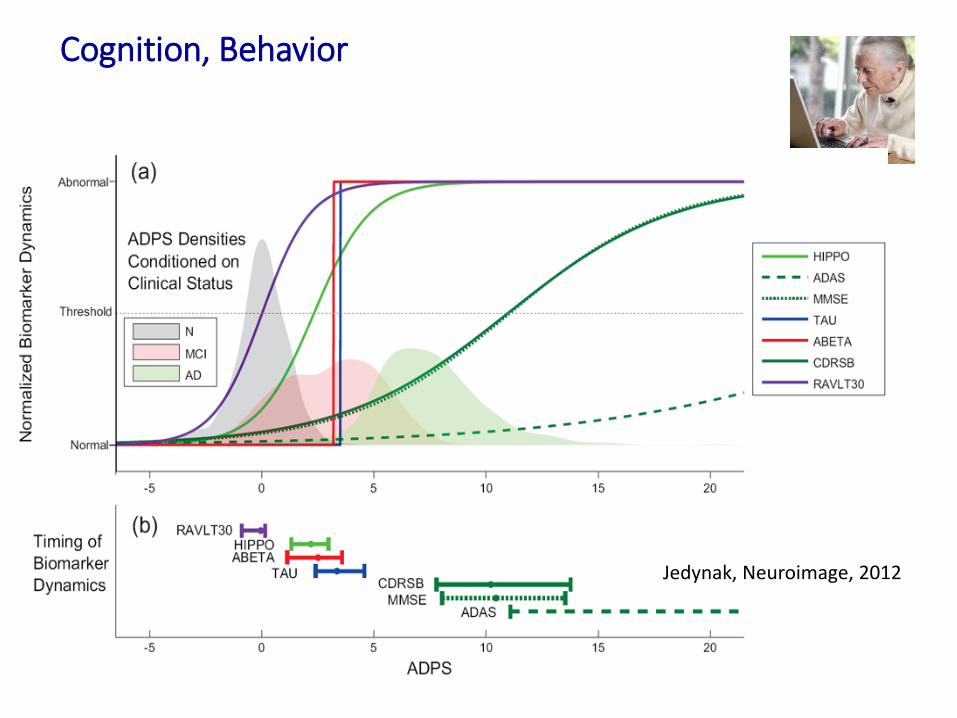
Cognition, Behavior
Jedynak, Neuroimage, 2012

Cognition, Behavior, (Motor Function)
Kaye, et al. Alzheimers Dement. 2014; Silbert et al., Alzheimers Dement, 2015; Seelye et al. Alzheimers Dement.: Diagnosis, Assessment & Disease Monitoring, 2015; Seelye et al. Alzheimer’s Disease & Assoc. Disorders, 2015
Frequent Behavior/M
ood Self-Report
30
20
10
14
16
18
20
0 4 8 12 16 20 24 28 32
Me
an
Days
on
Co
mp
ute
r
Months of Continuous Monitoring
Intact MCI
MM
SE
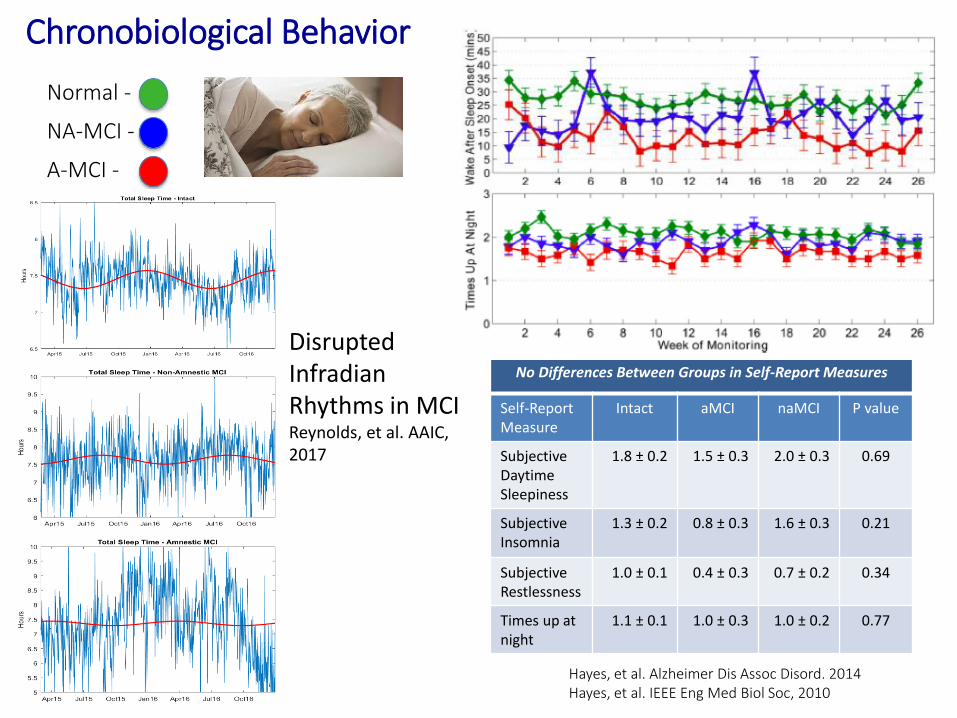
Chronobiological Behavior
Hayes, et al. Alzheimer Dis Assoc Disord. 2014Hayes, et al. IEEE Eng Med Biol Soc, 2010
No Differences Between Groups in Self-Report Measures
Self-Report Measure
Intact aMCI naMCI P value
Subjective DaytimeSleepiness
1.8 ± 0.2 1.5 ± 0.3 2.0 ± 0.3 0.69
SubjectiveInsomnia
1.3 ± 0.2 0.8 ± 0.3 1.6 ± 0.3 0.21
Subjective Restlessness
1.0 ± 0.1 0.4 ± 0.3 0.7 ± 0.2 0.34
Times up at night
1.1 ± 0.1 1.0 ± 0.3 1.0 ± 0.2 0.77
NA-MCI -
Normal -
A-MCI -
Disrupted InfradianRhythms in MCIReynolds, et al. AAIC, 2017
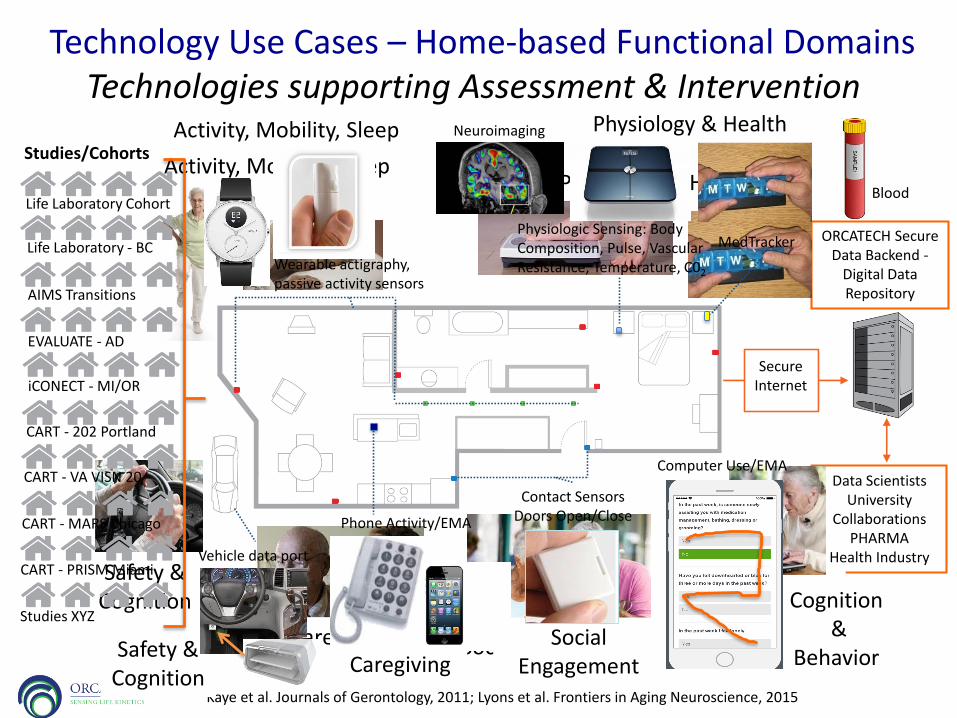
Activity, Mobility, Sleep
Kaye et al. Journals of Gerontology, 2011; Lyons et al. Frontiers in Aging Neuroscience, 2015
Technology Use Cases – Home-based Functional Domains
Secure Internet
Data Scientists University
CollaborationsPHARMA
Health Industry
ORCATECH Secure Data Backend -
Digital Data Repository
Safety & Cognition
Physiology & Health
Cognition&
BehaviorSocial EngagementCaregiving
Cognition&
Behavior
Computer Use/EMA
Safety & Cognition
Vehicle data port
iCONECT - MI/OR
CART - 202 Portland
CART - MARS Chicago
CART - PRISM Miami
CART - VA VISN 20
EVALUATE - AD
AIMS Transitions
Life Laboratory - BC
Life Laboratory Cohort
Studies/Cohorts
Studies XYZ
Wearable actigraphy, passive activity sensors
Activity, Mobility, Sleep
Social Engagement
Contact Sensors Doors Open/ClosePhone Activity/EMA
Caregiving
Technologies supporting Assessment & Intervention
Blood
Physiologic Sensing: Body Composition, Pulse, Vascular Resistance, Temperature, C02
MedTracker
Physiology & Health Neuroimaging

BiomarkerTarget
EnrichmentImaging, CSF, Plasma,
Genetics, other risk factors
Traditional Trial Enrichment:
Stratification accordingto increased risk of AD, LBD, VD...
Does not predict who/how progresses
Population
TargetPathologyGroup
6 months
High Efficiency Clinical Trials (Focus on Phase II)
BehavioralPhenotypeEnrichmentSleep hygiene,
Mobility, Computer Use, etc…
FurtherEnrichment:
Stratification accordingto who will progress.
Can predict who progresses
Disease Progression Group(s)
TargetPathology
Group
2-3 months
ContinuousAssessmentComputer use, Walking speed,
Activity, Mobility,etc…
Efficient LongitudinalAssessment:
Continuously assessed objective measures.
Detects individual relevantchange rapidly
Continuous Assessment:Clinical Progression
6 months
Precision Phenotyped
Thank You!
orcatech.org
“Something to make the world look sane again – Is there an app for that?”

Physical Activity & Mobility: Out of home assessment –Driving (and Cognition)
26
Table 2. Summary Driving Characteristics; (Per day; six month observation period)
Variable Total Intact MCI p-value
N 28 21 7
Mean # of (one-way) trips per day 4.2 (1.0) 4.1 (0.9) 4.7 (1.4) 0.19
Day-to-day variability in # of trips 2.1 (0.6) 2.1 (0.5) 2.3 (0.8) 0.49
Mean distance driven per day (miles) 20 (13) 22 (13) 14 (11) 0.06
Day-to-day variability in distance driven 26 (17) 31 (17) 13 (12) 0.01*
Mean time driven per day (hours) 0.9 (0.4) 0.9 (0.4) 0.8 (0.4) 0.26
Day-to-day variability in time driven 0.7 (0.3) 0.8 (0.3) 0.5 (0.2) <0.01**
Mean first clock starttime of driving per
day
11.1 (1.2) 11.3 (1.2) 10.6 (1.4) 0.43
Day-to-day variability in first starttime
(hrs)
2.8 (0.8) 2.8 (0.6) 2.7 (1.1) 0.78
Mean last clock starttime of driving per
day
15.4 (1.6) 15.2 (1.4) 15.9 (1.9) 0.33
Day-to-day variability in last starttime
(hrs)
3.2 (0.6) 3.2 (0.6) 3.2 (0.8) 0.79
Mean # of days monitored 206 (36) 208 (38) 201 (33) 0.70
% of days at least one trip was taken out
of all days monitored
52% 49% 60% 0.21
% of driving days with >=20 miles driven 26% 27% 21% 0.51
Mean time of highway driving per day
(seconds)
450 (506) 543 (533) 172 (288) 0.01*
Seelye et al. Journal of Alzheimer’s Disease, 2017
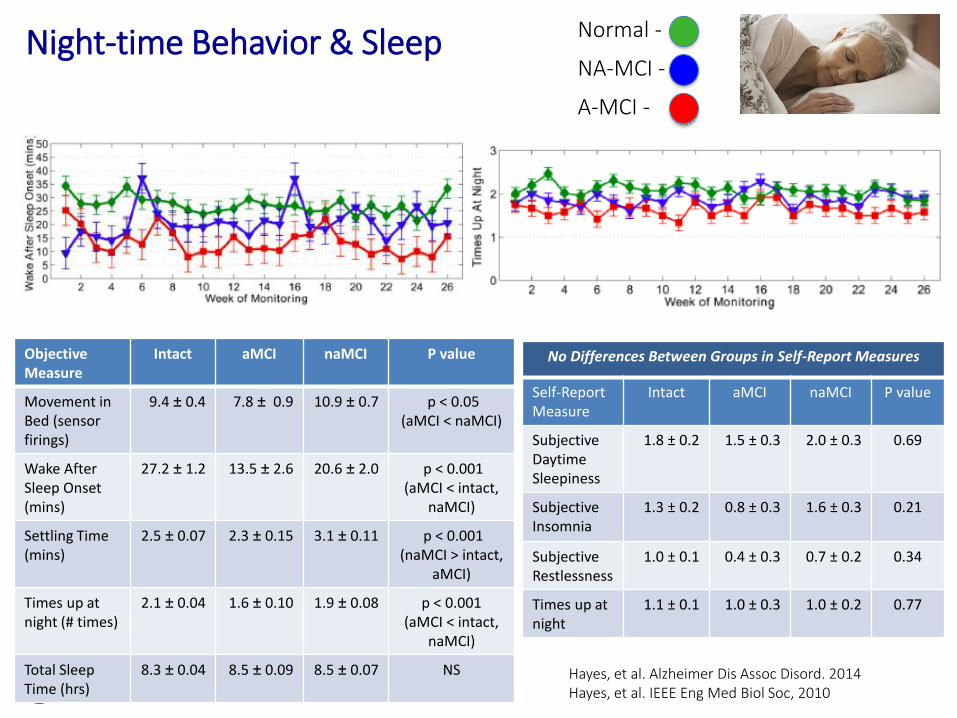
Night-time Behavior & Sleep
Hayes, et al. Alzheimer Dis Assoc Disord. 2014Hayes, et al. IEEE Eng Med Biol Soc, 2010
No Differences Between Groups in Self-Report Measures
Self-Report Measure
Intact aMCI naMCI P value
Subjective DaytimeSleepiness
1.8 ± 0.2 1.5 ± 0.3 2.0 ± 0.3 0.69
SubjectiveInsomnia
1.3 ± 0.2 0.8 ± 0.3 1.6 ± 0.3 0.21
Subjective Restlessness
1.0 ± 0.1 0.4 ± 0.3 0.7 ± 0.2 0.34
Times up at night
1.1 ± 0.1 1.0 ± 0.3 1.0 ± 0.2 0.77
ObjectiveMeasure
Intact aMCI naMCI P value
Movement in Bed (sensor firings)
9.4 ± 0.4 7.8 ± 0.9 10.9 ± 0.7 p < 0.05 (aMCI < naMCI)
Wake After Sleep Onset (mins)
27.2 ± 1.2 13.5 ± 2.6 20.6 ± 2.0 p < 0.001 (aMCI < intact,
naMCI)
Settling Time (mins)
2.5 ± 0.07 2.3 ± 0.15 3.1 ± 0.11 p < 0.001 (naMCI > intact,
aMCI)
Times up at night (# times)
2.1 ± 0.04 1.6 ± 0.10 1.9 ± 0.08 p < 0.001 (aMCI < intact,
naMCI)
Total Sleep Time (hrs)
8.3 ± 0.04 8.5 ± 0.09 8.5 ± 0.07 NS
NA-MCI -
Normal -
A-MCI -
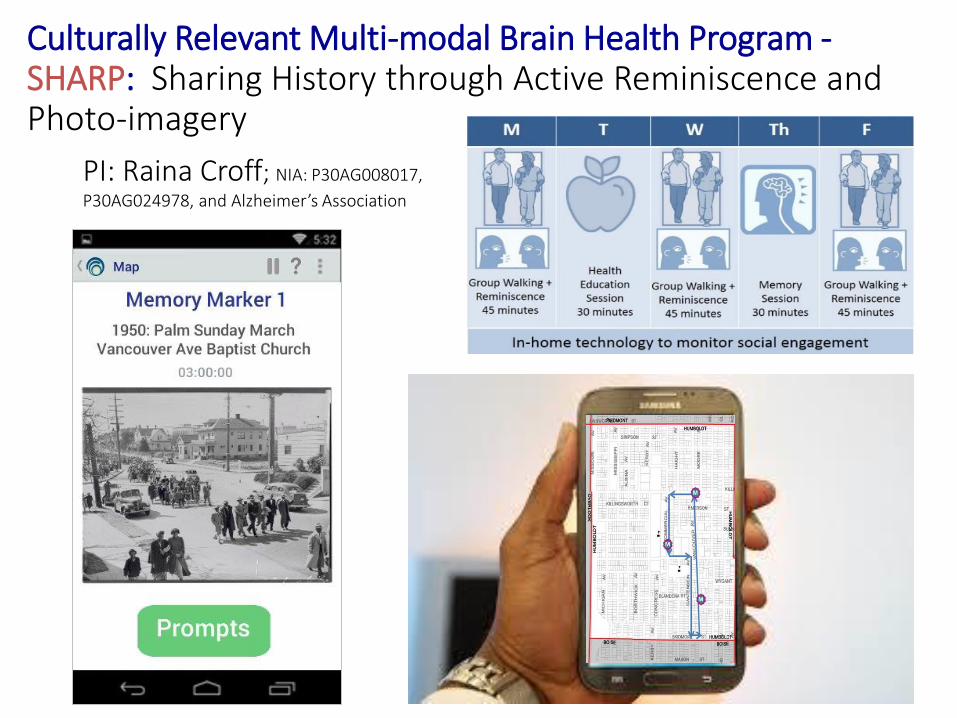
Culturally Relevant Multi-modal Brain Health Program -SHARP: Sharing History through Active Reminiscence and Photo-imagery
PI: Raina Croff; NIA: P30AG008017,
P30AG024978, and Alzheimer’s Association

“In focusing attention on the mortality associated with Alzheimer disease, our goal is not to find a way to prolong the life of severely demented persons, but rather to call attention to our belief that senile as well as pre-senile forms of Alzheimer are a single disease, a disease whose etiology must be determined, whose course must be aborted, and ultimately a disease to be prevented.Robert Katzman, Archives of Neurology, 1976
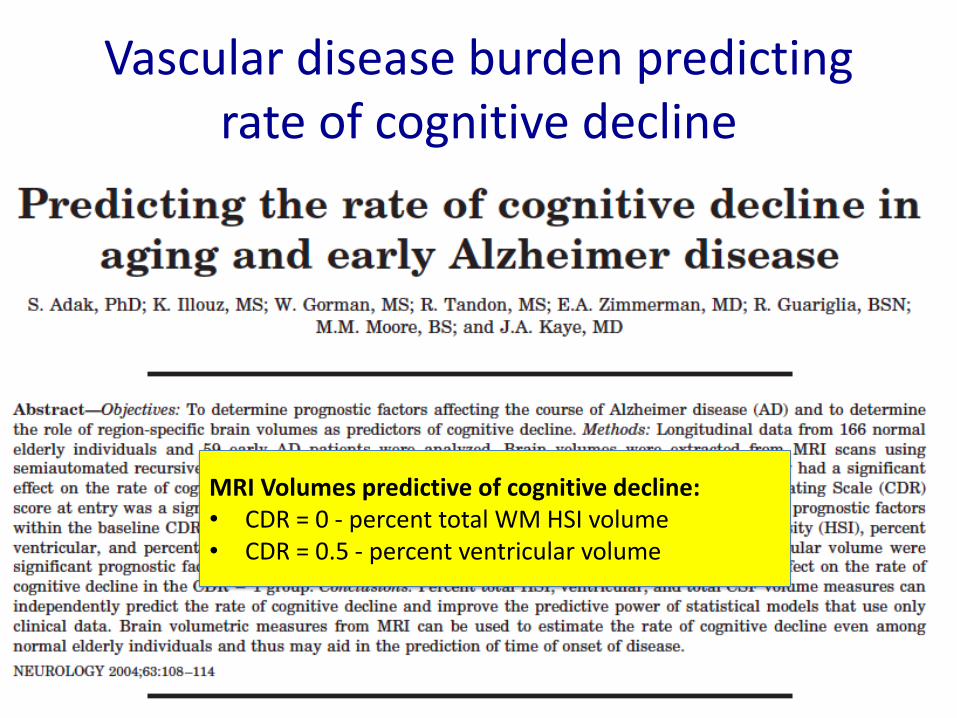
Vascular disease burden predicting rate of cognitive decline
MRI Volumes predictive of cognitive decline: • CDR = 0 - percent total WM HSI volume• CDR = 0.5 - percent ventricular volume

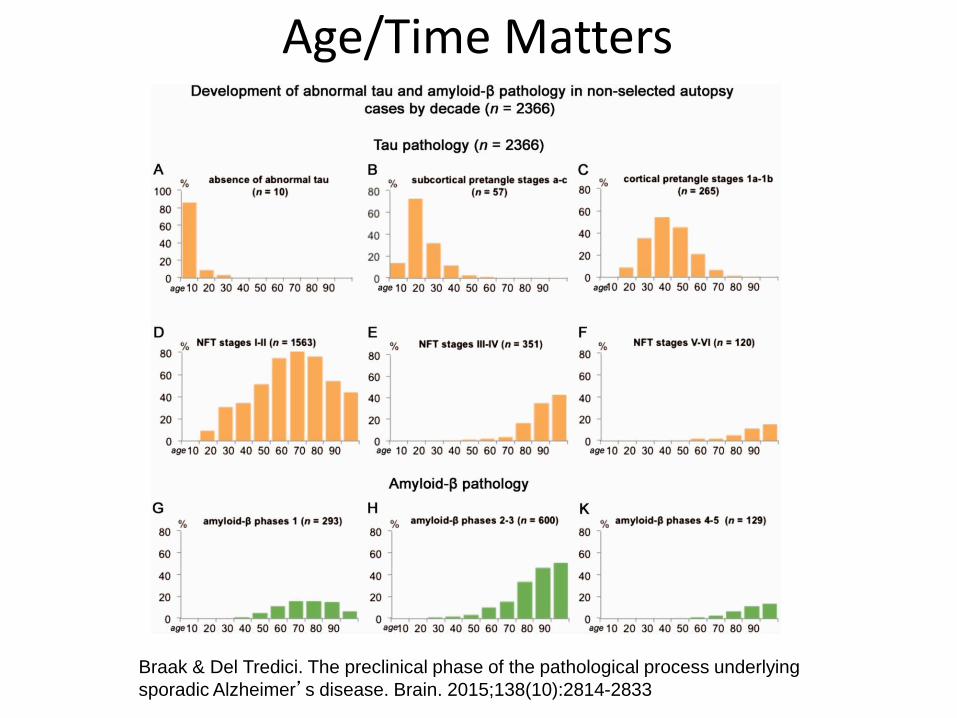
Age/Time Matters
Braak & Del Tredici. The preclinical phase of the pathological process underlying
sporadic Alzheimer’s disease. Brain. 2015;138(10):2814-2833