anaesthetic consideration for one lung ventilation
TRANSCRIPT

Anaesthetic concern for one lung ventilation
BY- DR.BHUSHAN KINGE,
M.D.
IMS – BHU , VARANASI

One Lung Ventilation (OLV) is a technique that
allows isolation of the individual lungs and each
lung functioning independently by preparation of
the airway under anaesthesia.
One Lung Ventilation first in 1931 by Gale and
Waters complex lung resection surgery. He used
a single-light tube that was inserted into the right or
left main bronchus.

Objectives
• Indication/contraindication of OLV
• Physiology changes of OLV
• Selection of the methods for OLV
• Management of common problems associated with OLV.
Introduction
• One-lung ventilation, OLV, means separation of the two lungs and each lung functioning independently by preparation of the airway
• OLV provides:– Protection of healthy lung from infected/bleeding one
– Diversion of ventilation from damaged airway or lung
– Improved exposure of surgical field
• OLV causes:– More manipulation of airway, more damage
– Significant physiologic change and easily development of hypoxemia

Absolute indication for OLV
– Isolation of one lung from the other to avoid spillage or contamination
• Infection
• Massive hemorrhage
– Control of the distribution of ventilation
• Bronchopleural / - cutaneous fistula
• Surgical opening of a major conducting airway
• giant unilateral lung cyst or bulla
• Tracheobronchial tree disruption
• Life-threatening hypoxemia due to unilateral lung disease
– Unilateral bronchopulmonary lavage

Relative indication – Surgical exposure ( high priority)
• Thoracic aortic aneurysm
• Pneumonectomy
• Upper lobectomy
• Mediastinal exposure
• Thoracoscopy
– Surgical exposure (low priority)• Middle and lower lobectomies and subsegmental resections
• Esophageal surgery
• Thoracic spine procedure
• Minimal invasive cardiac surgery .
– Postcardiopulmonary bypass status after removal of totally occluding chronic unilateral pulmonary emboli.
– Severe hypoxemia due to unilateral lung disease.

Two-lung ventilation and OLV

Lateral Decubitus Position
Patient remains in this position to facilitate Thoracic surgery.
The lower and upper lung in this position is termed dependent
and non-dependent respectively.
There is considerable V/Q mismatch as there is greater
ventilation but less perfusion to the non-dependent lung and
converse to the dependent lung.
The blood flow is determined by the gravity.

Lateral Decubitus Position
• The good ventilation of the upper lung is due to
open chest while the poor ventilation of the
lower lung is due to compression of the lung by
mediastinum, diaphragm and chest wall
compression.

Diagrammatic representation of the V/Q relationship in
patient with open chest in LDP

BLOOD FLOW DISTRIBUTION DURING OLV
The main physiological changes in OLV is the redistribution of lung
perfusion between the ventilated (dependent) and blocked
(nondependent) lung
The major determinants of blood flow distribution between both lungs
are: Gravity, Amount of lung disease, Magnitude of HPV, Surgical
interference (Nondependent Lung) Ventilatatory mode (dependent Lung)

During one-lung ventilation
Greater decrease in oxygenation than during two-lung
ventilation in LDP due to an obligatory Rt-Lt
transpulmonary shunt through the nonventilated
nondependent lung. Consequently, lower PaO2 & larger
P(A-a) O2 gradient.
Usually carbon dioxide elimination is not a problem;
retention of CO2 by blood traversing the nonventilated
lung slightly exceeds the increased elimination of CO2
from blood traversing the ventilated lung, and the PaCO2
will usually slowly increase and P(A-a) CO2 decreases .

Hypoxic pulmonary vasoconstriction
• HPV is a physiological response of the lung to alveolar
hypoxia, which redistributes pulmonary blood flow from
areas of low oxygen partial pressure to areas of high
oxygen availability.
• The mechanism of HPV is not completely understood.
Vasoactive substances released by hypoxia or hypoxia itself
(activating K+, Ca++ and TRP channels) cause pulmonary
artery smooth muscle contraction.

table summarizing the V/Q changes in LDP
Dependent Lung Non-dependent Lung
Ventilation Reduced Increased
Perfusion Increased Reduced
Pulmonary blood
flow80% 20%

HPV• HPV aids in keeping a normal V/Q relationship by
diversion of blood from underventilated areas, responsible for the most lung perfusion redistribution in OLV
• HPV is graded and limited, of greatest benefit when 30% to 70% of the lung is made hypoxic.
• HPV is effective only when there are normoxic areas of the lung available to receive the diverted blood flow

HPV
• HPV is inhibited directly by volatile anesthetics (less with N20), vasodilators (NTG, SNP, NO, dobutamine, ß2-agonist), increased PVR (MS, MI, PE) and hypocapnia.
• HPV is indirectly inhibited by PEEP; vasoconstrictor drugs (epinephrine, norepinephrine, phenylephrine, dopamine) constrict normoxic lung vessels preferentially.

Gravity and V-Q
• Upright LDP

Physiology of LDP
Awake/closed chest Anesthetized .
V Q V Q V Q
ND
D

Shunt and OLV
• Physiological (postpulmonary) shunt
• About 2-5% CO,
• Accounting for normal A-aD02, 10-15 mmHg
• Including drainages from – Thebesian veins of the heart
– The pulmonary bronchial veins
– Mediastinal and pleural veins
• Transpulmonary shunt increased due to continued perfusion of the atelectatic lung and A-aD02 may increase.

Cardiac output and OLV
• Decreased CO may reduce SvO2 and thus impair SpO2 in presence of significant shunt– Hypovolemia
– Compression of heart or great vessels
– Thoracic epidural sympathetic blockade
– Air trapping and high PEEP
• Increased CO increases PA pressures which increases perfusion of the non-ventilated lung → increase of shunt fraction

Methods of OLV
• Double-lumen endotracheal tube, DLT
• Single-lumen ET with a built-in bronchial blocker, Univent Tube
• Single-lumen ET with an isolated bronchial blocker
– Arndt (wire-guided) endobronchial blocker set
– Balloon-tipped luminal catheters
• Endobronchial intubation of a single-lumen ET

DLT
• Type:– Carlens, a left-sided + a carinal hook
– White, a right-sided Carlens tube
– Bryce-Smith, no hook but a slotted cuff/Rt
– Robertshaw, most widely used
• All have two lumina/cuffs, one terminating in the trachea and the other in the mainstembronchus
• Right-sided or left-sided available
• Robertshaw -Available size: 41,39, 37, 35, 28 French (ID=6.5, 6.0, 5.5, 5.0 and 4.5 mm respectively).

DIFFERENT TYPES OF DLT

Left DLT…• Most commonly used• The bronchial lumen is longer, and a simple round
opening and symmetric cuff.• Better margin of safety than Rt DLT• Easy to apply suction and/or CPAP to either lung• Easy to deflate lung• Lower bronchial cuff volumes and pressures• Can be used
– Left lung isolation: clamp bronchial + ventilate/ tracheal lumen– Right lung isolation: clamp tracheal + ventilate/bronchial lumen

DLT• More difficult to insert (size and curve, cuff)
• Risk of tube change and airway damage if kept in position for post-op ventilation
• Contraindication:– Presence of lesion along DLT pathway
– Difficult/impossible conventional direct vision intubation
– Critically ill patients with single lumen tube in situ who cannot tolerate even a short period of off mechanical ventilation
– Full stomach or high risk of aspiration
– Patients, too small (<25-35kg) or too young (< 8 yrs)

TO ENSURE CORRECT POSITION OF DLT CLINICALLY
Breath sounds are Normal (not diminished) & follow the expected
unilateral pattern with unilateral clamping
The chest rises and falls in accordance with the breath sounds
The ventilated lung feels reasonably compliant
No leaks are present
Respiratory gas moisture appears and disappears with each tidal
ventilation

Complications of DLT
Impediment to arterial oxygenation
Tracheobronchial tree disruption, due to
-excessive volume and pressure in bronchial balloon
-inappropriate tube size
-malpositioning
Traumatic laryngitis (hook)
Inadvertent suturing of the DLT

Relative Contraindications to Use of DLT
Full stomach (risk of aspiration);
Lesions (stricture, tumor) along the pathway of DLT (may be traumatized);
Small patients;
Anticipated difficult intubation;
Extremely critically ill patients who have a single-lumen tube already in placeand who will not tolerate being taken off mechanical ventilation and PEEPeven for a short time;
Patients having some combination of these problems.
Under these circumstances, it is still possible to separate the
lungs by :
- Using a single-lumen tube + FOB placement of a bronchial blocker; or
- FOB placement of a single-lumen tube in a main stem bronchus.

Univent Tube• Developed by Dr. Inoue
• Movable blocker shaft in external lumen of a single-lumen ET tube
• Easier to insert and properly position than DLT (diff airway, C-s injury, pedi or critical pts)
• No need to change the tube for postop ventilation
• Selective blockade of some lobes of the lung .
• Suction and delivery CPAP to the blocked lung.
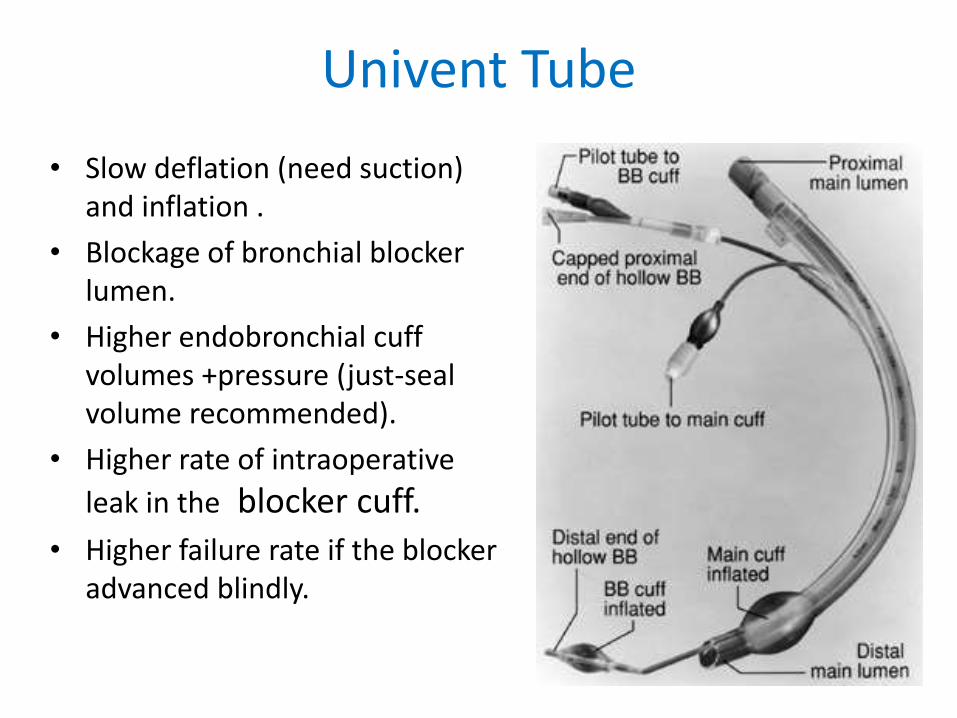
Univent Tube
• Slow deflation (need suction) and inflation .
• Blockage of bronchial blocker lumen.
• Higher endobronchial cuff volumes +pressure (just-seal volume recommended).
• Higher rate of intraoperative
leak in the blocker cuff.
• Higher failure rate if the blocker advanced blindly.

Univent Tube

Arndt Endobronchial Blocker set• Invented by Dr. Arndt, an anesthesiologist
• better for difficult intubation, pre-existing ETT and postop ventilation needed
• Requires ETT > or = 8.0 mm
• Similar problems as Univent
• Inability to suction or ventilate the blocked lung

Arndt endobronchial blocker[Wire guided Endobronchial Blocker (WEB)]

Cohen Flexitip Endobronchial Blocker

Other methods of OLV• Single-lumen ETT with a balloon-tipped catheter
– Including Fogarty embolectomy catheter, Foley, and Swan-Ganz catheter (children < 10 kg)
– Not reliable and may be more time-consuming
– Inability to suction or ventilate the blocked lung
• Endobronchial intubation of single-lumen ETT
– The easiest and quickest way of separating one lung from the other bleeding one, esp. from left lung
– More often used for paediatric patients
– More likely to cause serious hypoxemia or severe bronchial damage

Broncho-Cath CPAP system

Preoperative assessment
• Assess ability to withstand OLV & possible lung resection.
• In lung surgery, assess each patient as if for lung resection.
• Possibility of extensive surgical manipulation, significant blood loss, postoperative impaired function of remaining lung, asssociated pnuemonia, atelectasis.

Preoperative Measures
Patient should be in optimal condition for surgery
Cessation of smoking
Bronchial dilatation: Beta-2 agonists, Theophylline, Steroids
Loosening the secretions: Airway hydration, Systemic hydration, Mucolytic and expectorant drugs
Removal of Secretions: Postural drainage, Coughing, Chest physiotherapy
Increase Patient Participation: Psychological preparation, Educate and motivate for secretion removal measures and exercise (Incentive spirometry)

Poor candidate for OLV
• Limited exercise tolerence
• Cardiac pathology(moderate MS, MR)
• Breathlessness at rest
• Moderate to severe pulmonary hypertension
• Cor pulmonale

Indicator of High risk for perioperativecomplications on spirometry
• FEV1 < 50% predicted value or less than 2 litres.
• FVC < 50% predicted value .
• MBC <50% predicted value .
• RV/TLC <50% predicted value .

ABG ANALYSIS
Preoperative PaO2 < 60 mm Hg.
Preoperative paCO2 > 50 mm Hg.
these conditions are more likely to have perioperative hypoxia and hypercapnea during
OLV.

Assessment of indidual lung functions
• For pt. with boarderline respiratory function.
• Perfusion/ventilation of indidual lung is assessed by radioisotope Xe 133, Tc99 scan.
• Predicted postoperative FEV1 < 40% OR < 0.850 LITRE is associated with more risk of respiratory failure.

Risk for postoperative ventilation
• PATIENT FACTORS –
• Current smoker
• ASA STATUS> 2
• Age more than 70 yrs in COPD pts.
• COPD with exercise intolerence

Risk for postoperative ventilation
• Surgery dependant factors –
• Duration more than 4 hrs
• Emergency procedure
• Reexploration.

Risk for postoperative ventilation
• Nunn milledge crieteria-
FEV1 < 1litre, low paO2, normal paCO2- may need prolonged oxygen supplymentation.
FEV1 < 1 Litre, low paO2, high paCO2- may need postoperative ventilation.

Risk for postoperative ventilation
• Based on spirometry-
• Predicted FEV1 < 50 % or < 2 litres
• Predicted FVC < 50 %
• Predicted MVV < 50 % OR < 50 litre/ min
• Predicted DLCO2 < 50 % predicted
• Predicted RV/TLC > 50 %

technique of choice
• GA with controlled ventilation is method of choice.
• GA with thoracic epidural analgesia, intercostalblock, paravertebral block.
• Aim is to –
suppress airway reflexes, irritability,
Decrease inhibition of HPV,
maintain the cardiovascular status.
Maintain both lung ventilation as far as possible.

Management of OLV
– Maintain two-lung ventilation as long as possible.
– Prior switching to OLV give 100 % oxygen.
– Start OLV with 100% O2 then start backing off the FiO2 if
saturations are OK
– Manual ventilation for the first few minutes of OLV to get a
sense of pulmonary compliance / resistance
– Be attentive to inspiratory pressures and tidal volumes and
adjust the ventilator to optimize oxygenation and alveolar
ventilation, with minimal barotrauma
– Look at the surgical field to see if the non-dependent lung
is collapsed

Management of OLV
– Tidal volume = 8-10 ml/kg
– Adjust RR (increasing 20-30%) to keep PaCO2 = 40 mmHg approx.
– No PEEP (or very low PEEP, < 5 cm H2O)
– Continuous monitoring of oxygenation and ventilation (SpO2, ABG and ET CO2) .

hypoxemia in OLV
– Mechanical failure of O2 supply or airway blockade.
– Hypoventilation.
– Resorption of residual O2 from the clamped lung.
– Factors that decrease SvO2 (CO, O2
consumption).

Management of hypoxemia during OLV
– FiO2 = 1.0
– Manual ventilation
– Check DLT position with FOB
– Check hemodynamic status
– CPAP (5-10 cm H2O, 5 L/min) to nondependent lung.
– PEEP (5-10 cm H2O) to dependent lung .
– Intermittent two-lung ventilation.
– Temporary Clamp pulmonary artery of non-ventilated lung .

Management of hypoxemia during OLV
Pulmonary edema in non ventiated lung-
• Intraoperative collapse .
• handling of lung tissue.
• Imaired capillary function in postoperatveperiod.
• Needs Judicious use of perioperative fluid and vasopressor.

Management of hypoxemia during OLV
• Ability to maintain OLV in lateral decubitusshould be checked prior to start of surgery for feaesibilit
• airway pressure is to be monitored closely.
• Intermittent inflation of collapsed lung may be necessary sometimes.

OLV postoperative complications
• Oedema of operative site
• Collapse
• Consolidation.
• Retention of sputum.
• Inadequate pain relief limiting adequate chest expansion
May need diuretics , high peep, higher fiO2, inotropic support.

OLV postoperative complications
• Arrhythmia,
• RVF,
• cardiac herniation,
• cardiovascular hemorrhage.

Postoperative period
• Before resuming both lung ventilation do suction and fully inflate lungs.
• Postopearative x-ray is advised to rules out pneumo, hemothorax, collapse, misplaced drains.
• Adequate pain relief, ability to cough, moisturisedair/ oxygen therapy, breathing exercises , physiotherapy are essentially appropriate to prevent complications.
• judicious fluid therapy - Positive fluid balance is kept below 20 ml/kg.

Thank you..