anaesthesia for liver transplantation
TRANSCRIPT

Liver Transplantation
Speaker: Dr S. N Bhagirath
Moderated by Dr Jayanth

History
• First human liver transplantation – 1963
• Attempted by Thomas Starzl
• First recipient was a three year old – unsuccessful
• First Successful transplant was in 1967

Team Work
PERSONNEL INVOLVED
SURGEONS
NEPHROLOGISTS
PAEDIATRICIAN
RADIOLOGIST
PATHOLOGIST
PHYSICIAN
TRANSPLANT CO-ORDINATOR
NURSES
BLOOD BANK PERSONNEL
ANAESTHESIOLOGISTS
SPECIALISTS IN INFECTIOUS DISEASE
HEPATOLOGISTS & INTENSIVISTS

Indications
73%
21%
4%
2%
Decompensated Cirrhosis
Malignancy
Acute Liver FailureMetabolic Disease

Pathophysiology
Chronic Parenchymal Inflammation & Necrosis
Fibrosis
Disruption of hepatic architectureIncreased resistance to blood flow
Portal HTN
Formation of vascular shunts between portal & systemic shunts
10 – 12 mm of Hg of pressure gradient between portal & hepatic veins
Complications
Ascites, Esophageal Varices, Encephalopathy, Hepatorenal Syndrome

Complications - Cardiovascular
Portal HTN
Vasodilators
• Natriuretic Peptides
• VIP• Endotoxin• Glucagon• Nitric Oxide
Circulating volume sequestered into splanchnic circulation
• Low SVR/ Low Arterial Blood Pressure
• Hyperdynamic Circulation – High CO
• Blunted response to Sympathetic stimulation
Cirrhotic Cardiomyopathy

Complications - Cardiovascular
Cirrhotic Cardiomyopathy
• Systolic dysfunction – inability to increase CO
• Diastolic dysfunction – Vulnerability to Heart failure
• Resistance to β-adrenergic stimulation
• Electro physiologic abnormalities
• Autonomic dysfunction
Chronotropic/ Hemodynamic incompetence
Prolonged QTc interval
• Increased risk of CAD

Complications - Pulmonary
Two Entities
Hepatopulmonary Syndrome Porto-Pulmonary Syndrome
• Fluid retention
• Pleural Effusion
• Decreased lung capacity sec to large volume ascites
• α – 1 Antitrypsin deficiency
Broad Etiology

Complications – Pulmonary – Hepatopulmonary Syndrome
Diagnostic Criteria
• Portal HTN• PaO2 < 80 mm of Hg on room air
orAlveolar – Arterial O2 gradient > 15 mm of Hg
• Evidence of Intrapulmonary Vascular Dilatation (IPVD)
More about IPVD • Normally, Micro bubbles/ Albumin injected into venous
circulation get trapped in pulm. capillary bed
• But with IPVD, these are no longer trapped
• They re-appear in left atrium (2D Echo)
• Suggestive of increase in pulm. capillary diameter from
between 8 – 15 μm to 50 – 500 μm
• This compromises O2 diffusion causing hypoxia

Complications – Pulmonary – Porto-pulmonary Syndrome
Definition • Pulm. HTN in presence of Portal HTN
Diagnostic Criteria
• Clinical evidence of Portal HTN• Mean Pulm. artery pressure of 25 mm of Hg. at rest or 30
mm of Hg. during exercise• Mean Pulm. artery occlusion pressure < 15 mm of Hg• PVR > 240 Dyn Sq. Cm2 or 3 Wood units.
Implication • Poor prognosis for liver transplantation (without treatment)
• Post – treatment P.A. pressure < 35 mm of Hg.&PVR < 400 Dyn Sq. Cm2
Favourable candidates for
Liver transplantation

Complications – Renal – Hepatorenal Syndrome
Definition • Pre-renal abnormality due to circulatory derangements
Etiology • NO & other vasodilators which divert circulation thus compromising renal perfusion.
Type I HRS Type II HRS
• Rapidly progressive Renal Failure• Doubling of Creatinine over 2 weeks• Precipitating causes: Sepsis, Peritonitis, Surgical Stress• Median survival – 2 – 4 weeks.
• Median survival – 6 months
Treatment 1. Arginine – Vasopressin2. Nor-Epinephrine, Somatostatin3. Midodrine4. Volume expansion5. TIPS 6. Definitive treatment – Liver Transplantation.
Focus not on renal vasodilation but on
splanchnic vasoconstriction

Complications – Hepatic Encephalopathy
Definition • Serious, reversible neuro-psychiatric complication
Etiology• Hyperammonemia• Gut – derived neurotoxins• γ – Amino butyric Acid• Oxidative stress, Inflammatory mediators• Hyponatremia• Abnormal Serotonin/ Histamine Neurotransmitters
Treatment1. Non-absorbable Disaccharide - Lactulose2. Non-absorbable Antibiotics – Neomycin, Metronidazole,
Rifaximin.3. Floral washout reduces production of Ammonia.
Etiology • Uremia – Sepsis• Glucose & Electrolyte abnormalities• Endocrinopathies• Infections• Vascular lesions

Complications – Ascites
Etiology • Cirrhosis• Malignancy• Cardiac Failure• Renal disease• Pancreatitis• Tuberculosis
Eventuality May progress to Spontaneous Bacterial Peritonitis
Management• Serial Paracentesis• Liver Transplantation• TIPS placement• Peritoneovenous shunt• Never rapidly correct Hyponatremia–Central Pontine Myelinosis

Complications – Varices
Definition • Dilatation of Porto – Systemic shunts sec to Portal HTN
Diagnosis• Wedge Hepatic Venous Pressure (WHVP) > 10 – 12 mm of Hg.• Gold standard – Esophago-gastro duodenoscopy
Acute Variceal Bleeding
1. Intravascular volume resuscitation2. Correction of severe coagulopathy3. Pharmacologic manipulation of portal
pressure (eg. Vasopressin & Somatostatin)
4. Endoscopic variceal ligation5. Elective Intubation6. Balloon Tamponade
Treatment • Non selective β - Blockers (β1 reduces Cardiac Output & β2 causes Splanchnic Vasoconstriction)
• Endoscopic Ligation• TIPS
Buy time until Liver
Transplantation.!
Complications - Hemostasis
• Imbalance between Pro and Anticoagulant factors
• Thrombocytopenia (Splenic sequestration)
• Altered Fibrinolysis (TEG)
• DIC

Why are all these important..?
Liver Transplant Recipient
AUTONOMIC DYSFUNTION HEPATORENAL
SYNDROME
HEPATIC ENCEPHALOPATHY
ASCITES
VARICES
ACUTE VARICEAL BLEEDING
COGULATION ABNORMALITIES
PRE-EXISTENT CO-MORBIDITY
HEPATOPULMONARY SYNDROME
PORTOPULMONARY HYPERTENSION
BUNTED RESPONSE TO SYMPATHETIC STIMULATION
CIRRHOTIC CARDIOMYOPATHY
For Pre-operative preparation
Alert the Blood Bank
Neurologist consultation
Nephrologist consultationCardiologist
consultation, Inotropic
Support, etc.
Pulmonologist consultation
Oral immunosuppresants
/ bowel decontamination
antibiotics

Preoperative considerations
1. Complete Blood Work Up
• Hb, Platelets, WBCs, INR, Coagulation profile with Fibrinogen and PTT, ABG
• Electrolytes – Na+, K+, Cl-, Mg2+ Ca2+, Phosphate
2. Liver Function Tests
• Albumin (drug binding and oncotic pressure)
3. Renal Function Tests
• Urea and Creatinine
5. Baseline Cytomegalovirus and Epstein Barr Virus status.
6. Blood cultures
7. Chest X Ray
• Fluid overload, Infection
5. 2D Echo (Pulm. HTN/ Hepatopulmonary Syndrome)
6. Complexity of previous surgery (e.g.: Kasai’s Procedures)

Preoperative considerations
1. Specific Medication
• Immunosuppressants: Tacrolimus 0.2 mg/kg, Cyclosporine 5 mg/kg
• Mycostatin: 2 – 5 ml
• Depending on Coagulation status: transfuse 1 FFP.
2. Premedication
• Anxiolysis (especially in children): 0.25 – 0.5 mg/kg
• Supplemental O2 (in presence of HPS)
3. Counseling
• Psychological counseling to dispel fears and answer any lingering doubts.

Intraoperative considerations - Preliminaries
1. Rapid Sequence Induction
2. Arterial Blood Pressure monitoring
3. CVP
4. PA Cath (?)
5. TEE
6. Rapid Infusion Systems
7. Volatile Anaesthetic – 0.5 to 1.0 MAC (preferably Isoflurane as it
preserves Splanchnic Circulation)
8. Opioid (Fentanyl)
9. Muscle Relaxant (Cis-atracurium)

Intraoperative considerations – Stages of surgery
1. Preanhepatic stage
Surgical Incision Vascular exclusion of native liver
2. Anhepatic stage
Vascular occlusion Graft Reperfusion
(inflow to liver obstructed)
3. Neohepatic stage
Post reperfusion via portal vein
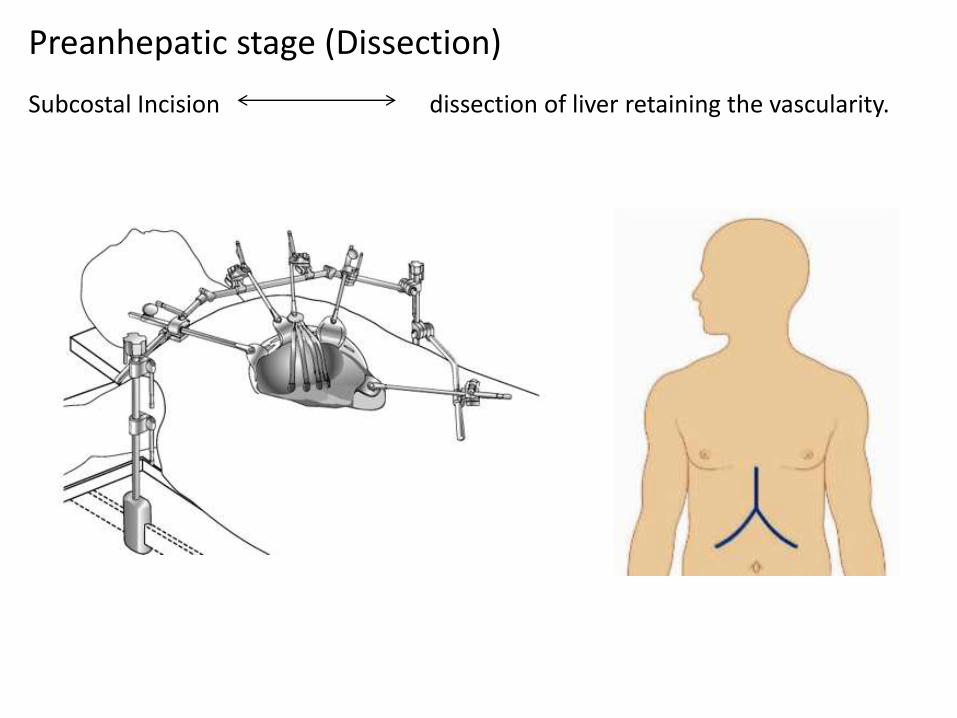
Preanhepatic stage (Dissection)
Subcostal Incision dissection of liver retaining the vascularity.

1. Trial clamping of infrahepatic IVC for 30 – 60 seconds
2. Anesthesiologist should judge CVS effects, adequacy of blood replacement and
patients ability to withstand drop in preload.
3. If SBP falls by 70% of pre-existent values, then bypass support may be needed.
Trial Clamping
Preanhepatic stage (Dissection Phase) Considerations
1. Blood loss, Manipulation of liver hilum and direct compression of IVC.
2. Adequate volume resuscitation (blood & colloid) is required.
3. Calcium chloride is preferred over Calcium Gluconate.
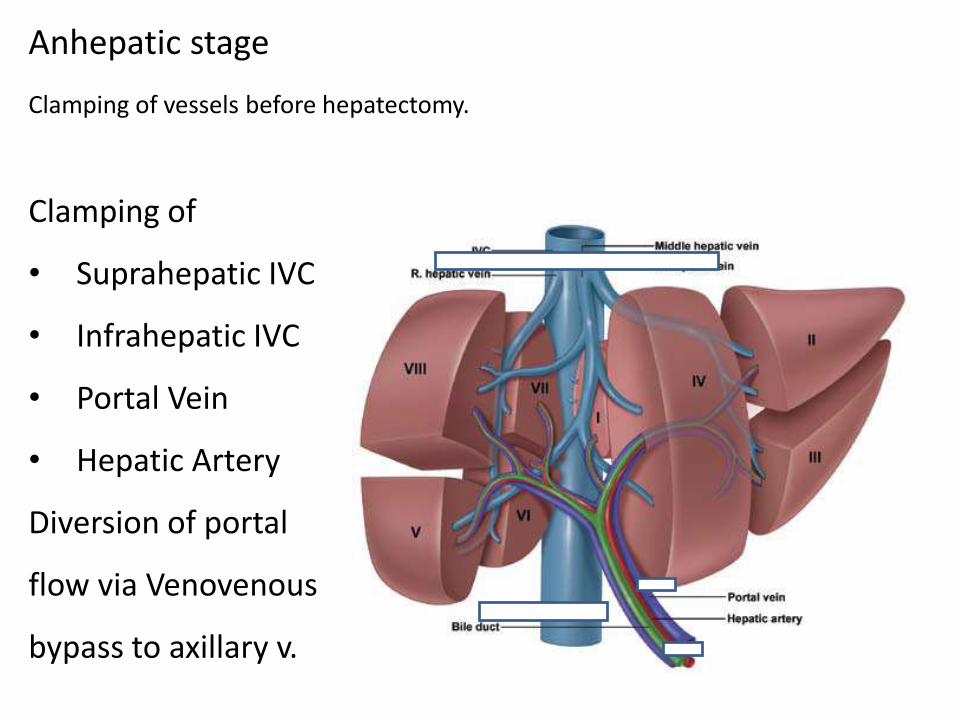
Anhepatic stage
Clamping of
• Suprahepatic IVC
• Infrahepatic IVC
• Portal Vein
• Hepatic Artery
Diversion of portal
flow via Venovenous
bypass to axillary v.
Clamping of vessels before hepatectomy.

Anhepatic stage
Order of anastomosis
• IVC Clamp – Suprahepatic,
then Infrahepatic IVC
• Portal Vein
• Hepatic Artery
Order of clamping
1. Suprahepatic IVC
2. Infrahepatic IVC
3. Portal Vein
4. Infrahepatic IVC
Removal of Vascular clamps
• Portal Vein
• Suprahepatic IVC
• Infrahepatic IVC

Anhepatic stage
DisadvantagesAdvantages
Venovenous bypass
1. Prevention of precipitous
reduction in preload
2. Improves Renal Perfusion
Pressure
3. Lessens Splanchnic
Congestion
4. Delays development of
Metabolic Acidosis
1. Air Embolism
2. Thromboembolism
3. Inadvertent decannulation
4. Delays development of
Metabolic Acidosis
Fibrinolysis during anhepatic stage is a risk due to unopposed action of tissue
plasminogen activator.
Neohepatic stage
1. When was it harvested i.e. Graft Ischemia time.?
2. Is the Graft compatible.?
3. Is the donor an adult or child.? (dictates requirement of size down surgery on
the side and consequent blood loss)
4. Has the new liver been washed to minimize reperfusion effects.? (washed
with Stabilized Human Serum, Ringers Lactate or Albumin)
5. If the Liver was cut down, how was the free edge sealed (This has an impact
on blood loss following revascularisation)
What do we need to know about the new liver..?

Neohepatic stage
Reperfusion of graft through portal vein
Consequences of Reperfusion
1. Hyperkalemia
• ECG changes
• Calcium Chloride/ Sodium Bicarbonate – treatment
• Albuterol & Insulin
• Intraoperative Dialysis
2. Hydrogen ion concentration increases
3. Increase in preload
4. Decrease in SVR, decrease in B.P.
Post – Reperfusion Syndrome
Azathioprine,Medrol 10 mg/kg
Antibiotics

Neohepatic stage
Systemic Hypotension + Pulmonary HTN (5 mins)
1. Probable Causes
• Hyperkalemia
• Acidosis
• Hypothermia
• Air/ Thrombotic emboli
• Vasoactive substances
• First venous reperfusion, then arterial anastomosis and biliary reconstruction comes later.
Post – Reperfusion Syndrome
1. Risk factors for PRS
• Elevated Preanhepatic K+ levels
• Use of “donated after cardiac death” liver
• Suboptimal grafts i.e.
> 50 yrs. of age h/o Cardiac arrest Hypotension Need for high dose inotropes > 5 days of ICU stay Elevated Liver fat content
• Graft Cold Ischemia time > 6 hours

Steps & Implications
HypovolemiaColloid
Infusion
Bleeding/ Coagulopathy
1. FFP after Incision
2. Prothrombin Complex Concentrates (PCCs)
3. Recombinant activated factor VII
4. Parameters to assess
• TEG
• PT
• Fibrinogen
• Platelet Count
Risk of TRALI, Circ. Overload
Thrombo-embolic complications
I. Abdominal Incision & Drainage of Ascites
II. Hyponatremia Central Pontine Myelinosis

Steps & Implications
Hyperkalemia
III. Blood Transfusions - Citrate Intoxication
VII. Other precautions
Hypocalcaemia, Hypomagnesaemia
IV. Reperfusion
1. Hourly blood gases
2. Electrolytes, Glucose, Ionised Ca2+ and Hb levels
3. Maintain Urine Output
V. Hyperglycaemia Wound site infection
Diuretics, Insulin + Glucose or last resort Dialysis
VI. Massive Infusions Hypothermia Heated Venovenous bypass

1. Preanhepatic stage
2. Anhepatic stage
3. Neohepatic stage
Bleeding
Cardiovascular Compromise
Hypoglycemia
Hypoglycaemia
Hypocalcemia
Severe Hypotension
Bradycardia
Arrhythmia
Dyselectrolytemia

Signs of successful graft function
1. Decreased Ca2+ requirements.
2. Improvements in acidosis.
3. Increased Urine Output.
4. Rise in core temperature.
5. Bile Output.
Antifibrinolytics
Graft Endothelial cell
Tissue Plasminogen activator
releases
Severe Fibrinolysis Treatment with Antifibrinolytics & cryoprecipitates.

Post Operative Care
Broad Based goals
1. Hemodynamic Stability
2. Metabolic Homeostasis
3. Analgesia• Opioids• Patient Controlled infusion • Epidural analgesia is contraindicated (Coagulopathy)
4. Monitoring Graft Function• Transaminase levels• PT• Bilirubin levels• Bile• Urine Output• Acid Base Status

Post Operative Care
Broad Based goals
5. Watch out for
• Bleeding
• Bile leaks
• Vascular thrombosis
• Primary Non-function
• Hyperglycemia (steroid usage)
6. Bear in mind
• Derangement of Transaminase levels (first 2 -3 days) is common.
Persistence beyond this period should raise suspicion of Hepatic
Artery Thrombosis.
• No clear guidelines for early extubation.

Organ Matching and allocation
Primary Criteria
1. ABO Blood type
2. Graft Size
• ABO incompatible is for emergent situations.
• Disease severity decides que priority
• Disease severity was earlier assessed by Child – Turcott – Pugh Score
1 2 3
Encephalopathy None 1-2 3-4
Ascites Absent Slight Moderate
Prothrombin time <4 4-6 >6
Albumin >3.5 2.8 – 3.5 <2.8
Bilirubin <2 2-3 >3

Organ Matching and allocation
• Presently Disease severity is assessed by MELD score
1. Serum Bilirubin
2. Creatinine level
3. INR
• MELD score fails to recognise HCC patients early on so they are given priority.
• MELD score between 12 – 14 benefit most from Liver Transplantation.
Living Liver Donor
1. First introduced in 1988
2. Full regeneration in 2 – 3 weeks
3. For pediatric recipients – left lobe is preferred
4. For adult recipients – right lobe is preferred
Anaesthetic Management
1. G.A.+ IPPV + Muscle relaxant
2. Adequate Venous Access
3. Arterial line
4. Nasogastric Tube

Living Liver Donor
1. During mobilization of liver watch for hypotension and bradycardia
2. To minimize blood loss
• Maintain low CVP (<5 cms H2O) (decreases Graft Edema)
• However, newer surgical techniques no longer require low CVP.
Anaesthetic Management
Blood Saving Strategies
1. Cell salvage technique
2. Preop donation of 1 – 2 units of autologous blood.
3. Intraoperative isovolemic hemodilution with retrieval of 1 – 2 units of
blood.

Living Liver Donor
1. Living donors can be extubated
2. Discontinuation of Mechanical ventilation reduces intrathoracic
pressure which reduces congestion.
3. Maintain optimal perfusion of liver by
• Adequate CO
• Avoidance of Hypovolemia
• Anemia
• Hypothermia induced coagulopathy
4. Post op analgesia
• Epidural Placement is advised (risk of hematoma due to coagulopathy have to be weighed)
5. Statistical
• R Hepatectomy has higher complication than L Hepatectomy.

Gracias