an urban healthcare model for outpatient care and wellness - final report
DESCRIPTION
Final Report for AIA Tuttle Fellowship: An Urban Healthcare Model for Outpatient Care and WellnessTRANSCRIPT
An Urban Modelfor Outpatient Careand Wellness
Amy D. KircherM.Arch, LEED AP BD+C, EDAC
AIA Arthur N. Tuttle Jr. Graduate Fellowshipin Health Facility Planning and Design

a special thanks to...
My Graduate Advisory Committee at Texas A&M UniversityKirk Hamilton, FAIA, FACHA, EDAC, Committee Chair
Mardelle Shepley, D.Arch., FAIA, FACHA, EDAC, LEED AP, Committee MemberJon Rodiek, Ph.D., FASLA, Committee Member
The AIA Arthur N. Tuttle Fellowship
and for their support and input... Deborah Sweetland, MBA, FACHE, HKS Architects
Alejandro Iriarte, M.Arch, WHR Architects

pg 3
Final Report November 2012
Table of Contents
IntroductionThe Concept: Major Issues
Project Goals
Case Study Selection
Part One: Background
Part Two: Best Practices
Case Studies
89
16
2024
Project Concepts
Part Three: Application4446Evidence Based Design Concepts50User Groups52City Master Plan58Flagship Facility
Literature Review 11
Conclusions and Future Studies
Part Four: Conclusions82
References
Appendix86
About This Document
Discussions and ConferencesBest Practices and Guidelines
3839
Acknowledgments 89

pg 4
An Urban Healthcare Model for Outpatient Care and Wellness
pg 5
Final Report November 2012
This document illustrates the work completed for the AIA Arthur N. Tuttle Jr. Graduate Fellowship in Health Facility Planning and Design. This study explores a new healthcare model for outpatient care and wellness through observation of built projects and discussions with those who share an interest in this topic. The lessons learned through the Tuttle Fellowship are incorporated in the design of a parallel thesis project completed for a Master of Architecture at Texas A&M University.
This document...
Is written for those interested in the design of healthcare spaces as related to outpatient care and wellness.
Does not seek to be the singular answer to the problems facing outpatient care and wellness today but is an exploration of what is plausible to create today or in the future.
Thank you for reading...
About ThisDocument
(Amy Kircher 2012)

pg 6
An Urban Healthcare Model for Outpatient Care and Wellness
Part One

pg 7
Final Report November 2012
-Introduction-The Concept: Major Issues-Literature Review-Project Goals
Background

pg 8
An Urban Healthcare Model for Outpatient Care and Wellness
Introduction
This project explores a new healthcare model for outpatient care and wellness.
The concept of an urban, decentralized, outpatient facility that provides primary care and wellness services is demonstrated through the development of one 40,000 square foot prototype facility located in downtown Portland, Oregon. A master plan incorporating variations of this facility is generated for the city of Portland to explore the concept of a network. The prototype facility is one example of a new model for community healthcare and addresses several current trends and issues in outpatient and chronic disease care. This model is designed to create new venues for patient and public education, staff collaboration, wellness activity, and an identity different from the current institutionalized healthcare setting.
This is a timely study due to the current rise of policy changes regarding continuum of care and preventive care. There is a great need to design a facility with a wellness approach to health in the United States. Architectural definitions for this type of facility will be beneficial to the development of future preventive care and wellness facilities. This study will illustrate a new direction that could be taken by preventive care design and it will potentially impact how we think about healthcare architecture beyond treatment-only facilities.
(Amy Kircher 2012)

pg 9
Final Report November 2012
The Concept: Major IssuesThe Main Question
project goals defining typology
• Location/Access to care • Program components • Functional adjacencies • Create link wellness to outpatient care architecturally • Urban context • Landscape design & elements • Welcoming and interactive environment
WELLNESS OUTPATIENT ?
• Policy changes. Accountable Care Act • Reimbursement models and soft costs (ACO, PCMH) • Health management
Impacts of Healthcare Reform
• Increase in % of population with chronic diseases • Patient-centric era • Changes in medical procedures and technology
Shift Towards Outpatient Care
• Need for preventive care and wellness • Education about health • Changing image of primary care
Need for a New Healthcare Typology
• Organizational changes • New architectural spaces • Aesthetics
Challenges to Address
the concept major issues
Major Issues to Explore
(Amy Kircher 2012)

pg 10
An Urban Healthcare Model for Outpatient Care and Wellness
project goals recent guidelines
Incorporate initiatives and published guidelines as a foundation for ideas, information, resources, and project goals
New Ways of Thinking
This project and document incorporates initiatives and recently published guidelines as foundation for information, ideas, resources, and project goals.
Active Design Guidelines by the City of New York • The Portland Plan by the City of Portland• The Model Design Manual for Living Streets by the Los Angeles County• Clinic Design Database through the Center for Health Design• Safety Net Clinic Design through the California Healthcare Foundation •

pg 11
Final Report November 2012
LiteratureReviewImpacts of Healthcare Reform
Within the last few years, there has been much discussion and speculation about the changes needed in the U.S. healthcare system. New and old buzz words like Accountable Care Organization (ACO), Patient Centered Medical Home (PCMH), and Patient Centered Primary Care Collaborative (PCPCC) are coming to the surface and there is an effort to define what these speculations mean in a concrete form (Fierce Healthcare, 2011). There are serious and urgent needs that are not being met by insurance and the existing reimbursement models, just as much as there are shortcomings in the education of the public at large in regards to the management of their health and focus on well-being. In the New England Journal of Medicine, an article shows that the poor performance of the U.S. Healthcare system in worldwide rankings is not because of the amount of money per capita, where the U.S. is ranked number 1, but lies in the number of preventable deaths related to overall health (Murray & Frenk, 2010). Murray and Frenk believe that the current approach taken to healthcare reform is not going to be enough to close the gap between the amount of money spent and health outcomes. They believe the U.S. needs to completely re-evaluate how the general public perceives health and the policies related to promoting better living and preventive services (Murray & Frenk, 2010; Peek & Oftedahl, 2010).
Several healthcare systems and other organizations are working together to assess what is needed in the healthcare environment of the future and how healthcare reform impacts these needs (Peek & Oftedahl, 2010). Some of the implications defined by the efforts of Peek and Oftedahl include a consensus operational definition of the PCMH and a list of main paradigm case clauses (Peek & Oftedahl, 2010). Many of these parameters are organizational, but several will change the architectural spaces in a facility. For example supporting a team based approach to care will need to be supported by a work environment designed to promote collaboration. As healthcare providers, insurance companies, the government and many other entities involved in healthcare try to define what needs to occur, there is a great opportunity to explore what this will mean architecturally for healthcare and the role the architect can have in improving public health.
pg 12
An Urban Healthcare Model for Outpatient Care and Wellness
literature review major topics explored
Wellness Outpatient
U.S Healthcare
System
Chronic Disease
Health Education
Access Types of Facilities
Urban Models
Health Literacy
Policy Changes
Community Involvement
Demographics
Active Living & Built Environment
Day Surgery
Diagnostics Diagnosis
Primary Care
Location
Insurance Types of
Programs Management ACO, PCMH
Location
Decentralized
Part of Campus
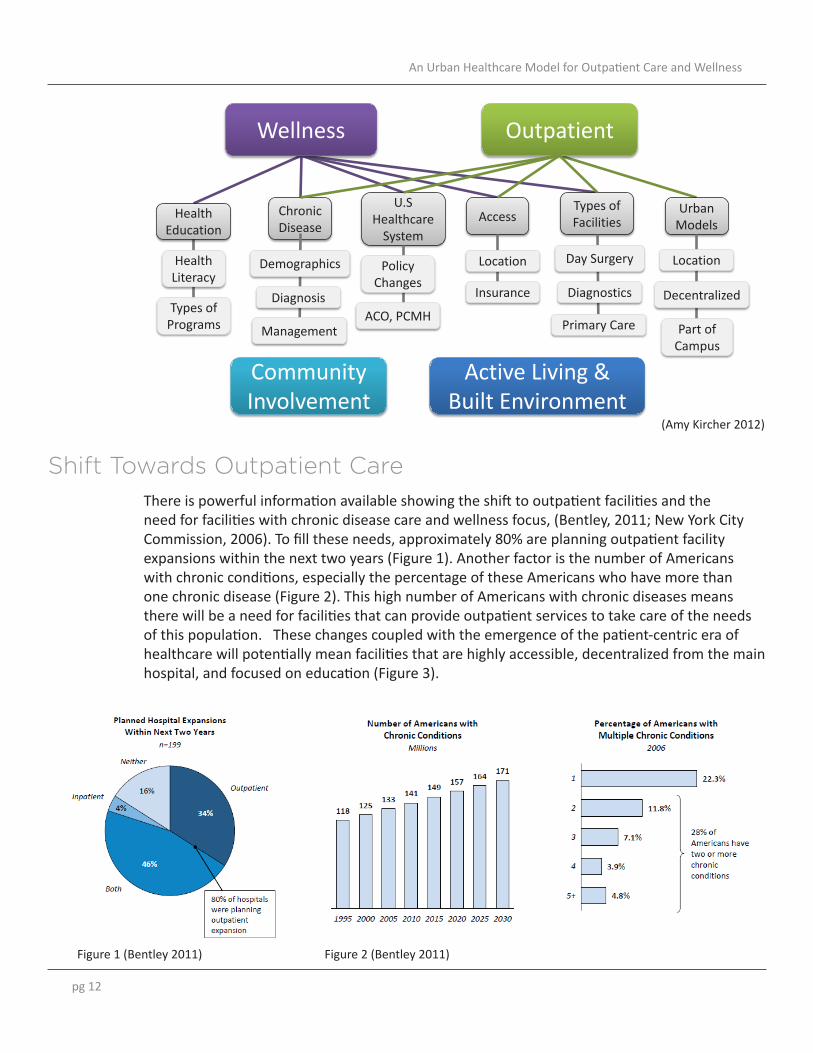
There is powerful information available showing the shift to outpatient facilities and the need for facilities with chronic disease care and wellness focus, (Bentley, 2011; New York City Commission, 2006). To fill these needs, approximately 80% are planning outpatient facility expansions within the next two years (Figure 1). Another factor is the number of Americans with chronic conditions, especially the percentage of these Americans who have more than one chronic disease (Figure 2). This high number of Americans with chronic diseases means there will be a need for facilities that can provide outpatient services to take care of the needs of this population. These changes coupled with the emergence of the patient-centric era of healthcare will potentially mean facilities that are highly accessible, decentralized from the main hospital, and focused on education (Figure 3).
Shift Towards Outpatient Care
(Amy Kircher 2012)
Figure 2 (Bentley 2011)Figure 1 (Bentley 2011)

pg 13
Final Report November 2012
New prototypes have emerged in the past few years for outpatient care, prevention, and wellness, and these are coming from some of the most respected healthcare providers in the nation (Hospital Compare, 2011; U.S. News, 2011). For example, Kaiser Permanente recently opened the Center for Total Health adjacent to its New Capitol Health Medical Center. It is described by Kaiser as a place open to the public where people come to learn, share, and connect about health (Kaiser Permanente, 2011). This new typology for patient education on healthcare is one example of how healthcare providers and architects are thinking outside of the box for how healthcare education is presented. Now is the opportune time to step back and re-evaluate the healthcare services provided, and the facilities in which they occur (Bentley, 2011).
Another emerging topic is wellness as a disease prevention tool, and the development of wellness facilities beyond the high-end boutiques (Figure 4). Here lies a great opportunity to develop new healthcare typologies that incorporate wellness facility type services alongside other types of patient care. In 2007, the Mayo Clinic opened the Dan Abraham Healthy Living Center supported by a generous donor who wanted to do something in return to those who had cared for him (Mayo Clinic, 2008). The Healthy Living Center is focused on employee health and wellness and the Mayo Clinic recently announced the center will be expanded to include patient health and wellness services thanks to the same donor. The center will be focused on providing ongoing support to patients aimed at the prevention of future disease (Mayo Clinic, 2011).
Need for a New Healthcare Typology
Figure 3 (Bentley 2011)

pg 14
An Urban Healthcare Model for Outpatient Care and Wellness
Figure 4 (Bentley 2011)
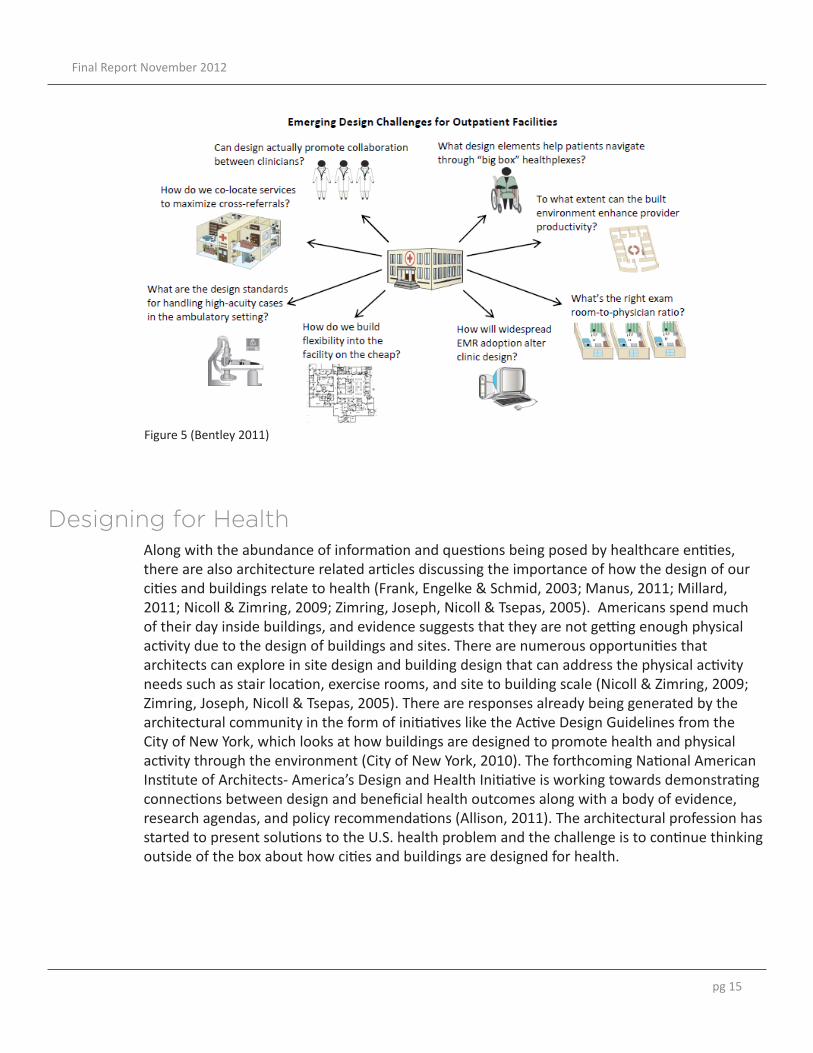
There are many challenges and unanswered questions when it comes to defining the healthcare policies needed and the interpretation of these needs for architecture. In addition to the challenges described by Figure 5 taken from the Advisory Board Report on the Ambulatory Facility of the Future (Bentley, 2011), there are additional challenges that need to be addressed and explored in the design of an urban healthcare model for outpatient care and wellness.
How could this new outpatient care model be incorporated into various cities.• The architectural implications for being based in urban areas and in communities.• Organizational changes that could influence the programming or functional adjacencies.• How the hospital infrastructure could be affected by the emergence of new departments or • care giving programs. The potential for spaces that will allow interdisciplinary teams to work to their full potential • as the care giving entity.Designing the spaces in which patient education will be enhanced. • Defining architectural aesthetics that lead away from traditional or institutional healthcare • design.
In addition to providing care, there is a need for higher levels of patient education (Hoving, Visser, Mullen, Van Der Borne, 2010). A study by Downey and Zun looked at health literacy levels among those visiting an emergency department compared to those visiting a community clinic (2008). Their findings included observing a less-than-adequate functional health literacy at all of the studied sites. They determined that the location or type of healthcare facility did not predict health literacy, but demographics regarding age and education levels were strong indicators (Downey& Zun, 2008). This demonstrates a need for better patient education outside of the hospital setting, and a venue that welcomes and engages the public to learn about their health. The study by Downy and Zun also supports and suggests a need for highly accessible healthcare that can provide better health education to the community (2008).
Challenges to Address for Outpatient Care and Wellness
pg 15
Final Report November 2012
Figure 5 (Bentley 2011)
Along with the abundance of information and questions being posed by healthcare entities, there are also architecture related articles discussing the importance of how the design of our cities and buildings relate to health (Frank, Engelke & Schmid, 2003; Manus, 2011; Millard, 2011; Nicoll & Zimring, 2009; Zimring, Joseph, Nicoll & Tsepas, 2005). Americans spend much of their day inside buildings, and evidence suggests that they are not getting enough physical activity due to the design of buildings and sites. There are numerous opportunities that architects can explore in site design and building design that can address the physical activity needs such as stair location, exercise rooms, and site to building scale (Nicoll & Zimring, 2009; Zimring, Joseph, Nicoll & Tsepas, 2005). There are responses already being generated by the architectural community in the form of initiatives like the Active Design Guidelines from the City of New York, which looks at how buildings are designed to promote health and physical activity through the environment (City of New York, 2010). The forthcoming National American Institute of Architects- America’s Design and Health Initiative is working towards demonstrating connections between design and beneficial health outcomes along with a body of evidence, research agendas, and policy recommendations (Allison, 2011). The architectural profession has started to present solutions to the U.S. health problem and the challenge is to continue thinking outside of the box about how cities and buildings are designed for health.
Designing for Health
pg 16
An Urban Healthcare Model for Outpatient Care and Wellness
Project GoalsTo incorporate the wellness and preventive care model with the outpatient care model.
Define programmatic requirements for combining wellness and outpatient care. • Determine the appropriate functional adjacencies and organization of the units.• Address what can architecturally link wellness to outpatient care.• Address challenges and problems with the development of a new outpatient care • model and the current U.S. healthcare policies and legal structure.
1.
To incorporate Portland’s plan for urban development and sustainability into the design of an urban facility and master plan for the city.
The city of Portland has developed the Portland Plan which includes tools for • architects, developers, and urban designers to use when planning their projects. A few of the tools and concepts I will be using are 20 minute neighborhoods, city • hubs, green expansion, equality, and sustainability.
2.
To enhance the building’s connection to the urban fabric and define the message conveyed to the community by the architectural and site design.
Connect the facility to the surrounding street and buildings through the site design.• Define the relationship between the site and architecture and their relationship to • the surroundings streets. Define an architectural language for outpatient care that differs from traditional • healthcare hospital design. Locate the prototype facility to have access to public transportation and within • walking distances of businesses and downtown neighborhoods.
3.

pg 17
Final Report November 2012
To foster community and social support for visitors and their families.
Develop spaces throughout the facility that encourage visitors and their families to • learn about their health and actions they can take to improve it. These spaces should be welcoming, intuitive, and appeal kinesthetically and visually • to the user.
4.
Enhance the education of the community of health through interactive architecture, and develop venues to foster learning and community support.
Define and design landscape and site elements for public use. • Utilize the urban site to provide a space for the community to gather. Provide • elements in the architectural design that can be used by the community after business hours.
5.

pg 18
An Urban Healthcare Model for Outpatient Care and Wellness
Part Two

pg 19
Final Report November 2012
-Case Study Selection-Case Studies-Interviews and Conferences-Best Practices and Guidelines
Best Practices

pg 20
An Urban Healthcare Model for Outpatient Care and Wellness
Case StudySelection
PhysicalContext
Urban ContextServices Context Context
UrbanP bli S
Connection to CitySiteCli i D i
Arch. DesignServices OfferedP i C
Outpatient
LocationPublic Spaces
BrandingClinic Design
Facility Planning/ApproachWellnessPreventive Care
Message to the Community
Functional Context
Healthy CommunitiesEducation
Community Outreach/ProgramsOperationsFunctional Organization
Program Components
Best practices case study selection
Case studies were selected based on a variety of criteria. A few of the case study sites were visited based on recommendations by healthcare architects and other professionals in the healthcare industry. Other case study sites were selected based on announcements from top healthcare providers.
Due to the nature of this project, and the goal of the fellowship to look at best practices, some facilities were chosen based on specific elements, public spaces, clinic design, etc and branch out from a typical outpatient or wellness center.
During certain visits, discussions were set up with facility managers, innovative leaders, and operations directors, and architects added to the depth of this study and the range of ideas posed. In some cities, rather than a facility tour, a discussion of the topic and best practices was the priority.
In total, eleven cities were visited and a total of thirteen facilities are included in this report.
(Amy Kircher 2012)

pg 21
Final Report November 2012
(Amy Kircher 2012)

pg 22
An Urban Healthcare Model for Outpatient Care and Wellness
Case StudyConnection
to City UrbanPublic Spaces Location
Community Outreach
Healthy Communities Education
Outpatient Care
Services Offered
Preventive & Wellness Services
Programatic Components Operations
Functional Organization
Arch Design
Site Design
Clinic Design Branding
Facility Planning
Bloorview Kids Rehabilitation
CAMH
Kasier Center for Total Health & Capitol Hill Medical CenterMayo Dan Abraham Center for Healthy Living
Methodist Outpatient Center Wellness Facility
MGH Ambulatory Practice of the Future
Mills City Clinic
Polyclinic
Randall Children's Hospital
UMCG Outpatient Clinic
Wellspring Medical Center Woodburn
Whittier Clinic
YMCA Houston
Urban Context Message to Community
Services Functional Context Physical Context
This table consolidates all thirteen case studies based on the characteristics observed and evaluated during each facility tour.

pg 23
Final Report November 2012
Case StudyConnection
to City UrbanPublic Spaces Location
Community Outreach
Healthy Communities Education
Outpatient Care
Services Offered
Preventive & Wellness Services
Programatic Components Operations
Functional Organization
Arch Design
Site Design
Clinic Design Branding
Facility Planning
Bloorview Kids Rehabilitation
CAMH
Kasier Center for Total Health & Capitol Hill Medical CenterMayo Dan Abraham Center for Healthy Living
Methodist Outpatient Center Wellness Facility
MGH Ambulatory Practice of the Future
Mills City Clinic
Polyclinic
Randall Children's Hospital
UMCG Outpatient Clinic
Wellspring Medical Center Woodburn
Whittier Clinic
YMCA Houston
Urban Context Message to Community
Services Functional Context Physical Context
(Amy Kircher 2012)

pg 24
An Urban Healthcare Model for Outpatient Care and Wellness
Case StudiesBloorview Children’s Rehabilitation HospitalToronto, Ontario, Canada
Centre for Addiction and Mental Health (CAMH)Toronto, Ontario, Canada
Kaiser Permanente Center for Total HealthLocation: Washington DC
Mayo Clinic - Dan Abraham Healthy Living CenterLocation: Rochester, Minnesota
Methodist Outpatient CenterHouston, Texas
MGH Ambulatory Practice of the FutureBoston, Massachusetts
Mill City Clinic at University of MinnesotaLocation: Minneapolis, Minnesota
PolyclinicSeattle, Washington
Randall Children’s HospitalPortland, Oregon
UMCG Outpatient CenterGroningen, Netherlands
Wellspring Medical CenterWoodburn, Oregon
Whittier ClinicLocation: Minneapolis, Minnesota
YMCA - Tellepsen Family DowntownLocation: Houston, Texas
1
2
3
4
5
6
7
8
9
10
11
12
13

pg 25
Final Report November 2012
Bloorview Kids Rehabilitation HospitalLocation: Toronto, Ontario, CanadaArchitects: Montgomery Sisam Architects and Stantec ArchitectureOpened: 2006Visited: September 2012
Located near a residential area in Toronto, Bloorview is a unique multi-use facility that combines a hospital, rehabilitation center, research center, school, and recreation center. This facility creates a welcoming and supportive environment that has a holistic approach to health, treatment and rehabilitation of children and youth with disabilities. The 358,000 square foot L-shaped facility creates a hierarchy of public and private spaces. Public spaces within the facility are open and accessible to all users and encourage use by those living in the nearby neighborhoods.
The landscape design incorporates walking trails and multiple gardens designed for physical therapy and different types of play and healing. Creating an environment that incorporates natural light and a physical connection to the outdoors was a priority. The overall form of the facility and slope of the elevation was designed to integrally connect to the surrounding community and natural vegetation on the site. On the interior, the open design creates views to different functions and a sense of transparency of services. One example is the ability to see children taking swimming lessons in the pool and participating in aquatic rehabilitation classes from one of the main corridors.
Lessons Learned: This facility is an example of a hospital that has successfully become part of the community • and an inspirational place for children with disabilities. The landscape and site design in this facility create numerous opportunities for both physical • and visual access to nature. The facility incorporates several user groups in the services provided. For example • the school is for children who are patients as well as those of school age in the nearby neighborhood. Other services like the pool, gardens, cafe, and resource library are designed for public and patient use.
(Montgomery Sisam) (Montgomery Sisam)

pg 26
An Urban Healthcare Model for Outpatient Care and Wellness
Centre for Addiction and Metal Health (CAMH)Location: Toronto, Ontario, CanadaArchitects: Montgomery Sisam Architects, Kuwabara, Payne, McKenna, Blumberg and Kearns Mancini Architects.Opened: 2008Visited: September 2012
The Centre for Addiction and Mental Health located in downtown Toronto provides outpatient care and transitional residential care with the goal of creating a home-like environment that is supportive at every level. The complex is located on the original late 1800’s asylum site, but was designed to eliminate the stigma of mental health by becoming an integral part of the community. The master plan proposed eliminating the fortress like walls and facilities for buildings that are separate and designed more like an “urban village”. This concept incorporates apartment-like buildings and tree lined pedestrian friendly streets. Every part of the design reinforces the client vision of normalizing mental health care and a healthy connection to the community. The master plan for the complex also includes developments that are non-hospital buildings, with the intent of integrating the mental health facility into the urban fabric and community. Each individual facility is designed as a supportive environment that provides numerous opportunities for interactions between clients and staff members. The facility supports many activities in which clients are able to give back to the community ranging from art shows, volunteer work, and even cafes for the public where the employees are patients.
Lessons Learned: The new design and master plan have helped revive the commercial area nearby. New • business and populations have moved in and the facility has integrated well due to its openness and transparency with the community. The master plan incorporates not only the design of healthcare facilities but public • amenities and housing. The patients in this facility participate in community programs from art to volunteering for • charities and other events.
(Montgomery Sisam) (Montgomery Sisam)

pg 27
Final Report November 2012
Kaiser Permanente Center for Total Health Location: Washington DC Architects: Ralph Appelbaum Associates IncorporatedOpened: April 2011Visited: August 2011
Located adjacent to the Kaiser Permanente Capitol Hill Medical Center, The Center forTotal Health is a new approach to health education and discussion. It is described as a place for the community to gather and discuss the future of healthcare and what advancements have been made already. The Center for Total Health is designed to be an interactive environment with monitors and displays that respond to the users’ touch. The main feature is an 80’ by 9’ interactive wall display. Throughout the 13,000 square foot facility interactive LCD monitors are incorporated with bold graphics to create displays where a visitor can learn about a topic related to health or healthcare delivery. Several displays also feature different technologies used to deliver care such as hand held ultrasounds and heart monitors. One education room is dedicated to housing a mock-up of an exam room almost identical to an exam room found in any Kaiser Permanente facility around the country. The Center for Total Health is open to all visitors and is also used by medical professionals for events and small conferences. The program incorporates several open and enclosed spaces to create flexibility in how theCenter for Total Health can be used. The center is designed to be self-guided with a simple race track type floor plan to assist with wayfinding. The finishes in the center were simple and minimal to keep the focus on the interactive screens and colorful displays.
Lessons Learned: This facility is an example of healthcare education in the form of a museum type learning • environment. The entry to this facility was very similar in design to the adjacent Capitol Hill Medical Center • and the two are often confused by visitors. A clear language or hierarchy to identify the facility is important. Acoustics and lighting need to be considered carefully with interactive displays. Glare can be • an issue, as well as the noise from several displays being played all at once.
(Amy Kircher, 2011) (Amy Kircher, 2011)
pg 28
An Urban Healthcare Model for Outpatient Care and Wellness
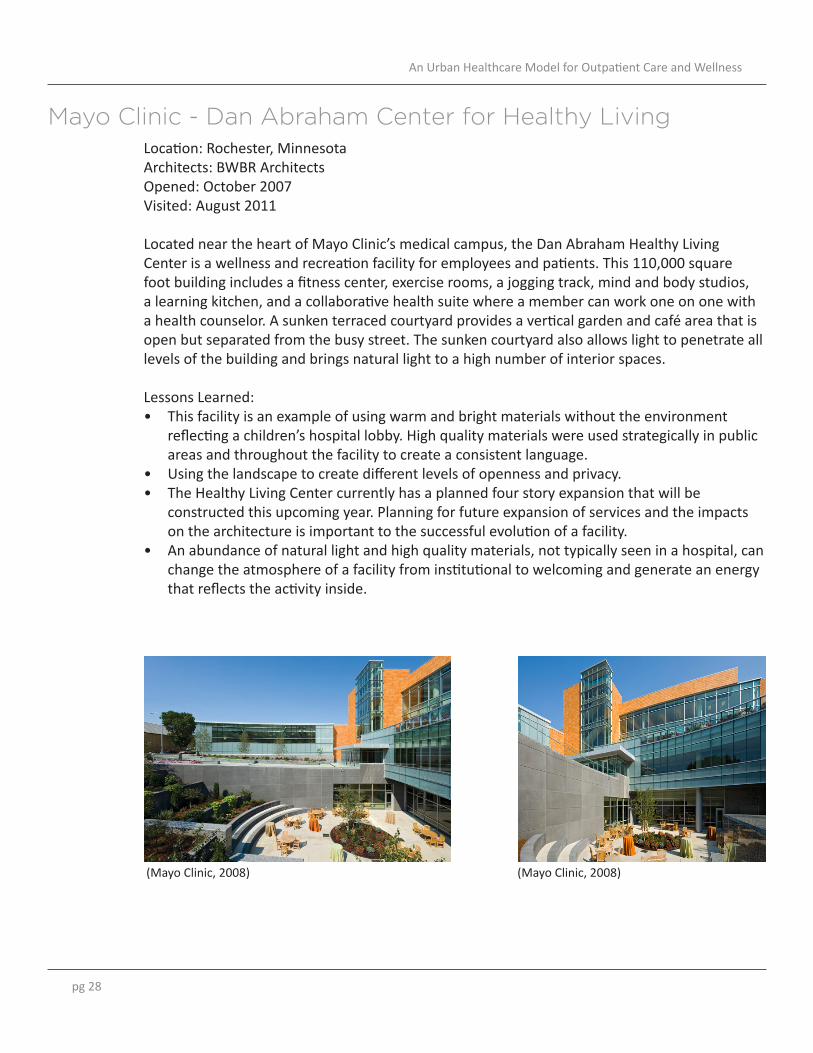
Mayo Clinic - Dan Abraham Center for Healthy LivingLocation: Rochester, Minnesota Architects: BWBR ArchitectsOpened: October 2007Visited: August 2011
Located near the heart of Mayo Clinic’s medical campus, the Dan Abraham Healthy Living Center is a wellness and recreation facility for employees and patients. This 110,000 square foot building includes a fitness center, exercise rooms, a jogging track, mind and body studios, a learning kitchen, and a collaborative health suite where a member can work one on one with a health counselor. A sunken terraced courtyard provides a vertical garden and café area that is open but separated from the busy street. The sunken courtyard also allows light to penetrate all levels of the building and brings natural light to a high number of interior spaces.
Lessons Learned: This facility is an example of using warm and bright materials without the environment • reflecting a children’s hospital lobby. High quality materials were used strategically in public areas and throughout the facility to create a consistent language. Using the landscape to create different levels of openness and privacy.• The Healthy Living Center currently has a planned four story expansion that will be • constructed this upcoming year. Planning for future expansion of services and the impacts on the architecture is important to the successful evolution of a facility. An abundance of natural light and high quality materials, not typically seen in a hospital, can • change the atmosphere of a facility from institutional to welcoming and generate an energy that reflects the activity inside.
(Mayo Clinic, 2008) (Mayo Clinic, 2008)

pg 29
Final Report November 2012
Methodist Outpatient Center - Wellness FacilityLocation: Houston, TexasArchitects: WHR ArchitectsOpened: October 2010Visited: September 2012
The Methodist Hospital in Houston, Texas, expanded their real estate in the Texas Medical Center with the completion of the 1.6 million square foot Outpatient Center. This 26 story facility created a new landmark in the skyline of the Texas Medical Center.
The Wellness Facility, located within the Outpatient Center serves staff, their familes, and referred patients through over 400 different services. A few of the programs include Executive Health Physicals, Corporate Wellness Services, Fitness Center, Seafarers Club, and Weight Management Program.
Lessons Learned: On the triangular floor plate, public spaces and group spaces are located on the perimeter • to provide views of the Medical Center and natural daylighting. Flexible spaces are provided to accomodate different activities. During most hours of the day • the fitness area is open for recreational activities, but on certain mornings is designated for cardio testing. The Wellness Facility was given dedicated space within the main tower, rather than another • building so that staff have easy access to a health facility. There are also future plans for expansion on other levels of the facility.
(The Methodist Hospital and WHR Architects)

pg 30
An Urban Healthcare Model for Outpatient Care and Wellness
MGH Ambulatory Practice of the FutureLocation: Boston, MassachusettsArchitects: Anshen+AllenOpened: Summer 2010Visited: August 2011
Located on the top floor of a multi-use building in downtown Boston, the Ambulatory Practice of the Future is a primary care clinic dedicated to patient centered care and a collaborative work environment. This 7,100 square foot clinic has 15 exam rooms served by a team of physicians, nurse practitioners, and allied health professionals. It currently serves MGH employees, and serves as a prototype for future facilities. Throughout the clinic, a welcoming environment incorporates natural wood tones and cool nature colors. The waiting area serves as a resource center with flexible seating, computers for patient use, and a small kitchen. Natural light pours into the waiting area through floor to ceiling windows, and provides a view of downtown Boston. The clinic features an open team work area central to the exam rooms. Located between the waiting area and team work area is a combination conference and education room that can be adapted to suit different purposes. This room can be divided into a large and small space using a motorized partition and rearranging the modular furniture. The Ambulatory Practice of the Future is designed to balance standardization and flexibility by incorporating each where it is most beneficial to the delivery of care.
Lessons Learned: Each exam room has standardized equipment including dual computer screens, bluetooth • electronics and vitals equipment, access to electronic medical records, and a printer. This set up is designed to promote collaboration and dialogue between the patient and the caregiver. The flexibility of the spaces in this facility allow for multiple set-ups that can accomodate • a range of activities from more traditional primary care to wellness activities with multiple patients.
(Amy Kircher, 2011) (Amy Kircher, 2011)

pg 31
Final Report November 2012
Mill City ClinicLocation: Minneapolis, Minnesota Architects: HGA ArchitectsOpened: 2008Visited: August 2011
The Mill City Clinic is a small 4,000 square foot primary care clinic that redefines the connection of the community to a healthcare facility. The clinic is located in the historic Mill District on the first level of a condominium building directly across from the prominent Guthrie Theater. The atmosphere of the street is reflected in the design of this clinic through the incorporation of art and light. Tall sheer curtains that mimic stage curtains create privacy for the public lobby space while allowing an abundance of natural light to penetrate the space. The exam rooms and work areas are designed with special attention to articulating a clean but not sterile look. Every piece of equipment has a space designed for it, but the use of different finishes brings a warmth to the work spaces.
Lessons Learned: This facility was retrofitted into the first level of a condominium building that had 20’ • high ceilings. Rather than bringing down the ceiling height to one consistent height, the architects used the high ceilings to bring in natural light to the inner portion of the floor plan. Definition of spaces and hierarchy was defined by different ceiling heights and partial walls. The clinic has a shell space in the back portion that is being used for community events • rather than a storage space. The staff at this clinic hold events about art and health, local artists display their work, book signings, and a new event called Hippocrates Café led by the head physician Dr. Jon Halberg. According to an interview I did with Dr. Jon Halberg, head physician, it has been important • on this project to keep a consistent architectural language and approach to the design. As the needs of the clinic have evolved and modifications made, having the same architects who started the project has led to the successful evolution of this project over the years.
(Perkins & Will, 2008) (Perkins & Will, 2008)
pg 32
An Urban Healthcare Model for Outpatient Care and Wellness
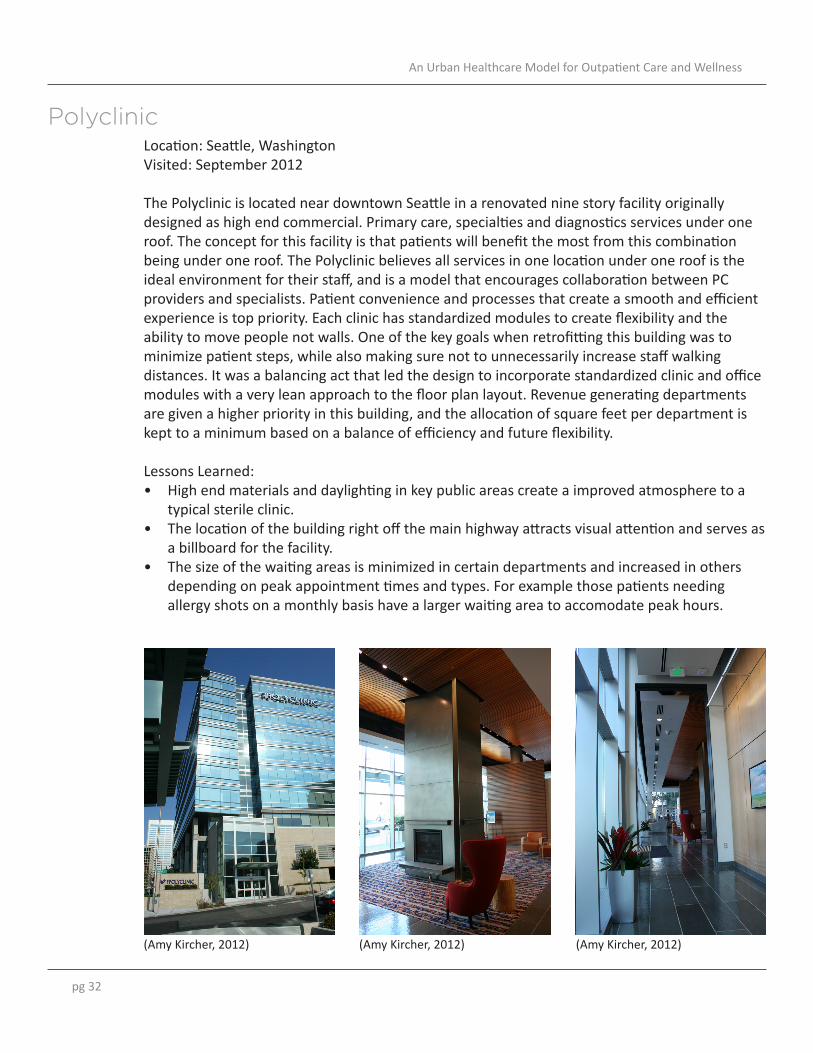
PolyclinicLocation: Seattle, WashingtonVisited: September 2012
The Polyclinic is located near downtown Seattle in a renovated nine story facility originally designed as high end commercial. Primary care, specialties and diagnostics services under one roof. The concept for this facility is that patients will benefit the most from this combination being under one roof. The Polyclinic believes all services in one location under one roof is the ideal environment for their staff, and is a model that encourages collaboration between PC providers and specialists. Patient convenience and processes that create a smooth and efficient experience is top priority. Each clinic has standardized modules to create flexibility and the ability to move people not walls. One of the key goals when retrofitting this building was to minimize patient steps, while also making sure not to unnecessarily increase staff walking distances. It was a balancing act that led the design to incorporate standardized clinic and office modules with a very lean approach to the floor plan layout. Revenue generating departments are given a higher priority in this building, and the allocation of square feet per department is kept to a minimum based on a balance of efficiency and future flexibility.
Lessons Learned: High end materials and daylighting in key public areas create a improved atmosphere to a • typical sterile clinic. The location of the building right off the main highway attracts visual attention and serves as • a billboard for the facility. The size of the waiting areas is minimized in certain departments and increased in others • depending on peak appointment times and types. For example those patients needing allergy shots on a monthly basis have a larger waiting area to accomodate peak hours.
(Amy Kircher, 2012) (Amy Kircher, 2012) (Amy Kircher, 2012)

pg 33
Final Report November 2012
Randall Children’s HospitalLocation: Portland, OregonArchitects: ZGF ArchitectsOpened: January 2012Visited: December 2011
This nine story facility with 165 beds and approximately 334,000 sq ft was designed to consolidate previously separated pediatric care and serves as a new identity for the children’s hospital. The project is located between the Legacy Emanuel campus and a residential neighborhood. The overall design strived to meet the needs of the functional program while respecting the scale and proximity of the residential neighborhood. The site placement and landscape design create a sense of place and arrival with pedestrian pathways and gardens. Legacy Emanuel has a reputation for playful healing gardens and this continues on the Randall Children’s site.
The public spaces and wayfinding for this project are inspired by the four geographic regions of Oregon and was used on many levels throughout the project to narrow the gap between hospitality and healthcare. The hospital has many amenities for families, patients, and staff with several at the main level accessible to the public including a gallery space and cafe.
Lessons Learned: Regional inspired graphics and images used for wayfinding give a unique identity to different • areas of the facility. Creating opportunities for communication among patients and patient’s families through • the design of common areas and lounges. This facility includes amenities in the public spaces for the community and strives to respect • the adjacent neighborhood.
ABOVE NW View of main hospital entrance PHOTOGRAPHER Nick Merrick @ Hedrich Blessing
(ZGF Architects, 2012) (ZGF Architects, 2012) (ZGF Architects, 2012)

pg 34
An Urban Healthcare Model for Outpatient Care and Wellness
UMCG Outpatient ClinicLocation: Groningen, The NetherlandsVisited: May 2011
The Outpatient Clinic is housed within the larger 1,100 bed University Medical Center Groningen (UMCG) located in the northern Netherlands. This facility is one of the largest in the Netherlands and serves a very large population. The Outpatient Clinic is located on the group floor for ease of access for patients and prevent visitors from getting lost. Inpatients are located on the floors above the Outpatient Clinic, and this separation helps staff keep control of who is on the inpatient floors.
The UMCG is dedicated to serving their patients and the surrounding community. There are several amenities for the public on the first levels including small grocery shops, flower shops, bookstores, cafes, and restaurants. The UMCG complex serves as a destination for many people within the community because of the friendly atmosphere it provides for all visitors.
Lessons Learned: Providing flexibility for patients can be done in a variety of ways. This clinic provided several • different types of furniture, from tables and chairs to lightweight foam, extremely mobile lounge chairs. This allows for patients who come to the facility several times a month or week to customize their experience to fit their needs. The use of color and graphics in this facility is uplifting and vibrant. • Art work in this facility was selected carefully for each user group. Staff areas incorporate • different art than patient areas, which usually are nature focused. Connecting to the community can be done in a variety of ways, from artwork to volunteering • and events at the facility.
(Amy Kircher, 2011) (Amy Kircher, 2011)

pg 35
Final Report November 2012
WellspringLocation: Woodburn, OregonArchitects: Clark/Kjos ArchitectsVisited: December 2011
This health and wellness center, located about 30 miles South of Portland, occupies and transforms the shell of an empty K-Mart building. To remove the image of the big box retailer, a new façade was added to the entry, the interior utilizes curved walls, and large interior courtyards were added throughout the floor plan. The main departments are designed around a main interior garden courtyard with a circular corridor that is the equivalent of a 16th of a mile.
This facility offers a variety of services including primary care, a fitness area with boot camps for patients, an urgent care area, dental and other wellness services. There are also retail and café areas that are used by the community not just visitors to the clinic. Several of the departments are designed to be easily renovated without impacting other areas of the facility. Since it opened several areas have adjusted over the years to accommodate changing needs in the community. This facility was envisioned to compliment the main hospital’s services and offer an environment outside the hospital setting for health education and wellness.
Lessons Learned: This facility demonstrates the adaptive re-use of a big box retail building into a healthcare • oriented facility. The flexibility of the spaces and overall design allow for changes in services offered. For • example one area of the facility is being renovated to be a small day surgery department to fill a need within the community. This facility works to integrate itself in the community and offer services that are needed by • the community based on cost and demographics.
(Clark/Kjos Architects)

pg 36
An Urban Healthcare Model for Outpatient Care and Wellness
Whittier ClinicLocation: Minneapolis, Minnesota Architects: HGA ArchitectsOpened: October 2010Visited: August 2011
This primary care clinic is part of the Hennepin County Medical Center and is located on an urban site and on a street with a variety of building types ranging from shops to restaurants to loft housing. The design of this 60,000 square foot facility builds on the pedestrian character of the street by limiting the height of the structure and using a variety of materials to minimize the building’s massing. Colorful accents are used on the façade and the interior architecture that reflect the character of the community and surrounding buildings. On the interior, each clinic is developed as a module and assigned a vibrant color and graphic image to aid in wayfinding. The colors and graphic elements are also a solution to have a diverse community that speaks multiple languages without needing signs to translate everything. The street side entry to this facility is treated like a public plaza space. There are “pocket parks” and gardens for different plants to be grown, places to sit, a bike rental rack, and other spaces for the community to use.
Lessons Learned: This facility uses a team work center rather than offices and nurse stations for staff. This has • positive results in generating a teamwork approach to care, but noise can be an issue even on the quietest days. From the beginning, the design of this clinic involved the community from the type of care • provided, aesthetic preferences, and amenities that could be used by the community. Organizational and architectural aspects that provide a community friendly atmosphere. For • example parking can be used by nearby businesses after hours, so the parking lot is open and visible from the street. Also, certain rooms in the facility are located near the entry so that the community can use them after hours, but organized in a way that the rest of the facility can be locked up properly.
(HGA Architects, 2010) (HGA Architects, 2010)

pg 37
Final Report November 2012
YMCALocation: Houston, TexasArchitects: Kirksey ArchitectsOpened: October 2010Visited: October 2011
The Tellepsen Family Downtown YMCA is located in downtown Houston and is the largest YMCA in the greater Houston area. This 100,000 square foot facility serves over 10,000 members and offers a variety of program space from an indoor swim center, running track, to counseling and educational services. This facility also has a large portion dedicated to community outreach. Support services like child watch areas, teen activity rooms, computer labs, a chapel, conference centers for public use, and a wellness center. The Tellepsen YMCA architecturally is a visual landmark for the surrounding streets. The lightness of the glass façade with the bold graphic elements stands out from surrounding buildings and creates a strong urban presence.
Lessons Learned: This facility’s urban presence at the street level is open and welcoming to those walking • around downtown Houston. The building introduces a new architectural language to this portion of downtown Houston • and becomes a landmark. The glass façade allows the different types of activity happening on the interior to be viewed • by the community and highlights health as a community activity. The different types of activity and programs are layered on top of one another in the • building, which allows for an open and interactive environment among the members.
(Kirksey Architecture, 2010) (Kirksey Architecture, 2010)
pg 38
An Urban Healthcare Model for Outpatient Care and Wellness
Discussions andConferences
Farrow Partnership
ICSI
Kaiser Permanente in Portland
Mayo Center for Innovation
Mayo Transform Conference
Phillips Powderhorn
Virginia Mason Institute
1
2
3
4
5
6
7The Fellowship allowed me to attend several conferences and attend sessions and to have discussions with a number of experts and people focused on outpatient care and wellness. Each new experience and discussion became an exchange of thoughts and ideas with a myriad of lessons learned.
Community input can encourage ownership and higher levels of involvement. • Many strive to have people to take responsibility of their own health and give them the tools to bring health back to the culture of the community. The goal of many of the “grassroots” organizations was not to undermine an existing • healthcare systems in place, but to add another avenue for partnerships and component of health in the community. Everyone has the opportunity to learn from another’s perspective, and no single person has • the magic solution or answer. The sharing of ideas and collaboration is the key to improving outpatient care, wellness, and community health. There are many differing types of practices, from pioneers in lean, to organizations that • customize each appointment. No matter the type of practice chosen, it was customized to the organization. In no circumstance is there a checklist to replicate and follow without considering the implications on the organization at all levels.

pg 39
Final Report November 2012
Best Practicesand Guidelines
PhysicalContext
Urban ContextServices Context Context
UrbanP bli S
Connection to CitySiteCli i D i
Arch. DesignServices OfferedP i C
Outpatient
LocationPublic Spaces
BrandingClinic Design
Facility Planning/ApproachWellnessPreventive Care
Message to the Community
Functional Context
Healthy CommunitiesEducation
Community Outreach/ProgramsOperationsFunctional Organization
Program Components
Best practices case study selection
The lessons learned from each case study were combined into the five main categories shown in the figure below. The chart on the next page shows a sampling of specific lessons learned within each of the categories and the exemplary case studies within that area.
There are a wide range of solutions each with their own merit and innovation. Based on the lessons learned, it is apparent there are many organizations testing new ideas, that are looking for ways to improve the care they provide while maintaining efficiency, cost effectiveness, and a positive image in their community.
(Amy Kircher 2012)

pg 40
An Urban Healthcare Model for Outpatient Care and Wellness
Connection to City Urban
Public Spaces Location
Community Outreach
Healthy Communities Education
Outpatient Care
Services Offered
Preventive & Wellness Services
Programmatic Components Operations
Functional Organization
Arch Design
Site Design
Clinic Design Branding
Facility Planning
Definition
Goals
Applications
Urban Context Message to Community
Services Functional Context Physical Context
Location of facility in city and the relation to adjacent buildings.
• YMCA Houston • CAMH • Wellspring Medical • Mayo DACHL
Types of services in the facility offered to patients, the public, and staff.
Provide a range of services for a variety of users, while balancing soft and hard costs.
• Include diagnostic and treatment services that keep some patient groups out of the main hospital• Provide wellness services that add value to the building and attract a range of demographics.
Connect to the community to increase health awareness of the public and users of the facility.
Programs, services, and approach to involving community in facility.
• Relate facility to nearby buildings through programs offered • Include nearby businesses and community in the design process. • Provide areas of the building that can be used “after hours” by the public
Position the facility as a destination point within the context of the city
• Allocate portion of site to public usage• Locate the facility to provide access from public transportation, pedestrians, bicycles, and vehicular traffic• Relate facility to nearby facilities architectural and site design
• YMCA Houston
• Create an open and welcoming environment at the public level and spaces• Design the site to allow wellness programs to utilize the space• Give the facility a brand that represents the values of the facility in regards to community health and wellness.
Create a facility that speaks of health rather than illness. Change the face of what a healthcare providing facility can be.
Architectural design and aesthetics of the facility. How the clinics were design and planned.
Adjacencies and locations of different functions and departments.
Design the facility to optimize the functional and operational aspects.
• Create adjacencies between treatment and wellness services where spaces and services can be shared• Evaluate the operations of the facility in terms of hours open vs services provided• Design the soft costs spaces to be flexible for future changes in services offered
Case Study Exemplars
• Whittier Clinic • Methodist Wellness • City Mills Clinic• Whittier Clinic • Wellspring Medical Center
• Whittier Clinic • City Mills Clinic• UMCG • Polyclinic ‐ Seattle
• Kaiser Center for Total • City Mills Clinic • Philips Powderhorn • Polyclinic ‐ Seattle
• Whittier Clinic• City Mills Clinic • Bloorview Kids Rehab
• City Mills Clinic • UMCG

pg 41
Final Report November 2012
Connection to City Urban
Public Spaces Location
Community Outreach
Healthy Communities Education
Outpatient Care
Services Offered
Preventive & Wellness Services
Programmatic Components Operations
Functional Organization
Arch Design
Site Design
Clinic Design Branding
Facility Planning
Definition
Goals
Applications
Urban Context Message to Community
Services Functional Context Physical Context
Location of facility in city and the relation to adjacent buildings.
• YMCA Houston • CAMH • Wellspring Medical • Mayo DACHL
Types of services in the facility offered to patients, the public, and staff.
Provide a range of services for a variety of users, while balancing soft and hard costs.
• Include diagnostic and treatment services that keep some patient groups out of the main hospital• Provide wellness services that add value to the building and attract a range of demographics.
Connect to the community to increase health awareness of the public and users of the facility.
Programs, services, and approach to involving community in facility.
• Relate facility to nearby buildings through programs offered • Include nearby businesses and community in the design process. • Provide areas of the building that can be used “after hours” by the public
Position the facility as a destination point within the context of the city
• Allocate portion of site to public usage• Locate the facility to provide access from public transportation, pedestrians, bicycles, and vehicular traffic• Relate facility to nearby facilities architectural and site design
• YMCA Houston
• Create an open and welcoming environment at the public level and spaces• Design the site to allow wellness programs to utilize the space• Give the facility a brand that represents the values of the facility in regards to community health and wellness.
Create a facility that speaks of health rather than illness. Change the face of what a healthcare providing facility can be.
Architectural design and aesthetics of the facility. How the clinics were design and planned.
Adjacencies and locations of different functions and departments.
Design the facility to optimize the functional and operational aspects.
• Create adjacencies between treatment and wellness services where spaces and services can be shared• Evaluate the operations of the facility in terms of hours open vs services provided• Design the soft costs spaces to be flexible for future changes in services offered
Case Study Exemplars
• Whittier Clinic • Methodist Wellness • City Mills Clinic• Whittier Clinic • Wellspring Medical Center
• Whittier Clinic • City Mills Clinic• UMCG • Polyclinic ‐ Seattle
• Kaiser Center for Total • City Mills Clinic • Philips Powderhorn • Polyclinic ‐ Seattle
• Whittier Clinic• City Mills Clinic • Bloorview Kids Rehab
• City Mills Clinic • UMCG
(Amy Kircher 2012)
pg 42
An Urban Healthcare Model for Outpatient Care and Wellness
Part Three

pg 43
Final Report November 2012
-Project Concepts-Evidence Based Design Concepts-User Groups-City Master Plan-Flagship Facility
Application

pg 44
An Urban Healthcare Model for Outpatient Care and Wellness
ProjectConceptsIntroduction
This project is a 40,000 square foot prototype facility located in downtown Portland, Oregon that will incorporate primary care and wellness services. This facility will be approximately 5 stories in height to minimize the footprint of the building on the site and allow a large square footage to be dedicated to landscape elements. A master plan for the city of Portland will be generated showing variations of this facility, and demonstrate the concept of a network of urban, decentralized, outpatient facilities. This network of facilities will be a new model for community health and will address several current trends and issues in outpatient care and chronic disease care. It will also be explored how this prototype facility creates new venues for wellness, public education on various health topics, and patient and staff collaboration. The notion of a link or connection to the community will also be defined and explored in the design of the prototype facility. The primary function of these facilities will be to provide outpatient and primary care services, wellness services, recreational opportunities, education on a variety of healthcare topics, and create a community identity related to health rather than treatment. This study illustrates a new direction that could be taken by preventive care design and it could potentially impact how we think about healthcare architecture beyond treatment-only facilities.
Mission StatementThe Urban Healthcare Model for Outpatient Care and Wellness will provide a new and accessible model for community health. The model will incorporate outpatient and primary care, wellness services, recreational opportunities, and community health education programs. This facility will inspire and empower the community to gain control of their health and create a strong, sustainable movement in health education and wellness.

pg 45
Final Report November 2012
program concept defining components
Connection
Ambulatory Services
Wellness Services
Education
Nutrition
Recreation
Retail
Specialty Services
PCP Clinic
Treatment
Diagnostics
Community
General Program ConceptThe program concept for this project is to combine ambulatory and wellness services in a single facility, and create a strong connection to the community. Based on the desired size of the facility, there could be several different components to ambulatory care or wellness added to the facility ranging from a robust diagnostics department to a full sized recreation and fitness area. The general concept is to maintain a balance of hard and soft costs within the facility, while generating a positive reputation in the community.
(Amy Kircher 2012)

pg 46
An Urban Healthcare Model for Outpatient Care and Wellness
Evidence Based Design Concepts
The goal is to encourage movement and various levels of physical activity through site planning and architectural features. Site design will work with principles that encourage walking and be designed to engage the visitor to explore the South Park Block. The design of the building will incorporate features that emphasize an active lifestyle and wellness.
Examples:Locate building near parks to encourage outdoor activities and use.• 5 ‘D’ Variables – Imageability, Enclosure, Human Scale, Transparency, Complexity.• Visibility - views to active portions of building to encourage use• Design of stairs for everyday use – especially routes under 4 stories.• Provide visually appealing environments.•
Selected Sources:
Lee, C. & Moudon, A. (2008). Operational Neighbourhood Design and Physical Activity. Building Research & Information. 36(5), 395-411.
Brownson, R., Baker, E., et. al. (2001). Environmental and Policy Determinants of Physical Activity in the United States. American Journal of Public Health. Vol 91, No. 12, 1995-2003
City of New York. (2010). Active Design Guidelines: Promoting Physical Activity and Health in Design. New York City: City of New York.
Frank, L., Engelke, P., & Schmid, T. (2003). Health and community design: the impact of the built environment on physical activity. (1st ed.). Washington, DC: Island Press.
Nicoll, G. & Zimring, C. (2009). Effect of innovative building design on physical activity. Journal of Public Health Policy, 30(S1), S111-S123.
Zimring, C., Joseph, A., Nicoll, G. & Tsepas, S. (2005). Influences of Building Design and Site Design on Physical Activity: Research and Intervention Opportunities. American Journal of Preventive Medicine, 28(2S2), 186-193.
Encourage an active lifestyle and wellness through architectural design and space planning.

pg 47
Final Report November 2012
The goal is to educate the user on a holistic approach to health. Spatial planning will be designed to incorporate hands-on learning experiences (i.e. cooking). Facility will strive to educate the user so they can continue on path to better health and give them the tools/knowledge needed. Flexible spaces will be provided to hold multiple purposes where interactions, learning, and support from staff and other users can occur.
Examples:Signage for active living strategically placed at stairs and elevators.• Integrate learning zones into already existing departments. For example an exhibition • kitchen with the café. Add interactive learning elements to waiting areas. •
Selected Sources:
Nahrsted, W. (2004). Wellness: A New Perspective For Leisure Centers, Health Tourism, and Spas in Europe on the Global Health Market. In The Tourism and Leisure Industry: Shaping the Future, (pp. 181-198).
McCusky, J. F. (2008). Creating Engaging Environments in Rehabilitation. Topics in Stroke Rehabilitation, 15(2), 80-86.
Downey, L. A., & Zun, L. S. (2008). Assessing adult health literacy in urban healthcare settings. Journal of the National Medical Association, 100(11), 1304-1304-8. Retrieved from http://lib-`ezproxy.tamu.edu:2048/login?url=http://search.proquest.com/docview/214046587?accountid=7082.
Hoving, C., Visser, A., Mullen, P. D., & van den Borne, B. (2010). A history of patient education by health professionals in Europe and North America: From authority to shared decision making education. Patient Education and Counseling, 78(3), 275-281. doi: 10.1016/j.pec.2010.01.015.
Kaiser Permanente. (2011). Kaiser Permanente Center for Total Health. Retrieved April 11, 2011, from http://www.centerfortotalhealth.org.
New York City Commission. (2006). Planning for the Future: Capacity Needs in a Changing Healthcare System. New York City Commission on Health Care Facilities in the 21st Century.
Incorporate learning environments throughout the building and site design.

pg 48
An Urban Healthcare Model for Outpatient Care and Wellness
The goal is to design multiple connections with nature that are healing, restorative and stimulating. Design will also create an immersion into nature that stimulates all senses: visual, auditory, touch, smell, taste, through a variety of plant types and landscape spaces. Gardens will be designed for both the building’s program and also for public access.
Examples:• Pedestrian pathways crossing the site to encourage use. • Aggregate outdoors spaces into one large area rather than several small ones.• Create a connection between indoor spaces and outdoor areas to encourage use.
Selected Sources:
Cooper Marcus, C . & Barnes, M. (1999). Healing Gardens: Therapeutic Benefits and Design Recommendations. New York: John Wiley & Sons, 1999.
Gerlach-Spriggs, N., Kaufman, R. & Warner Jr., S. (1998). Restorative Gardens: The Healing Landscape. New Haven, CT and London: Yale University Press.
Ulrich, R. S. (1999). Effects of Gardens on Healthcare Outcomes: Theory and Research. In Healing Gardens: Therapeutic Benefits and Design Recommendations. (pp. 27-85).
Rodiek, S. (2009). Outdoor Evaluation Tool. Access to Nature: Planning Outdoor Spaces for Aging.
Provide access and view to nature for all user groups.

pg 49
Final Report November 2012
The facility will be designed to give access to natural daylighting to various users of the building. The design will incorporate windows that bring in daylight for all appropriate user groups, and where possible skylights for internal portions of the floor plate. Where privacy is needed, smaller windows will be incorporated, but designed to bring in daylighting.
Examples:• Daylighting along paths of travel to make more visually appealing.• Use of skylights or light wells to bring light into typically windowless areas. • Access to daylight from staff work spaces.
Selected Sources:
Joseph, A. (2003). The Impact of Light on Outcomes in Healthcare Settings. The Center for Health Design.
Ulrich, R. S. (1991). Effects of Interior Design on Wellness. Journal of Healthcare Interior Design, 97-109.
Millard, B. (2011). Lightness of Being. Architect: The AIA Magazine, April 26-27.
Figueiro, M. G., Rea, M. S., Stevens, R. G., Rea, A. C. (2002). Daylight and Productivity – A Possible Link to Circadian Regulation. The Lighting Research Office of the Electric Power Research Institute (2002), 185-193.
Leather, P., Pygras, M., Beale, D., & Lawrence, C. (1998). Windows in the Workplace: Sunlight, View, and Occupational Behavior. Environment & Behavior, 30(6), 769-762.
Alimoglu, M. K., & Donmez, L. (2005). Daylight Exposure and the Other Predictors of Burnout Among Nurses in a University Hospital. International Journal of Nursing Studies, 42(5), 549-555.
Incorporate daylighting into the building design to give access to all major user groups.

pg 50
An Urban Healthcare Model for Outpatient Care and Wellness
User Groups
user groups definitions
Well Patient
Sick Patient
Non Patient
Traditional patient description – suffering from a health problem and in need of diagnosis and treatment.
Patient seeking preventive or routine care. Long term follow up for chronic patients. Also includes health education and counseling.
All other visitors and users of the facility. Wide range, includes healthy visitors, staff and service providers, and even pedestrians on the street.
Staff
(Amy Kircher 2012)
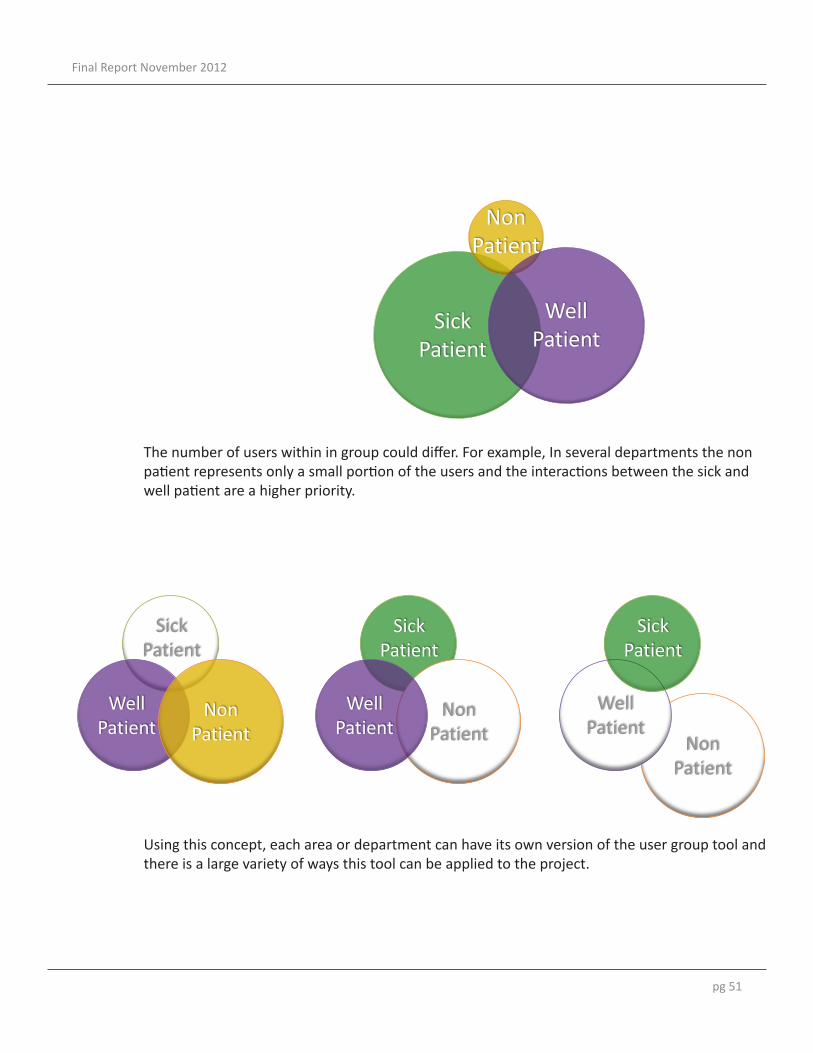
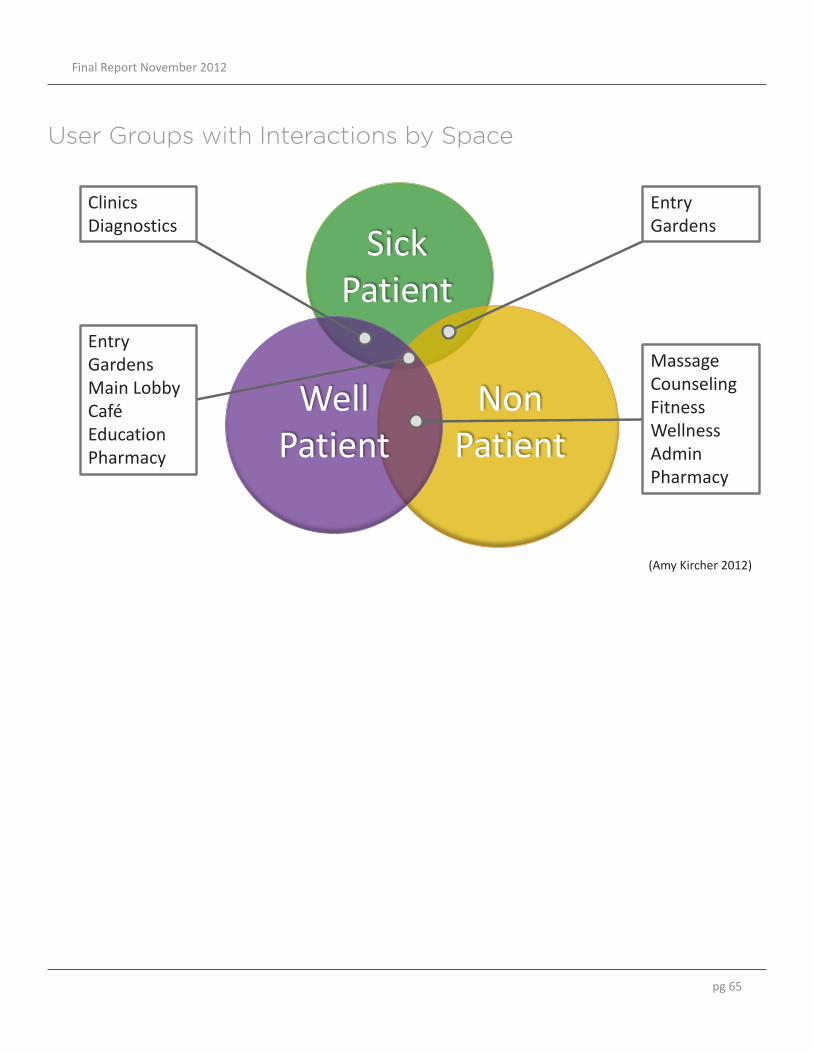
This project analyzes the functional planning and aesthetic design for multiple users. Many healthcare projects focus on the patient care and the patient’s perspective. In this project, my goal was to design for all potential users, so I created a tool to analyze design decisions. This tool is based on three user groups, the sick patient, well patient, and the non patient.
user groups interactions
Well Patient
Sick Patient
Non Patient
The overlaps between two or more groups represent the interactions. The interactions can be translated to architectural spaces.
All Diagrams (Amy Kircher 2012)
pg 51
Final Report November 2012
user groups variations
Well Patient
Sick Patient
Non Patient
user groups variations
Well Patient
Sick Patient
Well Patient
Non Patient
Well Patient
Sick Patient
Non Patient
Non Patient
Sick Patient
The number of users within in group could differ. For example, In several departments the non patient represents only a small portion of the users and the interactions between the sick and well patient are a higher priority.
Using this concept, each area or department can have its own version of the user group tool and there is a large variety of ways this tool can be applied to the project.

pg 52
An Urban Healthcare Model for Outpatient Care and Wellness
City Master PlanThe city of Portland developed the Portland Plan in response to the growing challenges for the city including growth, education, income, and environmental concerns.
The Portland Plan was created through the collaboration of the city and the public. Comments and involvement from the residents of Portland was welcome. (Over 20,000 comments from residents to date.) Advancing equity is the foundation of the Portland Plan.
There are numerous tools for urban planners and architects to use. A variety of mapping and analysis conducted by the city gives strategies for developing a project in relation to the city’s needs and urban planning goals.
Incorporation of Portland Plan in this Study... For my project, I utilized several key concepts and tools from the Portland Plan. The incredible amount of research and information prepared by the City of Portland aided in development of the Master Plan of Facilities and the Flagship Facility portion of this study. The following sections describe a few of these tools I incorporated.
(City of Portland)

pg 53
Final Report November 2012
20 Minute Neighborhood Analysis
Analysis based on an individual’s needs• Developed to track where amenities are concentrated• Describes in detail the services and amenities available• Can be used to determine the missing or lacking amenities in a community•
(City of Portland)
(City of Portland)
pg 54
An Urban Healthcare Model for Outpatient Care and Wellness
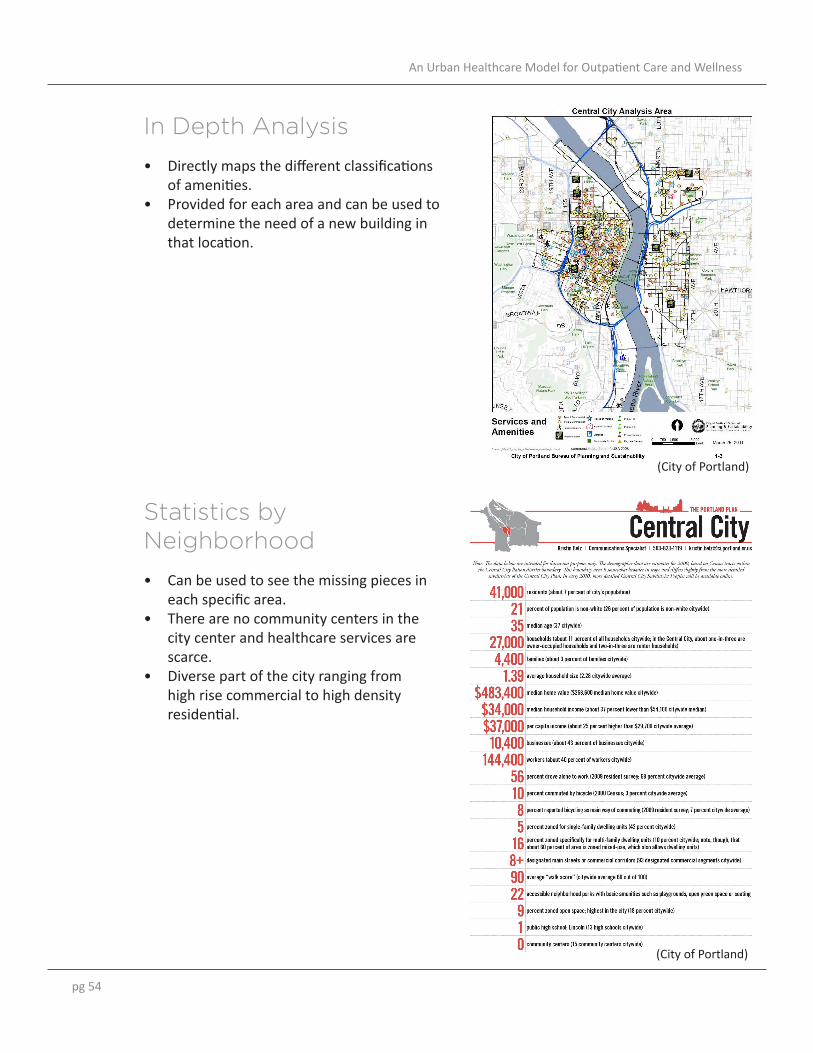
In Depth Analysis
Directly maps the different classifications • of amenities. Provided for each area and can be used to • determine the need of a new building in that location.
Statistics by Neighborhood
Can be used to see the missing pieces in • each specific area. There are no community centers in the • city center and healthcare services are scarce.Diverse part of the city ranging from • high rise commercial to high density residential.
(City of Portland)
(City of Portland)

pg 55
Final Report November 2012
Healthy Connected Neighborhoods
Based on the 20 Minute Neighborhood analysis. • Hubs are anchors for the 20 Minute Neighborhood.• Hub could be a community center, park, school, housing, or any public gather place. • Priority to create a network of city greenways.•
Greenways at different scales: preservation of forests• development of parks• tree canopy growth• neighborhood sidewalks• pedestrian boulevards•
(City of Portland)
pg 56
An Urban Healthcare Model for Outpatient Care and Wellness
(Amy Kircher 2012)
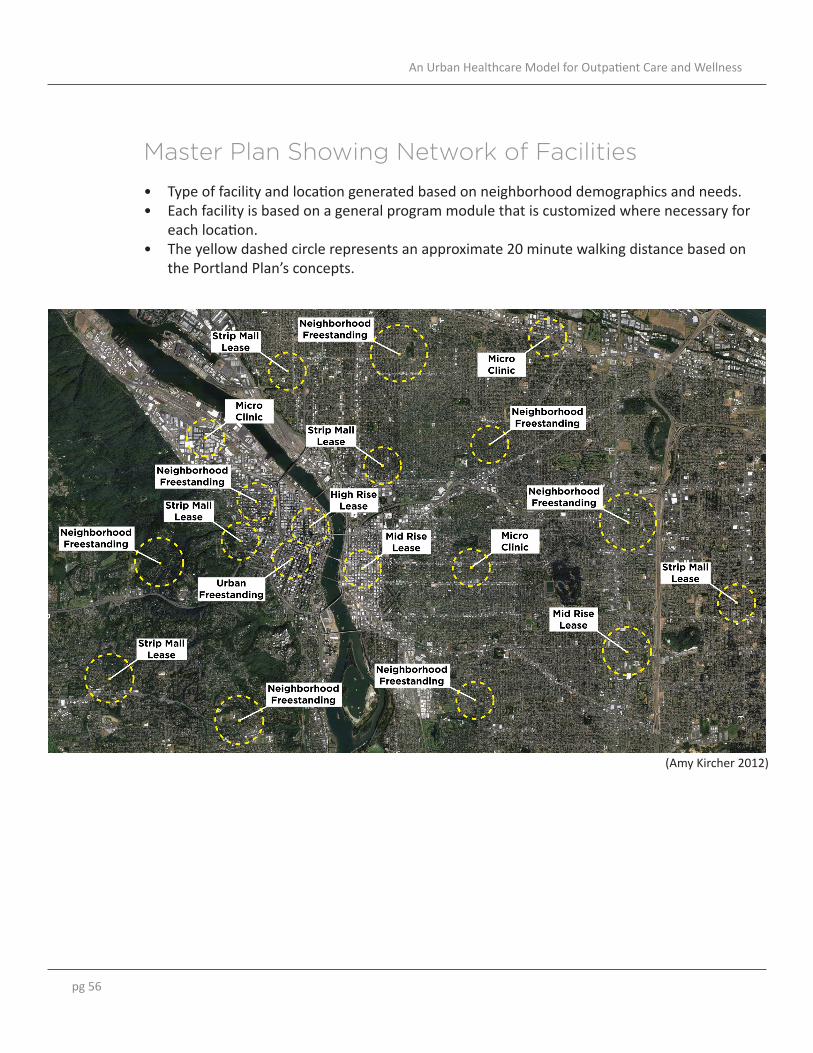
Master Plan Showing Network of Facilities
Type of facility and location generated based on neighborhood demographics and needs. • Each facility is based on a general program module that is customized where necessary for • each location. The yellow dashed circle represents an approximate 20 minute walking distance based on • the Portland Plan’s concepts.

pg 57
Final Report November 2012
example of types facilities within network
Neighborhood Strip Mall
Neighborhood Freestanding
Downtown Leased Floors
Downtown Freestanding
• Family Practice and/or Pediatric focused • Family oriented
education programs • Smaller facility in size
• Family Practice and Pediatric focused • Robust recreational
and wellness program •Medium to large
sized facility
• Family Practice and Internal Medicine focused •Wellness, nutrition, &
stress management focused • Smaller to medium
sized facility
• Family Practice and Internal Medicine focused • Recreation and
wellness focused •Medium to large
sized facility
(Amy Kircher 2012)
Sample of Facilities within the Network

pg 58
An Urban Healthcare Model for Outpatient Care and Wellness
Flagship Facility
(Amy Kircher 2012)
(Amy Kircher 2012)
example of types facilities within network
Neighborhood Strip Mall
Neighborhood Freestanding
Downtown Leased Floors
Downtown Freestanding
• Family Practice and/or Pediatric focused • Family oriented
education programs • Smaller facility in size
• Family Practice and Pediatric focused • Robust recreational
and wellness program •Medium to large
sized facility
• Family Practice and Internal Medicine focused •Wellness, nutrition, &
stress management focused • Smaller to medium
sized facility
• Family Practice and Internal Medicine focused • Recreation and
wellness focused •Medium to large
sized facility

pg 59
Final Report November 2012
the city portland, oregon
central city portland, oregon
Site Selection • Locate building near park
to encourage outdoor activity (Zimring, et. al. 2005; Nicole & Zimring, 2009)
• Add to the neighborhood
to encourage physical activity. (Lee & Moudon, 2008) • Impact of the built
environment on physical activity in the community. (Frank, Engelke, & Schmid, 2003).
Locate building near park to encourage outdoor activity (Zimring, et. al. 2005; Nicole & Zimring, 2009)
Add to the neighborhood to encourage physical activity. (Lee & Moudon, 2008)
Impact of the built environment on physical activity in the community. (Frank, Engelke, & Schmid, 2003).

pg 60
An Urban Healthcare Model for Outpatient Care and Wellness
ClinicalFamily Practice and Internal Medicine clinics for the surrounding area. Clinical areas include exam rooms, waiting areas, staff work areas, and a minor procedure room.
DiagnosticsThe Diagnostic department supplies a core component of preventive care at this facility. Screening services include women’s imaging, CT, stress tests, and EKG.
Wellness CenterSpaces relating to stress management, massage therapy, nutrition, fitness and recreation. This part of the program will be designed to be flexible and to accommodate changes in trends.
EducationThis space includes conference rooms, group meetings areas, consultation rooms, and resource areas ranging from computer labs, library, and health related exhibits. This space will be interactive and encourage visitors to learn about how to improve their health and well-being.
CommunityThis portion of the program focuses on reaching out to the community and includes a variety of learning spaces. A flexible/multi-purpose space will be incorporated into the lobby and public areas that can be used as an extension of the education program or community programs (art displays, health workshops, community meetings, etc).
Narrative Program
Conceptual Adjacency Diagram
(Amy Kircher 2012)

pg 61
Final Report November 2012
Space Program
program preliminary stacking
Clinics
Diagnostics
Support/Admin
Wellness
Public/Retail
Parking
Support/Parking
program preliminary stacking
Clinics
Diagnostics
Support/Admin
Wellness
Public/Retail
Parking
Support/Parking
Preliminary Stacking Diagram
(Amy Kircher 2012)
(Amy Kircher 2012)

pg 62
An Urban Healthcare Model for Outpatient Care and Wellness
the city urban context
HIGH RISE & COMMERCIAL
LOW RISE & MIXED USE / RESIDENTIAL
MID RISE & MIXED USE / RESIDENTIAL
THEATER & ART DISTRICT
(Amy Kircher 2012)
Site Context
The site for the Flagship Facility is at the intersection of several different downtown districts. The final design draws influence from the nearby theater and art district. The scale of the facility is designed to fit in the mid-rise and mixed use buildings nearby while respecting that it is located near the high rise commercial district with residential areas nearby.

pg 63
Final Report November 2012
the site existing conditions
Concepts • Ability to cross site
• Create new public spaces
• Limit size of building
footprint • 5 Design Variables: Image,
Enclosure, Human Scale, Transparency, Complexity (City of New York, 2010)
ConceptsAbility to cross site• Create new public spaces• Limit size of building footprint• 5 Design Variables: Image, Enclosure, Human Scale, Transparency, Complexity (City of New • York, 2010)
ChallengesSmall Site (200’ by 200’)• Sloped (19’ across diagonal)• Connection to existing building• Limited options for service entries• Multiple approaches to site from public and private transportation•
Site Design Concepts
(Amy Kircher 2012)

pg 64
An Urban Healthcare Model for Outpatient Care and Wellness
Landscape Program:Limit size of building footprint User exclusive gardensDense and open gardensPublic plazaCommunity SpacesGardensPlazaActive store front on first level
Locate building near park to encourage outdoor activity (Zimring, et. al. 2005; Nicole & Zimring, 2009)
5 Design Variables: Image, Enclosure, Human Scale, Transparency, Complexity (City of New York, 2010)
Parti for Site Design
(Amy Kircher 2012)
pg 65
Final Report November 2012
Well Patient
Sick Patient
Non Patient
user groups interactions
Clinics Diagnostics
Entry Gardens Main Lobby Café Education Pharmacy
Entry Gardens
Massage Counseling Fitness Wellness Admin Pharmacy
(Amy Kircher 2012)
User Groups with Interactions by Space

pg 66
An Urban Healthcare Model for Outpatient Care and Wellness
Incorporate skylights in staff working area of the Diagnostics Dept and Clinic. (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
Provide views and access to nature, including views from clinic interior to a roof top garden and access to the roof top garden for multiple building users (Ulrich, 2009). Roof top garden and clinic layout is designed to maintain privacy for clinic users.
Two different types of gardens are incorporated in the landscape design, public access and controlled access. The controlled access garden is only accessible from within the building and utilizes the sloped site to create a raised garden space separated from the rest of the site design. The public access gardens are open to the general public and are designed to be an extension of the park block located to the east.
Site Plan
SITTING AREA
PLAZA
PUBLIC ACCESS
GARDENS
CONTROLLED ACCESS
GARDEN ROOFTOP TERRACE
EXISTING BUILDING
STAFF TERRACE
“POCKET GARDENS”
SITTING AREA
PLAZA
PUBLIC ACCESS
GARDENS
CONTROLLED ACCESS
GARDENS
EXISTING BUILDING CAR
RAMP
DOCK
(Amy Kircher 2012)

pg 67
Final Report November 2012
Gardens and Services
“POCKET GARDENS”
SITTING AREA
PLAZA
PUBLIC ACCESS
GARDENS
CONTROLLED ACCESS
GARDENS
EXISTING BUILDING CAR
RAMP
DOCK
Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009)
Integrate learning zones in lobby and waiting areas. (Downey, 2008; Nahrsted, 2004; Kaiser Permanente, 2011)
Add education areas that are open and accessible to all users and the public. (Hoving, et. al., 2010)
Site design includes a thoroughfare across the site for public use. This is to break up the city grid and encourage use of the plaza, gardens, and provide another point of access to the park block.
(Amy Kircher 2012)

pg 68
An Urban Healthcare Model for Outpatient Care and Wellness
“POCKET GARDENS”
SITTING AREA
PLAZA
PUBLIC ACCESS
GARDENS
CONTROLLED ACCESS
GARDEN
PUBLIC
EDUC. CAFÉ
CAR RAMP
Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009)
Integrate learning zones in lobby and waiting areas. (Downey, 2008; Nahrsted, 2004; Kaiser Permanente, 2011)
Add education areas that are open and accessible to all users and the public. (Hoving, et. al., 2010)
Red ovals highlight methods of vertical transport from the underground parking, the monumental stairs to the second level, and elevators and stairs going to all levels of the facility.
Level One(Amy Kircher 2012)

pg 69
Final Report November 2012
level 2 physical therapy & fitness
• Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009) •Overlap departments with similar
functions to create interactions (McCusky, 2008) • Provide views to nature (Ulrich, 2009)
• Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
LOCKERS
YOGA
FITNESS PHYS. THERAPY
LOBBY
Well Patient
Sick Patient
Non Patient
AEROBICS
Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009)
Overlap departments with similar functions to create interactions (McCusky, 2008)
Provide views to nature (Ulrich, 2009)
Incorporate daylighting for all users (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
Level Two
level 2 physical therapy & fitness
• Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009) •Overlap departments with similar
functions to create interactions (McCusky, 2008) • Provide views to nature (Ulrich, 2009)
• Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
LOCKERS
YOGA
FITNESS PHYS. THERAPY
LOBBY
Well Patient
Sick Patient
Non Patient
AEROBICS
(Amy Kircher 2012)
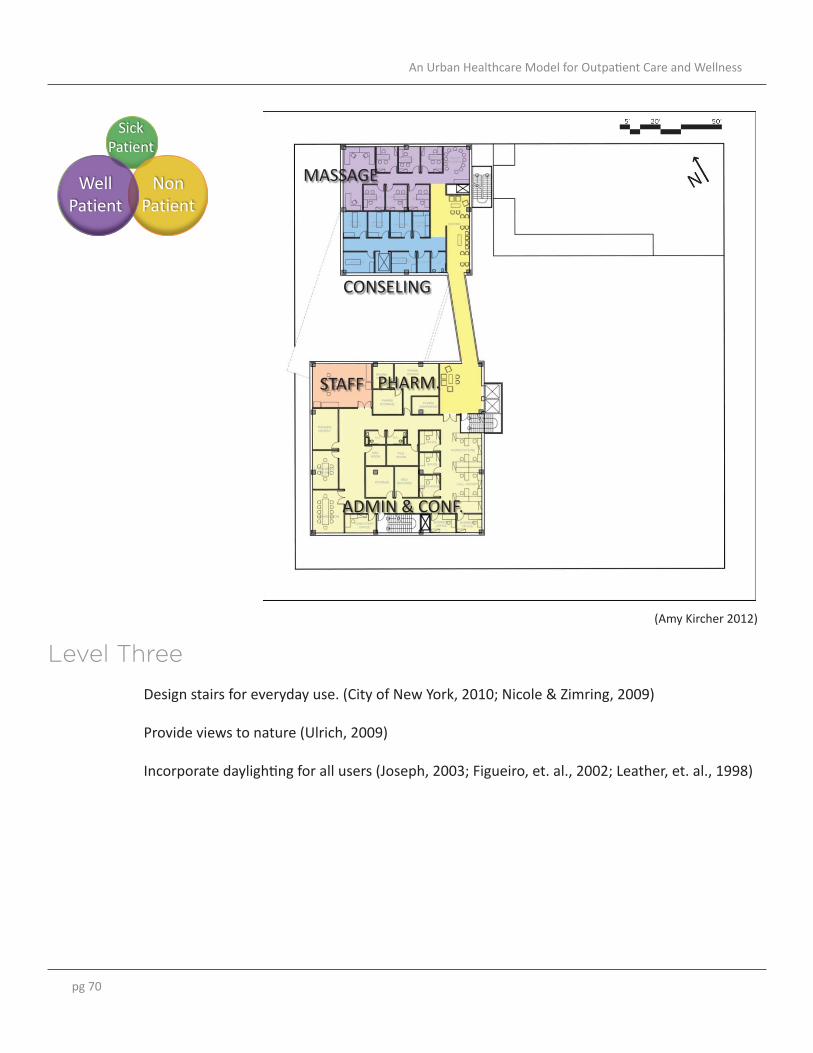
pg 70
An Urban Healthcare Model for Outpatient Care and Wellness
level 3 admin, staff, massage, counseling
• Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009) • Provide views to nature (Ulrich, 2009)
• Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
MASSAGE
CONSELING
PHARM. STAFF
ADMIN & CONF.
Well Patient
Sick Patient
Non Patient
Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009)
Provide views to nature (Ulrich, 2009)
Incorporate daylighting for all users (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
Level Three
level 3 admin, staff, massage, counseling
• Design stairs for everyday use. (City of New York, 2010; Nicole & Zimring, 2009) • Provide views to nature (Ulrich, 2009)
• Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
MASSAGE
CONSELING
PHARM. STAFF
ADMIN & CONF.
Well Patient
Sick Patient
Non Patient
(Amy Kircher 2012)

pg 71
Final Report November 2012
level 4 diagnostics
• Design stairs for everyday use between clinic and diagnostic staff areas. (City of New York, 2010; Nicole & Zimring, 2009) • Provide views to nature from select
clinic spaces and staff areas (Ulrich, 2009) • Incorporate daylighting in patient
waiting areas, for staff and selected clinical spaces. (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
CT
R/F
X-RAY
WAITING
DRESSING
LAB
MAMMO.
STAFF
ULTRA SOUND CARDIO.
STAFF ROOF TERRACE
Well Patient
Sick Patient
Non Patient
Design stairs for everyday use between clinic and diagnostic staff areas. (City of New York, 2010; Nicole & Zimring, 2009)
Provide views to nature from select clinic spaces and staff areas (Ulrich, 2009)
Incorporate daylighting in patient waiting areas, for staff and selected clinical spaces. (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
Level Four
level 4 diagnostics
• Design stairs for everyday use between clinic and diagnostic staff areas. (City of New York, 2010; Nicole & Zimring, 2009) • Provide views to nature from select
clinic spaces and staff areas (Ulrich, 2009) • Incorporate daylighting in patient
waiting areas, for staff and selected clinical spaces. (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
CT
R/F
X-RAY
WAITING
DRESSING
LAB
MAMMO.
STAFF
ULTRA SOUND CARDIO.
STAFF ROOF TERRACE
Well Patient
Sick Patient
Non Patient
(Amy Kircher 2012)
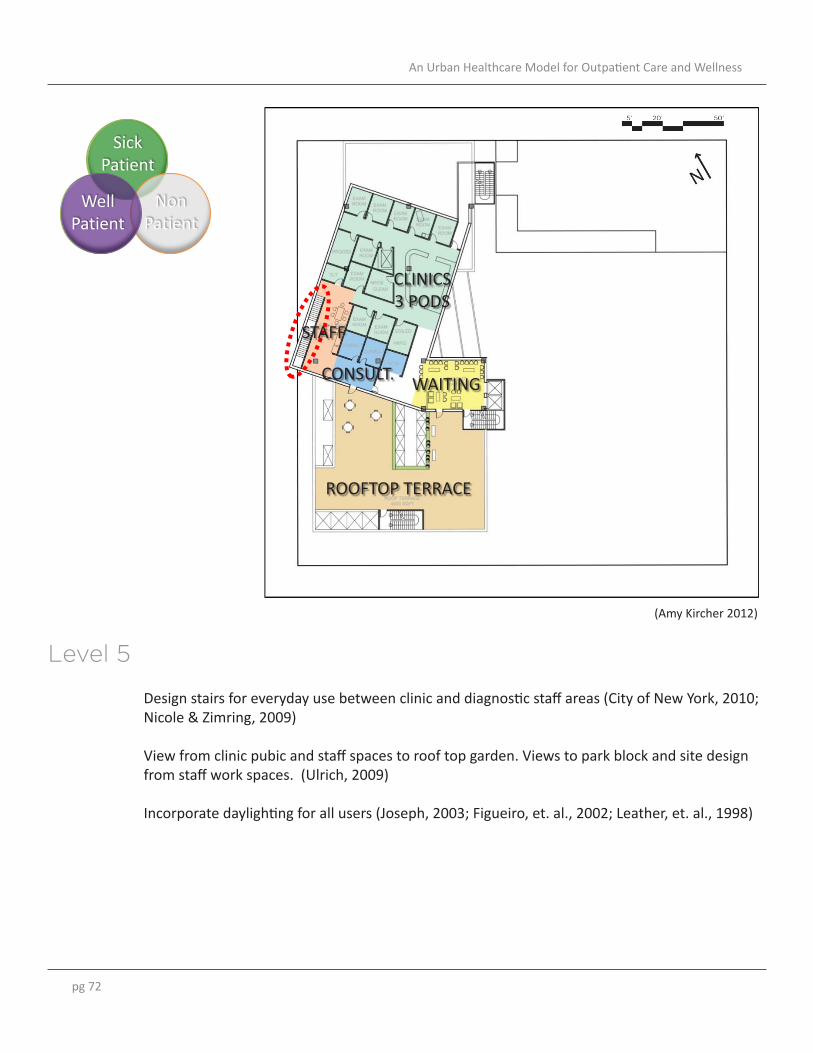
pg 72
An Urban Healthcare Model for Outpatient Care and Wellness
level 5 clinics – family practice
• Design stairs for everyday use between clinic and diagnostic staff areas (City of New York, 2010; Nicole & Zimring, 2009) • View from clinic pubic and staff spaces
to roof top garden. Views to park block and site design from staff work spaces. (Ulrich, 2009) • Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
STAFF
CONSULT.
CLINICS 3 PODS
WAITING
ROOFTOP TERRACE
Well Patient
Sick Patient
Non Patient
Design stairs for everyday use between clinic and diagnostic staff areas (City of New York, 2010; Nicole & Zimring, 2009)
View from clinic pubic and staff spaces to roof top garden. Views to park block and site design from staff work spaces. (Ulrich, 2009)
Incorporate daylighting for all users (Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
Level 5
level 5 clinics – family practice
• Design stairs for everyday use between clinic and diagnostic staff areas (City of New York, 2010; Nicole & Zimring, 2009) • View from clinic pubic and staff spaces
to roof top garden. Views to park block and site design from staff work spaces. (Ulrich, 2009) • Incorporate daylighting for all users
(Joseph, 2003; Figueiro, et. al., 2002; Leather, et. al., 1998)
STAFF
CONSULT.
CLINICS 3 PODS
WAITING
ROOFTOP TERRACE
Well Patient
Sick Patient
Non Patient
(Amy Kircher 2012)

pg 73
Final Report November 2012
section b. program stacking
STAFF TERRACE CONTROLLED ACCESS
TERRACE
LOBBY
DIAGNOSTICS
ADMIN
CLINICS
MECH. & SUPPORT PARKING
PARKING
WELLNESS
LOCKERS THERAPY
PASSAGE SERVICE
PARKING
Section A.
PORTLAND ART MUSEUMRESIDENTIAL &
COMMERCIAL ON 1ST LEVELON 1ST LEVEL
section b. city context
PORTLAND ART MUSEUMRESIDENTIAL &
COMMERCIAL ON 1ST LEVELON 1ST LEVEL
section b. city context
(Amy Kircher 2012)
(Amy Kircher 2012)
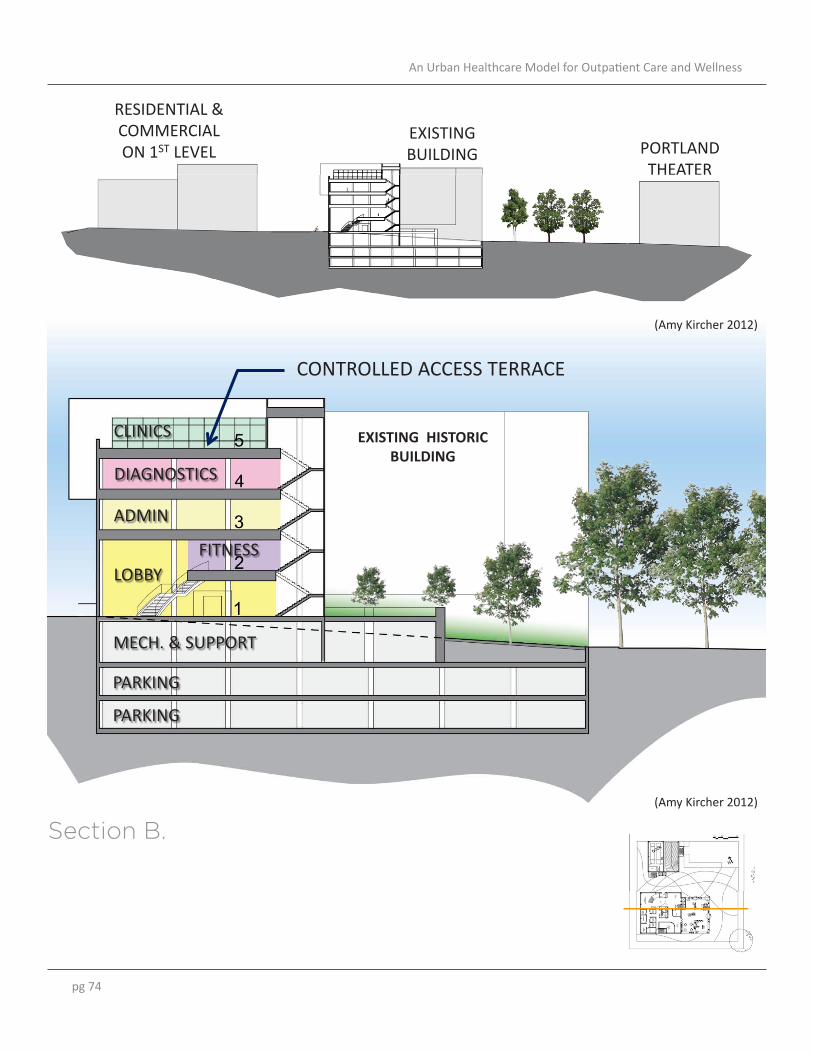
pg 74
An Urban Healthcare Model for Outpatient Care and Wellness
section a. program stacking
EXISTING HISTORIC BUILDING
CONTROLLED ACCESS TERRACE
FITNESS LOBBY
DIAGNOSTICS
ADMIN
CLINICS
MECH. & SUPPORT
PARKING
PARKING
EXISTING BUILDING
RESIDENTIAL & COMMERCIALON 1ST LEVEL PORTLAND
THEATERTHEATER
section a. city context
EXISTING BUILDING
RESIDENTIAL & COMMERCIALON 1ST LEVEL PORTLAND
THEATERTHEATER
section a. city context
Section B.
(Amy Kircher 2012)
(Amy Kircher 2012)

pg 75
Final Report November 2012
section b. user circulation
Well Patient
Sick Patient
Non Patient
User Group Circulation SickPatient
Well Patient
Non Patient
section b. user circulation
SickPatient
Well Patient
Non Patient
section b. user circulation
In this section, the three main user groups are illustrated to show how each “patient type” is integrated or separated from one another on the different levels of the building. The general concept is that the lower most levels of the facility are public and geared towards wellness and educational services. As one moves up the building it becomes more clinical towards the upper most levels. Staff and administration areas are mid level in the building to create a separation between clinical and public. While all three user groups have access to the first level, most of the amenities are geared towards the well patient and the non-patient. Services for sick patients are located higher in the building to create more privacy for this user group and create a separation between the clinical areas and the other areas of the building.
(Amy Kircher 2012)

pg 76
An Urban Healthcare Model for Outpatient Care and Wellness
Building designed to be a visual attraction and destination in the city. Goal is for this facility to be a community hub focused on health that integrates with other hubs from the Portland Plan. Façade design and orientation create unique views from the building from different users.
Pedestrian view of main entry. Architectural design creates different levels of transparency into the building.
(Amy Kircher 2012)
(Amy Kircher 2012)

pg 77
Final Report November 2012
Pedestrian view from the Portland Art Museum and theater district buildings. Façade designed to highlight building activities from pedestrian perspective.
View from mid-rise residential buildings. Shows main entry, service entry, and art installation on existing building done in collaboration with Portland Art Museum.
(Amy Kircher 2012)
(Amy Kircher 2012)
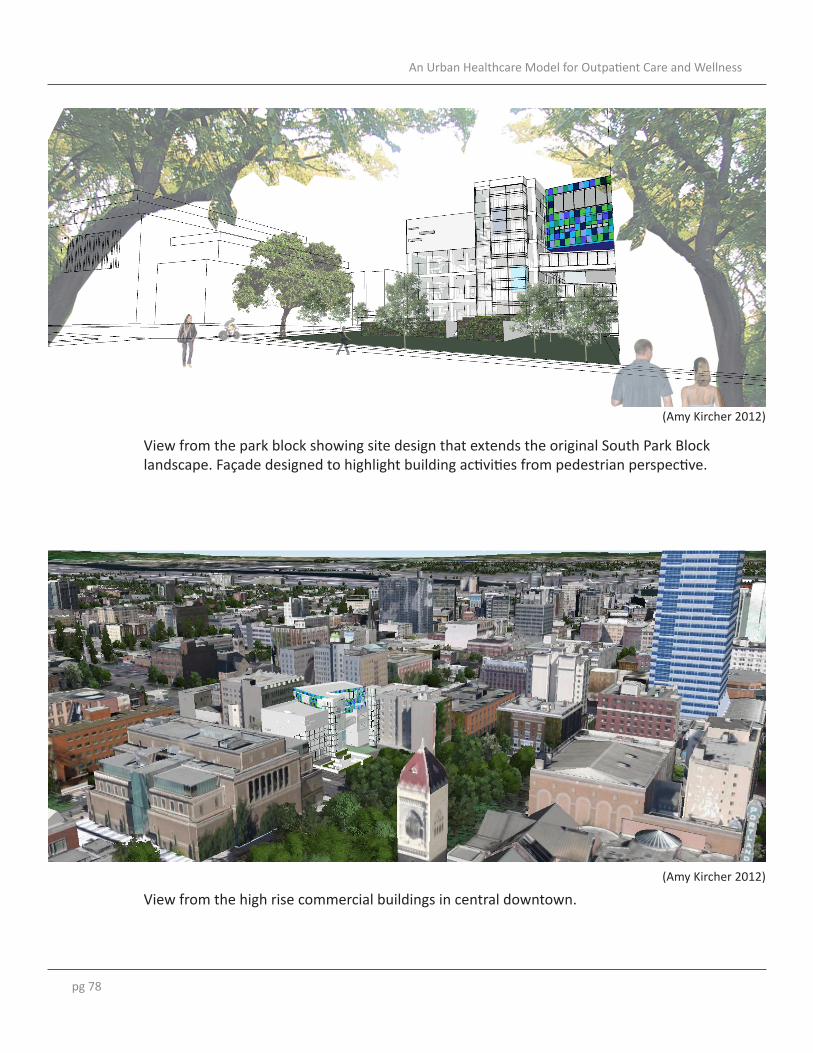
pg 78
An Urban Healthcare Model for Outpatient Care and Wellness
View from the park block showing site design that extends the original South Park Block landscape. Façade designed to highlight building activities from pedestrian perspective.
View from the high rise commercial buildings in central downtown. (Amy Kircher 2012)
(Amy Kircher 2012)

pg 79
Final Report November 2012
Conceptual rendering showing the characteristics of the lobby and public spaces. These spaces are design to be semi-open to one another to encourage exploration and have visual and physical transparency. The aesthetics incorporate color and bold graphic design for wayfindng purposes and to create an energetic environment.
Conceptual rendering showing the characteristics of the yoga and other meditative spaces. In this room, the morning sun will light the space, and the large windows frame views of the city skyline and park block. The cooler colors and use of wood on the floor and ceiling create a calm and meditative atmosphere.
(Amy Kircher 2012)
(Amy Kircher 2012)

pg 80
An Urban Healthcare Model for Outpatient Care and Wellness
Part Four

pg 81
Final Report November 2012
-Conclusions and Future Studies
Conclusions

pg 82
An Urban Healthcare Model for Outpatient Care and Wellness
Conclusions andFuture Studies
The United States has seen a rise of policy changes and debate regarding continuum of care and preventive care, and there is a great need for a wellness approach to health. Support from my professors and other knowledgeable professionals in the industry allowed me to explore this topic from not simply an organizational or policy standpoint but an architectural perspective. The effect of facility design on patient care and human needs is an important topic in the architecture profession and new approach to functional programming and space planning for healthcare facilities is needed. The incorporation of wellness and preventive care into an outpatient model is an approach worthy of continued exploration. There is the potential to greatly impact and advance the knowledge of the planning and design of outpatient and wellness healthcare environments through a variety of future studies and collaborations.
I believe that the outcomes of my proposed research study could potentially contribute to the way outpatient and wellness focused facilities are designed. I also believe the healthcare architecture profession will benefit from my analysis and observations of how different healthcare facilities relate to the city’s design and the impacts of a city’s urban fabric on ease of access to healthcare facilities.
The Tuttle Fellowship has been unique opportunity to learn about various new outpatient facilities emerging, and for me to reach a higher level of sophistication in my Master of Architecture final study project. The opportunity to study the connection of the healthcare facility to the urban environment will also have lasting impacts on my future as an architect and on how I design healthcare facilities.
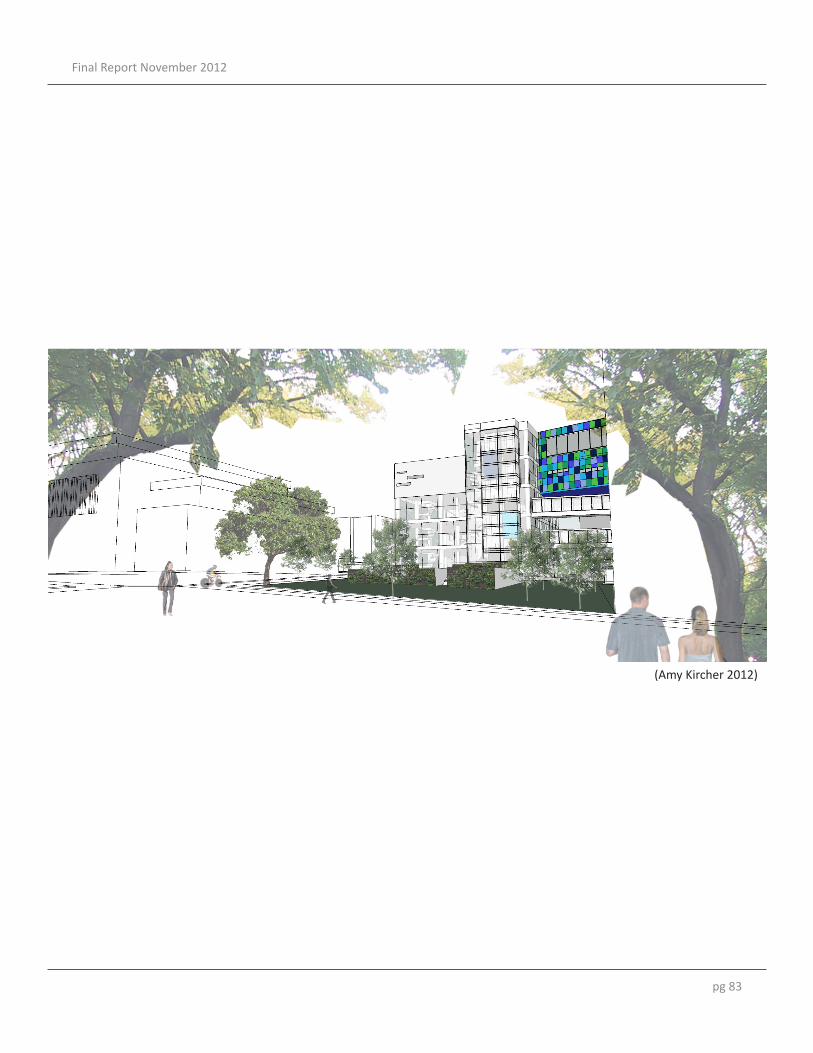
pg 83
Final Report November 2012
(Amy Kircher 2012)

pg 84
An Urban Healthcare Model for Outpatient Care and Wellness
Appendix

pg 85
Final Report November 2012
-References-Acknowledgments

pg 86
An Urban Healthcare Model for Outpatient Care and Wellness
ReferencesAlimoglu, M. K., & Donmez, L. (2005). Daylight Exposure and the Other Predictors of Burnout Among Nurses in a University Hospital. International Journal of Nursing Studies, 42(5), 549-555.
Allison, M. (2011). America’s Design and Health Initiative: An Important Value Proposition for Architects. Retrieved April 22, 2011, from http://www.aia.org/practicing/AIAB088657. Bentley, F. (2011). Ambulatory Facility of the Future: Rethinking Outpatient Strategy in the New Health Care Economy. Facility Planning Forum The Advisory Board Company.
Brownson, R., Baker, E., et. al. (2001). Environmental and Policy Determinants of Physical Activity in the United States. American Journal of Public Health. Vol 91, No. 12, 1995-2003
City of New York. (2010). Active Design Guidelines: Promoting Physical Activity and Health in Design. New York City: City of New York.
Cooper Marcus, C . & Barnes, M. (1999). Healing Gardens: Therapeutic Benefits and Design Recommendations. New York: John Wiley & Sons, 1999.
Downey, L. A., & Zun, L. S. (2008). Assessing adult health literacy in urban healthcare settings. Journal of the National Medical Association, 100(11), 1304-1304-8. Retrieved from http://lib-`ezproxy.tamu.edu:2048/login?url=http://search.proquest.com/docview/214046587?accountid=7082.
Fierce Healthcare. (2011). Fierce Healthcare: Daily News for Healthcare Executives. Retrieved April 1, 2011, from http://www.fiercehealthcare.com.
Figueiro, M. G., Rea, M. S., Stevens, R. G., Rea, A. C. (2002). Daylight and Productivity – A Possible Link to Circadian Regulation. The Lighting Research Office of the Electric Power Research Institute (2002), 185-193.
Frank, L., Engelke, P., & Schmid, T. (2003). Health and community design: the impact of the built environment on physical activity. (1st ed.). Washington, DC: Island Press.
Gerlach-Spriggs, N., Kaufman, R. & Warner Jr., S. (1998). Restorative Gardens: The Healing Landscape. New Haven, CT and London: Yale University Press.

pg 87
Final Report November 2012
HGA Architects. (2010). Whittier Clinic. Retrieved from http://hga.com/work/hennepin-county-medical-center. Hospital Compare. (2011). Retrieved April 18, 2011, from http://www.hospitalcompare.hhs.gov/.
Hoving, C., Visser, A., Mullen, P. D., & van den Borne, B. (2010). A history of patient education by health professionals in Europe and North America: From authority to shared decision making education. Patient Education and Counseling, 78(3), 275-281. doi: 10.1016/j.pec.2010.01.015.
Joseph, A. (2003). The Impact of Light on Outcomes in Healthcare Settings. The Center for Health Design. Kaiser Permanente. (2011). Kaiser Permanente Center for Total Health. Retrieved April 11, 2011, from http://www.centerfortotalhealth.org.
Kirksey Architecture. (2011). Tellepsen Family Downtown Ymca. Retrieved August 20, 2011, from http://www.kirksey.com/project/tellepsen_family_downtown_ymca.
Leather, P., Pygras, M., Beale, D., & Lawrence, C. (1998). Windows in the Workplace: Sunlight, View, and Occupational Behavior. Environment & Behavior, 30(6), 769-762.
Lee, C. & Moudon, A. (2008). Operational Neighbourhood Design and Physical Activity. Building Research & Information. 36(5), 395-411. Manus, C. D. (2011). A Prescription for a Healthier Nation. Architect: The AIA Magazine, April, 28.
Mayo Clinic. (2008). Dan Abraham Healthy Living Center. Retrieved March 30, 2011, from http://www.mayoclinic.org/intern-dahlc-rst/history.html. Mayo Clinic. (2011). Mayo Clinic Announces Life-Planning Services in Health and Wellness for Patients. Retrieved March 30, 2011, from http://www.mayoclinic.org/news2011-rst/6226.html. McCusky, J. F. (2008). Creating Engaging Environments in Rehabilitation. Topics in Stroke Rehabilitation, 15(2), 80-86.
Millard, B. (2011). Lightness of Being. Architect: The AIA Magazine, April 26-27. Murray, C. J. L., & Frenk, J. (2010). Ranking 37th — Measuring the Performance of the U.S. Health Care System. New England Journal of Medicine, 362(2), 98-99. doi: doi:10.1056/NEJMp0910064.
pg 88
An Urban Healthcare Model for Outpatient Care and Wellness
Nahrsted, W. (2004). Wellness: A New Perspective For Leisure Centers, Health Tourism, and Spas in Europe on the Global Health Market. In The Tourism and Leisure Industry: Shaping the Future, (pp. 181-198). New York City Commission. (2006). Planning for the Future: Capacity Needs in a Changing Healthcare System. New York City Commission on Health Care Facilities in the 21st Century.
Nicoll, G., & Zimring, C. (2009). Effect of innovative building design on physical activity. Journal of Public Health Policy, 30(S1), S111-S123.
Nicoll, G. & Zimring, C. (2009). Effect of innovative building design on physical activity. Journal of Public Health Policy, 30(S1), S111-S123.
Peek, C., Oftedahl, G. (2010). A Consensus Operational Definition of Patient-Centered Medical Home (PCMH): Also known as Health Care Home. University of Minnesota and the Institute for Clinical Systems Improvement.
Perkins & Will. (2008). Mill City Clinic. Retrieved from http://www.perkinswill.com/work/mill-city-clinic.html.
Rodiek, S. (2009). Outdoor Evaluation Tool. Access to Nature: Planning Outdoor Spaces for Aging.
Ulrich, R. S. (1999). Effects of Gardens on Healthcare Outcomes: Theory and Research. In Healing Gardens: Therapeutic Benefits and Design Recommendations. (pp. 27-85).
Ulrich, R. S. (1991). Effects of Interior Design on Wellness. Journal of Healthcare Interior Design, 97-109.
U.S. News. (2011). U.S. News Best Hospitals 2010-11. Retrieved April 15, 2011, from http://health.usnews.com/best-hospitals/rankings.
Zimring, C., Joseph, A., Nicoll, G., & Tsepas, S. (2005). Influences of Building Design and Site Design on Physical Activity: Research and Intervention Opportunities. American Journal of Preventive Medicine, 28(2S2), 186-193.

pg 89
Final Report November 2012
AcknowledgmentsA special thanks to…
The AIA Tuttle Fellowship Committee and The AIA Academy of Architecture for Health.
Steris for their generous sponsorship.
My Final Study Chair Prof. Kirk Hamilton and Committee Dr. Mardelle Shepley and Dr. Jon Rodiek for their guidance and support.
and to the many individuals and organizations who assisted me along the way:
Deborah Sweetland, Alejandro Iriarte, Freek de Bos, Heather Voorhaar, Karl Sonnenberg, Suanne Barton, Stephen Black, Tom Clark, David Frum, Ron Smith, Randal Brand, Michele Cohen Idoine, Ian Sinclair, Terry Montgomery, Alice Liang, Maggie Duplantis, Gary Oftedahl, Jon Hallberg, Chris Backous, Allison Schwab, Courtney Duke, Massachusetts General, Mayo Clinic and Center for Innovation, Methodist Hospital, Philips Powderhorn, City Mills Clinic, ICSI, Kaiser Permanente, Polyclinic, Virginia Mason, Wellspring Medical Center, and University Medical Center Groningen.