an overview of indian pharmaceutical...
TRANSCRIPT
1
AN OVERVIEW OF INDIAN PHARMACEUTICAL
INDUSTRY
The Indian Pharmaceutical industry is in the front rank of India’s science based industries
with wide ranging capabilities in the complex field of drug manufacture and technology.
Pharmaceutical Industry in India is one of the largest and most advanced among the
developing countries. The growth of the pharmaceutical industry in India is quite
phenomenal. Today the Indian Pharmaceutical industry is capable of meeting the country’s
demand for each and every drug. But with the development of pharmaceutical Industry,
pharmaceutical malpractices are also increasing. Pharmaceutical malpractices mean that a
drug company caused injury or death to a consumer by failing to act within the applicable
standard of care. The consumers have been exploited by the manufacturers and the traders.
The traders are dominating the market and the consumers are not united. Therefore, in such a
situation traders do not hesitate to indulge in various undesirable and immoral trade practices.
It is an undeniable fact that access to health care is one of the most basic needs and an
inviolable right of every human being. Today Pharmaceutical industry is forced to work in
an environment of stiff competition. The complexion of the pharmaceutical sector has thus
undergone a significant change in terms of trade and marketing practices. Pharmaceutical
companies found themselves in a market where the customer has more options than ever
before and firms while competing with one another adopt restrictive or unfair practices,
which are derogatory to the core of a competitive market. In the pursuit of profit making,
business failed to discharge social responsibilities of maintaining and charging fair prices,
supplying quality and standard goods and providing other services to the customer.
Adulterated stuffs and eatables poisoned by industrial pollution found their way into the
markets1.
Globally, the drug sector has been known for practices thwarting the spirit of
competition and regulation. Anti competitive system include price fixing abuse of
dominance, collusive agreements and tied selling2. Even practices such as kickbacks to
doctors and pharmacists may be deemed as unfair trade as they result in depriving patients of
the best possible prices. The primary effect of anticompetitive practices in the health sector
is that medicines and services are rendered costlier. Hospitals are an important part of the

2
health delivery system. But they are also known to exploit consumers, and enter into
agreements with drug manufacturers. Some drug companies offer incentives to doctors to
prescribe off label. All types of fraudulent products, unsafe or defective products, even
spurious drugs without proper regard for consumer health were pumped into the market.
Historically, Major pharmaceutical companies marketed their drug offering to patient
gatekeepers – physicians and health care professionals since the Food Drug and Alcohol
Administration (FDA) of USA prohibited advertising prescription drugs to consumers.
Companies used sales representatives to ‘detail’ doctors by educating them and promoting
prescription drugs. The companies also provided drug samples to the gatekeepers to
indirectly gain exposure to and trial by patients. In 1985 FDA legalized the marketing of
prescription drugs to consumers with the mandate that advertisement could not make false or
misleading claims and all side effects must be listed in detail with the products benefits.
Direct-to-consumers advertising of prescription drugs become more prominent in 1997 when
FDA issued less stringent guidelines, although FDA still prohibited misrepresentation or
false claims. But in order to gain more demand and attention of consumers, companies are
making advertisements with false claims and misleads. Doctors start selling the sample
medicines to the patients and companies start offering kickbacks to the doctors for giving
prescription of their drugs. Some other unfair trade practices are also prevailing in the market
like tied selling, attention deficit disorder (ADD), false advertisement, misrepresentation,
False offer or claims etc. these types of unfair and restrictive practices harm both customers
and economy. In this way pharmaceutical companies are adopting different unfair means to
increase the profits. For example an injection (Irinotecan salt based) used for treating cancer
is being sold in the market by a major pharmaceutical company for around Rs. 15000 when
the injection, made out of the same salt, is available under different brands for just Rs. 1500.
There are numerous cases like this where the patients are unaware of cheaper alternatives
with same salt. Officials in the government said that the companies, which sold higher
priced medicines offered a better share of profits for the chemists and retailers. Even if a
chemist offered a cheaper alternative with same salt, he would do so at the risk of losing his
license because the rules bind him to follow doctor’s prescription.

3
The protection of consumers from the undesirable, unethical or immoral trade
practices has both social and monetary benefits. As per the law, the consumer is to be
charged the minimum cost and while profits are the soul of the businesses it should not turn
into profiteering. Mahatma Gandhi had said, “There is enough in this world to meet every
man’s need but not enough in this world to satisfy every man’s greed. Display of wealth is
necessary for a man’s ego. But it is wrong to convert that ego into class struggle. Profit is
not a dirty word, but profiteering is.3”
NEED OF UNFAIR TRADE PRACTICES ACT
Unfair Trade Practices Act helps in protecting consumers from injuries caused by deceptive
trade practices, the remedies provided to redress such injuries are available only to business
entities and proprietors. Consumers who are injured by deceptive trade practices must avail
themselves of the remedies provided by unfair trade practices Act. Unfair Trade Practices
Act took on the role of a watchdog of consumer interest. In the new corporate and business
world today where there is cut throat competition, the business persons daringly use UTP to
edge over the other. Misleading and deceptive conduct is one of the most important
consumer parts of the Act. Unfair Trade Practices Act protects from five types of practices
which are regarded as unfair trade practices in certain situations. These practices are:
a) Misleading advertisements and false representations
b) Bargain sale
c) Offering gifts or prizes and conducting promotional contests
d) Supplying goods not adapting to product safety standards
e) Hording or destruction of goods, or refusal to sell the goods.
FIVE MAJOR FORCES OF DRIVING COMPETITION IN
THE PHARMACEUTICAL MARKET IN INDIA
1. Buyer Power: Over recent years, the hospital segment has experienced a reduced
share in market sales, with other sources such as pharmacies taking a larger share.
This reduces buyer power as pharmaceutical companies are supplying to different
4
sources. Many drugs are unavailable without prescription. Furthermore
pharmaceutical companies market their products largely through physicians, meaning
individual consumers have little control over what pharmaceuticals are at their
disposal. There are often multiple drug treatments available for a given medical
condition. This means that buyer power is reduced further as the manufacturer can
differentiate its product from others by demonstrating the genuine clinical benefits of
its branded and patented product. However, generic equivalents of branded drugs do
exist meaning that there is increased differentiation of prescription drugs, which
serves to increase buyer power. Additionally end users may be given a choice of
treatment medicine and so the buyer power is enhanced to some extent. Switching
costs can often be considerably high.
2. Supplier power: Main supplier to the pharmaceutical industry are manufacturers
who provide active pharmaceutical Ingredients(API). API’s are needed by
pharmaceutical companies in their development of drugs, as such the market player is
in a weaker position. Most large multinational pharmaceutical companies have major
investments in fine chemical manufacturing, providing them a degree of self-
sufficiency. However due to pharmaceutical companies requiring a wide range of
chemicals, power remains with the supplier. It is unlikely that suppliers would
forward integrate into the pharmaceutical market; however their capabilities in
chemical synthesis make them ideal candidates for forward integration into the
manufacture of generic drugs. Over recent years, larger pharmaceutical companies
have turned to produce their own chemicals in a bid to enhance profits. However
smaller companies lack the resources required to do this and remain reliant on API
manufacturers. APIs are supplied on a contractual basis. Pharmaceutical companies
are likely to risk high switching costs if they consider taking their business elsewhere.
This serves to increase supplier power further. In turn, pharmaceutical companies
employ sourcing managers to minimize costs in the purchase of APIs and mitigate
supplier power. The development of new therapeutic agents requires the sourcing of
newer APIs, for which chemical manufacturers can charge pharmaceutical companies
high prices. If the novel drug successfully reaches the market, the supplier of the API

5
can make a large amount of money. Supplier power with respect to the
pharmaceutical market is considered to be strong.
3. New Entrants: The cost of developing a novel prescription drug is in the
excess of millions. Vigorous and extensive clinical trials are required to satisfy the
safety protocols of regulatory bodies. A high level of proprietary knowledge is
required to compete successfully in this market, as established companies usually
keep their drug discovery processes very secretive. This can prove off putting to new
entrants. Additionally the process of developing a new drug is fraught with problems
and is a risk to financiers. Players may yield poor revenues due to leading
incumbents such as Cipla Ltd., GlaxoSmithKline Plc, Ranbaxy Laboratories Limited,
Piramal Healthcare(PHL) etc. dominates the market and the development of
substitute therapies, which are considered as a weak threat to prescription
pharmaceuticals. However patents for new drugs protect the interests of the
developer, allowing the recouping of development expenses, and ensuring
profitability. As well as this strong market growth is seen as enticing new entrants.
Recently, Asia has become vital in pharmaceutical outsourcing. Leading
international incumbents are processing their products in India over the European and
US markets.
4. Threats of substitutes: Generic substitutes of branded drugs exist in the
market. However there are very few viable substitutes for ethical pharmaceuticals
overall. Recently, there has been a growth in the popularity of alternative therapies
which prove cheaper than some drugs. The medical community heavily disputes the
benefits of these alternatives, claiming them to lack the rigorous clinical testing
required for all pharmaceutical products. Additionally, alternative therapies are
claimed not to target medical problems specifically unlike their pharmaceutical
counterpart. OTC medicines are threatened by alternative therapies more than
prescription medicines. It is the individual consumer who purchases alternative
therapies, whereas the price of most ethical drugs to the patient is heavily subsidized
by either the state or health insurers. It is these substitutes which are regarded as
more expensive.

6
5. Degree of Rivalry: The key players in the pharmaceutical market are usually
large multinational companies who own a high level of capital investment. Large
companies are likely to keep their leading position for this reason, as new entrants are
less likely to have the same degree of capital investment. The Indian market is
relatively fragmented with four major companies sharing 22% of the total market
value. Rivalry is intensified further by the high fixed and exit costs from suppliers.
The market is highly competitive for a number of reasons. Firstly the development
costs for a prescription drug are high. Secondly, there are often other drugs
competing for a market share of a given therapeutic area. Furthermore, there are no
switching costs for practitioners. These reasons mean that rivalry between key
players is high. Excellent market growth serves to ease rivalry to some extent. Key
players must invest in marketing and sales operations in order to maximize their
revenues. Overall, the pharmaceutical market displays a strong level of rivalry.
INDIAN PHARMACEUTICAL INDUSTRY
Medicines contribute enormously to the health of the nation. The discovery, development
and effective use of drugs have improved many people’s quality of life, reduced the need for
surgical intervention and the length of time spent in hospital and saved many lives. Over the
years pharmacy has grown in the form of pharmaceuticals sciences through research and
development processes. It is related to product as well as services. The various drugs
discovered and developed are its products and the healthcare it provides comes under the
category of services. Pharmacy involves all the stages that are associated with the drugs, i.e.
discovery, development, action, safety, formulation, use, quality control, packaging, storage,
marketing etc.
The Indian pharmaceutical industry is a successful, high-technology-based industry that has
witnessed consistent growth over the past three decades. Indian Pharmaceutical Industry has
an important role in promoting public health. The origin of the Indian pharmaceutical
Industry may be traced to the establishment of the Bengal Chemicals and Pharmaceutical
works, which exist today as one of 5 government owned drug manufacturers, in Calcutta in
1930.4 For the next 60 years, most of the drugs in India were imported by multinationals
7
either in fully formulated or bulk form. The government started to encourage the growth of
drug manufacturing by Indian companies in the early 1960s and with the patent Act in 1970,
enabled the Industry to become what it is today. This patent act removed composition
patents from food and drugs and though it kept process patents, these were shortened to a
period of five to seven years. The lack of patent protection made the Indian market
undesirable to the multinational companies that had dominated the market, and while they
streamed out, Indian companies started to take their places. They carved a niche in both the
Indian and world markets with their expertise in reverse engineering new processes for
manufacturing drugs at low costs. Although some of the larger companies have taken baby
steps towards drugs innovation, the industry as a whole has been following this business
model until the present.
CLASSIFICATION OF PHARMACEUTICAL INDUSTRY
The global pharmaceutical industry structure can be divided into two:
• Bulk drugs (20%) The bulk drug segment of the market has increased in the past decade at
around 20% annual growth rate.
• Formulations (80%) Production of formulations has increased by around 15% annually.
The Indian Pharmaceutical Industry is among the top five producers of bulk drugs in the
world. The largest firms account for the majority of the R& D investment in the industry and
hold the majority of the patents. A small number of multinational enterprises (MNEs)
dominate the global pharmaceutical industry; top twenty-five MNEs having accounted for
64.5 percent of the world (2003) Firms can be either in production of bulk drugs or
formulations or may manufacture both. Firms in to formulations may be further classified
into innovating firms and non- innovating firms. However, R&D is insignificant when
compared to MNEs. There are about 8174 bulk drug manufacturing units and 2389
formulations units spread across India. Total: 10563 units.
Statistics
The net worth of the industry is about 8 Billion Dollars with a growth rate of 8-9% PA. It
exports to nearly 212 countries.5 In 2002, over 20,000 registered drug manufacturers in India

8
sold $9 billion worth of formulations and bulk drugs. 85% of these formulations were sold in
India while over 60% of the bulk drugs were exported, mostly to the United States and
Russia. Most of the players in the market are small-to-medium enterprises; 250 of the largest
companies control 70% of the Indian market. Multinationals represent only 35% of the
market, down from 70% thirty years ago.
Most pharmaceutical companies operating in India, even the multinationals, employ Indians
almost exclusively from the lowest ranks to high level management. Mirroring the social
structure, firms are very hierarchical. Homegrown pharmaceuticals, like many other
businesses in India, are often a mix of public and private enterprises. Although many of these
companies are publicly owned, leadership passes from father to son and the founding family
holds a majority share.
In terms of the global market, India currently holds a modest 1-2% share, but it has been
growing at approximately 10% per year. India gained its foothold on the global scene with its
innovatively-engineered generic drugs and active pharmaceutical ingredients (API), and it is
now seeking to become a major player in outsourced clinical research as well as contract
manufacturing and research. There are 74 U.S. FDA-approved manufacturing facilities in
India, more than in any other country outside the U.S, and in 2005, almost 20% of all
Abbreviated New Drug Applications (ANDA) to the FDA are expected to be filed by Indian
companies. Growth in other fields notwithstanding, generics is still a large part of the picture.
The pharmaceutical market generated total revenue of $ 10838.7 million in 2009,
representing a compound annual growth rate of 11.3% for the period spanning 2005-2009.
Alimentary/metabolism sales proved the most profitable for the Indian pharmaceuticals
market in 2009, generating total revenues of $1498.8 million equivalent to 13.8% of the
market’s overall value. India accounts for 8.7% of the Asia-Pacific pharmaceuticals market’s
value. Japan leads the Asia-Pacific pharmaceuticals market, accounting for 53.8% of
market’s value.
9
GROWTH OF INDIAN PHARMACEUTICAL INDUSTRY
The Indian Pharmaceutical industry today is in the front rank of India’s science-based
industries with wide ranging capabilities in the complex field of drug manufacture and
technology. Pharmaceutical Industry in India is one of the largest and most advanced among
the developing countries. It provides employment to million and ensure that essential drugs
at affordable prices are available to the vast population of India. Indian Pharmaceutical
Industry has attained wide ranging capabilities in the complex field of drug manufacture and
technology. From simple pain killer to sophisticated antibiotics and complex cardiac
compounds, almost every type of drug is now made indigenously. A highly organized sector,
the Indian Pharmaceutical Industry is estimated to be worth $ 7.8 billion, growing at about 8
to 9 percent annually.
The growth of the pharmaceutical industry in India is quite phenomenal. From small
beginnings during the first post-independence decade, the industry has come a long way and
become very robust today. This industry is able to weather the impact of the three F’s –
Finance (inflation in the economy), Fuel price escalation and food shortage on the
pharmaceutical sector reflect robustness, as the prices are hardly hit despite the rapid fall of
the sensex. The pharmaceutical industry produces valuable life-saving drugs along with
numerous over-the-counter drugs such as paracetamol. The growth of an industry is highly
dependent on the regulatory environment. India had a product patent regime for all
inventions under the Patents and Designs Act 1911. However, in 1970, the government
introduced the new Patents Act, which excluded pharmaceuticals and agrochemical products
from eligibility for patents. This exclusion was introduced to break away India’s dependence
on imports for bulk drugs and formulations and provide for development of a self-reliant
indigenous pharmaceutical industry and the same helped in6-
1. Reduction in the manufacturing costs in terms of license fee.
2. Reduction in the costs involved in R&D.
3. Diffusion of technology and knowledge through reverse engineering.
10
The lack of protection for product patents in pharmaceuticals and agrochemicals had a
significant impact on the Indian pharmaceutical industry and resulted in the development of
considerable expertise in reverse engineering of drugs that are patentable as products
throughout the industrialized world but unprotect able in India. As a result of this, the Indian
pharmaceutical industry grew rapidly by developing cheaper versions of a number of drugs
patented for the domestic market and eventually moved aggressively into the international
market with generic drugs once the international patents expired. Till 1970, the growth of the
Indian pharmaceutical industry was very slow and after that government investment in the
pharmaceutical industry infused life into the domestic pharmaceutical sector. In addition, the
Patents Act provides a number of safeguards to prevent abuse of patent rights and provide
better access to drugs. The Indian Patents (Amendment) Act, 2005 introduced product
Patents in India and marked the beginning of a new patent regime aimed at protecting the
Intellectual property rights of patent holders. The Act was in fulfillment of India’s
Commitment to World Trade Organization (WTO) on matters relating to Agreement on
Trade Related Aspects of Intellectual Property Rights (TRIPS Agreement). Product patents
for pharmaceuticals, food and agro-chemicals were removed by the Act, allowing patents
only for production processes. Automatic licensing was put in place and the statutory terms
was shortened to seven years on drug patents. This led to the era of reverse engineering,
where new products were developed by a firm by changing their production processes.
During the last three decades, the private Indian pharmaceutical firms focused their efforts on
reverse engineering-oriented research and development, and this activity was very much
limited to applying known knowledge, or to making minor adjustments and modifications.
In addition, a few public sector laboratories operated in pharmaceutical research and
development under the Council of Scientific and Industrial Research (CSIR). Thus, the lag
period between the launch of a new product in its maiden market abroad and in India was
reduced in some cases to two years low, as a result of well-mastered production
technologies.7
Indian Pharmaceutical Industry plays an important role in the country to improve the quality
of life of the people by way of manufacturing host of drugs and pharmaceuticals for the
health of the citizens. The primary objective of the industry is to ensure the availability of
11
quality medicines for the masses including essential and life saving drugs and formulations at
reasonable prices. The foundation of the modern Indian Pharmaceutical Industry was laid in
the beginning of the current century when in 1901 a small factory known as M/s. Bengal
Chemical & Pharmaceutical Works was established in Calcutta. In the period immediately
after independence, the industry was totally dependent upon imports and by 1960s a number
of bulk drugs were produced in the country. During the period 1960 to 1970, the Indian
companies along with multinational companies laid the foundation of a truly modern
pharmaceutical industry.8
Advantage India:
India does have quite a few advantages, but the pharmaceutical industry needs a proper
marketing strategy to be put in place before banking on the government for concessions9.
The advantages India has are:
Cost – effective chemical synthesis: Implementation of value engineering in
chemical synthesis of various drug molecules drastically improves cost benefit. Fast
development track record
Provides bulk drugs: Provides a vast variety of bulk drugs and also enhances
exports of sophisticated bulk drugs.
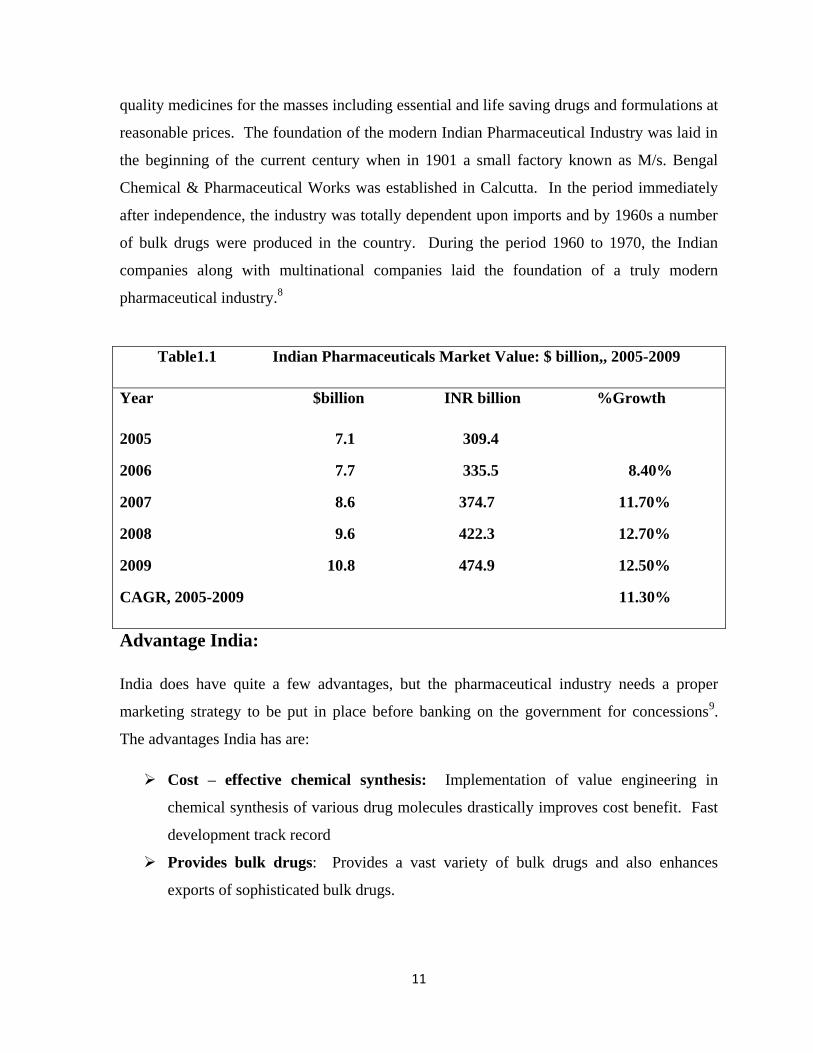
Table1.1 Indian Pharmaceuticals Market Value: $ billion,, 2005-2009
Year $billion INR billion %Growth
2005 7.1 309.4
2006 7.7 335.5 8.40%
2007 8.6 374.7 11.70%
2008 9.6 422.3 12.70%
2009 10.8 474.9 12.50%
CAGR, 2005-2009 11.30%

12
Competent workforce: India has a pool of easily available professional expertise
with high managerial and technical competence and these professionals are proficient
in English and other international languages, which facilitates international trading.
Legal and financial framework: A successful 60-year-old democracy of India
supports a strong legal framework and financial markets. Established international
industry and business s community also provide development framework.
Globalization: India has a free market economy and supports globalization.
Consolidation: India is now generating great opportunities from international
pharmaceutical industries.
Above all India has a huge population (16% of the world’s population), which is really in
need of good health. The prescription audit revealed the following information on the types
and category of drugs being prescribed generic(50.57%), branded (49.43%) and fixed dose
combination (18.27%) antibiotics (22.76%), analgesics(21.76%), anti-histaminies (12.56%),
drugs for gastro intestinal tract diseases (9.47%) steroids (3.57%) and drug for
cardiovascular diseases (3.16%) were prescribed. Doses were mentioned correctly for
19.28% of the antibiotics prescribed.10
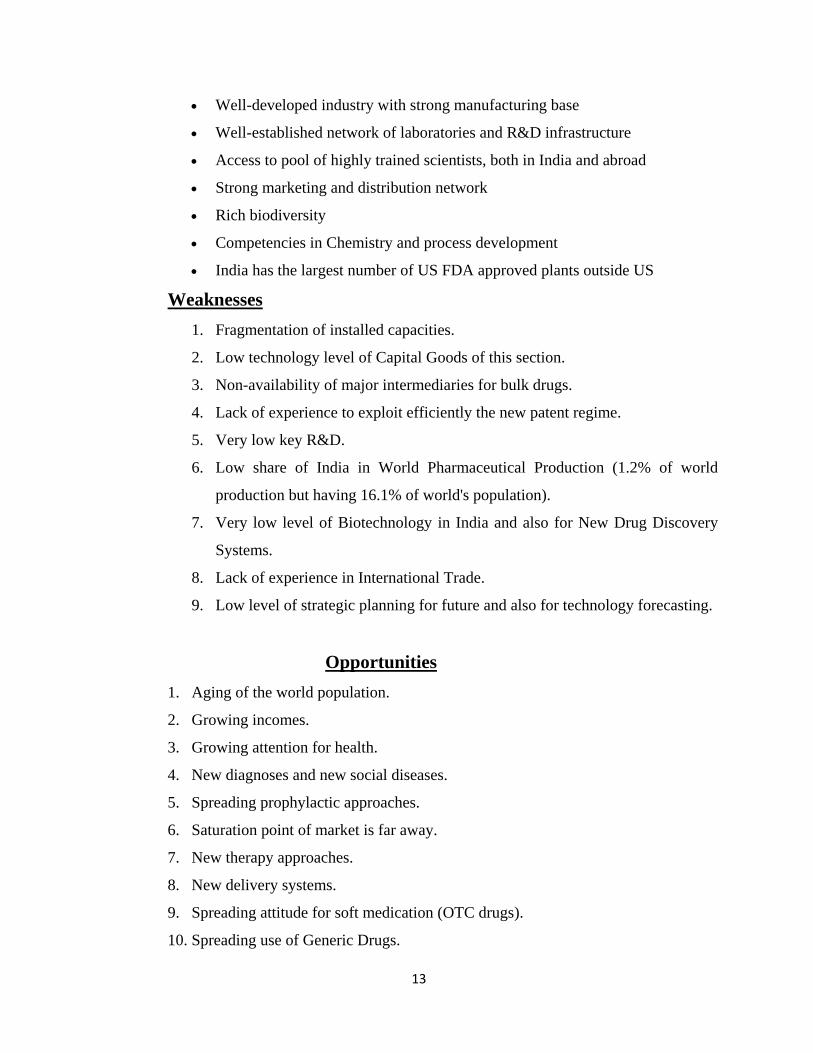
SWOT ANALYSIS11
Strengths
Cost Competitiveness
Table No:1.2 Category – wise sale of Pharmaceutical Products in India (By
value)
Category % Sales
Anti-infectives 18
Alimentary/metabolism 11
Cardiovascular 10
Respiratory 9
Central Nervous System 5
Others 47
Total 100
13
Well-developed industry with strong manufacturing base
Well-established network of laboratories and R&D infrastructure
Access to pool of highly trained scientists, both in India and abroad
Strong marketing and distribution network
Rich biodiversity
Competencies in Chemistry and process development
India has the largest number of US FDA approved plants outside US
Weaknesses
1. Fragmentation of installed capacities.
2. Low technology level of Capital Goods of this section.
3. Non-availability of major intermediaries for bulk drugs.
4. Lack of experience to exploit efficiently the new patent regime.
5. Very low key R&D.
6. Low share of India in World Pharmaceutical Production (1.2% of world
production but having 16.1% of world's population).
7. Very low level of Biotechnology in India and also for New Drug Discovery
Systems.
8. Lack of experience in International Trade.
9. Low level of strategic planning for future and also for technology forecasting.
Opportunities
1. Aging of the world population.
2. Growing incomes.
3. Growing attention for health.
4. New diagnoses and new social diseases.
5. Spreading prophylactic approaches.
6. Saturation point of market is far away.
7. New therapy approaches.
8. New delivery systems.
9. Spreading attitude for soft medication (OTC drugs).
10. Spreading use of Generic Drugs.
14
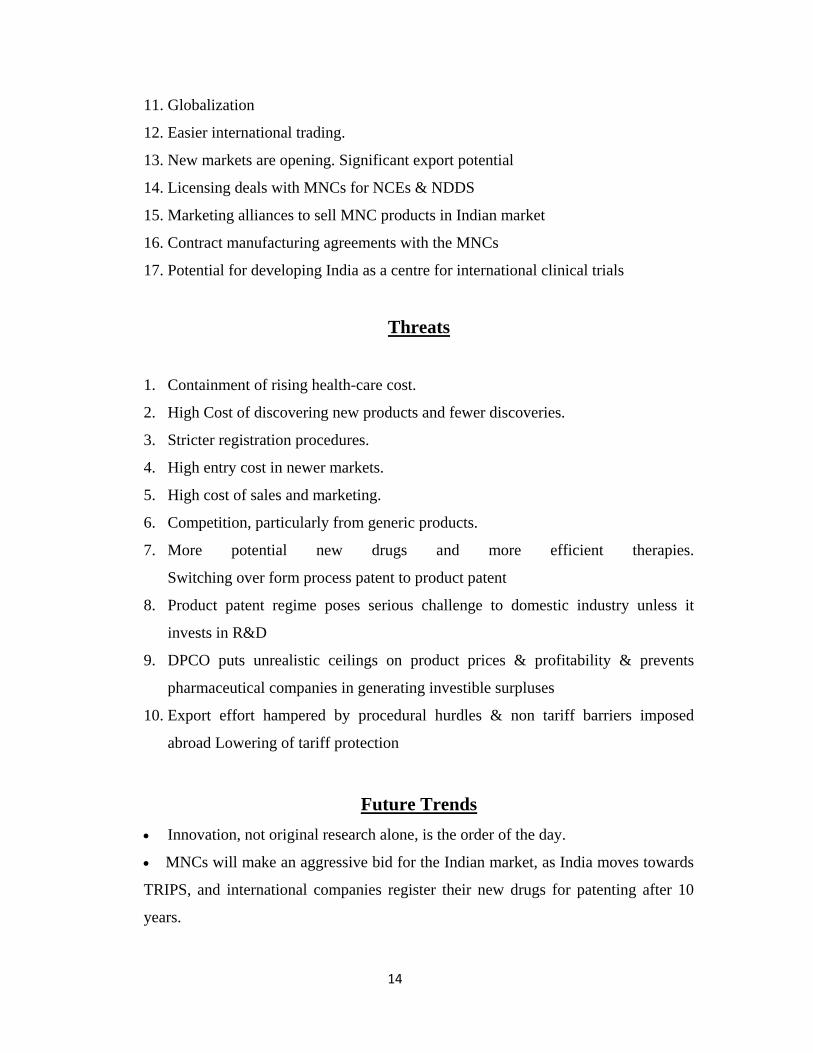
11. Globalization
12. Easier international trading.
13. New markets are opening. Significant export potential
14. Licensing deals with MNCs for NCEs & NDDS
15. Marketing alliances to sell MNC products in Indian market
16. Contract manufacturing agreements with the MNCs
17. Potential for developing India as a centre for international clinical trials
Threats
1. Containment of rising health-care cost.
2. High Cost of discovering new products and fewer discoveries.
3. Stricter registration procedures.
4. High entry cost in newer markets.
5. High cost of sales and marketing.
6. Competition, particularly from generic products.
7. More potential new drugs and more efficient therapies.
Switching over form process patent to product patent
8. Product patent regime poses serious challenge to domestic industry unless it
invests in R&D
9. DPCO puts unrealistic ceilings on product prices & profitability & prevents
pharmaceutical companies in generating investible surpluses
10. Export effort hampered by procedural hurdles & non tariff barriers imposed
abroad Lowering of tariff protection
Future Trends
Innovation, not original research alone, is the order of the day.
MNCs will make an aggressive bid for the Indian market, as India moves towards
TRIPS, and international companies register their new drugs for patenting after 10
years.

15
Smaller companies, which had so far benefited from the protective regime, may
be forced to become contracting units, or close shop.
Generics will have a huge demand.
Increasing R&D costs will lead to more consolidation among international
companies. Within 5 years, the top ten pharmaceutical companies will control over
60% of the world market.
International companies could set up their own R&D labs in India and develop
drugs for tropical diseases.
Innovations in R&D process such as genomics and combinatorial chemistry.
Indian pharmaceutical companies are expected to move up the value chain from
merely being reverse engineers to developers of proprietary products in the US
market.
10 MAJOR INDIAN DRUG COMPANIES
1) Dr. Reddy’s Laboratories Ltd.
2) Ranbaxy Laboratories Ltd.
3) Lupin Ltd.
4) Sun Pharmaceutical industries Ltd.
5) Cipla Ltd.
6) Orchid Chemicals & Pharmaceuticals Ltd.
7) Nicholas Piramal India Ltd.
8) Wockhardt Ltd.
9) IPCA Laboratories Limited
10) Cadila Healthcare Limited
1) Dr. Reddy’s Laboratories Ltd.: Dr. Reddy Laboratories was incorporated in
India by Dr. K. Anil in 1984. The company went public in 1985 was listed on the Indian
Stock Exchange in 1986. Dr. Reddy’s Laboratories is a global pharmaceutical company.
The company produces and distributes finished dosage forms, active ingredients and
intermediates and biotechnology products. It also conducts research in the areas of cancer,
16
diabetes, cardiovascular, inflammation and bacterial infection. The company primarily
operates in India, the US, Europe and Russia. It is headquartered in Hyderabad, India and
employs around 11228 people. It was listed on the New York Stock Exchange in 2001. Dr.
Reddy Laboratories specializes in the production of generic and branded drugs. The
company’s key products and services are:
PRODUCTS
Active pharma ingredients
Custom pharma Services
Generic biopharmaceuticals
Generics
New chemical entities and differentiated formulations
SERVICES
Custom chemical Services
Drug Research and development Services
The company recorded revenues of $ 8727 million in the Fiscal year ended Mar. 2009, an
increase of 20.1% over 2008.
2) Ranbaxy Laboratories Ltd.:
Ranbaxy company was incorporated in 1961. Ranbaxy was registered as private sector
company in 1973 and start a multi purpose chemical plant for manufacturing APIs at Mohali
in India. In 1985 Ranbaxy research foundation was established. Ranbaxy is the largest
generic pharmaceutical company in India. The company’s operations are divided into two
business segments: dosage forms and APIs. The dosage forms produced by the company
include a range of prescription and non- prescription drugs. The division places a particular
emphasis on anti-infective and anti bacterial. API division has a portfolio of over 50
products covering a wide therapeutic range such as anti infective, anti ulcer ants, anti
diabetics etc. the other products includes therapeutics for orthopedics, pain management,
17
nutritional, multivitamins, central nervous system disorders etc. Ranbaxy today has global
footprint in 46 countries, world-class manufacturing facilities in 7 countries and serves
customers in over 125 countries. It is headquartered in Gurgaon.
For the year 2009, the company recorded Global sales of US $ 1519 mn. The company has a
balanced mix of revenues from emerging and developed markets that contribute 54% and
39% respectively. In 2009, North America, the company’s largest market contributed sales
of US $ 397 Mn, followed by Europe garnering US $ 269 Mn and Asia clocking sales of
around US $ 441 Mn.
3) Lupin Ltd.:
Lupin Pharmaceuticals, Inc. is the U.S. wholly owned subsidiary of Lupin Limited, which is
among the top six pharmaceutical companies in India. Through our sales and marketing
headquarters in Baltimore, MD, Lupin Pharmaceuticals, Inc. is dedicated to deliver high-
quality, branded and generic medications trusted by healthcare professionals and patients
across geographies.
Lupin Limited, headquartered in Mumbai, India, is strongly research focused. It has a
program for developing New Chemical Entities. The company has a state-of-the-art R&D
center in Pune and is a leading global player in Anti-TB, Cephalosporins (anti-infectives) and
Cardiovascular drugs (ACE-inhibitors and cholestrol reducing agents) and has a notable
presence in the areas of diabetes, anti-inflammatory and respiratory therapy.
4) Sun Pharmaceutical industries Ltd.
Sun Pharma began in 1983 with just 5 products to treat psychiatry ailments. Sales were
initially limited to 2 states - West Bengal and Bihar. Sales were rolled out nationally in 1985.
Products that are used in cardiology were introduced in 1987, and Monotrate, one of the first
products launched at that time has since become one of the largest selling products.
Important products in Cardiology were then added; several of these were introduced for the
first time in India. Realizing the fact that research is a critical growth driver, we established
research center SPARC in 1993 and this created a base of strong product and process
18
development skills. Sun Pharma was listed on the main stock exchanges in India in 1994;
first API manufacturing plant was built in Panoli in 1995, for access to high quality actives
ahead of competition, and to tap the vast international opportunity for specialty APIs.
The tally at the end of 2008:
17 manufacturing plants in 3 continents
8000 employees
World class research centers
Brand selling in markets worldwide
A growing presence in the US generic market
Company makes specialty pharmaceuticals and active pharmaceutical ingredients. Our
brands are prescribed in chronic therapy areas like cardiology, psychiatry, neurology,
gastroenterology, diabetology and respiratory and dermatology.
5) Cipla Ltd.: Khwaja Abdul Hamied, the founder of Cipla. In 1935, he set up The
Chemical, Industrial & Pharmaceutical Laboratories, which came to be popularly known as
Cipla. He gave the company all his patent and proprietary formulas for several drugs and
medicines, without charging any royalty. On August 17, 1935, Cipla was registered as a
public limited company with an authorised capital of Rs 6 lakhs.
The search for suitable premises ended at 289, Bellasis Road (the present corporate office)
where a small bungalow with a few rooms was taken on lease for 20 years for Rs 350 a
month.
Cipla was officially opened on September 22, 1937 when the first products were ready for
the market. The Sunday Standard wrote: "The birth of Cipla which was launched into the
world by Dr K A Hamied will be a red letter day in the annals of Bombay Industries. The
first city in India can now boast of a concern, which will supersede all existing firms in the
magnitude of its operations. India has lagged behind in the march of science but she is now
awakening from her lethargy. The new company has mapped out an ambitious programme

19
and with intelligent direction and skillful production bids fair to establish a great reputation
in the East. "
6) Orchid Chemicals & Pharmaceuticals Ltd.:
Orchid Chemicals & Pharmaceuticals Ltd (Orchid) was established in 1992 as a 100%
Export Oriented Unit (EOU). Commencing operations in 1994, Orchid has achieved amazing
and consistent growth, quantitatively and qualitatively to emerge among the Top-15
companies in the Indian pharmaceutical industry in a short span of fifteen years of
operations. Orchid employs over 4000 people, of which over 700 are scientists, technologists
and other professionals.
Orchid's growth and positioning in the global pharmaceutical industry are indeed distinctive.
A robust leadership position in the antibiotics space, a core competence in oral and sterile
manufacturing, a broad-based multi-therapeutic coverage and an end-to-end connectivity
over the pharmaceutical value chain, from discovery to delivery, have positioned Orchid
uniquely.
Orchid has two manufacturing sites for APIs (at Alathur near Chennai and at Aurangabad,
near Mumbai) and three manufacturing sites for Dosage forms (at Irungattukottai and Alathur
in Chennai), besides a world-class R&D centre (at Sholinganallur, Chennai). Orchid’s
facilities are state-of-the-art and have several international regulatory approvals, including
the US FDA and UK MHRA. Orchid’s API facilities are ISO certified for their quality,
environmental management and operational health and safety systems. Orchid has a Joint
Venture in China for manufacturing sterile APIs.
Orchid’s scientific and technical strengths have made it a partner of choice for several
multinational corporations. Orchid has long-term exclusive marketing alliances with reputed
global companies for distribution of its products in the advanced markets.
20
7) Nicholas Piramal India Ltd.:
Piramal Healthcare (PHL) (formerly Nicholas Piramal India) was incorporated in 1947,
under the name Indian Schering; Later changing to Nicholas Laboratories India in 1979. The
name of the company changed to Nicholas Piramal India, in 1992. In May 2008, the
company again changed its name to Piramal Health care Limited. PHL manufactures
antibiotics, nutritionals products and general medicines under the brands such as phensedyl,
Haemaccel, stemetil, Tixlix, Ismo etc. Piramal Health care primarily operated in India,
headquarted in Mumbai. The company’s business operations are divided into pharmaceutical
business and other business. Piramal Health care ltd.’s pharmaceutical business segment
consists of the manufacture and trading of bulk durgs and formulations. It manufactures
creams and powder, tablets, capsules, liquids, ointments, bulk drugs and intermediates.
PHL and Minrad, a provider of generic inhalation anesthetics signed a definitive merger and
agreement fro PHL to acquire Minrad in Dec 2009. Piramal Health care generated revenue of
$ 750 million in the financial year (FY) ended March 2009, an increase of 14.2% over FY
2008. The company’s net income totaled $ 72.2 million in FY 2009, a decrease of 5.3% over
FY 2008. India accounted for 59.9% of the total revenue generated I FY 2009. Revenues
from India reached $ 449.8 million in FY 2009, an increase of 20.9% over 2008.
8) Wockhardt Ltd.
Wockhardt is a global, pharmaceutical and biotechnology company that has grown by
leveraging two powerful trends impacting the world of medicine - globalization and
biotechnology.
The Company has a market capitalization of over US$ 1 billion and an annual turnover of
US$ 650 million. Wockhardt’s pace of growth and momentum permeates every mindset,
system and technology within the organization.
Wockhardt today, is distinguished by a strong and growing presence in the world’s leading
markets, with more than 65% of its revenue coming from Europe and the United States.
Wockhardt’s market presence covers formulations, biopharmaceuticals, nutrition products,
21
vaccines and active pharmaceutical ingredients (APIs). The Company has its headquarters in
India, and has 14 manufacturing plants in India, UK, Ireland, France and US Subsidiaries in
US, UK, Ireland and France Marketing offices in Africa, Russia, Central and South East
Asia.
Wockhardt has a strong track record in acquisition management, with five successful
acquisitions in the European market. These acquisitions have strengthened Wockhardt’s
position in the high-potential markets of Europe, and have expanded the global reach of the
organisation.
Wockhardt Advantage
Wockhardt’s manufacturing facilities in India, UK, Ireland, France and US have the approval
of major regulatory bodies, including US FDA and UK's MHRA, with capabilities for both
Finished Dosage Formulations and APIs. The output includes
Steriles (Injectables)
Biopharmaceuticals
Orals (Tablets & Liquids)
Topicals (Creams & Ointments).
22
Wockhardt is a partner of choice for manufacturing, having entered into manufacturing
alliances with leading pharmaceutical and biotechnology majors, including
Astra Zeneca
Aventis
Schering-Plough
Cell Therapeutics
AFT, New Zealand
Lab Aguettant
Amylin
Eisai
LSI, UK
Ebewe, Austria
A key growth driver at Wockhardt is its state-of-the-art, multi-disciplinary research
capability backed by a team of 500 skilled scientists. Consistent efforts have resulted in six
breakthrough biotechnology products, 750+ patent filings and a pipeline of promising new
molecules.
Wockhardt’s strategies are aligned towards being a significant player in the emerging global
biopharmaceuticals market. In order to achieve this goal, the company has set up the
Wockhardt Biotech Park, India’s largest biopharmaceuticals complex, with six dedicated
plants built to international standards.
9) IPCA Laboratories Limited
One of the first modern pharma factory of yesteryears was commissioned by Ipca at
Mumbai in 1969. The company was originally promoted by a group of medical
professionals and businessmen and was incorporated as 'The Indian Pharmaceutical
Combine Association Limited.' in October 1949. Ipca is a fully integrated, rapidly
growing Indian pharmaceutical company with a strong thrust on exports. Ipca's APIs and

23
Formulations produced at world class manufacturing facilities are approved by leading
drug regulatory authorities including the US-Food and Drug Administration (FDA), UK-
Medicines and Healthcare products Regulatory Agency (MHRA), South Africa-Medicines
Control Council (MCC), Brazil-Brazilian National Health Vigilance Agency (ANVISA)
and Australia-Therapeutic Goods Administration (TGA). With operations in over 100
countries, exports account for over 52% of the company's income.
Forbes, a leading US business magazine, selected Ipca in 2003 among its top 200
successful, rising companies outside USA, with sales under USD 1 Billion. Over 19,000
companies were considered by Forbes, and of the 18 companies from India that figured in
this list, only four were from the 'Indian Pharmaceutical Sector'. Ipca happens to be one of
them. Subsequently, Ipca was selected by FORBES in this prestigious list for two
consecutive years; 2004 and 2005.
From a modest income of Rs. 0.54 crores in 1975-76, the net income has soared to Rs.
753.30 crores in 2005-06 with exports accounting for Rs. 401.83 crores. The net profit for
the year ending 31st March, 2006 stood at Rs. 63.98 crores. Formulations constitute 67
percent of the total income for 2005-06. Today, Ipca is one of the biggest manufacturers
in the world of APIs Atenolol (Antihypertensive), Chloroquine Phosphate (Antimalarial),
Furosemide (Diuretic) and Pyrantel Salts (Anthelmintic) right from the basic stage. Ipca is
also one of the largest suppliers of these APIs and their intermediates world over.
10) Cadila Healthcare Limited:
'Cadila Healthcare' is an Indian pharmaceutical company head quartered at Ahmedabad in
Gujarat state of western India. The company is the fifth largest pharmaceutical company in
India, with US$290m in turnover in 2004. It is a significant manufacturer of generic drugs.
Cadila Pharma have developed a drug named Roserin which has reduced the cost of curing
TB by 33%. Cadila Laboratories was founded in 1952 by Ramanbhai Patel (1925-2001),
formerly a lecturer in the L.M. College of Pharmacy, and his business partner Shri
Indravadan Modi. The company evolved over the next four decades into one of India's
established pharmaceutical companies.
24
STEPS REQUIRED TO BOOST THE COMPETITIVENESS OF
THE PHARMA -INDUSTRY
• Extension of deduction of 150% of R&D expenses. This would encourage more
and more companies to invest in R&D. The government has earmarked 150 crores for R&D.
This is just not enough. It should be augmented to at least 2000 crores.
• To rationalize Drug Price Control Order (DPCO). The objective of the price
control was to ensure adequate availability of quality medicines at affordable prices. The
product patent regime will make it obligatory for Indian companies to compete in R&D if
they want to survive. Similarly, WTO led global trading system will result in import tariffs
coming down. For Indian companies to compete with cheap imports, they will have to invest
in cost effective technology and processes. Therefore, it is imperative that the pharma
industry has surplus for investment. In this context, a liberalized price control regime
becomes more important.
• An academic –industrial relationship can be further explored, on the lines of
the US model, where the universities are the sites of innovation and the industry
commercializes the product. The universities are permitted to own the Intellectual Property
Rights (IPR) and get a share of the profits. Academic institutions will then become the
engines of entrepreneurship. This also requires setting up of greater number of centers of
academic excellence throughout India in different states, so that people from across the
country can avail of such education and make their contributions without feeling the need to
look beyond India for achieving academic excellence.
• Income tax exemptions should be given on clinical trials and contract
research done outside the company and abroad. This is because India is seen as
emerging as a major center for outsourcing of clinical trials for the Pharmaceutical MNCs.
• The problem of spurious drugs has to be tackled. The procedure for
procurement of licence should be made more stringent, including extensive disclosure of
detailed personal, financial and business information and a thorough background check.

25
There is a strong need to strengthen and streamline the Central and State Drug Control
Organizations. State drug controllers should take measures like setting up of separate
intelligence-cum-legal machinery with police assistance. Faking should be made non-bailable
and cognizable offence and the prosecution should be instituted by any police or Central
Bureau of Investigation officer not less than the rank of a sub-inspector (instead of an
inspector in the extant provision). Most of the cases relating to spurious drugs remain
undecided for years. Hence there is a strong need for setting up separate courts for speedy
trials of such offences. The case should be tried by the court of the rank of a Session Judge or
above whereas the extant provision provides for a trial by a metropolitan magistrate or a first
class judicial magistrate or above. Each state should set up accredited testing laboratories
that are well equipped and adequately staffed. The staff should be trained well for drawing
samples for test and monitoring the quality of drugs and cosmetics moving in the State. It is
most important and essential to have training programmes for technical staff of central and
state drug control laboratories and private testing laboratories as it is based on the report of
these testing laboratories that a manufacturer releases his product or otherwise. Legal action
against the manufacturer is likely to be taken on the basis of the test report given by a
government analyst.
• India should exploit its know-how in herbal medicines. Since these medicines
do not come under the purview of the TRIPS regime and the research in new chemical
entities involves millions of dollars of investment, the Indian companies should engage in
R&D in herbal medicine. The companies should try to exploit the Indian traditional
knowledge in ayurveda and herbal cures and file as many patents for herbal medicine as they
can. For this the government should set up R&D laboratories undertaking research
exclusively in the area of herbal medicines and support the companies in their research and
patent filing.
• The government should encourage setting up of USFDA-compliant plants
by providing tax holidays for a specified period (as given in regions like
Baddi), so that the Indian companies can exploit the opportunity arising out of patented
drugs and take up marketing of generics in the developed countries like USA.

26
SIGNIFICANCE OF THE STUDY
According to the World Bank “Competition” is “a situation in a market in which firms or
sellers independently strive for the buyers” patronage in order to achieve a particular
business objective for example profits, sales or market share.” Sometimes firms while
competing with one another, adopt restrictive or unfair practices, which are derogatory to the
core of a competitive market.
Today unfair trade practices are increasing day by day. The provisions pertaining to unfair
trade practices are applicable to any person, trader, business, or industry etc. excepting to
certain undertakings or trade associations. These include: 1) any undertaking owned or
controlled by a Government company; 2) any undertaking owned or controlled by the
Government Company; 3) any undertaking owned or controlled by a corporation (not being
a company) established by or under any central, provincial or State Act; 4) any trade union
or other association of workmen or employees formed for their own reasonable protection as
such workmen or employees; 5) any undertaking engaged in any industry the management
of which has been taken over by any person or body of persons in pursuance of any
authorization made by the central Government under any law for the time being in force; 6)
any undertaking owned by a co-operative society formed and registered under any central,
provincial or state Act relating to co-operative societies; and 7) any financial institution.
This research highlights the unfair trade practices done in the pharmaceutical sector and also
highlights the steps that should be taken to remove the unfair trade practices.
SCOPE OF THE STUDY
To achieve the above objectives this study a set of questions were asked from Doctors,
Patients and Wholesalers & retailers of different pharmaceutical companies. In this
Researcher has found what type of unfair trade practices are conducted in Pharmaceutical
sector in India. The study covers data over the period ranging from 1998-99 to 2008-09.
However, in some of the cases where the secondary data for those years could not be made
available, the range of period has been shifted.

27
CONTRIBUTION OF THE STUDY
The finding of the present research endeavor will be of interest to pharmaceutical companies,
academicians, managers of pharmaceutical companies, distribution channels, doctors and
customers. An attempt has been made to add to the knowledge about what type of unfair
trade practices are there in present competitive scenario. This study also checks the
awareness of the customers towards these practices. This study will tell the customers how
they are cheated in the market and what steps can be taken by them so that they don’t let
others to cheat them. This study will throw light on the process of filing complain under
Unfair Trade Practices Act.
LIMITATIONS OF THE STUDY
The present study is made to analyze Unfair Trade Practices in Pharmaceutical Industry.
Lack of relevant research work special on Unfair Trade Practices in Pharmaceutical Industry
has been the greatest limitation of the study as this absence created problems in collecting
qualitative information pertaining to various areas of Unfair Trade Practices.
It is important to highlight the limitations of a work especially in case of a research. The
limitations help us to understand and appreciate the work in proper perspective.
The research work has been completed under the following other main limitations:
(i) For the individual researcher certainly some constraints and restraint of time money
and sufficient authority to enquire about information.
(ii) Techniques used in the study are subject to their own limitation, which might have
affected the finding of the study.
(iii) In the collection of first hand information some respondents tried to conceal the
actual facts regarding unfair trade practices followed by them.
(iv) The non-availability of detailed operational data from the individual branch has been
greatest limitation to the present study.
(v) There is no free access to the records; most of the information has been taken to be
true on the basis of the questionnaire.
28
(vi) Self-structured questionnaires have own limitation because such type of
questionnaires never used in previous research.
(vii) The present study is a study of sample. Alternatively, the complete universe
would have been studied. This has not been done because of two reasons.
First, it was not possible to study the entire universe with the limited resources and
time available at hand. Secondly, it is well established fact that the study of universe
and representative sample would provide similar results. It is in this background that
a sample study was opted. It is hoped that the results obtained would be appropriate
for the strata studied as well as the universe.
Of course, every possible effort has been made to achieve the goal of the present
study. Despite these limitations, researcher has tried to find out the significant conclusions on
the subject to the study.
29
REFERENCES
1) Chaudhary Harish Chandra, Consumerism and consumer Protection: A Paper presented
at all India Seminar on Government and Business Environment in India at Jaipur
(Rajasthan)
2) “Dealing with anti-competitive practices in the Indian pharmaceuticals and the health
delivery sector”, “CUTS C-CISR” No. 5/2008
3) http://www.blogandearn.in/blogs/unfair-and-restrictiver-trade-practices-by
Yaduvanshi1974
4) http://en.wikipedia.org/wiki/Pharmaceuticals_in_India
5) M S Nair, India: Product patent regime & Pharmaceutical industry in India- The
Challenges ahead, LEX ORBIS, Jan 2007, 58-65.
6) ZafarMirza, WTO/TRIPs, Pharmaceuticals and Health: Impacts and strategies, The
Society for International Development, SAGE Publications.
7) Gester Richard, “The phenomenal Growth of pharma Industries in India”, Marketing
mastermind, September 2008.
8) “Pharmaceutical Industry in India”, iNDExTB-Industrial Extention Bureau (A
Government of GujratOrganisation)
9) http://www.pharmaceutical-drug-manufacturers.com/pharmaceutical-industry/
10) Research on Rational drug use in India: A Glimpse; Delhi Society for promotion of
Rational use of drugs & India-WHO essential drug programme, study conducted at
Punjab university Health centre (PUHC), chandigarh
11) http://www.pharmabiz.com/article/detnews.aspşarticleid=167382sectionid=50