“an evaluation of the effect of different irrigating
TRANSCRIPT
i
“AN EVALUATION OF THE EFFECT OF DIFFERENT IRRIGATING
SOLUTIONS AS A FINAL RINSE ON THE MICROHARDNESS OF ROOT
CANAL DENTIN - AN IN VITRO STUDY’’
Dissertation Submitted to the Rajiv Gandhi University of
Health Sciences, Karnataka; Bangalore
In partial fulfilment
Of the requirements for the degree of
MASTER OF DENTAL SURGERY
In
CONSERVATIVE DENTISTRY AND ENDODONTICS
Under the guidance of
DR. JAYAKUMAR T., M.D.S, PROFESSOR
DEPARTMENT OF CONSERVATVE DENTISTRY AND ENDODONTICS,
THE OXFORD DENTAL COLLEGE,
BOMMANAHALLI, BANGALORE- 68
2016-2019
By
DR. NOORIE ABDUL SALAM
Scanned by CamScanner

Scanned by CamScanner
Scanned by CamScanner

Scanned by CamScanner
Scanned by CamScanner
Scanned by CamScanner
i
List of abbreviations
ANOVA Analysis of Variance
Ca:P Calcium: Phosphate
ClO2 Chlorine Dioxide
EDTA Ethylenediaminetetraacetic acid
ISO International Organisation for Standardisation
K-Files Kerr files
KHN Knoop Hardness Number
NaOCl Sodium Hypochlorite
NiTi Nickel Titanium
SD Standard Deviation
VHN Vicker’s Hardness Number

i
List of tables
Sl. No. Tables Page No.
1. Comparison of mean Micro Hardness values
between 05 groups using One-way ANOVA Test
41
2. Multiple comparison of mean difference in Micro
hardness values between groups using Tukey's HSD
Post hoc Analysis
42
3. Individual values obtained 65
List of graphs
Sl. No. Tables Page No.
1. Comparison of mean Micro Hardness values
between 05 groups
43
2. Comparison of mean Micro Hardness values [with
standard errors] between 05 groups
44
i
List of Photographs
Fig. No. Photographs Page No.
1. Teeth samples 39
2. Protaper Universal rotary files 39
3. Endomotor 39
4. Teeth embedded in resin 39
5. Saline 39
6. Sodium hypochlorite 39
7. EDTA 40
8. Chlorine dioxide 40
9. QMix 40
10. Matricaria recutita 40
11. Application of irrigating solution 40
12. Vicker’s microhardness test 40
13. Illustration of the Vicker’s indentation and
digital measurement of the diagonals
68
i
ABSTRACT
Aim:
The objective of this in vitro study is to evaluate the effect of EDTA, ClO2, QMix,
and Matricaria recutita, on the microhardness of root dentin.
Materials & Methodology:
Forty extracted single rooted premolars were randomly assigned to 5 groups (n=16).
The root canals were prepared using Protaper Universal rotary files (Dentsply, India)
and distilled water for irrigation. Each group was treated with NaOCl as initial rinse
and then with EDTA, ClO2, QMix, Matricaria recutita, and Saline as final rinse. All
the samples were then placed on the Vicker’s microhardness tester and the results
statistically analyzed to determine which irrigating solution had the least effect on
the microhardness of root dentin.
Results:
Matricaria recutita had the least effect on the microhardness of root dentin, followed
by QMix and ClO2. EDTA showed the maximum reduction in microhardness of root
dentin.
Conclusion:
Under the limitations of this study, Matricaria recutita and QMix show promise for
use as irrigants because of less detrimental effect on the microhardness of root
dentin.
Keywords: EDTA, ClO2. German chamomile, QMix, root dentin, irrigation, microhardness, Vicker’s, NaOCl, final rinse .

Introduction
1
A successful root canal treatment involves the root canal system being
thoroughly cleansed and disinfected, followed by a three dimensional obturation of
this space.1 The mechanical instrumentation of the root canal produces a smear layer
that covers the dentinal tubules. The smear layer, being an amorphous irregular layer
containing inorganic dentin debris as well as organic materials like pulp tissue,
odontoblastic process, necrotic debris, microorganisms and their metabolic by-
products, needs to be removed before and during shaping.2 Hence, it involves the
simultaneous action of endodontic instruments and irrigating solutions which
eliminate the pre-existent organic and inorganic remnants and reduce the microbial
content and its by-products from the root canal system.2
Irrigation is one of the most important aspects of root canal preparation and is
currently the best method for the removal of tissue remnants and dentin debris during
instrumentation.3 It facilitates this removal through a flushing mechanism and can
also help in preventing the packing of hard and soft tissue in the apical third of the
root, which could otherwise cause a variety of complications such as transportation,
zipping, and extrusion of infected material into the periapical area. Berutti et al. in
1997 stated that solutions used as irrigants could penetrate 130µm of the dentinal
tubules, but bacteria can penetrate up to 1000µm; and to achieve proper antibacterial
effectiveness, irrigating agents should remove organic and inorganic tissues in root
canals, open the tubules, and penetrate in to the root canal system.4 Because of the
central role of irrigation in endodontic treatment and their multitude of tasks, there is
a continuing search for an optimal irrigating solution and strategy. None of the
presently available irrigating solutions can be regarded as optimal; however, using a
Introduction
2
combination of products in the correct sequence can contribute to a successful
treatment outcome.5
The most widely used endodontic irrigant is sodium hypochlorite (NaOCl),
because of its antibacterial activity and ability to dissolve vital and necrotic organic
tissue.6 It is formed by the bonding of chemical compounds like hypochlorous acid
(HOCl) and Sodium hydroxide (NaOH). It is hypertonic and alkaline which makes its
pH higher than 11, and is antibacterial, acts as a solvent of organic matrix, oxidizes
and hydrolyzes protein, removes intracellular fluids as well as magnesium and
carbonate ions. It also destroys fungi, spores, and viruses when used in low
concentrations ranging from 1% to 5.25%, thereby reducing its toxicity.7
Hypochlorite is the only root canal irrigant of those in general use, that dissolves
necrotic and vital organic tissue. It is difficult to imagine successful irrigation of the
root canal without sodium hypochlorite.5
The complete removal of smear layer requires the use of a chelating agent or
other demineralizing agents and a soft tissue solvent because no single solution can
provide both effects.8 Nygaard Ostby in 1957 introduced chelating agents in
endodontics for the preparation of calcified and narrow canals. Chelation is a physio-
chemical process which involves the uptake of multivalent positive ions, reacts with
the calcium ions in hydroxyapatite crystals and causes changes in the microstructure
of the dentin and changes the Ca:P ratio of the dentin surface.2 EDTA according to
Nygaard Ostby was recommended to be used at 15% concentration with a pH of 7.3
and the following composition: Disodium salt of EDTA (17g), Distilled water
(100mL), 5M sodium hydroxide (9.25mL). The main mineral components of dentin,
Introduction
3
phosphate and calcium, are soluble in water. When the disodium of EDTA is added to
this equilibrium, the calcium ions are removed from the solution which leads to the
further dissolution of the ions from the dentin, keeping the solubility of the product
constant and thus causing decalcification of the dentin.5 Based on a review on the
applications of EDTA in endodontics by Mazen et al. in 2017, EDTA decalcified
dentin to a depth of 20-30µm in 5 minutes. The liquid EDTA at a concentration of
17% removes the smear layer better as compared to paste type EDTA when it comes
in contact with the root canal dentin for less than 1 minute.9 According to a study by
Jose et al. in 1998 which studied the antibacterial properties of endodontic irrigants,
the antimicrobial effect of EDTA was stronger than that of citric acid and 0.5%
NaOCl but weaker than 2.5% NaOCl and 0.2% CHX.10
Chlorine dioxide (ClO2) is chemically similar to chlorine or hypochlorite and
this makes it a likely substitute for the hypochlorite due to its reduced toxicity and
irritating effect when applied to the human body. According to the manufacturer, it is
known to have certain tuberculocidal, bactericidal, virucidal and fungicidal properties
and is known to kill bacteria by disrupting the transport of nutrients across the cell
wall, due to its powerful oxidizing properties. ClO2 has recently come under
consideration as a possible root canal irrigant because of its similar reported
antibacterial activity in eliminating E.faecalis to NaOCl within 30 minutes on
dentinal discs. A study by Cobankara et al. in 2010 demonstrated that 13.8% ClO2
was as effective as 5.25% NaOCl in dissolving bovine pulp tissue.11
Although the combination of EDTA and Sodium Hypochlorite (NaOCl) have
been advocated as an effective irrigation regimen to remove the organic and the
Introduction
4
inorganic matter, a study by Deepa et al. in 2015 has shown that using 17% EDTA
solution also resulted in the maximum amount of calcium loss as the treatment time
increased, accompanied by a decrease in dentin microhardness.12 Since various
irrigants had to be used together to achieve the maximum effect, it resulted in dentists
spending a lot of time on the irrigation protocol alone. Hence, new irrigants were
introduced which has favourable properties as well as the same effect on the root
canal system, for better patient management and cleaning and shaping of the canal.10
BioPure MTAD marketed by Dentsply, Tulsa is a mixture of 3% tetracycline
isomer (doxycycline), 4.25% citric acid, and 0.5% detergent and has been shown to
be effective in the smear layer removal (Torabinejad et al., 2003).10 According to a
study by Kandil et al. in 2014, which evaluated the effect of different irrigating
solutions on the microhardness of root dentin, MTAD showed a lower effect on the
microhardness of root dentin than Malic acid and EDTA.13 Its action induced
inconsiderable erosion but promoted a significant decrease in dentin microhardness
(Dineshkumar et al., 2012; Saghiri et al., 2009).10 The results of the study differed
from other authors like Garcia Godoy et al. in 2005 who stated that both MTAD and
EDTA decrease the microhardness of root canal dentin because they collapsed the
dentin matrix structure. This effect by MTAD could be because of the presence of 3%
doxycycline hyclate component (an isomer of tetracycline) which acts as a calcium
chelator and causes root surface demineralization, as well as 4.25% citric acid which
dissolves mineral content of dentin.13
QMix 2in1 (Dentsply Tulsa Dental, Tulsa, USA) is a new irrigation solution of
antimicrobial agents for smear layer removal; it contains EDTA, CHX and a

Introduction
5
surfactant. The addition of a surfactant to chelating agents results in reduction of
dentin microhardness, but according to the study by G. Charul et al. in 2017, QMix
showed least reduction in microhardness of root canal dentin as compared to 17%
EDTA and MTAD, and has properties like biocompatibility, antimicrobial action, and
smear layer removal. Normally, the mixing of EDTA and CHX produces a white
precipitate, but in QMix 2in1 this is avoided because of its chemical design.10
The role of natural extracts for endodontic purpose in smear layer removal has
been evaluated for plants such as Morinda citrifolia and German chamomile
(Marticaria recutita) extract and tea tree (Melaleuca alternifolia) oil in a review of
Natural therapeutic option in Endodontics by V. Nagendrababu et al. in 2016.
Lahijani et al. in 2006 compared the chamomile hydroalcoholic extract and tea tree
oil to 2.5% NaOCl for smear layer removal. They concluded that chamomile has the
ability to remove the smear layer better when compared to NaOCl, but lesser than the
combination of NaOCl and EDTA. The smear layer removal could be attributed to the
presence of acidic components (capric acid, caprylic acid, chlorogenic acid, o-
caumaric acid, p-caumaricacid, dihydroxybenzoic acid) in the extract.14 The
antibacterial effects of German chamomile could be attributed to the presence of
active components like α-bisabolol and azulenes, which show anti-inflammatory
effects as well. More than 120 chemical constituents have been identified in the
flower as secondary metabolites, including 28 terpinoids, 36 flavonoids, and 52
additional compounds with potential pharmacological activity. Components like α-
bisabolol and cyclic ethers are antimicrobial, umbelliferone is fungistatic,
chamazulene is antiseptic, and flavonoids like apignine and luteoline are anti-

Introduction
6
inflammatory. Higher concentrations like 250mg/mL showed antimicrobial activity
against Enterococcus faecalis and Candida albicans too, but not more that 2%
CHX.15 To date, there are no studies comparing the effect of Marticaria recutita on the
root canal dentine as opposed to other root canal irrigants.
The structural properties of dentin, such as microhardness, permeability, and
solubility, may change after the use of chemical irrigants, which can alter the
proportion of organic and inorganic components. Microhardness is considered as
indirect evidence of mineral changes in root dentin; such changes could affect the
adhesive properties of dentin surface.16 In the specific case of root dentin, the agents
react with the calcium ions in the hydroxyapatite crystals. This process can cause
changes in the microstructure of the dentine and changes in the Ca:P ratio.17
Microhardness is sensitive to the composition and surface changes on the tooth
structure and Knoop hardness and Vicker’s Microhardness tester are responsible for
measuring the hardness of the dentin. Pashley et al. reported in a study conducted in
1985 that there is an inverse correlation between the dentin microhardness and tubular
density so, any significant alteration in the dentin microhardness after irrigation with
different chemicals will indicate the direct effect the chemicals have on the
components of the dentin structure.12
Previously studies have been conducted on Matricaria recutita (German
chamomile) to evaluate its effect on smear layer removal and on the disinfection of
the root canal space, but currently there are no studies that evaluate the effect of this
herbal product on the microhardness of root canal dentin.
Introduction
7
Thus, this study was aimed to evaluate for the first time, the effect Matricaria
recutita or German chamomile has on the microhardness of the root canal dentin and
to compare the effects with conventional irrigating solutions such as EDTA, ClO2,
and a novel irrigating solution QMix, which is already available in the market.
Objectives
8
The objectives of this in vitro study are:
i. To evaluate the effect of Matricaria recutita on the microhardness of the root
canal dentin.
ii. To compare and evaluate the difference in microhardness of root canal dentin
after exposure to the different root canal irrigants.
Null Hypothesis
The null hypothesis is that there is no significant difference between the effect of
EDTA, CHX, QMix, and Marticaria recutita when used as a final rinse, on the root
canal dentin.

Review of Literature
9
The objective of a successful endodontic treatment is to essentially remove all
vital or necrotic and gelatinous mass pulp remains that accumulate in the pulpal
chamber and the root canal wall in order to decontaminate it. This is achieved by
debridement with manual and mechanical instruments inside the canal along with
simultaneous irrigation. It is known that tissue debridement with manual or rotary
instruments produce a smear layer of about 2-2.5 mm thickness that accumulates on
the surface of the dentinal tubules and inside them and is composed mainly of
bacteria, toxins, hydroxyapatite crystals, saliva, and blood, making root canal
irrigation necessary for its success.7
With every thrust of an instrument, noxious materials like necrotic pulp or
shreds of mummified tissues are most likely to be pushed into the periapical area
through the apical foramen, resulting in possible periradicular pathologies. Thus
during each instrumentation it becomes important to irrigate simultaneously with
irrigating solutions capable of disinfecting them and dissolving organic and inorganic
material.18
Sodium hypochlorite is a salt formed by the bonding of chemical compounds
like hypochlorous acid (HOCl), and sodium hydroxide (NaOH). It is also hypertonic
and alkaline and has a pH higher than 11. NaOCl possesses certain good properties
like antibacterial action, dissolution of organic matrix, oxidisation and hydrolysis of
protein, and removal of intracellular fluids as well as magnesium and carbonate ions
present in root canal dentin. In addition, it also destroys fungi, spores, and viruses
when used at low concentration ranging from 1 to 5.25% without resulting in
toxicity.19 And although 5.25% sodium hypochlorite is used as a single irrigant in
Review of Literature
10
most root canals, it does not have the capacity to completely remove the inorganic
portion of the dentinal smear layer and does not appropriately moisten the root canal
walls in narrow canals. Therefore, it has been proposed to alternate hypochlorite with
chelating agents that expand the root canal lumen facilitating access. The most widely
used is ethylenediaminetetraacetic acid (EDTA); and although this particular protocol
is the most effective for cleaning and shaping of root canals, it is still controversial on
the topic of reduction in microhardness of the root canal dentin.7
In its chemical structure, ethylenediaminetetraacetic acid, EDTA, has six
potential sites for binding metal ions and thus forms stable complexes with calcium
ions and demineralizes superficial root canal walls by simplifying the preparation of
narrow canals.20 However, it does not possess any disinfectant capacities and cannot
remove the organic component of dentinal smear. It is also believed that when
combined with sodium hypochlorite, it inactivates chlorine, removing its proteolytic
capacity.21
Goldberg and Abramovich in 1977 conducted a study analysing the effect of
EDTAC which reported that addition of a quaternary ammonium bromide (Cetavlon)
increased the action of EDTA by reducing its surface tension, because EDTA
solutions act only through direct contact with the substrate. This combination, known
as EDTA plus Cetavlon (EDTAC), was shown to be very effective in smear layer
removal and increasing the diameter of the opened dentinal tubules. Recently Çalt
and Serper in 2000 reported that ethylene glycol-bis [b-aminoethylether]-N,N,N=,
N=-tetraacetic acid (EGTA) was also effective in removing the smear layer, without
inducing dentinal erosion commonly caused by EDTA. Tetracycline-hydrochloride
Review of Literature
11
(HCl) has also been proposed as a root canal irrigant and in addition to its
antimicrobial effect tetracycline-HCl also acts as a calcium chelating agent due to its
low pH. One percent tetracycline HCl has been shown to be as effective as 50% citric
acid in the removal of smear layer, while causing less demineralization of peritubular
dentin.1
Dogan et al. in 2001 reported that some chemicals used for endodontic
irrigation are capable of causing alterations in the chemical composition of dentin and
that any change in the Ca:P ratio may alter the original proportion of organic and
inorganic components, which in turn could change the microhardness, permeability,
and solubility characteristics of dentin.22 Studies have also shown that different
concentrations of EDTA, EDTAC, and EGTA are capable of decreasing the
microhardness of root canal dentin and that this effect can increase by extended
application times. Changes in the mineral content of superficial dentin may also
adversely affect the sealing ability and adhesion of dental materials such as resin-
based cements and root canal sealers to dentin.23
Effect of EDTA on microhardness
A study aimed to evaluate the effect of citric acid, ethylenediaminetetraacetic
acid (EDTA) and ethylenediaminetetraacetic acid plus Cetavlon (EDTAC) solutions
on the microhardness of human root canal dentine. Sixteen maxillary human canines
were sectioned transversely at the cemento-enamel junction and the crowns were
discarded. Subsequently, each root was embedded in an epoxy resin cylinder and their
middle third sectioned horizontally into 4 mm thick slices. The samples were
Review of Literature
12
randomly divided into three groups according to the chelating agent employed, as
follows (n = 6): group 1: EDTA 17%, group 2: EDTAC 17% and group 3: citric acid
10%. Dentine microhardness was then measured with a load of 50 g for 15 s. At the
beginning of the experiment, reference microhardness values were obtained for
samples without any etching (t = 0 min). The same samples were then exposed to 50
microL of the chelator solution for 1, 3 and 5 min. The Student's t-test (P < 0.05) was
used to compare results for different times for each chelator and different chelator for
each time. Microhardness decreased with increasing time of application of chelating
solutions. There were no significant (P > 0.05) differences between initial
microhardness for the three groups as well as after 1 min of application of the
substances. After 3 min, EDTA produced a significantly greater reduction in
microhardness. However, there was no significant difference between EDTA and
EDTAC after 5 min. Citric acid caused significantly less reduction in microhardness.
Overall, citric acid was least effective in reducing dentine hardness whilst EDTA had
the strongest effect.17
A study evaluated the effect of single and combined use of ethylenediamine
tetra acetic acid (EDTA), ethylene glycol bis [b-aminoethylether] N,N,N=,N=-
tetraacetic acid (EGTA), EDTA plus Cetavlon (EDTAC), tetracycline-HCl, and
NaOCl on the microhardness of root canal dentin. The crowns of 30 single-rooted
human teeth were discarded at the cementoenamel junction and the roots were
bisected longitudinally to obtain root halves (N 60). The specimens were embedded
in auto polymerizing acrylic resin, leaving the root canal dentin exposed. Dentin
surfaces were prepared for microhardness test by grinding and polishing. The
Review of Literature
13
reference microhardness values of untreated specimens were recorded using a
Vicker’s microhardness tester at the apical, mid-root, and cervical levels of the root
canal. Thereafter, the specimens treated with single (test solution only) or combined
(test solution, followed by 2.5% NaOCl) versions of the irrigants for 5 minutes. Post
treatment microhardness values were obtained as with initial ones. Statistical
comparisons between the test groups and among single and combined treatments
were carried out using 2-way ANOVA with repeated measures (P .05). Comparisons
within each group with respect to application regions were made with Friedman’s
nonparametric 2-way analysis of variance at the same level of significance. It was
found that, all treatment regimens except distilled water significantly decreased the
microhardness of the root canal dentin (P. 05). The single and combined use of EDTA
decreased the microhardness of the root canal dentin significantly more than all other
treatment regimens (P .05). Compared with their single-treatment versions, all
combined treatment regimens decreased the mean microhardness values significantly
(P .05). A comparison of single and combined treatment regimens revealed
significant decreases only for EDTA and EDTA NaOCl in the coronal region and for
EDTAC and EDTAC NaOCl in the apical and middle regions of the root canal (P
.05). Therefore they concluded that the use of EDTA alone or prior to NaOCl resulted
in the maximum decrease in dentin microhardness. The softening effect of subsequent
NaOCl treatment was both material and region dependent. However, for combined
treatment regimens, subsequent use of NaOCl levels the statistical differences
between the regional microhardness values obtained after treatment with EGTA,
EDTAC, and tetracycline-HCl.1
Review of Literature
14
The aim of an in vitro study was to evaluate the effect of 7% maleic acid and
17% EDTA solutions on the microhardness and the surface roughness of human root
canal dentin. Forty-five extracted human maxillary central incisors were sectioned
longitudinally into a total of 90 segments, which were embedded in auto
polymerizing acrylic resin, and were grounded flat with silicon carbide abrasive
papers. Based on the test solutions used, samples were divided randomly into three
groups: (1) the EDTA group, 1 mL of 17% EDTA for 1 minute (n = 30), (2) the
maleic acid group, 1 mL of 7% maleic acid for 1 minute (n = 30), and (3) the control
group, 1 mL of 0.9% saline for 1 minute (n = 30). Every group was then divided into
two subgroups of 15 specimens each. In group 1a, 2a, and 3a, specimens were used to
determine the microhardness of the root canal dentine in the coronal, middle, and
apical third using Vicker's hardness tester. In groups 1b, 2b, and 3b, specimens were
used for the determination of surface roughness of the root canal dentine using a
roughness tester (Surtronic, Leicester, England). The data were statistically analyzed
using the Kruskall Wallis and Mann Whitney U tests. There was no significant
difference between EDTA and maleic acid in the reduction of microhardness. The
increase in roughness was significantly greater with maleic acid when compared with
EDTA. Maleic acid reduced the microhardness of root dentin similar to EDTA but
increased the surface roughness significantly more than EDTA.24
Another study aimed to evaluate the microhardness of human dentin by using
four irrigating solutions. A total of 40 extracted mandibular premolars were selected
and sectioned horizontally in the middle third of the root. Forty specimens of 4 mm
thickness were embedded in acrylic resin and polished. Four test groups, each group

Review of Literature
15
containing ten specimens were immersed in respective irrigating solution and
subjected to Vicker’s microhardness test at T0, T2 and T5min. The data obtained
were analyzed using the one way ANOVA followed by Tukey HSD method with
p=0.05 as the level for statistical significance. The results suggested that there was no
statistically significant difference in mean values between four experimental
irrigating solutions. Mixture of Tetracycline isomer i.e. Doxycycline, Citric acid and
a Detergent (Tween 80) MTAD did not alter the microhardness of root canal dentin
significantly and seemed to be an appropriate irrigating solution, because of its
harmless effect on the microhardness of the root canal dentin.2
An in vitro study was conducted to compare the effect of different irrigants on
root dentin microhardness and smear layer removal. A total of 50 roots were equally
divided into two halves to measure dentin microhardness and to evaluate the amount
of smear layer. One hundred root halves were divided into five equal groups 20
sample each according to the final irrigants used: Group 1: 2.5% NaOCl, Group 2:
2.5% sodium hypochlorite (NaOCl) followed by 7% malic acid (MA), Group 3: 2.5%
NaOCl followed by 17% ethylenediaminetetraacetic acid (EDTA), Group 4: 2.5%
NaOCl followed by mixture of tetracycline, acid and detergent (MTAD) and Group 5:
saline. Ten root halves from each group were prepared to measure dentin
microhardness at baseline measurement and after treatment to determine the change
in microhardness, while the remains 10 root halves were prepared for
scanning electron microscope to evaluate the amount of smear in the coronal, middle
and apical thirds. Data were analyzed using one-way ANOVA and Student's t-test for
microhardness and Kruskall–Wallis and Mann–Whitney for smear layer. Malic acid
Review of Literature
16
showed the greatest significant reduction in dentin microhardness (P < 0.05),
followed by EDTA, MTAD, NaOCl and saline (control). EDTA, malic acid and
MTAD efficiently removed smear layer, respectively, in the coronal and middle
thirds of root canal. However, in the apical region, malic acid showed more efficient
removal of the smear layer than the other irrigants. As a conclusion, Malic acid is the
most efficient final irrigant solution after NaOCl irrigation throughout
instrumentation.13
A study aimed to evaluate the effects of root canal irrigants on the
microhardness of root canal dentin in the presence and absence of surface-modifying
agents. Forty-eight root halves were prepared by longitudinal splitting of the distal
roots of 24 freshly extracted mandibular human third molars and embedded in auto
polymerizing acrylic resin, leaving the dentin surface exposed. After polishing, the
microhardness values of the untreated dentin surfaces were recorded by using Vickers
tester at the mid-root level. The root halves were randomly assigned to 6 groups
composed of 8 samples each and treated for 5 minutes with one of the following
irrigants: 17% EDTA, REDTA, 2% chlorhexidine gluconate (CHX), 2% CHX with
surface modifiers (CHX-Plus), 6% NaOCl, or 6% NaOCl with surface modifiers
(Chlor-XTRA). After surface treatment, dentin microhardness values were recorded
at close proximity to the initial indentation areas. Experimental data were statistically
analyzed by using the t test and one-way analysis of variance, followed by Tukey
honestly significant difference test at α = 0.05. EDTA, REDTA, NaOCl, and Chlor-
XTRA significantly decreased the microhardness of root dentin compared with intact
Review of Literature
17
controls (P < .05). The addition of surface modifiers to the irrigants did not affect the
microhardness of the samples.25
A study aimed to evaluate the influence of the following irrigating solutions on
the microhardness of root canal dentin: 2% sodium hypochlorite (2NaOCl), 5%
sodium hypochlorite (5NaOCl), super-oxidized water (400 ppm Sterilox - Sx) and
17% EDTA (E). Eighty roots from bovine incisors were randomly divided into 8
groups (n=10): 2NaOCl, 5NaOCl, Sx, and 2NaOCl + E, 5NaOCl + E, Sx + E
(associated with E as final irrigant for 5 min), E solely and distilled water (dH2O) as
the negative control. Root canal preparation was performed by hand instruments,
using one of the irrigation protocols for 30 min. Then, 5 mm of the cervical root third
were cut out from each sample and subjected to the Vickers microhardness test, at
two points, one at approximately 500-1000 µm from the root canal lumen (distance
1), and the other at approximately 500-1000 µm from the external root surface
(distance 2). Data were analyzed by Wilcoxon and Kruskal-Wallis tests at 5%
significance level. Microhardness values at distance 1 were significantly lower than
those at distance 2 for all groups, except 5NaOCl and 5NaOCl + E groups (p>0.05).
EDTA showed the lowest microhardness values. However, no statistically significant
difference was detected among groups at distance 1 and EDTA was significantly
different only from Sx at distance 2. In conclusion, all tested solutions showed lower
microhardness at the most superficial root canal dentin layer compared to the one
found near the external root surface, except 5NaOCl and 5NaOCl + E; EDTA
promoted lower microhardness values in comparison to Sterilox at this site.26
Review of Literature
18
Another study was done to determine the Calcium loss and its effect on
microhardness of the root canal dentin following treatment with aqueous solution of
17% Ethylenediaminetetraacetic acid at different time intervals. In this study, twenty
extracted human canine teeth were bisected longitudinally and root halves were
embedded individually in rings with polyester resin. Samples were randomly divided
into 7 groups based on different time intervals i.e., each group had 5 samples each
(n=5 samples) and the remaining 5 samples served as a negative control group.
Initially, 20 ml of 17% EDTA solution was prepared as a blank to determine the
calcium levels in absence of the specimen. Then each sample was immersed in a
beaker containing 20 ml of experimental solution according to the different time
intervals and maintained under constant agitation using a magnetic multi-stirrer
(SBSA-09 series C, Barcelona, Spain) to homogenize the extracted calcium in the
solution. Then the samples were taken out of the beaker after the respective time
interval. Five ml aliquots were extracted from the beaker using a calibrated micro
pipette. These extracts were then placed in hermetically sealed and labeled glass
tubes. By this way, extracts were obtained for each sample at different time intervals.
The same samples were subjected for the evaluation of amount of Ca2+ release into
the solution by Atomic Absorption Spectrophotometer. Then the microhardness of the
sample used for determining the Ca2+ loss was evaluated at different dentin surface
adjacent to the root canal lumen in a microhardness testing machine (Micromet 2100
Microhardness Tester, Buehler). All experiments were completed under the same
conditions: 50 g load and 15s dwell time, following the guidelines given by Cruz-
Filho et al. The results were statistically analyzed (p<0.05) showing the time

Review of Literature
19
dependant effect of 17% EDTA in both calcium loss as well as microhardness
reduction in comparison with saline (control group). And thus it was concluded that,
root canal irrigation with 17% EDTA solution is time dependant, increased irrigation
time leads to structural changes, as evidenced by reduction of dentin microhardness.12
An in vitro study was carried out to compare of the effect of 17%
ethylenediamine tetra-acetic acid (EDTA), 2% chlorhexidine (CHX), 18% etidronic
acid (HEBP), and 4% propolis as an irrigant on the microhardness of root dentin. The
sample size for the study was 100. Each specimen consisted of a longitudinally
sectioned half of a root of a single-rooted tooth which was embedded in acrylic resin.
The prepared specimens were divided randomly into five groups of twenty specimens
each. Each group was treated with the irrigants to be tested. Group I was the control -
the specimens were treated with distilled water. The specimens in Group II were
treated with sodium hypochlorite (NaOCl) followed by EDTA. Specimens in Group
III were treated with NaOCl followed by CHX. Specimens in Group IV were treated
with NaOCl followed by HEBP, and specimens in Group V were treated with NaOCl
followed by propolis. Following this, all the specimens were placed on the Vickers
hardness tester and three readings were taken for each specimen. An average reading
was obtained for each group. The results were tabulated and statistically analyzed to
determine which of the irrigant solutions had the least effect on the microhardness of
root dentin. Eighteen percent HEBP had the least effect on the root dentin
microhardness, followed by 4% propolis and 2% CHX. Seventeen percent EDTA
showed maximum effect on the microhardness of the dentin. Under the limitations of
Review of Literature
20
this study, 18% HEBP and 4% propolis show promise for use as irrigants because of
less detrimental effect on the hardness of root dentin.27
An in vitro study evaluated the effects of root canal irrigants on the
microhardness of root canal irrigants on the microhardness of root canal by using
three types of irrigant solutions with different concentration and normal saline used as
control group. In this study the root halves were prepared by longitudinal splitting of
the roots of 56 freshly extracted caries free maxillary second premolars and
embedded in auto polymerizing acrylic resin, leaving the dentin surface exposed. The
root halves were randomly divided to seven groups composed of 16 samples each and
treated for 5 min with one of the following irrigants: normal saline (control group),
0.2% chlorhexidine, 2% chlorhexidine, 2.5% sodium hypochlorite, 5.25%, 5%
ethylene dimetha tera hydrate EDTA and 17% EDTA. After surface treatment, the
dentin microhardness of the root samples was recorded at the mid-root level by using
vicker’s microhardness tester. The data were statistically analyzed by using one-way
analysis of variance, followed by Duncans test with a significant difference test at
p<0.05. The results showed that EDTA, sodium hypochlorite, and 2% chlorhexidine
significantly decreased the microhardness of root dentin compared with controls
(p,0.05), while 0.2% chlorhexidine had no significant effect on the microhardness of
root dentin. Therefore, it was concluded that the irrigant solutions affect the
microhardness of the samples except 0.2%.28
Another study was conducted to study the microhardness of root canal dentin
after irrigation with different irrigant solutions for different periods. Twenty five
newly extracted non carious human permanent incisors were sectioned at
Review of Literature
21
cementoenamel junction and split longitudinally then divided into five groups; Gr1
(control) distilled water, G2: 5.25% sodium hypochlorite (NaOCl) for (10 min) then
17% EDTA for (1 min), G3: 5.25% sodium hypochlorite (NaOCl) for (10 min) then
17% EDTA for (5 min), G4: 5.25% sodium hypochlorite(NaOCl) for (20 min) then
17% EDTA for (1 min) and G5: 5.25% sodium hypochlorite(NaOCl) for (20 min)
then 17% EDTA for (5 min). Vickers microhardness was evaluated. Data were
analyzed using one-way ANOVA and paired t-test. The results indicated that all
treatment time with 5.25% NaOCl and 17% EDTA decreased dentin microhardness
significantly compared to distilled water (control). There were significant differences
(P<0.001) between the tested groups with increasing time of exposure of irrigation
solutions. Treatment with distilled water (control) showed significantly the highest
microhardness value, while 5.25% sodium hypochlorite for 20 minute followed by 5
minutes (G5) with 17% EDTA showed significantly the least microhardness value
followed by G4, G3 and G2. Therefore it was concluded that, increasing irrigation
time with both 5.25% sodium hypochlorite and 17% EDTA decreased dentin
microhardness.6
A study was conducted to evaluate the effect of different irrigation protocols on
microhardness of human root canal dentin. Forty extracted single rooted lower
premolars were used. All teeth were instrumented using manual stainless steel files
and irrigated by 2ml distilled water between each file, then were sectioned by
longitudinal splitting of each tooth. The root halves were randomly assigned into 4
parallel groups (n=10) and immersed for 5 minutes with one of the following
irrigants: Group I: 10 ml of 2.5% Sodium Hypochlorite (NaOCl), Group II: 10 ml of
Review of Literature
22
17% ethylene diamine tetra-acetic acid (EDTA) followed by 10 ml of 2.5% NaOCl,
Group III: 10 ml of 2.5% NaOCl followed by 10 ml of 2% chlorhexidine di gluconate
(CHX), Group IV: 10 ml of 2.5% NaOCl followed by 10 ml distilled water then were
followed by 10ml of 2% CHX. Ten root halves from each group were prepared to
measure dentin microhardness at baseline measurement and after treatment to
determine the change in microhardness, using Vickers tester. Data were analysed
using t-test, ANOVA test and Post Hoc test. Group II showed the highest percentage
decrease in microhardness values, followed by group III, then group IV and the
lowest was group I. All groups showed a significant difference between each other (P
< 0.05), except group III and IV. The coronal third showed the highest percentage
decrease with significant difference between apical and middle thirds (P < 0.05), in
which there was no significant difference between them. In conclusion, CHX is the
best final irrigant if there is excellent intermediate flush for prevention of its
precipitation with NaOCl. The coronal third needs conservative approach as it is the
most affected third.28
The aim of a study was to evaluate the effect of various endodontic irrigants on
the micro-hardness of the root canal dentin. This in vitro study was carried out on
eighty freshly extracted mandibular premolars with single canals. They were
decoronated at the cemento-enamel junction. Roots were sectioned longitudinally into
two halves. They were then polished and placed in auto polymerized resin moulds
with the polished surface facing outside. The samples were divided into four groups
based on the irrigants in which they were immersed i.e., 3% Sodium Hypochlorite
(3% NaOCl), 17% Ethylene Dioxide Tetra Acetic Acid (17% EDTA), 0.2% Chitosan
Review of Literature
23
and 6% Morinda citrifolia Juice (MCJ) for 15 minutes each. All the specimens were
then subjected to micro-hardness testing using a Vickers micro-hardness tester.
Statistical analysis was done using one way Analysis of Variance (ANOVA), Post-
Hoc Tukey test and Paired t-test to compare the pre and post immersion micro-
hardness values of the selected samples. The results of the present study indicated that
17% EDTA and 0.2% Chitosan significantly decreased the micro-hardness of root
dentin whereas 6% MCJ and 3% NaOCl had no significant effect on the
microhardness before and after immersing in the irrigants. A 6% MCJ and 3% NaOCl
which have significant antibacterial, antifungal, anti-inflammatory and smear layer
removing properties showed negligible effect on the micro-hardness of root canal
dentin making them suitable endodontic irrigating solution.
Effect of Chlorine Dioxide on microhardness
A study evaluated the effect of chlorine dioxide and various other more
common irrigation solutions on the microhardness and surface roughness of root
canal dentin. Fifty human maxillary central incisors were sectioned longitudinally and
treated for 1 minute with 5 ml of the following aqueous solutions (v/v%): Group 1:
13.8% chlorine dioxide, Group 2: 17% ethylene diamine tetraacetic acid (EDTA).
Group 3: 7% maleic acid, Group 4: 2.5% sodium hypochlorite (5ml/min), Group 5:
Saline (control). Specimens were subjected to microhardness and surface roughness
testing. Chlorine dioxide and sodium hypochlorite reduced the microhardness more
than other test agents. The highest surface roughness was produced with maleic acid.
Chlorine dioxide should be used cautiously during chemo-mechanical preparation of
the root canal system in order to prevent untoward damage to the teeth.11
Review of Literature
24
Effect of QMix on microhardness
A study aimed to compare the changes in microhardness of root dentin caused
by two novel irrigation regimens with conventional irrigation. Forty extracted human
permanent incisor teeth were selected. Decoronated roots were separated
longitudinally to get 80 specimens that were embedded in auto polymerizing acrylic
resin and grounded flat with silicon carbide abrasive papers. Of these, 60 root
segments without any cracks or defects were selected and divided into four groups
according to the irrigation regimen used (n = 15). Group I: 5% sodium hypochlorite
(NaOCl) + 17% ethylenediaminetetraacetic acid (EDTA) + 0.2% chlorhexidine di
gluconate (CHX) (conventional). Group II: 6% Morinda Citrifolia Juice + 17%
EDTA (MCJ). Group III: 5% NaOCl + Q Mix 2 in 1 (QMix). Group IV: Distilled
water (control). Irrigation regimens were performed for 5 minutes. Dentin
microhardness was measured with a Vickers indenter under a 200-g load and a 20-s
dwell time at the mid-root level of root dentin. The data were analyzed using Kruskal
Wallis test and Dunn's multiple comparison tests. A significant difference was seen in
the median values of the four groups. The control group showed the least reduction in
microhardness when comparison with the other groups. Except for Group III (Q Mix),
the other groups that were tested (MCJ and conventional regimens) showed
statistically significant difference from the control group. In conclusion, within the
limitation of this study, it was concluded that NaOCl + Q Mix were least detrimental
to root dentin microhardness when compared with MCJ and conventional irrigation
regimens.30
Review of Literature
25
Another study evaluated the effects of QMix, EDTA + CHX, EDTA + NaOCl
and maleic acid on the microhardness of root canal dentine. Forty recently extracted
human maxillary canine teeth were longitudinally sectioned into 80 segments and
then embedded in an auto polymerizing acrylic resin. The microhardness of the
dentine in the specimen was measured with a Vickers diamond indenter at the
Coronal, middle and apical thirds of the roots. Finally, the specimens were divided
randomly into four groups: 17% EDTA + 2.5% NaOCl; 17% EDTA + 2% CHX;
QMix; and 7% maleic acid. Post-treatment microhardness values were obtained and
the decrease in microhardness was calculated as a percentage. Microhardness values
were statistically analysed using the Kruskal-Wallis and Mann-Whitney U tests.
According to this study Maleic acid significantly decreased microhardness in all
regions, compared to the other groups. In the coronal and middle regions, there was
no significant difference among the other groups. In the apical region, there was no
significant difference between QMix and 17% EDTA + 2% CHX but these groups
presented significant dentine microhardness reduction compared to the 17% EDTA +
2.5% NaOCl group. In conclusion, while maleic acid showed the greatest reduction in
dentine microhardness, it was found that QMix, 17% EDTA + 2% CHX and 17%
EDTA + 2.5% NaOCl cause the same reduction in the microhardness of root canal
dentine in the coronal and middle regions.31
Another study aimed to evaluate the effect of final irrigation protocols (17%
EDTA, BioPure MTAD, SmearClear, and QMix) on microhardness and erosion of
root canal dentin. Fifty roots were sectioned transversely at the cemento-enamel
junction and each root was sectioned horizontally into 4-mm-thick slices. The

Review of Literature
26
samples were divided into five groups (n = 10) according to the final irrigation
protocol: G1: distilled water (control group); G2: 17% EDTA; G3: BioPure MTAD;
G4: SmearClear; and G5: QMix. The dentin microhardness was then measured with a
load of 25 g for 10 s. Initially, the reference microhardness values were obtained for
the samples without any etching. The same samples were then submitted to the final
irrigation protocols. A new measure was realized and the difference between before
and after the procedures was the dentine microhardness reduction. In sequence, the
specimens were submitted to SEM analysis to verify the dentinal erosion. The
Kruskal Wallis and Dunn tests (α = 5%) were used to compare the results. The dentin
microhardness decreased for all final irrigation protocols. There was no significant
difference between groups 2, 3, 4, and 5 (P > 0.05), but these groups presented
significant dentine microhardness reduction than G1 (P < 0.05). In G2, occurred the
highest incidence of dentinal erosion (P < 0.05). 17% EDTA, BioPure MTAD,
SmearClear, and QMix promoted significant dentine microhardness reduction.
Dentinal tubules erosion was promoted by 17% EDTA.32
A study aimed to evaluate the effect of final irrigation protocols on
microhardness reduction and erosion of root canal dentin. Sixty root canals from
mandibular incisors were instrumented and randomly divided into six groups (n = 10)
according to the irrigant used: QMix, 17% EDTA, 10% citric acid (CA), 1% peracetic
acid (PA), 2.5% NaOCl (solution control), and distilled water (negative control). The
chelating solutions were used to irrigate the canal followed by 2.5% NaOCl as a final
flush. After the irrigation protocols were completed, all the specimens were rinsed
with 10 mL of distilled water to remove any residue of the chemical solutions. Before
Review of Literature
27
and after the final irrigation protocols, dentin microhardness was measured with a
Knoop indenter. Afterwards, the specimens were prepared for scanning electron
microscopic analysis and the amount of dentin erosion was examined. Wilcoxon and
Kruskal-Wallis tests were used to analyze the results with a significance level set at
5%. At 100 µm, all protocols significantly reduced dentin microhardness (p < .05),
while at 500 µm, this effect was detected only in the EDTA and QMix groups (p <
.05). CA was the irrigant that caused more extensive erosion in dentinal tubules,
followed by PA and EDTA. QMix opened dentinal tubules, but did not cause dentin
erosion. Results suggest that QMix and 17% EDTA reduced dentin microhardness at
a greater depth. Additionally, QMix did not cause dentin erosion.33
A study aimed to evaluate and compare the effect of QMix, Tea tree oil,
Tamarindus indica, Green tea extract and 17% EDTA on root dentine micro-hardness.
Sixty freshly extracted human single rooted premolars were selected and divided into
six groups and subjected to various treatments as follows: Group 1-Q mix, Group 2-
Tea tree oil, Group 3 - 5% Tamarindus indica, Group 4 - 5% Green tea, Group 5 -
17% EDTA and Control group-normal saline. Each group was immersed in their
solutions for 5 minutes and then subjected to Vickers micro-hardness testing.
According to this study, maximum reduction in micro-hardness was seen in the
EDTA group, followed by QMix and then Tamarindus indica groups. Tea tree oil
group and Green tea groups did not show significant reduction in microhardness.
Least reduction was seen in the control group saline. In conclusion, EDTA induced
maximum reduction in root dentin microhardness, followed by QMix and Tamarindus
Review of Literature
28
indica. There was no significant reduction by Green tea, Tea tree oil and saline (p >
0.05) Tamarindus indica caused significantly less reduction than EDTA (p < 0.001).34
Vicker’s Microhardness testing on root dentin
In another study, Vickers micro hardness was assessed on root dentin and
cementum in 30 canines obtained from the Periodontics Discipline tooth bank. Crown
and cervical portion of the root were discarded by a transverse section situated 3mm,
apically, from the cemento-enamel junction on the buccal surface, thus obtaining the
root specimen. On root dentin, mean micro hardness values were obtained for 3
regions: (DR1) from 0.05 to 0.1 mm of the cemento dentin junction; (DR2) from 0.3
to 0.5 mm of the cemento dentin junction and (DR3) from 0.8 to 1.0 mm of the
cemento dentin junction. After statistical analysis (Variance Analysis test, p < 0,05),
we conclude that micro hardness at the DR2 region was statistically greater than that
at the DR3 region which was, in turn, greater than that at the DR1 region. The mean
micro hardness of cementum was 19.70 VHN.35
Another study aimed to determine the effect of variations in indentation load
and time on the Knoop and Vickers hardness numbers (KHN and VHN) for enamel
and dentin. Twenty molar teeth were divided into twenty enamel and twenty dentin
specimens. Each specimen was tested using a Knoop or Vickers microhardness tester
at different loads and times. The difference in hardness between the groups was
analyzed with two-way ANOVA followed by a Tukey test. The results revealed that a
difference of indentation time did not influence the microhardness number of enamel
and dentin. The KHN values of enamel and the VHN values of dentin were affected
Review of Literature
29
by variation of test loads. Therefore, the tooth hardness number for different loads
may not be acceptable for comparison.36
A study aimed to measure the microhardness of root dentin after
instrumentation with different file types and using irrigation with 2.5% sodium
hypochlorite. Root canal of 10 roots were irrigated only, root canal of 10 roots were
instrumented with stainless steel files, root canal of 10 roots were instrumented with
rotary nickel titanium files. Root canals of 10 roots were instrumented with nickel
titanium K-files. Additionally, five roots pulp was extirpated only, without irrigation
and served as control. The roots were sliced and root dentin microhardness was
determined at distance of 500 mm and 1000 mm from the pulp dentin interface. There
was a significant difference found between the microhardness at 500 mm and 1000
mm (P<0.001) in all groups. Instrumentation with Nickel titanium rotary files
affected dentin microhardness significantly to a lesser extent when compared to
stainless steel K files and Nickel titanium K-File. Therefore it was concluded that
instrumentation and irrigation with NaOCl changes the biomechanical properties of
dentin.3
Materials and Methodology
30
Source of Data
This study was conducted in the Department of Conservative Dentistry and
Endodontics, The Oxford Dental College, Bangalore.
Forty single rooted premolar teeth were collected from the Department of Oral
and Maxillofacial Surgery, The Oxford Dental College, Bangalore. Ethical clearance
was obtained from the institutional ethical committee of The Oxford Dental College,
Bangalore. All patients were explained about the need for their extracted teeth and
informed consent was taken for dental research purpose.
Inclusion criteria
Single rooted human premolar teeth
Presence of single canal
Exclusion criteria
Direct and indirect restorations
Cracks
Fractured
Grossly decayed
Resorption
Dilacerations
Materials and Methodology
31
Method of collection of data
The sample size was calculated based on the following criteria,
ANALYSIS: A priori: Compute required sample size
INPUT: Effect size f = 0.40
α err prob = 0.05
Power (1-β err prob) = 0.80
Number of groups = 5
OUTPUT: Noncentrality parameter λ = 12.8000000
Critical F = 2.4936960
Numerator df = 4
Denominator df = 75
Total Sample size = 80
Actual power = 0.8030845
The sample size has been estimated using the software Gpower v. 3.1.9.2.
Considering the effect size to be measured (d) at 40%, power of the study at 80% and
the margin of error at 5%, the total sample size needed is 80. So, each study group
will comprise of 16 samples.
Materials and Methodology
32
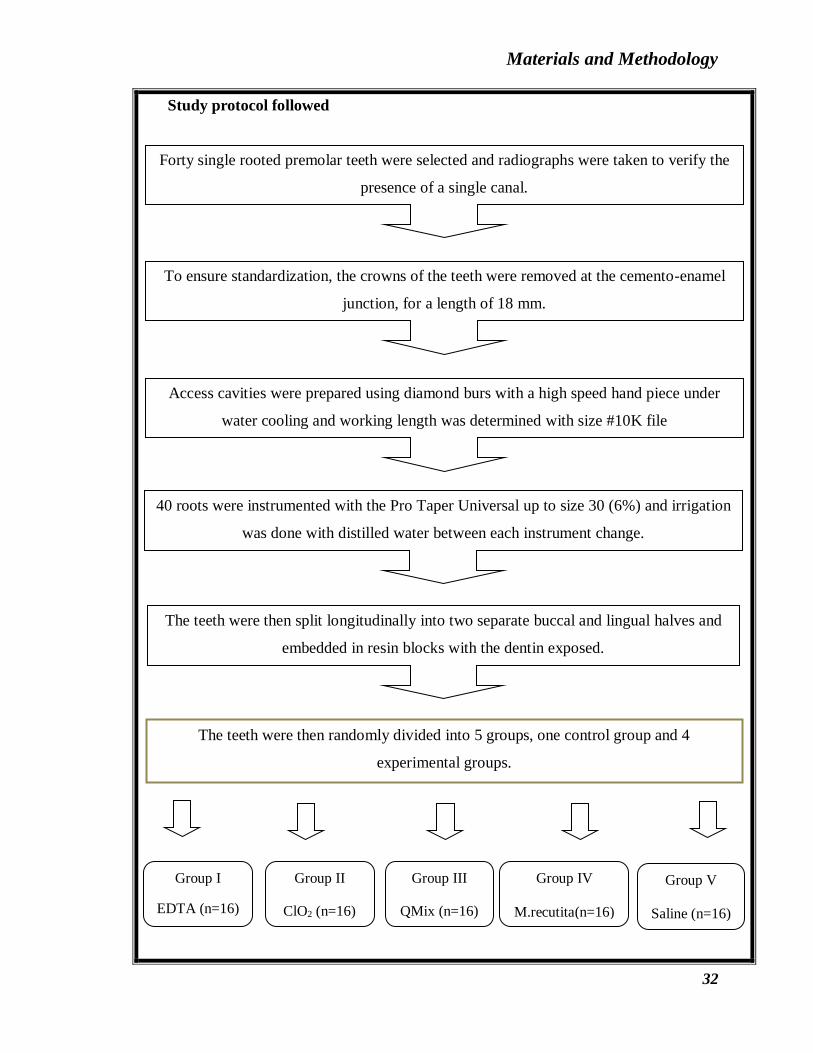
Study protocol followed
Forty single rooted premolar teeth were selected and radiographs were taken to verify the
presence of a single canal.
To ensure standardization, the crowns of the teeth were removed at the cemento-enamel
junction, for a length of 18 mm.
Access cavities were prepared using diamond burs with a high speed hand piece under
water cooling and working length was determined with size #10K file
40 roots were instrumented with the Pro Taper Universal up to size 30 (6%) and irrigation
was done with distilled water between each instrument change.
The teeth were then split longitudinally into two separate buccal and lingual halves and
embedded in resin blocks with the dentin exposed.
The teeth were then randomly divided into 5 groups, one control group and 4
experimental groups.
Group I
EDTA (n=16)
Group II
ClO2 (n=16)
Group III
QMix (n=16)
Group IV
M.recutita(n=16)
Group V
Saline (n=16)

Materials and Methodology
33
Instruments / Equipments (Table 1)
Equipment Purpose of use Manufacturer
Airotor hand
piece
Tooth
preparation
NSK, Inc Japan
Endomotor Root canal
preparation
Dentsply
Sirona, India
Vicker’s
Microhardness
Tester
Microhardness Struers, Gatan,
USA
Isomet Tooth
sectioning
Buehler, Lake
Bluff, IL, USA
The teeth were then treated with 3% NaOCl for 5 min, as an initial rinse and for 5 min
with each irrigant, as a final rinse.
The teeth were then subjected to a 100g load for a dwell time of 15 sec using Vicker’s
Microhardness Tester.
The two diagonals of the indentation left in the surface of the material after removing the
load were measured under microscope and the average calculated.
The area of the sloping surfaces of the indentation was calculated. Vicker’s hardness is
the quotient obtained by dividing the kgf load by the square mm area of indentation.

Materials and Methodology
34
Materials (Table 2)
Material Purpose of use Manufacturer Batch No.
Single rooted
teeth
Specimen
Burs Access
preparation
Mani. Inc
Japan
K-files Biomechanical
preparation
Mani. Inc
Japan
Pro Taper
Universal files
Biomechanical
preparation
Dentsply
Maillefer, USA
Acrylic resin Embedding tooth
3% Sodium
hypochlorite
Irrigation 23286
Saline (0.9%
N.W.)
Irrigation IA80092
Paper Points Drying the canal Dentsply
Maillefer, USA
17% EDTA Irrigation Pulpdent 17042602
0.2% Chlorine
Dioxide
Irrigation Solumium
Dental,
Hungary
H270514
QMix Irrigation Dentsply, Tulsa 170519
Matricaria
recutita
Irrigation Biocarve, India
Materials and Methodology
35
Composition of irrigants (Table 3)
EDTA E.D.T.A. di-sodium salt, distilled water
QMix Chlorhexidine and EDTA
Root canal Treatment
The teeth were stored in Hydrogen peroxide for a week and then in normal
saline until further use. They were thoroughly rinsed prior to use and the residual pulp
tissue was removed using barbed broaches. The working length for each tooth was
determined by inserting International Standard Organization (ISO) 10 K-file into the
canal and each canal was prepared till the working length with the Pro-Taper
Universal rotary system up to size 30 (6%) taper. The canals were then irrigated with
distilled water between each instrument change to avoid any unwanted changes to the
root canal dentin before conducting the study.
To ensure standardization of 18 mm, the teeth were decoronated at the
cemento-enamel junction using low speed diamond points and under copious water
irrigation to prevent overheating. The teeth were then sectioned longitudinally into
two halves and the separated buccal and lingual halves were then embedded in acrylic
resin, leaving the dentin surface exposed. The dentin surface was then polished using
silicon carbide abrasives to remove any surface irregularities, under distilled water
(prevent overheating).
The teeth were then randomly assigned to 5 groups, one control group and 4
experimental groups.
Materials and Methodology
36
Preparation of Matricaria recutita
10g of the weighed plant material were soaked in 100 mL of hot water and
boiled for 30 min in a conical flask for 24 hrs. The solution was then filtered using
filter paper.
Sample treatment
All the samples were initially treated for 5 min with 3% NaOCl as an initial
rinse for its bactericidal properties. The specimens were then randomly divided into 5
groups (n=16) and treated for 5 min with 5 mL of one of the following irrigants:
Group I was cleaned and shaped using the protocol mentioned above and treated
with 17% EDTA (Prime Dental Products, India)
Group II was cleaned and shaped using the protocol mentioned above and treated
with 0.2% Chlorine Dioxide (Solumium Dental, Hungary)
Group III was cleaned and shaped using the protocol mentioned above and treated
with QMix (Dentsply, Tulsa)
Group IV was cleaned and shaped using the protocol mentioned above and treated
with Matricaria recutita (Biocarve, India)
Group V was cleaned and shaped using the protocol mentioned above and treated
with Saline (Control group)
After the surface treatment, the samples were washed and dried, and the dentin
microhardness of each sample was determined as described below.
Materials and Methodology
37
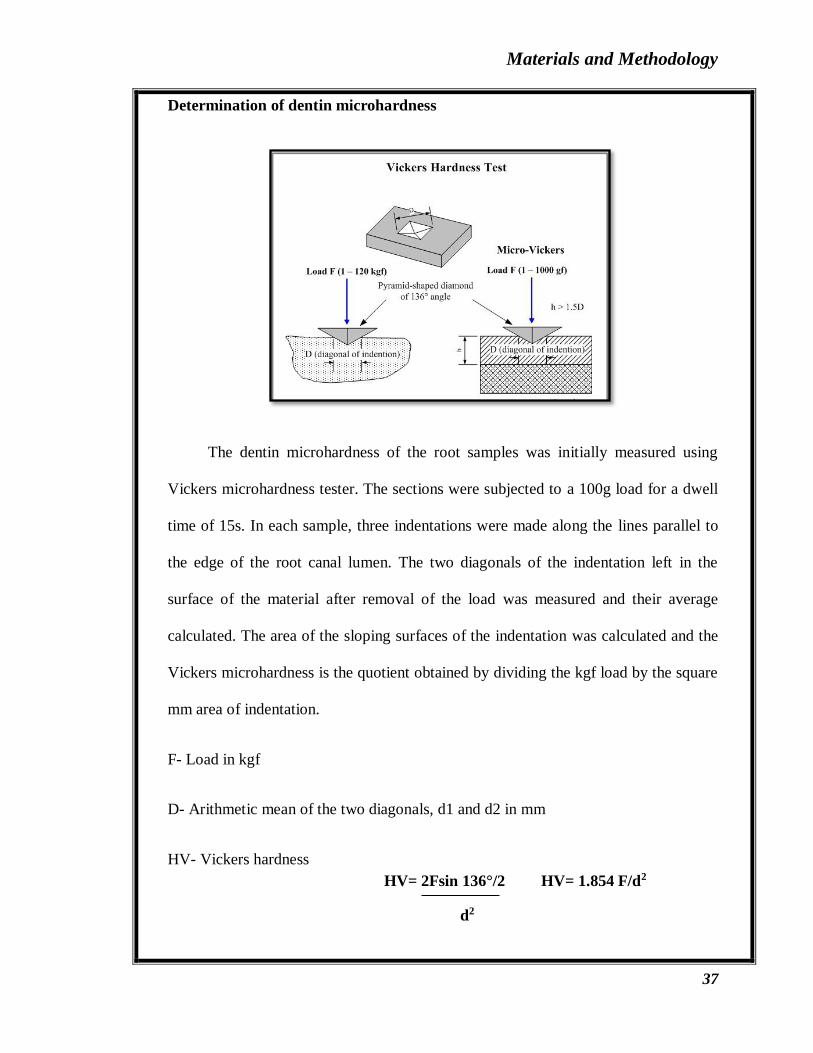
Determination of dentin microhardness
The dentin microhardness of the root samples was initially measured using
Vickers microhardness tester. The sections were subjected to a 100g load for a dwell
time of 15s. In each sample, three indentations were made along the lines parallel to
the edge of the root canal lumen. The two diagonals of the indentation left in the
surface of the material after removal of the load was measured and their average
calculated. The area of the sloping surfaces of the indentation was calculated and the
Vickers microhardness is the quotient obtained by dividing the kgf load by the square
mm area of indentation.
F- Load in kgf
D- Arithmetic mean of the two diagonals, d1 and d2 in mm
HV- Vickers hardness
HV= 2Fsin 136°/2 HV= 1.854 F/d2
d2
Materials and Methodology
38
Statistical Analysis
Statistical Package for Social Sciences [SPSS] for Windows Version 22.0 Released
2013. Armonk, NY: IBM Corp. was used to perform statistical analysis.
Descriptive Statistics:
Descriptive analysis includes expression of Micro Hardness in terms of Mean & SD.
Inferential Statistics:
One-way ANOVA test followed by Tukey's HSD post hoc Analysis was used to
compare the mean Micro Hardness values between study groups.
The level of significance was set at P<0.05.
Results
41
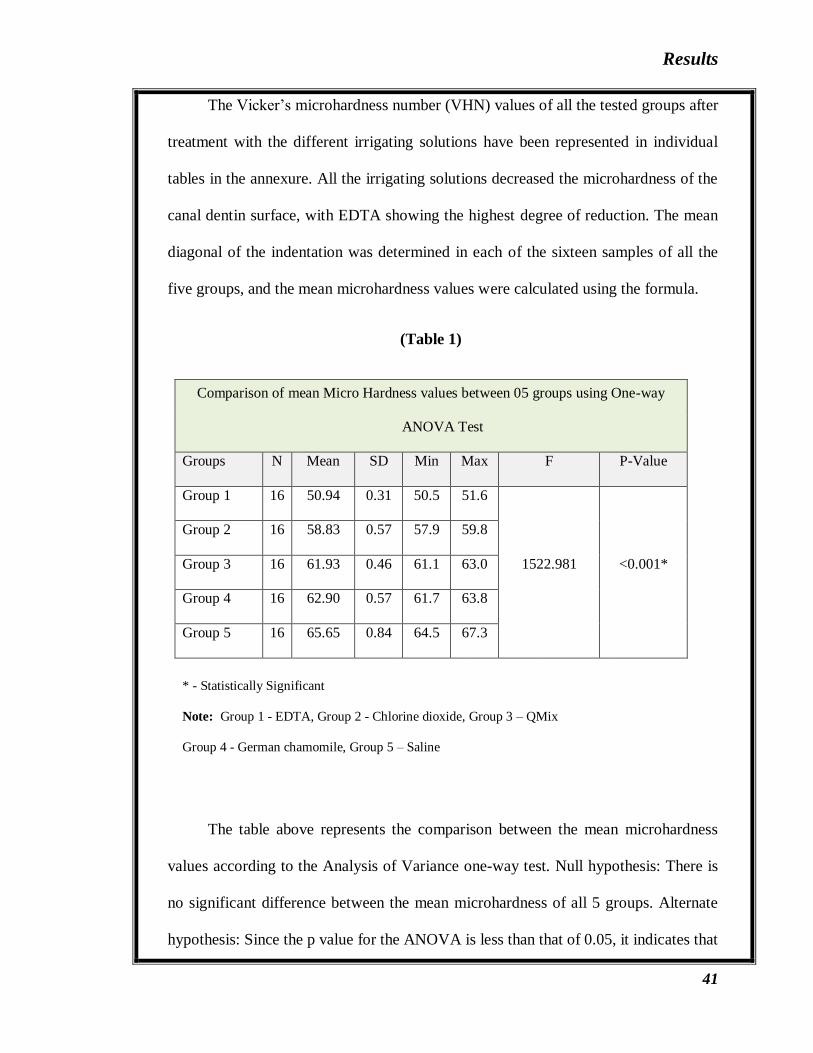
The Vicker’s microhardness number (VHN) values of all the tested groups after
treatment with the different irrigating solutions have been represented in individual
tables in the annexure. All the irrigating solutions decreased the microhardness of the
canal dentin surface, with EDTA showing the highest degree of reduction. The mean
diagonal of the indentation was determined in each of the sixteen samples of all the
five groups, and the mean microhardness values were calculated using the formula.
(Table 1)
Comparison of mean Micro Hardness values between 05 groups using One-way
ANOVA Test
Groups N Mean SD Min Max F P-Value
Group 1 16 50.94 0.31 50.5 51.6
1522.981 <0.001*
Group 2 16 58.83 0.57 57.9 59.8
Group 3 16 61.93 0.46 61.1 63.0
Group 4 16 62.90 0.57 61.7 63.8
Group 5 16 65.65 0.84 64.5 67.3
* - Statistically Significant
Note: Group 1 - EDTA, Group 2 - Chlorine dioxide, Group 3 – QMix
Group 4 - German chamomile, Group 5 – Saline
The table above represents the comparison between the mean microhardness
values according to the Analysis of Variance one-way test. Null hypothesis: There is
no significant difference between the mean microhardness of all 5 groups. Alternate
hypothesis: Since the p value for the ANOVA is less than that of 0.05, it indicates that
Results
42
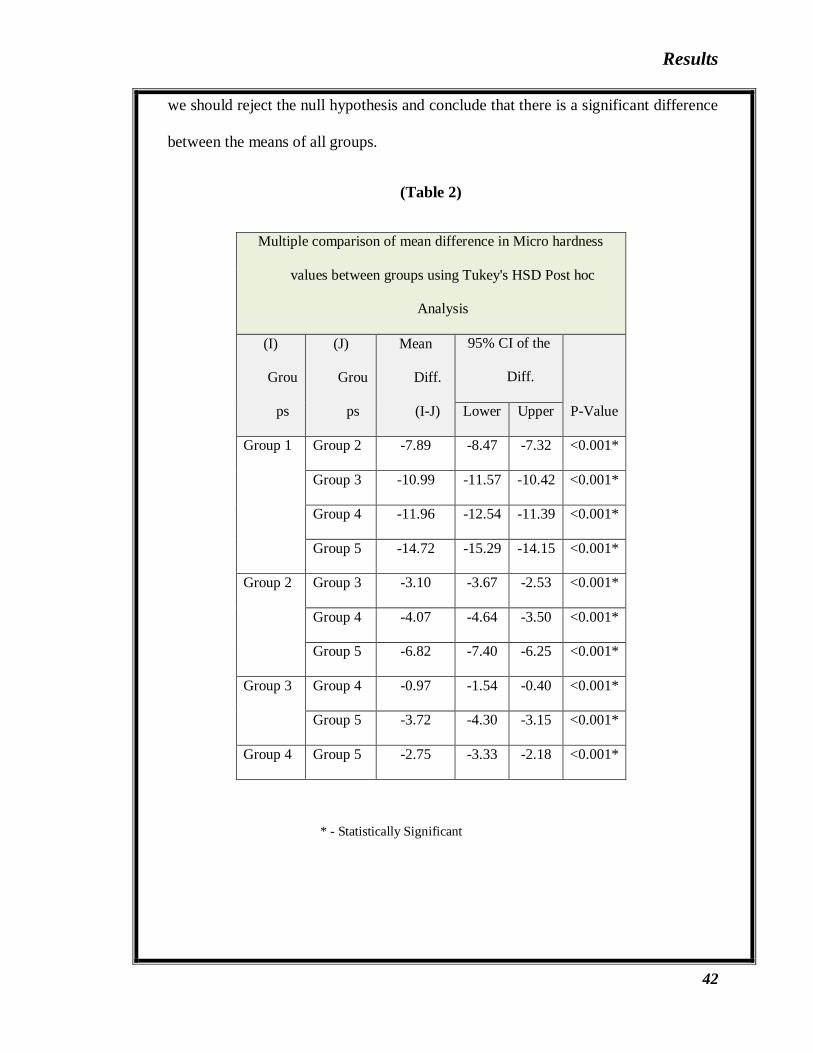
we should reject the null hypothesis and conclude that there is a significant difference
between the means of all groups.
(Table 2)
Multiple comparison of mean difference in Micro hardness
values between groups using Tukey's HSD Post hoc
Analysis
(I)
Grou
ps
(J)
Grou
ps
Mean
Diff.
(I-J)
95% CI of the
Diff.
P-Value Lower Upper
Group 1 Group 2 -7.89 -8.47 -7.32 <0.001*
Group 3 -10.99 -11.57 -10.42 <0.001*
Group 4 -11.96 -12.54 -11.39 <0.001*
Group 5 -14.72 -15.29 -14.15 <0.001*
Group 2 Group 3 -3.10 -3.67 -2.53 <0.001*
Group 4 -4.07 -4.64 -3.50 <0.001*
Group 5 -6.82 -7.40 -6.25 <0.001*
Group 3 Group 4 -0.97 -1.54 -0.40 <0.001*
Group 5 -3.72 -4.30 -3.15 <0.001*
Group 4 Group 5 -2.75 -3.33 -2.18 <0.001*
* - Statistically Significant

Results
43
The Tukey’s multiple comparisons between the five groups interprets that the
mean microhardness of EDTA differs significantly (p<0.001) from ClO2, QMix, and
Matricaria recutita.
(Graph 1)
All the irrigating solutions decreased the microhardness of root canal dentin
with the exclusion of the control group. The above represented graph shows a
significant difference between the microhardness of all five groups. EDTA exhibited
the highest reduction in root canal dentin microhardness followed by ClO2, QMix,
and German chamomile. The control group with saline showed the least reduction in
the microhardness of root canal dentin.
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
Group 1 Group 2 Group 3 Group 4 Group 5
50.94
58.8361.93 62.90
65.65
Mic
ro H
ard
nes
s V
alu
es
Comparison of mean Micro Hardness
values between 05 groups

Results
44
(Graph 2)
Represented above is a graph showing the average microhardness of dentin
when treated with various irrigants in Vicker’s microhardness numbers on Y-axis.
The tabulated results and the statistical analysis revealed that EDTA showed
the highest degree of reduction in dentin microhardness with a significant difference
of 23.47 % more reduction than Matricaria recutita, which showed the least amount
of dentin microhardness reduction with just a 4.18% difference than the control group
saline. Between ClO2 and QMix, and QMix and Matricaria recutita, there was only
5.26% and 1.51% difference respectively. But EDTA still showed a good 13.41%
higher reduction rate than ClO2.
50.94
58.8361.93 62.90
65.65
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
Group 1 Group 2 Group 3 Group 4 Group 5
Mic
ro H
ard
nes
s V
alu
es
Comparison of mean Micro Hardness
values [with standard errors] between 05
groups

Discussion
45
Long term prognosis of root canal treatment is entirely dependent on the quality
of instrumentation, irrigation, disinfection, and finally the obturation of the root canal
system. A root canal treatment is essentially deemed to be successful, once complete
debridement and disinfection has been achieved. It is a procedure that requires the
removal of irritants from the canal and the periapical tissues carried out in various
ways as the case demands, and includes the instrumentation of the canal, placement
of the medicament and irrigant.30
An irrigant plays a vital role in root canal therapy as they aid not only in
cleaning and shaping, but also in lubricating the canal while using endodontic
instruments. These solutions are required to be used simultaneously with each file
change to avoid unnecessary mishaps like, ledging, canal transportation, improper
cleaning and disinfection till the apex, or instrument separation. The use of chelating
agents as irrigants have helped in opening calcified and narrow canals for better
instrumentation, but at the same time it causes changes in the microstructure of dentin
and the Ca:P ratio which will in turn cause changes in the dentin solubility and
permeability characteristics.
Distilled water was initially used as an irrigant while preparing the canal of the
samples because it has no effect on the microhardness of root canal dentin surface,
thus not considering it as a variable which might affect the results.
This study used single rooted premolar teeth in order to obtain a standardisation
of the teeth and as they were more often extracted for orthodontic purposes, which
increased the chances of its ease of availability for research purposes. Premolars with
Discussion
46
straight canals were important as they are easy to instrument and the procedural errors
like ledging, zipping, apical transportation, and canal blockage can be avoided. To
ensure standardisation, the crown of the selected teeth were removed to maintain a
length of 18mm for each tooth as these served as a reservoir for the solvent to be
present inside the canal for more than the recommended exposure time.
Longitudinal sectioning of the teeth was preferred over cutting it transversally
into discs because as Cruz-Filho et al. in 2013 observed, it provides an accurate
representation of the clinical situations. 37 Ground polishing of the samples eliminated
any surface irregularities and provided a mirror like finish, as the glossy surface
ensures the reflection of light so that the indentation can be clearly visualised when
testing the Vicker’s hardness machine.
A possible limitation of the current study is that the experiments were
performed at room temperature and not body temperature.
An initial rinse with 3% NaOCl can affect the microhardness of root canal
dentin, so it can possible add to the chelating action of the irrigating solutions to be
evaluated; this could be a possible limitation of the present study. De-Deus et al in
2006 limited the contact time of chelator solutions to 5 minutes, stating that this
duration is more realistic in terms of clinical practice. Other researchers like Goldberg
et al in 1982 and Panighi et al in 1992 have suggested extending the application time
to 10 to 15 minutes to obtain optimum results.1
Sodium hypochlorite is known to have an extensive history in medicine and
dentistry and continues to be popular even today. When the Hypochlorous acid
Discussion
47
present in the NaOCl solution comes in contact with the organic tissue it acts as a
solvent and releases chlorine which has antimicrobial action and inhibiting bacterial
enzymes. NaOCl is an efficient organic solvent and has also been known to cause
dentin degeneration because of the dissolution of collagen by the breakdown of bonds
between carbon atoms and disorganisation of the protein primary structure, although
the degeneration of dentin is not as much as EDTA.
EDTA reacts with the calcium ions present in dentin and forms soluble calcium
chelates which decalcifies dentin to a depth of 20-30µm in 5 minutes. When 17%
EDTA is alternated with 5% NaOCl it causes a significant increase in tooth surface
strain which was not seen when used in conjunction with 3% NaOCl. The
consequence of chemical interactions between NaOCl and EDTA results in a loss of
free chlorine, which could explain the inability of their mixture to dissolve soft
tissues. But this was proved otherwise by studies conducted by Grawher et al. in
2003, Irala et al. in 2010, and Saquy et al. in 1994, which reported that the addition of
NaOCl did not alter EDTA’s ability to decalcify human dentin. Nygaard-Ostby in
1957 stated that even though EDTA was forced into the periapical tissues, no
periapical tissue damage could be detected even after 14 months. But on the contrary,
Segura et al. in 1996 showed that the extrusion of even a low concentration of EDTA
solution through the apical constriction can cause irreversible decalcification of
periapical bone and have consequences on the neuro-immunological regulatory
mechanisms.
Chlorhexidine digluconate has been widely used as a disinfectant because of its
excellent antimicrobial activity, but however completely lacks tissue dissolving

Discussion
48
capacity. It has the ability to bind to phosphate present in the structure of
hydroxyapatite which is present in the calcium carbonate complexes in dentin and this
leads to the release of small amounts of calcium from the root canal dentin. CHX also
reacts with EDTA to form a white precipitate, but the clinical significance of this
precipitate is largely unknown. It has been known to cause side effects like contact
dermatitis, desquamative gingivitis, teeth and tongue discolouration.
MTAD was developed as an irrigant by Torabinejad et al. which combined
both chelating and antimicrobial properties. It is a mixture of a detergent, citric acid
which removes the smear layer, making way for the antimicrobial action of
doxycycline in the dentinal tubules. Torabinejad et al. in 2003 stated that a 5 minute
final rinse with MTAD was appropriate after an initial rinse with NaOCl. But another
study by Gopikrishna et al. in 2010 contradicted this by stating that MTAD as a final
rinse reduced the sealing ability of sealers by precipitate formation.
Tetraclean was introduced as a final rinse with a lower concentration of
doxycycline than MTAD. However a study by Giardino et al. in 2007 stated that, only
5.25% NaOCl could result in complete biofilm disgregation, but Tetraclean showed
higher degree of biofilm disgregation than MTAD.38
Herbal products like Triphala, Propolis, Morinda citrifolia juice, green tea etc.
have been later introduced as possible endodontic irrigants with less potential side
effects on the dentin microhardness, even at higher concentrations aimed at removing
smear layer and disinfecting canals.
Discussion
49
Reduction in microhardness could be beneficial under clinical conditions since
it allows rapid preparation and negotiation of tight canals, and the degree of softening
and demineralisation can be an indication that there has been a complete removal of
smear layer which might act as a physical barrier that limits the antibacterial effects
of intracanal medicaments and root canal sealers. Moreover the removal of smear
layer further improves the retention of the root canal filling material. The penetration
of the root canal sealer enables to entomb the residual bacteria that the irrigants failed
to completely remove and also extends the antibacterial effect deep into the dentinal
tubules.37
In the present study, Vicker’s microhardness tester was preferred over Knoop
hardness test due to its suitability and practicality of the test for evaluating surface
changes occurring in the deeper dental hard tissues. This test is also widely accepted
because of its accurate readings and the fact that in this method, just one type of
indentation is used for all types of surface treatments.29
Microhardness testing of materials is usually done by applying small loads and
it is one of the simplest and non-destructive methods of its mechanical
characterisation and is measured as its resistance to the penetration of an indenter that
is harder than the standard to be analysed.32 These tests provide numerical values
which depend on several factors like Young’s modulus of a material, the yield stress
in compression, anisotropy, and thus it cannot be considered a basic property of a
material but rather an indication of the behaviour given the specific conditions of the
penetration test.27
Discussion
50
Based on the results of the present study, all the root canal irrigants reduced the
microhardness of root canal dentin except for the control group, saline. EDTA
showed a microhardness value of 50.94 which was significantly different and 15.48%
higher than ClO2 which showed a hardness value of 58.83. The fact that EDTA acts
efficiently in reduction of dentin microhardness is because of its chelating property
and there are several theories that attempt to explain this chemical reaction.
According to the Crystal Field Theory, the attraction force between the central metal
and the ligands is purely electrostatic. Therefore the attraction force exerted by the
metallic ion is greater than the repulsive force offered by the atoms of the EDTA
molecule. Chelators such as EDTA form a stable complex with the calcium ions in
the dentin and at the same moment the carboxyl ions of the EDTA molecule are
ionized, releasing hydrogen atoms that compete with the calcium ions.37
This result is in accordance with studies conducted by Saleh and Ettman in
1999 which evaluated the effect of EDTA and NaOCl on the microhardness of root
canal dentin and reported that both the solutions decreased the microhardness of root
canal dentin but EDTA irrigation induced more reduction.13 Rama et al., Keyur et al.,
and Anusree et al., in 2014 also stated that EDTA showed the highest amount of
reduction in dentin microhardness as compared to other irrigants used in their
studies.2,39,30 Baldasso et al., in 2017 reported that EDTA showed the highest
reduction in dentin microhardness compared to the other irrigants used in his study.33
Sousa and Silva, Khedmat and Shokouhenijad, and Da Silva et al in 2005 and 2008
respectively, have shown that EDTA facilitates chelation of the inorganic portion of
dentin. Regarding the depths under evaluation, the present study revealed similar
Discussion
51
results about the reduction in microhardness after irrigating with NaOCl followed by
EDTA.1 On the contrary, Kandil et al. in 2014 and Kara et al. in 2015 stated in their
studies that Maleic acid showed higher reduction in dentin microhardness than
EDTA.31,13 They concluded that significant alteration in dentin microhardness after
the irrigation treatment indicates potent direct effects of these chemical solutions on
the components of dentin structure.
The capacity of ClO2 in smear layer removal could be attributed to its low pH
i.e. 4.67 and in the present study, ClO2 also showed high reduction in dentin
microhardness although not more than EDTA. A previous study by Cruz-Filho et al.
in 2011 has suggested that the pH of an irrigant is indirectly proportional to the
demineralisation of root canal dentin. Also ClO2 being a weak acid, it is likely that it
will affect the dentin similar to other organic acids such as Maleic acid or Lactic acid
and it may cause a mineral gradient that could yield itself better to sealer
penetration.22 Another study by Anna et al. in 2013 demonstrated that high purity
ClO2 had the ability to eliminate intracanal biofilm and nearly all the bacteria thus
preventing re-infection in most cases, even more so than NaOCl and CHX when used
as disinfectants.41 Hence, high purity 0.2% chlorine dioxide was used in this study.
QMix being a novel irrigant showed minimum amount of reduction in dentin
microhardness. It is mainly composed of EDTA, CHX, and a surfactant; and the
addition of a surfactant to a chelating agent increases its ability to penetrate the dentin
easily.10 The results of the present study showed that QMix causes a 5% less
reduction in dentin microhardness than ClO2 with a mean microhardness value of
61.93, and a good 17% difference from EDTA. There is only one previous study by
Discussion
52
Aranda-Garcia et al. in 2013 that evaluated the effect of QMix on dentin
microhardness and found that there was no significant difference between QMix and
EDTA. This could be because of the EDTA present in QMix, thus resulting in a
similar reduction in dentin microhardness.31 A study by Tay et al. in 2010 has
reported that QMix completely removed the smear layer and the smear plugs but was
less aggressive than EDTA in that there is less demineralisation of the intact dentin
collagen. The study also showed the long shelf life of QMix, producing a continued
effect on the smear layer as well as its ability to kill resilient strains of Enterococcus
faecalis with induced accelerated aging at 60˚C for 8 weeks, which was the equivalent
of 2 years.42
An herbal product Matricaria recutita or German chamomile has been used
before as an effective natural irrigant which has shown a positive effect on smear
layer removal. In the present study German chamomile showed the least amount of
reduction in dentin microhardness with a good 19% less decrease in microhardness
than EDTA. A study by Hena et al. in 2015 reported that although 2% CHX had a
better effect on smear layer removal and canal disinfection, Matricaria recutita was
better in terms of it being a natural substance with fewer side effects, easy
availability, and a healthier and acceptable host response.15 Its superior medicinal
properties and effective smear layer removal could be attributed to its acidic
components like capric acid, caprylic aid, chlorogenic acid, o-caumaric acid, p-
caumaric acid, and dihydroxybenzoic acid in the extract, which also could be the
reason for the mild reduction in the dentin microhardness.14

Discussion
53
Since there are no studies that showcase the effect of Matricaria recutita on
dentin microhardness, this is the first study to compare and evaluate its difference in
the reduction of dentin microhardness from known irrigants like EDTA, ClO2, and
QMix.
The research focus is increasing more towards natural products for root canal
disinfection owing to their inherent properties like easy availability, cost-
effectiveness, increased shelf life, and low toxicity. Although only few natural
products have shown promising results, more combinations and various
concentrations can improve their efficacy and usage for root canal disinfection in a
bio-friendly way.
Conclusion
54
During cleaning and shaping procedure, the canals should be irrigated using
copious amounts NaOCl. Once the shaping is complete, a rinse with EDTA solution
ensures the removal of smear layer and the decreased application time will minimise
the chelating effect on the root canal dentin. After the smear layer removal procedure,
a final rinse with an antiseptic solution appears beneficial. Since NaOCl has also been
known to reduce the microhardness of root canal dentin, out of the previous irrigating
solutions like CHX, ClO2, MTAD, the herbal product German chamomile appears to
be the most promising agent for use as a final antiseptic irrigant as it produces the
least amount of reduction in the microhardness root canal dentin.
Under the limitations of the present study it was concluded that EDTA showed
the highest degree of reduction in microhardness of root canal dentin surface with an
application time of 5 min followed by ClO2, QMix, and Matricaria recutita
respectively.
Summary
55
Root canal therapy is deemed to be a success when complete debridement
and disinfection of the canal has been established. Although mechanical preparation
of the root canal is a necessity, the process produces a smear layer composed of
organic and inorganic substances. This layer occludes the dentinal orifices and
hinders the penetration of intracanal medicaments and sealers into the dentinal
tubules, thus affecting the fluid tight seal of the root canal system. Chelating agents
were introduced to eliminate microbes, dissolve organic tissue, and remove the smear
layer; but they have been known to cause reduction in microhardness of root canal
dentin.
Novel irrigants like QMix which is a combination of conventional irrigating
solutions like EDTA and CHX have been introduced, that produce the same effect as
conventional irrigants but with a lesser degree of decalcifying detrimental effects
affecting the root canal dentin. Irrigating solutions play a key role in the cleaning and
shaping of the root canal system by producing a chelating effect on the root canal
dentin as well as deliver antimicrobial properties into the root canal.
This study aimed to evaluate and compare the effect of novel root canal
irrigants like QMix and Matricaria recutita with conventional irrigants like EDTA and
ClO2, on the microhardness of root canal dentin. The null hypothesis is that there is
no difference between EDTA, QMix, ClO2, and Matricaria recutita on the
microhardness of root canal dentin.
Forty single rooted premolar teeth were selected in this study and stored in
hydrogen peroxide for a week and then normal saline until it was used. The root
Summary
55
canals were prepared using Protaper Universal files and distilled water for irrigation
to avoid unnecessary changes to the dentinal structure. Initial rinsing was done for 5
minutes using NaOCl and then the samples were treated with EDTA, ClO2, QMix,
and Matricaria recutita for another 5 minutes. The teeth were decoronated to ensure
standardization of 18mm and split longitudinally before embedding in acrylic resin.
The teeth were then randomly divided into 5 groups with 16 samples each. Group I-
EDTA, Group II- ClO2, Group III- QMix, Group IV- Matricaria recutita, Group V-
Saline.
Each sample was then subjected to a load of 100g for 15 seconds on the
Vicker’s hardness tester to obtain 3 readings for each sample in each group. The
results were tabulated and statistically analysed to obtain a mean result which
determined which of the irrigating solutions caused the most reduction in root canal
dentin microhardness. And it was concluded that EDTA caused the most reduction in
dentin microhardness followed by ClO2, QMix, and the herbal product Matricaria
recutita.

Bibliography
56
1. Sayin TC, Serper A, Cehreli ZC, Otlu HG. The effect of EDTA, EGTA, EDTAC,
and tetracycline-HCl with and without subsequent NaOCl treatment on the
microhardness of root canal dentin. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 2007;104(3):418-24
2. Kalluru RS, Kumar D, Ahmed S, Sathish ES, Jayaprakash T, Garlapati R et al.
Comparative evaluation of the effect of EDTA, EDTAC, NaOCl, and MTAD on
microhardness of human dentin. J Clin Diagn Res 2014;8(4):39-41
3. Dayal C, Sajjan GS, Subhash TS. An n vitro evaluation of microhardness of root
dentin prepared with different file types with 2.5% sodium hypochlorite. Endod
2016:23-9
4. Birajdar A, Sathe S, Srilata. Effect of different irrigating solutions on dentin
microhardness at the furcation area of mandibular molars. Int J Appl Dent Sci
2016;2(2):16-18
5. Qian W. Quantitative analysis of the effect of irrigation sequences on root canal
wall dentin erosion. J Endod 2011;37(10):1437-41
6. Saleh HAJ. Comparative evaluation of effect of irrigation solutions with various
exposure time on microhardness of root canal dentin. Iraq Dent J 2016;38(3):124-
8
7. Reyes LMT, Rodriguez CT. Characterization of endodontically treated dentin.
Rev Fac Odontol Univ Antioq 2014;25(2)
8. Qian W, Shen Y, Haapasalo M. Quantitative analysis of the effect of irrigant
solution sequences on dentin erosion. J Endod 2011;37(10):1437-41

Bibliography
57
9. Doumani M, Habib A, Doumani A, Seirawan MK, Sadeka MA, Alnofiai SR. The
applications of EDTA in Endodontics. J Dent Med Sci 2017;16(9):83-5
10. Gupta C, Singh G, Singh MP, Agarwal M, Singh KS, Mishra A. Effect of QMix,
BioPure MTAD, and Ethylenediaminetetraacetic acid on microhardness of root
canal dentin. Int J Prosthodont Res Dent 2017;7(1):17-20
11. Ballal NV, Khandewal D, Karthikeyan S, Somayaji K, Foschi F. Effect of
Chlorine Dioxide irrigating solution on the microhardness and surface roughness
of root canal dentin. Eur J Prosthodont Restor Dent 2015;23(4):173-8
12. Thangaraj DN, Ballal V, Acharya SR. Determination of calcium loss and its effect
on microhardness of root canal dentin following treatment with 17%
ethylenediaminetetraacetic acid solution at different time intervals. Endod
2015;20(5):9-15
13. Kandil HE, Labib AH, Alhadainy HA. Effect of different irrigant solutions on
microhardness and smear layer removal of root canal dentin. Tanta Dent J
2014;11:1-11
14. Venkateshbabu N, Anand S, Abarajithan M, Sheriff SO, Jacob PS, Sonia N.
Natural therapeutic options in endodontics. Open Dent J 2016;10:214-26
15. Rahman H, Chandra A. Microbiologic evaluation of Matricaria and Chlorhexidine
against E.faecalis and C.albicans. Indian J Dent 2015;6(2):60-8
16. Aslantas EE, Buzoglu HD, Altundasar E, Serper A. Effect of EDTA, sodium
hypochlorite, and chlorhexidine gluconate with or without surface modifiers on
dentin microhardness. J Endod 2014;40(6):876-9
Bibliography
58
17. De-Deus G, Paciornik S, Mauricio MHP. Evaluation of the effect of EDTA,
EDTAC and citric acid on the microhardness of root dentin. Int Endod J
2006;39:401-7
18. Patil CR, Uppin V. Effect of endodontic irrigating solutions on the microhardness
and roughness of root canal dentin. Indian J Dent Res 2011;22(1):22-7
19. Estrela C, Estrela CR, Barbin EL, Spano JC, Marchesan MA, Pecora JD.
Mechanism of action of sodium hypochlorite. Braz Dent J 2002;13(2):113-7
20. Varlan C, Dimitriu B, Varlan V, Bodnar D, Suciu I, Davila C et al. Current
opinions concerning the restoration of endodontically treated teeth. J Med Life
2009;2(2):165-72
21. Gao S, Cai S, Huang S, Qian L. Nano-scratch behaviour of human root canal wall
dentin lubricated with EDTA pastes. Tribol Int 2013;63:169-76
22. Kamalasanan RR, Devarasanahalli SV, Ashwathanarayana RM, Rashmi K,
Gowda Y, Nadig RR. Effect of 5% Chlorine Dioxide Irrigant on Micro Push-Out
Bond Strength of Resin Sealer to Radicular Dentin. J Clin Diagn Res
2017;11(5):49-53
23. Abuhaimed TS, Abou Neel EA. Sodium hypochlorite irrigation and its effect on
bond strength to dentin. BioMed Res Int 2017;1-8
24. Ballal NV, Mala K, Bhat KS. Evaluation of the effect of Maleic acid and
ethylenediaminetetraacetic acid on the microhardness and surface roughness of
human root canal dentin. J Endod 2010;36(8):1385-8
25. Bakr DK, Saleem SS, Amin BK. Effect of sodium hypochlorite, chlorhexidine
and EDTA on dentin microhardness. Zanco J Med Sci 2016;20(1):1175-9
Bibliography
59
26. Ghisi AC, Kopper PMP, Baldasso FER, Sturmer CP, Rossi-Fedele G, Steier L et
al. Effect of super-ozidized water, sodium hypochlorite and EDTA on dentin
microhardness. Braz Dent J 2014;25(4):420-4
27. Bhagwat SA, Lopez TA, Mandke LP. Comparison of the effect of
ethylenediaminetetraacetic acid, chlorhexidine, etidronic acid and propolis as an
irrigant on the microhardness of root dentin. J Dent Res Rev 2016;3(1):23-30
28. Massoud SF, Moussa SM, Hanafy SA, Backly RM. Evaluation of the
microhardness of root canal dentin after different irrigation protocols. Alex Dent J
2017;42:73-9
29. Saha SG, Sharma V, Bharadwaj A, Shrivastava P, Saha MK, Dubey S et al.
Effectiveness of various endodontic irrigants on the microhardness of the root
canal dentin. J Clin Diagn Res 2017;11(4):1-4
30. Das A, Kottoor J, Mathew J, Kumar S, George S. Dentin microhardness changes
following conventional and alternate irrigation regimens. J Conserv Dent
2014;17(6):546-9
31. Tuncer KA, Tuncer S, Siso Sh. Effect of QMix irrigant on the microhardness of
root canal dentin. Aust Dent J 2015;60:163-8
32. Aranda-Garcia AJ, Kuga MC, Chavez-Andrade GM, Kalatzis-Sousa NG, Duarte
MAH, Faria G et al. Effect of final irrigation protocols on microhardness and
erosion of root canal dentin. Microsc Res Tech 2013;76:1079-83
33. Baldasso FER, Roleto L, Silva VD, Morgental RD, Kopper PMP. Effect of
irrigation protocols on microhardness reduction and erosion of root canal dentin.
Braz Oral Res 2017;31(40):1-8
Bibliography
60
34. Rapgay T, Gupta P, Gupta H, Singh A, Jain A. Effect of different irrigating
solutions on root dentin microhardness. Acta Sci Dent Sci 2018;2(8):3-8
35. Cirano FR, Romito GA, Todescan JH. Determination of root dentin and
cementum microhardness. Braz J Oral Sci 2004;3(8):420-4
36. Chuenarrom C, Benjakul P, Daosodsai P. Effect of indentation load and time on
Knoope and Vicker’s microhardness tests for enamel and dentin. Mat Res
2009;12(4):473-6
37. Kesim B, Ustun Y, Delikan E, Gungor A. Effect of Chitosan on Sealer
Penetration into the Dentinal Tubules. Nig J Clin Prac 2018:1-7
38. Kandaswamy D, Venkateshbabu N. Root canal irrigants. J Cons Dent
2010;13(4):256-64
39. Chande KP, Manawar NU, Chandak MG, Lokade J, Chandak SR. Effect of
chelating agents and irrigants on mineral content of root canal dentin. Int J Clin
Prev Dent 2014;10(3):135-8
40. Hodge HC, McKay H. The microhardness of teeth. J Am Dent Assoc
1922;20(2):227-33
41. Solumium Dental Instructions.
42. Dai L, Khechen K, Khan S, Gillen B, Tay FR, Guttman JL. The effect of QMix;
an experimental antibacterial root canal irrigant, on the removal of canal wall
smear layer and debris. J Endod 2011;37(1):80-4
43. Ferrer-Luque CM, Perez-Heredia M, Baca P, Arias-Moliz MT, Gonzalez-
Rodriguez MP. Decalcifying effects of antimicrobial irrigating solutions on root
canal dentin. Med Oral Patol Oral Cir Bucal 2013;18(1):158-61
Bibliography
61
44. Ari H, Erdemir A. Effects of irrigation solutions on mineral content of root canal
dentin using ICP-AES technique. J Endod 2005;31(3):187-9
45. Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo M. Tissue dissolution by
sodium hypochlorite: Effect of concentration, temperature, agitation, and
surfactant. J Endod 2010:1-5
46. Zwick Roell. Vicker’s microhardness Tester.
47. Hulsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals:
shaping goals, techniques and means. Endod Top 2005;10(1):30-76
48. Haapsalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin N Am
2010;54:291-312
49. Khoshbin E, Donyavi Z, Atibeh EA, Roshanaei G, Amani F. The Effect of Canal
Preparation with Four Different Rotary Systems on Formation of Dentinal Cracks.
Iran Endod J 2018;13(2):163-8
Annexure
62
Annexure
63
Annexure
62

Annexure
63
Annexure
64
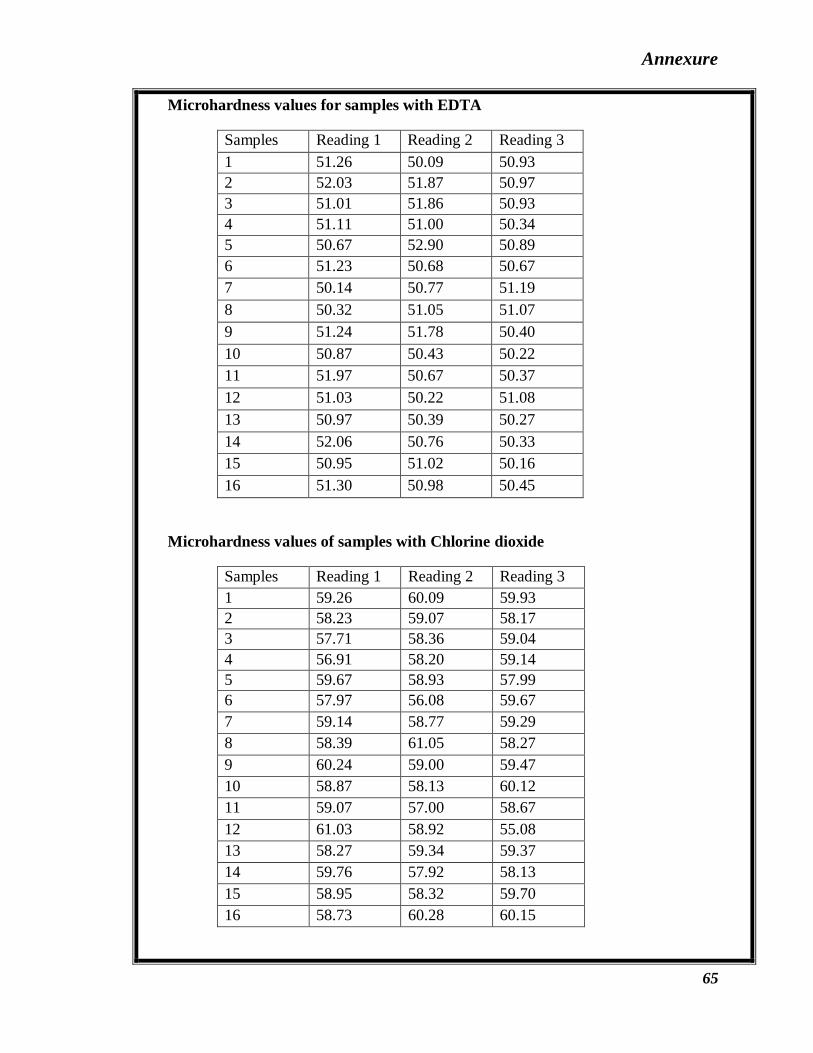
Annexure
65
Microhardness values for samples with EDTA
Samples Reading 1 Reading 2 Reading 3
1 51.26 50.09 50.93
2 52.03 51.87 50.97
3 51.01 51.86 50.93
4 51.11 51.00 50.34
5 50.67 52.90 50.89
6 51.23 50.68 50.67
7 50.14 50.77 51.19
8 50.32 51.05 51.07
9 51.24 51.78 50.40
10 50.87 50.43 50.22
11 51.97 50.67 50.37
12 51.03 50.22 51.08
13 50.97 50.39 50.27
14 52.06 50.76 50.33
15 50.95 51.02 50.16
16 51.30 50.98 50.45
Microhardness values of samples with Chlorine dioxide
Samples Reading 1 Reading 2 Reading 3
1 59.26 60.09 59.93
2 58.23 59.07 58.17
3 57.71 58.36 59.04
4 56.91 58.20 59.14
5 59.67 58.93 57.99
6 57.97 56.08 59.67
7 59.14 58.77 59.29
8 58.39 61.05 58.27
9 60.24 59.00 59.47
10 58.87 58.13 60.12
11 59.07 57.00 58.67
12 61.03 58.92 55.08
13 58.27 59.34 59.37
14 59.76 57.92 58.13
15 58.95 58.32 59.70
16 58.73 60.28 60.15
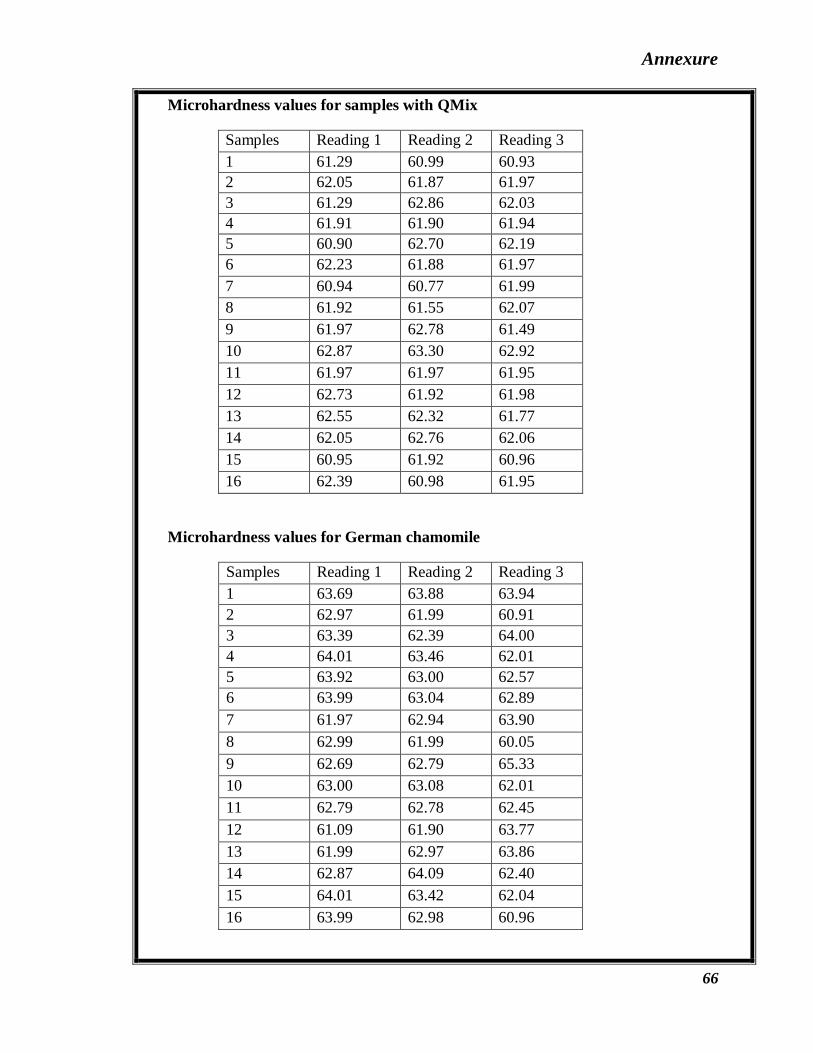
Annexure
66
Microhardness values for samples with QMix
Samples Reading 1 Reading 2 Reading 3
1 61.29 60.99 60.93
2 62.05 61.87 61.97
3 61.29 62.86 62.03
4 61.91 61.90 61.94
5 60.90 62.70 62.19
6 62.23 61.88 61.97
7 60.94 60.77 61.99
8 61.92 61.55 62.07
9 61.97 62.78 61.49
10 62.87 63.30 62.92
11 61.97 61.97 61.95
12 62.73 61.92 61.98
13 62.55 62.32 61.77
14 62.05 62.76 62.06
15 60.95 61.92 60.96
16 62.39 60.98 61.95
Microhardness values for German chamomile
Samples Reading 1 Reading 2 Reading 3
1 63.69 63.88 63.94
2 62.97 61.99 60.91
3 63.39 62.39 64.00
4 64.01 63.46 62.01
5 63.92 63.00 62.57
6 63.99 63.04 62.89
7 61.97 62.94 63.90
8 62.99 61.99 60.05
9 62.69 62.79 65.33
10 63.00 63.08 62.01
11 62.79 62.78 62.45
12 61.09 61.90 63.77
13 61.99 62.97 63.86
14 62.87 64.09 62.40
15 64.01 63.42 62.04
16 63.99 62.98 60.96
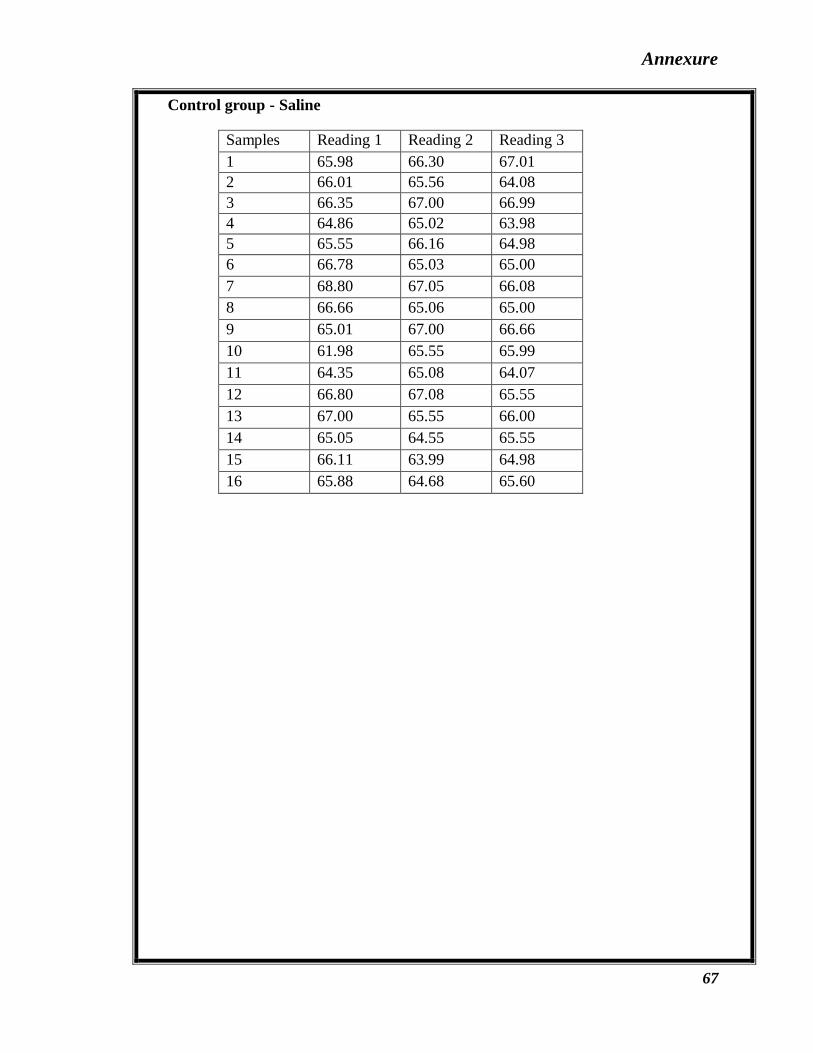
Annexure
67
Control group - Saline
Samples Reading 1 Reading 2 Reading 3
1 65.98 66.30 67.01
2 66.01 65.56 64.08
3 66.35 67.00 66.99
4 64.86 65.02 63.98
5 65.55 66.16 64.98
6 66.78 65.03 65.00
7 68.80 67.05 66.08
8 66.66 65.06 65.00
9 65.01 67.00 66.66
10 61.98 65.55 65.99
11 64.35 65.08 64.07
12 66.80 67.08 65.55
13 67.00 65.55 66.00
14 65.05 64.55 65.55
15 66.11 63.99 64.98
16 65.88 64.68 65.60

Annexure
68
Annexure
62
Microhardness values for samples with EDTA
Samples Reading 1 Reading 2 Reading 3
Microhardness values of samples with Chlorine dioxide
Samples Reading 1 Reading 2 Reading 3

Annexure
63
Microhardness values for samples with QMix
Samples Reading 1 Reading 2 Reading 3
Microhardness values for German chamomile
Samples Reading 1 Reading 2 Reading 3

Annexure
64
Control group - Saline
Samples Reading 1 Reading 2 Reading 3
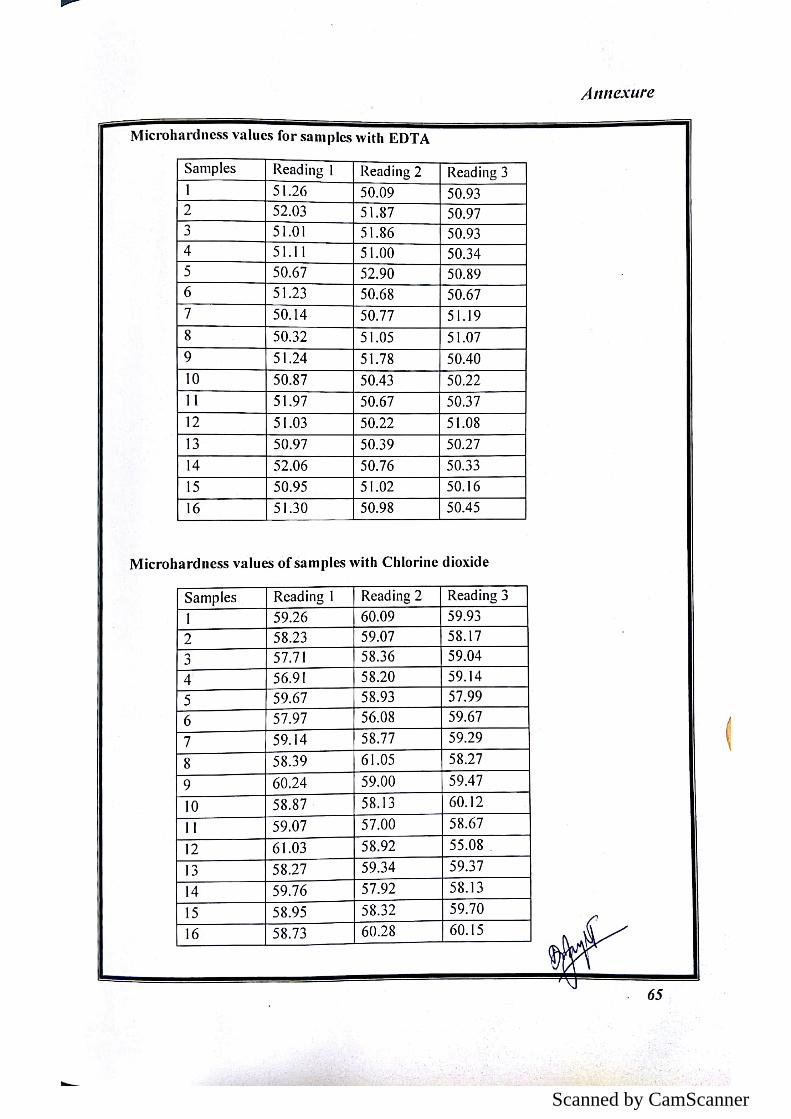
Scanned by CamScanner
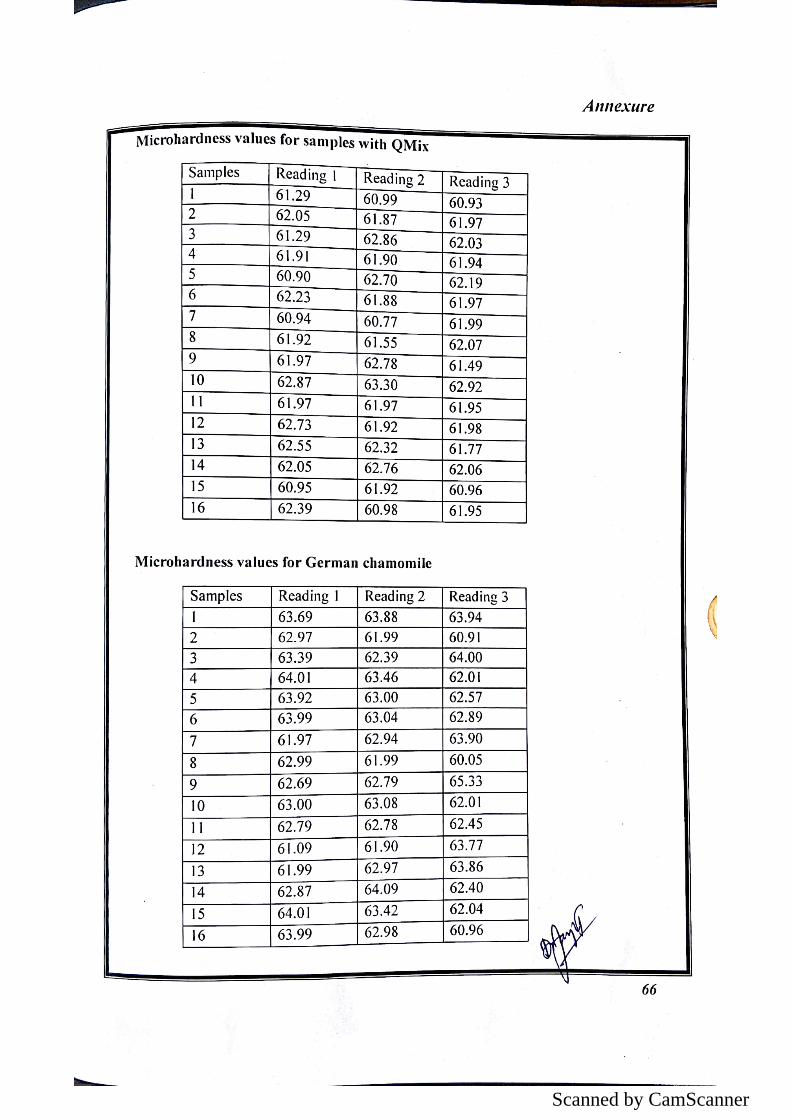
Scanned by CamScanner
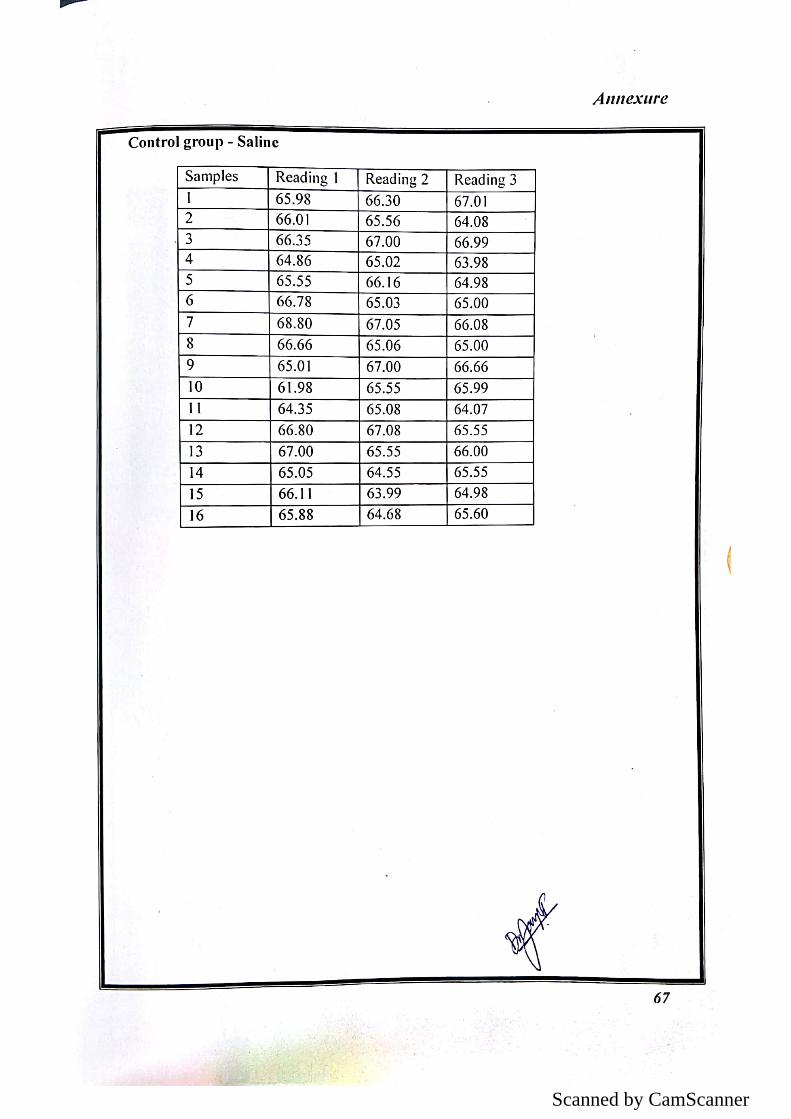
Scanned by CamScanner
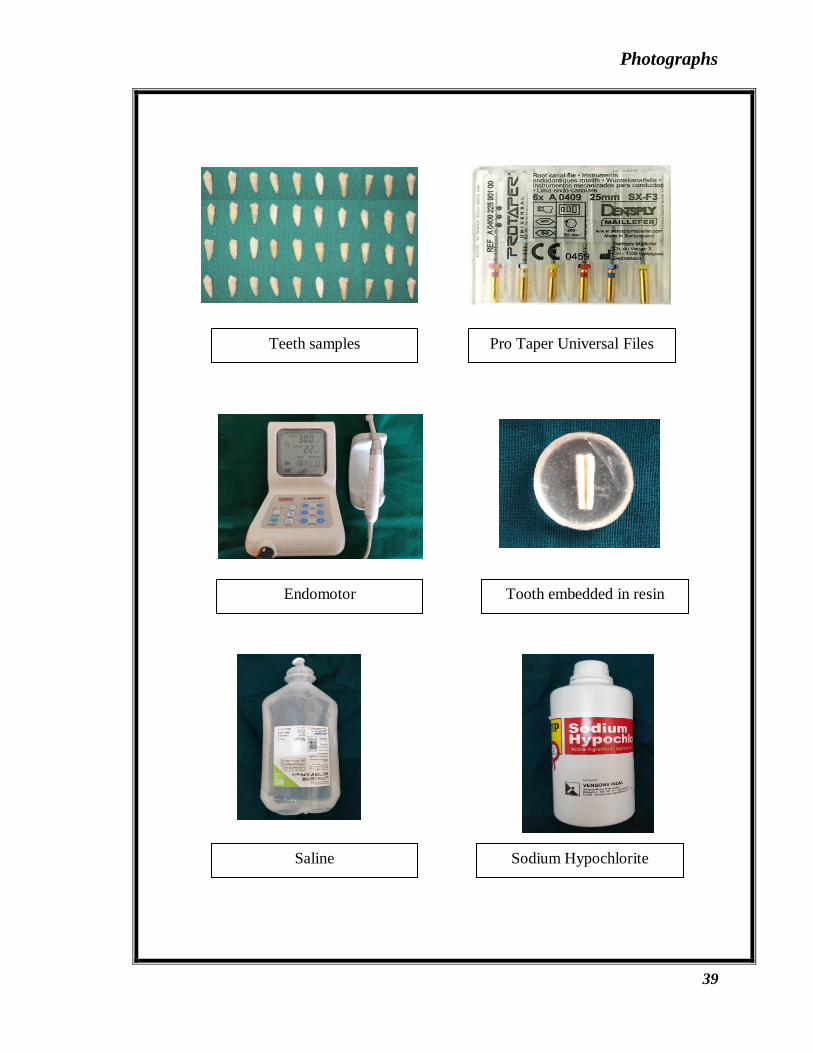
Photographs
39
Teeth samples Pro Taper Universal Files
Endomotor Tooth embedded in resin
Saline
Sodium Hypochlorite

Photographs
40
EDTA
Matricaria recutita seeds
Chlorine dioxide
Application of irrigants
Vicker’s microhardness test
QMix 2in1 solution

Photographs
41