an evaluation of incisor relapse in premolar...
TRANSCRIPT
ANAHTAR KELİMELER Relaps, Çekimli tedavi, Çekimsiz tedavi, Kesici
çapraşıklığı
Amaç: Bu çalışmanın amacı, maksiller ve mandibuler dental arklardaki relapsı belirlemek ve alt ve üst kesici diş çapraşıklığıyla ilişkili faktörleri ortaya koymak için dört I.premolar çekimli ve çekimsiz hastalardaki retansiyon sonrası kısa dönemde görülen değişiklikle-ri incelemektir.Bireyler ve Yöntem: 15 olgu dört I.premolar çekimiy-le ve 30 olgu çekimsiz olarak tedavi edildi. 45 olgu-nun tümüne edgewise mekanoterapisi uygulanmıştır. Lateral sefalometrik filmler ve dental modeller tedavi öncesi (T0), tedavi sonrası (T1) ve ortalama 3 yıllık retansiyon sonrası (T2) dönemde değerlendirilmiştir. Maksiller ve mandibuler çapraşıklık indeksi, interkanin ark genişliği ve ark uzunluğu dental modeller üzerinde ölçülmüştür. Sefalometrik filmler üzerinde, büyüme yönünü gösteren açılar (FMA, GoGnSN, Y-Aksı açıla-rı), üst ve alt kesici eğimleri (U1-SN, U1-APog ve L1-APog, IMPA açıları), overjet ve overbite ölçülmüştür. Grupiçi ve gruplar arası farklılıklar eşleştirilmiş t-testi, Wilcoxon, Student t-testi ve Mann-Whitney U testi kullanılarak test edilmiştir. Olası ilişkiler Spearman korelasyon analizi ile değerlendirilmiştir. Bulgular: T2 döneminde, çekimli ve çekimsiz tedavi gruplarının maksiller ve mandibuler arklarında orta-lama 3 mm’lik çapraşıklık oluşmuştur. Postretansiyon dönemde, mandibuler interkanin genişlikteki ekspan-siyon orijinal değerine dönme eğilimindeydi. Maksiller ve mandibuler ark uzunlukları postretansiyon takipte azalmaya devam etmiştir.Sonuçlar: Retansiyon sonrası çapraşıklık artışı, kıs-men interkanin genişlikteki postretansiyon azalmayla ilişkili olabilir. Tedaviyle oluşturulan alt kesici prokli-nasyonunun, retansiyon sonrasındaki alt kesici çapra-şıklığı artışı üzerine etkisi yok gibi gözükmektedir.
ÖZET
KEYWORDSRelapse, Extraction therapy, Nonextraction therapy,
Incisor crowding
ABSTRACT
Objective: The purpose of this study was to evaluate the short-term postretention changes in four first premolar extraction and nonextraction patients to detect relapse in maxillary and mandibular dental arches and consider the associated factors with upper and lower incisor crowding. Subjects and Method: 15 cases were treated by four first premolar extraction and 30 cases without extraction. All of the 45 cases had undergone edge-wise mechanotheraphy. Lateral cephalometric films and dental models were assessed at pretreatment (T0), posttreatment (T1) and an average of 3 years postretention (T2). On dental models, maxillary and mandibular irregularity index, intercanine width and arch length were calculated. On lateral cephalomet-ric films, the angles indicating facial growth directi-on (FMA, GoGnSN, Y-Axis angles), upper and lower incisor inclinations (U1-SN, U1-APog and L1-APog, IMPA angles), overjet and overbite were measured. Intragroup and intergroup differences were tested by using paired t-test, Wilcoxon, Student’s t-test and Mann-Whitney U tests. Spearman correlation analy-sis was used to evaluate the possible associations.Results: An average of 3 mm of crowding occured at T2 in maxillary and mandibular arches of the extraction and nonextraction treatment groups. Expansion of mandibular intercanine width tended to return to its original value at the postretention. Maxillary and mandibular arch lengths continued to decrease at the postretention follow-up. Conclusion: Postretention irregularity increase see-med to be partly associated with postretention decrease in the intercanine width. Proclination of mandibular incisors during treatment seemed to have no effect on postretention increase in lower incisor irregularity.
Hacettepe Dişhekimliği Fakültesi DergisiCilt: 29, Sayı: 1, Sayfa: 12-23, 2005
An Evaluation of Incisor Relapse in Premolar Extraction and Nonextraction
Patients
Premolar Çekimli ve Çekimsiz Hastalarda Kesici Relapsının Değerlendirilmesi
*Tülin (Uğur) TANER DDS, PhD, **Semra CİĞER DDS, PhD, ***Derya GERMEÇ DDS
* Associate Professor; Hacettepe University, Faculty of Dentistry, Department of Orthodontics ** Professor; Hacettepe University, Faculty of Dentistry, Department of Orthodontics
*** Research Asistant; Hacettepe University, Faculty of Dentistry, Department of Orthodontics
ARAŞTIRMA (Research)

13
INTRODUCTION
Stability of anterior dental arch alignment has always been a challenge facing the clinical ort-hodontist. Postretention relapse of anterior teeth especially recrowding of incisors occur in most of the cases following orthodontic treatment.
Studies were mainly based on extraction 1-10 and nonextraction 11-18 type of treatment. Few authors compared the effects of extraction and nonextraction edgewise treatments in Class II patients 19-21.
Stability of the lower arch was focused in most of the studies and many factors have been described concerning the lower incisor instabi-lity such as; expansion of the lower intercanine width 11,15,21-23 , proclination of lower incisors 24-
29 , arch length change 30 , pretreatment incisor irregularity 21,23 , incisor shape and dimension 31 , periodontal fiber pull 32-34 , direction of mandibu-lar growth 35-39 , late mandibular anterior growth 9 , perioral musculature 37 and third molars 40,41 . However, there is no consensus on the effect and cause relationship to date.
Few data is available evaluating the postreten-tion maxillary incisor crowding 9,15, 22,42-45 . Pret-reatment rotational displacement of maxillary in-cisors were reported to be a significant risk factor for postretention relapse of alignment 44 .
The causes of postorthodontic change invol-ves dental relapse, continued growth and the aging process 29 . Arch length and width cons-triction with time is a normal phsiologic process that routinely occurs following orthodontic tre-atment 1,3,4,12 . The same process occurs with the untreated patient as evidenced by studies of untreated occlusions 46-49 . Thus, it is necessary to differentiate the maturational growth changes from early relapse changes and should not be considered as a failure of orthodontic treatment 11,39 .
The purpose of the present study was to eva-luate the short-term postretention changes in four first premolar extraction and nonextraction patients to detect relapse in maxillary and man-dibular dental arches and consider the associated factors with upper and lower incisor crowding.
SUBJECTS AND METHOD
Two thousand and four hundred patients tre-ated by faculty members or graduate students of the Department of Orthodontics at the Univer-sity of Hacettepe were evaluated. Patients with complete records at the beginning (T0), and end of orthodontic treatment (T1) were recalled for a follow-up examination time of at least two years after orthodontic treatment (T2). Patients trea-ted with palatal expansion, functional appliances or orthognathic surgery were excluded from the study. 65 patients agreed to participate in this study. 20 of them were eliminated because of low-quality cephalograms and models. 45 pati-ents (30 nonextraction, 15 extraction) who had high quality cephalograms and models at T0, T1,
T2 time periods comprised the study sample. The pretreatment malocclusions of the nonext-raction group consisted of 11 Class I, 16 Class II Div 1 and 3 Class II Div II malocclusions. In the extraction group there were 13 Class I and 2 Class II Div 1 malocclusions. All subjects were treated by upper and lower fixed appliance the-rapy. Four first premolars were removed in the extraction group. All subjects had acceptable orthodontic results at T1 considering crowding, molar relationship, intercuspation, incisor rela-tionship and tooth alignment as determined by subjective evaluation of two experienced faculty members at the University of Hacettepe, Depart-ment of Orthodontics.
The mean ages of the patients in the extracti-on group were 14.5 ± 2.8 years with a range of 10 to 20 years at T0. The mean treatment time was 2.7 ± 1 years followed by a mean retention time of 1.3 ± 0.5 years. The mean postretenti-on time of the extraction group was 4.3 ± 3.5 years.
In the nonextraction group, mean ages of the patients were 13.6 ± 3.8 years with a range of 10 to 24 years at T0. The mean treatment time was 2.4 ± 1 years followed by a mean retention time of 1.2 ± 0.3 years. The mean postretention time of the nonextraction group was 2.8 ± 1.4 years.
14
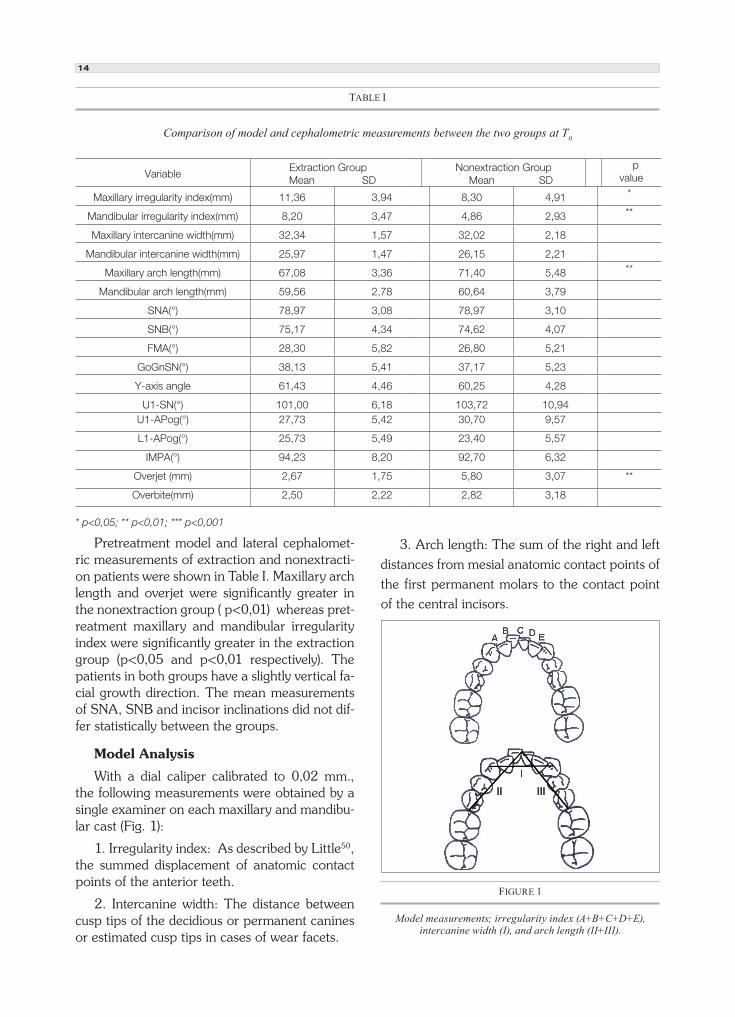
Pretreatment model and lateral cephalomet-ric measurements of extraction and nonextracti-on patients were shown in Table I. Maxillary arch length and overjet were significantly greater in the nonextraction group ( p<0,01) whereas pret-reatment maxillary and mandibular irregularity index were significantly greater in the extraction group (p<0,05 and p<0,01 respectively). The patients in both groups have a slightly vertical fa-cial growth direction. The mean measurements of SNA, SNB and incisor inclinations did not dif-fer statistically between the groups.
Model Analysis
With a dial caliper calibrated to 0,02 mm., the following measurements were obtained by a single examiner on each maxillary and mandibu-lar cast (Fig. 1):
1. Irregularity index: As described by Little50, the summed displacement of anatomic contact points of the anterior teeth.
2. Intercanine width: The distance between cusp tips of the decidious or permanent canines or estimated cusp tips in cases of wear facets.
3. Arch length: The sum of the right and left
distances from mesial anatomic contact points of
the first permanent molars to the contact point
of the central incisors.
TABLE I
Comparison of model and cephalometric measurements between the two groups at T0
VariableExtraction Group
Mean SDNonextraction Group Mean SD
p value
Maxillary irregularity index(mm) 11,36 3,94 8,30 4,91 *
Mandibular irregularity index(mm) 8,20 3,47 4,86 2,93 **
Maxillary intercanine width(mm) 32,34 1,57 32,02 2,18
Mandibular intercanine width(mm) 25,97 1,47 26,15 2,21
Maxillary arch length(mm) 67,08 3,36 71,40 5,48 **
Mandibular arch length(mm) 59,56 2,78 60,64 3,79
SNA(°) 78,97 3,08 78,97 3,10
SNB(°) 75,17 4,34 74,62 4,07
FMA(°) 28,30 5,82 26,80 5,21
GoGnSN(°) 38,13 5,41 37,17 5,23
Y-axis angle 61,43 4,46 60,25 4,28
U1-SN(°) 101,00 6,18 103,72 10,94U1-APog(°) 27,73 5,42 30,70 9,57
L1-APog(°) 25,73 5,49 23,40 5,57
IMPA(°) 94,23 8,20 92,70 6,32
Overjet (mm) 2,67 1,75 5,80 3,07 **
Overbite(mm) 2,50 2,22 2,82 3,18
* p<0,05; ** p<0,01; *** p<0,001
FIGURE 1
Model measurements; irregularity index (A+B+C+D+E), intercanine width (I), and arch length (II+III).
15
Cephalometric Analysis
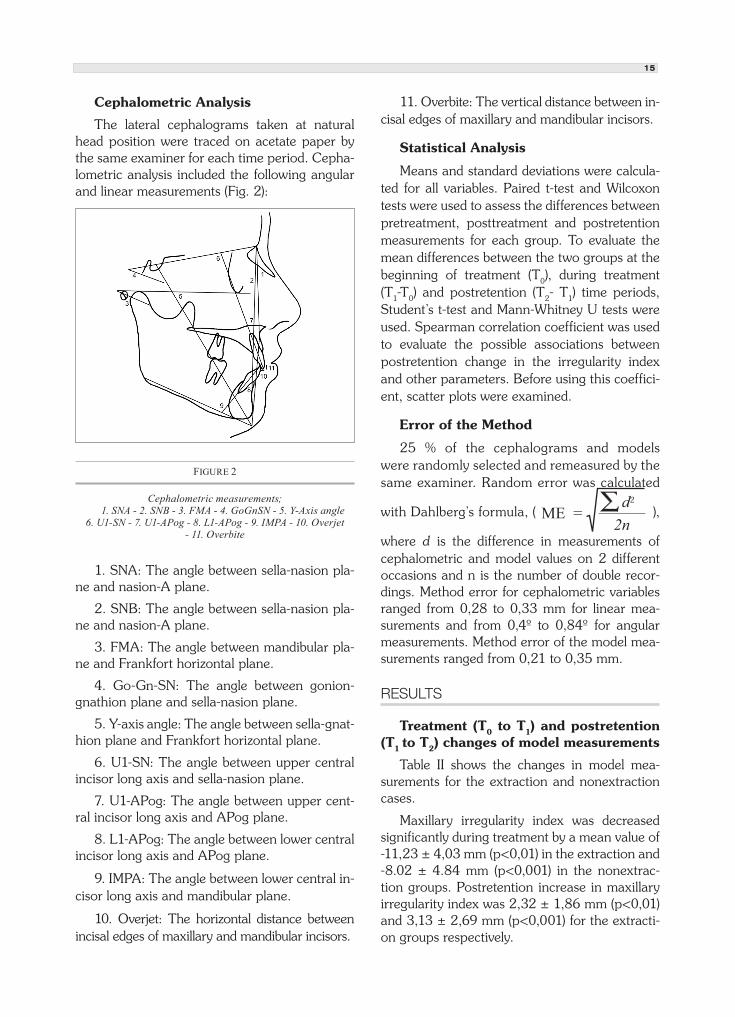
The lateral cephalograms taken at natural head position were traced on acetate paper by the same examiner for each time period. Cepha-lometric analysis included the following angular and linear measurements (Fig. 2):
1. SNA: The angle between sella-nasion pla-ne and nasion-A plane.
2. SNB: The angle between sella-nasion pla-ne and nasion-A plane.
3. FMA: The angle between mandibular pla-ne and Frankfort horizontal plane.
4. Go-Gn-SN: The angle between gonion-gnathion plane and sella-nasion plane.
5. Y-axis angle: The angle between sella-gnat-hion plane and Frankfort horizontal plane.
6. U1-SN: The angle between upper central incisor long axis and sella-nasion plane.
7. U1-APog: The angle between upper cent-ral incisor long axis and APog plane.
8. L1-APog: The angle between lower central incisor long axis and APog plane.
9. IMPA: The angle between lower central in-cisor long axis and mandibular plane.
10. Overjet: The horizontal distance between incisal edges of maxillary and mandibular incisors.
11. Overbite: The vertical distance between in-cisal edges of maxillary and mandibular incisors.
Statistical Analysis
Means and standard deviations were calcula-ted for all variables. Paired t-test and Wilcoxon tests were used to assess the differences between pretreatment, posttreatment and postretention measurements for each group. To evaluate the mean differences between the two groups at the beginning of treatment (T0), during treatment (T1-T0) and postretention (T2- T1) time periods,
Student’s t-test and Mann-Whitney U tests were used. Spearman correlation coefficient was used to evaluate the possible associations between postretention change in the irregularity index and other parameters. Before using this coeffici-ent, scatter plots were examined.
Error of the Method
25 % of the cephalograms and models were randomly selected and remeasured by the same examiner. Random error was calculated
with Dahlberg’s formula, ( ),
where d is the difference in measurements of cephalometric and model values on 2 different occasions and n is the number of double recor-dings. Method error for cephalometric variables ranged from 0,28 to 0,33 mm for linear mea-surements and from 0,4º to 0,84º for angular measurements. Method error of the model mea-surements ranged from 0,21 to 0,35 mm.
RESULTS
Treatment (T0 to T1) and postretention (T1 to T2) changes of model measurements
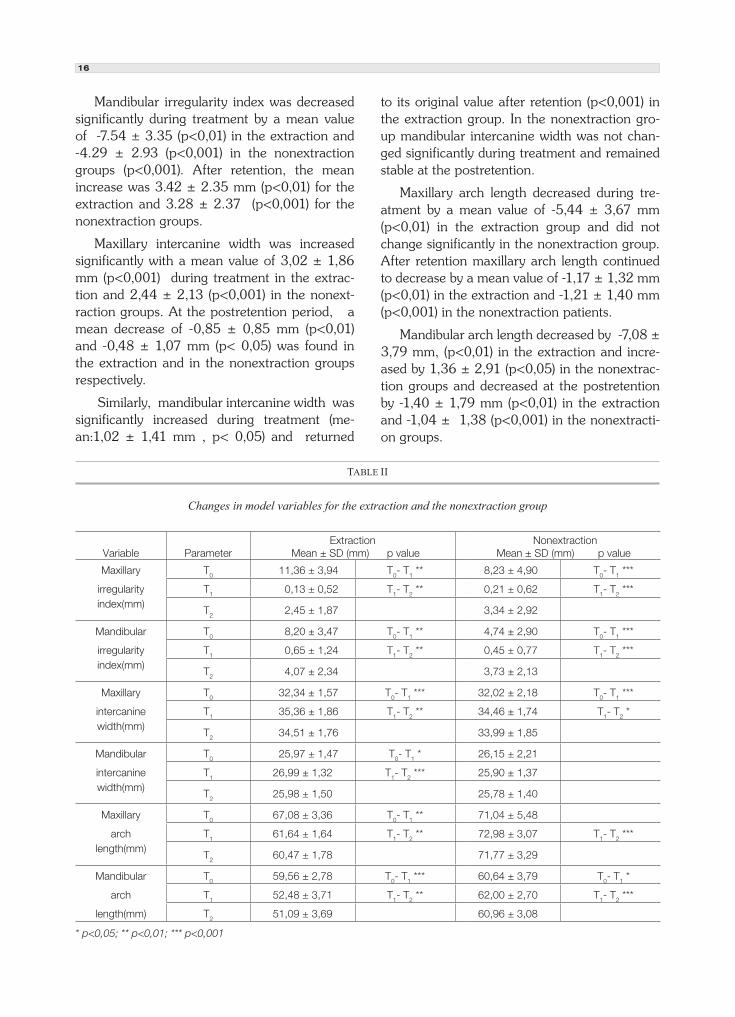
Table II shows the changes in model mea-surements for the extraction and nonextraction cases.
Maxillary irregularity index was decreased significantly during treatment by a mean value of -11,23 ± 4,03 mm (p<0,01) in the extraction and -8.02 ± 4.84 mm (p<0,001) in the nonextrac-tion groups. Postretention increase in maxillary irregularity index was 2,32 ± 1,86 mm (p<0,01) and 3,13 ± 2,69 mm (p<0,001) for the extracti-on groups respectively.
FIGURE 2
Cephalometric measurements; 1. SNA - 2. SNB - 3. FMA - 4. GoGnSN - 5. Y-Axis angle 6. U1-SN - 7. U1-APog - 8. L1-APog - 9. IMPA - 10. Overjet
- 11. Overbite
ME = d2
2n
16
Mandibular irregularity index was decreased significantly during treatment by a mean value of -7.54 ± 3.35 (p<0,01) in the extraction and -4.29 ± 2.93 (p<0,001) in the nonextraction groups (p<0,001). After retention, the mean increase was 3.42 ± 2.35 mm (p<0,01) for the extraction and 3.28 ± 2.37 (p<0,001) for the nonextraction groups.
Maxillary intercanine width was increased significantly with a mean value of 3,02 ± 1,86 mm (p<0,001) during treatment in the extrac-tion and 2,44 ± 2,13 (p<0,001) in the nonext-raction groups. At the postretention period, a mean decrease of -0,85 ± 0,85 mm (p<0,01) and -0,48 ± 1,07 mm (p< 0,05) was found in the extraction and in the nonextraction groups respectively.
Similarly, mandibular intercanine width was significantly increased during treatment (me-an:1,02 ± 1,41 mm , p< 0,05) and returned
to its original value after retention (p<0,001) in the extraction group. In the nonextraction gro-up mandibular intercanine width was not chan-ged significantly during treatment and remained stable at the postretention.
Maxillary arch length decreased during tre-atment by a mean value of -5,44 ± 3,67 mm (p<0,01) in the extraction group and did not change significantly in the nonextraction group. After retention maxillary arch length continued to decrease by a mean value of -1,17 ± 1,32 mm (p<0,01) in the extraction and -1,21 ± 1,40 mm (p<0,001) in the nonextraction patients.
Mandibular arch length decreased by -7,08 ± 3,79 mm, (p<0,01) in the extraction and incre-ased by 1,36 ± 2,91 (p<0,05) in the nonextrac-tion groups and decreased at the postretention by -1,40 ± 1,79 mm (p<0,01) in the extraction and -1,04 ± 1,38 (p<0,001) in the nonextracti-on groups.
TABLE II
Changes in model variables for the extraction and the nonextraction group
Variable ParameterExtraction
Mean ± SD (mm) p value Nonextraction
Mean ± SD (mm) p value
Maxillary T0 11,36 ± 3,94 T0- T1 ** 8,23 ± 4,90 T0- T1 ***
irregularity T1 0,13 ± 0,52 T1- T2 ** 0,21 ± 0,62 T1- T2 ***index(mm)
T2 2,45 ± 1,87 3,34 ± 2,92
Mandibular T0 8,20 ± 3,47 T0- T1 ** 4,74 ± 2,90 T0- T1 ***
irregularity T1 0,65 ± 1,24 T1- T2 ** 0,45 ± 0,77 T1- T2 ***index(mm)
T2 4,07 ± 2,34 3,73 ± 2,13
Maxillary T0 32,34 ± 1,57 T0- T1 *** 32,02 ± 2,18 T0- T1 ***
intercanine T1 35,36 ± 1,86 T1- T2 ** 34,46 ± 1,74 T1- T2 *width(mm)
T2 34,51 ± 1,76 33,99 ± 1,85
Mandibular T0 25,97 ± 1,47 T0- T1 * 26,15 ± 2,21
intercanine T1 26,99 ± 1,32 T1- T2 *** 25,90 ± 1,37width(mm)
T2 25,98 ± 1,50 25,78 ± 1,40
Maxillary T0 67,08 ± 3,36 T0- T1 ** 71,04 ± 5,48
arch T1 61,64 ± 1,64 T1- T2 ** 72,98 ± 3,07 T1- T2 ***length(mm)
T2 60,47 ± 1,78 71,77 ± 3,29
Mandibular T0 59,56 ± 2,78 T0- T1 *** 60,64 ± 3,79 T0- T1 *
arch T1 52,48 ± 3,71 T1- T2 ** 62,00 ± 2,70 T1- T2 ***
length(mm) T2 51,09 ± 3,69 60,96 ± 3,08
* p<0,05; ** p<0,01; *** p<0,001
17
TABLE III
Changes in cephalometric variables for the extraction and the nonextraction group
Variable Parameter Extraction
Mean ± SD p value Nonextraction
Mean ± SD p value
SNA ( º ) T0 78,97 ± 3,08 T0- T1 ** 78,97 ± 3,10
T1 77,13 ± 3,28 T1- T2 * 78,17 ± 3,43
T2 77,77 ± 3,43 78,27 ± 3,53
SNB ( º ) T0 75,17 ± 4,34 T0- T1** 74,62 ± 4,07
T1 73,67 ± 5,03 75,10 ± 3,58
T2 74,30 ± 5,33 75,47 ± 3,69
FMA ( º ) T0 28,30 ± 5,82 26,80 ± 5,21
T1 29,43 ± 6,65 27,03 ± 5,96 T1- T2 *
T2 29,10 ± 6,90 26,37 ± 5,94
GoGnSN ( º ) T0 38,13 ± 5,41 37,17 ± 5,23
T1 39,93 ± 7,08 36,78 ± 5,58
T2 38,90 ± 7,36 36,27 ± 5,86
Y-axis angle ( º ) T0 61,43 ± 4,46 T0- T1 * 60,25 ± 4,28
T1 62,50 ± 4,37 60,88 ± 4,88
T2 62,67 ± 4,69 60,82 ± 4,62
U1-SN ( º ) T0 101,00 ± 6,18 103,72 ± 10,94
T1 101,50 ± 9,52 103,82 ± 7,78
T2 101,57 ± 8,77 103,92 ± 7,59
U1-APog ( º ) T0 27,73 ± 5,42 30,70 ± 9,57
T1 28,27 ± 6,54 28,43 ± 4,35
T2 27,40 ± 6,10 28,23 ± 4,40
L1-APog ( º ) T0 25,73 ± 5,49 23,40 ± 5,57 T0- T1 ***
T1 26,20 ± 4,58 27,85 ± 5,50
T2 25,23 ± 4,77 28,08 ± 5,36
IMPA ( º ) T0 94,23 ± 8,20 92,70 ± 6,32 T0- T1 *
T1 93,03 ± 7,61 95,13 ± 6,88
T2 92,27 ± 7,91 96,28 ± 6,81
Overjet (mm) T0 2,67 ± 1,75 5,80 ± 3,07 T0- T1 ***
T1 2,67 ± 0,98 T1- T2 * 2,73 ± 0,69 T1- T2 **
T2 3,10 ± 1,27 3,28 ± 1,06
Overbite (mm) T0 2,50 ± 2,22 2,82 ± 3,18
T1 2,23 ± 1,03 2,58 ± 1,00
T2 2,57 ± 1,39 2,55 ± 1,60
* p<0,05; ** p<0,01; *** p<0,001

18
Treatment (T0 to T1) and postretenti-on (T1 to T2) changes of cephalometric measurements
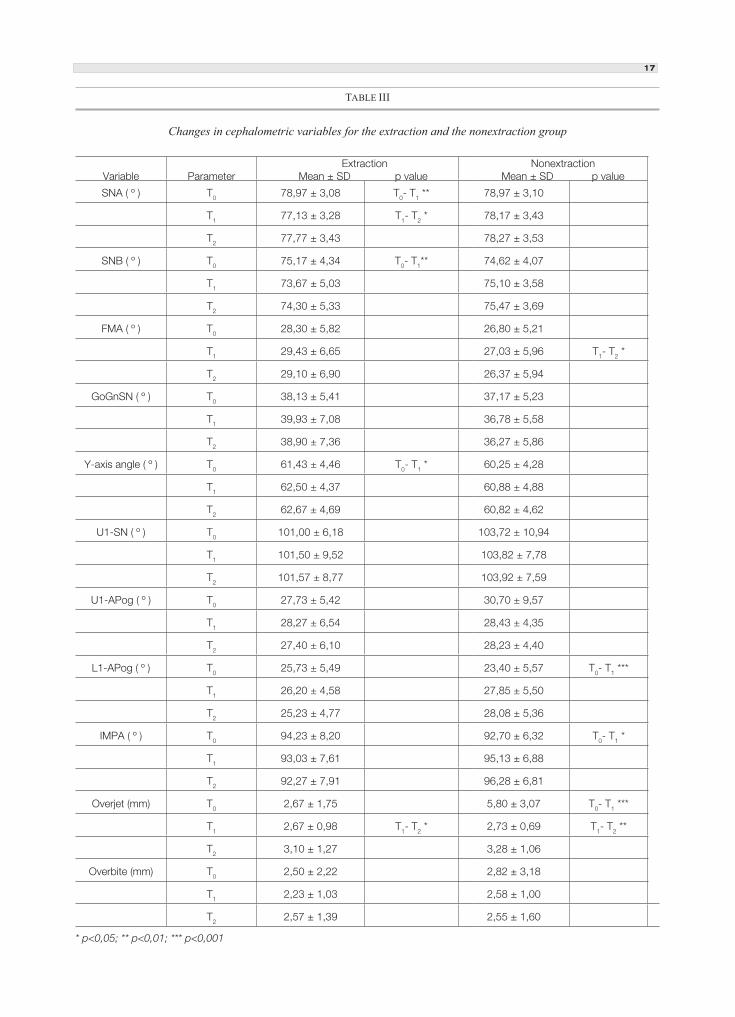
Table III shows the changes in cephalometric measurements for extraction and nonextraction cases.
In the extraction group, in terms of mandi-bular rotation the only change during treatment was seen in Y-axis angle which showed a sig-nificant increase by a mean value of 1, 07º ± 1,88º ( p< 0,05). At the postretention period, Y- axis angle was found to be stable as the other angles describing mandibular rotation. In the no-nextraction group, mandibular growth rotation did not change during treatment whereas at the postretention stage, FMA decreased by a mean value of - 0,67º ± 1,64º (p< 0,05).
Upper and lower incisor inclinations were not changed significantly by the treatment and remained stable after the retention in the ext-raction group. In the extraction group though upper incisor inclinations were preserved during treatment, lower incisor inclinations were incre-ased significantly ( mean: IMPA: 2,43º ± 4,70º , p<0,05; L1-APog: 4,45º ± 5,31º , p<0,001). At the postretention period, both upper and lower incisor inclinations remained stable.
Overjet increased slightly but significantly at the postretention period (mean: 0,43 ± 0,65 mm, p<0,05) in the extraction group. In the nonextraction group, overjet significantly decre-ased by the treatment ( mean: -3,07 ± 3,19 mm, p<0,001) and increased at the postretention period with a mean value of 0,55 ± 1,08 mm (p<0,01).
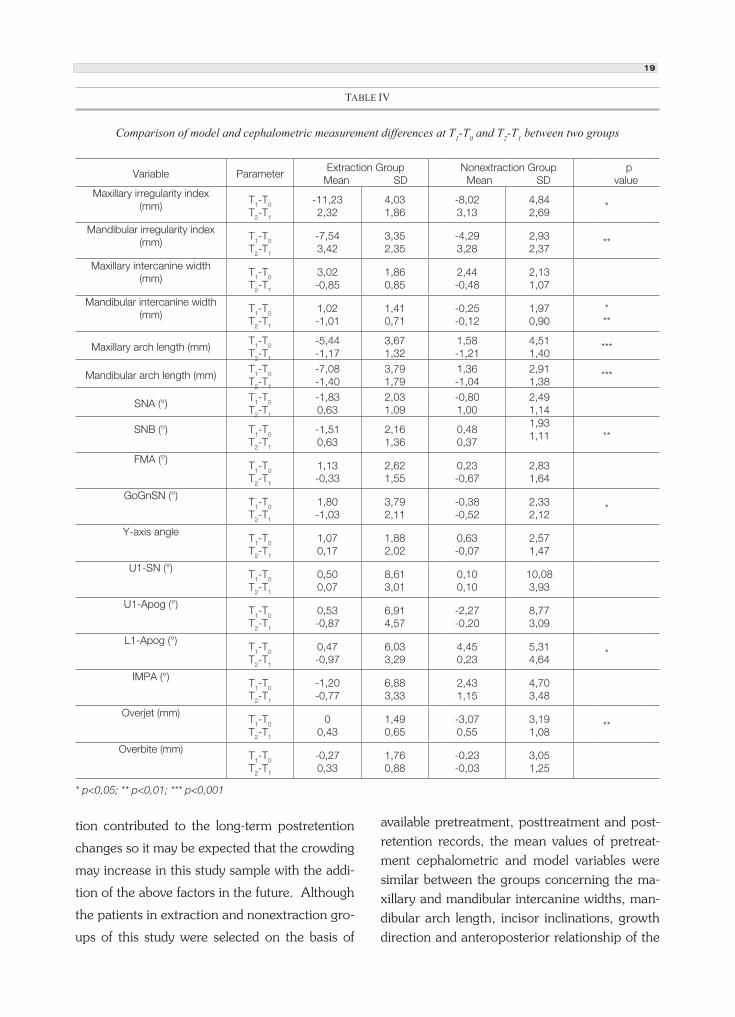
Changes in extraction group versus nonextraction group at T1-T0 and T2-T1
Comparison of the changes occurring during treatment and after retention between the two groups are shown in Table IV. During treatment mandibular intercanine width was increased in the extraction group and decreased in the no-nextraction group. Maxillary and mandibular
arch lengths were reduced in the extraction and increased in the nonextraction group. Lower in-cisors were inclined significantly labially in the nonextraction group compared to the extraction group. The postretention decrease in the mandi-bular intercanine width was significantly greater in the extraction group compared to the nonext-raction group (p<0,01).
Postretention (T2-T1) versus pretreatment (T0) and posttreatment (T2-T1) associations
Correlation tests were performed to find any association between the increase in maxillary and mandibular irregularity index at the postretenti-on stage and the changes in intercanine width, arch length, pretreatment amount of crowding and cephalometric variables.
In the extraction group, maxillary irregularity index at the postretention period did not show any correlation with any of the parameters exa-mined. However, mandibular irregularity index showed a weak but significant correlation with the decrease in intercanine width (r: -0,59 , p< 0,05).
Postretention increase in maxillary irregula-rity index in the nonextraction group correlated with the decrease in maxillary intercanine width ( r: -0,56 , p<0,01).
Overjet relapse in the nonextraction group was correlated with the amount of pretreatment overjet ( r: 0,47 , p<0,01).
DISCUSSION
The purpose of this retrospective study was to detect the early relapse of maxillary and man-dibular incisor irregularity in first premolar ext-raction and nonextraction cases and evaluate the associated factors. Regarding the long-term stu-dies concerning 5 to 20 years of postretention period, this study evaluated the incisor relapse in the short-term. However, it was mentioned that the majority of the relapse occurred soon after the discontinuation of the retention appliances9.
The continued growth and craniofacial matura-
19
tion contributed to the long-term postretention
changes so it may be expected that the crowding
may increase in this study sample with the addi-
tion of the above factors in the future. Although
the patients in extraction and nonextraction gro-
ups of this study were selected on the basis of
available pretreatment, posttreatment and post-retention records, the mean values of pretreat-ment cephalometric and model variables were similar between the groups concerning the ma-xillary and mandibular intercanine widths, man-dibular arch length, incisor inclinations, growth direction and anteroposterior relationship of the
TABLE IV
Comparison of model and cephalometric measurement differences at T1-T0 and T2-T1 between two groups
Variable Parameter Extraction Group
Mean SD Nonextraction Group
Mean SD p
valueMaxillary irregularity index
(mm)T1-T0
T2-T1
-11,232,32
4,031,86
-8,023,13
4,842,69
*
Mandibular irregularity index (mm)
T1-T0
T2-T1
-7,543,42
3,352,35
-4,293,28
2,932,37
**
Maxillary intercanine width (mm)
T1-T0
T2-T1
3,02-0,85
1,860,85
2,44-0,48
2,131,07
Mandibular intercanine width (mm)
T1-T0
T2-T1
1,02-1,01
1,410,71
-0,25-0,12
1,970,90
***
Maxillary arch length (mm)T1-T0
T2-T1
-5,44-1,17
3,671,32
1,58-1,21
4,511,40
***
Mandibular arch length (mm)T1-T0
T2-T1
-7,08-1,40
3,791,79
1,36-1,04
2,911,38
***
SNA (°)T1-T0
T2-T1
-1,830,63
2,031,09
-0,801,00
2,491,14
SNB (°) T1-T0
T2-T1
-1,510,63
2,161,36
0,480,37
1,931,11 **
FMA (°)T1-T0
T2-T1
1,13-0,33
2,621,55
0,23-0,67
2,831,64
GoGnSN (°)T1-T0
T2-T1
1,80-1,03
3,792,11
-0,38-0,52
2,332,12
*
Y-axis angleT1-T0
T2-T1
1,070,17
1,882,02
0,63-0,07
2,571,47
U1-SN (°)
T1-T0
T2-T1
0,500,07
8,613,01
0,100,10
10,083,93
U1-Apog (°)T1-T0
T2-T1
0,53-0,87
6,914,57
-2,27-0,20
8,773,09
L1-Apog (°)T1-T0
T2-T1
0,47-0,97
6,033,29
4,450,23
5,314,64
*
IMPA (°)T1-T0
T2-T1
-1,20-0,77
6,883,33
2,431,15
4,703,48
Overjet (mm)T1-T0
T2-T1
00,43
1,490,65
-3,070,55
3,191,08
**
Overbite (mm)T1-T0
T2-T1
-0,270,33
1,760,88
-0,23-0,03
3,051,25
* p<0,05; ** p<0,01; *** p<0,001

20
jaws. Greater irregularity index values of the ext-raction and greater overjet in the nonextraction group reflected the different treatment approach between the two groups.
The results of this study revealed a 3 mm mandibular dental irregularity at the postreten-tion follow-up of three years. The amount of lower incisor crowding was comparable to the findings of the long-term extraction-nonextrac-tion studies in Class II cases 19-21 . On the other hand, this amount of crowding was considered to be minimal according to Little50. The amount of lower incisor relapse was found to be greatest in mixed dentition arch length increase cases (mean: 6,06 ± 2.79 mm) 13 followed by crowded first premolar extraction patients (mean: 4,63 ± 1,91 mm) 1 , serial extraction cases (mean: 4,39 ± 1,64 mm) 51 , second premolar extraction ca-ses (mean: 4.00 ± 1.70 mm) 5 and generalized spacing cases (mean: 3.83 ± 1,91 mm) 12 . The most stable results were reported for first premo-lar extractions of Class I subjects 10,52 , mandibu-lar incisor extractions 6 , nonextraction treatment with palatal expansion 15,17 and cervical facebow therapy in Class II Div 1 patients 16 .
A notable amount of maxillary incisor relap-se was demonstrated both in the extraction and nonextraction groups of this study. This is in contrast to the findings of previous reports which show lesser amounts of maxillary incisor relap-se compared to the mandibular incisors 9,14, 22,43
. In one study high pretreatment irregularity and contact displacement were reported to be associ-ated with upper incisor crowding 44 but could not be demonstrated in this study.
Postretention decrease in maxillary intercani-ne width was found to be partly associated with the postretention increase in maxillary incisor ir-regularity in this study. However, as the correla-tions were low, the cause of postretention upper incisor irregularity cannot be solely explained by the decrease in intercanine width.
The changes in lower intercanine width oc-
curred differently between the extraction and nonextraction groups of this study. In the ext-raction group, mandibular intercanine width was increased during treatment as demonstrated also by Gianelly 53 due to the position of cani-nes that were more distally placed as a result of extractions. In the nonextraction group inter-canine width was preserved during treatment. At the postretention period, a reduction toward the original dimension was found in the extrac-tion group compared to the stable intercanine dimension in the nonextraction group. These findings confirmed the general conclusion that the expansion of lower intercanine width tend to constrict at the postretention54 and preserva-tion of intercanine width is essential to achieve long-term stability 11,30,55,56 .
Postretention increase in lower incisor crow-ding in the extraction group seemed to be partly associated with the decrease in intercanine width in this study. However, maintenance of mandi-bular intercanine width could not guarantee in-cisor alignment stability since in the nonextrac-tion group of this study, although postretention mandibular intercanine width was preserved, the same amount of postretention lower incisor crowding occurred. Although the association between the reduction in intercanine width and mandibular crowding relapse was also demons-trated by other authors 21,23 , this single factor cannot solely explain the relapse in lower incisor crowding. The cause of lower incisor crowding appears to be multifactorial 1,5,12,21 .
Arch length reduction at the postretention period was a common finding as reported in the literature 3,5,11,14,19,20 . An explanation for arch length decrease with time may be a mesial drift due to aging or the anterior component of the functional forces 9 . Maxillary and mandibular arch lengths showed a significant reduction at the postretention period in both the extraction and nonextraction groups of this study. Howe-ver, the postretention increase in incisor irregu-larity was not found to be related with the arch

21
length reduction in accordance with the findings of long-term studies 1,3-5,12 .
According to Björk’s growth studies, forward growth rotation may be associated with mandi-bular incisor crowding and deepening of the bite. Backward rotation may also be associated with incisor crowding due to compensatory retrocli-nation of the incisors in such cases, and ope-ning of the bite 35 . In this study, the mandibular rotational change was significant only for the nonextraction group but the decrease of 0,7º in the mandibular plane angle could be considered clinically negligible and too small to be effective on incisor alignment. Pretreatment overbite was normal and remained stable during the postre-tention period for both groups. Similar findings were reported in a nonextraction cephalometric and model study by Glenn and coworkers’ 11 .
It was suggested that lower incisors should be retracted or positioned 90 degrees over basal bone to stay stable over time 24,25,29,55 . Procli-nation of incisors was only justified when they were initially retroclined 26,57 . However, lower incisors were inclined labially during treatment in the nonextraction treatment group of this study and remained stable at the postretention follow-up. Thus, other factors may be responsib-le for postretention lower incisor irregularity in this group. However, the amount of labial incisor inclination was small and this finding should not be interpreted as lower incisors may be inclined labially to gain space for lower anterior crowding. Furthermore, the evaluation of axial inclinations of incisors on cephalometric radiographs could be misleading as it was not possible to measure the axial inclination of a single incisor radiograp-hically.
A significant but slight increase in overjet was found after retention in both the extraction and nonextraction groups of this study. A slight chan-ge in overjet toward pretreatment values was also demonstrated in other studies 16,58 . The relapse of overjet was reported to be associated by the pretreatment overjet values 59,60 . A significant
correlation between the postretention change in overjet and pretreatment overjet was also found in this study. However, the amount of postreten-tion overjet increase was clinically insignificant and the correlation between the pretreatment overjet values was weak. Greater overjet changes with large pretreatment overjet values may show stronger associations.
The results of this short-term lateral cepha-lometric and model study in extraction and no-nextraction cases revealed the following conclu-sions:
1. Relapse of maxillary incisor alignment was as common as the postretention increase in mandibular incisor irregularity.
2. Expansion of the mandibular intercanine width tended to return to its original value at the postretention. When this width was preserved during treatment, it remained stable at 3 years postretention follow-up.
3. Postretention irregularity increase in ma-xillary and mandibular anterior crowding seemed to be associated with the postretention decrease in maxillary and mandibular intercanine widths. However, the associations were weak to be so-lely responsible for incisor relapse.
4. Proclination of mandibular incisors see-med to have no effect on postretention increase of lower incisor irregularity.
5. Maxillary and mandibular arch lengths decreased after retention both in extraction and nonextraction cases.
REFERENCES
1. Little RM, Wallen TR, Reidel RA. Stability and relapse of mandibular anterior alignment- first premolar extraction cases treated by traditional edgewise orthodontics.
Am J Orthod. 1981; 80: 349-365.
2. Shields TE, Little RM, Chapko MK. Stability and relapse of mandibular anterior alignment: A cephalometric appraisal of first-premolar-extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1985; 87: 27-38.
3. Little RM, Riedel RA, Årtun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years
22
postretention. Am J Orthod Dentofacial Orthop. 1988; 93: 423-428.
4. Little RM. Stability and relapse of dental arch alignment. Br J Orthod. 1990; 17: 235-241.
5. McReynolds DC, Little RM. Mandibular second premolar extraction-postretention evaluation of stability and relapse. Angle Orthod. 1991; 61:133-144.
6. Riedel RA, Little RM, Bui TD. Mandibular incisor extraction-postretention evaluation of stability and relapse. Angle Orthod. 1992; 62: 103-116.
7. Miyazaki H, Motegi E, Yatabe K, Isshiki Y. Occlusal stability after extraction orthodontic therapy in adult and adolescent patients. Am J Orthod Dentofacial Orthop. 1997; 112: 530-537.
8. Haruki T, Little RM. Early versus late treatment of crowded first premolar extraction cases: Postretention evaluation of stability and relapse. Angle Orthod. 1998; 68: 61-68.
9. Vaden JL, Harris EF, Gardner RZ. Relapse revisited. Am J Orthod Dentofacial Orthop. 1997; 111: 543-553.
10. Boley JC, Mark JA, Sachdeva RCL, Buschang PH. Long-term stability of Class I extraction treatment. Am J Orthod Dentofacial Orthop. 2003; 124: 277-287.
11. Glenn G, Sinclair PM, Alexander RG. Nonextraction orthodontic therapy: Posttreatment dental and skeletal stability. Am J Orthod Dentofacial Orthop. 1987; 92: 321-328.
12. Little RM, Riedel RA. Postretention evaluation of the stability and relapse- mandibular arches with generalized spacing. Am J Orthod Dentofacial Orthop. 1989; 95: 37-41.
13. Little RM, Riedel RA, Stein A. Mandibular arch length increase during the mixed dentition: Postretention evaluation of stability and relapse. Am J Orthod Dentofacial Orthop. 1990; 97:393-404.
14. Sadowsky C, Schneider BJ, BeGole EA, Tahir E. Long-term stability after orthodontic treatment: nonextraction with prolonged retention. Am J Orthod Dentofacial Orthop. 1994; 106: 243-249.
15. Moussa R, O’Reilly MT, Close JM. Long-term stability of rapid palatal expander treatment and edgewise mechanotherapy. Am J Orthod Dentofacial Orthop. 1995; 108: 478-488.
16. Elms TN, Buschang PH, Alexander RG. Long-term stability of Class II Division 1 nonextraction cervical face-bow therapy, I. Model analysis. Am J Orthod Dentofacial Orthop. 1996; 109: 271-276.
17. Azizi M, Shrout MK, Haas AJ, Russell CM, Hamilton EH. A retrospective study of Angle Class I malocclusions treated orthodontically without extractions using two palatal expansion methods. Am J Orthod Dentofacial Orthop. 1999; 116: 101-107.
18. Yavari J, Shrout MK, Russell CM, Haas AJ, Hamilton EH. Relapse in Angle Class II Div 1 malocclusion treated by tandem mechanics without extraction of permanent teeth: A retrospective analysis. Am J Orthod Dentofacial Orthop. 2000;118: 34-42.
19. Paquette DE, Beattie JR, Johnston LE. A long-term comparison of nonextraction and premolar extraction edgewise therapy in “borderline” Class II patients. Am J Orthod Dentofacial Orthop. 1992; 102: 1-14.
20. Luppanapornlarp S, Johnston L. The effects of premolar-
extraction: A long-term comparison of outcomes in “clear-cut” extraction and nonextraction Class II patients. Angle Orthod. 1993; 63: 257-272.
21. Årtun J, Garol JD, Little RM. Long term stability of mandibular incisors following successfull treatment of Class II Division 1 malocclusion. Angle Orthod. 1996; 66: 229-238.
22. Uhde MD, Sadowsky C, BeGole EA. Long-term stability of dental relationships after orthodontic treatment. Angle Orthod. 1983; 53: 240-252.
23. Kahl-Nieke B, Fischbach H, Schwarze CW. Treatment and postretention changes in dental arch width dimensions – a long term evaluation of influencing cofactors. Am J Orthod Dentofacial Orthop. 1996; 109: 368-378.
24. Tweed CJ. Indications of the extraction of teeth in orthodontic procedures. American Journal of Orthodontics and Oral Surgery. 1944; 30: 405-428.
25. Tweed CH. A philosophy of orthodontic treatment. Am J Orthod. 1945; 31: 74-103.
26. Mills JRE. Long-term results of the proclination of lower incisors. British Dental Journal 1966; 120: 355-363.
27. Reitan K. Principles of retention and avoidance of posttreatment relapse. Am J Orthod. 1969; 55: 776-790.
28. Houston WJB, Edler R. Long-term stability of the lower labial segment relative to the A-Pog line. Eur J of Orthod. 1990; 12: 302-310.
29. Gardner RA, Harris EF, Vaden JL. Postorthodontic dental changes: A longitudinal study. Am J Orthod Dentofacial Orthop. 1998; 114: 582-587.
30. Rossouw PE, Preston CB, Lombard CJ. A longitudinal evaluation of the anterior border of the dentition. Am J Orthod Dentofacial Orthop. 1993; 104: 146-52.
31. Peck S, Peck H. Crown dimensions and mandibular incisor alignment. Angle Orthod. 1972; 42: 148-153.
32. Boese LR. Fiberotomy and reproximation without lower retention. 9 years in retrospect: Parts I and II. Angle Orthod. 1980; 50: 88-97, 169-178.
33. Edwards JG. A long-term prospective evaluation of the circumferential supracrestal fiberotomy in alleviating orthodontic relapse. Am J Orthod Dentofacial Orthop. 1988; 93: 380-387.
34. Taner TU, Haydar B, Kavuklu İ, Korkmaz A. Short-term effects of fiberotomy on relapse of anterior crowding. Am J Orthod Dentofacial Orthop. 2000; 118: 617-623.
35. Björk A, Palling M. Adolescent age changes in sagittal jaw relation, alveolar prognathy, and inclination. Acta Odont Scand. 1955; 12: 201-232.
36. Björk A, Skieller V. Facial development and tooth eruption: an implant study at the age of puberty. Am J Orthod. 1972; 42: 148-153.
37. Sanin C, Savara BS. Factors that affect the alignment of the mandibular incisors : a longitudinal study. Am J Orthod. 1973; 64: 248-257.
38. Schudy GF. Posttreatment craniofacial growth: its implications in ortodontic treatment. Am J Orthod. 1974; 65: 39-57.

23
39. Gilliland JD, Buschang PH, Behrents RG. An evaluation of growth and stability in untreated and treated subjects. Am J Orthod Dentofacial Orthop. 2001; 120: 588-597
40. Lindquist B, Thilander B. Extraction of third molars in cases of anticipated crowding in the lower jaw. Am J Orthod. 1982; 81: 130-139.
41. Richardson ME. Late lower arch crowding in relation to primary crowding. Angle Orthod. 1982; 52: 300-312.
42. Swanson WD, Riedel RA, D’Anna JA. Postretention study: Incidence and stability of rotated teeth in humans. Angle Orthod. 1975; 45: 198-203.
43. Sadowsky C, Sakols E. Long-term assessment of orthodontic relapse. Am J Orthod. 1982; 82: 456-463.
44. Surbeck BT, Artun J, Hawkins NR, Leroux B. Associations between initial, posttreatment, and postretention alignment of maxillary anterior teeth. Am J Orthod Dentofacial Orthop. 1998; 113:186-95.
45. Huang L, Artun J. Is the postretention relapse of maxillary and mandibular incisor alignment related? Am J Orthod Dentofacial Orthop. 2001; 120: 9-19.
46. Sinclair PM, Little RM. Maturation of untreated normal occlusions. Am J Orthod Dentofacial Orthop. 1983; 83: 114-123.
47. Bishara SE, Jacobsen JR, Treder JE, Stasi MJ. Changes in the maxillary and mandibular tooth size-arch length relationship from early adolescence to early adulthood. Am J Orthod Dentofacial Orthop. 1989; 95: 46-59.
48. Bishara SE, Treder JE, Jacobsen JR. Facial and dental changes in adulthood. Am J Orthod Dentofacial Orthop. 1994; 106: 175-186.
49. Carter GA, McNamara JA. Longitudinal dental changes in adults. Am J Orthod Dentofacial Orthop. 1998; 114: 88-99
50. Little RM. The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod. 1975; 68: 554-563.
51. Little RM, Riedel RA, Engst E. Serial extraction of first premolars- postretention evaluation of stability and relapse. Angle Orthod. 1990; 60: 255-262.
52. Persson M, Persson EC, Skagius S. Long-term spontaneous change following removal of all first premolars in Class I cases. Eur J Orthod. 1989; 11: 271-282.
53. Gianelly AA. Arch width after extraction and nonextraction treatment. Am J Orthod Dentofacial Orthop. 2003; 123: 25-28.
54. Burke SP, Silveira AM, Goldsmith JL, Yancey JM, Stewart AV, Scarfe WC. A meta-analysis of mandibular intercanine width in treatment and postretention. Angle Orthod. 1997; 68: 53-60.
55. Riedel RA. A review of the retention problem. Angle Orthod. 1960; 30: 179-194.
56. Gardner SD, Chaconas SJ. Posttreatment and postretention changes following orthodontic therapy. Angle Orthod. 1976; 46: 151-161.
57. Årtun J, Krogstad O, Little RM. Stability of mandibular incisors following excessive proclination: a study in adults with surgically treated mandibular prognatism. Angle Orthod. 1990; 60: 99-106.
58. Bishara SE, Chadha JM, Potter RB. Stability of intercanine width, overbite and overjet correction. Am J Orthod. 1973; 63: 588-595.
59. Benneth TG, Tullock TFC, Vig KWL, Webb WG. Overjet stability after treatment of Class II Division 1 malocclusion. Br J Orthod. 1975; 2: 239-246.
60. Wood CM. The effect of retention on the relapse of Class II Division 1 cases. Br J Orthod. 1983; 10: 198-202.
CORRESPONDING ADRESS
Tülin (Uğur) TANER DDS, PhDHacettepe University Faculty of Dentristry, Department of Orthodontics
Tel: 90-312-305 22 90 Fax: 90-312-309 11 38 E-mail: [email protected]