an atypical turner syndrome patient with ring x chromosome ... · turner syndrome patient with ring...
TRANSCRIPT

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 25, No. 1 Copyright © 1995, Institu te for Clinical Science, Inc.
An Atypical Turner Syndrome Patient with Ring X Chromosome Mosaicism*
EDUARDO S. CANTO, Ph.D .,t DONNA F. JACOBS, B.S.,t
and G. SHASHIDHAR PAI, M .D.i
fCytogenetics Section, D epartm ent o f Pathology and Laboratory Medicine, and tD ivision o f Genetics and Chibd Development,
Departm ent o f Pediatrics, Medical University o f South Carolina,
Charleston, SC 29425
ABSTRACT
Small m arker chromosomes (SMC) associated with severe Turner syndrome (TS) variants often represent reduced X chromosomes lacking the X inactivation center (XIC), perturbed dosage compensation, and unbalanced gene expression. A TS patient with mental retardation (MR), unusually short stature, facial and limb malformations, and karyotypic mosaicism involving SMCs is described. Cytogenetic and fluorescence in situ hybridization (FISH) studies of blood and lymphoblastoid cells showed that the SMC was X-chromosome derived, contained a functional centromere, and had ring formation. Karyotypes of 45/46,X,r(X) in blood cells and 45,X/46,- XX/46,X,r(X)/47,X,r(X), + r(X) in fibroblasts were found. Late-replication of the SMC was inconclusive, bu t the X inactivation specific transcript (XIST) locus w ithin XIC was dem onstrated by fluorescent in situ hybridization (FISH). M echanisms are rev iew ed that can account for our p a tien t’s unusual TS phenotype.
Introduction
T urner syndrom e (TS) is associated with complete or partial monosomy of the X chromosome and occurs with an incidence of about 1 in 5,000 hum an female live births. It is highly lethal in utero, and only 1.0% of all 45,X conceptuses are thought to survive. Subsequently , this sex chromosome imbalance is character
* Send reprin t requests to: Eduardo S. Cantu, P h .D ., C y to g en e tic s S ection , D e p a rtm e n t of Pathology and Laboratory M edicine, M edical University o f South C arolina, 171 A shley A venue, Charleston, SC 29425.
ized by relatively benign physical stigmata which include short stature, broad chest with widely spaced nipples, characteristic facial features, gonadal dysgenesis, w ebbed neck, low posterior ha irline, and high incidence o f renal and cardiovascular anomalies . 1
Although some studies have suggested a specific cogn itive d e fic ien cy w ith visual perceptual deficits , 2 the incidence of m ental re ta rda tion (MR) does not appear to be higher in TS than in the population at large, except in a subgroup of patients who have mosaicism involving small marker chromosomes (SMC ) . 3 Van
600091-7370/95/0100-0060 $00.90 © Institute for Clinical Science, Inc.
TURNER SYNDROME PATIENT WITH RING X 61
Dyke et al3 have proposed that MR, and perhaps other features uncharacteristic of TS, may be due to the presence of inappropriately activated small r(X) chromosomes which lack the XIC. Other studies have associated SMC with MR,4,5 with m osaicism ,6 and other severe pheno types7 w hen they w ere r(X) chrom osomes, but with risk for gonadoblastoma8 when they were Y chromosome derived.
In light of the present understanding of SMC in TS individuals, a TS patient with MR and a dim inutive body has been reviewed. Our findings from thorough clinical assessment, conventional cytogenetic analysis, and fluorescent in situ hybridization (FISH) studies using X and
Y chromosome specific DNA probes, are reported and their significance is evaluated in terms of how they may be related to MR and other severe characteristics found in TS.
Clinical Report
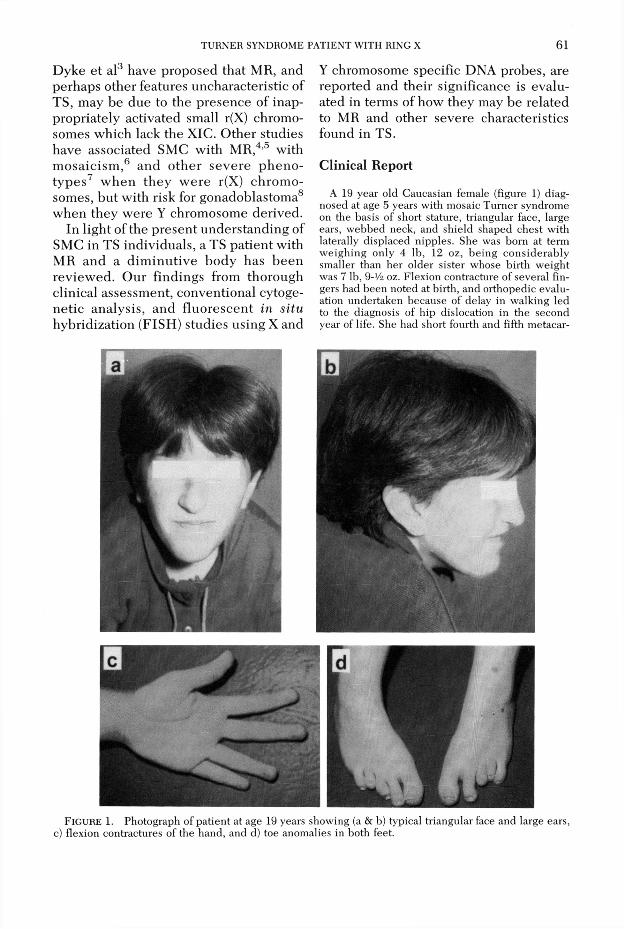
A 19 year old Caucasian female (figure 1) diagnosed at age 5 years with mosaic Turner syndrome on the basis of short stature, triangular face, large ears, webbed neck, and shield shaped chest with laterally displaced nipples. She was born at term w eighing only 4 lb, 12 oz, being considerably smaller than her older sister whose birth w eight was 7 lb, 9-V4 oz. Flexion contracture of several fingers had been noted at birth, and orthopedic evaluation undertaken because of delay in walking led to the diagnosis of hip dislocation in the second year of life. She had short fourth and fifth metacar-
FlGURE 1. Photograph of patient at age 19 years showing (a & b) typical triangular face and large ears, c) flexion contractures of the hand, and d) toe anomalies in both feet.

62 CANTO, JACOBS, AND PAI
pals, and, unexpectedly, severe shortening, mal- im plantation, and lateral deviation of the toes on both of her feet.
O ther features not usually seen in T urner syndrome w ere p resen t in this child. These included extreme short stature w hich was non-responsive to growth horm one treatm ent, strabismus, scoliosis, m ental retardation, and mitral regurgitation, presum ed to be secondary to rheum atic heart disease. T hrom boem bolic ep isodes secondary to m itral valve prosthesis left her w ith m ild left-sided hemi- paresis. At 17 years of age, her most recent psychological evaluation showed her cognitive abilities to be in the range of moderate mental retardation. She has had intractable hypertension, possibly secondary to renal vascular stenosis associated w ith horseshoe shaped kidneys.
M ethods and M aterials
C y t o g e n e t i c S t u d i e s
M ethanol/acetic acid fixed m etaphase cells from peripheral blood, lymphoblas- toid cell cultures, and skin fibroblast cultures d e riv ed from our patien t, w ere s tu d ie d by th e c o n v e n tio n a l G TG - b ind ing tec h n iq u e . 9 Peripheral blood and lym phoblastoid cells w ere further c h a r a c te r iz e d by C B G -b a n d in g , 1 0
Ag-NOR staining , 11 and late-replication s tu d i e s . 1 2 T h e s e te c h n iq u e s w e re ap p lie d in o rd er to ch arac te rize the nature and extent of the karyotypic mosaicism found, and also to determ ine the origin and the structural configuration of the SMC.
F l u o r e s c e n c e I n S it u H y b r i d i z a t i o n ( F I S H )
Cytological materials from blood and lymphoblastoid cell cultures, prepared as described for routine cytogenetic studies, were evaluated by a m odified FISH protocol previously reported . 13 Three sex chrom osom e derived non-isotopically
labelled deoxyribonucleic acid (DNA) probes com m ercially available* w ere used for the in situ hybridization experiments. These included DNA probes with sequence homology to locus DXZ1 (X chromosome specific centrom eric DNA), to locus DYZ3 (Y chromosome specific centromeric DNA), and to the X inactivation specific transcrip t gene (XIST ) . 14
The X and Y alphoid (centromeric) DNA probes are chromosome specific subsets of hum an alpha-satellite repetitive DNA fam ily w hich have re la te d seq u en ce hom ology . 1 5 ,1 6 ,1 7 The m ethod of nonisotopic probe labelling of these probes was by inco rp o ra tio n o f d e riv a tiz e d nucleotides using nick translation . 18
After the DNA probes are labelled, the essential steps of the general FISH protocol include: RNase treatm ent of fixed m etaphase cells; dén a tu ra tio n of the probe DNA and of previously prepared m etaphase chrom osom e DNA; in situ hy b rid iza tion o f the non-iso top ica lly lab e lled p robe DNA to chrom osom al DNA; removal of non-specifically bound DNA by using specific washing conditions; d e tec tio n of h y b rid ized p robe DNA by re a c tin g w ith f lu o re s c e in isothiocyanate (FITC) labe lled avidin (for biotin labelled DNA probes) or with FITC labelled antibody (for digoxigenin labelled DNA probes); and, if necessary, am plification of the signal by fu rther reaction w ith fluo resce in con jugated antibodies. Assessment of localized fluorescein signals after counterstaining with propidium iodide was conducted by epi- fluorescence microscopy using a Zeiss photomicroscope II with a HBO 50 watt DC m ercury lamp and filters having maximums of 492 nm and 520 nm absorption and emission, respectively.
Results
* Oncor, Inc., Gaithersburg, MD 20877.Cytogenetic GTG-banding studies of
peripheral blood, lymphoblastoid cells,

TURNER SYNDROME PATIENT W ITH RING X 63
and cultured skin fibroblasts, showed the presence of mosaicism involving a SMC (smaller than a chromosome 20) in the form of a ring (figure 2a). The CBG- banding suggested the presence of a centromere in this SMC (figure 2b); Ag-NOR staining showed no evidence of a nucleolus organizer region, and late replication studies were inconclusive owing to the small size of the SMC. Furthermore, cytogenetic studies of the skin fibroblast culture detected a single cell with a normal 46,XX karyotype and an additional cell line with a second ring chromosome presum ed to be X chromosome derived.
Fluorescent in situ hybridization studies of blood and lym phoblastoid cells identified the ring chromosome to be X chromosome derived since signals were found over the ring only when X chromosome specific DNA probes (DXZ1 and XIST) were used with no signals found w ith Y ch rom osom e sp ec ific DNA probes.
Mosaicism was also confirmed when the X chromosome specific probes were
used. Two major cell categories were evident, one with single signals, representing cells with only one X chromosome and no r(X), and one with double signals representing cells with both an X and a r(X) chromosome (figure 3a). The FISH stud ies using the XIST DNA p robe yielded positive signals not only over the expected Xql3.3 locus of the normal X chromosome, but also over the r(X) chromosome (figure 3b).
Information collected from both the cytogenetic and FISH studies showed 45,X/46,X,r(X) mosaicism in peripheral lymphocytes and transform ed lym phoblasts with presence of the XIST locus on the r(X). In fibroblasts, cytogenetic studies showed 45,X/46,XX/46,X,r(X)/47,X, r(X), + r(X). The FISH studies were not conducted on fibroblast cells.
Discussion
Since there is quantitative disparity betw een the sexes with respect to the gene loci on human X and Y chromo
FlGURE 2. Photomicrographs of partial metaphases showing (a) ring formation of the small marker using GTG-banding, and (b) positive C bands suggesting the presence of a centromere by CBG-banding.

64 CANTO, JACOBS, AND PAI
FIGURE 3. Representative photomicrographs of FISH results (a) using the X chromosome specific alpha DNA probe on a 46,X,r(X) metaphase showing signals over the normal X and the r(X) chromosomes; and, (b) using the XIST DNA probe showing specific hybridization to the normal X and to the r(X) chromosomes in a 46,X,r(X) cell.
somes, a mechanism for dosage compensation betw een females and males has evolved in o rder to ach ieve genetic equivalency betw een the two. The X chromosome inactivation is a develop- mentally regulated process by which dosage compensation occurs and is governed by the X inactivation center which contains the XIST gene. Mental retardation, severe short stature, and other malformations are not normally associated with TS patients having a 45,X karyotype. These atypical features in TS correlate with the presence of small r(X) chromosomes and may be due to the absence or malfunction of the XIST g e n e .19,20 T hese a lte ra tions are likely to result in the inappropriate expression of X chromosome loci that should normally be transcriptionally inactive.
Results from our study are consistent with the observations that SMCs associated with unusual TS phenotypes tend to be small, annular in structure, and X chromosome derived. Further studies of fibroblast cultures with cells having two r(X) chrom osom es d e riv ed from our
patient* have shown: (1) the presence of XIST sequences in the larger ring, but the absence of XIST sequences in the smaller ring by FISH analysis; and (2) XIST expression by molecular methods. These results indicate that in the cell line having the two r(X) chrom osom es in fibroblasts, one ring indeed inactivates normally (and expresses XIST), but the second ring appears to be activated and not to contain sequences homologous to the XIST locus.t Therefore, the likely explanation for the severe phenotype in our patient is that other tissue types may contain r(X)s in which the XIST may be missing or malfunctioning, and that this defect may be limited to a particular tissue type.
The absence of the XIST transcript (either because the gene is missing or because of regulatory dysfunction) may represent a general m echanism which results in an altered pattern of dosage
* In laboratory of Dr. B. R. Migeon, Johns Hopkins University, Baltimore, MD.
t Jani et al: manuscript in preparation.
TURNER SYNDROME PATIENT W ITH RING X 65
com pensation having unexpected clinical consequences. Further investigations of these small r(X) chrom osomes may lead to a long awaited, better understanding of the genetic mechanisms regulating dosage com pensation in mammals and may also provide a better idea of how aberrant X chromosome inactivation may be related to specific hum an pathologies.
References
1. Smith DW. Recognizable patterns of hum an m alform ations. M ajor Problem s in C lin ical Pediatrics, vol VII, 3rd ed. Philadelphia: Saunders, 1982:72-5.
2. Bender B, Puck M, Salbenblatt J, Robinson A. C ognitive developm en t o f unse lec ted girls w ith complete and partial X monosomy. Pediatrics 1984;73:175-82.
3. Van Dyke DL, Wiktor A, Palm er CG, M iller DA, W itt M, Babu VR, Worsham MJ, Roberson JR, Weiss L. Ullrich-Turner syndrome w ith a small ring X chromosome and presence of m ental retardation. Am J Med G enet 1992;43:996- 1005.
4. Kushnick T, Irons TG, Wiley JE , G ettig EA, Rao KW, Bowyer S. 45X/46X,r(X) w ith syndactyly and severe m ental retardation. Am J M ed G enet 1987;28:567-74.
5. Fryns JP, Kleczkowska A, Van D en Berghe H. H igh incidence of m ental retardation in T urner syndrome patients with ring chromosome X formation. G enet Couns 1990;38:161-5.
6. Berkovitz G, Stamberg J, Plotnick LP, Lanes R. T urner syndrome patients with a ring X chromosome. C lin G enet 1983;23:447-53.
7. D ennis NR, Collins AL, Crolla JA, Cockwell AE, Fisher AM, Jacobs PA. Three patients with ring (X) chromosomes and a severe phenotype. J M ed G enet 1993;30:482-6.
8. Nagafuchi S, Tamura T, Nakahori Y, Takano K, N ishi Y, Iwatani N, Kitao M, Hori Y, Konda H, Hasegawa T, Numabe H, Fujieda K, Tanaka T, H ibi I, Nakagome Y. The majority of the marker chromosomes in Japanese patients w ith stig
mata of Turner syndrome are derived from Y chromosomes. Hum G enet 1992;89:590-2.
9. Seabright M. A rapid banding technique for human chromosomes. Lancet 1971;2:971-2.
10. Sum ner AT. A simple technique for dem onstrating centromeric heterochrom atin. Exp Cell Res 1972;75:304-6.
11. Bloom SE, Goodpasture C. An im proved technique for selective silver staining of nucleolar o rganizer regions in hum an chrom osom es. Hum G enet 1976;34:199-206.
12. Perry P, Wolff S. New Giemsa m ethod for the d iffe ren tia l sta in in g of s is te r ch rom atid s. Nature 1974;251:156-158.
13. Pinkel D, Straume T, Gray JW. Cytogenetic analysis using quantitative, high sensitivity, fluorescence hybridization. Proc Natl Acad USA 1986;83:2934-8.
14. Brown CJ, Ballabio A, Rupert JL, Lafreniere RG, Grompe M, Tonlorenzi R, W illard HF. A gene from the region of the hum an X inactivation centre is expressed exclusively from the inactive X chromosome. Nature 1991;349:38-44.
15. M itchell AR, Gosden JR, M iller DA. A cloned sequence, p82H , of alphoid rep ea ted DNA found at the centromeres of all hum an chromosomes. Chromosoma 1985;92:369-77.
16. Jorgensen AL, Bostock CJ, Bak AL. Chromo- som e-spec ific sub -fam ilies w ith in hum an alphoid repetitive DNA. J Mol Biol 1986; 187: 185-96.
17. W illard HF. Chromosome-specific organization o f hum an alpha satellite DNA. Am J Hum G enet 1985;37:524-532.
18. Rigby PWJ, Dieckmann M, Rhodes C, Berg P. Labeling Deoxyribonucleic acid to high specific activity in vitro by nick translation with polymerase I. J Mol Biol 1977;113:237-51.
19. Migeon BR, Luo S, Stasiowski BA, Jani M, Axelman J, Van Dyke DL, Weiss L, Jacobs PA, Yang-Feng TL, Wiley JE. D eficient transcription of XIST from tiny ring X chromosomes in fem ales w ith severe phenotypes. Proc Natl Acad Sci USA 1993;90:12025-9.
20. Migeon BR, Luo S, Jani M, Jeppesen P. The severe phenotype of females w ith tiny ring X chromosomes is associated w ith inability of these chromosomes to undergo X inactivation. Am J Hum G enet 1994;55:497-504.