an assessment of the status of adults with cerebral palsy
TRANSCRIPT
Develop. Med. Child Neurol. 1917, 19, 803-810
An Assessment of the Status of Adults with Cerebral Palsy
Gavin Andrews L. J. Platt P. T. Quinn P. D. Neilson
Introduction The plight of the cerebral-palsied child
has been the stimulus for much rehabilit- ative effort. In most countries specialised centres have been constructed in which the full force of rehabilitation medicine and special education have been deployed to minimise the consequences of the perinatal damage to the central nervous system.
The plight of the cerebral-palsied adult, on the other hand, appears to have passed unnoticed; certainly it is undocumented. This paper is an attempt to remedy this oversight. The aim of our research was to gather information on the health and well-being of 50 adults with cerebral palsy who, having received intensive rehabilita- tion and education during their formative years, had graduated to a work-training unit housed in an electronics manufactur- ing firm. This industrial enterprise has successfully completed telecommunication contracts gained on the open international market. In maintaining a normal work environment, the facility meets the criteria established by Gray (1972) as being necessary to develop or maintain the work and social skills of institutionalized people.
Vaillant ( I 974) examined the adult adjustment of 100 very healthy college men in terms of physical health, psychological
health, social adjustment and work success. Similar measures were included in the present study to assess the adult adjustment of 50 very handicapped men. There were two specific aims: (1) to examine their current status in terms of the physical limitations on self-care and mobility, of evident neuromuscular handicap and speech disorder, and of psychological health; and (2) to describe the social adjustment and work success of these 50 men and determine the relationship be- tween the measures of disability and these life-style measures.
Method Patients
The Spastic Centre of New South Wales, Australia, conducts an industrial enter- prise to which people with cerebral palsy graduate when they reach adulthood. From this pool of 200 cerebral-palsied people, all men believed to have intelligence and hearing within normal limits were referred for assessment (N = 65). Those for whom the diagnosis of cerebral palsy was in doubt, and those with IQS below 60 or who had no verbal speech or with bilateral hearing loss (determined by audiometric pure-tone values > 30dB over 0.5 to 8kHz) were excluded (N = 15).
Correspondence to Dr. Gavin Andrews, Human Communication Laboratory, University of New South Wales, Prince Henry Hospital, Little Bay, N.S.W. 2036, Australia.
803
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1977, 19
804
The ages of the remaining 50 men ranged from 17 to 55 years (mean 28 years). Five were married. Four were living in their own homes, 23 with their parents and 18 in hostel accommodation. 32 of the men were diagnosed as spastic, 18 as athetoid; 17 had evidence of both syndromes and were classified accord- ing to the dominant syndrome. 39 had normal hearing, the remainder showing varying degrees of mild hearing-loss. Their IQS ranged from 62 to 118 (mean 83). The purpose of screening for rQ was to exclude the more severely mentally handicapped men who would not have been employable even if there had been no additional neuromuscular disorder, but to include those ‘dull’ or ‘backward’ men who con- ceivably would have been employable had there been no spasticity or athetosis. Raven Progressive Matrices were used as the screening test (Raven 1956). It is difficult to assess the specific factor of intelligence in people with diverse per- ceptual and cognitive handicaps without using an elaborate battery of tests. It is possible that those with specific perceptual deficits will have difficulties with the particular form of test we used and thus attain scores below their optimal level of functioning. Accordingly, the lower boun- dary of IQ for the ‘employable’ group was taken as 60 rather than the usual 70.
Assessment of Current Status Four measures were taken of the degree
of physical disability. Items on the dis- ability scale constructed by Garrad and Bennett (1971) were divided into two sub-scales which measured self-care and general mobility. Numerical values were given to each item and each individual scored in terms of his degree of success in independent self-care and mobility. Scores were expressed as a percentage of fully independent behaviour. The third measure was the mean of visual analogue scale
scores for disability, as rated by four members of the medical and supervisory staff of the workshop. The fourth measure was a rating of neurological impairment, as judged by the examining physician. The first three measures were found to be highly intercorrelated and were condensed for subsequent computations by summing the standardized scores to form a single measure of physical disability. Detailed results were given for five men selected from the sample on the basis of their scores on this single measure of physical disability, and these men represent the mean, upper and lower quartiles and extremes of the range.
Speech was assessed by measuring single-word intelligibility, prose intelligi- bility, articulation error and diadocho- kinetic rates. A visual analogue scale of speech handicap was also completed by the workshop staff (Platt et al. 1977). Factor analysis showed that all these measures intercorrelated highly and loaded on a single factor. Single-word intelligi- bility accounted for 73 per cent of the variance and was chosen as the single measure of speech intelligibility. For this measure, each man recorded a phonetically balanced list of 50 monosyllabic words. The intelligibility index for each individual was the mean percentage of words cor- rectly identified by three independent judges.
Estimates of psychological health were obtained from a 30-item general health questionnaire (Goldberg 1972), which was interviewer-administered. A visual ana- logue scale of ‘adjustment to cerebral palsy’ was also completed by the workshop staff. These two measures were significantly intercorrelated and the general health questionnaire score was chosen as the index of mental health for further com- putations because of its proven validity and reliability.

GAVIN ANDREWS L. J. PLATT P. T. QUINN P. D. NEILSON
Assessment of Life Adjustment Work achievement was measured by
three indices: the salary paid to the man by the workshop, the social status of his occupational title and his level of respons- ibility within the workshop. The restricted range of the last two indices made them less valuable than the first for differentiating within the group, so salary was used as the measure of work achievement.
Social adjustment was assessed by three measures selected from a larger battery. In this battery the men were asked how many friends outside the workshop they had been in contact with in the previous week, how many organised social events they had attended in the past month, their marital status and the independence of their living arrangements, and the extent of their social resources from friends and family. A visual analogue scale of social participation was also completed by the workshop staff. The first two scores and the visual analogue scale were found to be highly intercorrelated and were condensed into a single measure of social adjustment by summing the standardized scores.
Case Histories Case histories of five of the 50 men are
presented to illustrate the nature of the clinical sample. The five were chosen according to their scores on the standard- ized measure of physical disability, and represent the mean, upper and lower quartiles and extremes of the range. (Details of all 50 men are given in Table 111).
CASE 48 Most severely disabled. Diagnosis: tension
athetosis. Age 22 years. Birth: First child of middle-class teachers. Forceps delivery after prolonged labour. Was not expected to survive: tube-fed for 30 days. Development: Noted to have poor hand and leg control at I 1 months. Included in Spastic Centre mother and baby programme. At two years was able to stand in frame but unable to walk. At three years had single words; could stand in calipers. Never developed useful hand or
leg movements. Any attempt at voluntary move- ment followed by massive tension and involuntary scissoring of legs and arms. Schooling: Assessed as being of normal intelligence; was able to manage electric typewriter by means of headpiece pointer. Present status: Travels to sheltered workshop by special bus each day. Unable to do useful work. Lives with parents and is totally dependent on others for all functions. Cheerfulness and bright manner, coupled with parents' devotion, have ensured that he has considerable social contact despite the extent of his disability.
CASE 27 Upper quartile for disablement. Diagnosis :
athetoid quadriplegia. Age 21 years. Birth: Twin birth and second child of well-to-do country family. Co-twin died on day 3 . Had R h incom- patibility; jaundiced for six weeks, never trans- fused. Development: Brought to Spastic Centre at one year because of failure to sit and tension in arms and legs. Stood and walked in calipers by six years; able to walk but unable to feed himself at 16 years. Schooling: Made only limited progress in Spastic Centre residential school. Present status: Lives in Spastic Centre hostel and is occupied in sheltered workshop. Able to walk on level ground but involuntary movements and poor hand-control preclude any useful activity, particularly when coupled with his severe myopia. Has no useful speech. Social isolation is lessened by his residence in hostel.
CASE 19 Mean disablement score. Diagnosis: spastic
quadriplegia. Age 18 years. Birth: First child of country labourer. 'Mother had toxaemia, labour was prolonged but child appeared to be normal at birth. Six hours later a cerebral cry was heard, there was twitching in the right hand and leg and a period of hyperpyrexia followed. Perinatal cerebral damage resulting from haemorrhage was diagnosed. At 10 weeks he showed ankle clonus and increased reflexes. Development: At one year could not sit alone, showed reflex spread of tension and scissoring with voluntary movement. By age nine years could walk 50 feet with calipers, manage stairs with aid of a rail and was judged to have 50 per cent fine hand function. Spoke single words by 2) years. Schooling: Progress was slow, despite mastering use of electric typewriter: at 16 years was still doing first-year high-school work at remedial standard. Never developed intelligible speech. Present status: Has been in sheltered workshop for one year. Despite his physical capacities it has not been possible to integrate him
805

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY, 1977, 19
into Spastic Centre Industries because of his poor concentration. Lives at home with parents and travels to centre by special bus every day.
CASE 40 Lower quartile for disablement. Diagnosis:
spastic quadriplegia. Age 26 years. Birrh: Second child of middle-class business family. Born after prolonged labour, posterior presentation; noted to have cord around neck and to be difficult to resuscitate. Appeared to be normal by 12th day. Development: Abnormality suspected a t nine months; did not sit up until 17 months. Walked at four years on broad base with feet internally rotated. Given calipers at eight years; had teno- tomy of left psoas at 15 years. Fair co-ordination and power in all limbs. Schooling: Entered Spastic Centre school at four years; progressed normally, completed external examination for school certificate, then electronic engineering certificate at technical college. Present status: Works in Spastic Centre Industries as quality control officer for electronics workshop. Married to girl with athetosis; they have their own home. Drives a car and is socially independent. Obvious physical difficulty with precise arm and leg movements. Can walk on level ground for 400 yards and can manage one flight of stairs. Dysarthria evident; speech intelligible but slow.
CASE 24 Least disabled. Diagnosis : spastic hemiplegia.
Age 35 years. Birth and Development: Little is known about this man’s history. He was admitted
to Spastic Centre workshop at age 22 years. History of congenital hydrocephalus, retarded mental development and epilepsy. In normal school system until age 13, then at home for 10 years doing nothing. Had shunt diversion at age 28 years. Present status: Works in Spastic Centre Industries, sorting semiconductors. Is single, lives at home with middle-class parents and travels to work by public transport. Has little social life. Has mild spastic gait, bilateral tremor, evidence of mild left hemiplegia. Speech is consistent with intelligence.
Results The measures of central tendency of the
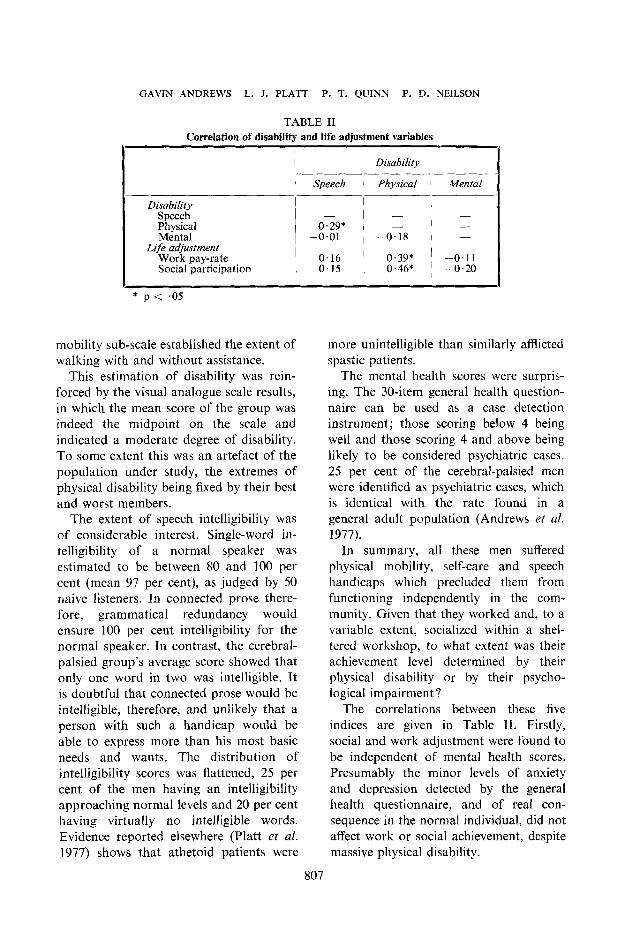
scores for the various items are given in Table I. A correlation matrix of the derived score for physical ability, the score for speech ability, the score for mental health and the life adjustment scores for work and social participation are presented in Table 11.
The self-care sub-scale measured whether these men could feed, dress, undress, wash and use the toilet without assistance, or with specified degrees of assistance. The average patient could only function with help or in specially prepared circumstances, so they would not be capable of being independent in the outside world where such activities are taken for granted. The
TABLE I Characteristics of 50 adult men with cerebral palsy
I Mean
Indices of current status Disability level:
self-care (normal = 100) mobility (normal = 100) VAS* disability (massive = 1, minor = 7) neurological impairment (none = 0, severe = 3) speech intelligibility (normal = 100)
Indices of life adjustment Psychological impairment (normal = < 4) VAS* adjustment to cerebral palsy
(adjusted = 7, frustrated = I ) Work pay-rate (dollars per week) Social life:
number friends contacted number organized activities VAS* social life (full = 7, isolated = 1)
79 57 4 2.1
51
3.5
5.3 25.0
2.4 1 .5 4 .3
SD
25 31
1.3 0.8
29
5.6
I .o 2.6
2.9 1 . 1
Range
0-99 4-95 1-6 1-3 0-90
0-24
2-7 1-135
0-9 0-4
i 2-6 * VAS = visual analogue scale
806
GAVIN ANDREWS L. J. PLATT P. T. QUINN P. D. NEILSON
TABLE I1 Correlation of disability and life adjustment variables
I
I Disability
i Speech ~ Physical 1 Mental
Disability Speech Physical Mental
Work pay-rate Social participation
Life adjustment
- I 1
- l - 0.29* I - 1 -
-0.01 , -0.18 I -
0.16 0.39* ' -0.11 0.15 ' 0.46* ~ -0.20
I
* p < .05
mobility sub-scale established the extent of walking with and without assistance.
This estimation of disability was rein- forced by the visual analogue scale results, in which the mean score of the group was indeed the midpoint on the scale and indicated a moderate degree of disability. To some extent this was an artefact of the population under study, the extremes of physical disability being fixed by their best and worst members.
The extent of speech intelligibility was of considerable interest. Single-word in- telligibility of a normal speaker was estimated to be between 80 and 100 per cent (mean 97 per cent), as judged by 50 naive listeners. In connected prose there- fore, grammatical redundancy would ensure 100 per cent intelligibility for the normal speaker. In contrast, the cerebral- palsied group's average score showed that only one word in two was intelligible. It is doubtful that connected prose would be intelligible, therefore, and unlikely that a person with such a handicap would be able to express more than his most basic needs and wants. The distribution of intelligibility scores was flattened, 25 per cent of the men having an intelligibility approaching normal levels and 20 per cent having virtually no intelligible words. Evidence reported elsewhere (Platt et al. 1977) shows that athetoid patients were
more unintelligible than similarly afflicted spastic patients.
The mental health scores were surpris- ing. The 30-item general health question- naire can be used as a case detection instrument; those scoring below 4 being well and those scoring 4 and above being likely to be considered psychiatric cases. 25 per cent of the cerebral-palsied meti were identified as psychiatric cases, which is identical with the rate found in a general adult population (Andrews et al. 1977).
In summary, all these men suffered physical mobility, self-care and speech handicaps which precluded them from functioning independently in the com- munity. Given that they worked and, to a variable extent, socialized within a shel- tered workshop, to what extent was their achievement level determined by their physical disability or by their psycho- logical impairment ?
The correlations between these five indices are given in Table 11. Firstly, social and work adjustment were found to be independent of mental health scores. Presumably the minor levels of anxiety and depression detected by the general health questionnaire, and of real con- sequence in the normal individual, did not affect work or social achievement, despite massive physical disability.
807

TABL
E 11
1 C
hara
cter
istic
s of 5
0 ad
ult m
en w
ith c
ereb
ral p
alsy
(46
infa
ntile
cer
ebra
l pal
sy, 4
oth
er*
post
nata
l cer
ebra
l dam
age)
Cor
e no
. 1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
Age
b
-s)
19
17
35
28
21
29
17
31
28
17
33
26
32
46
27
44
52
27
18
30
27
26
17
35
27
17
21
41
27
32
21
29
32
25
23
18
39
20
26
26
23
29
55
30
38
23
39
22
23
31
IQ
65
70
93
88
68
101 70
71
87
84
118 72
73
98
86
87
64
75
88
68
66
64
108 70
93
72
76
63
80
71
95
97
87
67
86
62
66
80
97
103 70
98
109 80
75
118 84
97
99
73
No.
A
sses
sed
% N
orm
al %
Nor
mal
Ass
esse
d N
errr
olos
ical
%
Spe
ech
Psyc
holo
gica
l A
sses
sed
Wor
k N
o. fr
iend
s ac
tiviti
es
adeq
uacy
se
y-ca
re
mob
ilit
y ph
ysic
al
impa
irm
ent
inte
lligi
ble
impa
irm
ent
adju
stm
ent
achi
evem
ent
cont
acte
d/
atte
nded
/ of
soc
ial
to 52
. w
eek
wee
k lif
e A
80
87
80
73
80
87
80
99
93
53
87
73
93
99
99 6 80
20
87
67
47
93
99
99
87
93
67
99
99
99
27
93
73
87
40
80
99
53
93
99
93
87
87
93
33
99
87
99
99
-
63
29
99
70
70
79
80
87
70 5 96
34
91
70
74 9 13
4 59 4 7 49
74
91
68
89
76
68
91
10 4 20
78
64
49
27
31
43
91
87
74
74
57
87 6 90
79 4 19
74
disa
bilit
y 3 4 4 5 5 3 3 3 4 6 3 5 2 4 4 5 5 7 3 6 5 5 2 2 3 3 6 5 3 4 6 4 4 3 6 4 4 5 3 4 4 4 5 3 6 3 3 7 2 2
43
82
51 1 7 67
79
89
90
25 9 85
53 5 4 58 7 4 23
84
89
75
87
20
52
15
24
47
80
77
63
47
32
61
43
77
89
64
64
45
89
28
51
38
76
59
37
82
57
-
3
L
4 3
1 2
6 3
2 4
- 2
- 3
- 2
- 2
3 3
- 2
1 2
1 3
1 3
- 3
2 3
1 2
20
3 1
3 3
2 11
4
- 2
- 1
2 2
3 2
1 3
- 3
- 3
3 2
- 2
1 2
- 2
5 1
7 2
- 3
1 2
- 1
1 3
- 3
9 2
2 2
9 3 2
5 6
9 6
- 3
24
6 9
3 22
4
- 2
-
1: - 3 2 3 2 3 3 1 3 1 2 2 I - - - - - - 1 2 1 3 3 1 3 3 2 1 3 2 1 - - -
2 1 2 3 1 2 1 3 2 2 3 1 3 -
-
4 1 2 1 2 4 3 1 2 1 1 1 1 1 1 1 1 2 1 3 1 2 2 3 2 1 3 2 3 2 2 2 3 3 2 1 - - - - - - 2 1 - - - 2 2
4 6 4 3 6 5 6 5 3 6 5 3 5 4 3 2 2 4 2 3 4 6 5 5 4 4 6 6 3 4 6 5 4 5 3 4 4 5 6 5 4 3 5 3 5 3 3 5 6
Mar
ital
st
atus
C
omm
ents
S S M
S S S S S S S S S S S S S S S S S S S S S S S S M
S M
S S S S S S S S S M
S S S S S S M
S S S
Hea
d in
jury
' -
-
-
Abn
orm
. E
EG
Abn
orm
. E
EG
-
-
-
-
Ast
hmat
ic
-
Hea
d in
jury
*
-
-
-
-
-
-
CD
hip
s C
D h
ips
-
Enc
epha
litis
* -
t K
ey:
S =
spa
stic
; A =
ath
etoi
d: H
= h
emip
legi
a; Q
= q
uadr
iple
gia;
D =
dip
legi
a.
$ 1 =
min
imal
; 2 =
ave
rage
; 3
= g
ood.
1
= m
ild;
2 =
mod
erat
e: 3
= s
ever
e.

GAVIN ANDREWS L. J. PLAT1
The level of physical disability was directly related to work and social adjust- ment, the less disabled being more successful. An interesting finding, in view of the fact that the speech handicap of the cerebral-palsied is often seen as limiting the expression of an active mind, was the weak relationship between speech com- petence and work or social success. This finding was unexpected and is probably evidence of the detailed care with which the Spastic Centre of New South Wales attempts to understand the needs of each individual and to place him in a compatible work and social environment.
Conclusions The cerebral-palsied child with multiple
handicaps may, without energetic re- habilitative effort, develop into an adult encased in contractured limbs and an untutored mind. With energetic rehabilita- tion, and despite the continuing presence
P. T. QUlNN P. D. NEILSON
of severe intellectual, sensory, speech and motor handicaps, they will be able to contribute useful work to society, live a meaningful social life and experience the peace of mind of their more fortunate compatriots.
Acknowledgements: This work was supported by the National Health and Medical Research Council of Australia, the Ramaciotti Foundations of New South Wales and the Spastic Centre of New South Wales. We are grateful to the men who co-operated so willingly in the assessment pro- cedures.
AUTHORS’ APPOINTMENTS J. G. Andrews, M.D., F.R.A.N.Z.C.P., M.R.C. Psych., Associate Professor of Psychiatry; Direc- tor, Human Communication Laboratory; Prince Henry Hospital, Sydney, N.S.W., Australia. L. J. Platt, Ph.D., Director, Department of Speech Pathology, The Hospital for Sick Children, 555 University Avenue, Toronto, Canada. P. T. Quinn, M.B., B.S., Ph.D., Project Scientist, Human Communication Laboratory, Prince Henry Hospital, Sydney, N.S.W., Australia. P. D. Neilson, Ph.D., Director, Spastic Centre Research Laboratory, Prince Henry Hospital, Sydney, N.S.W., Australia.
SUMMARY The physical disability, speech disability and mental health of 50 adult men with cerebral
palsy were measured. Most men needed help with self-care and in moving around, yet were able to do productive work in a work training unit. On average, only half their words were intelligible to normal listeners, yet their mental health scores were similar to those found in the normal population.
When their life adjustment was measured in terms of success in work and complexity of social life, it was found to be independent of their speech disability and mental health but directly commensurate with the extent of their physical disability. c
RESUME
Apprkciation de I’ktat d’adultes I.M.C. Le handicap nioteur, les difficultes de langage et la santt mentale de 50 adultes masculins
I.M.C. ont CtC apprCciCs. La plupart exigeaient de l’aide pour leurs soins personnels et leurs deplacements mais etaient capables d’un travail productif dans une unit6 d’entraine- ment au travail. Environ seulement la moitiC de leurs mots Ctait comprehensible par des interlocuteurs normaux et leur scores de santC mentale Ctaient semblables a ceux que Yon trouve dans une population normale.
Quand on apprkciait leur ajustement A la vie en terme de travail fourni et de complexite de vie sociale, cet ajustement paraissait independant de leur trouble du langage et de leur Ctat mental, mais directement en rapport avec l’importance de leur trouble physique.
809

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY.’ 1977, 19
ZUSAMMENFASSUNG
Eine Beurteilung des allgemeinen Status Erwuchsenev init Cerebralparese Bei 50 erwachsenen Mannern mit Cerebralparese wurden die physische Beeintrachtigung,
die Sprachbehinderung und die geistigen Fahigkeiten untersucht. Die meisten Manner benotigten Hilfe bei der Versorgung und um sich zu bewegen, sie konnten jedoch produktive Arbeit in Beschaftigungszentren leisten. Fur gewohnliche Zuhorer waren etwa nur die Halfte ihrer Worte verstandlich, der Durchschnitt ihrer geistigen Fahigkeiten entsprach jedoch ungefahr dem der Allgemeinbevolkerung.
Wenn man die Anpassung an ihr Leben gemessen am Erfolg bei der Arbeit und am sozialen Leben iiberhaupt beurteilt, so war diese unabhangig von der Sprachbehinderung und den geistigen Fahigkeiten sondern entsprach direkt dem Ausmass ihrer physischen Beeintrachtigung.
RESUMEN
Evaluacioit del estado de un grupo de adultos con pardisis cerebral A 50 adultos con pardisis cerebral se les midi6 su incapacidad fisica, incapacidad de la
palabra y salud mental. La mayoria de ellos necesitaban ayuda para valerse por si mismos y desplazarse, si bien eran capaces de realizar un trabajo productivo en una unidad de aprendizaje. Como tCrmino medio, solo la mitad de sus palabras eran intelegibles para 10s auditores normales, aunque el puntaje de su salud mental era similar a1 de la poblacion normal.
Cuando se midi6 su adaptaci6n a la vida normal, en tCrminos de Cxito en el trabajo y complegidad de vida social, se hallo que era independiente de su incapacidad de palabra y salud mental, per0 en relacion directa con la extension de su incapacidad fisica.
REFERENCES Andrews, G., Schonell, M., Tennant, C . (1977) ‘The relation between physical, psychological and social
Garrad, J., Bennett, A. E. (1971) ‘A validated interview schedule for use in population surveys of chronic
Goldberg, D. P. (1972) The Detection of Psychiatric Illness by Questionnaire. London: O.U.P. Gray, M. (1972) ‘Effects of hospitalization on work-play behavior.’ American Journal of Occupational
Platt, L. .I., Andrews, G., Young, M., Quinn, P. T. (1977) ‘Dysarthria of adult cerebral palsy: intelligibility
Raven, J. C. (1956) Guide to Using Progressive Matrices. London: H . K . Lewis. Vaillant, G. E. (1974) ‘Natural history of male psychological health. I I . Some antecedents of healthy adult
morbidity in a suburban community.’ American Journal of Epidemiology, 105, 324-329.
disease and disability.’ British Journal of Preventive and Social Medicine, 25, 97-104.
Therapy, 26, 180-185.
and articulatory impairment.’ Journal of Speech and Hearing Research, (in press).
adjustment.’ Archives of General Psychiatry, 31, 15-22.
810