ambulatory try off catheter (atoc) program for the patient ...€¦ · retention of urine –...
TRANSCRIPT

Ambulatory Try off Catheter (ATOC) Program for the
Patient with Acute Retention of Urine – Outpatient Service
Mr. Tang, Chi Chiu Kevin (APN)
Urology Center
Department of Surgery
Kwong Wah Hospital

Redevelopment Project of Kwong Wah Hospital

Redevelopment Project of Kwong Wah Hospital
Phase I and II
Total ~ 10 years till 2025
Department of Surgery
4 wards > 2.5 wards
inpatient services > outpatient services

ATOC program
Co-operation between Surgery and Emergency Department
Develop ATOC protocol
Selected Acute Retention Of Urine (AROU) patients
Ambulatory care
PWH, UCH…

AROU
Definition
Sudden and painful inability to void voluntarily (1)
Mx: bladder decompression
Urethral catheterization/ Suprapubic catheterization
Conventionally, Hospitalization x observation
Costly, hospital-acquired infection
Average 3-4 days
Try without catheter (TWOC) during admission
If failed, may need to re-admit for next TWOC

Benign Prostatic Hyperplasia (BPH)
Age and male hormonal stimulation
Increase cell number
Epithelial and stromal proliferation or impaired programmed cell death leading to cellular accumulation (8)
Obstructive and Irritative symptoms
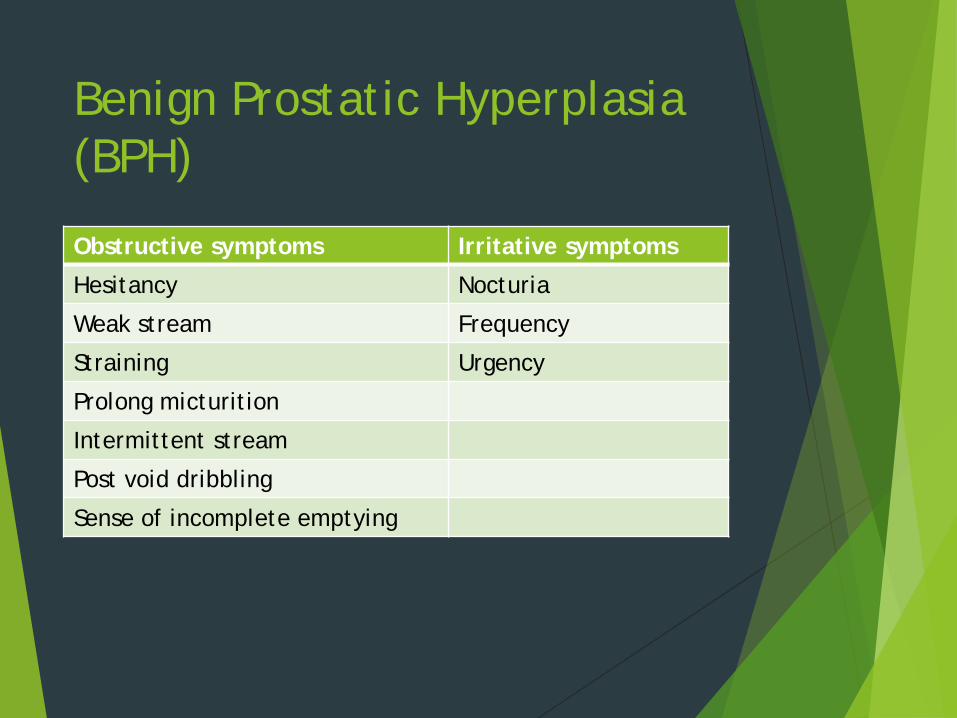
Benign Prostatic Hyperplasia (BPH)
Obstructive symptoms Irritative symptoms
Hesitancy Nocturia
Weak stream Frequency
Straining Urgency
Prolong micturition
Intermittent stream
Post void dribbling
Sense of incomplete emptying

Benign prostatic hyperplasia (BPH)
Majority of male AROU associate with BPH (2)
Over 50% male population aged 50-60 yrs had BPH (3,8)
Age Incidence of BPH
40-50 yr 20 %
50-60 yr 50 %
60-70 yr 55 %
70-80 yr 80 %
80-90 yr 90 %

Hong Kong Population (2016 Population By-census)
0
1000000
2000000
3000000
4000000
5000000
6000000
7000000
8000000
2006 2011 2016
No.
of
pers
ons
(pop
ulat
ion)
male female

Male 60+/65+(2016 Population By-census)
0
100000
200000
300000
400000
500000
600000
2006 2011 2016
No.
of
pers
ons
(pop
ulat
ion)
60+ 65+

4/2016-1/2017 AROU Hospitalization (male)
0
20
40
60
80
100
120
20 30 40 50 60 70 80 90
No.
of
pati
ents
Age distribution

9/2016-1/2017 ATOC program (male)
0
5
10
15
20
25
40 50 60 70 80 90 100
No.
of
pati
ents
Age distribution

ATOC program
Objective:
reduce unnecessary hospitalization and reduce bed occupancy
Manage AROU patient and try without catheter in outpatient setting
Analyze the economical outcomes

ATOC Program
Method:
ATOC Program established in 9/2016
Recruit 69 males selected AROU patients
Data collected from 9/2016 – 1/2017
Data Compared before and after established ATOC program


ATOC program
Medication prescribe in A&E
Harnal OCAS 0.4mg daily
Current on Hytrin, consider increase dosage, max: 6mg
Already on max dose, continue current dose

ATOC clinic in Urology Center
Mx in ATOC clinic:
Detail history
?side effect on medication, dizziness
Vital sign
Explanation of the pathophysiology of AROU
Male urinary system and anatomy
D/S PR if no B.O. ≥ 2 days
Try wean off foley
Physical exam and DRE
Phimosis, Paraphimosis, hernia, prostate nodule, hard prostate

ATOC clinic in Urology Center
Health education and counseling
Fluid management
Bladder training
Life style modification
Uroflow and PVRU
Repeat at least 2-3 times
Interpretation and explanation

ATOC clinic in Urology Center
Nurse led TRUS sizing (4,5)
Increase job satisfaction (4,5)
Releases medical staff for other activity (4,5)
Early detection on BPH
Shorten waiting time compare with x ray department

Success wean off catheter
Home
Bladder diary
Arrange uroflow before next Urology FU
IPSS on the day of uroflow
Telephone FU

Failed wean off catheter
Failed to void
Large RU, risk explanation, i.e. renal impairment
Counsel x learn CISC
Foley reinsertion if failed or not fit for CISC
Poor premorbid and advanced age, counsel x long term Foley or SPC
Refer CNS x Foley care
Urine x R/M, C/ST
Counsel x TURP
Video, pamphlet, Blood taking, CXR, KUB, ECG
Arrange early Urology FU

No. of 30 days readmission in ATOC program
AROU x 3
Suicidal idea ?due to Foley insertion x 1
Haematuria x 2
Unplanned readmission rate: 8.7%

Success rate of wean off catheter
0
10
20
30
40
50
60
70
80
90
100
Hospitalization (4/16-1/17) ATOC (9/16-1/17)
Succ
ess
wea
n of
f fo
ley
(%)

Comparisons before and after ATOC Program
Hospitalization Before ATOC (5 months)
Hospitalization After ATOC (5 months)
ATOC clinic (5 months)
No. of bed days 669 402 0
No. of patient 176 112 69
Mean length of stay
3.8±1.8 3.6±1.3 0
Mean catheterization day
3.4±3.4 3.3±1.2 6.8±2.4
Mean age 77.3±8.5 77.3±7.9 79±10.5
Total cost per patient (HKD)
19584 18618 3578.9
Success rate of wean off foley
60.2% 52.3% 62.3%

Estimated cost from HA Annual Report 2015-2016
Cost per A&E attendance (HKD): 1230
Cost of hospitalization per day (HKD): 4830
Cost per SOPD attendance (HKD): 1190

Estimated cost reduction and bed days after establish ATOC Program If all ATOC program patient need admission
The mean length of hospital stay: 3.6 days
Total saving bed days: 248.4 days
Total cost per patient: 4830 x 3.6 + 1230 = 18618 (HKD)
Total cost of all patients: 18618 x 69 = 1284642 (HKD)
Total cost reduction: Total cost of all ATOC patients – total cost in ATOC program:
= 1284642 – 246950
= 1037692 (total cost saving in 5 months)

conclusion
The ATOC program is effective
Reduce unnecessary hospitalization
Reduce bed occupancy in surgical ward
Reduce cost
Increase job satisfactory
Early detection on BPH
Early suitable Tx to patient
Increase patient satisfaction

Discussion
Currently one ATOC session/week
The duration of the catheterization
Mean catheterization day: 6.82±2.41 (range from 1-13)
Future may increase two session/week
May be regular audit/meeting for discuss the case pathway for recruit more patient
Not enough patient: due to pilot phase, some patient refuse, not all the physician refer patient to ATOC


Reference
1. Emberton M, Anson K (1999). Acute urinary retention in men: an age old problem. BMJ 318(7188): 921-925
2. Choong S, Emberton M (2000). Acute urinary retention. BJU, 85(2), 186-201
3. Berry SJ, Coffey DS, Walsh PC, Ewing LL (1984). The development of human benigh prostatic hyperplasia with age. J Urol, 132(3), 474-479
4. Nicola J & Gail MP (2008). The success of a nurse-led, one-stop suspected prostate cancer clinic. Cancer nursing practice, 7(3), 28-32
Reference
5. Wright L (2006). Sonographer or nurse-led transrectal ultrasound (trus) and biopsy. Synerygy, , 24-27.
6. Hospital authority annual report 2015-2016
7. 2016 Population By-census
8. McConnell, J (1998). Epidemiology, Etiology, Pathophysiology, and Diagnosis of Benign Prostatic Hyperplasia. In Walsh, P., Retik, A., Vaughan, D. & Wein, A. (Ed.), Campbell’s Urology (pp1429-1452)