alzheimer’s disease diagnosis and treatment j. wesson ashford, m.d., ph.d. stanford / va...
TRANSCRIPT

ALZHEIMER’S DISEASEALZHEIMER’S DISEASEDIAGNOSIS and TREATMENTDIAGNOSIS and TREATMENT
J. Wesson Ashford, M.D., Ph.D.J. Wesson Ashford, M.D., Ph.D.Stanford / VA Alzheimer’s CenterStanford / VA Alzheimer’s Center
VAMC, Palo Alto, CaliforniaVAMC, Palo Alto, California
San Francisco, CaliforniaSan Francisco, CaliforniaOctober 5, 2004October 5, 2004
Slides at: Slides at: www.medafile.comwww.medafile.com (Dr. Ashford’s (Dr. Ashford’s lectures)lectures)

Alzheimer IssuesAlzheimer Issues
Definition of dementia, differential Definition of dementia, differential diagnosisdiagnosis
Epidemiology (why diagnosis is important)Epidemiology (why diagnosis is important) Diagnosis of Alzheimer’s disease (how to)Diagnosis of Alzheimer’s disease (how to) Treatment optionsTreatment options
The need to treatThe need to treat The benefits of cholinesterase inhibitorsThe benefits of cholinesterase inhibitors The advantage of galantamine (Reminyl)The advantage of galantamine (Reminyl)

Dementia DefinitionDementia Definition
Multiple Cognitive Deficits:Multiple Cognitive Deficits: Memory dysfunctionMemory dysfunction
especially new learning, a prominent especially new learning, a prominent early symptomearly symptom
At least one additional cognitive deficitAt least one additional cognitive deficit aphasia, apraxia, agnosia, or aphasia, apraxia, agnosia, or
executive dysfunctionexecutive dysfunction Cognitive Disturbances:Cognitive Disturbances:
Sufficiently severe to cause impairment Sufficiently severe to cause impairment of occupational or social functioning of occupational or social functioning and and
Must represent a decline from a Must represent a decline from a previous level of functioningprevious level of functioning

Differential Diagnosis: Differential Diagnosis: Top Ten Top Ten
(commonly used mnemonic device: AVDEMENTIA)(commonly used mnemonic device: AVDEMENTIA)1.1. AAlzheimer Disease (pure ~40%, + mixed~70%, ? lzheimer Disease (pure ~40%, + mixed~70%, ? dLbd)dLbd)
2.2. VVascular Disease, MID (5-20%)ascular Disease, MID (5-20%)3.3. DDrugs, rugs, DDepression, epression, DDeliriumelirium4.4. EEthanolthanol (5-15%) (5-15%)5.5. MMedical / edical / MMetabolic Systemsetabolic Systems6.6. EEndocrine (thyroid, diabetes), ndocrine (thyroid, diabetes), EEars, ars, EEyes, yes, EEnviron.nviron.7.7. NNeurologic (other primary degenerations, fronto-eurologic (other primary degenerations, fronto-
temporaltemporal- Consider diffuse Lewy body dementia, Parkinson - Consider diffuse Lewy body dementia, Parkinson
component)component)8. 8. TTumor, umor, TToxin, oxin, TTraumarauma9.9. IInfection, nfection, IIdiopathic, diopathic, IImmunologicmmunologic10. 10. AAmnesia, mnesia, AAutoimmune, utoimmune, AApnea, pnea, AAAMIAMIAdapted from Yesavage, 1979

Diagnostic Criteria For Diagnostic Criteria For Dementia Of The Alzheimer Dementia Of The Alzheimer
TypeType (DSM-IV, APA, 1994)(DSM-IV, APA, 1994)
A.A. Multiple Cognitive DeficitsMultiple Cognitive Deficits1. Memory Impairment 1. Memory Impairment 2. Other Cognitive Impairment2. Other Cognitive Impairment
B. Deficits Impair Social/Occupational B. Deficits Impair Social/Occupational C.C. Course Shows Gradual Onset And DeclineCourse Shows Gradual Onset And DeclineD.D. Deficits Are Not Due to:Deficits Are Not Due to:
1. Other CNS Conditions1. Other CNS Conditions2. Substance Induced Conditions2. Substance Induced Conditions
E. Do Not Occur Exclusively during DeliriumE. Do Not Occur Exclusively during DeliriumF. Not Due to Another Psychiatric DisorderF. Not Due to Another Psychiatric Disorder

PREVALENCE of AD PREVALENCE of AD Estimated 4 million cases in US (2000)Estimated 4 million cases in US (2000)
(2000 - 46 million individuals over 60 y/o)(2000 - 46 million individuals over 60 y/o) Estimated 500,000 new cases per yearEstimated 500,000 new cases per year Increase with age (prevalence)Increase with age (prevalence)
1% of 60 - 65 (10.7m) = 107,000 1% of 60 - 65 (10.7m) = 107,000 2% of 65 - 70 ( 9.4m) = 188,0002% of 65 - 70 ( 9.4m) = 188,000 4% of 70 - 75 ( 8.7m) = 350,0004% of 70 - 75 ( 8.7m) = 350,000 8% of 75 - 80 ( 7.4m) = 595,0008% of 75 - 80 ( 7.4m) = 595,000 16% of 80 - 85 ( 5.0m) = 800,00016% of 80 - 85 ( 5.0m) = 800,000

U.S. Census 2000 by age
0
250,000
500,000
750,000
1,000,000
1,250,000
1,500,000
1,750,000
2,000,000
2,250,000
2,500,000
0 10 20 30 40 50 60 70 80 90 100
Age
# p
eo
ple
Males,138,053,563Females,143,368,343
Total = 281,421,906>60 = 45,809,291>65 = 35,003,844>85 = 4,251,678>100= 62,545
www.census.gov
JW Ashford, MD PhD, 2003

U.S. mortality by age - 1999
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
0 10 20 30 40 50 60 70 80 90 100
Age
Nu
mb
er
of
pe
op
le
Males, 1,175,460
Females, 1,215,939
www.cdc.gov
JW Ashford, MD PhD, 2003

U.S. mortality rate by age1999 CDC / 2000 census
0.0001
0.0010
0.0100
0.1000
1.0000
0 10 20 30 40 50 60 70 80 90 100
Age
prob
abi
lity
MalesFemalesAlzheimer incidence
JW Ashford, MD PhD, 2003

Mortality EquationsMortality Equationst = age in yearst = age in years
Td = time for mortality rate to Td = time for mortality rate to doubledouble
Ro = mortality rate at time zeroRo = mortality rate at time zeroalpha = ln(2) / Tdalpha = ln(2) / Td
Mortality rate u(t)Mortality rate u(t)R = Ro x exp (alpha x t)R = Ro x exp (alpha x t)
Survival curve s(t)Survival curve s(t)S = exp ( - Ro/alpha x (exp (alpha x t) –1 ))S = exp ( - Ro/alpha x (exp (alpha x t) –1 ))
Number of deaths per year d(t)Number of deaths per year d(t)D = -ds/dt = ( Ro + alpha x ln (1/s(t) )) x D = -ds/dt = ( Ro + alpha x ln (1/s(t) )) x s(t)s(t)
= u(t) x s(t)= u(t) x s(t)

Probability Not Demented
00.10.20.30.40.50.60.70.80.9
1
50 60 70 80 90 100
Age
Pro
po
rtio
n o
f p
op
ula
tio
n
JW Ashford, MD PhD, 2003

U.S. Alzheimer Incidence
(4 million / 8yr)
02000400060008000
10000120001400016000
50 60 70 80 90 100
Age
# /
yr
male=170,603
female=329,115
JW Ashford, MD PhD, 2003
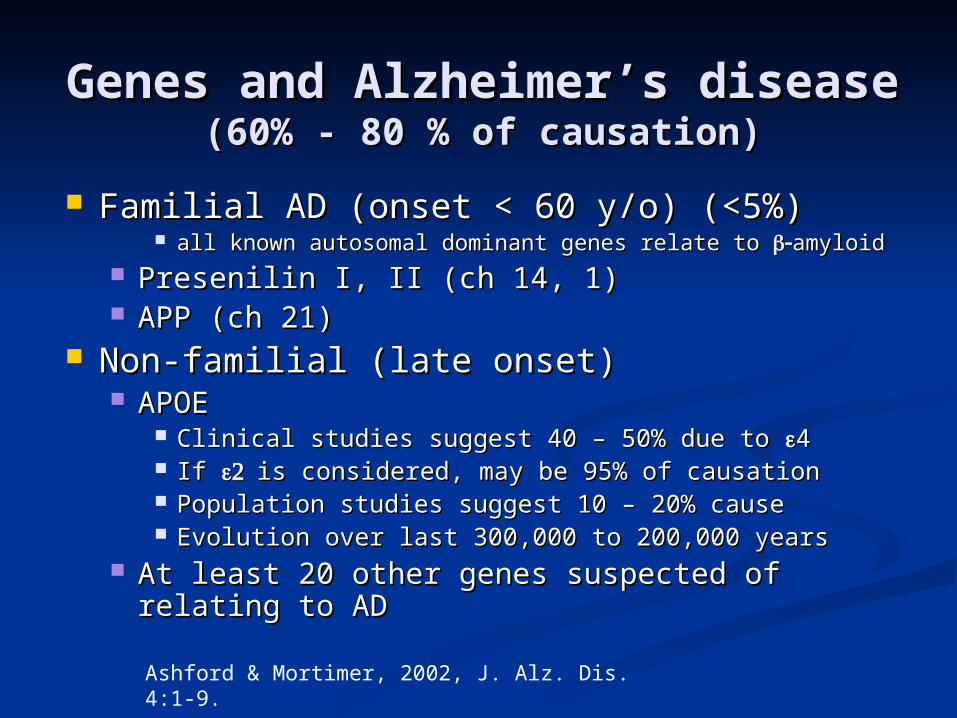
Genes and Alzheimer’s diseaseGenes and Alzheimer’s disease(60% - 80 % of causation)(60% - 80 % of causation)
Familial AD (onset < 60 y/o) (<5%)Familial AD (onset < 60 y/o) (<5%) all known autosomal dominant genes relate to all known autosomal dominant genes relate to amyloidamyloid
Presenilin I, II (ch 14, 1)Presenilin I, II (ch 14, 1) APP (ch 21)APP (ch 21)
Non-familial (late onset)Non-familial (late onset) APOEAPOE
Clinical studies suggest 40 – 50% due to Clinical studies suggest 40 – 50% due to 44 If If is considered, may be 95% of causationis considered, may be 95% of causation Population studies suggest 10 – 20% causePopulation studies suggest 10 – 20% cause Evolution over last 300,000 to 200,000 yearsEvolution over last 300,000 to 200,000 years
At least 20 other genes suspected of relating to At least 20 other genes suspected of relating to ADAD
Ashford & Mortimer, 2002, J. Alz. Dis. 4:1-9.

APO-E genotype and AD riskAPO-E genotype and AD risk46 Million in US > 60 y/o //// 4 Million have AD46 Million in US > 60 y/o //// 4 Million have AD
(data from Saunders et al., 1993; Farrer et al., 1997)(data from Saunders et al., 1993; Farrer et al., 1997)
GenT %pop %AD #pop #AD risk If all US
E2/2 1% 0.1% 0.5M .004M 0.8% .4 M
E2/3 12 % 4% 5.5M .18M 3.2% 1.5 M
E3/3 60% 35% 27.6M 1.4M 5.1% 2.3 M
E3/4 21% 42% 9.6M 1.7M 18% 8.2 M
E4/4 2% 16% .9M .6M 67% 30.7M
JW Ashford, MD PhD, 2003

Dementia rate, for Td = 5 yrs
0.0001
0.001
0.01
0.1
1
10
100
1000
50 60 70 80 90 100
Age
Nu
mb
er
of
peo
ple
/yr
mean rateAPOE 4/4APOE 3/4APOE 3/3presenilin
J. W. Ashford, 2004

Probability Not Demented
00.10.20.30.40.50.60.70.80.9
1
50 60 70 80 90 100
Age
Pro
po
rtio
n o
f p
op
ula
tio
n
mean rateAPOE 4/4APOE 3/4APOE 3/3presenilin
J. W. Ashford, 2004

Probability of Dementia Onset
0
0.01
0.02
0.03
0.04
0.05
0.06
50 60 70 80 90 100
Age
pro
bab
ilit
y / y
r
mean rateAPOE 4/4APOE 3/4APOE 3/3Presenilin J. W. Ashford, 2004

U.S. Dementia Incidence by APOE(% of cases)
00.10.20.30.40.50.60.70.80.9
1
50 60 70 80 90 100Age
% D
ev
elo
pin
g/Y
ea
r
4/4 3/4 3/3
JW Ashford, MD PhD, 2000

Estimated Number of New AD Cases, in Thousands
377 411 454 491615
820959
0
200
400
600
800
1000
1200
1995 2000 2010 2020 2030 2040 2050
1000

Reprinted with permission from Brumback, RA, Leech RW, J. Ohio State Med Assoc. 1994: 87, 103-111

ECONOMIC IMPACT OF ECONOMIC IMPACT OF ADAD
2 million AD patients in nursing homes2 million AD patients in nursing homes Projection to California – 240,000Projection to California – 240,000
Nursing homes cost - $120 to $160 per dayNursing homes cost - $120 to $160 per day Annualized cost of nursing homes rangesAnnualized cost of nursing homes ranges
from $40,000 to $70,000 per yearfrom $40,000 to $70,000 per year Nursing Home Care of AD patients costs $80 Nursing Home Care of AD patients costs $80
billion per yearbillion per year for life-time cost – about $175,000 per patientfor life-time cost – about $175,000 per patient
The majority of patients live at home and The majority of patients live at home and are cared for by family and friendsare cared for by family and friends
With lost wages of patients and families plus With lost wages of patients and families plus costs for non-nursing home patients:costs for non-nursing home patients: Total costs: $Total costs: $120 billion annually120 billion annually ( (Am J Publ HlthAm J Publ Hlth)) Projection to California – $14.5 billion annually!Projection to California – $14.5 billion annually!

AD Can Be Readily AD Can Be Readily DiagnosedDiagnosed
A diagnosis of Alzheimer’s disease can be A diagnosis of Alzheimer’s disease can be made with a high degree of certaintymade with a high degree of certainty
Using NINCDS-ADRDA criteria, accuracy Using NINCDS-ADRDA criteria, accuracy in in autopsy-verified cases is approximately autopsy-verified cases is approximately 90%90%
Diagnosis is a 2-step process:Diagnosis is a 2-step process: Detection through screeningDetection through screening Confirmation through patient history and Confirmation through patient history and
physical, caregiver interview, brain imaging, physical, caregiver interview, brain imaging, and appropriate laboratory studiesand appropriate laboratory studies
McKhann G et al. Neurology. 1984;34:939-944. Kazee AM et al. Alzheimer Dis Assoc Disord. 1993;7:152-164.Ashford JW et al, Psychiaric Annals, 1996;26:262-268.

AD Is Often MisdiagnosedAD Is Often Misdiagnosed
Source: Consumer Health Sciences, LLC. Alzheimer’s Caregiver Project. 1999.
Patient initially diagnosed with AD
Patient’s first diagnosis other than AD
Yes 28%
NoNo 72% 72%
21%
7%
9%
14%
14%
35%
Normal aging
Depression No diagnosis
Dementia (not AD) Stroke
Other

AD is Under-diagnosedAD is Under-diagnosed Early Alzheimer’s disease is subtle, the diagnosis continues Early Alzheimer’s disease is subtle, the diagnosis continues
to be missed to be missed it is easy for family members to avoid the problem and compensate it is easy for family members to avoid the problem and compensate
for the patient for the patient physicians tend to miss the initial signs and symptomsphysicians tend to miss the initial signs and symptoms
Less than half of AD patients are diagnosedLess than half of AD patients are diagnosed Estimates are that 25% to 50% of cases remain undiagnosedEstimates are that 25% to 50% of cases remain undiagnosed Diagnoses are missed at all levels of severity: mild, moderate, Diagnoses are missed at all levels of severity: mild, moderate,
severesevere Undiagnosed AD patients often face avoidable social, Undiagnosed AD patients often face avoidable social,
financial, and medical problemsfinancial, and medical problems Early diagnosis and appropriate intervention may lessen Early diagnosis and appropriate intervention may lessen
disease burdendisease burden Early treatment may improve overall course substantiallyEarly treatment may improve overall course substantially
No definitive laboratory test for diagnosing AD existsNo definitive laboratory test for diagnosing AD exists Efforts to develop biomarkers, early recognition by brain scanEfforts to develop biomarkers, early recognition by brain scan
Evans DA. Milbank Quarterly. 1990; 68:267-289

AssessmentAssessmentHistory Of The Development Of The DementiaHistory Of The Development Of The Dementia
Ask the Patient What Problem Has Brought Him to See Ask the Patient What Problem Has Brought Him to See YouYou
Ask the Family, Companion about the ProblemAsk the Family, Companion about the Problem Specifically Ask about Memory ProblemsSpecifically Ask about Memory Problems Ask about the First SymptomsAsk about the First Symptoms Enquire about Time of OnsetEnquire about Time of Onset Ask about Any Unusual Events Around the Time of Onset, Ask about Any Unusual Events Around the Time of Onset,
e.g., stress, trauma, surgerye.g., stress, trauma, surgery Ask about Nature and Rate of Progression, Activities of Ask about Nature and Rate of Progression, Activities of
Daily LivingDaily Living
Physical ExaminationPhysical Examination Neurological ExaminationNeurological Examination Neuropsychological AssessmentNeuropsychological Assessment Routine Laboratory TestsRoutine Laboratory Tests Brain ScanBrain Scan

LABORATORY TESTS LABORATORY TESTS (routine)(routine)
BLOOD TESTSBLOOD TESTS electrolytes, liver, kidney function tests, electrolytes, liver, kidney function tests,
glucoseglucose thyroid function tests (T3, T4, FTI, TSH)thyroid function tests (T3, T4, FTI, TSH) vitamin B12, folatevitamin B12, folate complete blood count, ESRcomplete blood count, ESR VDRL, HIV (if indicated)VDRL, HIV (if indicated)
EKG (if indicated)EKG (if indicated) CHEST X-RAY (if indicated)CHEST X-RAY (if indicated) URINALYSISURINALYSIS ANATOMICAL BRAIN SCAN – CT (cheapest), MRIANATOMICAL BRAIN SCAN – CT (cheapest), MRI

SPECIAL LABORATORY SPECIAL LABORATORY TESTS TESTS
FUNCTIONAL BRAIN IMAGING FUNCTIONAL BRAIN IMAGING (SPECT, PET – Medicare will pay special (SPECT, PET – Medicare will pay special cases)cases)
EEG, Evoked Potentials (P300)EEG, Evoked Potentials (P300) REACTION TIMES (slowed in the elderly, REACTION TIMES (slowed in the elderly,
especially when complex response is requiredespecially when complex response is required CSF ANALYSIS - ROUTINE STUDIESCSF ANALYSIS - ROUTINE STUDIES
ELEVATED TAU (future possible)ELEVATED TAU (future possible) DECREASED AMYLOID (future possible)DECREASED AMYLOID (future possible)
HEAVY METAL SCREEN (24 hr urine)HEAVY METAL SCREEN (24 hr urine) GENOTYPINGGENOTYPING
APO-LIPOPROTEIN-E (for supporting dx)APO-LIPOPROTEIN-E (for supporting dx) AUTOSOMAL DOMINANT (young onset)AUTOSOMAL DOMINANT (young onset)

Why Diagnose AD Early?Why Diagnose AD Early?
Safety (driving, compliance, cooking, etc.)Safety (driving, compliance, cooking, etc.) Family stress and misunderstanding (blame, denial) Family stress and misunderstanding (blame, denial) Early education of caregivers of how to handle patient Early education of caregivers of how to handle patient
(choices, getting started)(choices, getting started) Advance planning while patient is competent (will, proxy, Advance planning while patient is competent (will, proxy,
power of attorney, advance directives)power of attorney, advance directives) Patient’s and Family’s right to knowPatient’s and Family’s right to know Promotes advocacy for research and treatment developmentPromotes advocacy for research and treatment development Specific treatments now availableSpecific treatments now available
May slow underlying disease process, the sooner the betterMay slow underlying disease process, the sooner the better May delay nursing home placement longer if started earlierMay delay nursing home placement longer if started earlier May prevent conversion from Mild Cognitive Impairment to ADMay prevent conversion from Mild Cognitive Impairment to AD

Estimate MMSE as a function of time
0
5
10
15
20
25
30
-10 -8 -6 -4 -2 0 2 4 6 8 10
Estimated years into illness
MM
SE
scor
e
AAMI / MCI/ early AD -- DEMENTIA
ALZHEIMER’S DISEASE
Ashford et al., 1995

Need to Develop Better ScreeningNeed to Develop Better Screening and Early Assessment Tools and Early Assessment Tools
Genetic vulnerability testing (trait risk)Genetic vulnerability testing (trait risk) Vulnerability factors (education, occupation, head Vulnerability factors (education, occupation, head
injury)injury) Early recognition (10 warning signs)Early recognition (10 warning signs) Screening tools (6th vital sign in elderly)Screening tools (6th vital sign in elderly) Positive diagnostic testsPositive diagnostic tests
CSF – tau levels elevated, amyloid levels lowCSF – tau levels elevated, amyloid levels low Brain scan – PET – DDNP, Congo-red derivativesBrain scan – PET – DDNP, Congo-red derivatives
Mild Dementia severity assessmentsMild Dementia severity assessments Detecting early change over timeDetecting early change over time
predicting progression, measuring ratepredicting progression, measuring rate

Alzheimer Warning SignsAlzheimer Warning SignsTop TenTop Ten
Alzheimer AssociationAlzheimer Association
1. Recent memory loss affecting job1. Recent memory loss affecting job 2. Difficulty performing familiar 2. Difficulty performing familiar
taskstasks 3. Problems with language3. Problems with language 4. Disorientation to time or place4. Disorientation to time or place 5. Poor or decreased judgment5. Poor or decreased judgment 6. Problems with abstract thinking6. Problems with abstract thinking 7. Misplacing things7. Misplacing things 8. Changes in mood or behavior8. Changes in mood or behavior 9. Changes in personality 9. Changes in personality 10. Loss of initiative10. Loss of initiative

Need for a Brief Screening Need for a Brief Screening Test for Dementia, Test for Dementia,
Alzheimer’s DiseaseAlzheimer’s Disease Recent evidence of benefits of anti-Recent evidence of benefits of anti-
cholinesterase agents in the treatment of cholinesterase agents in the treatment of mild Alzheimer’s diseasemild Alzheimer’s disease Improvement of cognitionImprovement of cognition Slowing of progressionSlowing of progression Delay of conversion to diagnosisDelay of conversion to diagnosis
How to get elderly, clinicians interested in How to get elderly, clinicians interested in screening for dementiascreening for dementia
How to handle positive screens sensitively How to handle positive screens sensitively and efficientlyand efficiently Doctors have been reluctant to diagnose Doctors have been reluctant to diagnose
Alzheimer’s disease because of the time required Alzheimer’s disease because of the time required to explain the problem to the family and to to explain the problem to the family and to coordinate treatment.coordinate treatment.

Brief Alzheimer Screen (BAS)Brief Alzheimer Screen (BAS) Repeat these three words: “apple, table, penny”.Repeat these three words: “apple, table, penny”. So you will remember these words, repeat them again.So you will remember these words, repeat them again. What is today’s date? What is today’s date?
D = 1 if within 2 days.D = 1 if within 2 days. Spell the word “WORLD” backwardsSpell the word “WORLD” backwards
S = 1 point for each word in correct orderS = 1 point for each word in correct order ““Name as many animals as you can in 30 seconds, GO!”Name as many animals as you can in 30 seconds, GO!”
A = number of animals A = number of animals ““What were the 3 words I asked you to repeat?” (no prompts)What were the 3 words I asked you to repeat?” (no prompts)
R = 1 point for each word recalledR = 1 point for each word recalled
BBAS = 3 x AS = 3 x RR + 2/3 x + 2/3 x AA + 5 x + 5 x DD + 2 x + 2 x SS
(Mendiondo et al., 2003)(Mendiondo et al., 2003)

Dementia Screening TestDementia Screening Test Need test to screen patients for Alzheimer’s diseaseNeed test to screen patients for Alzheimer’s disease Test needs to be on multiple platforms:Test needs to be on multiple platforms:
Doctor’s officesDoctor’s offices Best if computerized for rapid, objective assessmentBest if computerized for rapid, objective assessment World-Wide Web – based testing, World-Wide Web – based testing, CD-distributionCD-distribution KIOSK administration – drug stores, shopping mallsKIOSK administration – drug stores, shopping malls
Test needs to be very brief (about 1-minute)Test needs to be very brief (about 1-minute) Multiple test forms needed so it can be repeated Multiple test forms needed so it can be repeated
often often (quarterly)(quarterly) Screening should be done yearly after age 50, and Screening should be done yearly after age 50, and
repeated every 3 months for individuals over 65 repeated every 3 months for individuals over 65 years of age or with concernsyears of age or with concerns
Any change over time needs to be detectedAny change over time needs to be detected The test should be freeThe test should be free
MEMTRAX - Memory TestMEMTRAX - Memory Test(to detect AD onset)(to detect AD onset)
New test to screen patients for AD: New test to screen patients for AD: World-Wide Web – based testing, World-Wide Web – based testing, CD-distributionCD-distribution KIOSK administrationKIOSK administration
Determine level of ability / impairmentDetermine level of ability / impairment Test takes about 1-minuteTest takes about 1-minute Test can be repeated often Test can be repeated often (e.g., quarterly)(e.g., quarterly) Any change over time can be detectedAny change over time can be detected Free test is at: Free test is at: www.medafile.comwww.medafile.com

FIRST SUCCESSFUL FIRST SUCCESSFUL TREATMENT:TREATMENT:
CHOLINESTERASE INHIBITIONCHOLINESTERASE INHIBITION (1st double blind study - Ashford et al., 1981)(1st double blind study - Ashford et al., 1981)
Presumably increases acetylcholine at Presumably increases acetylcholine at synapsessynapses
Improvement in cognition Improvement in cognition (? 6-12 months (? 6-12 months better)better)
Improvement in function Improvement in function (ADLs, variable)(ADLs, variable) Improvement in behavior Improvement in behavior (? basal ganglia)(? basal ganglia) Slowing of disease courseSlowing of disease course
Treatment delays nursing home placement Treatment delays nursing home placement There is loss of benefit with delay of treatmentThere is loss of benefit with delay of treatment
Need to consider early interventionNeed to consider early intervention

Treatment of Alzheimer’s Treatment of Alzheimer’s DiseaseDisease
Source: Decision Resources, March 2000.
* Any drug treatment, not limited to acetylcholinesterase inhibitors.
0
1
2
3
4
5P
atie
nts
(m
illi
on
s)
Prevalence
4,523,100
Diagnosed
2,261,600
Treated*
904,600
Treated with AChEIs
543,800


Cholinergic Changes in Cholinergic Changes in ADAD
The most prominent neurotransmitter The most prominent neurotransmitter abnormalities are cholinergicabnormalities are cholinergic Reduced activity of choline acetyltransferase Reduced activity of choline acetyltransferase
(synthesis of acetylcholine)(synthesis of acetylcholine)11
Reduced number of cholinergic neurons in Reduced number of cholinergic neurons in late AD (particularly in basal forebrain)late AD (particularly in basal forebrain)22
Selective loss of nicotinic receptor Selective loss of nicotinic receptor subtypes in hippocampus and cortexsubtypes in hippocampus and cortex1,31,3
1. Bartus RT et al. Science. 1982;217:408-414. 2. Whitehouse PJ et al. Science. 1982;215:1237-1239. 3. Guan ZZ et al. J Neurochem. 2000;74:237-243.


Stimulated by acetylcholinethrough muscarinic receptor
Favored when lipid raft too large
Lipid raftFormed by cholesterolTransported by ApoEFrom macroglia
intracellularextra cellular
NEXIN? To establishnew connections
? Free-radical generator? To remove old synapses
JW Ashford, MD PhD, 2003
Need to divide effects of drug Need to divide effects of drug treatment into 2 groupstreatment into 2 groups
Acute effects of treatmentAcute effects of treatment e.g., 3 monthse.g., 3 months are the acute effects related to severity?are the acute effects related to severity?
e.g., do AChEases may work very well in mild patients,e.g., do AChEases may work very well in mild patients, and in nursing home patients?and in nursing home patients? do these medications work in very early phases of the disease?do these medications work in very early phases of the disease?
Chronic effects of treatment Chronic effects of treatment rate of change, after acute effectsrate of change, after acute effects are the effects on rate of change related to severityare the effects on rate of change related to severity
are very mild patients improved over time by AChEases?are very mild patients improved over time by AChEases? are new AChEase molecules created which require dose are new AChEase molecules created which require dose
increases?increases? does sudden discontinuation lead to catastrophic decline?does sudden discontinuation lead to catastrophic decline?
do early, chronic benefits suggest prevention? do early, chronic benefits suggest prevention?

ExelonExelonImproves Cognitive Function: Improves Cognitive Function:
ADAS-Cog mean change from baselineADAS-Cog mean change from baseline††
Mea
n c
han
ge
inA
DA
S-C
og
sco
re
Improvement
Worsening
12 18 26
Weeks
***
6–12 mg/day Exelon® 1–4 mg/day Exelon® Placebo
**
†B352 OC study analysis; *p<0.05 vs placebo
4.94
2
1
0
–1
–2
–3
–4
–5
Corey-Bloom J et al, for the ENA 713 B352 Study Group. Int J Geriatr Psychopharmacol. 1998;1:55-65.

ExelonExelon Longterm Effects on Cognition: Longterm Effects on Cognition:Mean Change in ADAS-Cog from Mean Change in ADAS-Cog from
Baseline at Week 52Baseline at Week 52
-7
-6
-5
-4
-3
-2
-1
0
1
0 10 20 30 40 50 60
Study Week
AD
AS
-Co
g M
ea
n C
ha
ng
e
fro
m B
as
elin
e
6-12 mg
1-4 mg
Placebo
Proj. PBO All Patients Taking Exelon
B352 Patients in B353 (OC) at Week 52
*
*
*
* p< 0.05 vs projected placebo
*
**
*
*
*
Sohn et al. In: Proceedings of the CPNP. April 2000.

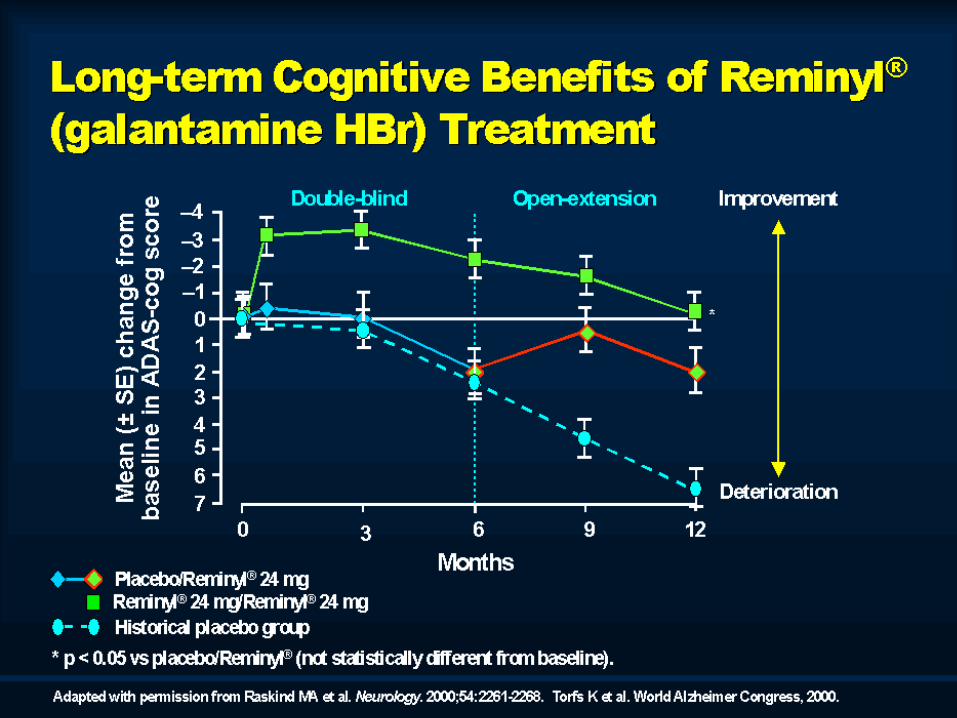

REMINYLREMINYL®® (galantamine HBr) Pooled Analysis: (galantamine HBr) Pooled Analysis:
Change in ADAS-cog Scores at 6 and 12 MonthsChange in ADAS-cog Scores at 6 and 12 Months
Advanced Moderate AD Patients With Baseline ADAS-cog Scores >30
Adapted from Blesa R et al. Dement Geriatr Cogn Discord. 2003;15:79-87.
*p<0.001 vs placebo.†p<0.001 vs historical placebo. ‡Not significant vs baseline.Baseline ADAS-cog score: 37.3 (REMINYL 24 mg/d) vs 37.4 (placebo).
Imp
rove
men
t
Mea
n (
SE
) C
han
ge
in
AD
AS
-co
g F
rom
Bas
elin
e–8
–6
–4
–2
0
2
4
6
8
10
12
Baseline 1 3 6 9 12
Time (mo)
† ‡
REMINYL 24 mg/d
Placebo from RCTs
Historical placebo
* ** †




GAL-GBR-2GAL-GBR-2MMSE: Change From BaselineMMSE: Change From Baseline
* p 0.0001 vs baseline; † p = 0.0006 vs baseline; # p = 0.0003 vs baseline. NS = p > 0.1.
–2.5
–2
–1.5
–1
–0.5
0
0.5
1
1.5
2
2.5
Mea
n M
MS
E c
han
ge
(± S
E)
fro
m b
asel
ine
†
#
**
NS
Reminyl® (galantamine HBr)(n = 94)Aricept® (n = 87)
Weeks0 13 26 39 52
Data on file, Janssen Pharmaceutica Products, L.P. Bullock R et al. Poster presented at the 41st Annual Meeting of the ACNP, San Juan, Puerto Rico, December 8–12, 2002.
.

Benefits of Treatment of Benefits of Treatment of AD With AD With
Acetylcholinesterase Acetylcholinesterase InhibitorsInhibitors AChEIs may improve, maintain, or slow the decline AChEIs may improve, maintain, or slow the decline
of cognitive, behavioral, and functional of cognitive, behavioral, and functional performance in patients with mild-to-moderate ADperformance in patients with mild-to-moderate AD
Delay of treatment leads to loss of potential benefitDelay of treatment leads to loss of potential benefit AChEIs may delay nursing home placement over 20 AChEIs may delay nursing home placement over 20
months, and potentially much more when started months, and potentially much more when started early.early.
AChEIs have demonstrated consistent efficacy and AChEIs have demonstrated consistent efficacy and safety in maintaining cognitive function, as safety in maintaining cognitive function, as measured by ADAS-cog in patients with mild-to-measured by ADAS-cog in patients with mild-to-moderate AD for up to 1 year – relative to placebo!!moderate AD for up to 1 year – relative to placebo!!
DonepezilDonepezil11 38 weeks38 weeks RivastigmineRivastigmine22 38–42 weeks38–42 weeks GalantamineGalantamine33 52 weeks (25-30% 52 weeks (25-30%
better)better)1. Rogers SL et al. Eur Neuropsychopharmacol. 2000;10:195-203. 2. Farlow M et al. Eur Neurol. 2000;44:236-241.3. Raskind MA et al. Neurology. 2000;54:2261-2268.

IndicationsIndications REMINYL® (galantamine HBr) is is approved for the approved for the
treatment of patients with mild-to-moderate treatment of patients with mild-to-moderate dementia of the Alzheimer’s typedementia of the Alzheimer’s type
The most frequent adverse events associated with The most frequent adverse events associated with REMINYL included nausea, vomiting, diarrhea, REMINYL included nausea, vomiting, diarrhea, anorexia, and weight loss; most were generally anorexia, and weight loss; most were generally transient and mild to moderate in severitytransient and mild to moderate in severity
REMINYL is available in 4-mg, 8-mg and 12-mg REMINYL is available in 4-mg, 8-mg and 12-mg tablets and an oral solution (4 mg/mL) and is taken tablets and an oral solution (4 mg/mL) and is taken twice a day, preferably with morning and evening twice a day, preferably with morning and evening mealsmeals
May benefit very early cases, particular APOE-e4 May benefit very early cases, particular APOE-e4 carrierscarriers

ReminylReminyl®® (galantamine (galantamine HBr): Proposed HBr): Proposed
Mechanisms of ActionMechanisms of Action Increases amount of acetylcholine available in Increases amount of acetylcholine available in
synaptic cleft by inhibiting breakdown of synaptic cleft by inhibiting breakdown of acetylcholineacetylcholine
By modulating activity at nicotinic receptors, it may By modulating activity at nicotinic receptors, it may increase release of acetylcholine from surviving increase release of acetylcholine from surviving presynaptic nerve terminalspresynaptic nerve terminals
Combination action may diminish cholinesterase Combination action may diminish cholinesterase supersensitivity from developing, prolonging the supersensitivity from developing, prolonging the benefit.benefit.
May provide greatest delay of illness progressionMay provide greatest delay of illness progression May require increase of dose after patient declines May require increase of dose after patient declines
below initial baseline, to maintain benefit for longer below initial baseline, to maintain benefit for longer term.term.
Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170.

ReminylReminyl®® (galantamine (galantamine HBr) HBr)
GI TolerabilityGI Tolerability Nausea and vomiting: typically Nausea and vomiting: typically
transient and related to treatment transient and related to treatment initiation and dose escalationinitiation and dose escalation Among patients experiencing nausea, Among patients experiencing nausea,
median duration was 5 to 7 daysmedian duration was 5 to 7 days Weight loss: reported as an adverse Weight loss: reported as an adverse
event in event in 5% of patients, with none 5% of patients, with none discontinuing treatment due to weight discontinuing treatment due to weight lossloss
REMINYL Full Prescribing Information, 2001. Data on file, Janssen Pharmaceutica Products, L.P.

ReminylReminyl®® (galantamine (galantamine HBr) PharmacokineticsHBr) Pharmacokinetics Linear pharmacokineticsLinear pharmacokinetics Bioavailability: 90%Bioavailability: 90% Half-life: 7 hoursHalf-life: 7 hours
- can provide decrease inhibition at - can provide decrease inhibition at night!!night!!
Low (18%) plasma protein bindingLow (18%) plasma protein binding Hepatic metabolism via multiple Hepatic metabolism via multiple
pathways, primarily CYP2D6 and pathways, primarily CYP2D6 and CYP3A4CYP3A4
Renal excretionRenal excretion

ReminylReminyl® ® (galantamine (galantamine HBr): DosingHBr): Dosing
Simple, one-step dose escalationSimple, one-step dose escalation 8 mg/day starting dose8 mg/day starting dose
for 4 weeks (4 mg bid)for 4 weeks (4 mg bid) 16 mg/day maintenance dose16 mg/day maintenance dose
for at least 4 weeks (8 mg bid)for at least 4 weeks (8 mg bid) The flexibility to increase to 24 mg/dayThe flexibility to increase to 24 mg/day
(12 mg bid) – should try after 12 weeks if further benefit sought(12 mg bid) – should try after 12 weeks if further benefit sought Taken preferably with morning and evening mealsTaken preferably with morning and evening meals
Later, better with morning meal, mid-afternoon snack.Later, better with morning meal, mid-afternoon snack. (Avoid nocturnal cholinergic activation!!)(Avoid nocturnal cholinergic activation!!)
Available in 4-mg, 8-mg, and 12-mg tablets and Available in 4-mg, 8-mg, and 12-mg tablets and oral solution (4 mg/mL)oral solution (4 mg/mL)

Switching Guidelines Switching Guidelines (cont)(cont)
Switching from AriceptSwitching from Aricept®® to Reminyl to Reminyl® ®
(galantamine HBr)(galantamine HBr) No washout period of AriceptNo washout period of Aricept®® should be should be
undertaken before initiating REMINYL. The undertaken before initiating REMINYL. The standard dose escalation should be undertaken the standard dose escalation should be undertaken the next day after the last Ariceptnext day after the last Aricept®® administration administration
Switching from ExelonSwitching from Exelon®® to REMINYL to REMINYL No washout period of ExelonNo washout period of Exelon®® should be undertaken should be undertaken
before initiating REMINYL. The standard dose before initiating REMINYL. The standard dose escalation should be undertaken the next day after escalation should be undertaken the next day after the last Exelonthe last Exelon®® administration administration
Morris JC et al. Clin Ther. 2001;23(suppl A):A31-39.
Switching guidelines Switching guidelines (cont)(cont)
ExceptionsExceptions For patients who are experiencing poor For patients who are experiencing poor
tolerability on Aricepttolerability on Aricept®® or Exelon or Exelon®®, a washout , a washout period of up to 7 days should be undertaken, or period of up to 7 days should be undertaken, or until symptoms resolve until symptoms resolve
The standard dose escalation of ReminylThe standard dose escalation of Reminyl® ®
(galantamine HBr)(galantamine HBr) should then be undertaken should then be undertaken
Combined dosingCombined dosing Combination therapy with AChEIs is not Combination therapy with AChEIs is not
recommended by the manufacturing companyrecommended by the manufacturing company Galantamine may be combined with NamendaGalantamine may be combined with Namenda®®
(memantine)(memantine) Evidence suggests additional efficacyEvidence suggests additional efficacy Combination appears to be at least as effective as Combination appears to be at least as effective as
combination of donepezil and memantinecombination of donepezil and memantineMorris JC et al. Clin Ther. 2001;23(suppl A):A31-39.