alveolar condensation syndrome - isr · alveolar condensation syndrome dr etienne leroy-terquem...
TRANSCRIPT
Alveolar condensation syndrome
Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France
French-cambodian association for pneumology (OFCP)
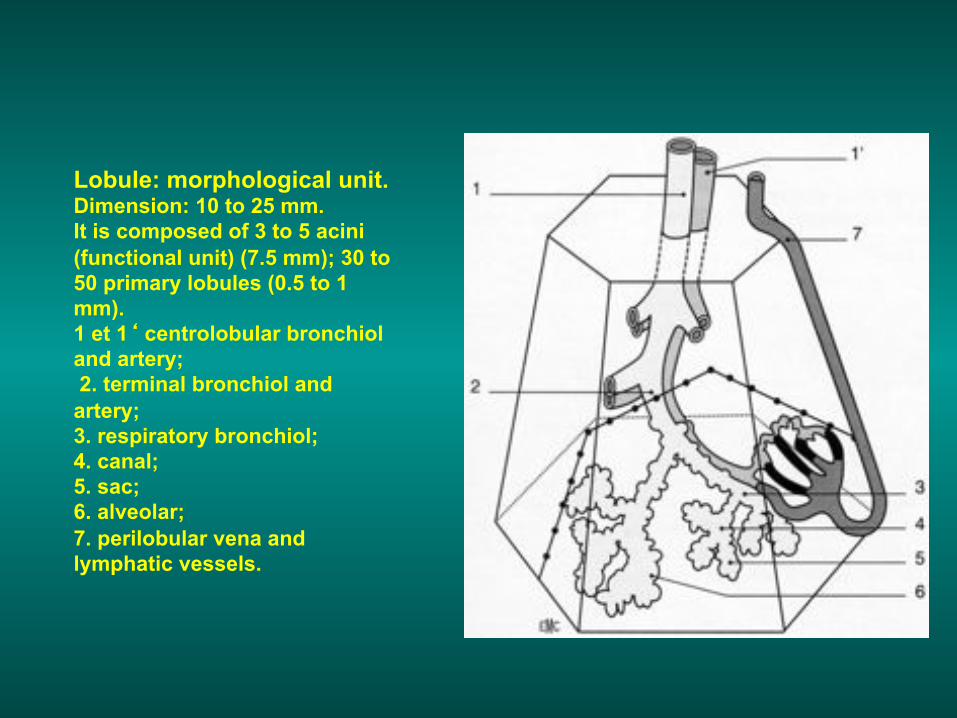
Lobule: morphological unit. Dimension: 10 to 25 mm. It is composed of 3 to 5 acini (functional unit) (7.5 mm); 30 to 50 primary lobules (0.5 to 1 mm). 1 et 1‘ centrolobular bronchiol and artery; 2. terminal bronchiol and artery; 3. respiratory bronchiol; 4. canal; 5. sac; 6. alveolar; 7. perilobular vena and lymphatic vessels.
Features of alveolar syndrome
• Non-homogeneous • Not well limited (except if there is
contact with the fissura, then the consolidation is «systematised»
• Aeric bronchogram present or not • No retraction in acute phase (but
retraction is possible if chronic evolution)
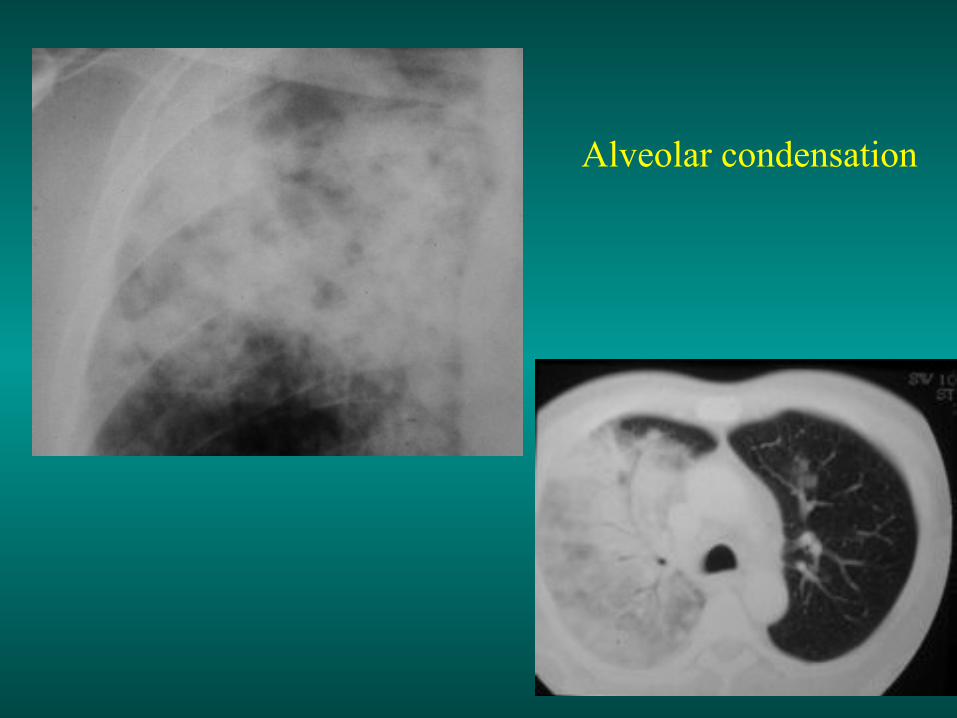
Alveolar condensation

Systematised opacity with aeric bronchogram
Acute Chronic
Infections (bacterial, viral) Tuberculosis Lung infarct and embolism Lung traumatism Post radiotherapy (acute phase ) Mycosis Loeffler syndrome Alveolar sarcoïdosis Localised alveolar oedema Chronic pneumonia Chronic pneumonia with eosinophilia Bronchiolo-alveolar cancer Lymphoma and haemopathy Pseudolymphoma
Main etiologies of localised alveolar syndrome
Main etiologies of diffused alveolar syndrome
Acute
Infections (bacterial, viral, opportunistic) Tuberculosis, mycosis Traumatism (contusion, fat embolism) Angeitis Pulmonary haemorrhage Pulmonary oedema Loeffler syndrome, eosinophilic lung Hypersensibility pneumonia (allergic alveolitis)
Chronic
Diffuse bronchiolo-alveolar damage Lymphoma and haemopathy Sarcoidosis Pulmonary alveolar proteinosis Lipidic pneumonia desquamative intersticial pneumonia
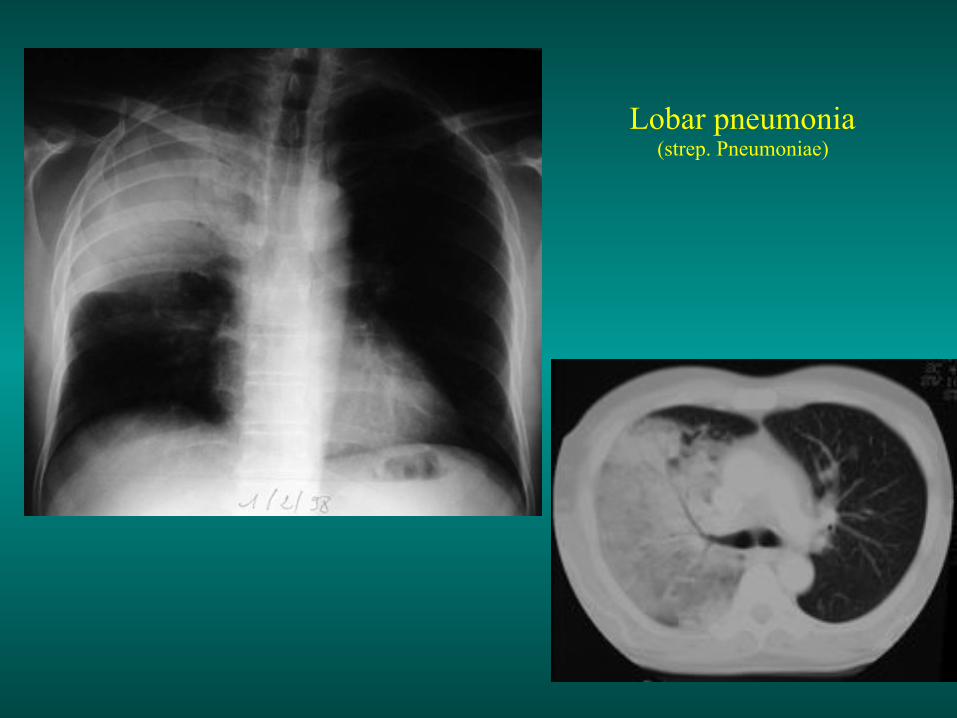
Lobar pneumonia (strep. Pneumoniae)

Lobar right inferior pneumonia (strep. Pneumoniae)

One of the frequent etiologies of infectious pneumonia is ear-nose-throat and dental infections

Bifocal infection: external segment of right sup. lobe and left inf. lobe
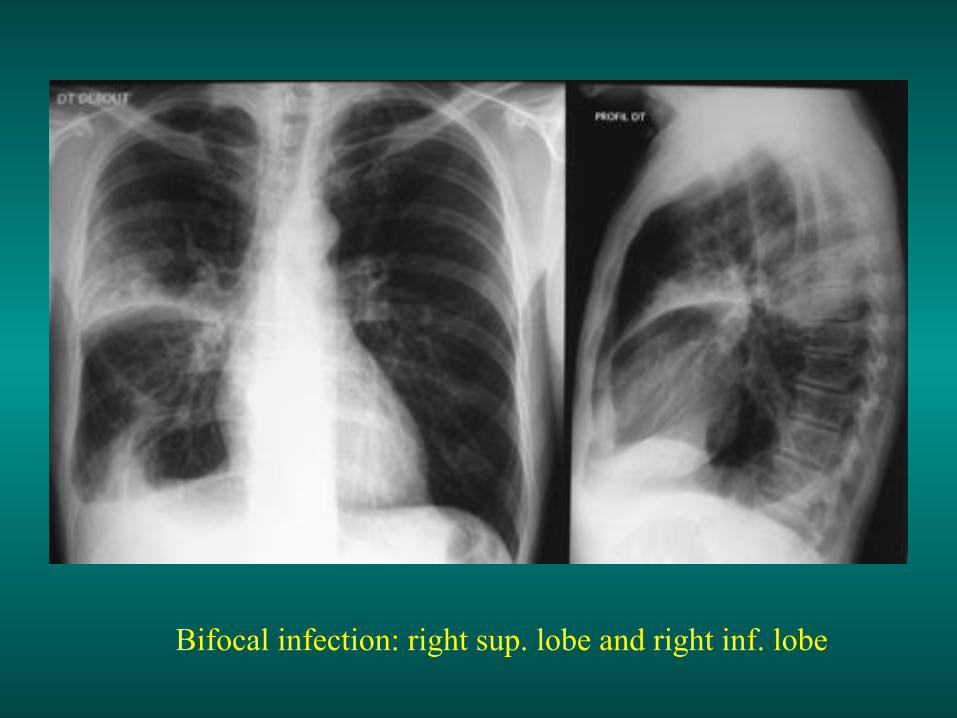
Bifocal infection: right sup. lobe and right inf. lobe
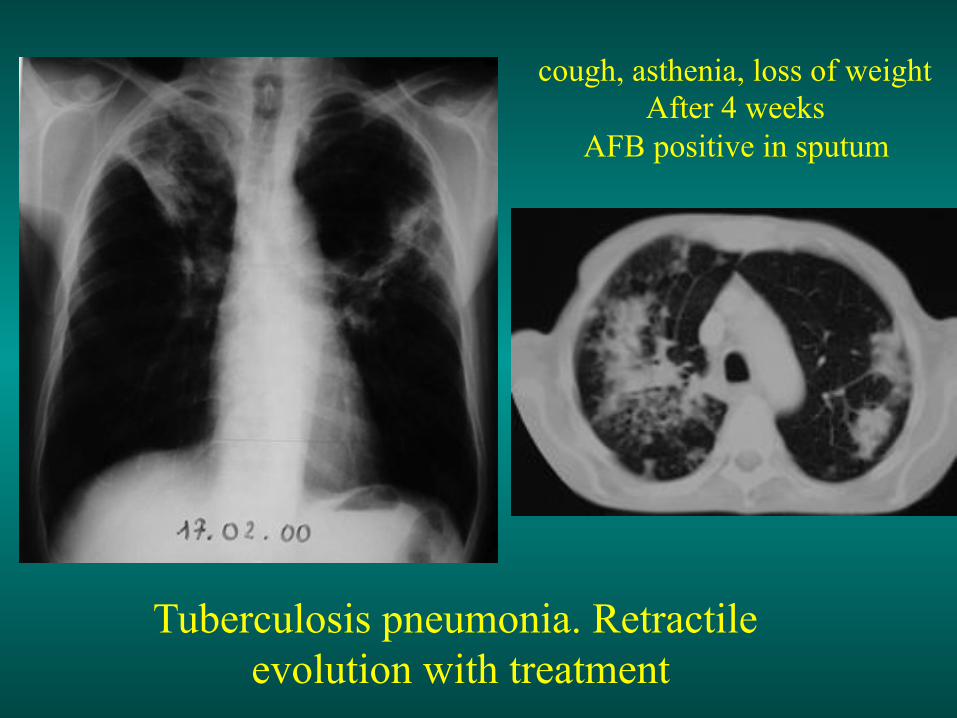
Tuberculosis pneumonia. Retractile evolution with treatment
cough, asthenia, loss of weight After 4 weeks
AFB positive in sputum
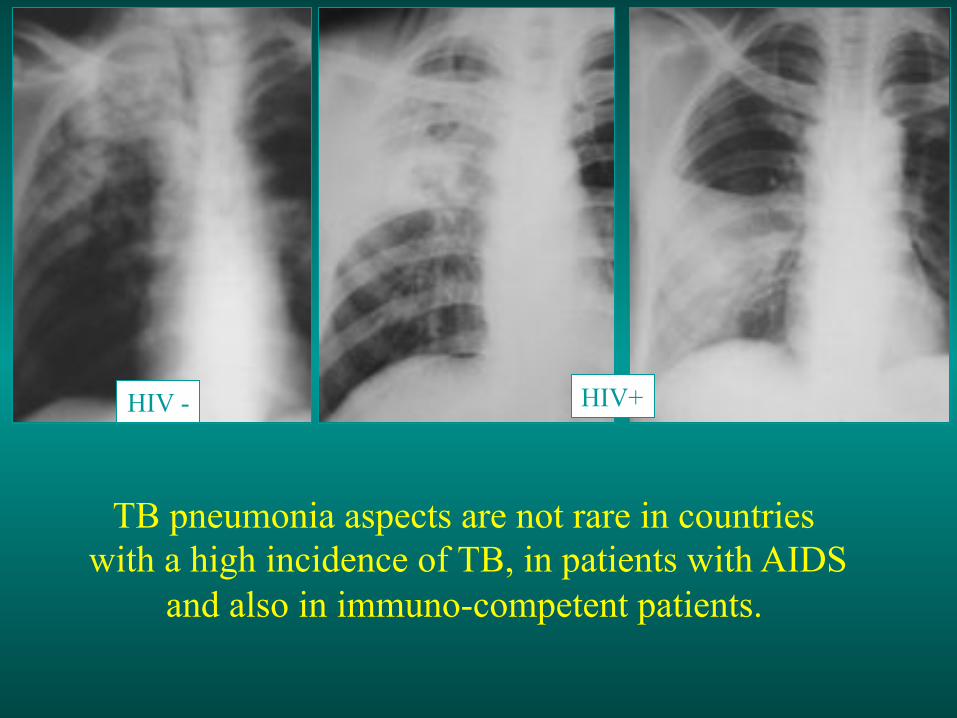
TB pneumonia aspects are not rare in countries with a high incidence of TB, in patients with AIDS
and also in immuno-competent patients.
HIV - HIV+
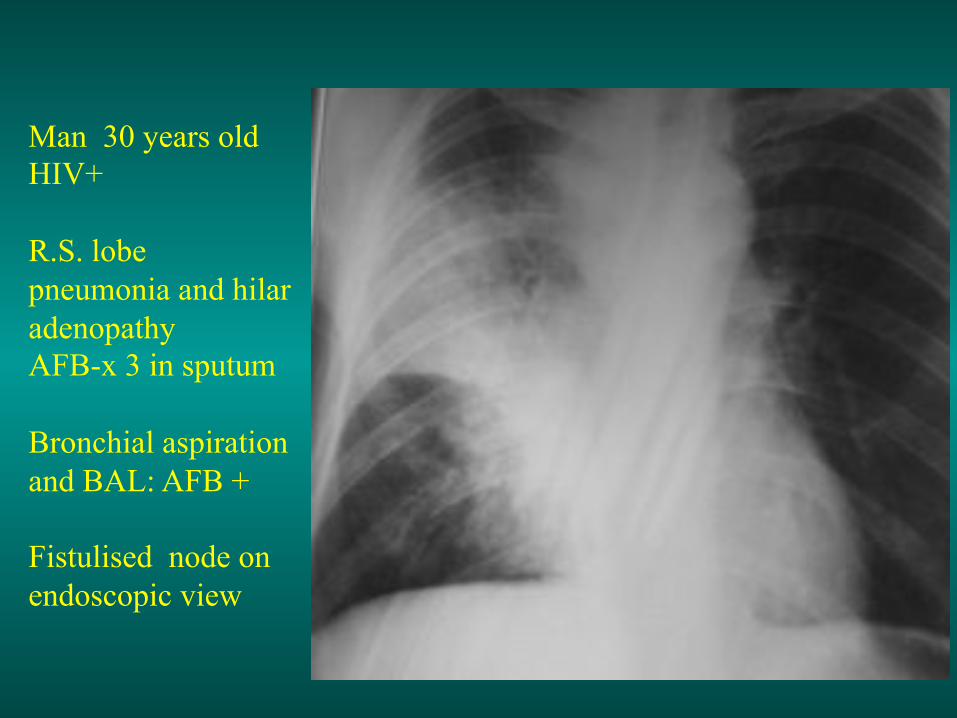
Man 30 years old HIV+ R.S. lobe pneumonia and hilar adenopathy AFB-x 3 in sputum Bronchial aspiration and BAL: AFB + Fistulised node on endoscopic view

25.04.01
Man 25 years old, weight, t° 39°C, cough, AFB + in sputum Left alveolar opacity. Treatment: 2RHZE
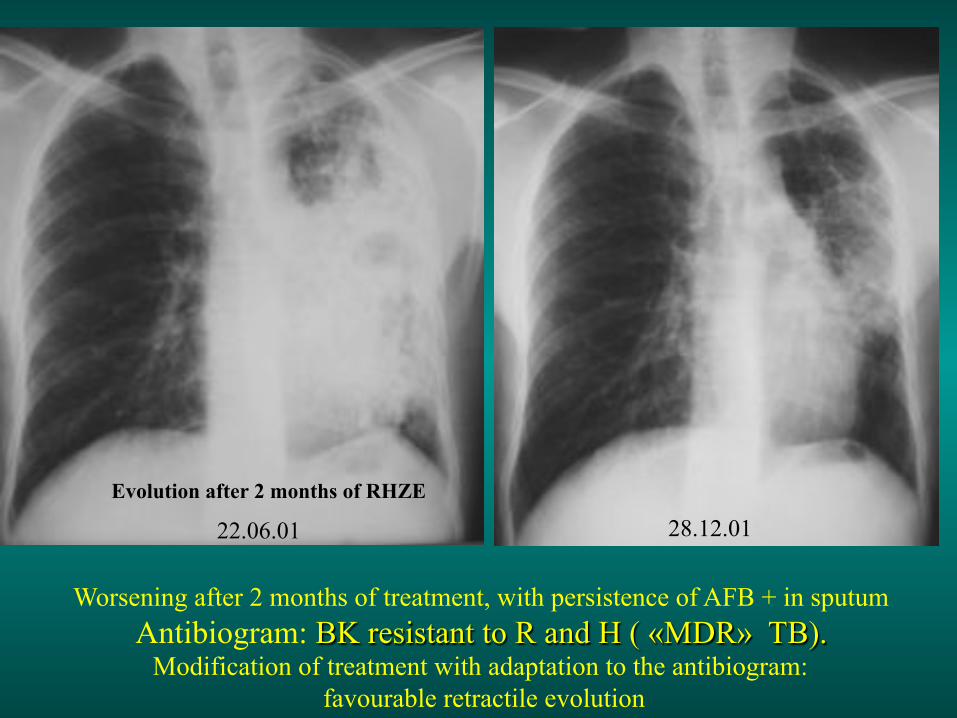
Worsening after 2 months of treatment, with persistence of AFB + in sputum Antibiogram: BK resistant to R and H ( «MDR» TB).
Modification of treatment with adaptation to the antibiogram: favourable retractile evolution
22.06.01 28.12.01 Evolution after 2 months of RHZE
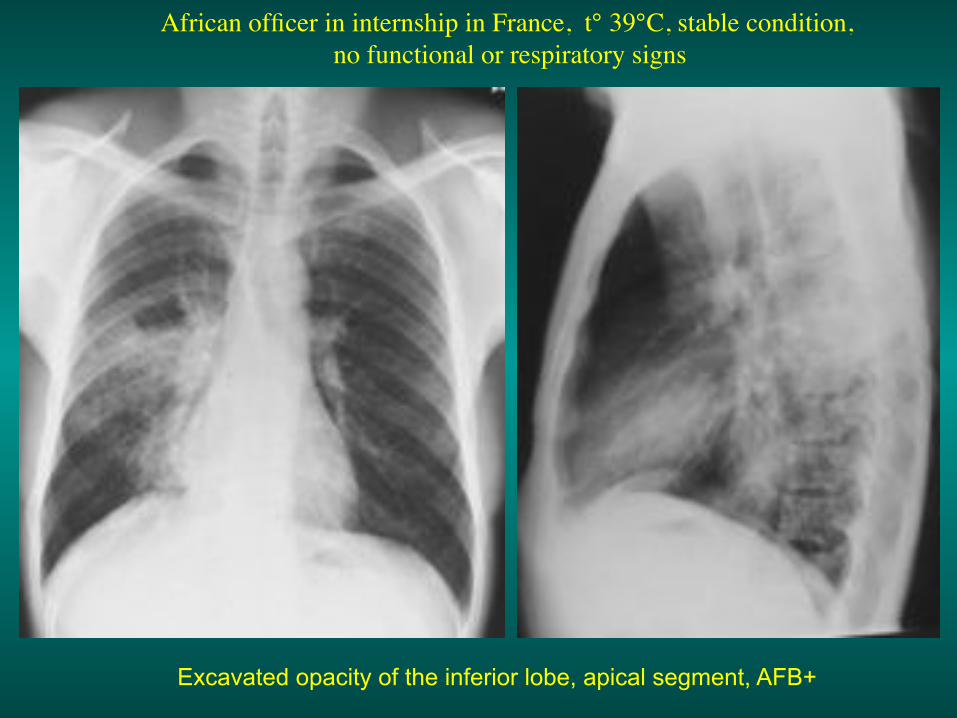
African officer in internship in France, t° 39°C, stable condition, ! no functional or respiratory signs!
Excavated opacity of the inferior lobe, apical segment, AFB+
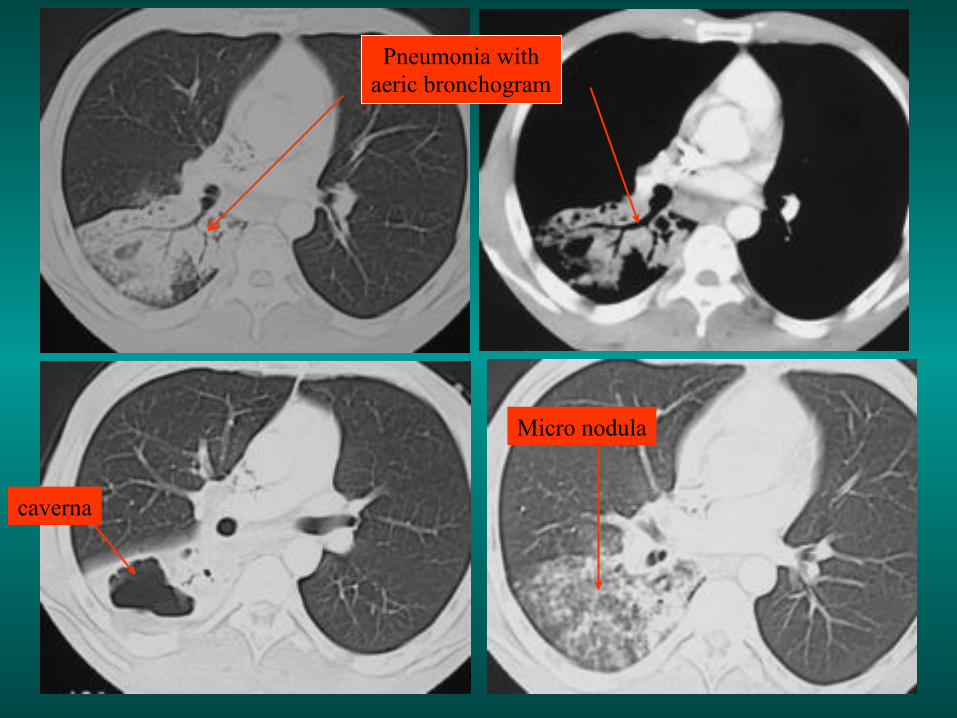
Pneumonia with aeric bronchogram
caverna
Micro nodula
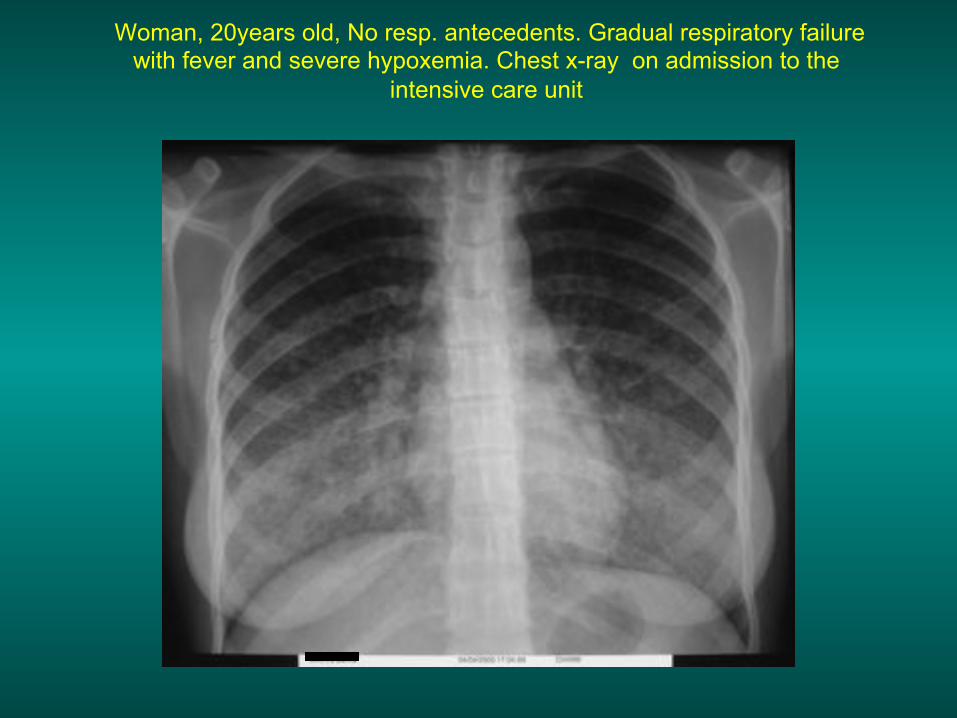
Woman, 20years old, No resp. antecedents. Gradual respiratory failure with fever and severe hypoxemia. Chest x-ray on admission to the
intensive care unit

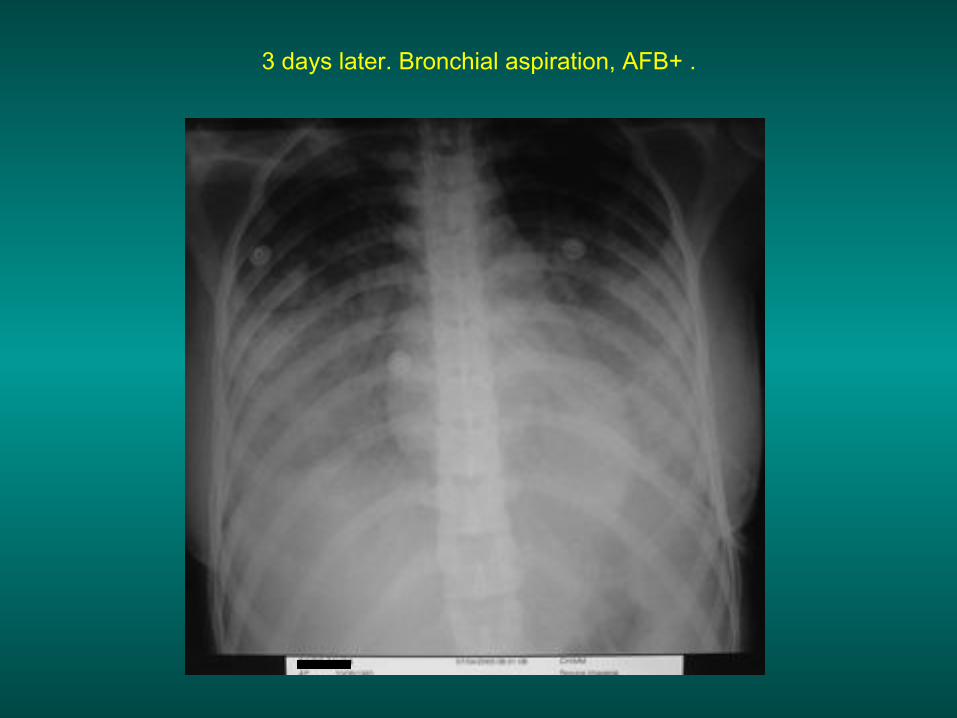
3 days later. Bronchial aspiration, AFB+ .
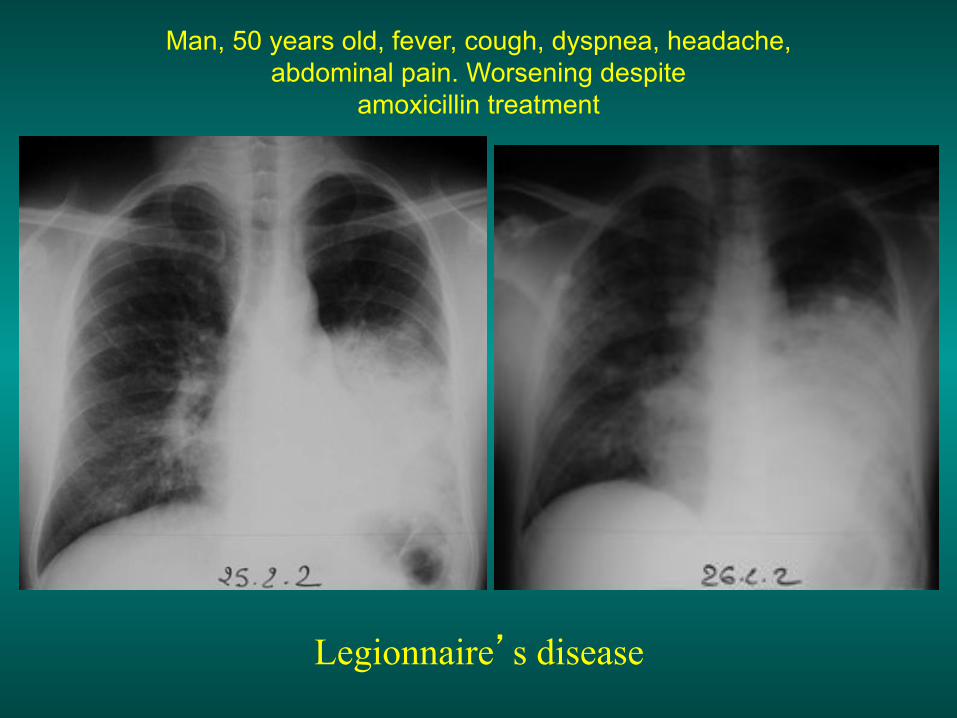
Legionnaire’s disease
Man, 50 years old, fever, cough, dyspnea, headache, abdominal pain. Worsening despite
amoxicillin treatment
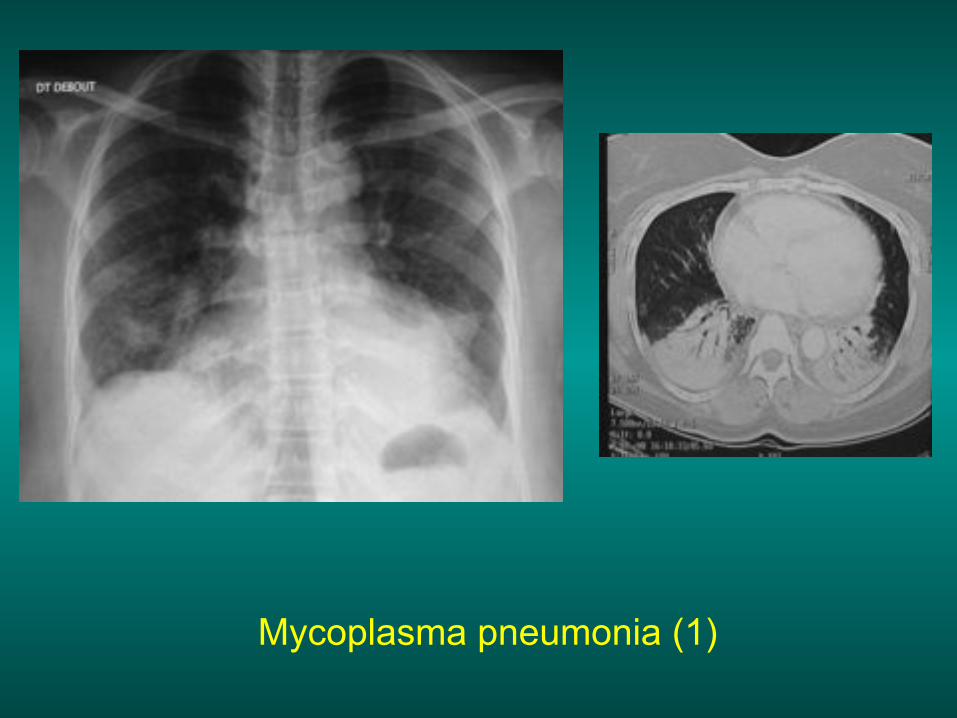
Mycoplasma pneumonia (1)
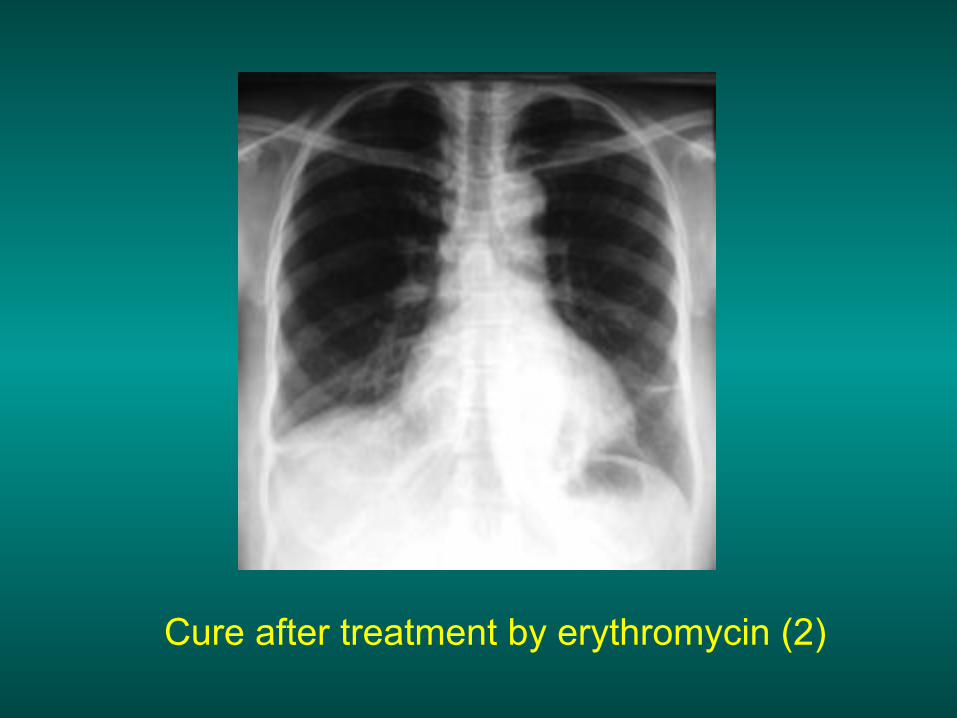
Cure after treatment by erythromycin (2)
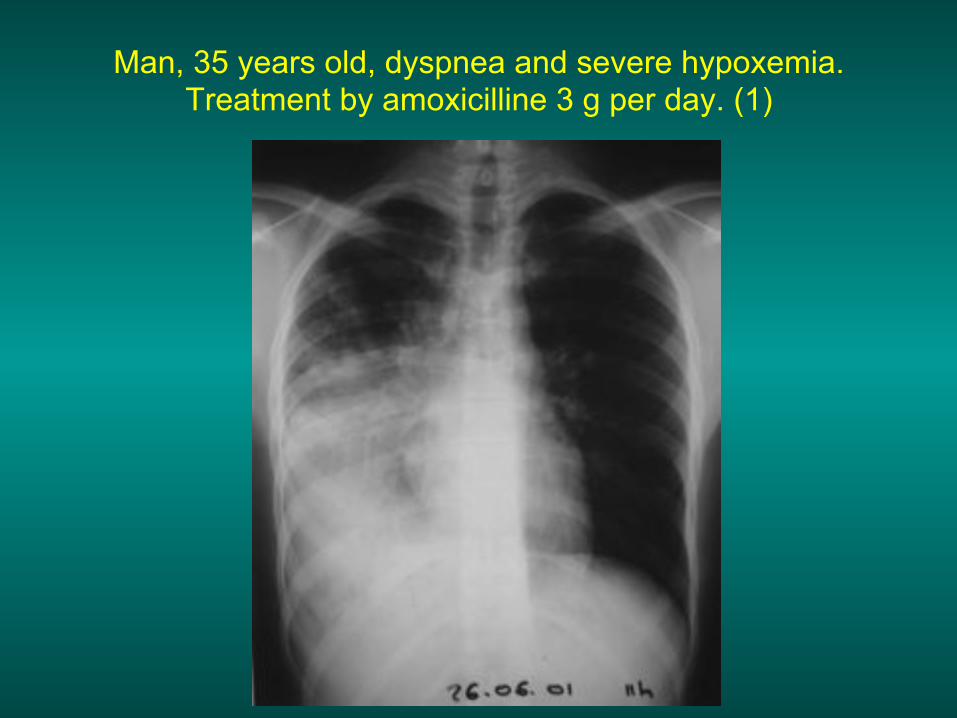
Man, 35 years old, dyspnea and severe hypoxemia. Treatment by amoxicilline 3 g per day. (1)
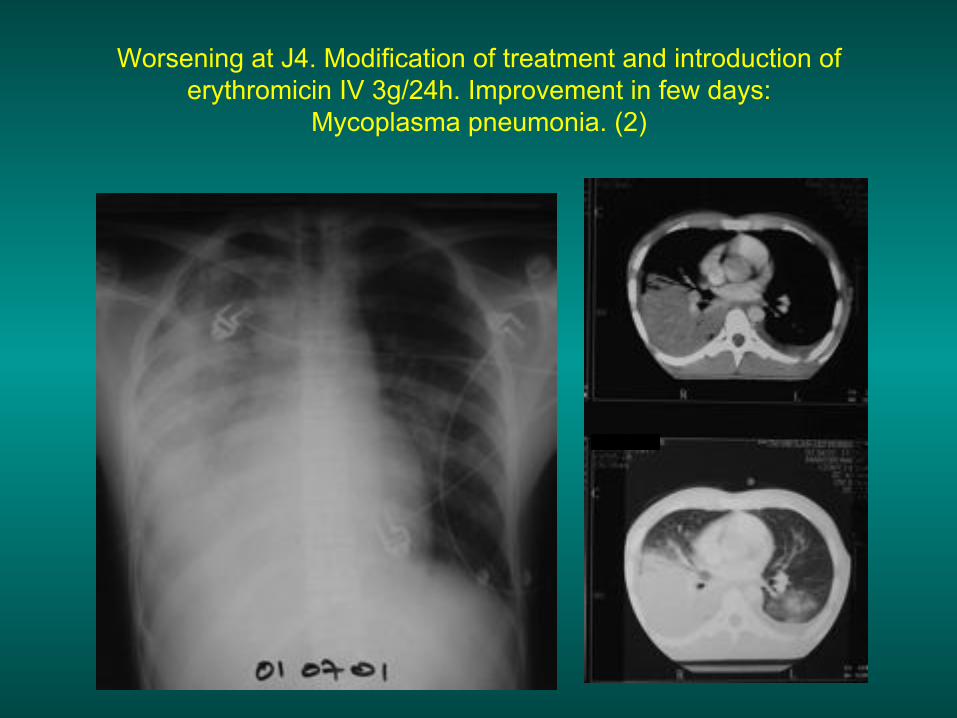
Worsening at J4. Modification of treatment and introduction of erythromicin IV 3g/24h. Improvement in few days:
Mycoplasma pneumonia. (2)

Bronchiolo-alveolar carcinoma


Pulmonary oedema
One can distinguish 2 physiopathological types: • The hemodynamic oedema, consequence of left
ventricular failure, with pulmonary arterial hypertension, of post-capillar type. Medical treatment is usually effective (O2, diuretic, TNT..). There is no anatomic lesion of the «alveolo capillar barrier»
• The lesionnal oedema: the etiologies are varied (viral or bacterial), toxic (for exemple inhalation of toxic gases), or complication from shock, regardless of the cause.
The prognosis is most often dismal. Death may occur by refractory hypoxemia. The alveolo-capillar barrier is more or less irreversibly altered.
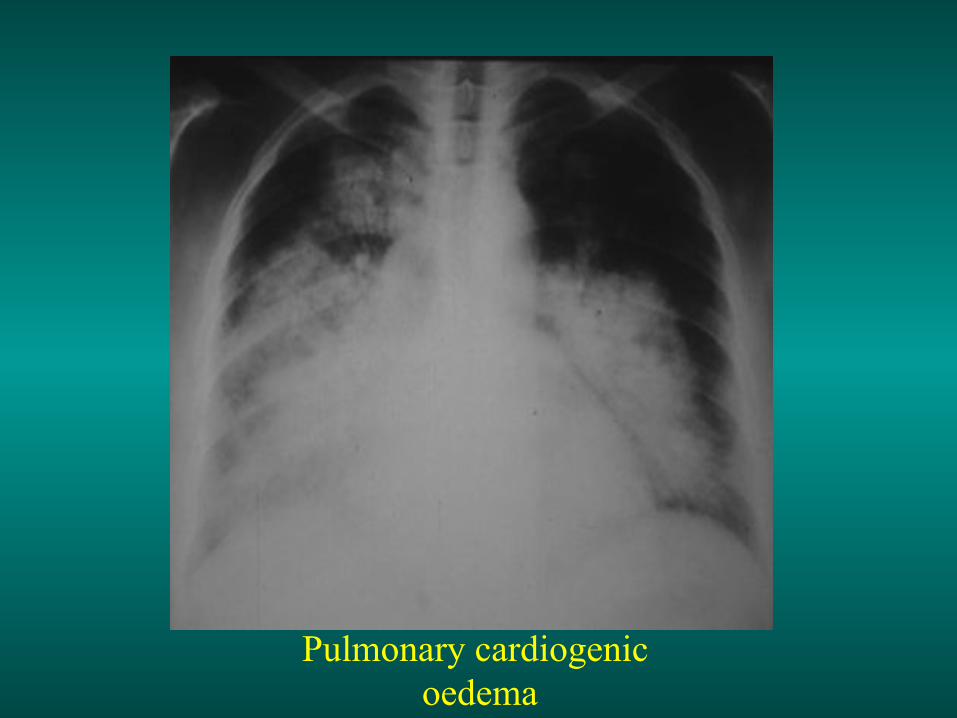
Pulmonary cardiogenic oedema
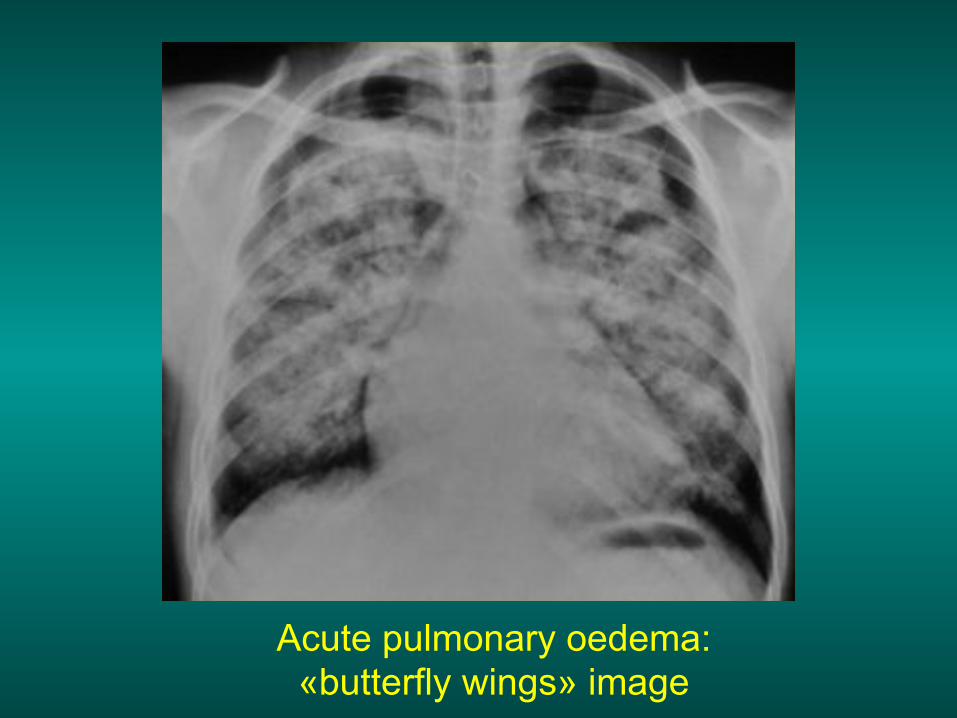
Acute pulmonary oedema: «butterfly wings» image

Acute pulmonary oedema
After furosemide

Acute pulmonary oedema. Notice the asymetry of the image.
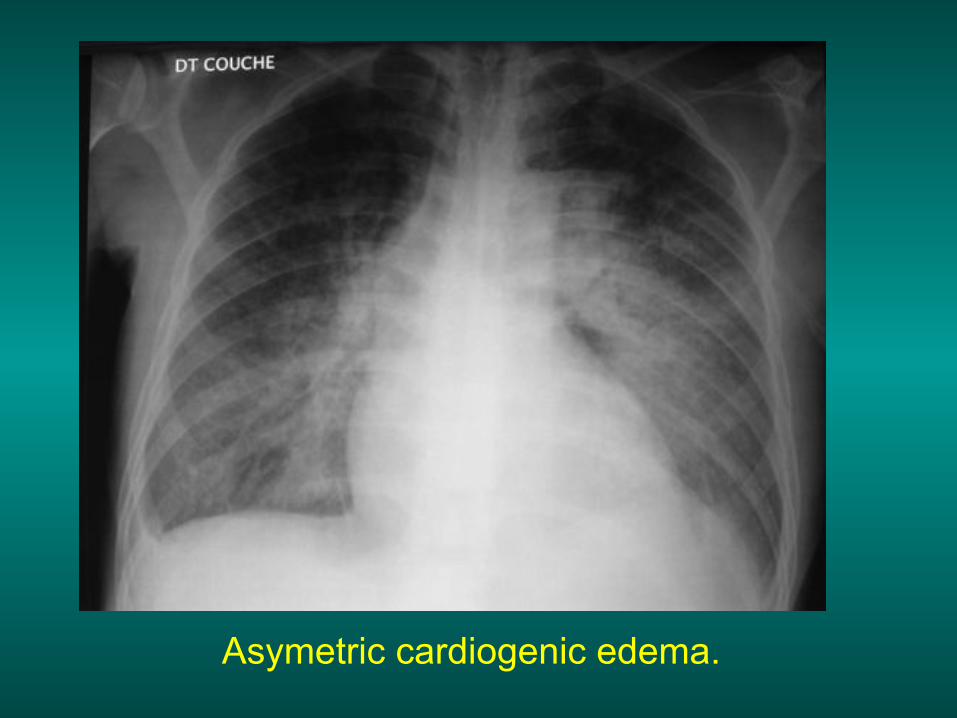
Asymetric cardiogenic edema.
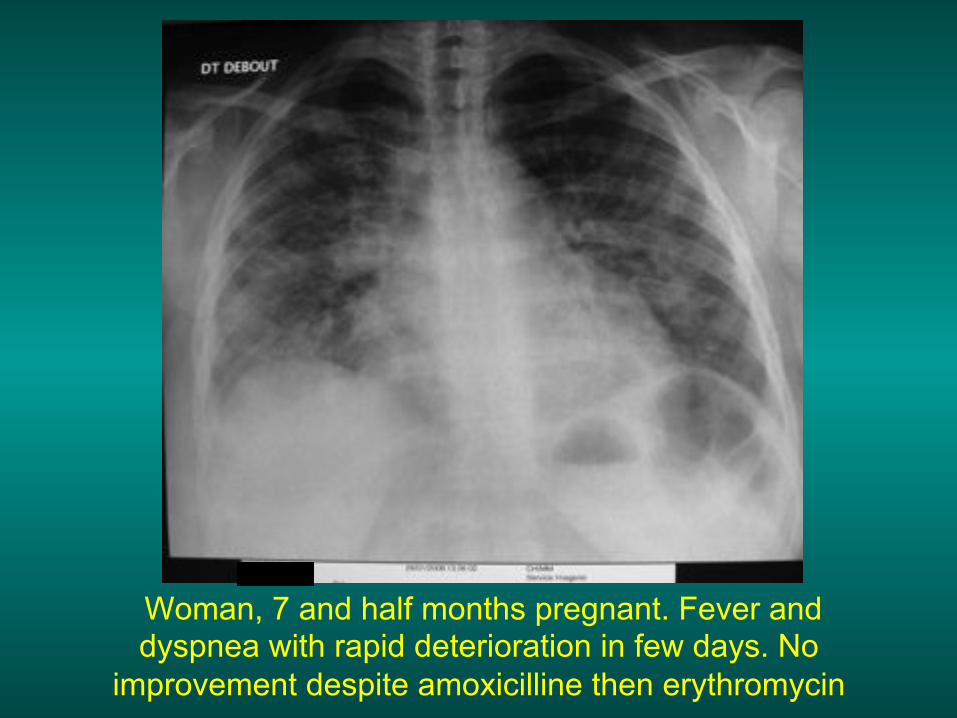
Woman, 7 and half months pregnant. Fever and dyspnea with rapid deterioration in few days. No
improvement despite amoxicilline then erythromycin

Worsening at J2 then J3: lesionnal oedema probably with a viral origin.