aluminium phosphide: toxicity mechanism and credible
TRANSCRIPT
www.wjpps.com Vol 4, Issue 10, 2015.
2276
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
ALUMINIUM PHOSPHIDE: TOXICITY MECHANISM AND
CREDIBLE TREATMENTS
Arshia Berry1, Garima Singh
2, Simran Jeet Kaur
3 and Kumud Bala
4*
1,2,3,4
*J 3 Block, 3rd Floor, Amity Institute of Biotechnology, Amity University, Sector-125,
Noida-201303, Uttar Pradesh, India.
ABSTRACT
Suicides and deaths by "accidental" ingestion or inhalation of
Aluminium Phosphide poisoning are rising at an alarming rate year
after year. Ascribing to the lack of an effective and safe antidote and
with almost a 100% mortality rate, it becomes next to impossible to
save the victim of this particular poisoning. In order to do the same, it
is imperative to fully comprehend the mechanism and action of AlP on
various organs, once it enters the body. Thus, this review explains the
mode of action of phosphine gas produced by AlP inside the human
body, with a special emphasis on the nucleophilic nature of phosphine
and its role in inducing cytochrome c - mediated oxidative stress,
giving way to metabolic acidosis and multiple organ failure. The
predicted treatments will include moieties capable of inhibiting the
cytochrome c pathway and neutralizing the serum acid content along with already established
agents combating various aspects of AlP poisoning.
KEYWORDS: Aluminium Phosphide, Phosphine, poisioning, fumigant.
INTRODUCTION
A highly toxic fumigant with the chemical formula of AlP, aluminium phosphide continues to
kill millions around the globe, with an astonishing mortality rate of 40%-100%
(Moghadamnia, 2002). The lack of a proper antidote is regarded as the underlying reason that
accentuates the mortality rate associated with acute aluminium phosphide poisoning. The
lethal dose (LD50) is 11.5 mg/kg and the estimated time intervals beginning from the
ingestion of its tablet to death has approximately been reported as 3 hours, or on an average,
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 5.210
Volume 4, Issue 10, 2276-2293 Review Article ISSN 2278 – 4357
Article Received on
24 Aug 2015,
Revised on 16 Sep 2015,
Accepted on 04 Oct 2015
*Correspondence for
Author
Kumud Bala
J 3 Block, 3rd Floor,
Amity Institute of
Biotechnology, Amity
University, Sector-125,
Noida-201303, Uttar
Pradesh, India.

www.wjpps.com Vol 4, Issue 10, 2015.
2277
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
between 1-48 hours, with the most common cause of death being cardiac arrhythmias. 95% of
the patients die within 24 hours of ingestion of AlP (Chugh et al, 1993). Also, in a 25-year-
long study reported by Singh et al (2003), a total of 5933 unnatural deaths by poisoning
reported in north-west India, aluminium phosphide was found out to be a major cause.
The pesticidal activity of AlP is attributed to its property of releasing phosphine gas, also
known as hydrogen phosphide (PH3), first discovered by a German company named Degesch.
Later, the Hollywood Termite Control Company, Inc in the United States of America
registered it as a pesticide in 1958. The gas, if inhaled or if produced inside the human body
after ingestion of AlP, affects a number of organs, like: kidneys, lungs, liver, gastrointestinal
tract as well as the central nervous system (Chemistry learner).
Physically, it has a solid, colourless appearance and is sold in the market as yellow or grey
crystals (3gm tablet) or as a grey-green powder (Kirk-Othmer Encyclopedia of Chemical
Technology, 1982). The colour imparted is a result of residing impurities form hydrolysis or
oxidation process. The smell usually resembles that of garlic or rotten fish (Ellenhorn et
al, Medical Toxicology - Diagnosis and Treatment of Human Poisoning, 1988).The crystals
or tablets, which are more commonly available in the markets have a zincblende crystal
structure (Van Zeghbroeck, 1997) and are stable thermodynamically up to a 1000˚C or 1830˚
F with the substance density of 2.85 gm/cm3.
The molar mass and the melting point of
aluminium phsophide is 57.9552 g/mol and 2530˚ C or 4590˚ F respectively. Aluminium
phosphide is readily soluble in water and reacts both, with water as well as moisture present
in the air, to yield the highly toxic phosphine gas. The reaction takes place as follows, where
the water molecule breaks down to produce H+
and OH- ion (Holleman, 2001): AlP + 3 H2O
→ Al(OH)3 + PH3; AlP + 3 H+ → Al
3+ + PH3
Similarly, for the production of aluminium phoshide in laboratories, the mixture of red
phosphorous (P) and powdered aluminium (Al) is made to react with each other and
subjected to ignition in order to yield AlP (White et al, 1953). The reaction takes place as
follows: 4Al + P4 → 4AlP
AlP has a wide number of applications in agricultural industry, namely, as a fumigant,
rodenticide, pesticide, insecticide as well as semiconductor material, as in aluminium gallium
indium phosphide, when alloyed with different binary materials in order to be used in light-
emitting diodes (Corbridge et al, 1995). As a fumigant, it is used to preserve a wide variety of
www.wjpps.com Vol 4, Issue 10, 2015.
2278
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
food products before they are sold in the market for human consumption. The products
include various grains, like wheat, and many dry fruits and cereals (Chemistry learner).
Commonly known as the ―wheat pill‖, it is used to kill several varieties of verminous
mammals, such as, rodents or moles. The phosphine gas, responsible for the killings is highly
toxic and flammable, hence, in order to control its spontaneous and sudden ignition leading to
explosion and development of toxic gas, aluminium phosphide preparations are commonly
mixed with stabilizers such as ammonium carbamate (White et al, 1944). Commercially, it is
supplied by the following companies worldwide: Pestcon (United States), Shanghai Kima
Chemical Co. Ltd. (China), Sandhya Organic Chemicals P. Ltd. (India), Chemcolour (New
Zealand), Excel Industries (Australia), Taiwan Chemicals (Taiwan) ,Globe Chemicals GmbH
(Germany), Agrosynth (India), Penglai Chemical Inc. (China), Central & Western Chemicals
(India).
The compound, AlP, is also available under the following most common brand names, like,
Quick Phos, Phostoxin, Celphos, Talunex and Fumitoxin (White et al, 1944).
EPIDEMIOLOGY
An extremely toxic pesticide and a notably cheap fumigant since 1940, aluminium phosphide
(Moghadamnia, 2012) causes approximately 68% of the total poisoning causalities reported
in the Indian sub-continent. Most of the cases reported in India are, however, associated with
the ingestion of phosphides, mainly among the agricultural workers (Mostafazadeh, 2012).
This, in turn results from the improper storage facility for these fumigants. In India, AlP
poisoning is most prevalent in the age group of 11-30 years, in rural areas (Moghadamnia,
2012). From 1979 to 2004, approximately, 895 patients have been admitted in PGIMER,
Chandigarh, with acute AlP poisoning (Singh, unpublished data). Similarly, a year-round
study conducted in Allahabad managed to record 301 suspicious cases of poisoning, out of
which 11.7% were reported due to AlP. The affected male to female ratio in this study was
2:1 (Moghadamnia, 2012).
Other than in India, a few cases annually are reported from Iran and Jordan, mainly in an
attempt to commit suicide from aluminium phosphide, commonly called as the ―rice tablet‖
there. In Iran, a four-year study was conducted from 1997-2001, which was successful in
recording about 1571 poisoning cases, of which, approximately, 2.1% or 33 cases had their
underlying cause as aluminium phosphide (Moghadamnia, 2012).

www.wjpps.com Vol 4, Issue 10, 2015.
2279
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fatal dose in all the cases has been reported for a healthy adult of 70 kg as 150-500 mg
(Chugh, 1988). Except for in India, Iran and Jordan, a few cases annually are reported from
United Kingdom (Bogle, 2006), Australia (Nocera, 2000), Germany (Alter, 2001), Canada
and the United States (Ragone, 2002), to name a few.
MECHANISM OF TOXICITY
The exact mechanism by which aluminum phosphide causes poisoning is still not known.
Systemic complications and multi-organ failure are involved in acute aluminum phosphide
poisoning (Abedini et al, 2014). Phosphine gas is generally released when aluminum
phosphide is ingested (Moghadamnia, 2012). Phosphine molecule has three hydrogen atoms
and a phosphorus atom i.e. PH3. Phosphorus in turn, has 5 valence electrons, with 2 paired
electrons in s-orbital and 3 unpaired electrons in its p-orbital. Three molecular bonds can
easily be formed by these three unpaired electrons in the p-orbital (Kutzelnigg, 1984). Also,
s-orbital electrons can participate in bond formation with oxygen. This happens in case of
sufficient oxygen, where oxiderivatives of phosphine like H3PO are formed with imbalances
between blood phosphorous and oxygen.
Phosphine is cytotoxic and is mainly involved in free radical mediated injury. It is a
nucleophile and a strong reducing agent and hence is capable enough of holding back many
cellular enzymes in various metabolic processes (Mathai and Bhanu, 2010). PH3 is fully
reduced form of phosphorus in contrast to phosphate which is fully oxidized form and is
thermodynamically favoured in biological tissues (Price and Sadler, 1988). It oxidizes slowly
in weak acids and forms unstable H3PO only if sufficient oxygen is available. This H3PO is
an intermediate and extremely unstable product and had not been observed either in vivo or
experimental procedures (Robinson and Bond, 1970). In H3PO, O2 carries a partial negative
charge and phosphorus carries a partial positive charge. Phosphorus acts as an electrophile
due to polarity of the molecule which also contributes to the reactivity of the whole structure
(Nath et al, 2011). But mechanism by which this transient H3PO causes phosphine toxicity is
yet to be fully discovered.
There are evidences that phosphine inhibits respiration in rat liver mitochondria (Nakakita et
al, 1971) and insect mitochondria (Chefurka et al, 1976). This inhibition is significant when
there is addition of precursors to ATP synthesis or any chemical uncoupler. It is also
suggested that inner membrane of mitochondria, being highly impermeable, is a major hurdle
in PH3 uptake. But usually, it is overcome by activation of transport across mitochondrial

www.wjpps.com Vol 4, Issue 10, 2015.
2280
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
inner membrane (Nath et al, 2011). It is gradually absorbed by gastro-intestinal tract
following a simple diffusion method wherein phosphine released inhibits cytochrome c
oxidase in the mitochondria, which in turn inhibits cellular utilization. In an experimental
procedure it was revealed that Complex IV, also known as cytochrome c oxidase, is a
primary site for electron transport chain (ETC) and PH3 interaction (Chefurka et al, 1976).
Kashi and Chefurka later suggested that oxidation state of cytochrome a was highly reduced
on treatment with phosphine. Also, PH3 can form complex with metal ion cofactors at active
site of enzymes which is basis of cytochrome c oxidase inhibition (Chaudhry and Price,
1990). Due to this, around 70% of oxidative respiration which occurs in mitochondria is
inhibited. Various harmful cellular radicals like superoxides and peroxides are generated as a
result of lipid peroxidation which is a result of reduction in oxidative respiration
(Moghadamnia, 2012). Furthermore, it promotes protein denaturation that results in
breakdown of integrity of cell (Mehrpour et al, 2012). Cellular oxidative stress, hence, is a
result of this suppression of oxidative respiration and ETC-PH3 interaction (Nath et al, 2011).
Fig. 1: pictorial representation shows the interaction of PH3 with various enzymes
involved in metabolic processes in mitochondria and synapse.

www.wjpps.com Vol 4, Issue 10, 2015.
2281
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
Phosphine is shown in light blue, NO in orange, and ROS in red. The cross symbol behind
enzymes indicate that they are inhibited. ROS generated at various sites in mitochondria leads
to inhibition of various metabolic processes. The potassium and calcium currents are
regulated by acetylcholine via NO. Ca2+
triggers the release of acetylcholine in cytoplasm into
the neuronal synapse. The acetylcholinesterase degrades acetylcholine, reducing the strength
of neurotransmission. [FAD/FADH2 (Flavin adenine dinucleotide oxidized/ reduced),
NAD+/NADH (Nicotinamide adenine dinucleotide oxidized/ reduced), ADP/ ATP (adenosine
di/ tri nucleotide), NO (nitric oxide), ROS (reactive oxygen species) and TCA (tricarboxylic
acid)].
A study conducted in 1996 by Chugh et al, stated that levels of serum superoxide dismutase
(SOD) and malonyldialdehyde (MDA) were high and serum catalase levels were low which
resulted in peroxide load in patients within first day of the poisoning. It confirmed the
phosphine release. It was observed that indicators of oxidative stress reached their peak levels
within 48 hours of exposure. Autopsy results in non survivors confirmed high levels of SOD
and MDA indicating their direct relation with mortality and low catalase levels indicating the
inverse relationship. However, patients who survived till fifth day of poisoning showed
normal levels of SOD, MDA and catalase which suggested that phosphine was eliminated
and there was a significant drop in levels of oxidative stress indicators.
Phosphine is mainly metabolized and excreted by kidneys, although, it has been studied that
some amount of aluminum phosphide is slowly absorbed and later metabolized by liver. This
results in release of phosphine at a very slow rate which is responsible for delayed onset of
toxicity of aluminum phosphide (Wahab et al, 2008). In the same study it was revealed that,
focal myocardial necrosis is also one of the signs observed in aluminum phosphide poisoning.
This is due to alteration in the ionic permeability of ions such as sodium, magnesium and
calcium. This is evident in a patient as cardiac arrhythmias and ECG anomalies. Also, adrenal
gland damage, fluid loss (Mathai and Bhanu, 2010), hypoxemia with severe metabolic
acidosis are some of the other abnormalities which are observed in aluminum phosphide
poisoning (Anger et al, 2000).
Certain evidences of agitation followed by convulsions in humans and twitching after
hyperactivity in non-human animals have been reported post ingestion of aluminium
phosphide. Lethargy is also observed in a few individuals (Potter et al, 1993). Phosphine also
contributes in increasing acetylcholine neurotransmission by suppressing acetylcholine

www.wjpps.com Vol 4, Issue 10, 2015.
2282
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
esterase (Mittra et al, 2001). This activation in acetylcholine signaling increases metabolic
demand which can also cause hypersensitivity towards phosophine (Valmas et al, 2008).
Patients usually die within 24 hours due to cardiac toxicity. But if a person survives more
than a day, acute respiratory distress syndrome (ARDS) is a major manifestation. There are
also evidences of diffuse alveolar damage (DAD) which appear as alveolar edema and
hemorrhages at times of autopsy, thereby confirming ARDS (Hugar et al, 2015). Also, it has
been reported that ulcerations, gastro-intestinal disorders, liver failure and metabolic
disorders were observed within 24 hours of poisoning.
Ischemic stroke can be considered as one of the delayed responses of aluminum phosphide
poisoning as studied in case report of a 30 year old right-handed man in Iran (Abedini et al,
2014). It was revealed that the stroke was a result of sudden onset of left side hemiplegia
(total or partial paralysis of one side of the body that results from disease of or injury to the
motor centers of the brain) which occurred 11 days after the ingestion of aluminum
phosphide. MRI (Magnetic Resonance Imaging) and MRA (Magnetic Resonance
Angiogram) confirmed ischemic lesions and stenosis in the middle cerebral artery of brain
respectively.
www.wjpps.com Vol 4, Issue 10, 2015.
2283
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
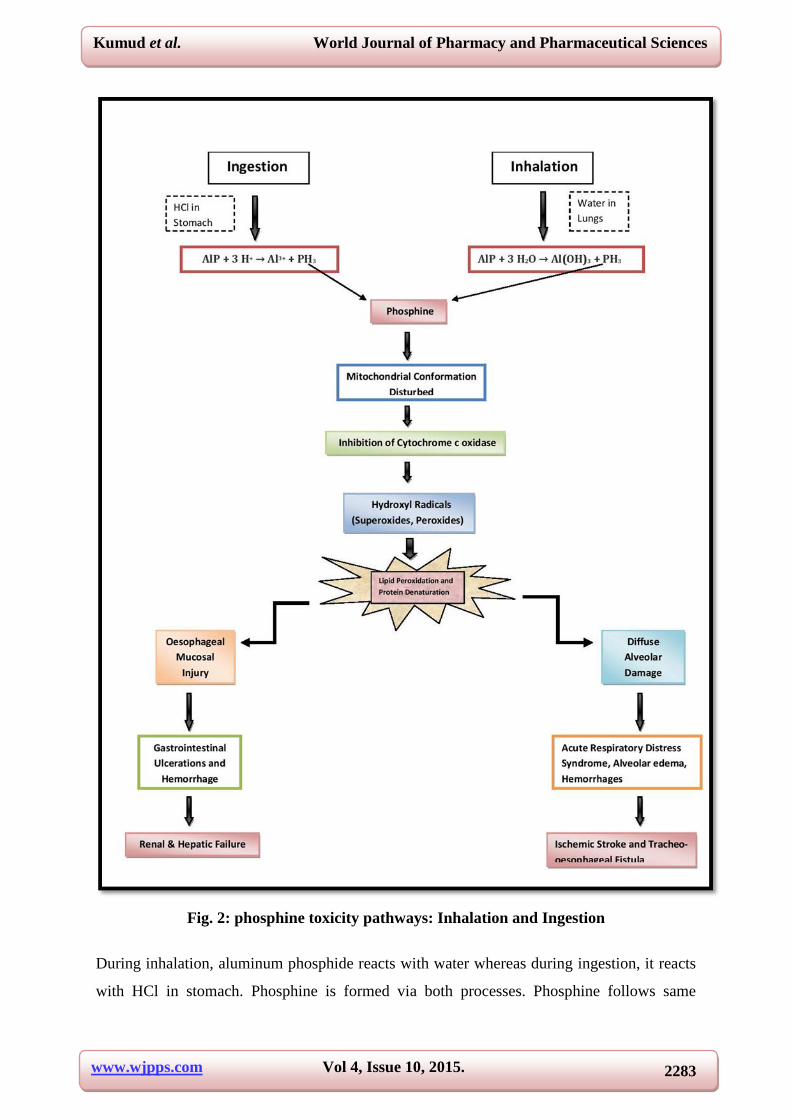
Fig. 2: phosphine toxicity pathways: Inhalation and Ingestion
During inhalation, aluminum phosphide reacts with water whereas during ingestion, it reacts
with HCl in stomach. Phosphine is formed via both processes. Phosphine follows same
www.wjpps.com Vol 4, Issue 10, 2015.
2284
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
pathway in both the cases and leads to mitochondrial damage by inhibiting Cytocohrome c
oxidase. Hydroxyl radicals, thus, produced cause lipid peroxidation and protein denaturation.
This mitochondrial damage in gastro-intestinal tract cause ulcers and hemorrhages and
eventually renal and hepatic failure whereas it causes diffused alveolar damage in lungs
leading to alveolar edema, hemorrhages and in many cases Ischemic stroke.
SYMPTOMS AND DIAGNOSIS
Signs and Symptoms
The general signs and symptoms of aluminium phosphide poisoning (AlPP) are: metabolic
acidosis, which may occur due to the accumulation of lactic acid caused by blockage of
oxidative phosphorylation and poor tissue perfusion (Agarwal et al, 2014), gastrointestinal
hemorrhage and ulcerations (Hugar et al, 2015), abdominal pain, vomiting, abnormality in
Glasgow coma scale, systolic blood pressure, and central venous pressure (Louriz et al,
2009). Major complications observed in the course of severe aluminium poisoning are
cardiac dysrhythmias, shock, respiratory distress, hypomagnesemia and lack of vomiting
(leading to retention of AlP in body).
Some studies have reported that aluminium poisoning causes neurological toxicity which, in
turn, can cause clinical effects like headache, stupor (a state of near-unconsciousness),
restlessness, agitation, anxiety, ataxia (loss of full control on body), paresthesia (an abnormal
sensation, typically tingling or pricking) and central nervous system depression leading to
coma and seizures ( Goel and Aggarwal, 2007).
Diagnosis
The diagnosis of AlPP ingestion can be confirmed by detecting phosphine in exhaled air or in
GI aspirate. In stomach, phosphine gas can be detected by the silver nitrate test. To perform
this test, gastric contents are diluted with of water in a flask and the flask is heated at 50oC for
15-20 minutes. Then, two round pieces of filter paper, one impregnated with 0.1 N silver
nitrate and other with 0.1 N lead acetate are placed alternately on the mouth of the flask, if
phosphine gas is present in the gastric contents, then due to conversion silver nitrate to
metallic silver, the silver nitrate paper turns black while the lead acetate paper does not
change color. If hydrogen sulphide is present, both the papers turn black. The reaction takes
place as follows: 8AgNO3 +PH3 +4H2O → 8Ag +H3PO4 + 8HNO3

www.wjpps.com Vol 4, Issue 10, 2015.
2285
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
A variant of silver nitrate test to detect phosphine gas is the breath test. The patient is asked
to breathe through a filter paper impregnated with 0.1N silver nitrate for 15 minutes. Due to
the presence of phosphine in the breath, the filter paper turns black. The test on gastric
aspirate is much more sensitive than the breath test (Louriz et al, 2009).
The breath test is not reliable. A false negative result may occur in patients being given
oxygen as phosphine may get converted to phosphorus pentoxide. A false positive result may
also occur due to the presence of hydrogen sulfide in the air (Mehrpour et al, 2012). Gas
chromatography is the most specific and sensitive method for detecting the presence of
phosphine in blood/ air and can detect even minute amounts of phosphine in the air (Anand et
al, 2011).
LABORATORY ASSESSMENT AND PROGNOSIS
Laboratory assessment is generally done to obtain the prognosis. In case of AlP toxicity
general prognostic factors are : elevated serum creatinine, low APACHE II (Acute
Physiology and Chronic Health Evaluation II) score, low pH value (< 7.2), low serum bio
carbonate value (<15mmol/L). Louriz et al have also reported that, the prognostic factors
associated with mortality from acute AlP poisoning, includes a low APACHE II score, low
Glasgow coma scale score, shock, electrocardiogram abnormalities, the presence of acute
renal failure, low prothrombin rate, hyperleukocytosis (an unusual large increase in number
and proportion of white blood cells in blood or tissues), use of vasoactive drugs and use of
mechanical ventilation. Recently in 2008, Wahab, et al, reported that the development of
refractory shock, ARDS, aspiration pneumonitis, anaemia, metabolic acidosis, electrolyte
imbalance, coma, severe hypoxia, gastrointestinal bleeding, and pericarditis are the factors
associated with poor prognosis (Mathai and Bhanu, 2010; Louriz et al, 2009; Wahab et al,
2008). Simplified Acute Physiology Score II (SAPSII) was proposed for better estimating the
outcome of patients with acute AlP poisoning requiring ICU admission. SAPSII calculated
within the first 24 hours was recognized as a good prognostic indicator (Moghadamnia,
2012).
Leukopenia (decrease in the number of white blood cells in blood) indicates severe AlP
toxicity. Increased amount of glutamic oxaloacetic transaminase (SGOT) or glutamic pyruvic
transaminase (SGPT) in serum and induced metabolic acidosis signifies moderate to severe
AlP toxicity. Analysis of body electrolytes show decreased magnesium level while level of
potassium may be increased or decreased (Chugh et al, 1990). Analysis of plasma renin is

www.wjpps.com Vol 4, Issue 10, 2015.
2286
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
significant as its level in blood carries a direct relationship with mortality and is raised in
direct proportion with the dose of pesticide. In case of severe poisoning, the level of cortisol
in serum is usually found to be decreased. Chest X-ray may reveal hilar or perihilar
congestion if ARDS develops (Chugh et al, 1989).
Changes in cardiovascular and respiratory system can also result in death. In myocardial
tissue, AlP induces congestion, necrosis and leucocytes infiltration. ECG shows various
manifestations such as arrhythmias (Sinus tachycardia, bradycardia), supraventricular
ectopics, ventricular ectopics, atrial fibrillation, ventriclar fibrillation conduction defects
(Wide QRS complex, A-V conduction defects), bundle branch block, complete heart block,
ST depression, ST elevation, T wave changes (Singh and Bhalla, 2015).
TREATMENT AND MANAGEMENT OF ALP
Table 1: Various treatment strategies for managing Aluminum phosphide poisoning
Treatment option Type of Study Effects Conclusion Reference
Digoxin (0.5 mg initially
followed by 0.5 mg
at 6 h intervals)
Case Report
Resolved cardiogenic
shock due to left ventricle
failure
Administration of digoxin as
an adjustment therapy can
improve the outcome
Mehrpour
et al, 2011
Hyperbaric
Oxygen
Experimental
(Rats)
Increasing survival
Time
Administration of hyperbaric
oxygen may also be effective
in humans
Saidi et al,
2011
25Mg 2 + carrying
nanoparticle
Experimental
(Rats)
Increased blood pressure
and heart rate; increase in
antioxidant power, Mg
level in the plasma and
the heart; reduction in
lipid peroxidation and
ADP/ATP ratio
25Mg PMC16 at 0.025 LD50 +
Nabicarbonate was the most
effective
combination
Baeeri et
al, 2011
Intragastric
irrigation with
Sweet Almond oil
Experimental
(Rats)
Protective role for plasma
cholinesterase
inhibition in AlP
poisoning, decreased
mortality rate
Significant reduction
of mortality
Saidi and
Shojaie,
2011
Vitamin C
(1 g at 6 h intervals,
i.v.) +
methylene blue
(1 mg/kg of 1 %
solution)
Case Report
Twelve hours after
treatment with vitamin C,
the methaemoglobin
concentration decreased
from 46 % to 33 %. high
doses of methylene blue,
the methaemoglobin
concentration decreased
to 23 %
Administration of
vitamin C followed by
methylene blue may have a
role in successful treatment of
methaemoglobinaemia
and haemolysis following
phosphine poisoning
Soltaninejad
et al, 2011
Extensive gastric Case Series Survival rate 42 % Recommendation to Bajwa et

www.wjpps.com Vol 4, Issue 10, 2015.
2287
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
lavage
with aliquots of 50
mL of
Coconut oil+ 50
mL of
Sodium
bicarbonate
Solution with
simultaneous
aspiration
(33 patients) intensivists and physicians to
use this
particular regimen of gastric
decontamination
al, 2010
Intra-aortic
Balloon Pump
(IABP)
Case Report
IABP was used for
cardiovascular support
until the effects of AlP
resolved
IABP used for treatment of
cardiogenic shock due
to AlP poisoning can
improve the outcome
Siddaiah et
al, 2009
N-Acetylcysteine
(NAC)
(6.25 mg/kg/min, i.
v. for
30 min)
Experimental
(Rats)
Significantly increased
survival time, stabilization
of blood pressure and
heart rate, decreased
Malonyldialdehyde level
and increased Glutathione
peroxidase
Levels
NAC increased the survival
time by reducing myocardial
oxidative injury
Azad et al,
2011
N-omega-nitro-L-
arginine methyl
ester (L-NAME)
(1 mg/kg/min,, i. v.
for 60 min)
Experimental
(Rats)
Significant rise in
blood pressure but
precipitated ECG
abnormalities. Pre and
post-treatment of L-
NAME with AlP
neither improved the
survival time nor the
biochemical parameters
despite significant rise in
blood pressure
L-NAME showed no
protective effects in
rats exposed to AlP
Azad et al,
2011
Atropine
(1 mg kg-1,
intraperitoneal) +
Pralidoxime
(5 mg/kg,
intraperitoneal)
administered five
minutes
after AlP exposure
Experimental
(Rats)
Increased survival
time. Plasma
cholinesterase levels were
inhibited in rats
poisoned with AlP as
compared to controls
Atropine and pralidoxime can
increase survival time
Mittra et al,
2001
Oral dose of 20 mg
Trimetazidine
twice daily
Case Report
Resolved dysrhythmia
due to AlP poisoning after
48 h [ventricular
premature complexes
(>600 per h) with periods
of bigeminy]
Ventricular dysrhythmias were
treated solely with
oral trimetazidine resulting in
rapid disappearance of all
electrocardiographic
abnormalities
Duenas et
al, 1999

www.wjpps.com Vol 4, Issue 10, 2015.
2288
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
OTHER POSSIBLE TREATMENTS
Patients suffering from AlP poisoning, toxicity occurs basically due to three reasons, i.e.
inhibition of cytochrome c oxydase, increased pH of body and production of reactive oxygen
species (ROS) so we need a treatment which could counter and restore all the three changes.
Phosphine produced by AlP inhibits the cytochrome c oxidase. Phosphine is a reducing agent
having potential of -1.18, it forms a complex with the metal ion cofactor at the active site of
enzyme cytochrome c oxidase inside mitochondria. Inhibition of cytochrome c oxidase
causes oxidative stress.
It is well known that metal phosphides having lower reduction potential are strong electron
donors and therefore considered as strong poisons. Phosphine donates electron to cytochrome
c oxidase (E = +0.29) that leads to disruption of electron transport chain. Therefore,
according to the electrochemical law, if a receiver with a reducing potential of more than
+0.29 is given to the patient, then it will strongly interact with phosphine and in turn,
cytochrome c oxidase will be left vacant and undisrupted.
Table 2: metal ions having reduction potential more than cytochrome c oxidase
Metal ions Reduction potential
Re 3+
+0.30
Bi3+
+0.308
Cu2+
+0.337
Fc+ +0.4
Cu+ +0.520
Fe3+
+0.77
Ag+ +0.7996
Depending upon the severity of patients these metals can be given to patients either as food
supplements (in case of acute AlPP) or as recombinant biotech drug (in case of sever AlPP).
Supportive treatments to reduce pH and degrade ROS should also be given. To maintain the
pH of body as normal, various minerals can be used. Magnesium is an alkali forming mineral
which can give best result when administered transdermally (via skin). Oral supplementation
of magnesium alone is not enough since most of it is excreted without being processed in
body. Antioxidants like polyphenols and ascorbic acid (vitamin C) can enhance the process of
inhibition of oxidation and prevent the formation of ROS.
Another hope in the treatment for AlPP could come through the phosphine resistant gene
found in Rhyzopertha dominica which requires further intensive studies and manipulations
before it can be regarded as a plausible method to treat human patients.

www.wjpps.com Vol 4, Issue 10, 2015.
2289
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
CONCLUSION
Phosphine released from AlP has been identified as the primary culprit accentuating the
morbidity and mortality associated with the acute poisoning cases. Owing to the rapidly
increasing number of deaths and suicides due to ingestion or inhalation of aluminium
phosphide, the need of the hour is the generation and development of a specific antidote
capable of countering the action of PH3 molecules, thus preventing the free radical mediated
cellular and mitochondrial injury: the factors associated with the high mortality rate. We have
suggested a number of possible treatments to combat the acute cases of poisoning, however,
fumigants and compounds containing high levels of aluminium phopshide need to be phased
out of the country as soon as possible or number of organic alternatives could also be
employed to be used as fumigants for example, neem oil fumigation, chrysanthemum flower
tea spray or using eucalyptus oil emulsion as fumigant, to name a few. In addition to this,
public awareness and easy availability of AlP become the two most important issues. Strict
measures, both at the administrative as well as the legislative levels are required to
strategically modify and restrict the supply of AlP in India.
REFERENCES
1. Abedini, M., Fatehi, F., & Tabrizi, N. Ischemic Stroke as a Rare Manifestation of
Aluminum Phosphide Poisoning: a Case Report. Acta Medica Iranica,, 2014; 52(12):
947-949.
2. Agarwal, A., Robo, R., Jain, N., Gutch, M., Consil, S., & Kumar, S. Oxidative stress
determined through the levels of antioxidant enzymes and the effect of N-acetylcysteine
in aluminum phosphide poisoning. Indian journal of critical care medicine: peer-
reviewed, official publication of Indian Society of Critical Care Medicine., 2014; 18(10);
666.
3. Alter, P., Grimm, W., & Maisch, B. Lethal heart failure caused by aluminium phosphide
poisoning. Intensive care medicine., 2001; 27(1): 327-327.
4. Anand, R., Binukumar, B. K., & Gill, K. D. Aluminum phosphide poisoning: an unsolved
riddle. Journal of Applied Toxicology., 2011; 31(6): 499-505.
5. Anger, F., Paysant, F., Brousse, F., Le Normand, I., Develay, P., Galliard, Y., ... & Anger,
J. P. Fatal aluminum phosphide poisoning. Journal of analytical toxicology., 2000; 24(2):
90-92.
www.wjpps.com Vol 4, Issue 10, 2015.
2290
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
6. Azad, A., Lall, S. B., & Mittra, S. Effect of N-acetylcysteine and L-NAME on aluminium
phosphide induced cardiovascular toxicity in rats. Acta pharmacologica Sinica.,
2001; 22(4): 298-304.
7. Baeeri, M., Shariatpanahi, M., Baghaei, A., Ghasemi-Niri, S. F., Mohammadi, H.,
Mohammadirad, A., & Abdollahi, M. On the benefit of magnetic magnesium nanocarrier
in cardiovascular toxicity of aluminum phosphide.Toxicology and industrial health.,
2013; 29(2): 126-135.
8. Bajwa, S. J. S., Bajwa, S. K., Kaur, J., Singh, K., & Panda, A. Management of celphos
poisoning with a novel intervention: A ray of hope in the darkest of clouds. Anesthesia,
essays and researches., 2010; 4(1): 20.
9. Bogle, R. G., Theron, P., Brooks, P., Dargan, P. I., & Redhead, J. Aluminium phosphide
poisoning. Emergency Medicine Journal., 2006; 23(1): e03-e03.
10. Chaudhry, M. Q., & Price, N. R. A spectral study of the biochemical reactions of
phosphine with various haemproteins. Pesticide Biochemistry and Physiology.,
1990; 36(1): 14-21.
11. Chefurka, W., Kashi, K. P., & Bond, E. J. The effect of phosphine on electron transport in
mitochondria. Pesticide Biochemistry and Physiology., 1976; 6(1): 65-84.
12. Chemistry learner (http://www.chemistrylearner.com/aluminum-phosphide.html)
13. Chugh, S. N., Ram, S. A. N. T., Sharma, A. N. J. A. L. I., Arora, B. B., Saini, A. S., &
Malhotra, K. C. Adrenocortical involvement in aluminium phosphide poisoning. The
Indian journal of medical research., 1989; 90: 289-294.
14. Chugh, S. N., Juggal, K. L., Sharma, A., Arora, B., & Malhotra, K. C. Magnesium levels
in aluminium phosphide poisoning. J Assoc Physicians India., 1990; 38: 32.
15. Chugh, S. N., Arora, V., Kaur, S., & Sood, A. K. Toxicity of exposed aluminium
phosphide. The Journal of the Association of Physicians of India., 1993; 41(9): 569-570.
16. Chugh, S. N., Arora, V., Sharma, A., & Chugh, K. Free radical scavengers & lipid
peroxidation in acute aluminium phosphide poisoning. The Indian journal of medical
research., 1996; 104: 190-193.
17. Corbridge, D. E. C. (1995). Phosphorus: An Outline of its Chemistry, Biochemistry, and
Technology (5th ed.). Amsterdam: Elsevier.
18. Dua, R., Kumar, V., Sunkaria, A., & Gill, K. D. Altered glucose homeostasis in response
to aluminium phosphide induced cellular oxygen deficit in rat. Indian journal of
experimental biology., 2010; 48(7): 722.

www.wjpps.com Vol 4, Issue 10, 2015.
2291
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
19. Duenas A, Perez-Castrillon JL, Cobos MA, Herreros V. Treatment of the cardiovascular
manifestations of phosphinepoisoning with trimetazidine, a new antiischemic drug. Am J
Emerg Med., 1999; 17: 219-20.
20. Ellenhorn, M.J. and D.G. Barceloux. Medical Toxicology - Diagnosis and Treatment of
Human Poisoning. New York, NY: Elsevier Science Publishing Co., Inc., 1988; 1053.
21. Goel, A., & Aggarwal, P. Pesticide poisoning. National medical journal of India.,
2007; 20(4): 182.
22. Holleman, A. F.; Wiberg, E. (2001), Inorganic Chemistry, San Diego: Academic Press.
23. Hugar, B. S., Praveen, S., Hosahally, J. S., Kainoor, S., & Shetty, A. R. S.
Gastrointestinal hemorrhage in aluminum phosphide poisoning. Journal of forensic
sciences., 2015; 60(s1): S261-S263.
24. Kashi, K. P., & Chefurka, W. The effect of phosphine on the absorption and circular
dichroic spectra of cytochrome c and cytochrome oxidase.Pesticide Biochemistry and
Physiology, 1976; 6(4): 350-362.
25. Kirk-Othmer Encyclopedia of Chemical Technology. 3rd ed., Volumes 1-26. New York,
NY: John Wiley and Sons, 1978-1984; 17: 488(1982).
26. Louriz, M., Dendane, T., Abidi, K., Madani, N., Abouqal, R., & Zeggwagh, A. A.
Prognostic factors of acute aluminum phosphide poisoning. Indian journal of medical
sciences, 2009; 63(6): 227.
27. Mathai, A., & Bhanu, M. S. Acute aluminium phosphide poisoning: Can we predict
mortality?. Indian journal of anaesthesia., 2010; 54(4): 302.
28. Mehrpour O, Farzaneh E, Abdollahi M. Successful Treatment of aluminum phosphide
poisoning with digoxin: a case report and review of literature. Int J Pharmacol., 2011; 7:
761-4.
29. Mehrpour, O., Jafarzadeh, M., & Abdollahi, M. (2012). A systematic review of
aluminium phosphide poisoning. Archives of Industrial Hygiene and Toxicology., 2012;
63(1): 61-73.
30. Mittra, S., Peshin, S. S., & Lall, S. B. (2000). Cholinesterase inhibition by aluminium
phosphide poisoning in rats and effects of atropine and pralidoxime chloride. Acta
Pharmacologica Sinica., 2000; 22(1): 37-39.
31. Moghadamnia, A. A., & Abdollahi, M. (2002). An epidemiological study of poisoning in
northern Islamic Republic of Iran.
32. Moghadamnia, A. A. (2012). An update on toxicology of aluminum
phosphide.Daru, 2002; 20(1): 25.

www.wjpps.com Vol 4, Issue 10, 2015.
2292
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
33. Moghadamnia AA, Khalilian E, Mahdipour E, Salar N, Ghafouri M. Epidemiological
study of poisoning in Babol. J Babol Univ Med Sci, 2012; 1–8.
34. Mostafazadeh, B., (2012). Aluminium phosphide poisoning. INTECH Open Access
Publisher.
35. Nakakita, H., KATSUMATA, Y., & OZAWA, T. The effect of phosphine on respiration
of rat liver mitochondria. Journal of biochemistry, 1971; 69(3): 589-593.
36. Nocera, A., Levitin, H. W., & Hilton, J. M. Dangerous bodies: a case of fatal aluminium
phosphide poisoning. The Medical journal of Australia, 2000; 173(3): 133-135.
37. Potter, W. T., Garry, V. F., Kelly, J. T., Tarone, R., Griffith, J., & Nelson, R. L.
Radiometric assay of red cell and plasma cholinesterase in pesticide appliers from
Minnesota. Toxicology and applied pharmacology, 1993; 119(1): 150-155.
38. Ragone, S., Bernstein, J., Lew, E., & Weisman, R. Fatal aluminum phosphide ingestion. J
Toxicol-Clin Toxic, 2002; 40: 690.
39. Saidi, H., & Shojaie, S. Effect of sweet almond oil on survival rate and plasma
cholinesterase activity of aluminum phosphide-intoxicated rats. Human & experimental
toxicology, 2012; 31(5): 518-522.
40. Saidi, H., Shokraneh, F., Ghafouri, H. B., & Shojaie, S. Effects of hyperbaric oxygenation
on survival time of aluminum phosphide intoxicated rats. Journal of research in medical
sciences: the official journal of Isfahan University of Medical Sciences, 2011; 16(10):
1306.
41. Siddaiah, L. M., Adhyapak, S. M., Jaydev, S. M., Shetty, G. G., Varghese, K., Patil, C.
B., & Iyengar, S. S. Intra-aortic balloon pump in toxic myocarditis due to aluminum
phosphide poisoning. Journal of medical toxicology, 2009; 5(2): 80-83.
42. Singh, D unpublished data
43. Singh, D., Dewan, I., Pandey, A. N., & Tyagi, S. Spectrum of unnatural fatalities in the
Chandigarh zone of north-west India–a 25 year autopsy study from a tertiary care
hospital. Journal of clinical forensic medicine, 2003; 10(3): 145-152.
44. Soltaninejad, K., Nelson, L. S., Khodakarim, N., Dadvar, Z., & Shadnia, S. (2011).
Unusual complication of aluminum phosphide poisoning: Development of hemolysis and
methemoglobinemia and its successful treatment. Indian journal of critical care
medicine: peer-reviewed, official publication of Indian Society of Critical CareMedicine.,
2011; 15(2): 117.
45. Surjit Singh, Ashish Bhalla. (2015).Aluminum phosphide poisoning. Journal of Mahatma
Gandhi Institute of Medical Sciences., 2015; 20(1).

www.wjpps.com Vol 4, Issue 10, 2015.
2293
Kumud et al. World Journal of Pharmacy and Pharmaceutical Sciences
46. Valmas, N., Zuryn, S., & Ebert, P. R. Mitochondrial uncouplers act synergistically with
the fumigant phosphine to disrupt mitochondrial membrane potential and cause cell
death. Toxicology., 2008; 252(1): 33-39.
47. Van Zeghbroeck, B. J. (1997). "Bravais Lattices; Zincblende Lattice". University of
Colorado.
48. Wahab, A., Zaheer, M. S., Wahab, S., & Khan, R. A. Acute aluminium phosphide
poisoning: an update. Hong Kong J Emerg Med., 2008; 15(3): 152-5.
49. White, W. E., & Bushey, A. H. Aluminum Phosphide—Preparation and
Composition1. Journal of the American Chemical Society, 1944; 66(10): 1666-1672.
50. White, W. E., Bushey, A. H., Holtzclaw, H. F., & Hengeveld, F. W. Aluminum
Phosphide. Inorganic Syntheses., 1953; 4: 23-25.