alteration in metabolism in surgical patients. energy metabolism l in order to mount a metabolic...
TRANSCRIPT
Alteration in Alteration in MetabolismMetabolism
ininSurgical PatientsSurgical Patients

Energy MetabolismEnergy Metabolism
In order to mount a metabolic In order to mount a metabolic response to injury the body uses response to injury the body uses as a fuel glucose, fat and proteinas a fuel glucose, fat and protein
How much fuel does the body How much fuel does the body have?have?
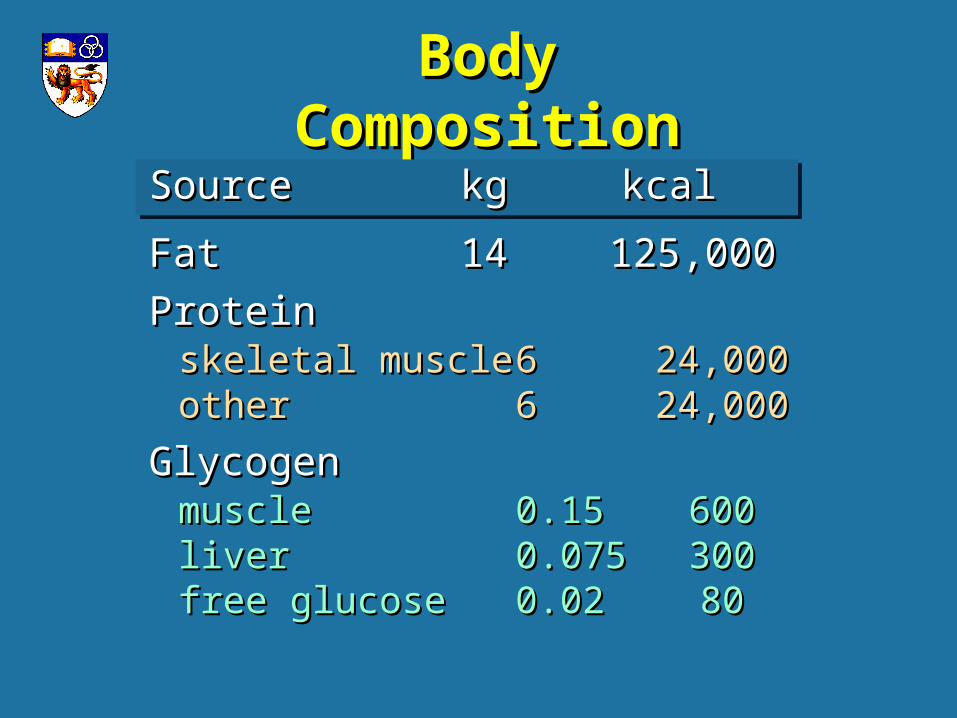
Body CompositionBody Composition
SourceSource kgkg kcal kcal
FatFat 1414 125,000125,000
ProteinProteinskeletal muscleskeletal muscle 66 24,00024,000otherother 66 24,00024,000
GlycogenGlycogenmusclemuscle 0.150.15 600600liverliver 0.0750.075 300300free glucosefree glucose 0.020.02 8080

Body CompositionBody Composition
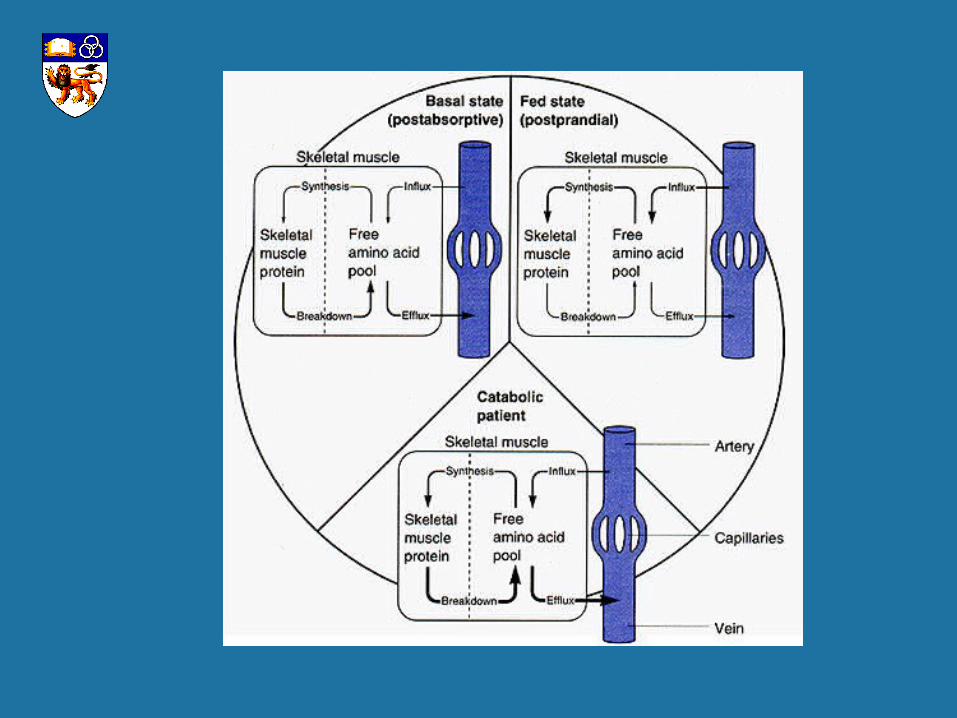
Even though protein is used as a fuel Even though protein is used as a fuel
in stress, its depletion is detrimental in stress, its depletion is detrimental
Body CompositionBody Composition
GlycogenGlycogen -- FuelFuel
FatFat - - FuelFuel
ProteinProtein - - Structure Structure (use as a fuel should be (use as a fuel should be minimised)minimised)
Protein & Amino AcidProtein & Amino AcidMetabolismMetabolism
ProteinProtein 15% body weight - 15% body weight - ½½ intracellular intracellular Enzymes, transport, hormones, immune Enzymes, transport, hormones, immune
Fx, muscleFx, muscle It is not usually a foodIt is not usually a food when needed it is converted to glucosewhen needed it is converted to glucose
Total protein turnoverTotal protein turnover 300g300g /day/day
Obligatory N loss in urineObligatory N loss in urine 12g12g /day/day
or 80g protein /dayor 80g protein /day
Protein & Amino AcidProtein & Amino AcidMetabolismMetabolism

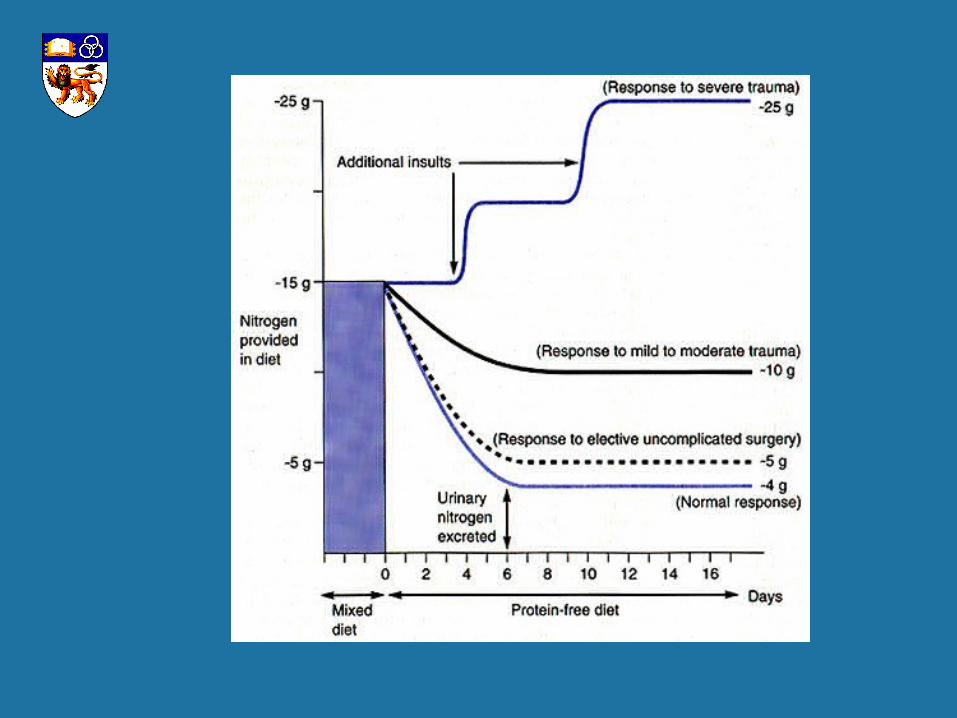
Nitrogen BalanceNitrogen Balance
NN balancebalance = N = N intakeintake - N - N outout
Negative in starvation, injury, Negative in starvation, injury, severe infectionsevere infection
Protein & Amino AcidProtein & Amino AcidMetabolismMetabolism

Response toResponse toStarvation vs InjuryStarvation vs Injury
ParameterParameter StarvationStarvation TraumaTrauma
BMRBMR -- ++++
MediatorsMediators -- ++++++
Major fuelMajor fuel FatFat MixedMixed
Ketone productionKetone production ++++++ +/-+/-
Hepatic ureagenesisHepatic ureagenesis ++ ++++++
Neg N balanceNeg N balance ++ ++++++
GluconeogenesisGluconeogenesis ++ ++++++
Muscle proteolysisMuscle proteolysis ++ ++++++
Hepatic protein synthesisHepatic protein synthesis ++ ++++++
If protein is depleted via proteolysis –If protein is depleted via proteolysis –ability to adapt in stress is compromisedability to adapt in stress is compromised
protein depletion results in protein depletion results in decreased wound healingdecreased wound healing decreased immune responsedecreased immune response defective gut-mucosal barrierdefective gut-mucosal barrier decreased mobility/ respiratory effortdecreased mobility/ respiratory effort
Protein & Amino AcidProtein & Amino AcidMetabolismMetabolism
Homeostatic ResponsesHomeostatic Responsesto Stressto Stress
Designed to maintain homeostasisDesigned to maintain homeostasis
Same response in controlled or Same response in controlled or uncontrolled stressuncontrolled stress
Trigger mechanisms:Trigger mechanisms: Volume lossVolume loss Tissue damageTissue damage PainPain FearFear

Volume Loss & Tissue UnderperfusionVolume Loss & Tissue Underperfusion
Pressure & Stretch receptors activated Pressure & Stretch receptors activated
HR / SV increasedHR / SV increased
ADH / Aldosterone secreted - ADH / Aldosterone secreted - renal and hypothalamic mechanismrenal and hypothalamic mechanism
Need for adequate resuscitationNeed for adequate resuscitation
Homeostatic ResponsesHomeostatic Responsesto Stressto Stress

Tissue DamageTissue Damage
Most important triggerMost important trigger
Neural pathways from wound Neural pathways from wound reach hypothalamusreach hypothalamus efferents go to pancreas efferents go to pancreas glucagon glucagon insulininsulin efferents to adrenal efferents to adrenal cortisol, catecolamines cortisol, catecolamines
Release of cytokinesRelease of cytokines
Homeostatic ResponsesHomeostatic Responsesto Stressto Stress
Pain & FearPain & Fear
Increased levels of Increased levels of catecholaminescatecholamines
Fight or flight responseFight or flight response
Homeostatic ResponsesHomeostatic Responsesto Stressto Stress

Homeostatic ResponseHomeostatic Response
Elective operationElective operation min tissue damagemin tissue damage pain/fear managedpain/fear managed less hypotensionless hypotension infection rareinfection rare stress response in controlledstress response in controlled
Homeostatic ResponseHomeostatic Response
TraumaTrauma major tissue damagemajor tissue damage pain/fear excessive managedpain/fear excessive managed hypotension commonhypotension common infection commoninfection common Stress response uncontrolledStress response uncontrolled
TriggersTriggers ResponseResponse
Volume loss Volume loss Neurohormonal andNeurohormonal and
Tissue damageTissue damage Inflammatory armsInflammatory arms
Pain & Fear Pain & Fear
Homeostatic ResponsesHomeostatic Responsesto Stressto Stress
Mediators ofMediators ofStress ResponseStress Response
Neurohormonal armNeurohormonal arm Catecolamines, glucocorticoids, Catecolamines, glucocorticoids,
glucagon, ADH, aldosteroneglucagon, ADH, aldosterone
Inflammatory armInflammatory arm Cytokines, complement, eicisanoids, Cytokines, complement, eicisanoids,
PAFPAF

Mediators of Stress ResponseMediators of Stress Response
Neurohormonal ArmNeurohormonal Arm- Counterregulatory Hormones- Counterregulatory Hormones
catecholaminescatecholamines maintain circulation, maintain circulation, hepatic glycolysis, lipolysis, hepatic glycolysis, lipolysis,
gluconeogenesis, gluconeogenesis, BMR BMR glucagonglucagon
glycogenolytic, gluconeogenicglycogenolytic, gluconeogenic glucocorticoids?/ACTHglucocorticoids?/ACTH
mobilise muscle protein, gluconeogenesismobilise muscle protein, gluconeogenesis ADH. AldosteroneADH. Aldosterone
Retain water and NaRetain water and Na

Inflammatory Arm - CytokinesInflammatory Arm - Cytokines
TNF-alpha, IL-1, IL-2, IL-6, TNF-alpha, IL-1, IL-2, IL-6, IFN-gammaIFN-gamma
Local effects - para or autocrineLocal effects - para or autocrine
Response to tissue injuryResponse to tissue injury
Mediators ofMediators ofStress ResponseStress Response
CytokinesCytokines
In elective surgeryIn elective surgery confined to woundconfined to wound
Trauma/sepsisTrauma/sepsis spill over/ endocrine effectspill over/ endocrine effect
Mediators ofMediators ofStress ResponseStress Response
Cytokines - local effectCytokines - local effect
Promote wound healing Promote wound healing
Stimulate angiogenesisStimulate angiogenesis
White cell migrationWhite cell migration
Ingrowth of fibroblastsIngrowth of fibroblasts
Localise the woundLocalise the wound
Mediators ofMediators ofStress ResponseStress Response


Cytokines - spill over Cytokines - spill over
Mobilisation of AA, stimulation of Mobilisation of AA, stimulation of acute phase protein synthesisacute phase protein synthesis
Increase WBC counts/HypoferremiaIncrease WBC counts/Hypoferremia
Fever, subjective discomfort, sleepFever, subjective discomfort, sleep
Mediators ofMediators ofStress ResponseStress Response

Cytokines - severe trauma /sepsisCytokines - severe trauma /sepsis
Increased organ vascular permeabilityIncreased organ vascular permeability
Multiple organ dysfunctionMultiple organ dysfunction
HypotensionHypotension
Mediators ofMediators ofStress ResponseStress Response
Stress Stress Response Response
The stress just described response The stress just described response may be characterised as a may be characterised as a adrenergic adrenergic corticoid phasecorticoid phase
When the patient recovers the When the patient recovers the adrenergic corticoid phase changes adrenergic corticoid phase changes to an to an anabolic phaseanabolic phase
Stress ResponseStress ResponseAdrenergicAdrenergic--Corticoid PhaseCorticoid Phase
ACTH and cortisolACTH and cortisol mobilises proteinmobilises proteingluconeogenesisgluconeogenesis
CatecolaminesCatecolamines circulatory adjustmentcirculatory adjustment metabolic response if prolongedmetabolic response if prolonged
Aldosterone and ADHAldosterone and ADH Salt and water retentionSalt and water retention
Insulin and Insulin and glucagon (via epinephrine) glucagon (via epinephrine) gluconeogenesisgluconeogenesis
Cytokines confined to woundCytokines confined to wound


Stress ResponseStress Response
Adrenergic - corticoid phaseAdrenergic - corticoid phase
Remains until insult correctedRemains until insult corrected
Hypermetabolism-BMR Hypermetabolism-BMR increasesincreases
10-15%10-15% in elective operationin elective operation
25% 25% in long bone fracturein long bone fracture
200% 200% in 50% burnin 50% burn
Stress Stress ResponseResponse
Adrenergic - corticoid phaseAdrenergic - corticoid phase
Altered Glucose MetabAltered Glucose Metab
Normal/low insulin and insulin resistanceNormal/low insulin and insulin resistance
persisting hyperglycaemiapersisting hyperglycaemia
injured tissue uses glucoseinjured tissue uses glucose
Stress ResponseStress Response
ADRENERGIC - CORTICOID PHASEADRENERGIC - CORTICOID PHASE
Altered protein metabolismAltered protein metabolism Extensive muscle protein releaseExtensive muscle protein release extensive urine N loss extensive urine N loss reduced by feedingreduced by feeding
Altered fat metabolismAltered fat metabolism Accelerated lipolysis via hormone Accelerated lipolysis via hormone
sensitivesensitive lipaselipase Ketosis bluntedKetosis blunted

ANABOLIC PHASEANABOLIC PHASE gluconeogenesisgluconeogenesis catecolaminescatecolamines
aldosterone and ADHaldosterone and ADH Salt and water lossSalt and water loss
insulin and insulin and glucagon glucagon protein anabolismprotein anabolism
cytokines reductioncytokines reduction
Stress ResponseStress Response

Elective Elective OperationsOperations
Adrenergic corticoid Adrenergic corticoid phasephase period of catabolism period of catabolism lasts 1-3 dayslasts 1-3 days
Anabolic phaseAnabolic phase starts D3-D6starts D3-D6 positive N balancepositive N balance protein synthesisprotein synthesis recovery of lean massrecovery of lean mass
Nutritional SupportNutritional Supportfor Elective Operationsfor Elective Operations
Because the adrenergic-corticoid phase is Because the adrenergic-corticoid phase is short in elective, uncomplicated surgery short in elective, uncomplicated surgery
– Fluid therapy with 5% dextrose is Fluid therapy with 5% dextrose is enough for up to 5-7 daysenough for up to 5-7 days
Nutritional SupportNutritional Supportfor Severe Stressfor Severe Stress
The adrenergic-corticoid phase is The adrenergic-corticoid phase is prolonged inprolonged in
severe injury severe injury Malnourished patientsMalnourished patients Infected patientsInfected patients
Nutritional therapy is neededNutritional therapy is needed

Stress ResponsesStress Responses
The response is The response is affectedaffected
MalnutritionMalnutrition
Age Age
GenderGender
InfectionInfection
ConsequencesConsequencesof Malnutritionof Malnutrition
Metabolic response needs increased energy Metabolic response needs increased energy expenditureexpenditure
If intake < expenditure - protein/fat mass lostIf intake < expenditure - protein/fat mass lost Loss of 15% BW interacts with disease Loss of 15% BW interacts with disease
process toprocess to compromise immune response - sepsis, MOFcompromise immune response - sepsis, MOF poor wound healingpoor wound healing edema due to edema due to albumin albumin reduced mobility, reduced mobility, respiratory muscle strength & respiratory muscle strength &
vital capacity vital capacity pneumonia pneumonia altered GI function/breached mucosal barrieraltered GI function/breached mucosal barrier

Normal Post Op Normal Post Op DripDrip
Energy provided as dextroseEnergy provided as dextrose
1 L of D5W - 50g or 170 kcal1 L of D5W - 50g or 170 kcal
Typical post op patient gets 500 kcal/dTypical post op patient gets 500 kcal/d enough to stimulate pancreatic insulinenough to stimulate pancreatic insulin not enough to support a severe stress not enough to support a severe stress
reactionreaction
Need for nutritional support to match Need for nutritional support to match energy expenditure if stress is prolongedenergy expenditure if stress is prolonged

Metabolic ResponseMetabolic Responseto Trauma / to Trauma /
Severe Surgical StressSevere Surgical Stress
Unfed trauma patients rapidly use their Unfed trauma patients rapidly use their protein and fat stores resulting in protein and fat stores resulting in increased susceptibility to effects of increased susceptibility to effects of haemorrhage, operations and infection haemorrhage, operations and infection resulting in organ system failure, sepsis resulting in organ system failure, sepsis and deathand death
Malnourished patients are at greater riskMalnourished patients are at greater risk

Determinants of HostDeterminants of HostResponses to Surgical StressResponses to Surgical Stress
AgeAge Fat mass increase with ageFat mass increase with age Loss of muscle massLoss of muscle mass Loss of strength with immobilityLoss of strength with immobility Decreased sensitivity to perturbationsDecreased sensitivity to perturbations Decreased effectiveness to maintain Decreased effectiveness to maintain
homeostasishomeostasis
GenderGender Lean body mass less in Lean body mass less in
femalesfemales
N loss more pronounced in N loss more pronounced in muscular malesmuscular males
Determinants of HostDeterminants of HostResponses to Surgical StressResponses to Surgical Stress

Invasive InfectionInvasive Infection
May complicate any operation / injuryMay complicate any operation / injury
Results in increases metabolic rate - Results in increases metabolic rate - fever, hyperventilation, etcfever, hyperventilation, etc
Nutritional depletion synergysticNutritional depletion synergystic
Determinants of HostDeterminants of HostResponses to Surgical StressResponses to Surgical Stress
Cuthbertson described in 1930 theCuthbertson described in 1930 the Ebb or shock phaseEbb or shock phase Flow phaseFlow phase
CuthbertsonCuthbertson ModernModernEbbEbb unresuscitatedunresuscitatedFlow Flow adrenergic-adrenergic-
corticoidcorticoidnot describednot described anabolic anabolic
Metabolic ResponseMetabolic Responseto Trauma / to Trauma /
Severe Surgical StressSevere Surgical Stress
Cuthbertson Cuthbertson Ebb or shock phaseEbb or shock phase
12-24 hours12-24 hours BP, BP, CO, CO, Temp, Temp, O O22 consumption consumption due to haemorrhage, hypoperfusion, due to haemorrhage, hypoperfusion,
lactic acidosislactic acidosis Flow phase (adrenergic - corticoid)Flow phase (adrenergic - corticoid)
hypermetabolism, hypermetabolism, CO, CO, Urine N loss, Urine N loss, altered glucose, tissue catabolismaltered glucose, tissue catabolism
similar to elective surgery but greatersimilar to elective surgery but greater
Metabolic ResponseMetabolic Responseto Trauma / to Trauma /
Severe Surgical StressSevere Surgical Stress

Questions ?Questions ?
A 64 year old 70 kg man comes for a gastrectomy. A 64 year old 70 kg man comes for a gastrectomy. Prior to operation he had been eating poorly for 4 Prior to operation he had been eating poorly for 4 weeks. On the 7th POD after Billroth II gastrectomy weeks. On the 7th POD after Billroth II gastrectomy he was drowsy and febrile. There was green fluid he was drowsy and febrile. There was green fluid coming from his drain.coming from his drain.
Describe the metabolic responses this patient has.Describe the metabolic responses this patient has.
What are the confounding factors that may What are the confounding factors that may complicate his recovery?complicate his recovery?
In a severely injured patient the priorities In a severely injured patient the priorities are:are: - resuscitation- resuscitation
- wound care- wound care
Nutritional support usually after 48 hrsNutritional support usually after 48 hrs
The next lecture will cover all aspects The next lecture will cover all aspects of nutritionof nutrition
Coming soon to aComing soon to aLecture Theatre near youLecture Theatre near you
– Nutritional Support– Nutritional Support

QuestionsQuestions