alpha blockers alpha receptors have been further subdivided into alpha 1 and alpha 2 receptors....
TRANSCRIPT

ALPHA BLOCKERS
Alpha receptors have been further subdivided into alpha1 and alpha2 receptors.
Alpha -1 receptors – Upon stimulation, leads to increased IP3 and DAG through Gq activated PLC.
contraction of arterioles and venules. contraction of radial fibers in the eye. contraction of vas deferens (ejaculation). contraction of bladder trigone.

ALPHA BLOCKERS
EFFECTS OF ALPHA-1 BLOCKER: Blockade of vasoconstriction - hypotension Postural reflex is interfered – postural
hypotension Reflex tachycardia – due to fall in BP Promote urinary outflow Failure of ejaculation

ALPHA BLOCKERS
ALPHA BLOCKERS
Irreversible Nonselective blockers
Reversible Nonselective blockers
Reversible Selective α-1 blockers
Reversible selective α-1A blockers
Selective α-2blockers
PROTYPEPhenoxy -benzamine (PBZ)
Phentolamine Prazosin Terazosin
Tamsulosin Silodosin
Yohimbine
INDICATIONSPheochromo cytoma
Pheochromocytoma
Hypertension BPH
BPH Erectile dysfunction

ALPHA -1 BLOCKERS
PRAZOSIN (Minipress): Orally active selective alpha-1 blocker. Used in hypertension and treatment of urinary
retention due to benign prostrate hypertrophy. Postural hypotension – first dose phenomenon
– start with low dose at bed time to reduce it. Sexual dysfunction – retrograde ejaculation. Favorable effects on lipoproteins

BETA BLOCKERS
Cornerstone of Coronary Artery Disease therapy – except prinzmetal’s angina
Standard therapy for unstable and stable angina.
One of the preferred therapies for hypertension with myocardial infarction.
One of the major anti-arrhythmic group of drugs.
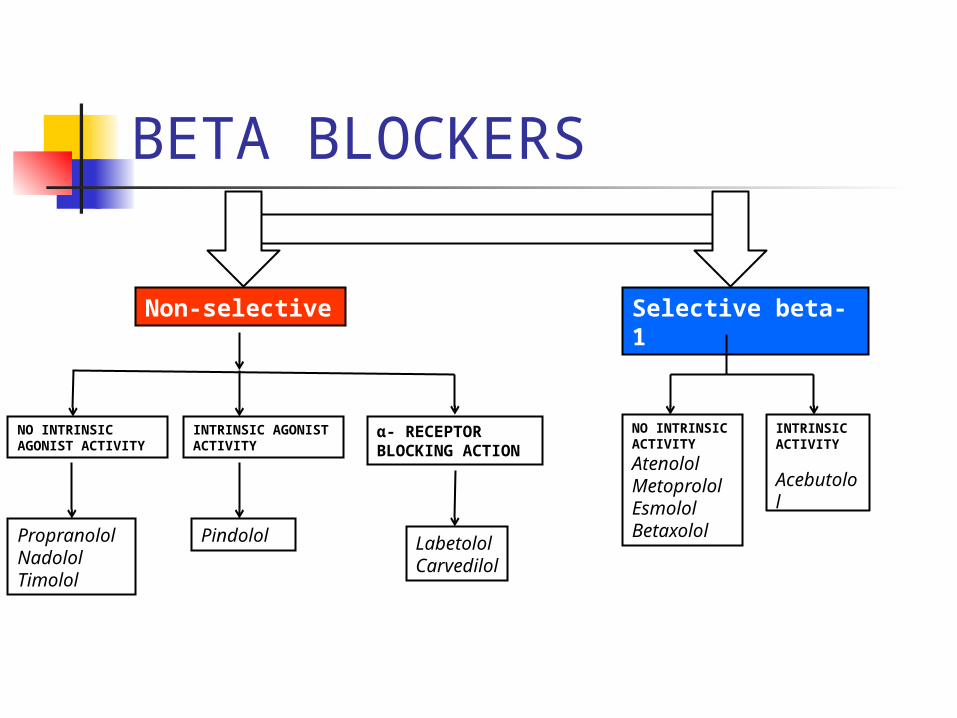
BETA BLOCKERS
α- RECEPTOR BLOCKING ACTION
Non-selective Selective beta-1
NO INTRINSIC AGONIST ACTIVITY
INTRINSIC AGONIST ACTIVITY
Propranolol Nadolol Timolol
Pindolol LabetololCarvedilol
NO INTRINSIC ACTIVITY
Atenolol MetoprololEsmololBetaxolol
INTRINSIC ACTIVITY
Acebutolol

BETA BLOCKERS
PROPRANOLOL : It undergoes extensive first pass
metabolism and oral bioavailability is low. The proportion of drug reaching systemic
circulation increases as the dose is increased suggesting that hepatic extraction mechanism may be saturated.

BETA BLOCKERS
PROPRANOLOL : Heart : Negative inotropic action
Negative chronotropic action
AV conduction is decreased Long term use of beta blockers are
associated with unfavorable increase in VLDL and decrease in HDL.

BETA BLOCKERS
PROPRANOLOL : Eyes : decrease intraocular tension in
chronic simple glaucoma by reducing aqueous humor production
CNS : sedation, lethargy, depression, sleep disturbances
Skeletal muscle : antagonizes the epinephrine induced tremors (β-2)
Respiratory tract : bronchoconstriction and can precipitate bronchial asthma

BETA BLOCKERS
PROPRANOLOL: Metabolic effects : blocks the warning signals due to counter
regulatory effects of catecholamines during hypoglycemia.
delays recovery from hypoglycemia in diabetes mellitus.
CAUTION in DM : Beta-1 selective – preferred Benefits outweigh risks in diabetics and
myocardial infarction.

BETA BLOCKERS
PRECAUTIONS AND ADVERSE EFFECTS : AV block and bradycardia Bronchial asthma and COPD Cold extremities Depression Hyperlipidemia Sexual dysfunction

BETA BLOCKERS
USES OF BETA BLOCKERS: Hypertension Coronary artery disease and Arrhythmia CCF – low dose and in mild and moderate cases Hypertrophic obstructive cardiomyopathy Chronic Simple Glaucoma Hyperthyroidism Migraine prophylaxis Prevention of esophageal varices bleeding in portal
hypertension / cirrhosis

Following abrupt cessation of therapy with certain beta-blocking agents, an increased incidence of angina pectoris and, in some cases, myocardial infarction have occurred. When discontinuing chronically administered metoprolol-XL (Toprol-XL ®), particularly in patients with ischemic heart disease, the dosage should be gradually reduced over a period of 1 - 2 weeks and the patient should be carefully monitored. If angina markedly worsens or acute coronary insufficiency develops, metoprolol-XL administration should be reinstated promptly, at least temporarily, and other measures appropriate for the management of unstable angina should be taken. Warn patients against interruption or discontinuation of therapy without the physician's advice. Because coronary artery disease is common and may be unrecognized, it may be prudent not to discontinue metoprolol-XL therapy abruptly even in patients treated only for hypertension.
Black Box Warning: SUDDEN DISCONTINUATION IN PATIENTS WITH ISCHEMIC HEART DISEASE

Ganglion blockers
Ganglion blockers are competitive antagonist at nicotinic N-type receptors in autonomic ganglia.
Net effect of the blocker is to reduce the predominant tone.
Effects are predictable and depend on the relative dominance in terms of PANS and SANS.

Ganglion blockersEFFECTOR ORGANS
DOMINANT SYSTEM
EFFECTS OF GANGLIONIC BLOCKADE
Arterioles/ veins SANS Vasodilatation, hypotension
Sweat glands SANS (cholinergic) Anhydrosis
Genitals PANS/SANS Impotence
Heart PANS Tachycardia
Iris PANS Mydriasis
Ciliary muscle PANS Cycloplegia
Bladder PANS Urinary retention
Salivary PANS Xerostomia
GIT PANS Constipation.
Ganglion blockers
Ganglionic blocking agents : Mecamylamine, Trimethaphan. It is occasionally used in treatment of
hypertensive crisis and dissecting aortic aneurysm.

Ganglion blocking agents
Ganglion blocking agents block the reflex changes in heart rate elicited by increase / decrease in blood pressure.
Trimethaphan will block the reflex bradycardia that occurs when phenylephrine causes vasoconstriction, but it will not block a bradycardia that results from direct activation of muscarinic receptors in heart.

Role of ganglionic blockers

Ganglion blocking agents The result of the test drug Z are shown in
the graph.
0
100
-100
Heart rateControl Trimetho
phanAtropine

Ganglion blocking agents
Drug Z is probably a drug similar to A. Acetylcholine B. Dopamine C. Epinephrine D. Phenylephrine D. Norepinephrine

GlaucomaGlaucoma is divided into• Chronic Simple Glaucoma - Common• Acute Congestive Glaucoma - Surgery The routes of aqueous humor drainage --
~ 90% through trabecular route
~ 10% passes through within the ciliary muscle into episceral vessels (uveosceral flow)
Objective of glaucoma therapy : ---
1. increase outflow of aqueous humor
2. decrease production of aqueous humor

Beta blockers Alpha-2 agonist CA inhibitor
Pilocarpine PG analog
TREATMENT OF CHRONIC SIMPLE GLAUCOMA

DRUG GROUP FOR CHRONIC SIMPLE GLAUCOMA
MECHANISM OF ACTION ADDITIONAL COMMENTS
PROSTAGLANDINS LatanoprostBimatoprost, Travoprost
Increase uveoscleral outflow and may decrease production of aqueous humor
Drugs of 1st Choice
BETA BLOCKERSTimolol (β1and β2 )Betaxolol (β1 selective)
Reduce formation of aqueous humor and may increase outflow
Can cause severe bronchospasm in asthmatics; probably 2nd choice
ALPHA2 AGONISTSBrimonidineApraclonidine
Reduce formation of aqueous humor and may enhance outflow
Usually “add on” choice
CARBONIC ANHYDRASE INHIBITORSDorzolamide, Acetazolamide
Reduce formation of aqueous humor
Usually “add on” choice
CHOLINOMIMETICSPilocarpineCarbachol
Increase outflow by its effects on ciliary and sphincter pupillae muscles
Much less popular now due to unwanted effects