all spc members have signed a coi form
TRANSCRIPT

2020-2021 MAHC Grand Rounds Program Committee Members:
Dr. Dave McLinden (Co-Chair) Dr. Jessica Reid (Co-Chair)
Dr. Scott Whynot Dr. Allison Small
Dr. Khaled Salem Dr. Dave Johnstone
Krista Hailstone

All SPC members have signed a COI form.
All speakers have been emailed the certification/accreditation requirements for their
presentation and have signed a COI and a speaker release form.
Each presentation is reviewed by the Education Coordinator prior to its delivery. The
coordinator will be looking for any signs of bias including use of brand names and logos.
If bias is detected in the presentation the SPC would review it and the speaker would be
notified so that the bias can be corrected before the presentation is given. If the bias
cannot be corrected or removed the session would be cancelled.
If a bias is detected by a planning committee member during the presentation they would
question the speaker about it.
All reported biases would be reviewed at the next SPC meeting.
Your Scientific Planning Committee has
taken the following precautions for security
and confidentiality purposes:
These sessions are being broadcast but not recorded.
All attendees are placed in a ‘waiting room’, the Education Coordinator acts as a moderator during the
sessions and is required to permit entrance to each attendee. If the moderator does not recognize a
name, she will message them privately to determine if they should actually be attending.
Case presentations have been de-identified as follows:
Intervals have been used for ages.
No specific dates have been used. Only the qualifier ‘early, mid or late’ and the month are indicated.
Patients’ initials (if used) have been altered.

CONFIDENTIALITY REMINDER
We all have a responsibility to ensure that any confidential information discussed during a Grand Rounds
remains that way.
Please ensure you are attending from an appropriate location and that this session can not be overheard by
unintended audiences.
No recording of any kind (audio, photo, video or other) is permitted.
Participant certificates will be based on the attendance list.
Anonymous evaluations will be collected using a survey monkey link which Krista
Hailstone will send via email to participants following the session.
Please use the “Chat” feature to ask questions or share comments you have
To unmute yourself click on this icon found at the bottom right hand corner of your
screen.
If you are having connectivity issues, try using ‘audio only’ by clicking on this icon to turn
your video off

A SHOCKING REVIEWELECTRICAL INJURIES

DISCLOSURES
None

OBJECTIVES
• Appropriately risk stratify electrocuted patients
• Identify sequelae and complications from electrocution
• Appropriately monitor patients with electrical injuries
• Identify potential long-term complications from electrocution
TYPES OF ELECTRICAL INJURIES
• Flash
• >50,000 C
• Superficial
• Flame
• +/- internal injuries
• Lightning
• True – Part of the electrical circuit
CASE #1 – MR. D.C. (CASE FROM LITERATURE)
• Huntsville ED, Mid July, 24 C, sunny, 38% humidity
• 47 YO M Hydro One worker, grabbed power line at work and fell. Complains of
pain to both hands and wrists and headache.
• HR: 112
• BP: 136/93
• RR: 20
• SpO2: 98%


RISK STRATIFICATION
• Voltage
• Low risk = <600 V
• Higher risk = >600 V
• AC vs DC
• Path of the current
• Duration of contact
• Degree of wetness/humidity in environment
• Cardiac risk factors

ELECTRICITY TERMINOLOGY REVIEW
• Voltage – force that causes the electrons to flow (Volts)
• Current – flow of the electrons (Amperes)
• Resistance – how much an object impedes the flow of electrons (Ohms)
• Frequency – for AC
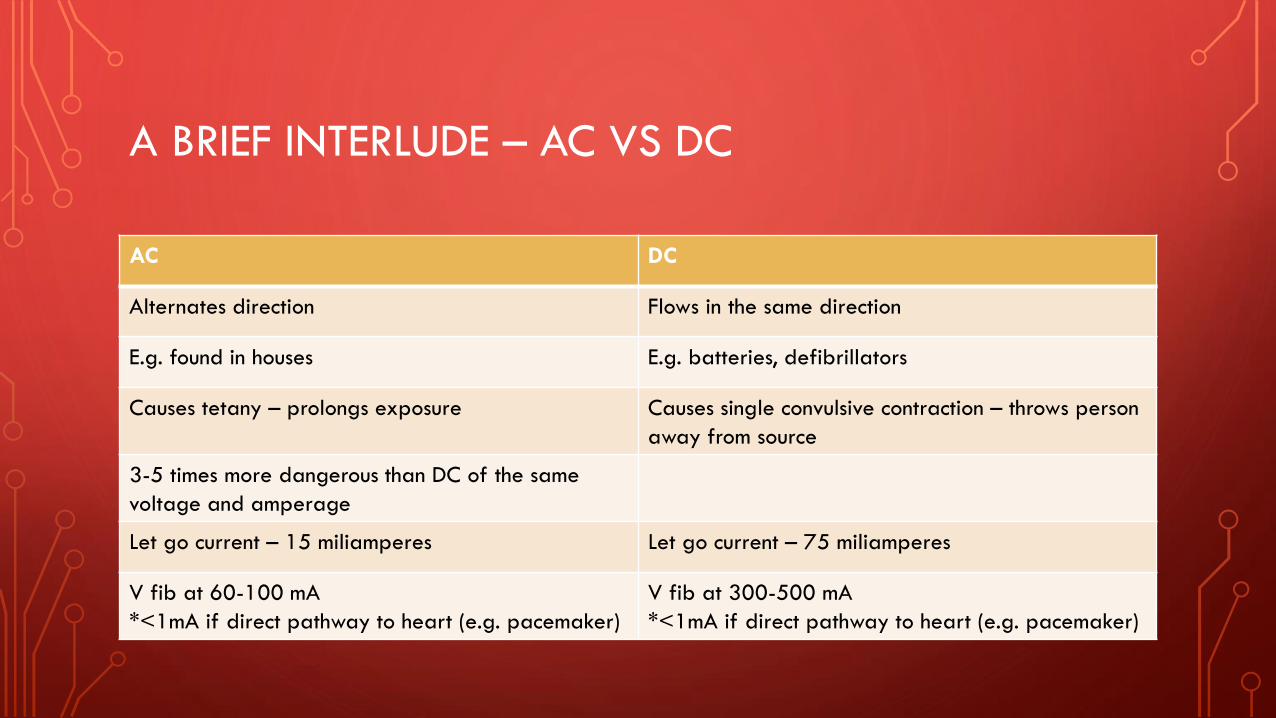
A BRIEF INTERLUDE – AC VS DC
AC DC
Alternates direction Flows in the same direction
E.g. found in houses E.g. batteries, defibrillators
Causes tetany – prolongs exposure Causes single convulsive contraction – throws person
away from source
3-5 times more dangerous than DC of the same
voltage and amperage
Let go current – 15 miliamperes Let go current – 75 miliamperes
V fib at 60-100 mA
*<1mA if direct pathway to heart (e.g. pacemaker)
V fib at 300-500 mA
*<1mA if direct pathway to heart (e.g. pacemaker)

0.1 mA to myocardium V fib
1000 A severe burn, loss of limb
>12,000 A (lightning) coma, severe burn, loss of limb
WHY RISK STRATIFYLow Risk (<600 V) High Risk (600 – 1000 V) Lightning
Exposure Household/office Industrial Environmental
Voltage (V) 110-240 600-1,000 Up to 1 billion
Current (A) <240 <1,000 >200,000
Contact Duration Prolonged Brief Milliseconds
Type of Current AC AC or DC DC
Cardiac Arrest Cause V fib V fib Asystole
Respiratory Arrest Cause Tetanic contractions of
resp. muscles
Indirect trauma or tetany Direct CNS injury
Muscle Contraction Tetanic DC: single; AC: tetanic Single
Burns Usually superficial Common, deep Rare, superficial
Rhabdo Common Very common Uncommon
Blunt Injury Cause Fall (uncommon) Muscle contraction, fall Blast effect, shock wave
Mortality (Acute) Low Moderate Very high

MR. D.C.
• Previously healthy, no meds, no surgeries
• High tension power lines
• Lost balance, grabbed wire with both hands
• 14,000 V
• Thrown from source, fell ~20 feet
• LOC at scene
• No CP or SOB
• GCS 15
• Hemodynamically stable
• Circumferential burns to bilateral wrists (full
and partial thickness)


SEQUELAE AND COMPLICATIONS
• General tissue damage
• Respiratory
• Cardiac
• Vascular
• Compartment Syndrome
• Nervous
• Rhabdomyolysis and AKI

HOW IT DAMAGES TISSUES
• Electrical heat (because of resistance) thermal injuries
• Electrochemical injuries
• Intrinsic electrical resistance of tissues
• Skin, bone, tendon >> nerves, blood etc.
• Dry vs. wet
• External Injuries DO NOT predict the severity of internal injuries

GENERAL TISSUE DAMAGE
• Hemolysis
• Protein coagulation
• Thrombosis
• Coagulation necrosis of muscles/
other tissues
• Muscle or tendon avulsion
• Joint dislocations
• Fractures
• Dehydration
• Ruptured tympanic membrane(s)

RESPIRATORY COMPLICATIONS
• Risk of respiratory arrest
• Chest wall muscle paralysis, or neurological
damage
• Lung tissue is a poor conductor
• Therefore often spared from damage
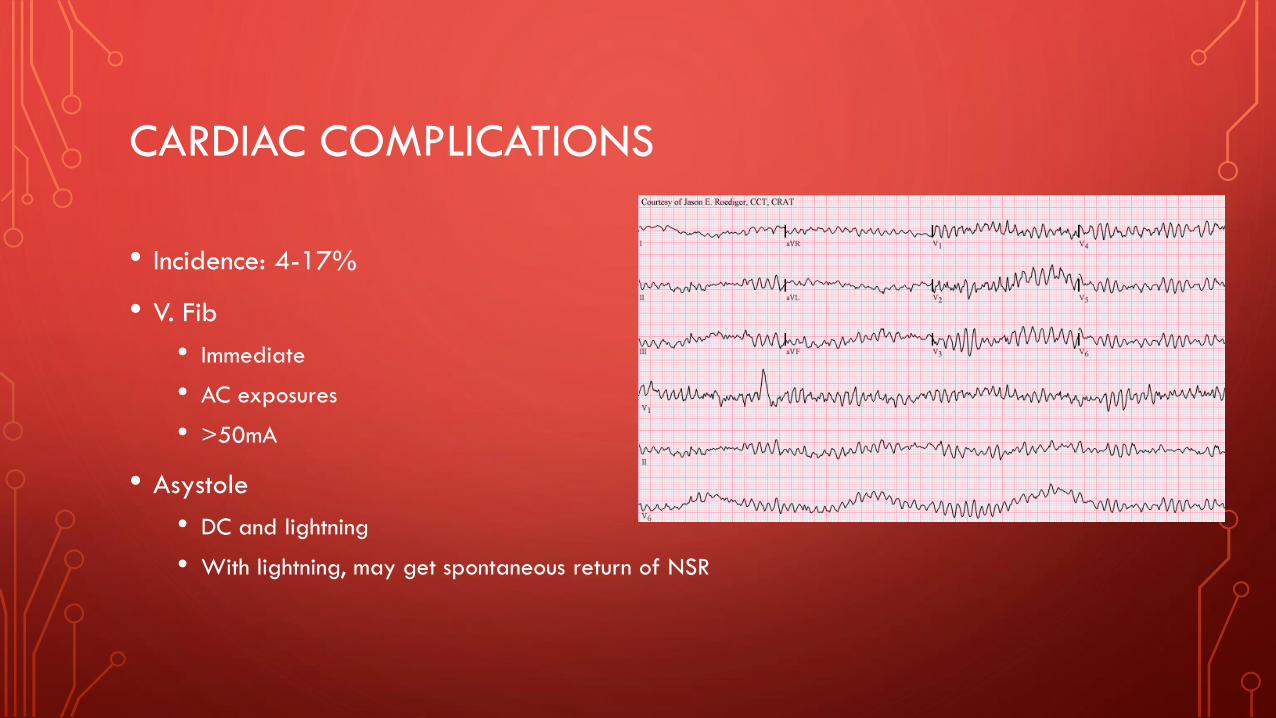
CARDIAC COMPLICATIONS
• Incidence: 4-17%
• V. Fib
• Immediate
• AC exposures
• >50mA
• Asystole
• DC and lightning
• With lightning, may get spontaneous return of NSR

CARDIAC COMPLICATIONS
• Necrosis of myocardium and/or dysrhythmias
• Most dysrhythmias benign
• First few hours post injury
• Bundle branch blocks
• AV blocks
• QT prolongation
• ST changes
• A. fib (most common)

CARDIAC COMPLICATIONS
TO TROP OR NOT TO TROP…THAT IS THE QUESTION…
• Rare cases of STEMI
• ?Higher risk for MI
• Electrical
• Thermal
• Thrombogenic
• Clinical presentation and pre-existing risk factors

VASCULAR INJURIES
• Varies based on vessel size
• Large arteries
• Medial necrosis aneurysm formation and rupture
• Small/medium vessels
• Coagulation necrosis

COMPARTMENT SYNDROME
• Direct and indirect injury to muscle, massive tissue edema, hypercoagulable
state
• Requires regular reassessment
• Significant pain on passive extension
• Rigid compartments
• Signs of poor perfusion
• Low threshold for fasciotomy

NERVOUS COMPLICATIONS
• Indirect injury
• Respiratory arrest
• Acute cranial nerve deficits
• LOC
• Seizures
• Transection of C4-C8

NERVOUS COMPLICATIONS
• Peripheral neuropathy
• Sensory and motor deficits
• Presentation may be delayed for days to months post injury
• Lightning-specific
• Transient autonomic dysfunction
• Hypoxic encephalopathy
• Intracerebral hemorrhage
• Cerebral infarction
• Spinal fractures

RHABDOMYOLYSIS AND AKI
• CK elevation
• Urine myoglobin
• Electrolyte disturbances
• AKI also from hypovolemia and hypotension

MR D.C. INVESTIGATION RESULTS
• Abnormal labs:
• CK – 32,000
• Myoglobinuria
• ECG – Sinus tachy (Rate 112)
• Imaging:
• Left frontal bone comminuted fracture
• Left subdural hematoma with 3mm shift


INITIAL MANAGEMENT OF ELECTRICAL INJURIES
• ACLS
• ATLS
• Burn Protocols

RHABDOMYOLYSIS AND AKI MANAGEMENT
• FLUID
• LR 300-500mL/hr
• Urine output >100cc/hr
• 1.5-2cc/kg/hr in kids
• Forced alkaline diuresis
• NaHCO3 to urine pH of >6.5
• Consider mannitol or Lasix
• Watch for hyperkalemia (q2hrs)

CARDIAC MONITORING
LOW VOLTAGE AND ASX
• No CP
• No syncope
• No monitoring
HIGH VOLTAGE WITH N ECG
• Debate
• 6-8 hours cardiac monitoring
BURN MANAGEMENT
• Fluids
• Early debridement and grafting
• Fasciotomies
• +/- Amputations
• Debridement of ischemic/necrotic tissue
• Tetanus

DISPOSITION
LOW VOLTAGE ASX
• Normal ECG
• Home
HIGH VOLTAGE
• Observe for 12 hours (with 6-8 on
cardiac monitoring)
• Referral to burn centre

MR D.C.
• Left frontal craniotomy
• CK peaked at 52, 235
• Bilateral compartment syndrome (hands)
• Lt hand amputated
• Bilateral pedicle groin flaps to wrists
• Hospital: 81 days, ICU 65 days, 7 visits to OR

DELAYED COMPLICATIONS
• Limb Ischemia
• Psychological
• Decreased concentration
• Difficulty sequencing events
• Memory issues
• PTSD
• Neurological
• Neuropathy
• Seizures
• Syncope
• Tinnitus
• Paresthesias
• Weakness
• Poor coordination
• Gait ataxia
• Ocular
• Cataracts
• Physical
• Pain
• Fatigue
• Contractures
• Muscle spasms
• Pruritus
• Headaches
• Fever, night sweats
• Joint stiffness
• Fractures (osteonecrosis)
• Gastric ulcers
CASE #2 (NOT A REAL CASE)
• 6 Huntsville Docs – Hiking in Algonquin
• Lightning strike
• Kirsten Unconscious, Rt lower leg deformity, head laceration, breathing with pulse
• Erin Conscious, clothes smoldering, complaining of back pain
• Nelson Unconscious, apneic, pulseless, blown Lt pupil
• Rich Conscious, open femur fracture, 1cm maple branch protruding from Rt side
chest


MULTIPLE CAUSALITY LIGHTNING STRIKE
• Reverse Triage
• No cardiac arrest, breathing spontaneously almost always survive
• Priority: Apneic or in cardiac arrest
• Fixed dilated pupil
• Asystole
• Respiratory arrest

CASE #3 (ALSO NOT A REAL CASE)
• 18 MO M who bit charging phone cord
• Charred corners of mouth, small tongue burn
• No other injuries, no concern for abuse

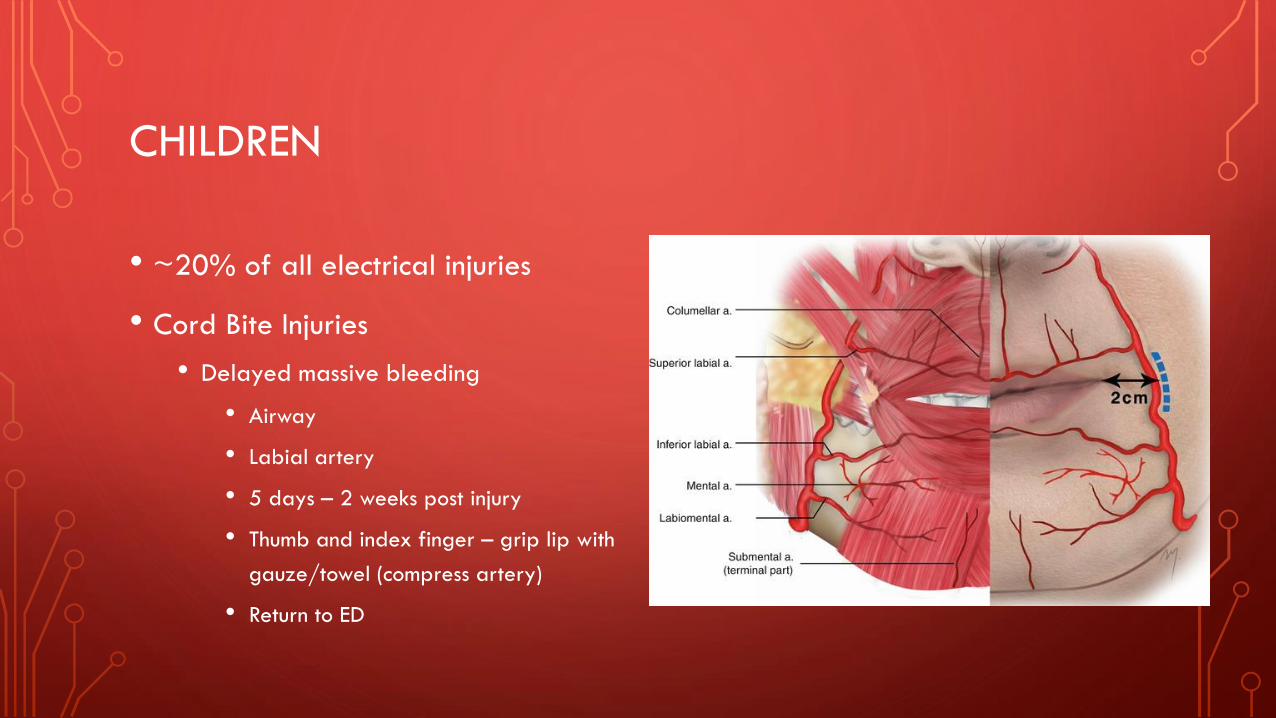
CHILDREN
• ~20% of all electrical injuries
• Cord Bite Injuries
• Delayed massive bleeding
• Airway
• Labial artery
• 5 days – 2 weeks post injury
• Thumb and index finger – grip lip with
gauze/towel (compress artery)
• Return to ED

SUMMARY
• ACLS and ATLS and burns
• Voltage, Duration, AC/DC
• Serial exams for compartment syndrome
• Check for rhabdo
• Fluid, Fluid, Fluid; titrate to urine output
and end-organ function
• Cardiac complications are rare, but:
• ECG all patients
• Trops only for risk factors and/or right
clinical presentation
• No investigations needed if:
• Asymptomatic + normal ECG
• Low-voltage exposure
• Unremarkable physical examination
• Discharge instructions
• Delayed complications
• Physical, psychological, neurological

REFERENCES
• Electrical Injuries - Injuries; Poisoning. (2020, January). Retrieved February 15, 2021, from
https://www.merckmanuals.com/professional/injuries-poisoning/electrical-and-lightning-injuries/electrical-injuries#:~:text=Electrical injury is
damage caused,cardiac arrhythmias and respiratory arrest.
• Helman, A. Electrical Injuries – The Tip of the Iceberg. Emergency Medicine Cases. June, 2019. https://emergencymedicinecases.com/electrical-
injuries. Accessed Feb 8, 2021.
• Jensen, J. D., Thurman, J., & Vincent, A. L. (2020). Lightning Injuries. STAT Pearls. PMID: 28722949
• Koumbourlis, A. C. (2002). Electrical Injuries. Critical Care Medicine, 30(11), S424-S430. doi:10.1097/01.CCM.0000035099.55766.EA
• Lee, J., Sinno, H., Perkins, A., Tahiri, Y., & Luc, M. (2020). 14,000 Volt Electrical Injury to Bilateral Upper Extremities: A Case Report. McGill
Journal of Medicine, 13(1). doi:10.26443/mjm.v13i1.245
• Nickson, C. (2020, November 03). Electrical Injury • LITFL • CCC Trauma. Retrieved February 20, 2021, from https://litfl.com/electrical-injury/
• Nickson, C. (2020, November 03). Lightning injury • LITFL • CCC Environmental. Retrieved February 20, 2021, from https://litfl.com/lightning-
injury/
• Pinto, D. S., & Clardy, P. F. (2021, January). Environmental and weapon-related electrical injuries (D. F. Danzl & M. E. Moreira, Eds.). Retrieved
February 15, 2021, from https://www.uptodate.com/contents/environmental-and-weapon-related-electrical-injuries?search=electrical
injuries&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
• Zemaitis, M. R., Foris, L. A., Lopez, R. A., & Huecker, M. R. (2020). Electrical Injuries. STAT Pearls. PMID: 28846317

QUESTIONS?